 Leila Kahnami1,2
Leila Kahnami1,2 Mary Lou Smith1,3,4
Mary Lou Smith1,3,4 Ari Bitnun5,6Jason Brophy7,8
Ari Bitnun5,6Jason Brophy7,8 John G. Sled9,10
John G. Sled9,10 Elka Miller11,12
Elka Miller11,12 Jennifer Bowes7
Jennifer Bowes7 Mariève Hurtubise7
Mariève Hurtubise7 Lena Serghides13,14*†
Lena Serghides13,14*† Julia M. Young1,3*† on behalf of the KIND study group
Julia M. Young1,3*† on behalf of the KIND study group
- 1Department of Psychology, The Hospital for Sick Children, Toronto, ON, Canada
- 2Department of Psychology, York University, Toronto, ON, Canada
- 3Neurosciences and Mental Health Program, Research Institute, The Hospital for Sick Children, Toronto, ON, Canada
- 4Department of Psychology, University of Toronto Mississauga, Mississauga, ON, Canada
- 5Division of Infectious Diseases, The Hospital for Sick Children, Toronto, ON, Canada
- 6Department of Pediatrics, University of Toronto, Toronto, ON, Canada
- 7Division of Infectious Diseases, Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada
- 8Department of Pediatrics, University of Ottawa, Ottawa, ON, Canada
- 9Translational Medicine Program, Research Institute, The Hospital for Sick Children, Toronto, ON, Canada
- 10Department of Medical Biophysics, University of Toronto, Toronto, ON, Canada
- 11Department of Diagnostic and Interventional Radiology, The Hospital for Sick Children, Toronto, ON, Canada
- 12Department of Medical Imaging, CHEO, University of Ottawa, Ottawa, ON, Canada
- 13Toronto General Hospital Research Institute, University Health Network, Toronto, ON, Canada
- 14Department of Immunology and Institute of Medical Sciences, Toronto, ON, Canada
Background: Children who are HIV-exposed uninfected (CHEU) are at increased risk for neurodevelopmental impairments. Most studies report on neurodevelopmental outcomes in the first 2 years of life, with limited data available for school-aged CHEU. This interim study examined the intellectual and language outcomes in school-aged CHEU compared to children who are HIV-unexposed uninfected (CHUU).
Setting: CHEU and CHUU aged 6–10 years recruited at two sites in Ontario, Canada.
Methods: Intellectual and language abilities were measured using the WISC-V and CELF-5. Generalized linear models investigated associations of HEU-status with each neurodevelopmental outcome. An interaction term with sex was included to assess sex-specific effects. Gestational age, being small for gestational age (SGA), and household income were investigated as covariates.
Results: 65 CHEU (35 female, median age 9.00 years) and 42 CHUU (18 female, 8.96 years) were included. HEU-status was associated with significantly lower working memory and expressive language scores. In males, HEU-status was associated with lower scores on working memory, processing speed, overall intelligence, core, and expressive language abilities. No significant differences were observed in females by HEU-status. Household income was associated with all measures of intelligence and language. Lower working memory scores persisted in male CHEU after adjusting for covariates.
Conclusion: Male CHEU and those with lower household income were the most vulnerable to cognitive and language deficits. Working memory deficits in CHEU indicates a specific cognitive vulnerability due to HEU exposure status. Our findings highlight the need for early interventions, including ensuring financial security and close neuropsychological follow-up.
1 Introduction
Globally, there are more than 16 million children who are HIV-exposed but uninfected (CHEU) (1). In Canada, between 200 and 250 CHEU are born each year (2). Most of these children are also perinatally exposed to HIV antiretroviral therapy (ART). In utero exposure to HIV (3), and HIV-related mechanisms such as maternal immune activation and inflammation (4, 5), as well as ART exposure (6), may place CHEU at a higher risk of perinatal complications and developmental deficits (7). Developmental vulnerabilities have been reported in CHEU, including differences in early neuropsychological development compared to children who are HIV-unexposed and uninfected (CHUU) (8). Perinatal risk factors are known to influence the trajectories of the developing brain (9, 10). However, there is a limited understanding of the impact of the perinatal risk factors on the neuropsychological development of CHEU in later childhood.
CHEU are at increased risk of being born small for gestational age, having low birth weight, being born preterm, experiencing neonatal jaundice, and being admitted to the neonatal intensive care unit (NICU) (7, 11–13). While preterm birth, low birth weight, and admission to NICU have been associated with an increased risk of neurodevelopmental delays and cognitive challenges in all children (9, 10, 14–16), reports of these associations in CHEU are limited to the ages of 6–24 months, and data in older CHEU are lacking (11, 17). In addition, CHEU are at increased risk of intellectual (18) and language challenges (19, 20). Despite these insights, the literature remains fragmented, with studies suggesting no significant differences in the neurodevelopmental trajectory and language development of CHEU up to the age of 5 (11, 17, 18, 21), while longitudinal studies suggest that differences in overall intellectual and expressive and receptive language abilities between CHEU and CHUU may become more prominent over time (8, 22, 23). Moreover, while sex differences in the neurodevelopmental trajectory of CHEU have been considered in younger age groups, little is known about the emergence of sex differences in older age groups (24, 25).
The existing literature includes a combination of low- and high-income countries, with limited published data from high-income countries, such as Canada. Research examining sex differences in the neurodevelopmental trajectory of CHEU remains limited. Further, previous studies have explored these associations in younger age groups. The cognitive outcomes of CHEU and the role of perinatal, demographic, and socioeconomic factors on intellectual and language abilities in school-aged CHEU remain unclear. As part of a Canadian multidisciplinary study, this current study examined the impact of HIV-exposed uninfected (HEU) status on the cognitive outcomes in school-aged children. Our aim was to compare the intellectual and language abilities of school-aged CHEU and CHUU, while considering the differences in demographic and socioeconomic characteristics and perinatal risk factors to determine potential moderating factors influencing these cognitive outcomes.
2 Methods
2.1 Study population
The findings of this study are an interim analysis of the Kids Imaging and Neurocognitive Development (KIND) study, an ongoing Canadian prospective cohort study of CHEU and CHUU designed, with target sample size of 180 CHEU and 65 CHUU, to assess the long-term neurodevelopmental health of these children, at two time points across a two-year interval. The KIND study enrolls children between the ages of 6–10 since 2020 across two clinical sites—The Hospital for Sick Children (SickKids) in Toronto and Children’s Hospital of Eastern Ontario (CHEO) in Ottawa. The key inclusion criteria for the CHEU group were being born to a mother living with HIV with a known exposure to ART, and having negative HIV status (defined as two or more negative DNA PCR assays performed at or after one month of age or negative HIV serology at any age). The CHUU were recruited from the community and school programs operating in areas of similar socioeconomic status as the families of CHEU, and through word of mouth from participants. Group matching criteria included age, ethnic background, household income, caregiver education level. The inclusion criteria for CHUU were having a mother with HIV-negative status during pregnancy. Exclusion criteria for both groups included a history of previous developmental or neurological conditions (e.g., stroke, Down’s syndrome) that were not related to HIV/ART exposure (in the CHEU group), exposure to maternal smoking (>1 cigarette/day), regular alcohol consumption (>3 drinks/week for >1 month), or any substance use during pregnancy.
2.2 Ethics statement
The Institutional Review Boards of The Hospital for Sick Children, Children’s Hospital of Eastern Ontario, and University Health Network approved the protocol. All participating families provided written informed consent, and children provided assent to participate in the study.
2.3 Demographic and perinatal measures
Demographic and perinatal health information was collected through structured parent interviews for both groups and a review of hospital medical records for CHEU. Demographic and perinatal information was self-reported by the mothers throughout the structured interview. Information regarding maternal HIV status and ART usage during the relevant pregnancy for the CHEU group was collected from medical records. The following demographic measures were obtained through the structured interviews: family income, maternal race, maternal education level, and languages spoken at home. A translator was used, where needed, with parents who did not primarily speak English.
Our primary exposure of interest was HEU-status (CHEU vs. CHUU). Perinatal measures of interest included: birthweight, birth weight centiles [determined using the INTERGROWTH-21st calculator (26)], small for gestational age (SGA) status (below the 10th birth weight centile), gestational age at birth, prematurity (born at <37 weeks gestational age), NICU admission, and birth complications (e.g., jaundice, infection, induced delivery).
2.4 Neurodevelopmental outcomes
The primary outcome measures were scores from two psychological assessment measures the Wechsler Intelligence Scale for Children—Fifth Edition [WISC-V (27)] and the Clinical Evaluation of Language Fundamentals- Fifth Edition [CELF-5 (28)]). These measures were administered by experienced research staff under the supervision of a psychologist or directly by psychologists. Indices of Verbal Comprehension, Visual-Spatial, Fluid Reasoning, Working Memory, Processing Speed, and Full-Scale IQ were obtained through the WISC-V. Indices of Expressive Language, Receptive Language, and Core Language abilities (combination of expressive and receptive language skills) were obtained from the CELF-5. Standardized scores were derived for each measure, with a population mean of 100 corresponding to the 50th percentile of typical development, and a standard deviation (SD) of 15.
2.5 Statistical analyses
Chi-square (χ2 tests) were used to compare demographic characteristics between CHEU and CHUU groups. The mean standard scores and 95% confidence intervals of the intelligence and language outcomes were calculated by HEU-status (CHEU vs. CHUU), and stratified by sex. The proportion of children scoring within the clinically impaired range (2 SD below the mean standardized score, i.e., <70) on each measure was calculated by HEU-status. Chi-squared tests were used to compare the proportions of clinically impaired scores between the two groups. Generalized linear models with robust standard errors (29) were used to examine the associations between each neurodevelopmental outcome and HEU-status. To investigate sex-specific effects models including an interaction term of HEU-status and sex were also used.
Exploratory Pearson’s correlation coefficients were first calculated to examine relationships between demographic, socioeconomic, and perinatal measures with each neurodevelopmental outcome. Perinatal factors included in the models were chosen a priori. Household income and maternal education levels were considered to represent socioeconomic status. To investigate how these perinatal factors and socioeconomic factors modified the associations between HEU-status with each neurodevelopmental outcome, subsequent generalized linear regression models included chosen perinatal factors and socioeconomic factors as independent variables. Gestational age at birth and birthweight were considered due to the significant differences in these factors between the CHEU and CHUU, but to avoid collinearity due to their high correlation (r = 0.70), gestational age at birth was selected. Birthweight centile, prematurity, NICU admission, and birth complications were excluded due to high correlations with gestational age at birth (Supplementary Table 1). Being SGA at birth was retained based on its association with neurodevelopmental outcome measures and low correlation with gestational age at birth (r = 0.14). Two models were evaluated to examine the impact of gestational age at birth and SGA. The first model adjusted only for gestational age at birth (Supplementary Table 2). The second model adjusted for gestational age at birth and being SGA (Supplementary Table 3) and was identified as having the best fit for perinatal factors. The models also included a “HEU-status by sex” interaction term. To account for socioeconomic status, household income was chosen due to its correlations with the neurodevelopmental outcome measures. Household income was included in the final model that included the perinatal factors of gestational age at birth and SGA. Model fit was compared using the Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). All analyses were performed using R (v4.2.1) (30), STATA (v13) (31), and Prism (v9) (32), with statistical significance set at p < 0.05.
3 Results
3.1 Baseline demographic and perinatal measures
A total of 114 children were enrolled between January 2020 and April 2024. After excluding participants (n = 7) due to invalid results on the neurodevelopmental measures, 107 children (65 CHEU and 42 CHUU) were available for the analysis. Demographic and perinatal characteristics are shown in Table 1. Both groups had similar age (median age of 9.00 years for CHEU vs. 8.96 years for CHUU) and sex distribution (CHEU 53.8% girls vs. CHUU 42.9% girls). CHEU and CHUU were similar in maternal and socioeconomic characteristics. The majority of mothers identified as African/Caribbean/Black (70.3% of CHEU and 45.2% of CHUU). English was the primary language spoken at home for the majority of participants (89.1% for CHEU vs. 92.9% for CHUU). The majority of mothers had a college degree level education (42.9% of CHEU mothers vs. 47.6% of CHUU mothers). There were no statistically significant differences between groups in household income.
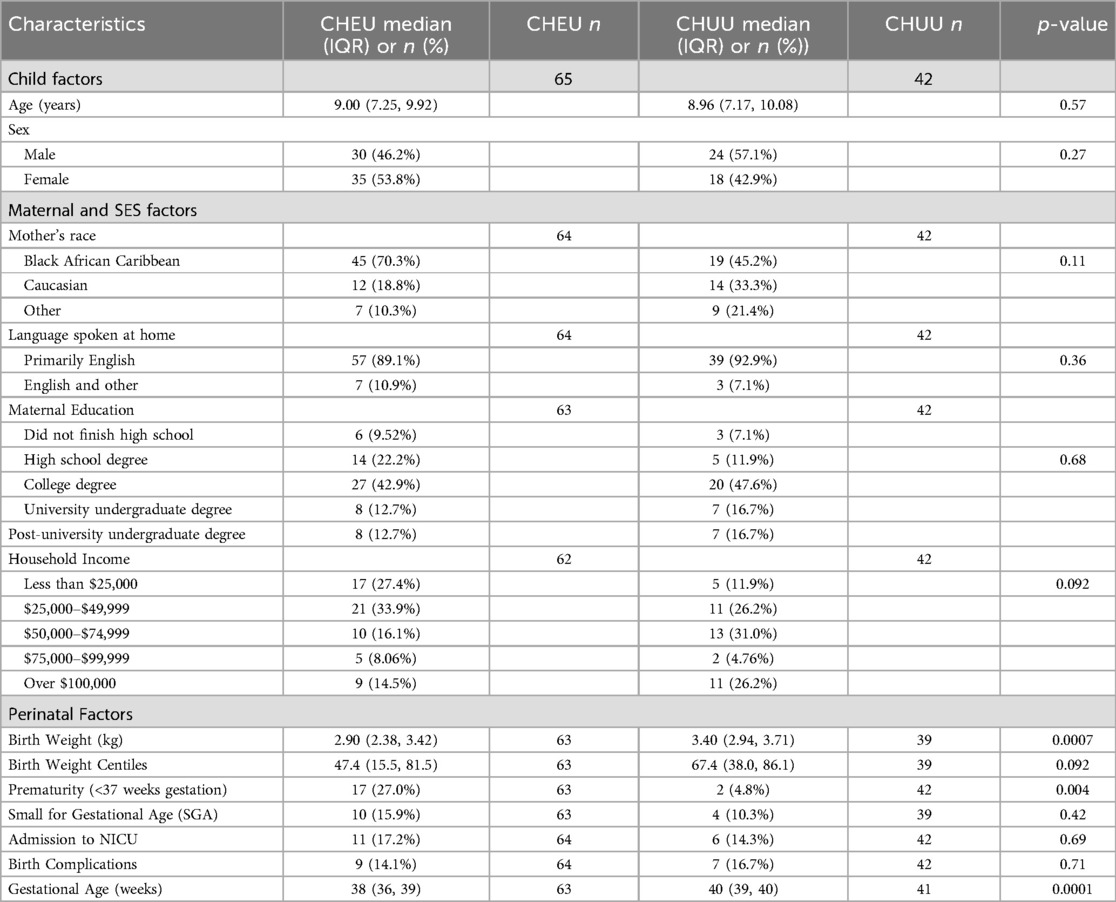
Table 1. Demographic and perinatal characteristics.
The median gestational age at birth was significantly lower for CHEU (38 weeks) compared to CHUU (40 weeks; p < 0.0001), with a greater proportion of CHEU being born prematurely (27% vs. 4.8%, p = 0.004). While the median birthweight for CHEU (2.90 kg) was significantly lower than that of CHUU (3.40 kg; p = 0.0007), the median birthweight centiles did not differ significantly between groups (47.4 vs. 67.4 percentile; p = 0.092). A similar proportion of children in each group were classified as SGA at birth (CHEU: 15.9% vs. CHUU: 10.3%; p = 0.42). The proportion of children experiencing birth complications (CHEU: 14.1% vs. CHUU: 16.7%; p = 0.71) was similar between groups, as were the proportion of children admitted to NICU (CHEU: 17.2% vs. CHUU: 14.3%; p = 0.69). In the CHEU group, the majority of NICU admissions were due to preterm birth (54.5%, n = 6), with other reasons including maternal uterine diverticulum, heart murmur, breastfeeding issues, low glucose levels, and small size (each n = 1). In the CHUU group, reasons for NICU admission included meconium aspiration, jaundice, maternal diabetes (each n = 1), or other reasons (n = 3).
3.2 Univariate analyses of neurodevelopmental outcomes
The mean scores for each measure were in the average range for both the CHEU and CHUU (Table 2 and Supplementary Figures 1, 2). Within the CHEU group, a higher proportion of participants scored in the clinically impaired range (standardized score <70) on all measures (Table 2) than expected in the normative population, whereas 2% of individuals in the general population are expected to fall within these ranges. The proportion of CHEU falling in the clinically impaired range was significantly higher for the Working Memory Index (10.9% vs. 0.0%, p = 0.027) and was marginally higher for the Visual Spatial Index (7.7% vs. 0.0%, p = 0.07) as compared to CHUU.
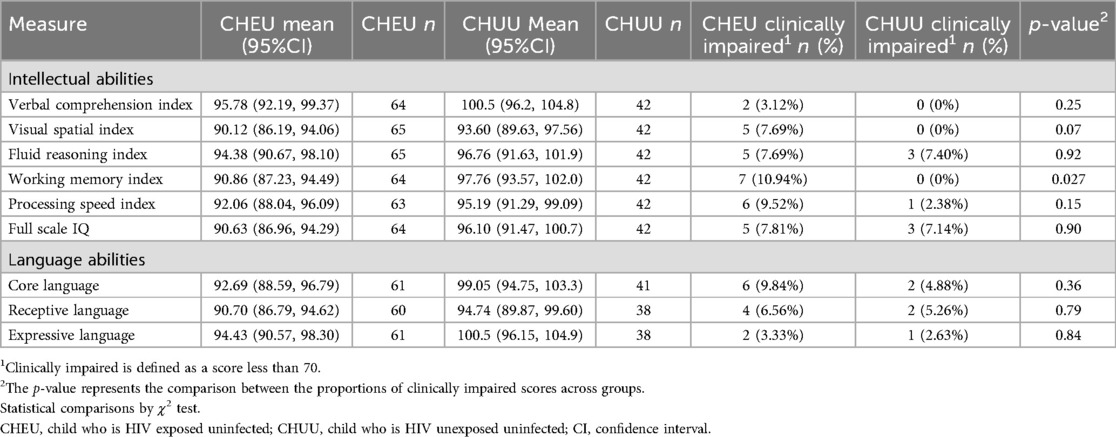
Table 2. Neurodevelopmental outcomes in CHEU and CHUU: mean and confidence intervals of standard scores, and comparison of clinically impaired proportions.
In the univariate analyses, CHEU had significantly lower mean standard scores for working memory (mean difference −6.90, p = 0.012), core language (mean difference −6.36, p = 0.030), and expressive language (mean difference −6.07, p = 0.035), and marginally lower for Full Scale IQ (mean difference −5.47, p = 0.06), compared to CHUU (Supplementary Table 4). Including sex as an interaction term in the models revealed that male CHEU were more vulnerable than female CHEU (Figures 1 and 2). Male CHEU had significantly lower mean standard scores for Verbal Comprehension (mean difference −8.72, p = 0.018), Working Memory (mean difference −12.12, p = 0.001), Processing Speed (mean difference −9.03, p = 0.017), Full Scale IQ (mean difference −10.83, p = 0.005), Core Language (mean difference −10.37, p = 0.007), and Expressive Language (mean difference −9.48, p = 0.011), and marginally lower for Receptive Language (mean difference −6.90, p = 0.092) (Figures 1 and 2, and Supplementary Table 5). Female CHEU had similar scores to female CHUU for all outcomes.
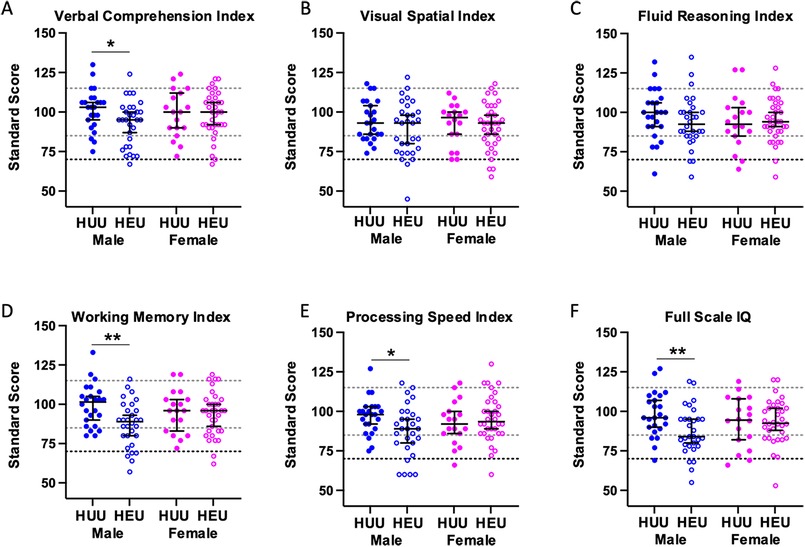
Figure 1. Standard scores of intellectual abilities for male and female CHEU compared to CHUU. Dot plot illustrating the distribution of standard scores for Verbal Comprehension (A) [CHEU (30 male, 34 female); CHUU (24 male, 18 female)], Visual-Spatial (B) [CHEU (30 male, 35 female); CHUU (24 male, 18 female)], Fluid Reasoning (C) [CHEU (30 male, 35 female); CHUU (24 male, 18 female)], Working Memory (D) [CHEU (30 male, 34 female); CHUU (24 male, 18 female)], Processing Speed (E) [CHEU (19 male, 34 female); CHUU (24 male, 18 female)], and Full-Scale IQ (F) [CHEU (30 male, 34 female); CHUU (24 male, 18 female)] indices in CHEU and CHUU, stratified by sex. Data are shown as dots for each individual participant with the mean and 95% confidence intervals indicated. Light dotted lines indicate ±1 standard deviation from the population mean of 100. The darker dotted line indicates 2 standard deviations below the population mean of 100. Dots falling below this line are classified as clinically impaired. Males are shown in blue, and females in pink. Closed circles indicate CHUU, and open circles indicate CHEU. *p < 0.05, **p < 0.01. Statistical comparisons by generalized linear models including an HEU-status*sex interaction term. CHEU, child who is HIV exposed uninfected; CHUU, child who is HIV unexposed uninfected. HUU, HIV unexposed uninfected; HEU, HIV exposed uninfected.
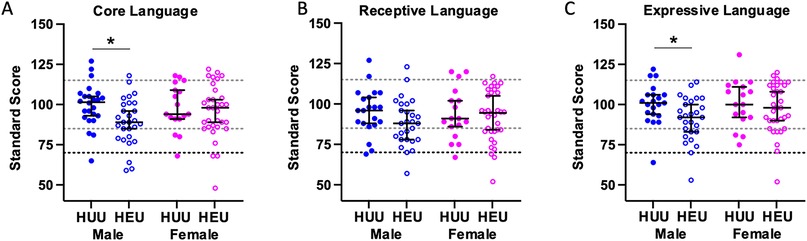
Figure 2. Standard scores of language abilities for male and female CHEU compared to CHUU. Dot plot illustrating the distribution of standard scores for Core Language (A) [CHEU (28 male, 33 female); CHUU (24 male, 17 female)], Receptive Language (B) [CHEU (27 male, 34 female); CHUU (21 male, 17 female)], and Expressive Language (C) [CHEU (27 male, 33 female); CHUU (21 male, 17 female)] indices in CHEU and CHUU, stratified by sex. Data are shown as dots for each individual participant with the mean and 95% confidence intervals indicated. Light dotted lines indicate ±1 standard deviation from the population mean of 100. The darker dotted line indicates 2 standard deviations below the population mean of 100. Dots falling below this line are classified as clinically impaired. Males are shown in blue, and females in pink. Closed circles indicate CHUU, and open circles indicate CHEU. *p < 0.05. Statistical comparisons by generalized linear models including an HEU-status*sex interaction term. CHEU, child who is HIV exposed uninfected; CHUU, child who is HIV unexposed uninfected. HUU, HIV unexposed uninfected; HEU, HIV exposed uninfected.
3.3 Multivariate analyses of neurodevelopmental outcomes- perinatal exposures and socioeconomic status
We next investigated how birth outcomes modified associations between HEU exposure status and the neurodevelopmental outcomes in multivariate models. Due to high correlation between perinatal variables (see methods) only gestational age at birth and being born SGA were considered. After controlling for these two variables, the differences in Verbal Comprehension were no longer significant in male CHEU. Working Memory (mean difference −12.14, p = 0.002) and Processing Speed indices (mean difference −9.17, p = 0.022), Full Scale IQ (mean difference −8.97, p = 0.027), and Core (mean difference −7.99, p = 0.041) and Expressive Language (mean difference −7.72, p = 0.048) scores remained significantly lower in male CHEU. Being SGA, regardless of HEU-status, was associated with significant declines in Processing Speed Index (mean difference −7.32, p = 0.047), Full Scale IQ (mean difference −9.03, p = 0.023), and Core (mean difference −9.31, p = 0.041) and Receptive (mean difference −9.97, p = 0.019) Language scores.
To account for socioeconomic status, we further controlled for household income in addition to gestational age at birth and SGA (Table 3). Household income was significantly associated with performance on all the cognitive measures except working memory. Including household income in the model led to a reduction in magnitude of all coefficients associated with HEU exposure status, with the exception of working memory (Table 3).
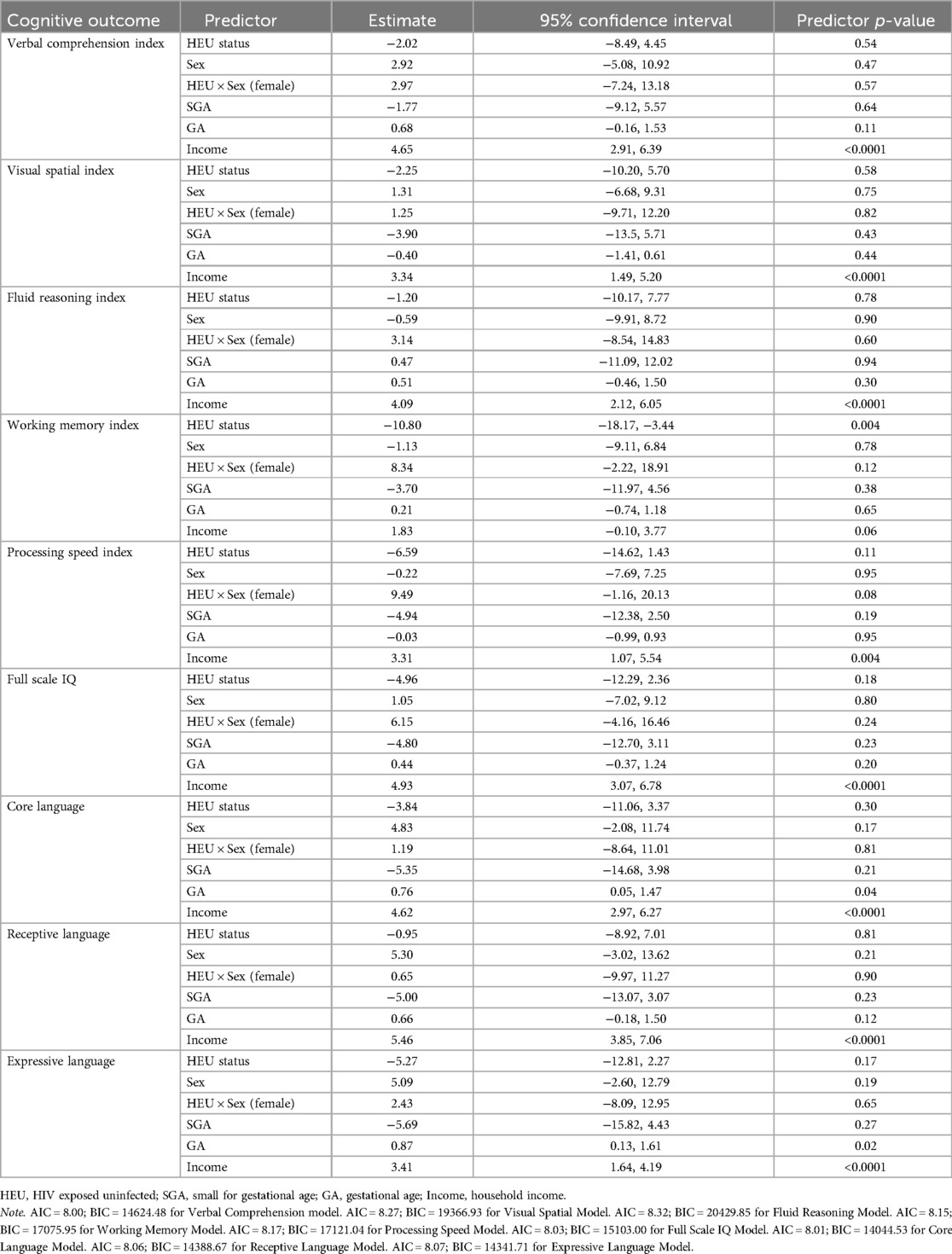
Table 3. Multivariate linear regression results for neurodevelopmental outcomes comparing groups, controlling for GA, SGA, and income.
4 Discussion
In this study, school-aged CHEU had lower mean scores on Working Memory and Expressive Language measures compared to CHUU. This is in contrast to previous studies that did not find these differences in infancy or early childhood (11, 17, 18, 21, 24, 25). Our results contribute to the understanding that cognitive deficits in CHEU may become more observable at later stages of childhood, as highlighted previously (23, 33–36). Importantly, our findings identify sex-specific vulnerabilities, with significant deficits being seen in male, but not female, CHEU in this cohort. Our results also highlight a distinct and persistent area of intrinsic challenge in working memory abilities, particularly for male CHEU, even after accounting for perinatal (gestational age at birth and SGA) and socioeconomic factors (income). Finally, our findings highlight the importance of economic factors, with household income being strongly associated with all neurodevelopmental measures, apart from Working Memory Index.
The sex-specific vulnerability observed in our study, even after controlling for perinatal risk factors, is a novel contribution to the literature. The few studies on school-aged CHEU (33, 35) have controlled for sex in their analysis rather than specifically examining for sex differences, and the limited research examining sex differences has not identified these discrepancies in younger groups (24, 25). Further, studies suggesting male vulnerabilities have not included comparisons with CHUU (37), hindering the generalizability of the findings, as without a comparison group, it can be speculated that males may be at a higher risk of neurodevelopmental deficits, regardless of HEU-status (38). These observed sex differences may indicate that male CHEU are more susceptible to maternal HIV and potentially ART exposures in the intrauterine environment. The intrauterine environment tends to be more pro-inflammatory for male fetuses compared to female fetuses (39, 40). Specifically, the male placenta has been shown to be less protective against inflammatory and infectious insults, which could make male fetuses more susceptible to in utero exposure to HIV and ARTs (39, 40). Studies have also shown that male and female fetuses respond differently to prenatal adversities, with male fetuses prioritizing physical growth at the expense of other organ processes. This may make male fetuses less adaptable to in utero changes, increasing the risk for adverse downstream effects, including on neurodevelopment (41). However, it is important to consider that societal and gender expectations may also contribute to the masking of more subtle language or cognitive challenges in girls that may not be captured through our standardized measures (42, 43).
Including perinatal factors (SGA and gestational age at birth) in the analyses led to only minor attenuations in HEU group differences. While factors such as prematurity and intrauterine growth restriction are known to influence early neurodevelopment, their long-term effects on cognition may be attenuated by other environmental factors as the child develops (10). In our study, household income had a substantial impact on intelligence and language outcomes in both CHEU and CHUU groups, highlighting the critical role of the broader socioeconomic environment in a child’s development over time. Socioeconomic status can impact neurodevelopment from conception through adulthood via direct and indirect pathways, such as perinatal exposure (e.g., nutrition), psychosocial stress, access to resources, educational opportunities, and cognitive stimulation (44). Further, the household and environmental context of CHEU is influenced by a series of indirect risks for child development, such as caregiver illness and hospitalization, and the mental health burden of HIV diagnosis (45, 46). These factors may limit social interaction and cognitive stimulation during early development, further impacting children’s cognitive, learning, and social development (47). The present finding raises the possibility of considering policies such as universal basic income, which is particularly relevant for the CHEU population where lower household income is more prevalent and income disparities are likely to compound neurodevelopmental challenges (23, 48). Further, the findings on household income can also indicate the impact of other related variables, such as single-parent households and additional socio-demographic challenges. Therefore, it is crucial to consider policies that address these broader socioeconomic disparities.
The most consistent finding of our study is that working memory deficits in CHEU persist even after controlling for perinatal risk factors and also socioeconomic status. In addition, the number of CHEU with clinically impaired Working Memory scores were significantly higher compared to CHUU, reflecting disparities between the groups (49). The observed working memory deficits align with the findings of a previous study on verbal working memory in school-aged CHEU (50). Working memory abilities may be more susceptible to the impacts of HIV and ART exposures in CHEU due to the prolonged development time of prefrontal lobes, and differences may become more evident in older children due to the later emergence of working memory and executive functioning abilities in childhood (49). Working memory is fundamental to learning and academic achievement (51), attentional control (52), development of cognitive abilities such as reasoning, problem-solving, decision-making (53), and social skills (54). Working memory deficits are also associated with broader executive functioning difficulties (55). These skills develop in later childhood and can be better assessed beginning at school age and into adolescence, when children have had more exposure to external factors, such as social and cognitive stimulation and learning environments. Working memory deficits may contribute to academic challenges observed in CHEU (56). Future research could further explore the association between working memory, executive functioning skills, and academic development in CHEU. Further, our findings suggest that a more extended follow-up period into middle childhood and adolescence is essential. Close follow-up of the CHEU population in the school-age period provides an opportunity for early intervention to improve broader executive functioning during these sensitive developmental stages.
Several limitations must be acknowledged. Our CHEU and CHUU samples are relatively small, impacting the statistical power to conduct between-sex analyses and the generalizability of the findings. In addition, recruitment bias might have impacted our findings, as parents suspecting neurodevelopmental challenges may have been more inclined for their children to participate in the study; however, this is unlikely to explain the observed sex differences. Further, while our study revealed a higher risk of working memory deficits in CHEU, we were unable to provide a precise mechanism underlying this association. Previous literature has identified associations between specific ART regimens and language outcomes (19), however, due to sample size limitations, we did not explore these associations. Finally, we are only able to present findings from assessment at a single time point. Tracking neurodevelopmental trajectories longitudinally would be more informative and is planned as part of the larger KIND study.
In conclusion, our study contributes to the growing body of research on the neurodevelopmental outcomes of CHEU. We found neurodevelopmental vulnerabilities in school-aged CHEU, with male CHEU showing greater vulnerability for poorer intellectual and language outcomes. Household income was identified as a contributing factor for most of these neurodevelopmental challenges, but even after controlling for income, working memory deficits persisted in CHEU, highlighting a poorer outcome due to HEU status. Our findings emphasize the need for close neuropsychological follow-up in this population beyond five years of age and potential early interventions and supports, particularly for CHEU males and those born into low-income households. Further, our findings highlight the necessity for future research to continue to explore the complex interplay between biological and psychosocial factors, HIV and ART exposure, brain development, and neurodevelopmental outcomes in CHEU.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the corresponding author upon reasonable request.
Ethics statement
The studies involving humans were approved by The Institutional Review Boards of The Hospital for Sick Children, Children’s Hospital of Eastern Ontario, and University Health Network approved the protocol. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
LK: Formal analysis, Writing – original draft. MS: Conceptualization, Supervision, Writing – original draft. AB: Conceptualization, Investigation, Writing – review & editing. JB: Conceptualization, Investigation, writing – review & editing. JS: Conceptualization, Writing – review & editing. EM: Conceptualization, Writing – review & editing. JB: Project administration, Data curation, Writing – review & editing. MH: Investigation, Writing – review & editing. LS: Conceptualization, Supervision, Formal analysis, Writing – original draft, Funding acquisition. JY: Conceptualization, Supervision, Formal analysis, Writing – original draft.
KIND study team
Dr. Ari Bitnun, Dr. Jason Brophy, Jennifer Bowes, Dr. Shreya Dhume, Dr. Eve Forster, Dr. Marieve Hurtubise, Haoua Inoua, Majorie Kabahenda, Cassandra Kapoor, Dr. Elka Miller, Dr. Stephanie León, Dr. Jason Lerch, Dr. Lena Serghides, Dr. John Sled, Dr. Mary Lou Smith, Nicci Stein, Dr. Michael Szego, Dr. Margot Taylor, Dr. Julia Young, Dr. Mark Yudin.
KIND study staff
Cheryl Arneson, Jennifer Brazeau, Meaghan Hall, Matt Head, Victoria Kim, Dr. Tamara Tavares, Bilal Syed, Lindsey Ure, Tharaniya Kumarathasan.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by funding from a Canadian Institutes of Health Research Team Grant HIV/AIDS Comorbidities Prevention and Healthy Living #HAL-157984. The funder had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript or in the decision to publish the results. JY is supported by the Canadian Institutes of Health Research Fellowship (HIV-176646). LS is supported by a Tier 1 Canada Research Chair in Maternal-Child Health and HIV. JS is supported by the Canada Research Chair in Biomedical Imaging. For the remaining authors none were declared.
Acknowledgments
We are grateful to the children and their families for making this study possible with their participation. We acknowledge all KIND study team members for their contributions to the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1540420/full#supplementary-material
References
1. UNAIDS. Latest data on HIV 2023 (2023). Available online at: https://aidsinfo.unaids.org/ (Accessed November 11, 2024).
2. Haddad N, Weeks A, Robert A, Totten S. HIV in Canada—surveillance report, 2019. Canada Commun Dis Rep. (2021) 47(1):77–86. doi: 10.14745/ccdr.v47i01a11
3. Afran L, Garcia Knight M, Nduati E, Urban BC, Heyderman RS, Rowland-Jones SL. HIV-exposed uninfected children: a growing population with a vulnerable immune system? Clin Exp Immunol. (2014) 176(1):11–22. doi: 10.1111/cei.12251
4. Mofenson LM. Editorial commentary: new challenges in the elimination of pediatric HIV infection: the expanding population of HIV-exposed but uninfected children. Clin Infect Dis. (2015) 60:1357–60. doi: 10.1093/cid/civ064
5. Tanabe S, Yamashita T. The role of immune cells in brain development and neurodevelopmental diseases. Int Immunol. (2018) 30(10):437–44. doi: 10.1093/intimm/dxy041
6. McCormack SA, Best BM. Protecting the fetus against HIV infection: a systematic review of placental transfer of antiretrovirals. Clin Pharmacokinet. (2014) 53:989–1004. doi: 10.1007/s40262-014-0185-7
7. Evans C, Jones CE, Prendergast AJ. HIV-exposed, uninfected infants: new global challenges in the era of paediatric HIV elimination. Lancet Infect Dis. (2016) 16(6):e92–107. doi: 10.1016/S1473-3099(16)00055-4
8. Wedderburn CJ, Weldon E, Bertran-Cobo C, Rehman AM, Stein DJ, Gibb DM, et al. Early neurodevelopment of HIV-exposed uninfected children in the era of antiretroviral therapy: a systematic review and meta-analysis. Lancet Child Adolesc Health. (2022) 6(6):393–408. doi: 10.1016/S2352-4642(22)00071-2
9. Miller K, Prokasky A, Roberts H, McMorris C, Needelman H. Associations between risk factors, developmental outcomes, and executive function in neonatal intensive care unit graduates at 2 years: a retrospective study. Infant Child Dev. (2023) 32(3):e2411. doi: 10.1002/icd.2411
10. Pritchard VE, Bora S, Austin NC, Levin KJ, Woodward LJ. Identifying very preterm children at educational risk using a school readiness framework. Pediatrics. (2014) 134(3):e825–32. doi: 10.1542/peds.2013-3865
11. Chaudhury S, Williams PL, Mayondi GK, Leidner J, Holding P, Tepper V, et al. Neurodevelopment of HIV-exposed and HIV-unexposed uninfected children at 24 months. Pediatrics. (2017) 140(4):e20170988. doi: 10.1542/peds.2017-0988
12. Powis KM, Smeaton L, Hughes MD, Tumbare EA, Souda S, Jao J, et al. In-utero triple antiretroviral exposure associated with decreased growth among HIV-exposed uninfected infants in Botswana. AIDS. (2016) 30(2):211–20. doi: 10.1097/QAD.0000000000000895
13. Wu J, Li J, Li Y, Loo KK, Yang H, Wang Q, et al. Neurodevelopmental outcomes in young children born to HIV-positive mothers in rural Yunnan, China. Pediatr Int. (2018) 60(7):618–25. doi: 10.1111/ped.13584
14. Cortese M, Moster D, Wilcox AJ. Term birth weight and neurodevelopmental outcomes. Epidemiology. (2021) 32(4):583–90. doi: 10.1097/EDE.0000000000001350
15. Stålnacke SR, Tessma M, Böhm B, Herlenius E. Cognitive development trajectories in preterm children with very low birth weight longitudinally followed until 11 years of age. Front Physiol. (2019) 10:307. doi: 10.3389/fphys.2019.00307
16. Wilcox AJ. On the importance—and the unimportance—of birthweight. Int J Epidemiol. (2001) 30(6):1233–41. doi: 10.1093/ije/30.6.1233
17. Wedderburn CJ, Evans C, Yeung S, Gibb DM, Donald KA, Prendergast AJ. Growth and neurodevelopment of HIV-exposed uninfected children: a conceptual framework. Curr HIV/AIDS Rep. (2019) 16:501–13. doi: 10.1007/s11904-019-00459-0
18. le Roux SM, Donald KA, Brittain K, Phillips TK, Zerbe A, Nguyen KK, et al. Neurodevelopment of breastfed HIV-exposed uninfected and HIV-unexposed children in South Africa. AIDS. (2018) 32(13):1781–91. doi: 10.1097/QAD.0000000000001872
19. Rice ML, Russell JS, Frederick T, Purswani M, Williams PL, Siberry GK, et al. Risk for speech and language impairments in preschool age HIV-exposed uninfected children with in utero combination antiretroviral exposure. Pediatr Infect Dis J. (2018) 37(7):678–85. doi: 10.1097/INF.0000000000001875
20. Van Rie A, Mupuala A, Dow A. Impact of the HIV/AIDS epidemic on the neurodevelopment of preschool-aged children in Kinshasa, democratic republic of the Congo. Pediatrics. (2008) 122(1):e123–8. doi: 10.1542/peds.2007-2558
21. Springer PE, Slogrove AL, Kidd M, Kalk E, Bettinger JA, Esser MM, et al. Neurodevelopmental and behavioural outcomes of HIV-exposed uninfected and HIV-unexposed children at 2–3 years of age in Cape Town, South Africa. AIDS Care. (2020) 32(4):411–9. doi: 10.1080/09540121.2019.1637506
22. Garvie PA, Zeldow B, Malee K, Nichols SL, Smith RA, Wilkins ML, et al. Discordance of cognitive and academic achievement outcomes in youth with perinatal HIV exposure. Pediatr Infect Dis J. (2014) 33(9):e232–8. doi: 10.1097/INF.0000000000000314
23. Smith ML, Puka K, Sehra R, Read SE, Bitnun A. Longitudinal development of cognitive, visuomotor and adaptive behavior skills in HIV uninfected children, aged 3–5 years of age, exposed pre-and perinatally to anti-retroviral medications. AIDS Care. (2017) 29(10):1302–8. doi: 10.1080/09540121.2017.1325436
24. Boivin MJ, Maliwichi-Senganimalunje L, Ogwang LW, Kawalazira R, Sikorskii A, Familiar-Lopez I, et al. Neurodevelopmental effects of ante-partum and post-partum antiretroviral exposure in HIV-exposed and uninfected children versus HIV-unexposed and uninfected children in Uganda and Malawi: a prospective cohort study. Lancet HIV. (2019) 6(8):e518–30. doi: 10.1016/S2352-3018(19)30083-9
25. Bulterys MA, Njuguna I, King’e M, Chebet D, Moraa H, Gomez L, et al. Neurodevelopment of children who are HIV-exposed and uninfected in Kenya. J Int AIDS Soc. (2023) 26(S4):e26149. doi: 10.1002/jia2.26149
26. Stirnemann J, Villar J, Salomon LJ, Ohuma E, Ruyan P, Altman DG, et al. International estimated fetal weight standards of the INTERGROWTH-21st project. Ultrasound Obstet Gynecol. (2017) 49(4):478–86. doi: 10.1002/uog.17347
27. Wechsler D. Wechsler Intelligence Scale for Children–Fifth Edition (WISC-V). Bloomington, MN: Pearson (2014).
29. White H. A heteroskedasticity-consistent covariance matrix estimator and a direct test for heteroskedasticity. Econometrica. (1980) 48:817–38. doi: 10.2307/1912934
33. Benki-Nugent SF, Yunusa R, Mueni A, Laboso T, Tamasha N, Njuguna I, et al. Lower neurocognitive functioning in HIV-exposed uninfected children compared with that in HIV-unexposed children. JAIDS J Acquir Immune Defic Syndr. (2022) 89(4):441–7. doi: 10.1097/QAI.0000000000002881
34. McHenry MS, McAteer CI, Oyungu E, McDonald BC, Bosma CB, Mpofu PB, et al. Neurodevelopment in young children born to HIV-infected mothers: a meta-analysis. Pediatrics. (2018) 141(2):e20172888. doi: 10.1542/peds.2017-2888
35. Kerr SJ, Puthanakit T, Vibol U, Aurpibul L, Vonthanak S, Kosalaraksa P, et al. Neurodevelopmental outcomes in HIV-exposed-uninfected children versus those not exposed to HIV. AIDS Care. (2014) 26(11):1327–35. doi: 10.1080/09540121.2014.920949
36. Young JM, Bitnun A, Read SE, Smith ML. Neurodevelopment of HIV-exposed uninfected children compared with HIV-unexposed uninfected children during early childhood. Dev Psychol. (2022) 58(3):551–9. doi: 10.1037/dev0001319
37. Rice ML, Zeldow B, Siberry GK, Purswani M, Malee K, Hoffman HJ, et al. Evaluation of risk for late language emergence after in utero antiretroviral drug exposure in HIV-exposed uninfected infants. Pediatr Infect Dis J. (2013) 32(10):e406–13. doi: 10.1097/INF.0b013e31829b80ee
38. Gilmore JC, Serghides L, Bendayan R. Differential effects of antiretroviral drug toxicity in male versus female children who are HIV-exposed but uninfected. AIDS. (2021) 35(1):1–14. doi: 10.1097/QAD.0000000000002707
39. Ghidini A, Salafia CM. Gender differences of placental dysfunction in severe prematurity. BJOG. (2005) 112(2):140–4. doi: 10.1111/j.1471-0528.2004.00308.x
40. Goldenberg RL, Andrews WW, Faye-Petersen OM, Goepfert AR, Cliver SP, Hauth JC. The Alabama preterm birth study: intrauterine infection and placental histologic findings in preterm births of males and females less than 32 weeks. Am J Obstet Gynecol. (2006) 195(6):1533–7. doi: 10.1016/j.ajog.2006.05.023
41. Hodes GE, Epperson CN. Sex differences in vulnerability and resilience to stress across the life span. Biol Psychiatry. (2019) 86(6):421–32. doi: 10.1016/j.biopsych.2019.04.028
42. Hirnstein M, Stuebs J, Moè A, Hausmann M. Sex/gender differences in verbal fluency and verbal-episodic memory: a meta-analysis. Perspect Psychol Sci. (2023) 18(1):67–90. doi: 10.1177/17456916221082116
43. Rinaldi P, Pasqualetti P, Volterra V, Caselli MC. Gender differences in early stages of language development. Some evidence and possible explanations. J Neurosci Res. (2023) 101(5):643–53. doi: 10.1002/jnr.24914
44. Hackman DA, Farah MJ. Socioeconomic status and the developing brain. Trends Cogn Sci. (2009) 13(2):65–73. doi: 10.1016/j.tics.2008.11.003
45. Joseph EB, Bhatti RS. Psychosocial problems and coping patterns of HIV seropositive wives of men with HIV/AIDS. Soc Work Health Care. (2005) 39(1–2):29–47. doi: 10.1300/J010v39n01_04
46. Sherr L, Cluver LD, Betancourt TS, Kellerman SE, Richter LM, Desmond C. Evidence of impact: health, psychological and social effects of adult HIV on children. AIDS. (2014) 28:S251–9. doi: 10.1097/QAD.0000000000000327
47. Sherr L, Skeen S, Hensels IS, Tomlinson M, Macedo A. The effects of caregiver and household HIV on child development: a community-based longitudinal study of young children. Child Care Health Dev. (2016) 42(6):890–9. doi: 10.1111/cch.12387
48. Walker SP, Wachs TD, Grantham-McGregor S, Black MM, Nelson CA, Huffman SL, et al. Inequality in early childhood: risk and protective factors for early child development. Lancet. (2011) 378(9799):1325–38. doi: 10.1016/S0140-6736(11)60555-2
49. Funahashi S. Dorsolateral prefrontal Cortex. In: Funahashi S, editor. Dorsolateral Prefrontal Cortex: Working Memory and Executive Functions, Singapore: Springer Nature Singapore (2022). p. 1–51.
50. Milligan R, Cockcroft K. Working memory profiles in HIV-exposed, uninfected and HIV-infected children: a comparison with neurotypical controls. Front Hum Neurosci. (2017) 11:348. doi: 10.3389/fnhum.2017.00348
51. Swanson HL, Jerman O. The influence of working memory on reading growth in subgroups of children with reading disabilities. J Exp Child Psychol. (2007) 96(4):249–283. doi: 10.1016/j.jecp.2006.12.004
52. Kane MJ, Brown LH, McVay JC, Silvia PJ, Myin-Germeys I, Kwapil TR. For whom the mind wanders, and when: an experience-sampling study of working memory and executive control in daily life. Psychol Sci. (2007) 18(7):614–21. doi: 10.1111/j.1467-9280.2007.01948.x
53. Baddeley A. Working memory: looking back and looking forward. Nat Rev Neurosci. (2003) 4(10):829–39. doi: 10.1038/nrn1201
54. McQuade JD, Murray-Close D, Shoulberg EK, Hoza B. Working memory and social functioning in children. J Exp Child Psychol. (2013) 115(3):422–35. doi: 10.1016/j.jecp.2013.03.002
55. Miyake A, Friedman NP. The nature and organization of individual differences in executive functions: four general conclusions. Curr Dir Psychol Sci. (2012) 21(1):8–14. doi: 10.1177/0963721411429458
Keywords: HIV-exposed uninfected, neurodevelopment, working memory, intellectual abilities, language abilities, developmental trajectory
Citation: Kahnami L, Smith ML, Bitnun A, Brophy J, Sled JG, Miller E, Bowes J, Hurtubise M, Serghides L and Young JM (2025) Intelligence and language outcomes in school-aged children who are HIV-exposed, uninfected: the role of sex, perinatal risk factors, and socioeconomic status. Front. Pediatr. 13:1540420. doi: 10.3389/fped.2025.1540420
Received: 6 December 2024; Accepted: 24 June 2025;
Published: 17 July 2025.
Edited by:
Rachana Singh, Tufts University, United StatesReviewed by:
Thais Louvain De Souza, Faculdade de Medicina de Campos, BrazilNadia Ikumi, University of Cape Town, South Africa
Copyright: © 2025 Kahnami, Smith, Bitnun, Brophy, Sled, Miller, Bowes, Hurtubise, Serghides and Young. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lena Serghides, bGVuYS5zZXJnaGlkZXNAdXRvcm9udG8uY2E=; Julia M. Young, anVsaWEueW91bmdAc2lja2tpZHMuY2E=
†These authors share senior authorship