 Alejandro Acosta-Rodríguez†
Alejandro Acosta-Rodríguez† Sandra A. Reza-López†
Sandra A. Reza-López† César R. Aguilar-Torres†
César R. Aguilar-Torres† Luis C. Hinojos-Gallardo†
Luis C. Hinojos-Gallardo† Dora V. Chávez-Corral*†
Dora V. Chávez-Corral*†
- Department of Embryology, Facultad de Medicina y Ciencias Biomédicas, Universidad Autónoma de Chihuahua, Chihuahua, México
Objective: External ear anomalies may lead to conductive hearing loss with significant childhood disability, psychological distress, anxiety, social avoidance, and behavioral problems. The aim of this study is to compile and review published literature on the frequency of isolated and non-isolated external ear anomalies, their associated factors, and associated malformations/deformations in non-isolated cases.
Methods: We conducted a systematic review in PubMed, Google Scholar, and Science Direct searching for any type of article (excluding reviews and meta-analyses) reporting isolated and non-isolated external ear anomalies in humans. Two authors extracted the information according to the main variables of interest according to PICO criteria. Details of studied population and main findings were also obtained (malformation type, unilateral or bilateral malformations and associated factors).
Results: Twenty-six studies met eligibility criteria to be included in this review. Anotia/microtia was the most reported malformation, more frequently found in males, mostly unilateral; being the right ear the most affected, and more frequent in Hispanic population. Associated factors for external ear anomalies included parental age, maternal education, multiple pregnancies, high maternal body mass index and diabetes, pregnancy, and perinatal complications (low birth weight, prematurity, threatened abortion, etc.), twining, and chemical/drug exposure. The most reported malformations and syndromes associated with congenital external ear defects included: skull/face anomalies, cleft lip/palate, congenital heart defects, musculoskeletal malformations of skull, face and jaw, Treacher-Collins, OAVS (oculo-auriculo-vertebral spectrum), and trisomy 18, 13 and 21.
Conclusion: Congenital external ear anomalies can occur isolated or associated with other malformations or syndromes. Environmental, socioeconomic, and cultural factors may partially explain the variation across populations for congenital external ear anomalies. Depending on their type and severity, they can lead to speech impediments and childhood disability, particularly in bilateral cases, highlighting the relevance of early detection and repair to avoid childhood disability.
1 Introduction
The incidence of ear malformations has been informed in approximately 1 per 3,800 newborns (1), while the incidence of external ear malformations occurs in 1 per 6,000 (2) to 6,830 newborns (3). Around 30% of them are associated with syndromes involving additional malformations and/or functional loss of organs and organ systems, such as Treacher-Collins, oculo-auriculo-vertebral spectrum or OAVS (also referred as Goldenhar syndrome or hemifacial microsomia), Crouzon, Apert, Klippel-Feil, Wildervanck, van der Hoeve-de-Kleyn, Albers-Schönberg, Patau, Edwards, Down, and 18q syndromes (4, 5). They can either affect the ear orientation, position (low set ear), size and/or shape of the auricle (microtia, cup ear, unfolded helix/Stahl ear); or result in a completely absent ear (anotia), while the middle ear can be atretic or hypoplastic. Minor malformations, such as ear tags, ear sinus and ear pits, may be also found (4). Atresia of the outer ear canal has been rarely observed in patients with a normal auricle (6).
Congenital anomalies of the external ear are genetic or acquired inborn anomalies of the auricle (4). They can be classified as deformations and malformations (7). A deformed ear is presented with fully developed components, with a misshaped auricle or pinna with intact cartilage and skin; while a malformed ear shows auricle alterations due to a partial or complete absence of cartilage and/or skin, because of underdevelopment during embryogenesis (8, 9). Most ear anomalies are acquired and originate from external forces applied to normal ear components in utero or postnatally (10), or by exposure to exogenous factors during the first trimester of pregnancy, such as: (a) infections, mainly viral, confirmed for rubella, cytomegalovirus, and herpes simplex virus; and possible for measles, mumps, hepatitis, poliomyelitis, chickenpox, Coxsackie virus and ECHO virus, and for toxoplasmosis, and syphilis; (b) chemical agents and medical drugs, such as thalidomide, quinine and aminoglycoside antibiotics, diphenylhydantoin, trimethadione, valproic acid, and excessively high doses of retinoic acid; (c) malnutrition and vitamin A deficiency during pregnancy; (d) Rh incompatibility; (e) hypoxia; (f) bleeding during the first trimester of pregnancy and disturbances of metabolism, such as diabetes. Environmental factors, including irradiation, atmospheric pressure changes, and noise exposure, should be also taken into consideration (1, 11–13). In many cases, however, the actual cause is unknown (14), because clinical and anamnestic data of exposure and exogenic influences are often missing or unclear (4).
Microtia/anotia is probably the most extensively studied external ear malformation. A recent metanalysis by Huang et al. (15), identified multiple risk factors with significant association for isolated microtia, including parental demographics, prenatal and perinatal characteristics (birth weight, chemical/medicinal exposure, infections), as well as familial history of ear malformations, among others, emphasizing the importance of identifying them to bring awareness and reinforce prevention. Expanding the scope for other congenital ear anomalies, that have received less attention and might also have consequences later in life, including non-isolated cases published reports, as well as exploring their associations with other congenital anomalies, could provide a more compelling review.
External ear anomalies could cause conductive hearing loss with a significant childhood disability, especially in bilateral cases (16, 17). Additionally, their effect on appearance may lead to psychological distress, anxiety, social avoidance, and behavioral problems (18). The purpose of this study was to compile and review published literature of isolated and non-isolated external ear anomalies, their characteristics, associated factors, and associated malformations/deformations in non-isolated cases.
2 Materials and Methods
2.1 Search strategy
A systematic literature review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (19). Studies reporting risk factors for isolated and non-isolated congenital external ear anomalies were independently selected by two reviewers through a manual screening process in January 2025 using the advanced search tools from PubMed, Google Scholar and ScienceDirect databases.
In PubMed, the search terms used were “Outer Ear Malformations” OR “Outer Ear Defect” OR “External Ear Defect” OR “Microtia/Anotia” OR “Aural Atresia” contained in title/abstract, using the Boolean operators “NOT” to exclude “Reconstruction Surgery”, “Implants”, “Middle Ear”, “Inner/Internal Ear” and “Deafness”. In Google Scholar, the search terms were “Outer Ear Malformations” OR “Outer Ear Defects” OR “Microtia/Anotia” OR “Aural Atresia” in title, and without the words “Deafness, Mice, Rats, Inner [ear] & Internal [ear]”. Finally, in ScienceDirect, the terms “Ear Malformations” OR “Microtia/Anotia” OR “Aural Atresia” in the title, abstract or author-specified key words were searched, using the same restriction words than those used in Google Scholar.
The filters applied in PubMed were article type (any type, excluding reviews and meta-analyses) and species (humans); in ScienceDirect they were article type (any type, excluding reviews and meta-analyses) and subject area (medicine); in Google Scholar, articles were manually selected excluding review articles and meta-analyses. In all databases, filters for year (2000 to 2025) and language (English, Spanish, French, Italian and Portuguese) were also applied. Duplicates were manually removed.
2.2 Eligibility criteria
Research articles that included any type of external ear anomalies, isolated and non-isolated, and reporting association measures with risk factors or results of comparison tests (relative risk, odds ratio, and P-value), in humans were included. Articles referring only to the middle and/or inner ear malformations, tumors, trauma, surgery, animal models, and specific syndromes were excluded, as well as case reports.
2.3 Data extraction
The title, authors, year of publication, language, and place of publication were obtained and registered. The information on the main variables of interest was extracted according to PICO (Population, Intervention, Comparison and Outcome) criteria as follows: [1] Population (individuals diagnosed with any outer ear anomalies); [2] Exposure -instead of intervention- (at least one identifiable risk factor for external ear anomalies); [3] controls in case control studies (individuals with unknown outer ear malformations and/or history of exposure), and [4] Outcomes: main findings, both descriptive (malformation type, unilateral or bilateral malformations), associated factors and association measures (relative risk, RR; odds ratio, OR) or those reporting a P-value for group comparisons, and associated deformations/malformations and syndromes, when reported.
3 Results
A total of 1,266 studies were identified −880 from Google Scholar, 158 from PubMed, and 228 from ScienceDirect. After screening of titles and abstracts, removing duplicates, and verifying eligibility criteria, 26 articles remained to be included in this review (Figure 1).

Figure 1. Flow diagram of publication selection process in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Source: Page et al. (19).
Sixteen studies were case-control studies (20–35), eight were retrospective reviews (36–43), one was a cohort study (44), and other was a cross-sectional study (45). Ten were studies from the U.S.A (22, 23, 25, 26, 29, 31, 33, 36–38), ten from China (21, 27, 28, 30, 32, 39–43), three from Mexico, Colombia, and South America (20, 24, 34), and the rest from Israel, Japan, and South Korea [n = 1, each] (35, 44, 45), as shown in Table 1. All studies were published in English.

Table 1. Characteristics of studies included in the review.
The reported external ear anomalies and their frequency by sex, laterality, and ethnicity are shown in Table 2. The anotia/microtia was the most studied malformation (20–31, 33–43, 45). A study reported low set ears as the most common malformation (44), and two studies reported the frequency of deformations: Stahl ear and preauricular tags (34, 44).

Table 2. External ear anomalies and their association with sex, and laterality.
From the selected studies, twenty-three reported subject sex, showing greater occurrence of ear anomalies in male population (20, 21, 24–33, 35–45). Fourteen studies reported laterality (20, 24, 27–29, 33, 35–38, 40, 43–45), from which thirteen reported that congenital external ear anomalies were mostly unilateral, and ten being the right ear the most affected (20, 24, 27, 28, 33, 35, 37, 40, 43, 45). Only one study reported higher prevalence for bilateral anomalies (44). Finally, eleven studies classified cases by ethnic background: nine observed higher frequency among Hispanic population, compared to non-Hispanic Caucasians and African Americans (22, 23, 25, 26, 29, 31, 33, 36, 38), and two studies focused on Jewish, Arab (44), Pacific Islanders and Filipino descendants (37) Table 3.
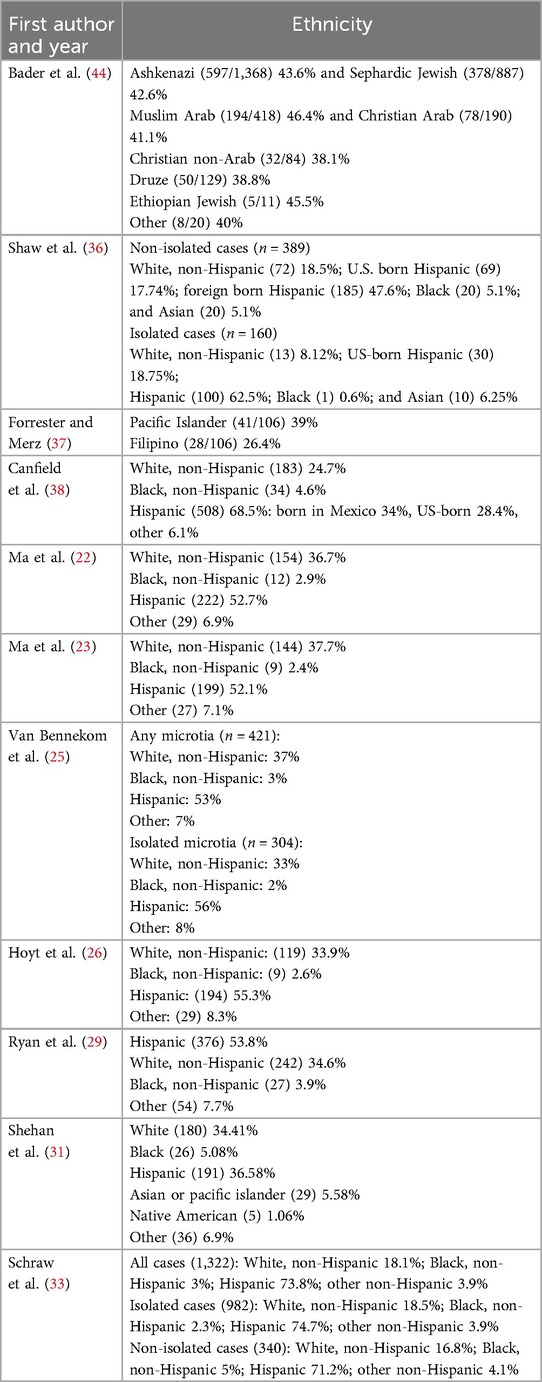
Table 3. External ear anomalies and their association with ethnicity.
3.1 Associated factors
Some authors associated congenital anomalies of the external ear with parental age, race/ethnicity, education level, residential area, infant sex, multiple pregnancies, twining, abortions, obesity, pregnancy and perinatal complications, and chemical/medication exposure. Risk factors by characteristics (demographics) and parental health behaviors are shown in Table 4, risk factors by pregnancy characteristics and parental clinical features are shown in Table 5, and risk factors of studies reporting microtia/anotia compared by all, isolated, and non-isolated cases are shown in Table 6.

Table 4. Risk factors for external ear malformations classified by demographics and parental health behavior.
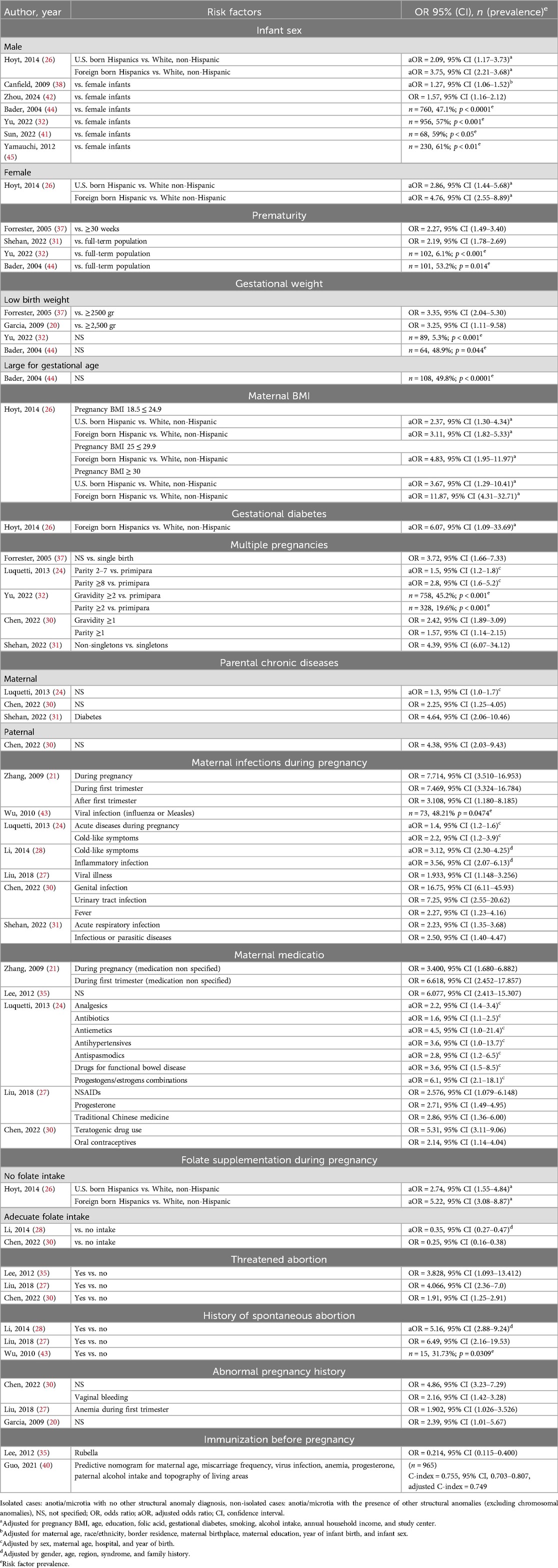
Table 5. Risk factors for external ear malformations classified by pregnancy and parental clinical features.
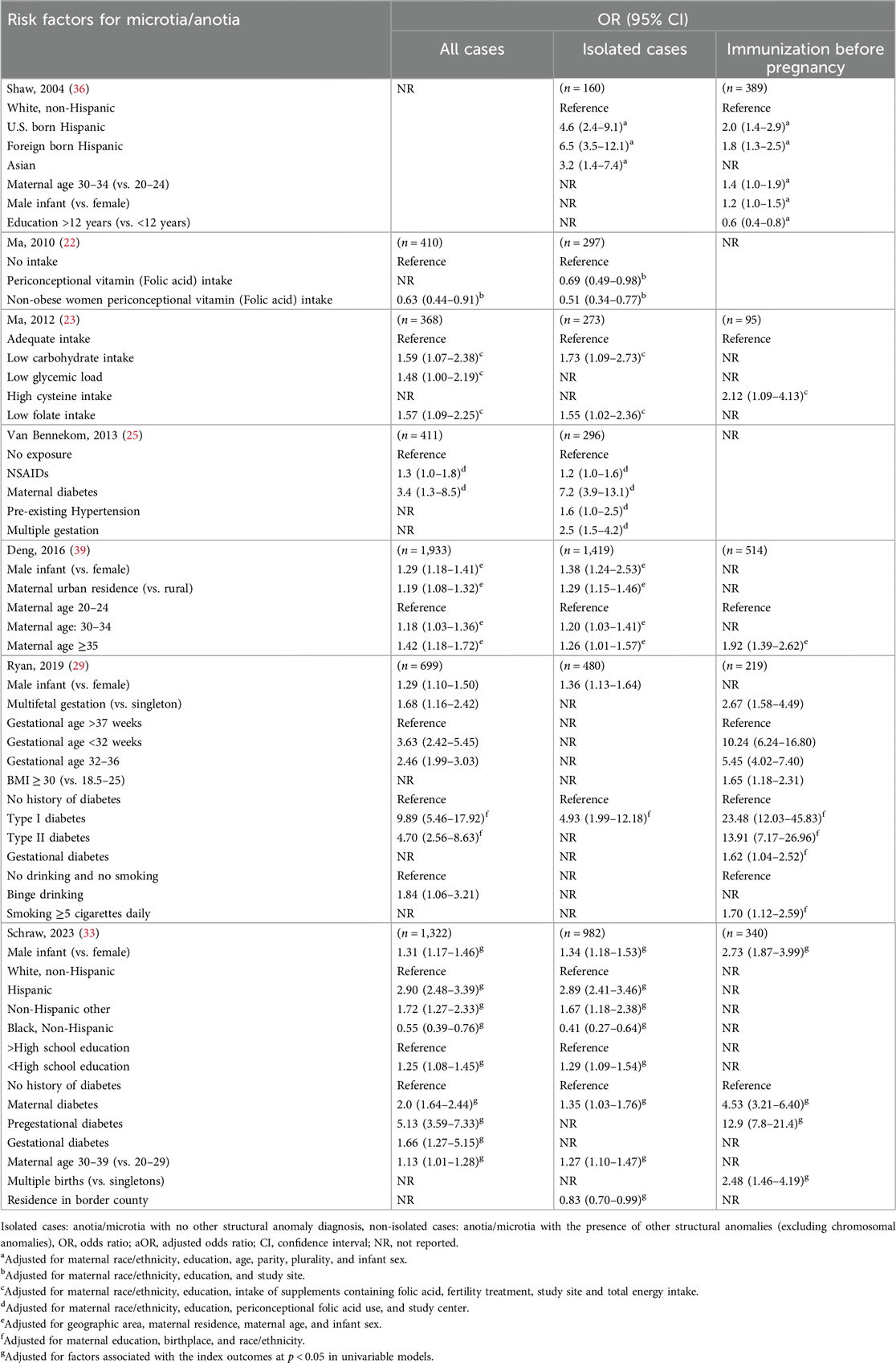
Table 6. Risk factors for microtia/anotia compared by all, isolated, and non-isolated cases.
Risk factors by demographics and parental health behaviors include:
(a) Parental age. One study reported that Hispanic mothers have higher risk of congenital ear malformations, compared to non-Hispanic white mothers for almost all age groups (26). Conversely, maternal, and paternal age ≥30 was associated with increased odds of microtia/anotia compared to those of younger age in two studies (27, 38), and in three studies, mothers of >30 years compared to mothers <30 years for isolated, non-isolated, and all cases of microtia/anotia (33, 36, 39). Another study reported that mothers of 25–29 years have a higher risk compared with control group (32). And one that there is a statistically significant difference (p < 0.01) between maternal mean age compared to controls (45).
(b) Maternal race/ethnicity. Multiple studies reported the risk association with maternal race/ethnicity, showing an increased risk for Hispanics compared to other groups (26, 31), and for isolated, non-isolated and all cases combined (33), and one also reporting increased risk in Asians for isolated cases (36). Some studies reported that African Americans have significant less risk of external ear malformations compared with other groups (26, 31), and one compared to with isolated and all cases of microtia/anotia (33).
(c) Parental education. Less educated parents (high school or less/<12 years of education) showed higher risk of having a newborn with congenital ear malformations in four studies (21, 32, 33, 38), one for Hispanic mothers compared to non-Hispanics regarding educational level (26), and other a decreased risk for mothers with ≥12 years of education (36).
(d) Maternal employment and household income. One study reported a greater risk for maternal employment outside of home, compared to housewives (24), and one for household income ranging from <10,000 to ≥40,000 (USD) for Hispanics compared to non-Hispanic whites (26).
(e) Parental residential area and altitude. One study reported a higher risk for external ear malformations in patients with urban residency compared with those with rural residency (42), other showed a greater risk for isolated cases of microtia/anotia (39) and one reported in risk for urban residency (35), while other reported the opposite (21). Only one study reported moderate altitude (1,511–2,426 m) as a risk factor, compared with lower altitudes [<1,499 m] (34), and one a decreased risk for mothers living in U.S.A-Mexico border counties, compared to other U.S.A counties (33).
(f) Parental chemical exposure. One study reported an association between chemical exposure such as formaldehyde, pesticides, and organic solvents, during the first trimester of pregnancy, and a significantly higher risk of having a child with severe microtia/atresia; medicines like progesterone; traditional Chinese medicines, such as radix isatidis, pseudo-ginseng and goldthread root; and NSAIDs (nonsteroidal anti-inflammatory drugs), were also significantly associated (27). Four studies showed that congenital ear malformations increase with parental chemical exposure, including heavy metals, dust, and SO2 exposure during the 3 months before conception and the 3 months after conception (21, 28, 30, 32), two reported environmental pollution as a risk factor for congenital microtia (21, 30). The association between parental drinking and smoking habits were reported by multiple studies; one study showed an association with alcohol and congenital microtia compared with non-drinkers (35), two with smoking ≥1 cigarette a day compared to non-smokers (24, 30), and one for smoking 1 month before to 3 months after conception compared to non-Hispanic whites (26). One reported increased risk only for binge drinking, associated with all cases of microtia/anotia, and smoking ≥5 cigarettes daily for non-isolated cases (29). Finally, only one study showed a significant risk increase of congenital microtia with pet contact during pregnancy (21).
(g) Family history of congenital ear malformations. Two studies showed a greater risk for congenital ear malformations on those with family history of malformations (20, 24).
Risk factors by pregnancy characteristics and parental clinical features, are shown in Table 5, and include:
(a) Infant sex. Multiple studies reported higher risk of congenital ear malformations in male infants compared to females (32, 38, 41, 42, 44, 45). Some reported similar results but comparing between isolated, non-isolated, and all cases combined of microtia/anotia (29, 33, 36, 39). While only one study showed increased risk for both male and females for U.S. born and foreign-born Hispanics compared to non-Hispanics (26).
(b) Gestational age and weight. Four authors showed increased risk of congenital external ear malformations for premature newborns compared to full-term newborns (31, 32, 37, 44), and one for premature (32–36 weeks), and very premature (<32 weeks) newborns for non-isolated and all cases of microtia/anotia (29).
(c) Maternal BMI and gestational diabetes. One study compared the risk association of pregnancy BMI and gestational diabetes for isolated microtia/anotia in U.S. born and foreign-born Hispanics compared to non-Hispanic whites, showing risk for all of the maternal BMI groups, and a greater risk for those with BMI ≥30 (26), one study for BMI ≥30 compared to a BMI of 18.5–25, and gestational diabetes for isolated cases (29), and one of maternal diabetes for isolated and all cases combined, with a greater risk for non-isolated cases, and gestational diabetes for all cases (33).
(d) Parental chronic diseases. Two studies reported an increased risk for microtia/anotia with maternal and paternal chronic diseases (30), and maternal chronic diseases (24), although no specific illness is mentioned, and one of mothers with chronic diabetes (31). One study reported higher risk for microtia/anotia with maternal diabetes (type I and II) in isolated and all cases of microtia/anotia, and with pre-existing hypertension with isolated cases (25), other showed increased risk with type I diabetes for all cases, including isolated and non-isolated, while type II increased the risk significantly only for non-isolated cases (29), and one study for maternal diabetes and pregestational diabetes for all cases, isolated and non-isolated, and for non-isolated and all cases respectively (33).
(e) Maternal medication and nutrition. Six studies showed a significant risk for external ear malformations in mothers taking medication during pregnancy, including analgesics (NSAIDs), antibiotics, antiemetics, antihypertensives, antispasmodics, oral contraceptives, and traditional Chinese medicine (21, 24, 25, 27, 30, 35). One showing that low folate intake increased the risk for isolated and all cases of microtia (23), and one showing higher risk in U.S. and foreign born Hispanics, than non-Hispanic white population (26); conversely, adequate periconceptional folate intake showed a marked reduction of risks in two studies (28, 30), and one showed a risk reduction for isolated cases, isolated cases and all cases for non-obese women, without significant results in non-isolated cases (22).
(f) Pregnancy complications and infections. Three studies reported greater risk for external ear malformations of mothers with abnormal pregnancies, including vaginal bleeding and anemia during the first trimester (20, 27, 30). Seven studies reported a significant increase of congenital external ear malformations with maternal infections during pregnancy (21, 24, 27, 28, 30, 31, 43), particularly in those presenting with viral infections and cold-like symptoms during pregnancy (24, 27, 28, 30, 43), and only one reported rubella vaccination before pregnancy to have a protective effect (35).
(g) Miscarriages. Two studies showed the risks of having an infant with congenital external ear malformations with threated abortion (30, 35), two with history of spontaneous abortion (28, 43), and one with both threatened abortion and history of miscarriages (27).
(h) Multiple pregnancies. Four studies showed that the risk of congenital ear malformations increased with multiple pregnancies and deliveries compared with primiparas (24, 30, 32, 37), and one showed an increased risk for non-singletons compared to singletons (31). One study reported higher risk of non-singletons for non-isolated and all cases of microtia/anotia (29), one only for isolated cases (25), and another only for non-isolated cases (33).
(i) Finally, one study compiled a predictive nomogram for maternal age, history of miscarriages, viral infections, anemia, progesterone use, paternal alcohol use, and topography of resident areas (40).
Table 7 summarizes some of the most reported defects and syndromes associated with external ear malformations from the included studies. The most common deformations associated with non-isolated cases of external ear malformations were cleft lip/palate, congenital heart defects, musculoskeletal deformities of skull, face and jaw, and preauricular tags and fistulas (25, 28, 33, 35, 36, 40, 43, 45). The multiple syndromes reported, include trisomy 18, 13, 21, Treacher-Collins, Nager syndrome, EEC syndrome, 4p- (Wolf-Hirschhorn) syndrome, X-linked dominant chondrodysplasia punctata, 22q11.2 deletion syndrome, and OAVS (25, 35, 37, 38, 40, 43, 45).
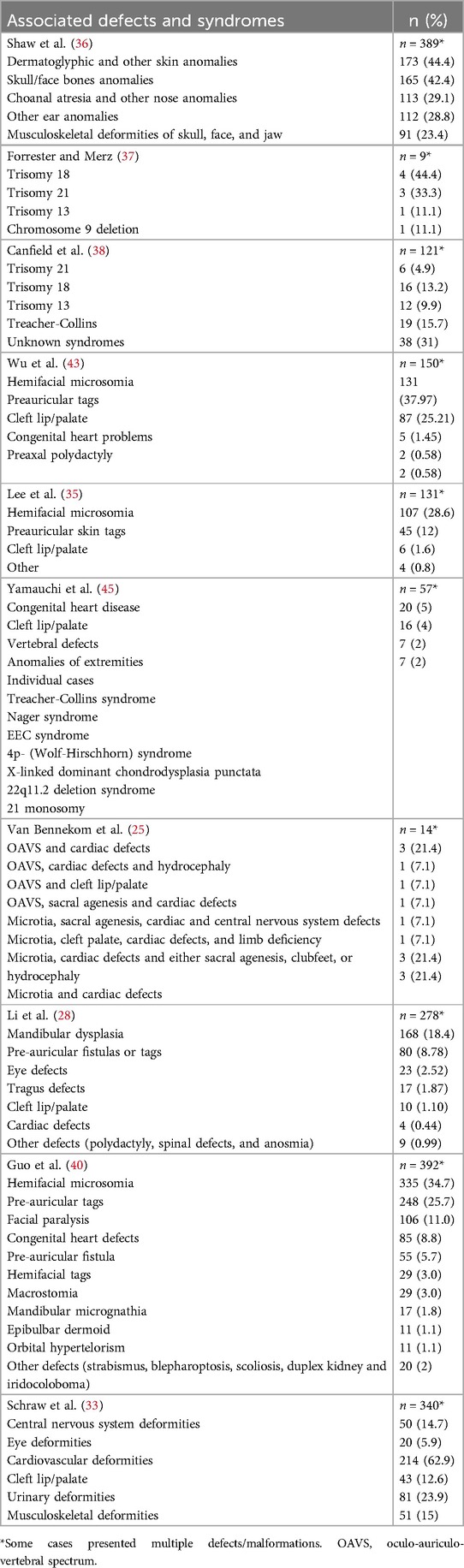
Table 7. Associated defects and syndromes with external ear malformations by study.
4 Discussion
This review aimed to compile and analyze the literature describing external ear congenital anomalies occurrence, characteristics, and associated factors. Congenital anomalies of the external ear vary widely in type and severity, while severe malformations such as anotia/microtia are uncommon. The frequency reported by the studies in this review ranged from 0.21 to 4.34 cases per 10,000 live births (36, 38, 46), higher than the reported by the literature of 0.8 to 2.4 per 10 000 live births (39, 47, 48). This variation might be due to inclusion criteria or higher rates reported in certain regions in comparison with other countries.
The studies reviewed show that external ear anomalies are more frequent in males, usually unilateral, more often in the right ear, Hispanic and Asian populations show higher prevalence compared to other ethnicities. Paternal and maternal age, environmental and pharmacological exposures, pregnancy, or perinatal related complications have been also associated with congenital ear malformations. From the studies presented in this review, twenty-three reported a frequency ranging from 47.1% to 78.5% for males (20, 21, 24–33, 35–45). This is consistent with other studies reporting male predominance: 68.6% in China (27), 58% in Finland (46), 60% in the United States (29, 36, 38, 49) and 54% in Hungary (50). It is worth noticing that both male and female, show similar severity grades (27, 49).
The reports included in this review show that 84% of external ear anomalies are unilateral, and mostly on the right ear (20, 24, 27, 28, 33, 35, 37, 40, 43, 45), consistent with the information presented in other studies (1, 51–53). The mechanisms for this predominance are still unclear; some authors have hypothesized that the greater prevalence of unilateral microtia cases may be related to a localized effect during embryogenesis, resulting in occlusion of a single vessel and thus, causing unilateral alterations (54). This has been attributed to a reduced or complete loss of blood flow to pharyngeal arches, resulting in hypoxia and damage to normal tissue (55), due to the interruption of blood flow to previously formed tissue, vasoconstriction, or underdevelopment of the arterial system required for adequate blood supply to the developing tissues (56). However, epidemiological, or experimental data are insufficient to support this hypothesis; and furthermore, even malformations caused by genetic alterations occur unilaterally, thus other factors acting through nonvascular mechanisms should be considered (55).
From the studies reporting ethnicity, nine found a higher prevalence among Hispanics compared to Caucasians and African Americans in the United States (22, 23, 25, 26, 29, 31, 33, 36, 38). Population-based studies have shown that the prevalence of external ear anomalies is more common in Asians, Hispanic, and Native American population, than in African American and Caucasian populations (57–59). This has been widely reported in studies from Mexico, Paraguay, China, Argentina, Chile, Ecuador, and Japan, where the prevalence ranges from 0.14 to 17.4 per 10,000 births (60–66), compared to studies from England, Italy, France, Hungary, and the United States of America, where the prevalence ranges between 0.66 to 4.34 per 10,000 births (36, 38, 50, 65–73). It is worth considering that prevalence rates are often calculated from live-births records, thus they might be underestimated in populations with high rates of stillbirths and abortions. Furthermore, several factors may relate to ethnicity differences in prevalence. For instance, the higher prevalence rate for Hispanic population in this review, for both US-born and Latin-American Hispanics (22, 23, 25, 26, 29, 31, 33, 36, 38) could be related to cultural behavior, regional differences, genetic variations, and environmental factors, such as socioeconomic status, nutrition, and prenatal care, or a combination of all (33, 56).
Studies report multiple environmental and demographic factors, that may be associated with external ear anomalies: parental age, education level, maternal employment, household income, residential area, altitude, environmental/chemical exposure during the three months before or after conception, drinking and smoking have shown to increase the risk of developing external ear malformations (21, 24–36, 38–40, 42, 45). Altitude has an important impact on external ear malformations in some countries in South America. For instance, there is a higher prevalence for microtia in Quito, Ecuador; La Paz, Bolivia; and Bogota, Colombia, that have higher altitude compared to other countries in South America (74–76). This is supported by the evidence of increased circulating levels of catecholamines and inflammatory cytokines during pregnancy, resulting in damage to the developing embryo and in intra-uterine growth restriction, and increased frequency of preeclampsia and stillbirths, in populations living at high-altitude (77, 78). Pregnancy and perinatal characteristics, as well as parental clinical features have shown to increase the risk of developing external ear anomalies. Among them: male sex, prematurity, low gestational weight, high maternal BMI, gestational diabetes, chronic illness, viral infections (common cold and influenza), some medications (NSAIDs, antihypertensives, antiemetics, progesterone, traditional Chinese medicines), low periconceptional vitamin intake, previous history of threatened abortion, bleeding, and anemia during the first trimester of pregnancy (20–33, 35–38, 40–45). Several risk factors differed between isolated and non-isolated cases of microtia/anotia. In the reviewed articles, the risk factors reported in isolated cases included: being of Asian and Hispanic descent (33, 36), low carbohydrate and folate intake (23), NSAIDs use, pre-existing maternal hypertension, multiple gestations (25), maternal education below high school (33), and urban residency (39); and protective factors were periconceptional folic acid intake (22) and maternal residence in border counties (33). Risk factors reported in non-isolated cases included: high cysteine intake (23), smoking ≥5 cigarettes daily, prematurity, BMI ≥30 (29), multiple births (33), and pre-gestational and gestational diabetes (29, 33); and maternal education above 12 years was reported as a protective factor (36). Notably, maternal diabetes has been consistently linked to a slight but significant increase in the risk of non-isolated cases of microtia/anotia by multiple studies (25, 31, 79–81).
These factors might disrupt the very complex sequence in the development of the external ear, but the mechanisms are not fully understood. This sequence can also be disrupted by mechanical trauma; as the external surface of the developing embryo is in close contact with the uterine wall, where increased tissue fragility or reduced cell-specific adhesiveness may increase the embryos susceptibility to physical or mechanical trauma (82), or in local vascular disruptions and transient focal tissue ischemia (56).
Some genetic studies have shown possible associations between gene mutations and their effect on the pharyngeal arches and external ear malformations. One of the most studied is HOXA2, an important transcriptional regulator for ear development (83, 84), suggesting that HOXA2 may be fundamental in orchestrating the auricle morphogenesis (56, 85, 86). Furthermore, twin studies, particularly those monozygotic with shared genotype, have also demonstrated a strong genetic association (87), suggesting that apart from environmental factors and behavioral factors, these malformations may also be linked genetically.
Multiple pregnancies have been reported to increase the risk of external ear malformations (24, 25, 29–33, 37), and more frequently in those by assisted reproduction techniques (44). Studies of In-vitro Fertilization (IVF) and intracytoplasmic sperm injection (ICSI) compared with those conceived naturally have shown a significantly higher risk of congenital malformations (88, 89), including eye, ear, face, and neck malformations (89–91). It has been reported that the techniques used with these procedures, such as medications used to induce ovulation and/or to maintain the pregnancy, culture media composition, length of time in culture, the freezing of embryos, among others, may be involved (92, 93). However, the specific ear malformations were not mentioned in these studies, thus further research is needed to define the type of ear malformations that are associated with these techniques.
Other factors such as consanguinity have been studied, with some studies reporting cases of autosomal-recessive and non-syndromic forms of bilateral microtia in consanguineous families (94, 95) However, the information about this topic is limited, and the association with external ear anomalies is still unclear.
Congenital external ear malformations may occur as an isolated defect, or with other defects and syndromes. Cleft lip/palate, congenital heart defects, musculoskeletal deformities of skull, face and jaw, and preauricular tags and fistulas were the most reported malformation associated with congenital external ear malformations in non-isolated cases (28, 35, 40, 43), as reported from multiple studies (35, 43, 44, 96). Treacher-Collins, trisomy 18, 13 21, and OAVS were the most reported syndromes (25, 37, 38, 45). It is important to note that many syndromes may not be reported due to the requirements for a karyotype to establish a diagnosis (37), and for those with known diagnosis, certain external ear malformations, such as milder forms of microtia, may be wrongly classified or not reported (38).
External ear malformations may relate to hearing loss, particularly in bilateral cases, justifying routine newborn hearing screening for early detection and prompt treatment (6). Surgical corrections of external ear malformations require a wide understanding of ear anatomy and its development (10). Over the years many techniques have been used and modified to accomplish optimal functional and aesthetic results. The type of technique depends on the presented malformation and whether the malformation is bilateral or unilateral (97). Many surgical techniques include cartilage sculpting from autogenous costal cartilage, and the use of sutures to reshape the ear (10, 17, 97, 98). Several complications can occur with these techniques, ranging from restenosis and otorrhea, to facial nerve injury, cartilage fracture, ear deformations, tympanic membrane perforation and inner ear trauma, worsening hearing impairment (10, 17, 97, 99).
Non-surgical techniques have proven to be highly effective in correcting minor malformations and deformations (such as deformities of the conchal crus, helix, Stahl ears, lidded ears, and prominent ears). Some of the most described techniques include ear molding techniques (7, 10, 100, 101), or laser assisted cartilage reshaping (102), offering an effective approach that can provide optimal results without the need for invasive procedures (7, 101, 102).
Missed diagnoses of congenital external ear malformations can result in delayed intervention and thus, speech developmental delays. Hearing screening in newborns has been reported as the most efficient method for early detection of hearing impairment (6). Once a diagnosis has been made, it is important to carefully select patients, according to strict criteria, including age and absence of sensorineural components of hearing loss, to avoid cases on where surgical intervention may not show favorable results (17, 99).
Overall, the results of this review describe several factors associated with congenital external ear anomalies. However, it has some limitations. There are few studies on external ear malformations, most of them focused on anotia/microtia only. Furthermore, the information regarding race/ethnicity predisposition is limited to a few populations, where the cultural aspects may go under-reported. Moreover, no studies were found of these anomalies in fetuses, thus the reports are limited to registered live births. Nevertheless, this review shows the complexity surrounding the external ear development and some of the associated factors that can result in its malformations.
In conclusion, congenital external ear anomalies include a wide variety of malformations that can occur isolated or associated with other malformations or syndromes. It is important to take environmental, cultural, and social aspects into consideration as a possible explanation for the wide variation across populations. External ear anomalies may cause conductive hearing loss, especially in bilateral cases, since the ear structure aids in the transmission of sound to the middle and inner ear and, depending on their type and severity, can lead to speech impediments. This highlights the importance of an early detection, classification, and repair to avoid childhood disability.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
AA: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. SR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. CA: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. LH: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. DC: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Thorn L. Entwicklung des ohres (einschließlich entstehung von missbildungen, experimentelle embryologie und in vitro-studien). In: Helms J, editor. Oto-Rhino-Laryngologie in Klinik und Praxis. Stuttgart: Thieme (1994). Vol. 1. p. 1–22.
2. Brent B. The pediatrician’s role in caring for patients with congenital microtia and atresia. Pediatr Ann. (1999) 28(6):374–83. doi: 10.3928/0090-4481-19990601-09
3. Conway H, Wagner KJ. Congenital anomalies of the head and neck as reported on birth certificates in New York city, 1952 to 1962 (inclusive). Plast Reconstr Surg. (1965) 36(1):71–9. doi: 10.1097/00006534-196507000-00010
4. Bartel-Friedrich S, Wulke C. Classification and diagnosis of ear malformations. GMS Curr Top Otorhinolaryngol Head Neck Surg. (2007) 6:Doc05.22073081
5. Tewfik T, Teebi A, Der Kaloustian V. Apendix A. Syndromes and conditions associated with congenital anomalies of the ear. In: Tewfik TL, der Kaloustian VM, editors. Congenital Anomalies of the ear, Nose, and Throat. New York, NY: Oxford University Press (1997). p. 125–44.
6. Kiefer J, Somers T, Arnold W. Malformations of the ear. In: Anniko M, Bernal-Sprekelsen M, Bonkowsky V, Bradley PJ, Iurato S, editors. Otorhinolaryngology, Head and Neck Surgery. Berlin, Heidelberg: Springer Berlin Heidelberg (2010). p. 33–41. doi: 10.1007/978-3-540-68940-9_2
7. Daniali LN, Rezzadeh K, Shell C, Trovato M, Ha R, Byrd HS. Classification of newborn ear malformations and their treatment with the EarWell infant ear correction system. Plast Reconstr Surg. (2017) 139(3):681–91. doi: 10.1097/PRS.0000000000003150
8. Byrd HS, Langevin CJ, Ghidoni LA. Ear molding in newborn infants with auricular deformities. Plast Reconstr Surg. (2010) 126(4):1191–200. doi: 10.1097/PRS.0b013e3181e617bb
9. Tan ST, Abramson DL, MacDonald DM, Mulliken JB. Molding therapy for infants with deformational auricular anomalies. Ann Plast Surg. (1997) 38(3):263–8. doi: 10.1097/00000637-199703000-00013
10. Joukhadar N, McKee D, Caouette-Laberge L, Bezuhly M. Management of congenital auricular anomalies. Plast Reconstr Surg. (2020) 146(2):205e–16e. doi: 10.1097/PRS.0000000000006997
11. Kil SH, Streit A, Brown ST, Agrawal N, Collazo A, Zile MH, et al. Distinct roles for hindbrain and paraxial mesoderm in the induction and patterning of the inner ear revealed by a study of vitamin-A-deficient quail. Dev Biol. (2005) 285(1):252–71. doi: 10.1016/j.ydbio.2005.05.044
12. Romand R, Dollé P, Hashino E. Retinoid signaling in inner ear development. J Neurobiol. (200610) 66(7):687–704. doi: 10.1002/neu.20244
13. Katzbach R, Klaiber S, Nitsch S, Steffen A, Frenzel H. Ohrmuschelrekonstruktion bei hochgradiger Mikrotie. HNO. (2006) 54(6):493–514. doi: 10.1007/s00106-006-1418-3
14. Helms J. Mittelohrmissbildungen. In: Helms J, Naumann HH, Herberhold C, Kastenbauer E, editors. Oto-Rhino-Laryngologie in Klinik und Praxis. Stuttgart: Thieme (1994). Vol. 1. p. 545–63.
15. Huang Y, Huang X, Li K, Yang Q. Risk factors of isolated microtia: a systematic review and meta-analysis. Plast Reconstr Surg. (2022) 151(4):651e–63e. doi: 10.1097/PRS.0000000000010007
16. Metwally MI, Alayouty NA, Basha MAA. Ear malformations: what do radiologists need to know? Clin Imaging. (2020) 66:42–53. doi: 10.1016/j.clinimag.2020.04.022
17. Jahrsdoerfer RA, Yeakley JW, Aguilar EA, Cole RR, Gray LC. Grading system for the selection of patients with congenital aural atresia. Am J Otol. (1992) 13(1):6–12. doi: 10.1016/S0196-0709(79)80003-4
18. Horlock N, Vögelin E, Bradbury ET, Grobbelaar AO, Gault DT. Psychosocial outcome of patients after ear reconstruction. Ann Plast Surg. (2005) 54(5):517–24. doi: 10.1097/01.sap.0000155284.96308.32
19. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
20. García-Reyes JC, Caro MA, Vega P, Ospina JC, Zarante AM, Zarante I. Epidemiology and risk factors for microtia in Colombia. Acta Otorrinolaringol Esp. (2009) 60(2):115–9. doi: 10.1016/S0001-6519(09)02007-X
21. Zhang Q-G, Zhang J, Yu P, Shen H. Environmental and genetic factors associated with congenital microtia: a case-control study in Jiangsu, China, 2004 to 2007. Plast Reconstr Surg. (2009) 124(4):1157–64. doi: 10.1097/PRS.0b013e3181b454d8
22. Ma C, Carmichael SL, Scheuerle AE, Canfield MA, Shaw GM. Association of microtia with maternal obesity and periconceptional folic acid use. Am J Med Genet A. (2010) 152A(11):2756–61. doi: 10.1002/ajmg.a.33694
23. Ma C, Shaw GM, Scheuerle AE, Canfield MA, Carmichael SL. Association of microtia with maternal nutrition. Birth Defects Res A Clin Mol Teratol. (2012) 94(12):1026–32. doi: 10.1002/bdra.23053
24. Luquetti DV, Saltzman BS, Lopez-Camelo J, da Graça Dutra M, Castilla EE. Risk factors and demographics for microtia in South America: a case–control analysis. Birth Defects Res A Clin Mol Teratol. (2013) 97(11):736–43. doi: 10.1002/bdra.23193
25. Van Bennekom CM, Mitchell AA, Moore CA, Werler MM. Vasoactive exposures during pregnancy and risk of microtia. Birth Defects Res A Clin Mol Teratol. (2013) 97(1):53–9. doi: 10.1002/bdra.23101
26. Hoyt AT, Canfield MA, Shaw GM, Waller DK, Polen KND, Ramadhani T, et al. Sociodemographic and hispanic acculturation factors and isolated anotia/microtia. Birth Defects Res A Clin Mol Teratol. (2014) 100(11):852–62. doi: 10.1002/bdra.23282
27. Liu Q, Fan X, Liu S, Wang L, Jiang Y, Chen X. Maternal risk factors for severe microtia/atresia in China: a case-control study. Int J Pediatr Otorhinolaryngol. (2018) 115:139–44. doi: 10.1016/j.ijporl.2018.09.033
28. Li C-L, Chen Y, Shan J, Hao S-J, Jin L, Qing F-H, et al. Phenotypic characterization and risk factors for microtia in east China, a case–control study. Int J Pediatr Otorhinolaryngol. (2014) 78(12):2060–3. doi: 10.1016/j.ijporl.2014.09.001
29. Ryan MA, Olshan AF, Canfield MA, Hoyt AT, Scheuerle AE, Carmichael SL, et al. Sociodemographic, health behavioral, and clinical risk factors for anotia/microtia in a population-based case-control study. Int J Pediatr Otorhinolaryngol. (2019) 122:18–26. doi: 10.1016/j.ijporl.2019.03.026
30. Chen W, Sun M, Zhang Y, Zhang Q, Xu X. Predicting the risk of microtia from prenatal factors: a hospital-based case-control study. Front Pediatr. (2022) 10:851872. doi: 10.3389/fped.2022.851872
31. Shehan JN, Danis DO, Bains A, Scott AR, Levi JR. Does prematurity play a role in newborn microtia-anotia? Ann Otol Rhinol Laryngol. (2022) 131(2):173–81. doi: 10.1177/00034894211015735
32. Yu WJ, Li N, Gong TT, Zhang JY, Jiang YT, Zhao YH, et al. Association between maternal exposure to SO2 and congenital ear malformations in offspring: a population-based case-control study in Liaoning province, China. Int J Public Health. (2022) 67:1604945. doi: 10.3389/ijph.2022.1604945
33. Schraw JM, Woodhouse JP, Benjamin RH, Shumate CJ, Nguyen J, Canfield MA, et al. Factors associated with nonsyndromic anotia and microtia, Texas, 1999–2014. Birth Defects Res. (2023) 115(1):67–78. doi: 10.1002/bdr2.2130
34. Ibarra-Ibarra BR, Luna-Muñoz L, Mutchinick OM, Arteaga-Vázquez J. Moderate altitude as a risk factor for isolated congenital malformations. Results from a case–control multicenter–multiregional study. Birth Defects Res. (2024) 116(7):e2335. doi: 10.1002/bdr2.2335
35. Lee KT, Yang EJ, Lim SY, Pyon JK, Mun GH, Bang SI, et al. Association of congenital microtia with environmental risk factors in South Korea. Int J Pediatr Otorhinolaryngol. (2012) 76(3):357–61. doi: 10.1016/j.ijporl.2011.12.009
36. Shaw GM, Carmichael SL, Kaidarova Z, Harris JA. Epidemiologic characteristics of anotia and microtia in California, 1989–1997. Birth Defects Res A Clin Mol Teratol. (2004) 70(7):472–5. doi: 10.1002/bdra.20042
37. Forrester MB, Merz RD. Descriptive epidemiology of anotia and microtia, Hawaii, 1986–2002. Congenit Anom. (2005) 45(4):119–24. doi: 10.1111/j.1741-4520.2005.00080.x
38. Canfield MA, Langlois PH, Nguyen LM, Scheuerle AE. Epidemiologic features and clinical subgroups of anotia/microtia in Texas. Birth Defects Res A Clin Mol Teratol. (2009) 85(11):905–13. doi: 10.1002/bdra.20626
39. Deng K, Dai L, Yi L, Deng C, Li X, Zhu J. Epidemiologic characteristics and time trend in the prevalence of anotia and microtia in China. Birth Defects Res A Clin Mol Teratol. (2016) 106(2):88–94. doi: 10.1002/bdra.23462
40. Guo R, Wang B, Wang Y, Zhang Y, Liu T, Zhang Q. Epidemiological analysis and the nomogram for possible risk factors for severe microtia. J Craniofac Surg. (2021) 32(2):e184–9. doi: 10.1097/SCS.0000000000007068
41. Sun P, Lin Q, Zhang M, Liu Z, Zhu L. Epidemiological study of neonatal congenital microtia in Shandong Province, China, 2011–2020. J Craniofac Surg. (2022) 33(8):e828–31. doi: 10.1097/SCS.0000000000008761
42. Zhou X, Fang J, Wang X, Kuang H, He J, Wang A, et al. Epidemiology of congenital malformations of the external ear in hunan province, China, from 2016 to 2020. Medicine. (2024) 103(15):e37691. doi: 10.1097/MD.0000000000037691
43. Wu J, Zhang R, Zhang Q, Xu Z, Chen W, Li D. Epidemiological analysis of microtia: a retrospective study in 345 patients in China. Int J Pediatr Otorhinolaryngol. (2010) 74(3):275–8. doi: 10.1016/j.ijporl.2009.12.001
44. Bader D, Grun M, Riskin-Mashiah S, Grunfeld A, Kogelman A, Chistyakov I, et al. Auricular mild errors of morphogenesis: epidemiological analysis, local correlations and clinical significance. Ann Genet. (2004) 47(3):225–34. doi: 10.1016/j.anngen.2004.02.007
45. Yamauchi M, Yotsuyanagi T, Ikeda K, Yoshikawa M, Urushidate S, Mikami M, et al. Clinical and genetic analysis of microtia in Japan. J Plast Surg Hand Surg. (2012) 46(5):330–4. doi: 10.3109/2000656X.2012.700018
46. Suutarla S, Rautio J, Ritvanen A, Ala-Mello S, Jero J, Klockars T. Microtia in Finland: comparison of characteristics in different populations. Int J Pediatr Otorhinolaryngol. (2007) 71(8):1211–7. doi: 10.1016/j.ijporl.2007.04.020
47. Harris J, Kallen B, Robert E. The epidemiology of anotia and microtia. J Med Genet. (1996) 33(10):809–13. doi: 10.1136/jmg.33.10.809
48. Stallings EB, Isenburg JL, Mai CT, Liberman RF, Moore CA, Canfield MA, et al. Population-based birth defects data in the United States, 2011–2015: a focus on eye and ear defects. Birth Defects Res. (2018) 110(19):1478–86. doi: 10.1002/bdr2.1413
49. Luquetti D V, Saltzman BS, Heike CL, Sie KC, Birgfeld CB, Evans KN, et al. Phenotypic sub-grouping in microtia using a statistical and a clinical approach. Am J Med Genet A. (2015) 167(4):688–94. doi: 10.1002/ajmg.a.36963
50. Paput L, Czeizel AE, Bánhidy F. Possible multifactorial etiology of isolated microtia/anotia—a population-based study. Int J Pediatr Otorhinolaryngol. (2012) 76(3):374–8. doi: 10.1016/j.ijporl.2011.12.012
51. Weerda H. Chirurgie der Ohrmuschel: Verletzungen, Defekte und Anomalien. 1st ed. Stuttgart: Georg Thieme Verlag (2004). Vol. 1. p. 105–226.
52. Swartz J, Faerber E. Congenital malformations of the external and middle ear: high-resolution CT findings of surgical import. Am J Roentgenol. (1985) 144(3):501–6. doi: 10.2214/ajr.144.3.501
53. O’Mara W, Guarisco L. Management of the preauricular sinus. J La State Med Soc. (1999) 151(9):447–50.
54. Poswillo D. The pathogenesis of the first and second branchial arch syndrome. Oral Surg Oral Med Oral Pathol. (1973) 35(3):302–28. doi: 10.1016/0030-4220(73)90070-4
55. Sadler TW, Rasmussen SA. Examining the evidence for vascular pathogenesis of selected birth defects. Am J Med Genet A. (2010) 152A(10):2426–36. doi: 10.1002/ajmg.a.33636
56. Luquetti DV, Heike CL, Hing AV, Cunningham ML, Cox TC. Microtia: epidemiology and genetics. Am J Med Genet A. (2012) 158A(1):124–39. doi: 10.1002/ajmg.a.34352
57. De la cruz A, Hansen M. Reconstruction surgery of the ear: auditory canal and tympanum. In: Cummings CW, Flint PW, Harker LA, Ballenger JJ, McCaffrey TV, Meyer T, editors. Cummings Otolaryngology Head & Neck Surgery. 5th ed. Philadelphia: Mosby (2004). p. 4439–44.
58. Murakami C, Quatela V. Reconstruction surgery of the ear: microtia reconstruction. In: Cummings CW, Flint PW, Harker LA, Ballenger JJ, McCaffrey TV, Meyer T, editors. Cummings Otolaryngology Head & Neck Surgery. 5th ed. Philadelphia: Mosby (2004). p. 4422–8.
59. Nelson SM, Berry RI. Ear disease and hearing loss among navajo children–a mass survey. Laryngoscope. (1984) 94(3):316–23. doi: 10.1288/00005537-198403000-00005
60. Aguinaga-Ríos M, Frías S, Arenas-Aranda DJ, Morán-Barroso VF. Microtia-atresia: aspectos clínicos, genéticos y genómicos. Bol Med Hosp Infant Mex. (2014) 71(6):387–95. doi: 10.1016/j.bmhimx.2014.11.001
61. Villamayor P, Ruiz-Diaz O, Zárate K, Saucedo M, Tandi L, Sanchez P, et al. Malformaciones congénitas del oído externo y medio en pacientes de la cátedra de otorrinolaringología, facultad de ciencias médicas, universidad nacional de Asunción, Paraguay. Medicina Clínica y Social. (2017) 1(2):105–13. doi: 10.52379/mcs.v1i2.14
62. Ministry of Health of China. Ministry of Health of China Publishing Maternal and Child Health Monitoring Web. Beijing, China (2020).
63. Campaña H, Pawluk MS, López Camelo JS, Grupo de Estudio del ECLAMC. Prevalencia al nacimiento de 27 anomalías congénitas seleccionadas, en 7 regiones geográficas de la Argentina. Arch Argent Pediatr. (2010) 108(5):409–17.
64. Nazer Herrera J, Lay-Son G, Cifuentes Ovalle L. Prevalencia al nacimiento de microtia-anotia.: Maternidad del Hospital Clínico de la Universidad de Chile, período 1983–2005. Rev Med Chil. (2006) 134(10):1295–301. doi: 10.4067/S0034-98872006001000012
65. Alasti F, Van Camp G. Genetics of microtia and associated syndromes. J Med Genet. (2009) 46(6):361–9. doi: 10.1136/jmg.2008.062158
66. Cho BC, Han KH. Surgical correction of cryptotia with V-Y advancement of a temporal triangular flap. Plast Reconstr Surg. (2005) 115(6):1570–81. doi: 10.1097/01.PRS.0000160692.21827.24
67. Tanzer RC. The constricted (cup and lop) ear. Plast Reconstr Surg. (1975) 55(4):406–15. doi: 10.1097/00006534-197555040-00003
68. Chami RG, Apesos J. Treatment of asymptomatic preauricular sinuses: challenging conventional wisdom. Ann Plast Surg. (1989) 23(5):406–11. doi: 10.1097/00000637-198911000-00005
69. Scheinfeld NS, Silverberg NB, Weinberg JM, Nozad V. The preauricular sinus: a review of its clinical presentation, treatment, and associations. Pediatr Dermatol. (2004) 21(3):191–6. doi: 10.1111/j.0736-8046.2004.21301.x
70. Huang XY, Tay GS, Wansaicheong GKL, Low WK. Preauricular sinus: clinical course and associations. Arch Otolaryngol Head Neck Surg. (2007) 133(1):65–8. doi: 10.1001/archotol.133.1.65
71. Meggyessy V, Méhes K. Preauricular pits in Hungary: epidemiologic and clinical observations. J Craniofac Genet Dev Biol. (1982) 2(3):215–8.7166595
72. Ewing MR. Congenital sinuses of the external ear. J Laryngol Otol. (1946) 61(1):18–23. doi: 10.1017/S0022215100007726
73. Tsai FJ, Tsai CH. Birthmarks and congenital skin lesions in Chinese newborns. J Formos Med Assoc. (1993) 92(9):838–41.7904869
74. González-Andrade F, López-Pulles R, Espín VH, Paz-y-Miño C. High altitude and microtia in Ecuadorian patients. J Neonatal Perinatal Med. (2010) 3(2):109–16. doi: 10.3233/NPM-2010-0102
75. Castilla EE, Orioli IM. Prevalence rates of microtia in South America. Int J Epidemiol. (1986) 15(3):364–8. doi: 10.1093/ije/15.3.364
76. Castilla EE, Lopez-Camelo JS, Campaña H. Altitude as a risk factor for congenital anomalies. Am J Med Genet. (1999) 86(1):9–14. doi: 10.1002/(sici)1096-8628(19990903)86:1%3C9::aid-ajmg3%3E3.0.co;2-x
77. Coussons-Read ME, Mazzeo RS, Whitford MH, Schmitt M, Moore LG, Zamudio S. High altitude residence during pregnancy alters cytokine and catecholamine levels. Am J Reprod Immunol. (2002) 48(5):344–54. doi: 10.1034/j.1600-0897.2002.01078.x
78. Zamudio S, Baumann MU, Illsley NP. Effects of chronic hypoxia in vivo on the expression of human placental glucose transporters. Placenta. (2006) 27(1):49–55. doi: 10.1016/j.placenta.2004.12.010
79. Correa A, Gilboa SM, Besser LM, Botto LD, Moore CA, Hobbs CA, et al. Diabetes mellitus and birth defects. Am J Obstet Gynecol. (2008) 199(3):237.e1–e9. doi: 10.1016/j.ajog.2008.06.028
80. Mastroiacovo P, Corchia C, Botto LD, Lanni R, Zampino G, Fusco D. Epidemiology and genetics of microtia-anotia: a registry based study on over one million births. J Med Genet. (1995) 32(6):453–7. doi: 10.1136/jmg.32.6.453
81. Wang R, Martínez-Frías ML, Graham JM. Infants of diabetic mothers are at increased risk for the oculo-auriculo-vertebral sequence: a case-based and case-control approach. J Pediatr. (2002) 141(5):611–7. doi: 10.1067/mpd.2002.128891
82. Vrontou S, Petrou P, Meyer BI, Galanopoulos VK, Imai K, Yanagi M, et al. Fras1 deficiency results in cryptophthalmos, renal agenesis and blebbed phenotype in mice. Nat Genet. (2003) 34(2):209–14. doi: 10.1038/ng1168
83. Gendron-Maguire M, Mallo M, Zhang M, Gridley T. Hoxa-2 mutant mice exhibit homeotic transformation of skeletal elements derived from cranial neural crest. Cell. (1993) 75(7):1317–31. doi: 10.1016/0092-8674(93)90619-2
84. Rijli FM, Mark M, Lakkaraju S, Dierich A, Dollé P, Chambon P. A homeotic transformation is generated in the rostral branchial region of the head by disruption of hoxa-2, which acts as a selector gene. Cell. (1993) 75(7):1333–49. doi: 10.1016/0092-8674(93)90620-6
85. Minoux M, Kratochwil CF, Ducret S, Amin S, Kitazawa T, Kurihara H, et al. Mouse Hoxa2 mutations provide a model for microtia and auricle duplication. Development. (2013) 140(21):4386–97. doi: 10.1242/dev.098046
86. Cox TC, Camci ED, Vora S, Luquetti DV, Turner EE. The genetics of auricular development and malformation: new findings in model systems driving future directions for microtia research. Eur J Med Genet. (2014) 57(8):394–401. doi: 10.1016/j.ejmg.2014.05.003
87. Artunduaga MA, Quintanilla-Dieck MDL, Greenway S, Betensky R, Nicolau Y, Hamdan U, et al. A classic twin study of external ear malformations, including microtia. N Engl J Med. (2009) 361(12):1216–8. doi: 10.1056/NEJMc0902556
88. Zheng Z, Chen L, Yang T, Yu H, Wang H, Qin J. Multiple pregnancies achieved with IVF/ICSI and risk of specific congenital malformations: a meta-analysis of cohort studies. Reprod Biomed Online. (2018) 36(4):472–82. doi: 10.1016/j.rbmo.2018.01.009
89. Liang Y, Chen L, Yu H, Wang H, Li Q, Yu R, et al. Which type of congenital malformations is significantly increased in singleton pregnancies following after in vitro fertilization/intracytoplasmic sperm injection: a systematic review and meta-analysis. Oncotarget. (2018) 9(3):4267–78. doi: 10.18632/oncotarget.23689
90. Sagot P, Bechoua S, Ferdynus C, Facy A, Flamm X, Gouyon JB, et al. Similarly increased congenital anomaly rates after intrauterine insemination and IVF technologies: a retrospective cohort study. Hum Reprod. (2012) 27(3):902–9. doi: 10.1093/humrep/der443
91. Klemetti R, Gissler M, Sevón T, Koivurova S, Ritvanen A, Hemminki E. Children born after assisted fertilization have an increased rate of major congenital anomalies. Fertil Steril. (2005) 84(5):1300–7. doi: 10.1016/j.fertnstert.2005.03.085
92. Hansen M, Kurinczuk JJ, Milne E, de Klerk N, Bower C. Assisted reproductive technology and birth defects: a systematic review and meta-analysis. Hum Reprod Update. (2013) 19(4):330–53. doi: 10.1093/humupd/dmt006
93. Qin JB, Sheng XQ, Wu D, Gao SY, You YP, Yang TB, et al. Worldwide prevalence of adverse pregnancy outcomes among singleton pregnancies after in vitro fertilization/intracytoplasmic sperm injection: a systematic review and meta-analysis. Arch Gynecol Obstet. (2017) 295(2):285–301. doi: 10.1007/s00404-016-4250-3
94. Alasti F, Sadeghi A, Sanati MH, Farhadi M, Stollar E, Somers T, et al. A mutation in HOXA2 is responsible for autosomal-recessive microtia in an Iranian family. Am J Hum Genet. (2008) 82(4):982–91. doi: 10.1016/j.ajhg.2008.02.015
95. Brown KK, Viana LM, Helwig CC, Artunduaga MA, Quintanilla-Dieck L, Jarrin P, et al. HOXA 2 Haploinsufficiency in dominant bilateral microtia and hearing loss. Hum Mutat. (2013) 34(10):1347–51. doi: 10.1002/humu.22367
96. Llano-Rivas I, Ariadna del Castillo V, Reyes R, Carnevale A. Microtia. Arch Med Res. (1999) 30(2):120–4. doi: 10.1016/S0188-0128(98)00023-2
97. Marres EH, Cremers CW. Surgical treatment of congenital aural atresia. Am J Otol. (1985) 6(3):247–9.4003534
98. Fanchella A, Pellegrinelli S, Carcini F, Zollino I, Carnevali G, Candotto V, et al. Congenital malformations of the ear. Eur J Inflamm. (2012) 10:35–8.
99. Cremers CWRJ, Teunissen E, Marres EHMA. Classification of congenital aural atresia and results of reconstructive surgery. Adv Otorhinolaryngol. (1988) 40:9–14. doi: 10.1159/000415666
100. Rozanski C, Rousso JJ. Congenital ear malformations: effectively correcting cryptotia with neonatal ear molding. Ear Nose Throat J. (2017) 96(9):359–60. doi: 10.1177/014556131709600905
101. Liu YCC, Kini S, Barton G, Pham T, Marcet-Gonzalez J, Novak B. Implementation of auricular malformation screenings in the newborn population. Int J Pediatr Otorhinolaryngol. (2020) 133:109999. doi: 10.1016/j.ijporl.2020.109999
Keywords: auricle, ear anomalies, congenital malformations, external ear, review
Citation: Acosta-Rodríguez A, Reza-López SA, Aguilar-Torres CR, Hinojos-Gallardo LC and Chávez-Corral DV (2025) A systematic review of congenital external ear anomalies and their associated factors. Front. Pediatr. 13:1520200. doi: 10.3389/fped.2025.1520200
Received: 30 October 2024; Accepted: 24 March 2025;
Published: 24 April 2025.
Edited by:
Yu Sun, Huazhong University of Science and Technology, ChinaReviewed by:
Hans Thomeer, Utrecht University, NetherlandsXiaowei Chen, Peking Union Medical College Hospital (CAMS), China
Copyright: © 2025 Acosta-Rodríguez, Reza-López, Aguilar-Torres, Hinojos-Gallardo and Chávez-Corral. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dora V. Chávez-Corral, ZG9jaGF2ZXpAdWFjaC5teA==
†These authors have contributed equally to this work