 Jule Heieis1,2,3*
Jule Heieis1,2,3* Ibrahim Duran3,4
Ibrahim Duran3,4 Eckhard Schönau3,4
Eckhard Schönau3,4 Christoph Fritzsche4Bettina Götz4Laura Kehe4Moritz Meier1Karoline Spiess4
Christoph Fritzsche4Bettina Götz4Laura Kehe4Moritz Meier1Karoline Spiess4 Wilhelm Bloch2
Wilhelm Bloch2 Jörn Rittweger1,3,†
Jörn Rittweger1,3,†
- 1Department of Muscle and Bone Metabolism, Institute of Aerospace Medicine, German Aerospace Center (DLR), Cologne, Germany
- 2Section Molecular and Cellular Sports Medicine, Institute of Cardiology and Sports Medicine, German Sports University, Cologne, Germany
- 3Department of Pediatrics and Juvenile Medicine, University of Cologne, University Hospital Cologne, Cologne, Germany
- 4Department of Pediatrics and Juvenile Medicine, UniReha Center for Prevention and Rehabilitation, Cologne, Germany
Introduction: Cerebral palsy (CP) is the most common disease affecting mobility among children. However, relatively little is known about the muscle phenotype and the resulting impairments in muscle function of this population. We therefore examined feasibility and acceptability of a muscle testing protocol that is based on the muscle examinations of astronauts and in bed-rest studies in children and adolescents with CP (clinical trial registry number DRKS00031107).
Methods: Twelve participants, aged between 8 and 18 years, with CP and age-matched able-bodied counterparts (Ctrl) have been included to the study. They completed testing procedures on two visits. Participants performed isometric maximum voluntary contractions, step and ramp contractions in plantarflexion on a custom build dynamometer. The tasks were visualized using a torque-controlled video game. We computed steadiness, defined as standard deviation of the fluctuations, and slope, as well as the achieved MVC. Data were statistically analyzed via Intraclass correlation coefficient (ICC) for between-visit analysis and Mann-Whitney U test for between-group analysis.
Results: One participant of the CP group was not able to perform the tasks and dropped out for the second visit. Especially younger children and children with cognitive impairments were not able to adequately answer the acceptance questionnaire. The MVC of Ctrl was higher in both visits and was excellently repeatable. During step contractions Ctrl showed lower fluctuations in both visits. Also, during ascending ramp contractions Ctrl showed less fluctuations but only at visit 1. During descending ramp contractions steadiness was better in Ctrl at both visits. Performance parameters were all poorly repeatable, because the CP group improved their performance in all tasks at visit 2.
Discussion: Application of our gamified muscle testing protocol was well acceptable and mostly feasible. Contrasting with constant isometric contractions and decreasing ramp contractions, the performance of children with CP during ascending ramp contractions improved to the level of control subjects within 2 visits. A crucial prerequisite to perform successful measurements are good cognitive skills and at least one familiarization visit.
Clinical Trial Registration: https://www.drks.de/DRKS00031107, identifier (DRKS00031107).
1 Introduction
Spasticity occurs secondary to lesions that affect the information stream from the upper to the lower motor neurons, as for example in persons affected by cerebral palsy (CP). Accordingly, these patients suffer from functional impairments in activities of daily living. Not all impairments can solely be explained by neural deficits. Secondary to the neuronal impairment, changes in the spastic muscle have been found. Cerebral palsy leads to decreased muscle belly length (1, 2), volume (1–4), cross-sectional area and thickness (3, 5–7), which correlate with decreases in muscle strength. The published literature is highly inconsistent with regards to effects on fiber pennation angle and length. At macroscopic level, the spastic muscle fiber is passively stiffer than the non-spastic muscle fiber. At single-fiber level, this is explained by alterations of the titin protein (8). Interestingly the exaggeration in passive stiffness becomes blunted at the level of fiber bundles, most likely due to the unorganized structure of the extracellular matrix (9). It has been found that changes in muscle architecture due to spasticity correlate with performance of different functional tasks (10). However, little is known about the direct impact of all these changes in muscle morphology on intramuscular strain-stress behaviour and function. Investigation on muscle function typically uses a testing protocol involving voluntary and controlled contractions. Based on the muscle examinations of astronauts and in bed-rest studies we created a measurement setup with a testing protocol including the essence of different examination procedures. This protocol includes the testing of three different isometric plantarflexion contractions—maximum voluntary contractions (MVC), ramp contractions and step contractions. Investigating plantar-flexors is of great interest because of the high prevalence of equinus (11) and the early manifestation of increased muscle stiffness within these muscles (12) in children suffering CP. Additionally, the triceps surae muscles play a key role during gait by controlling balance and velocity (13). Maximum voluntary contractions can be used to investigate muscle strength and are the basis for step and ramp contractions. Performing step contractions makes time-consuming measurements like muscle oxygenation or sonographic elastography possible. Ramp contractions on the other hand allow high resolution ultrasound imaging of muscle contraction at the muscle’s mid-belly to investigate fascicle kinematic or at the muscle-tendon-junction to measure tendon elongation and stiffness. Both contraction types can be used to analyse electromyographic signals of agonists and antagonists to investigate muscle activation patterns. Clearly, voluntary contraction assessments have potential not only for science but also for clinical application in cerebral palsy. However, it is not clear how well these patients can really perform the aforementioned types of voluntary contractions, given their specific disability. Therefore, we examined feasibility, repeatability and acceptability of our measurement setup and protocol in children and adolescents with CP and able-bodied controls.
2 Materials and methods
2.1 Study design
To judge feasibility and acceptability, the study was designed as parallel-group design with a group of CP patients and an age-matched group of able-bodied counterparts. To asses reproducibility, two visits were planned on separate days for each participant. The study setting was the UniReha’s Queen Rania Rehabilitation Center in Cologne. Prior to study commencement, it had been approved by the ethics committee of the university hospital cologne and registered with the German Register for Clinical Studies (DRKS) with the index DRKS00031107 (www.drks.de/DRKS00031107).
2.2 Participants
All participants gave informed, written consent before participation. In case of underaged participants, informed and written consent was obtained from their parents. The patient group consisted of twelve adolescents between 8 and 18 years with diagnosed unilateral or bilateral spastic cerebral palsy (CP). Participation was offered to the adolescents with CP upon recommendation of the treating physical therapists based on the patient’s cognitive and motor skills. Exclusion criterion was reduced knee and ankle joint mobility inhibiting the measurement position of knee flexion and neutral ankle position. For each patient healthy participants with matching sex and age (1 year) were recruited for the control group.
2.3 Measurement setup and protocol
The custom-built measurement device consisted of a adjustable seat and a fixed dynamometer (Figure 1). The dynamometer’s working principle was based on a foot plate that was rotatable around a fixed axis of rotation (AOR) and rested on a force sensor under the front foot. The participants’ medial malleolus was aligned with the dynamometer’s AOR. To achieve the anticipated measurement position, the seat platform’s height above the AOR was adjusted to the length of the shank (distance from medial malleolus to medial knee joint cleft). The distance from the seat to the dynamometer was adjusted until the shank was oriented vertically (neutral ankle joint angle). The heel was prevented from lifting during force generation by stabilizing the distal thigh from the ventral side by a padded metal bar, serving as resistance (Figure 1). A soft foam pad in front of the foot served as landmark for the foot position, in case the foot has been moved between trials. The foot has not been fixated further to allow motion in case of arising spasms. To increase acceptability and compliance of the participants the whole measurement was gamified. The dynamometer part of the measurment device was covered in a rocket-style aluminium shell and all tasks were visualized in a torque controlled video game in which a digital rocket rose up with increasing plantarflexion torque.

Figure 1. Measurement setup. Force, EMG and goniometer signals are collected simultaneously. The force signal is additionally transmitted to control the video game.
There were three tasks given with three trials per task, each of them demanding different types of isometric plantarflexion contractions. In participants with unilateral CP, the affected leg was chosen, while the leg with better movement was chosen in patients with bilateral CP. The control group participants’ right leg was examined. The first task was the maximum voluntary isometric contraction (MVC). Participants were asked to drive the game rocket as high as possible, meaning to physically exert their largest possible torque. During trial 2 and 3, the maximum previously achieved torque was always displayed. From the overall maximum achieved, submaximal levels were defined at , , and MVC. In three different trials these levels were presented for 16 s as horizontal stars in the second task “step contraction.” To accomplish this task, participants were asked to collect 30 stars, that were arranged in a step-wise fashion, with five stars at rest, followed by 20 stars at the desired contraction level, back to five stars at rest. During the third and last task “ramp contractions” participants performed continuously increasing and decreasing isometric contractions for eight seconds each from rest to MVC and back. This task was visualized by stars arranged in a triangular shape (Figure 1).
The repeatability measurements were taken after an interval of at least 24 h.
2.4 Data acquisition
At the beginning of the first visit height and weight data, as well as the Achilles tendon lever arm (ATLA) length were collected. Afterwards the participants have been equipped with electromyography (EMG) electrodes at the soleus, lateral gastrocnemius and tibialis anterior muscle according to SENIAM standards (www.seniam.org) and with a goniometer (Noraxon U.S.A. Inc., Scottdale, United states) at the ankle joint. Force, EMG, and goniometer signals as well as a trigger signal of a custom-built hand trigger have been transmitted to a Noraxon system (Noraxon U.S.A. Inc., Scottdale, United states) and recorded during the whole measurement using the software myoResearch®version 1.08 Master Edition and a sampling rate of 1,000 Hz. The hand trigger was pressed at the beginning and end of each trial.
2.5 Data processing
All data processing has been performed using the programming language R version 4.3.2 (www.r-project.org) with the RStudio development environment (14). Force and joint angle signals were filtered using a fourth order Butterworth low-pass filter with a cutoff frequency of 5 Hz. The force signal was converted to Nm via calibration with a 1 m lever and a 10 kg mass. Afterwards the data files of each subject cut into individual trial recordings with the hand trigger signals. Resting torque was defined in each of the three MVC trials as mean torque of a manually defining 200 ms period before contraction with no visible contraction in the EMG signals. The MVC torque of each trial was calculated as average torque of the torque plateau. The plateau was defined as the area where the torque reached over 90% of the maximal torque. The maximal MVC value out of the three trials was then set as total MVC to calculate the contraction levels for further trials of tasks 2 and 3. For all tasks performance parameters have been calculated and statistically analyzed. In case of comparable performances between groups, additional muscle parameters about fascicle mechanics and muscle activation have been analyzed.
2.5.1 Performance assessment
To quantify the performance in tasks 2 and 3, the torque parameters steadiness and slope have been calculated. For task 3 the performance parameters have been calculated for the ascending and descending part of the ramp separately. Steadiness was defined as the standard deviation of the difference between actual torque and regression line. This way fluctuations of the torque could be quantified while time-shifting was neglected (Figure 2). To quantify, if despite fluctuations the dictated slope has been achieved, the regression line through the torque data has been calculated additionally. A perfect slope was 0%/s for task 2 and 12%/s and 12%/s for the ascending and descending part of task 3, respectively.
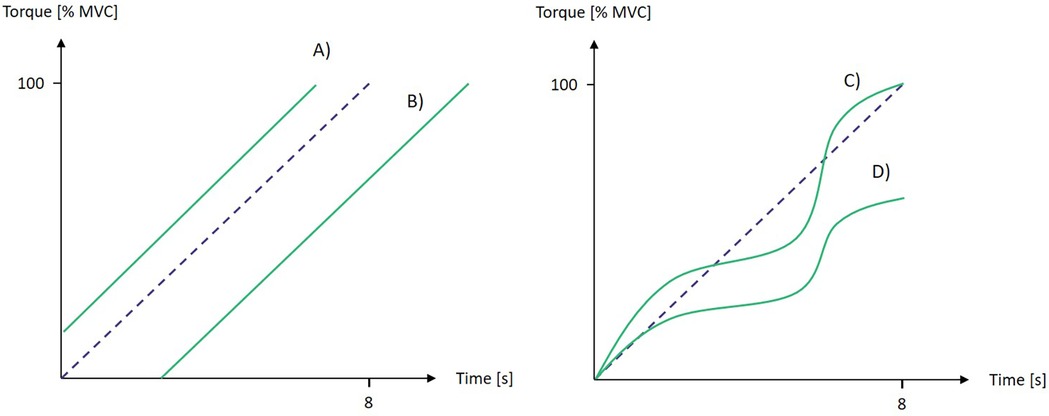
Figure 2. Influence of exemplary torque graphs (red lines) during ascending ramp contractions on performance parameters slope and steadiness. The blue dashed line indicates the prescribed path. (A) perfect steadiness and slope. (B) perfect steadiness and slope. (C) poor steadiness but perfect slope. (D) poor steadiness and slope.
2.5.2 Acceptance
After each task, participants were asked to rate the performed task on a scale from 1 to 5 for fun, difficulty and excitement. The scale was visualized on a board with smileys ranging from happy to sad emotions representing scores 1 to 5, respectively.
2.6 Statistical analyses
Statistical analyses followed the “per-protocol” principle, i.e., incomplete data sets were discarded. Repeatability of the MVC and the performance parameters steadiness and slope has been tested using the two-way agreement-type intraclass correlation coefficient (ICC). Between-group comparison within the visits has been performed using Mann-Whitney U-test with Holm correction for multiple comparisons. The statistical significance level was set to 5%.
3 Results
One participant of the CP group was not able to perform the tasks due to limited cognitive abilities and dropped out for the second visit. All other participants completed both visits successfully. Incomplete data sets were found in two further participants of the CP and one participant of the control group due to failures of the recording systems (Figure 3).
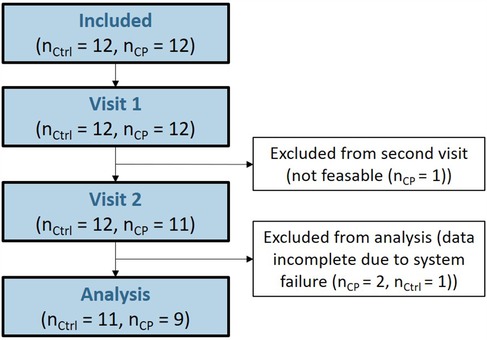
Figure 3. CONSORT-style flow chart.
With the remaining 20 participants we found no differences in age, female:male ratio, height and weight between groups (Table 1). Acceptability data collection was stopped after four participants, as these younger children were not able to understand and answer the questionnaire adequately.
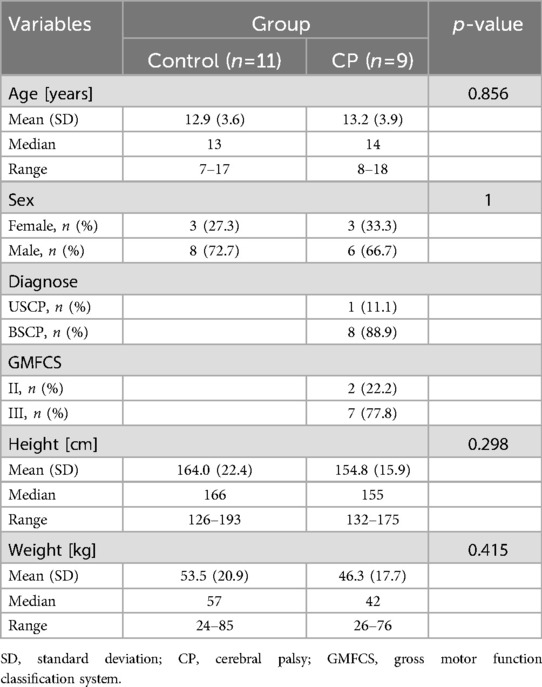
Table 1. Demographics.
3.1 Feasibility
During the first visit, participants of the CP group reached a MVC of 1.0 g while the control group reached 4.3 g (). Similar results have been found for visit two (1.4 g vs. 4.9 g, ). Plantarflexion torque fluctuated more in the CP group in all tasks at visit 1. During step contractions CP group’s torque fluctuated by 52.2% MVC vs. 6.1% MVC in the control group (). Similar differences could be seen during ascending ramp contractions (26.3% MVC vs. 7.0% MVC, ) and descending ramp contractions (34.1% MVC vs. 8.1% MVC, ). At visit 2 group differences in steadiness decreased but remained significant for step contractions (20.6% MVC vs. 5.3% MVC, ) and descending ramp contractions (15.9% MVC vs. 7.7% MVC, ) but vanished for ascending ramp contractions (Figure 4). There were no significant differences between groups in slopes during all tasks and visits.
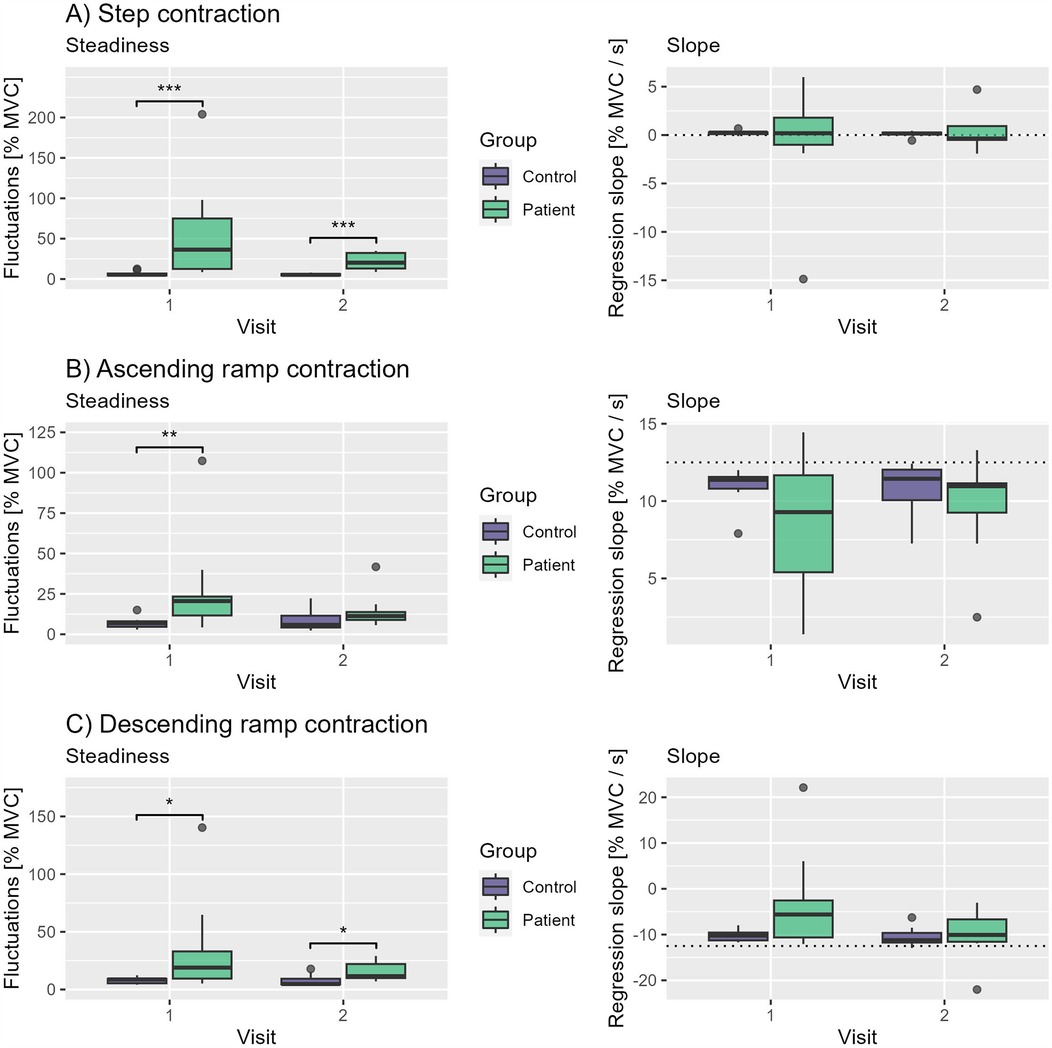
Figure 4. Boxplots of steadiness and slopes of both groups and visits during (A) step contractions, (B) ascending ramp contractions and (C) descending ramp contractions. Significance markers: * , ** and *** .
3.2 Repeatability
MVC showed excellent repeatability between the measurements with an ICC of 0.94 (), whilst all performance parameters of all tasks showed poor ICCs (Table 2). Consistent with the previously mentioned better performance of the control group during visit 1 and 2, we see only little differences in fluctuations between visits in this group (Figure 5). By contrast, almost all participants of the CP group improve their performance during step and ramp contractions from visit 1 to visit 2 (Figures 5B–D). Despite the lack of any significant group differences between slopes in both visits, there is a visible trend in all tasks of the group to converge (Figure 4).

Table 2. Between-visits analysis of MVC and performance parameters.
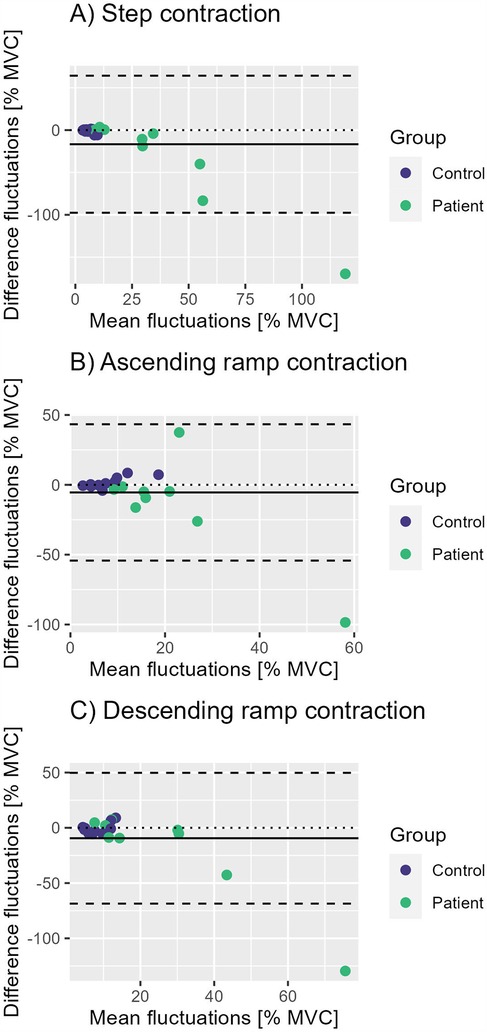
Figure 5. Bland-Altman plots for repeatability of steadiness during (A) step contractions, (B) ascending ramp contractions and (C) descending ramp contractions. The solid line represents the mean fluctuations of all participants, the dashed lines mean 1.96 standard deviations.
4 Discussion
Application of our Space-gamified muscle testing protocol turned out to be feasible in most participants and in most of its aspects. A crucial prerequisite to perform successful measurements were good cognitive skills and at least one familiarization visit. Although quantification of acceptance was not feasible with the used questionnaire, subjectively all participants accepted the measurement procedure exceptionally good and voluntarily repeated the testing for visit 2. While MVC testing was feasible and repeatable, the performance of the ramp and step contraction improved during visit two in the CP group. Contrasting with step contractions and decreasing ramp contractions, the performance of children with CP during ascending ramp contractions improved even to the level of control subjects.
This learning effect limits the application of the procedure to investigate interventions. With one familiarization visit, however, the ascending ramp contraction can be applied as measuring method during a second visit. As the measurement setup is at the moment, it requires multiple devices (Game, EMG, Dynamometer, Ultrasound, Trigger) at the same time which makes a rather rapid and easy execution difficult. However, a reduction to just the game run by the dynamometer signal is relatively simple and could be implemented in a clinical setting. A measurement system of choice could potentially be added as needed. The game itself applied to another dynamometer would even allow for measurements of other muscle groups.
The learning effect also shows that the procedure has therapeutic potential to improve contraction control in patients with CP. Especially the gamification of the measurement could be particularly motivating, as gaming technologies grow in popularity in neuropediatric rehabilitation to increase patient compliance (15).
The successfully performed ascending ramp contractions can retrospectively be analyzed in regards to different muscle parameters. The recorded EMG signals can be used to investigate muscle activation and co-contraction from 0% to 100% MVC. From the simultaneously recorded ultrasound sequences architectural parameters like fascicle length, pennation angle and muscle thickness can be extracted to gain insight into the muscle’s mechanics. In future studies the successful application of testing ascending ramp contractions makes additional analyses possible. In 2021 Schranz et al. investigated, inter alia, muscle-tendon-junction displacement to draw conclusions about Achilles tendon lengthening and stiffness. An application of this method during slow and continuous ascending ramp contractions could improve the method, because the slowed down contraction allows higher resolution ultrasound imaging. Ramp contractions could also be used to apply quick release protocols.
In the next step the collected data of muscle activation and architecture will be analyzed retrospectively for the evidentially feasible ascending ramp contraction to define characteristic muscle parameters of patients with CP. Additionally, a currently running follow-up study applies the feasible assessment of MVC and ramp contractions to investigate the effects of whole-body vibration training with 20 subjects and three visits.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://doi.org/10.6084/m9.figshare.27301788.v1.
Ethics statement
The studies involving humans were approved by Ethics Committee of the University Hospital Cologne, Kerpener Str. 62, 50937 Köln, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
JH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. ID: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. ES: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. CF: Investigation, Writing – original draft, Writing – review & editing. BG: Investigation, Writing – original draft, Writing – review & editing. LK: Investigation, Writing – original draft, Writing – review & editing. MM: Formal analysis, Investigation, Writing – original draft, Writing – review & editing. KS: Writing – original draft, Writing – review & editing. WB: Supervision, Writing – original draft, Writing – review & editing. JR: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study has been conducted using only internal funding of the Institute of Aerospace Medicine and has been approved by the Cologne University Hospital’s ethics committee. The participants and their parents gave their informed consent prior to their inclusion in the study.
Acknowledgments
We want to thank all participants, their parents and the whole team involved for their motivation and dedication to carry out this study. Special thanks goes to Professor Jörn Rittweger, who initiated the project and drove it forward with particular commitment. To the best of the co-authors’ knowledge, author Jörn Rittweger fulfils the authorship criteria in line with Frontiers policy. He will be dearly missed.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Malaiya R, McNee AE, Fry NR, Eve LC, Gough M, Shortland AP. The morphology of the medial gastrocnemius in typically developing children and children with spastic hemiplegic cerebral palsy. J Electromyogr Kinesiol. (2007) 17:657–63. doi: 10.1016/j.jelekin.2007.02.009
2. Oberhofer K, Stott N, Mithraratne K, Anderson I. Subject-specific modelling of lower limb muscles in children with cerebral palsy. Clin Biomech. (2010) 25:88–94. doi: 10.1016/j.clinbiomech.2009.09.007
3. Elder GC, Kirk J, Stewart G, Cook K, Weir D, Marshall A, et al. Contributing factors to muscle weakness in children with cerebral palsy. Dev Med Child Neurol. (2003) 45:542–50. doi: 10.1111/j.1469-8749.2003.tb00954.x
4. Shortland A. Muscle deficits in cerebral palsy and early loss of mobility: can we learn something from our elders? Dev Med Child Neurol. (2009) 51:59–63. doi: 10.1111/j.1469-8749.2009.03434.x
5. Mohagheghi AA, Khan T, Meadows TH, Giannikas K, Baltzopoulos V, Maganaris CN. Differences in gastrocnemius muscle architecture between the paretic and non-paretic legs in children with hemiplegic cerebral palsy. Clin Biomech. (2007) 22:718–24. doi: 10.1016/j.clinbiomech.2007.03.004
6. Bandholm T, Magnusson P, Jensen BR, Sonne-Holm S. Dorsiflexor muscle-group thickness in children with cerebral palsy: relation to cross-sectional area. NeuroRehabilitation. (2009) 24:299–306. doi: 10.3233/NRE-2009-0482
7. Moreau NG, Teefey SA, Damiano DL. In vivo muscle architecture and size of the rectus femoris and vastus lateralis in children and adolescents with cerebral palsy. Dev Med Child Neurol. (2009) 51:800–6. doi: 10.1111/j.1469-8749.2009.03307.x
8. Fridén J, Lieber RL. Spastic muscle cells are shorter and stiffer than normal cells. Muscle Nerve. (2003) 27:157–64. doi: 10.1002/mus.10247
9. Lieber RL, Runesson E, Einarsson F, Fridén J. Inferior mechanical properties of spastic muscle bundles due to hypertrophic but compromised extracellular matrix material. Muscle Nerve. (2003) 28:464–71. doi: 10.1002/mus.10446
10. Schranz C, Kruse A, Tilp M, Svehlik M. Is there a relationship between muscle-tendon properties and a variety of functional tasks in children with spastic cerebral palsy? Gait Posture. (2021) 85:14–9. doi: 10.1016/j.gaitpost.2021.01.009
11. Wren TA, Rethlefsen S, Kay RM. Prevalence of specific gait abnormalities in children with cerebral palsy: influence of cerebral palsy subtype, age, and previous surgery. J Pediatr Orthop. (2005) 25:79–83. doi: 10.1097/00004694-200501000-00018
12. Willerslev-Olsen M, Choe Lund M, Lorentzen J, Barber L, Kofoed-Hansen M, Nielsen JB. Impaired muscle growth precedes development of increased stiffness of the triceps surae musculotendinous unit in children with cerebral palsy. Dev Med Child Neurol. (2018) 60:672–9. doi: 10.1111/dmcn.13729
13. Honeine JL, Schieppati M, Gagey O, Do MC. The functional role of the triceps surae muscle during human locomotion. PLoS One. (2013) 8:e52943. doi: 10.1371/journal.pone.0052943
14. RStudio Team. RStudio: Integrated Development Environment for R. Boston, MA: RStudio, PBC (2023).
Keywords: cerebral palsy, muscle, spasticity, contraction, muscle control, gamification, biofeedback, neurorehabilitation
Citation: Heieis J, Duran I, Schönau E, Fritzsche C, Götz B, Kehe L, Meier M, Spiess K, Bloch W and Rittweger J (2025) A space-gamified approach to examine muscle contraction behaviour in children and adolescents with spastic cerebral palsy: feasibility, acceptability and repeatbility. Front. Pediatr. 13:1520162. doi: 10.3389/fped.2025.1520162
Received: 30 October 2024; Accepted: 16 May 2025;
Published: 5 June 2025.
Edited by:
Dejan Nikolic, University of Belgrade, SerbiaReviewed by:
Oussama Abousamra, Children’s Hospital of Los Angeles, United StatesAshok Kumar Banskota, Hospital and Rehabilitation Centre for Disabled Children, Nepal
Copyright: © 2025 Heieis, Duran, Schönau, Fritzsche, Götz, Kehe, Meier, Spiess, Bloch and Rittweger. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jule Heieis, SnVsZS5IZWllaXNAZGxyLmRl
†Deceased on April 21st 2025