 Ashlinn K. Quinn1*
Ashlinn K. Quinn1* Gila Neta2
Gila Neta2 Rachel Sturke1
Rachel Sturke1 Christopher O. Olopade3
Christopher O. Olopade3 Suzanne L. Pollard4
Suzanne L. Pollard4 Kenneth Sherr5
Kenneth Sherr5 Joshua P. Rosenthal1
Joshua P. Rosenthal1- 1Fogarty International Center, U.S. National Institutes of Health, Bethesda, MD, United States
- 2National Cancer Institute, U.S. National Institutes of Health, Bethesda, MD, United States
- 3University of Chicago Medicine, University of Chicago, Chicago, IL, United States
- 4Department of Medicine, Johns Hopkins University, Baltimore, MD, United States
- 5Department of Global Health, University of Washington, Seattle, WA, United States
Introduction: The use of models and frameworks to design and evaluate strategies to improve delivery of evidence-based interventions is a foundational element of implementation science. To date, however, evaluative implementation science frameworks such as Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) have not been widely employed to examine environmental health interventions. We take advantage of a unique opportunity to utilize and iteratively adapt the RE-AIM framework to guide NIH-funded case studies of the implementation of clean cooking fuel programs in eleven low- and middle-income countries.
Methods: We used existing literature and expert consultation to translate and iteratively adapt the RE-AIM framework across several stages of the NIH Clean Cooking Implementation Science case study project. Checklists and templates to guide investigators were developed at each stage.
Results: The RE-AIM framework facilitated identification of important emerging issues across this set of case studies, in particular highlighting the fact that data associated with certain important outcomes related to health and welfare are chronically lacking in clean fuel programs. Monitoring of these outcomes should be prioritized in future implementation efforts. As RE-AIM was not originally designed to evaluate household energy interventions, employing the framework required adaptation. Specific adaptations include the broadening of Effectiveness to encompass indicators of success toward any stated programmatic goal, and expansion of Adoption to include household-level uptake of technology.
Conclusions: The RE-AIM implementation science framework proved to be a useful organizing schema for 11 case studies of clean fuel cooking programs, in particular highlighting areas requiring emphasis in future research and evaluation efforts. The iterative approach used here to adapt an implementation science framework to a specific programmatic goal may be of value to other multi-country program efforts, such as those led by international development agencies. The checklists and templates developed for this project are publicly available for others to use and/or further modify.
Introduction
The Health Potential of Cooking With Clean Fuels
Reducing the morbidity and mortality attributable to cooking with solid fuels (e.g., wood, dung, charcoal, and crop residues) and kerosene is a significant public health priority. Approximately 3 billion people currently cook with these polluting fuels, and exposure to household air pollution (HAP) from burning these materials is estimated to result in 2.6–4.3 million premature deaths a year (1, 2). Shifting to cleaner alternatives [e.g., liquefied petroleum gas (LPG), ethanol, biogas, and electricity] would result in progress toward multiple global goals, from improvement in public health to climate change mitigation (3). As the transition to cleaner cooking technologies has already occurred in higher-income countries, the existing imperative is therefore one of implementation: how do we achieve the extension of what is known (clean fuels reduce air pollution and protect health) to what is practiced (sustained and exclusive use of clean fuels for cooking), in the variety of settings where people rely on polluting solid fuels to meet their cooking needs?
There are numerous examples demonstrating the implementation gap that has impeded the achievement of health goals in the clean cooking sphere. For example, many programs have promoted “improved” stoves that still use relatively unprocessed biomass fuels such as wood and charcoal. While they may reduce fuel use, often can be produced locally, and may provide some reduction in air pollution, these stoves generally do not reduce pollution to the guideline levels established by the World Health Organization (WHO) that are understood to be required to minimize adverse health impacts (2). A shift in focus to stoves powered by “clean” fuels such as gas (biogas/LPG/natural gas), electricity, and in some cases processed biomass pellets (4) would help greatly in at least setting the stage for achieving the HAP reductions that are sought.
All these fuels require money to purchase, however, so financing for clean stoves and fuels is another area ripe for implementation research. As is true for many other development objectives, the populations most affected by HAP are often those least able to afford the financial investments required to transition to clean fuels (5, 6). Nonetheless, income has been shown to be less strongly associated with use of clean fuels than otherwise might be expected (7). Meanwhile, despite the fact that recent field and modeling studies show that exclusive or near exclusive use of clean fuels is required to achieve the WHO air quality targets (8, 9), adoption of clean fuels for cooking is often incomplete. Households regularly continue to cook with their traditional stoves even as they begin cooking with a new and cleaner stove (10), a practice called “stacking” which subverts the achievement of substantial air pollution reductions. Lastly, to achieve meaningful reductions in household air pollution, attention must also be paid to background ambient air quality that reflects larger, community-scale energy use and structural dynamics, and not just individual and household-level behaviors (11).
The Clean Cooking Implementation Science Network's Case Study Project
The field of implementation science is well-suited to investigate these questions (12). Implementation science makes ample use of theories and frameworks, which have been shown to enhance the effectiveness of evidence-based health interventions (13) by informing development of nd implementation strategies that are adapted to different settings and improve intervention success (14, 15). Employing the tools of implementation science to better understand how to close the clean-fuel cooking implementation gap has been identified as a priority by the U.S. National Institutes of Health (16), which launched the Clean Cooking Implementation Science Network (ISN), https://www.fic.nih.gov/About/Staff/Policy-Planning-Evaluation/Pages/clean-cooking-implementation-science-network.aspx, in 2015 in partnership with the U.S. Agency for International Development (USAID), the Centers for Disease Control and Prevention (CDC), the Environmental Protection Agency (EPA), and the Clean Cooking Alliance (CCA). The network is composed of researchers working on issues related to household air pollution and cooking energy transitions hailing from a number of academic disciplines (e.g., environmental health, medicine, epidemiology, economics, anthropology, and ecology), as well as government officials from relevant agencies and ministries, representatives of clean fuel implementing organizations and NGOs, and experts in implementation science. The guiding aims for the network are to advance the science of uptake and scale-up of clean-fuel cooking technology in low-and middle-income countries and to foster collaborative efforts and understanding among researchers and implementers toward this end.
The Clean Cooking ISN's case study project was initiated after a series of meetings in 2016 with the ISN network and its Steering Committee. In these meetings, participants identified a notable lack of documented literature relating to specific cases of success and/or failure of clean-fuel cooking implementation efforts, despite the fact that clean fuel programs and clean cooking programs are rolling out around the world. The Clean Cooking Alliance, a network of partners invested in expanding adoption of clean cooking solutions, set an initial goal of fostering the adoption of clean cooking in 100 million homes globally by 2020 (17), a target that is likely to be exceeded. Meanwhile, efforts led by national governments and multinational organizations are promoting clean-fuel cooking solutions at a grand scale: India's Pradhan Mantri Ujjwala Yojana program, for example, reports that it has already expanded access to LPG to 85% of the national population (18). World Bank programs and other bilateral funders have also participated in funding and promoting clean-fuel cooking solutions. Despite all of this investment, however, evaluation of these programs has been minimal to date.
The ISN thus initiated a call for proposals in late 2016 for the development of case studies to evaluate clean fuel cooking programs in low and middle-income countries. Eleven programs were selected for development into case studies and were subsequently published as a Special Issue in Energy for Sustainable Development, titled “Scaling up clean fuel cooking programs in low and middle-income countries”(19). Briefly, the case studies comprise: four LPG scale-up initiatives, in Cameroon, Ghana, Indonesia, and Peru; two biogas programs, in Cambodia and East Africa; two compressed biomass projects, in Rwanda and China; two alcohol fuel programs, in Ethiopia and Nigeria; and a case study of energy transitions in Ecuador encompassing both a historical LPG effort and a more recent electric induction program (see Table 1).
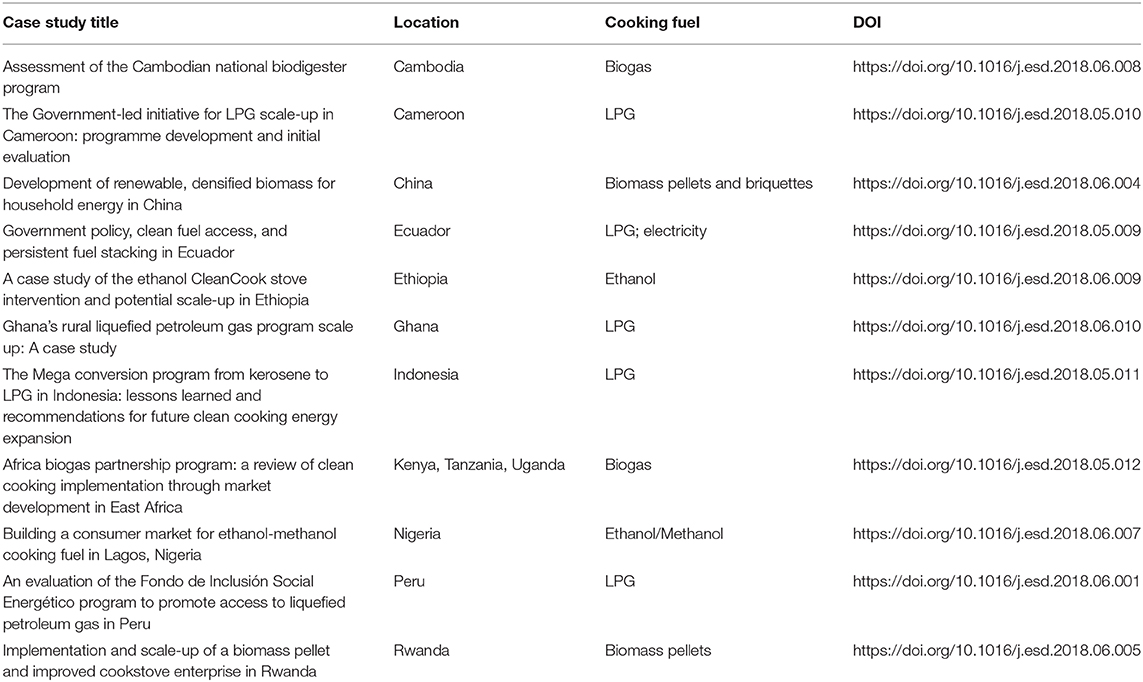
Table 1. Clean fuel cooking program case studies.
The RE-AIM Framework
We chose to organize the case study project around the commonly used implementation science framework, Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) (20), in an effort to standardize data collection and reporting. RE-AIM is one of the most frequently applied implementation frameworks (21), and had previously been introduced to the ISN network at its initial network meeting in 2015. RE-AIM is often used to evaluate programs and thus was seen as appropriate to the largely retrospective nature of the case study project. Although RE-AIM has previously been used outside of health care systems [see (21, 22) for some examples], and the developers of RE-AIM have been actively engaged in exploring applications of the framework in a diversity of settings (23), applications of RE-AIM in low- and middle-income countries (LMICs) are still relatively uncommon. To date there are also relatively few examples of the use of RE-AIM in the field of environmental health [see (24)]. The ISN felt that using RE-AIM to guide the case study project was an opportunity not only to learn generalizable lessons about clean cooking programs and compare case studies across countries, but also to provide the field with information that would advance the use of RE-AIM in LMIC settings.
The RE-AIM framework posits that public health impact of an evidence-based intervention will be achieved if an EFFECTIVE intervention REACHes a broad and representative segment of the population by being ADOPTED by willing organizations and staff, IMPLEMENTED as intended, and MAINTAINED over time by organizations and individuals. Each of the five elements, thus, is equally important to success as measured by public health impact—and importantly, data associated with all five aspects are essential to understanding the success, or failure of any implementation effort and to generalize from this experience to other settings. Initially used primarily as an evaluation tool for health behavior research, RE-AIM has expanded to cover diverse public health content and multiple research stages, including planning and study design, as well as assessment and evaluation of programs and policies (22, 25). Here, we discuss how we used RE-AIM to develop a generalizable framework for use in the evaluation of clean fuel adoption programs in LMIC settings.
Methods
RE-AIM was used at each stage of the case study project, namely: during the call for proposals, proposal evaluation and selection, data collection, manuscript writing, and summarization. The framework for clean-fuel cooking was iteratively adapted as the project progressed (see Figure 1). The main outputs of this process were two RE-AIM templates: first, a checklist used during the proposal stage (see Table 2); and second, a data collection template to guide case study teams in gathering and summarizing data for each RE-AIM dimension (see Table 3). The checklist in Table 2 contained fields for case study developers to indicate the availability of data pertaining to each RE-AIM dimension, indicating whether the data were qualitative or quantitative in nature and a description of plans to collect any data that were not pre-existing.
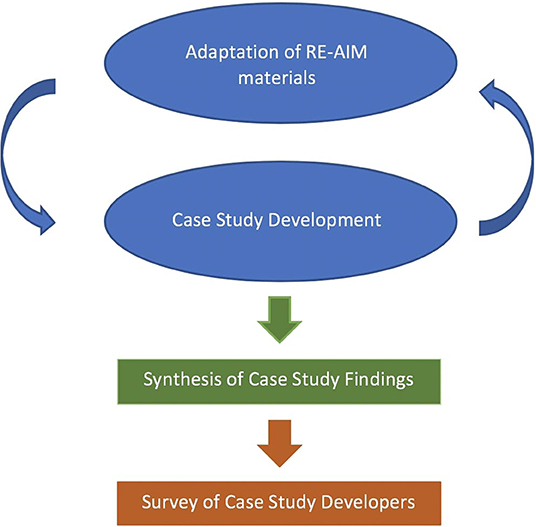
Figure 1. Flow chart of activities.
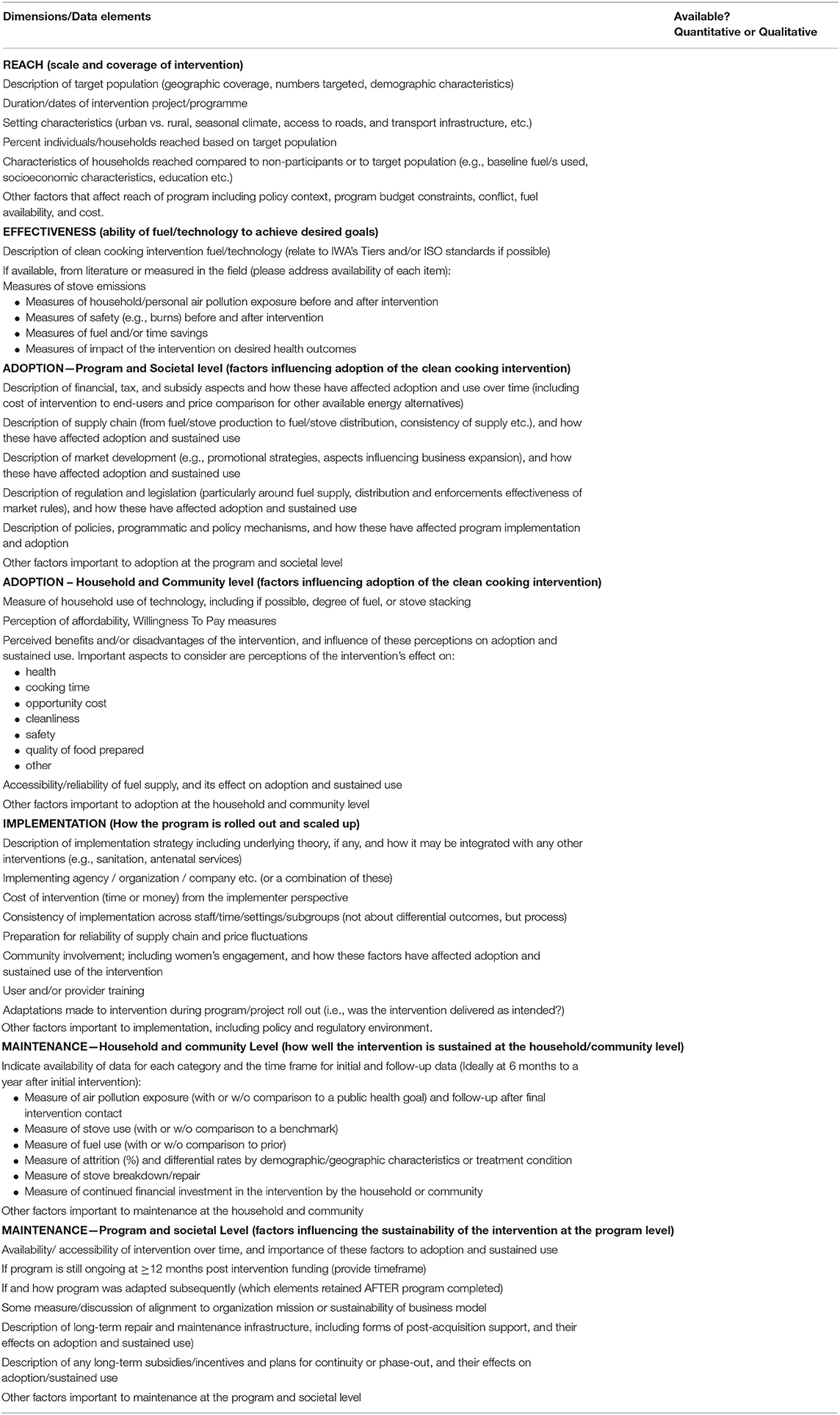
Table 2. Initial RE-AIM checklist developed for case study proposals.
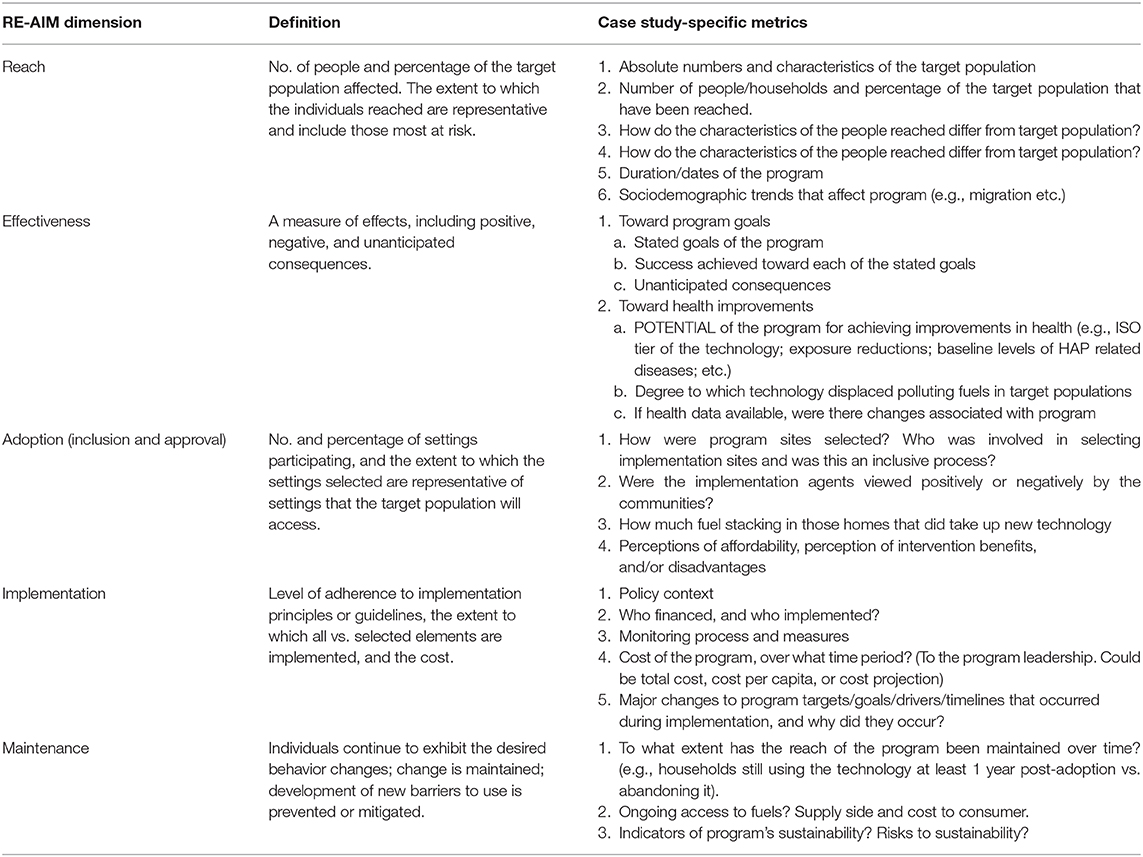
Table 3. Simplified RE-AIM data gathering template for clean cooking programs.
Development of Templates for Case Study Proposal Selection and Case Study Development
The development of each of the two templates (the RE-AIM checklist and the data collection template) occurred iteratively. A case study working group comprised of ISN leadership and interested ISN members convened in a series of virtual meetings and via email correspondence to develop and refine these templates. The working group members were academics and government officials trained in a variety of specialties spanning the health sciences (epidemiology, environmental health, medicine, global health), social sciences (economics, anthropology, and management), and implementation science. In developing the templates, we consulted existing RE-AIM material (e.g., that available on the website re-aim.org) and prior literature on the use of RE-AIM in environmental health and community-based applications [e.g., (24, 26)]. We used these pre-existing materials alongside our prior knowledge of clean cooking programs to generate indicators that were thought to be relevant to the case study project.
Over time, we iteratively modified the indicators based on feedback and the experiences of the case study teams. For example, each prospective case study team submitted a RE-AIM checklist (Table 2) along with their case study proposal. When the working group reviewed these checklists, we noted areas of potential overlap, points of confusion, and categories that were commonly reported as “data not available” across the proposals. We then used these learnings to create the case study development template (Table 3). Lastly, we made small modifications to each template prior to presenting them in this manuscript to further refine and clarify any elements that had presented any confusion during the development of the case studies. Elements that contributed to these iterative changes included the availability of data, clarity of indicators (and differentiation from other indicators), and qualitative and quantitative feedback from the case study authors.
Synthesis of Case Study Findings
After the case studies had been developed, ISN leadership consolidated and edited the 11 RE-AIM data tables submitted alongside the narrative case studies into a single summary spreadsheet that was published with the Special Issue in Energy for Sustainable Development (19).
Perceptions of Case Study Developers
We gathered the perceptions of the case study developers on the utility of RE-AIM for the case study project using a questionnaire. The questionnaire consisted of 13 questions covering the following general areas: (1) prior experience with RE-AIM; (2) Perceived ease and usefulness of employing RE-AIM for this project; (3) Challenges presented by the particular RE-AIM constructs (reach, effectiveness, adoption, implementation, maintenance); (4) Impact on future work. The questionnaire employed a mixture of question types, including multiple choice, Likert scale, ranking, and open-ended responses and was deployed to the case study developers using an online survey platform. The full set of survey questions can be found in the Supplemental Material. Eighteen case study developers provided feedback using the online questionnaire, and this feedback was synthesized and analyzed by the authors of this manuscript. Analysis of responses consisted of summary statistics (for quantitative items) and grouping of responses by theme and content (for qualitative items).
The clean cooking fuel case studies that employed the adapted RE-AIM tool were reviewed and approved through the institutional review boards (IRBs) of their respective lead investigators. Feedback from the case study investigators regarding the utility of this tool was treated as exempt, and the use of this data in this manuscript was cleared by the Fogarty International Center at the U.S. National Institutes of Health.
Results
Adapted RE-AIM Templates
Outputs of this project include the RE-AIM checklist (Table 2) and data collection template (Table 3) created for the case study developers. In the initial checklist (Table 2), general RE-AIM indicators were combined with domain-specific information about clean fuel cooking programs and policies. For example, the checklist asked for ratings of the stove and fuels used according to the International Organization for Standardization's Interim Workshop Agreement Guidelines for evaluating cookstove performance (27). We also asked for information about fuel supply policies, stove stacking, and women's engagement in implementation efforts. Some of these indicators were drawn from a framework of Adoption Indicators previously generated by the Clean Cooking Alliance (28).
Table 3 is the RE-AIM data collection template that was provided to case study developers to define case study metrics across the five RE-AIM dimensions as part of case study development. This template was informed by the information collected at the proposal stage (in the submitted Table 2 checklists). In some cases, alternative metrics were generated for data that were indicated in Table 2 as unlikely to be available. For example, the submitted Table 2 checklists indicated that health outcomes data were very seldom available. Due to this lack of data availability, the corresponding metric in Table 3 became one related to the potential health impact of the stove/fuel combination that was utilized in the case (relying, for example, on laboratory, and field emissions testing data conducted elsewhere for the same stove/fuel combinations being deployed; these data are often used to estimate health benefits that would be expected to accrue from reductions in exposure to particulate matter and other compounds). A comprehensive table of the RE-AIM data gathered across the eleven case studies can be found in Quinn et al. (19).
Synthesis of Case Study Findings
Figure 2 presents a summary of the availability of data for each RE-AIM dimension. In general, data were widely available for all five RE-AIM dimensions. Data to address Adoption (defined for the purposes of this project) was the most widely available, with no case studies reporting a lack of access to data related to this RE-AIM dimension. Data pertaining to Reach, Implementation, and Maintenance were also widely available. Across the 11 case studies, data was least available for the Effectiveness dimension. This was especially true for data concerning health outcomes—only two of the 11 case studies were able to report data on health impact, and these were on a limited scale. Nine of the case studies were not able to gather any data related to health outcomes. Other aspects of effectiveness that related to programmatic goals were sometimes unavailable as well, with three case studies each reporting a lack of data related to “success achieved toward each of the stated goals” and “unanticipated consequences.” The prospective nature of several case studies, e.g., Cameroon (29) and Nigeria (30), meant that less data were available across all dimensions to track RE-AIM indicators for these cases in particular.
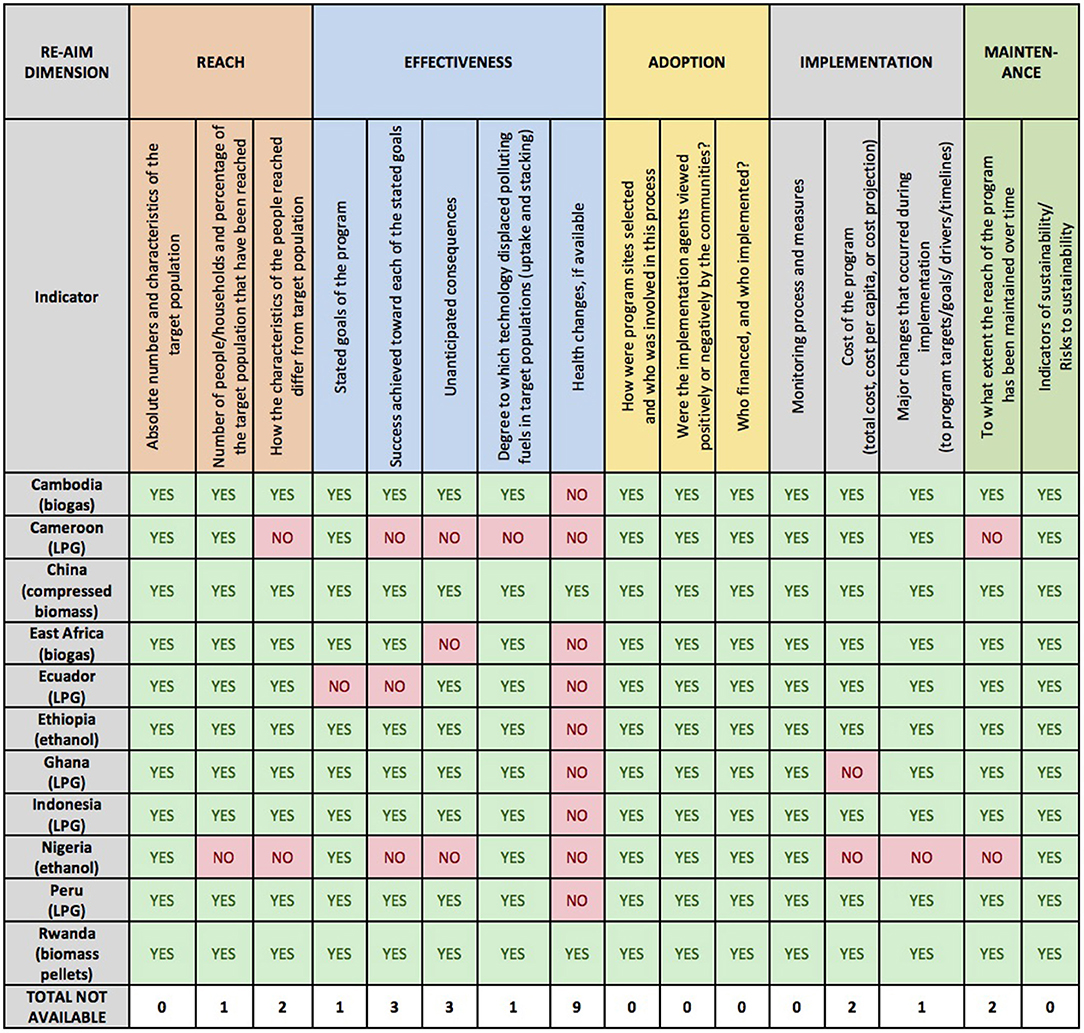
Figure 2. Summary of RE-AIM data availability across 11 case studies.
Perceptions of Case Study Developers
Perceptions of case study developers on using RE-AIM for this project were assessed using an online questionnaire. A total of 18 case study developers, including representatives from all 11 case studies, contributed their feedback on the utility of the tool. Despite the fact that the RE-AIM framework had been introduced to the ISN at a meeting in 2015, a number of case study developers did not attend that initial meeting. Thus, of the 18 respondents, the majority (12, or 67%) had never heard of RE-AIM prior to the case study project. Four respondents had heard of RE-AIM but had never used it, and only two had used it in a previous project. Nonetheless, 9 respondents (50%) found it “easy” to use, while seven found it “neither difficult nor easy,” and only two found it “difficult,” or “very difficult.”
Figure 3 shows how the case study developers ranked the different RE-AIM dimensions according to two factors: (a) level of conceptual challenge to understanding the dimension as it applied to their case; and (b) difficulty in gathering data for their case study. Case Study developers consistently ranked Reach as the least challenging dimension both for applicability to the case and for the ease of gathering relevant data. They found Effectiveness, Implementation and Maintenance to be the most challenging both to apply to the case and in terms of difficulty collecting relevant data for each dimension. This was because certain case studies were of programs at a nascent stage (with little implementation, maintenance, or outcome data yet available), and/or because of a perceived lack of fit between RE-AIM's emphasis on “program” implementation and the national-level policies and regulations that drove some cases. Across both the prospective and retrospective case studies, it was most difficult to gather data for Effectiveness (with 10 out of 18 respondents, or 55%, ranking the dimension as among the top two “most difficult” dimensions in terms of gathering data).
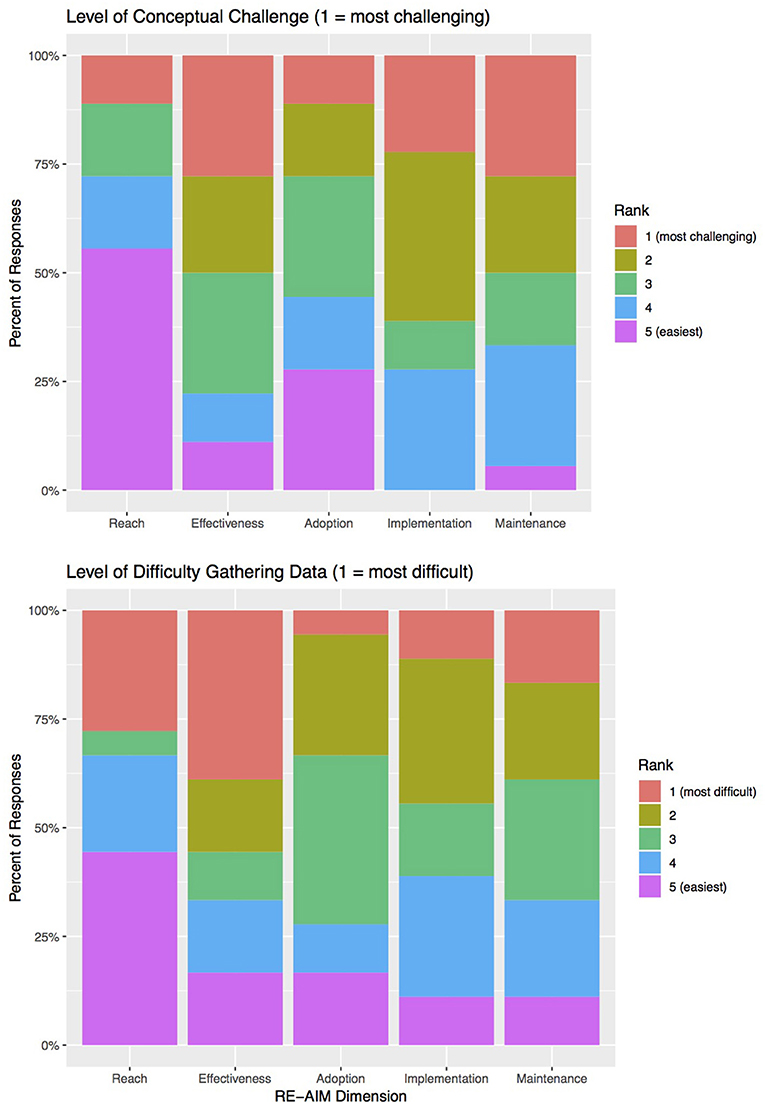
Figure 3. Case Study Developers' surveyed responses to questions about the conceptual challenge of, and difficulty gathering data for, the five RE-AIM dimensions. N = 18 responses.
Qualitative responses to open-ended questions in the survey enhance understanding of the reported challenges. For example, the reported challenges in understanding how to incorporate the dimensions of Implementation and Maintenance appear to derive from the fact that the case study project included several evaluations of clean-fuel cooking programs that had not yet been fully implemented, making evaluation of these facets difficult. Comments along these lines included, for example:
• The work on the ground is still in progress, so we were not yet able to report on many of the metrics.
• It seemed challenging to provide responses within the framework for programs that are just getting started and are anticipated to be ongoing and changing, rather than at steady state.
Difficulty in gathering data related to effectiveness often related to the fact, as discussed above, that these clean-fuel cooking programs were uniformly launched with goals that did not place health improvement at the forefront. They differ, therefore, from more clinically or public-health-oriented programs where effectiveness—in terms of achievement of health improvement—is easier to assess. A number of comments spoke to this, for example:
• My feeling was the RE-AIM was designed for a more clinical outcome and did not completely fit the context for household energy.
• RE-AIM assumes that the program driver is health, but of course often in cookstoves health is a co-benefit rather than the primary outcome.
Some case study developers additionally felt that it was difficult to fit certain contextual and implementation factors within the RE-AIM framework that were key to the case. Aspects of the case studies that the authors felt were difficult to fit in to RE-AIM included:
• The political and socio-cultural circumstances that circumscribe the subsidies
• The presence of a charismatic, committed leader.
• Use of behavior change concepts and techniques.
• The strategy for creating the conditions for investment
• ‘Logistical’ issues with clean cooking” (supply side of the fuel)
• Driving factors for decisions that were made politically
• Specific barriers to adoption and factors that can drive a wedge between adoption and health-relevant exposure reduction.
Despite these challenges and their relative lack of experience with RE-AIM, case study developers reported that the framework was useful to various aspects of the case study development process, as shown in Table 4. Using RE-AIM for understanding data availability was the aspect most commonly reported as being “very” or “extremely” useful (reported by 67% of respondents), followed by planning for data collection (56%). In their qualitative comments, however, case study team members also reported that RE-AIM was useful for comparisons across case studies:
• I do see that having a common framework among the case studies is quite beneficial.
• I found the RE-AIM summaries helped greatly in structuring information about quite complex and very different projects—a real asset.
• It has been a very useful tool for comparing across case studies.
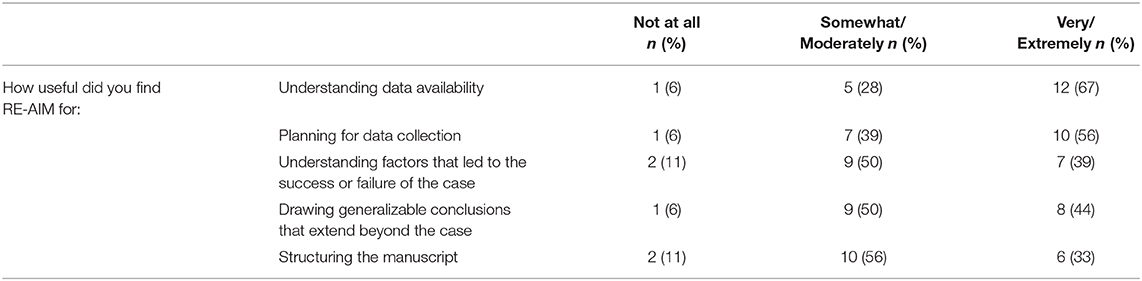
Table 4. Reported usefulness of RE-AIM for different aspects of the case study project.
Lastly, case study developers were asked to evaluate whether the experience of using RE-AIM for the clean fuel cooking case study project would lead them to approach their work differently in the future. Here, 13 out of 18 respondents (72%) replied “Yes,” with some of the specific ways that RE-AIM would influence future work outlined below:
• REAIM could help us broaden our view a little and possibly adjust some of our study design to be a bit more holistic.
• Taking a more holistic approach to data collection.
• More emphasis on measures for sustained use.
• I appreciated the variables/indicators identified under each heading, and this helped organize my thoughts.
• Having a suitable structured framework that covers all aspects of the initiative is very valuable, both for the specific example, but also for making comparisons with others.
Discussion
Clean-fuel cookstove programs are being rolled out on a massive scale, and a consolidated method for evaluating these initiatives is needed both for individual programs and also to enable cross-initiative comparisons. The NIH clean fuel case study project showed us that the RE-AIM framework has utility for these purposes, particularly with the adaptations that were made here.
The need to adapt RE-AIM for this project was not unlike previous efforts to employ RE-AIM for environmental health interventions. For example, King et al. (24) note that many of the RE-AIM dimensions are difficult to apply to environmental health interventions, such as those meant to affect air quality or improvements to public space. For example, how to calculate the “Reach” of an intervention that improves sidewalks? How to define the settings at which “Adoption” occurs in the context of an intervention targeting outdoor air pollution? Similar challenges—such as defining reach and measuring compliance—have been discussed when it comes to the use of RE-AIM for policy applications, which have some overlap with the case studies here. In the case of policy applications, enforcement is an important aspect of implementation that can directly affect compliance and strongly influence success [see (25) for examples]. In this set of clean fuel case studies, certain initiatives, such as Indonesia's “zero kero” plan, benefited from policy-like structures and robust enforcement measures, while other programs relied more on ground-up marketing and diffusion approaches that did not have the benefit of strong enforcement measures to enhance compliance and implementation.
Notable dimensions of the RE-AIM framework that required adaptation for use in the clean fuel case study project included Effectiveness and Adoption. First, translating Effectiveness for this project required acknowledgment that clean fuel scale-up initiatives have largely been driven by goals outside the health domain, e.g., pertaining to the environment and economic concerns. For example, Indonesia's “Zero Kero” program was designed to phase out highly-subsidized kerosene and thus provide savings to the national budget (31), while the aims of Ghana's rural LPG program included reducing deforestation, reducing drudgery, and creating jobs, as well as reducing the health impacts of cooking with wood and charcoal (32). We therefore proposed case study metrics for this dimension that covered effectiveness in two areas: not only effectiveness related to the reduction of household air pollution and associated health improvement, but also effectiveness in relation to the goals as put forth by the specific clean-fuel cooking program (however those may have been stated).
Adoption, in the context of clean-fuel cooking, presents a different problem since the term “adoption” is widely used in this field to refer to individual-level initial uptake of a new cooking technology, e.g., (2, 16, 33–35). This conflicts with the RE-AIM definition of adoption situated at the organizational and setting level. Defining the “setting” of a clean-fuel cooking program presented its own challenges as many programs are not managed by a clear intermediary organization (as would be the case, for example, in an intervention operating through a hospital or clinic to meet patient needs). Rather, many clean-fuel cooking programs are defined by geography or demographics (e.g., income). For the Adoption dimension of RE-AIM we therefore chose to focus on “inclusion and approval,” as suggested in King et al. (24). We developed metrics here that focused on how the program rollout was determined, who was involved in these decisions, and how the implementing agents were viewed by the community.
To minimize confusion for the clean cooking community who use adoption to mean household-level uptake of technology, we also included metrics within Adoption that pertained to cooking technology usage at the household level. An important aspect of clean fuel adoption in terms of achieving health gains is the distinction between uptake (adding a stove) and displacement (replacing a stove). This has important implications: without discontinuation of the use of polluting fuels for cooking, exposure to health-damaging emissions may not be sufficiently reduced to improve health outcomes [e.g., see (8)]. In the clean cooking research community the practice of using multiple types of stoves within a household (adding new stove technology to an existing mix, rather than replacing the older cooking technology with the newer one) is termed “stacking.” In the RE-AIM framework, the practice of stacking fuels could theoretically fit either into adoption (where it pertains to initial decisions upon adoption of a new technology) or implementation (where it pertains to patterns of use over time). The decision to include these activities in “adoption” in this project are justified by the fact that we considered fuel choice and fuel usage—including decisions to stack fuels—as intrinsic to the potential adoption process and not merely as patterns that emerge over time. Initial adoption is often only partial adoption. We also asked about household-level perceptions of the new cooking technology as part of Adoption, since these perceptions are important determinants of uptake and use of new cooking technology (36).
The remaining RE-AIM dimensions were less in need of adaptation for this purpose, although we included a metric in Maintenance focused on fuel supply (covering ongoing access to fuels and the cost to the consumer over time).
Despite its comprehensiveness, case study developers identified a number of aspects crucial to understanding their cases that were difficult to fit in to the RE-AIM framework, even after adaptations of data collection tools and templates to fit the household energy context. Some of these missing factors had to do with the larger sociopolitical context in which the cases were embedded. Notable missing elements included: “The political and socio-cultural circumstances that circumscribe the subsidies,” “driving factors for decisions that were made politically,” and the impact of “the presence of a charismatic, committed leader.” “Logistical” issues (e.g., all the steps involved in distributing clean fuels to customers and ensuring steady supply) were also mentioned as hard to fit into the RE-AIM framework, along with specific barriers impeding the transition to clean fuels for cooking, and the potential role of behavior change interventions in overcoming these barriers.
The fact that aspects of the contextual setting that are essential to implementation success were difficult to capture in RE-AIM has been noted by other researchers, and in fact RE-AIM extensions such as PRISM (37) combine RE-AIM outcome measures with other dimensions crucial to success, including “external environment” and “implementation and sustainability infrastructure.” In future applications of RE-AIM to complex community-based programs, we might suggest that researchers and program evaluators consider using PRISM or another RE-AIM extension to more comprehensively evaluate those aspects of the contextual environment that are difficult to describe using RE-AIM alone.
Using RE-AIM for the case study project also highlighted the fact that some key outcome data—in this case particularly pertaining to long-term program maintenance and health outcomes—was not routinely monitored and thus unavailable. This data gap highlights the need for engaging the health sector in longitudinal monitoring and evaluation of clean-fuel cooking initiatives. Current programmatic evaluation might focus, for example, on the number of stoves distributed. Such simplistic metrics, however, do not come close to covering the complexity of the processes related to adoption and sustained use of clean fuel cooking technologies. For example, in addition to tabulating the initial distribution of a clean-fuel cooking solution, it is imperative to also investigate whether households use the stoves, whether they continue to use them over time, and whether the use of the stoves is exclusive or in conjunction with other, polluting stoves and fuels. Employing systematic approaches, ideally with common metrics, will greatly enhance the ability of the international development community to evaluate projects taking place around the world against national, bilateral and global targets, for example targets associated with the Sustainable Development Goals (38).
The overall approach of this case study project was to engage interdisciplinary teams of researchers who employed RE-AIM in a complementary fashion with additional tools to enhance the value of the project by providing data on these additional dimensions of context and climate. This approach could certainly be extended to additional domains beyond clean fuels for cooking. Meanwhile, the specific adaptations and templates developed for this project could be useful starting points to guide future researchers in the household energy domain who are interested in program planning and/or evaluation.
Conclusions
Implementation science frameworks such as Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) have been shown to enhance the effectiveness of interventions and can be used to evaluate factors associated with implementation success. This is the first known example using RE-AIM to evaluate clean fuel cooking programs in low- and middle-income countries.
Utilizing RE-AIM for the clean cooking community required adapting and operationalizing the framework. Specific adaptations included: specifying the metrics that would be able to inform each of the RE-AIM dimensions, taking account of the pre-existing meaning of some terms (e.g., adoption) in the clean cooking community, and broadening certain dimensions (e.g., effectiveness) to capture program-relevant outcomes. Case study developers found RE-AIM to be useful and relatively easy to use for gathering data and evaluating the clean fuel initiatives. The case study teams reported particular value from the RE-AIM framework when it came to comparing common elements of disparate programs. In the future, RE-AIM extensions such as PRISM might be useful to consider when evaluating community-based interventions to capture aspects of the contextual environment that were difficult to describe using RE-AIM alone.
Key findings from the case study project suggest that long-term monitoring and evaluation of clean-fuel cooking scale-up programs is often lacking, particularly regarding indicators relevant to sustained use of new cooking technology. Health outcome measures and measures of air pollution reduction are also insufficiently tracked. A recommendation to future implementers and evaluators of clean fuel cooking programs is to build infrastructure into their programs that will ensure middle- and long-term monitoring of these key indicators of implementation success.
Finally, this effort demonstrates how a commonly used implementation science framework can be adapted for use in low-and middle-income settings and in contexts where programs are not specifically driven by health objectives. Employing frameworks like these can yield robust program evaluations that can be used to assess program performance in light of national and international goals.
Data Availability Statement
All datasets generated for this study are included in the article/Supplementary Material.
Author Contributions
AQ and JR managed the project. AQ, JR, GN, and RS contributed to the design of the RE-AIM templates. AQ and GN compiled the data. AQ drafted the manuscript. CO, SP, and KS contributed sections of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
Funding
The Clean Cooking ISN is hosted by the Center for Global Health Studies at NIH's Fogarty International Center (FIC) and was supported by the NIH Common Fund.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. National Institutes of Health or Department of Health and Human Services.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2019.00389/full#supplementary-material
References
1. GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the global burden of disease study 2016 - the lancet. Lancet. (2017) 390:1345–422. doi: 10.1016/S0140-6736(17)32366-8
2. World Health Organization. Who Indoor Air Quality Guidelines: Household Fuel Combustion. (2014). Available online at: http://www.who.int/indoorair/guidelines/hhfc/HHFC_guidelines.pdf
3. Rosenthal J, Quinn A, Grieshop AP, Pillarisetti A, Glass RI. Clean cooking and the sdgs: Integrated analytical approaches to guide energy interventions for health and environment goals. Energy Sust Dev. (2018) 42:152–9. doi: 10.1016/j.esd.2017.11.003
4. Champion WM, Grieshop AP. Pellet-fed gasifier stoves approach gas-stove like performance during in-home use in Rwanda. Environ Sci Technol. (2019) 53:6570–79. doi: 10.1021/acs.est.9b00009
5. Malla S, Timilsina GR. Household cooking fuel choice and adoption of improved cookstoves in developing countries: a review. In: Policy Research Working Paper Series 6903. The World Bank (2014). doi: 10.1596/1813-9450-6903
6. Mobarak AM, Dwivedi P, Bailis R, Hildemann L, Miller G. Low demand for nontraditional cookstove technologies. Proc Natl Acad Sci USA. (2012) 109:10815–20. doi: 10.1073/pnas.1115571109
7. van der Kroon B, Brouwer R, van Beukering PJH. The energy ladder: Theoretical myth or empirical truth? Results from a meta-analysis. Renew Sust Energy Rev. (2013) 20:504–13. doi: 10.1016/j.rser.2012.11.045
8. Johnson MA, Chiang RA. Quantitative guidance for stove usage and performance to achieve health and environmental targets. Environ Health Perspect. (2015) 128:820–6. doi: 10.1289/ehp.1408681
9. Snider G, Carter E, Clark S, Tseng JTW, Yang X, Ezzati M, et al. Impacts of stove use patterns and outdoor air quality on household air pollution and cardiovascular mortality in southwestern china. Environ Int. (2018) 117:116–24. doi: 10.1016/j.envint.2018.04.048
10. Ruiz-Mercado I, Masera O. Patterns of stove use in the context of fuel-device stacking: rationale and implications. Ecohealth. (2015) 12:42–56. doi: 10.1007/s10393-015-1009-4
11. Smith KR. Changing paradigms in clean cooking. Ecohealth. (2015) 12:196–9. doi: 10.1007/s10393-015-1020-9
12. Eccles MP, Mittman BS. Welcome to implementation science. Implement Sci. (2006) 1:1. doi: 10.1186/1748-5908-1-1
13. Tabak RG, Khoong EC, Chambers DA, Brownson RC. Bridging research and practice: Models for dissemination and implementation research. Am J Prev Med. (2012) 43:337–50. doi: 10.1016/j.amepre.2012.05.024
14. Galea S. An argument for a consequentialist epidemiology. Am J Epidemiol. (2017) 178:1185–91. doi: 10.1093/aje/kwt172
15. Neta G, Brownson RC, Chambers DA. Opportunities for epidemiologists in implementation science: a primer. Am J Epidemiol. (2017) 187:899–910. doi: 10.1093/aje/kwx323
16. Rosenthal J, Balakrishnan K, Bruce N, Chambers D, Graham J, Jack D, et al. Implementation science to accelerate clean cooking for public health. Environ Health Perspect. (2017) 125:A3–7. doi: 10.1289/EHP1018
17. Clean Cooking Alliance. 100 Million by 2020: the Global Alliance for Clean Cookstoves Is Expected to Reach Its Phase I Goal Ahead of Schedule. (2014). Available online at: https://www.cleancookingalliance.org/about/news/09-30-2014-100-million-by-2020-the-global-alliance-for-clean-cookstoves-is-expected-to-reach-its-phase-i-goal-ahead-of-schedule.html (accessed November 4, 2019).
18. Kar A, Zerriffi H. Pradhan Mantri Ujjwala Yojana: Smokeless Kitchens Are Becoming a Reality. New Delhi: Financial Express (2018).
19. Quinn AK, Bruce N, Puzzolo E, Dickinson K, Sturke R, Jack DW, et al. An analysis of efforts to scale up clean household energy for cooking around the world. Energy Sust Dev. (2018) 46:1–10. doi: 10.1016/j.esd.2018.06.011
20. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the re-aim framework. Am J Public Health. (1999) 89:1322–7. doi: 10.2105/AJPH.89.9.1322
21. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. Re-aim planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health. (2019) 7:64. doi: 10.3389/fpubh,0.2019.00064
22. Gaglio B, Shoup JA, Glasgow RE. The re-aim framework: a systematic review of use over time. Am J Public Health. (2013) 103:e38–46. doi: 10.2105/AJPH.2013.301299
23. Glasgow RE, Estabrooks PE. Pragmatic applications of re-aim for health care initiatives in community and clinical settings. Prev Chronic Dis. (2018) 15:E02. doi: 10.5888/pcd15.170271
24. King DK, Glasgow RE, Leeman-Castillo B. Reaiming re-aim: using the model to plan, implement, and evaluate the effects of environmental change approaches to enhancing population health. Am J Public Health. (2010) 100:2076–84. doi: 10.2105/AJPH.2009.190959
25. Jilcott S. Applying the re-aim framework to assess the public health impact of policy change. Ann Behav Med. (2007) 34:105–14. doi: 10.1007/BF02872666
26. Sweet SN, Ginis KAM, Estabrooks PA, Latimer-Cheung AE. Operationalizing the re-aim framework to evaluate the impact of multi-sector partnerships. Implement Sci. (2014) 9:74. doi: 10.1186/1748-5908-9-74
27. ISO/IWA. Guidelines for Evaluating Cookstove Performance. (2012). Available online at: https://www.iso.org/obp/ui/#iso:std:iso:iwa:11:ed-1:v1:en (accessed February 25, 2018).
28. Clean Cooking Alliance. How do we define and measure adoption (2016)? Available online at: http://cleancookingalliance.org/about/news/02-18-2016-how-do-we-define-and-measure-adoption.html (accessed March 6, 2019).
29. Bruce N, de Cuevas RA, Cooper J, Enonchong B, Ronzi S, Puzzolo E, et al. The government-led initiative for lpg scale-up in Cameroon: programme development and initial evaluation. Energy Sust Dev. (2018) 46:103–10. doi: 10.1016/j.esd.2018.05.010
30. Ozier A, Charron D, Chung S, Sarma V, Dutta A, Jagoe K, et al. Building a consumer market for ethanol-methanol cooking fuel in Lagos, Nigeria. Energy Sust Dev. (2018) 46:65–70. doi: 10.1016/j.esd.2018.06.007
31. Thoday K, Benjamin P, Gan M, Puzzolo E. The mega conversion program from kerosene to LPG in Indonesia: lessons learned and recommendations for future clean cooking energy expansion. Energy Sust Dev. (2018) 78:274–6. doi: 10.1016/j.esd,0.2018.05.011
32. Asante KP, Afari-Asiedu S, Abdulai MA, Dalaba MA, Carrión D, Dickinson KL, et al. Ghana's rural liquefied petroleum gas program scale up: a case study. Energy Sust Dev. (2018) 46:94–102. doi: 10.1016/j.esd.2018.06.010
33. Kumar P, Dhand A, Tabak RG, Brownson RC, Yadama GN. Adoption and sustained use of cleaner cooking fuels in rural India: a case control study protocol to understand household, network, and organizational drivers. Arch Public Health. (2017) 75:70. doi: 10.1186/s13690-017-0244-2
34. Puzzolo E, Pope D, Stanistreet D, Rehfuess EA, Bruce NG. Clean fuels for resource-poor settings: a systematic review of barriers and enablers to adoption and sustained use. Environ Res. (2016) 146:218–34. doi: 10.1016/j.envres.2016.01.002
35. Ruiz-Mercado I, Masera O, Zamora H, Smith KR. Adoption and sustained use of improved cookstoves. Energy Policy. (2011) 39:7557–66. doi: 10.1016/j.enpol.2011.03.028
36. Rehfuess EA, Puzzolo E, Stanistreet D, Pope D, Bruce NG. Enablers and barriers to large-scale uptake of improved solid fuel stoves: a systematic review. Environ Health Perspect. (2014) 122:120–30. doi: 10.1289/ehp.1306639
37. Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (prism) for integrating research findings into practice. Jt Comm J Qual Patient Saf. (2008) 34:228–43. doi: 10.1016/S1553-7250(08)34030-6
38. UN General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development. UN General Assembly (2015). Available online at: https://www.refworld.org/docid/57b6e3e44.html (accessed December 10, 2019).
Keywords: RE-AIM, household air pollution, case studies, clean cooking, implementation science, program evaluation
Citation: Quinn AK, Neta G, Sturke R, Olopade CO, Pollard SL, Sherr K and Rosenthal JP (2019) Adapting and Operationalizing the RE-AIM Framework for Implementation Science in Environmental Health: Clean Fuel Cooking Programs in Low Resource Countries. Front. Public Health 7:389. doi: 10.3389/fpubh.2019.00389
Received: 14 June 2019; Accepted: 02 December 2019;
Published: 20 December 2019.
Edited by:
Russell E. Glasgow, University of Colorado Hospital, United StatesReviewed by:
Sapana R. Patel, Columbia University, United StatesAnna Chapman, Deakin University, Australia
Copyright © 2019 Quinn, Neta, Sturke, Olopade, Pollard, Sherr and Rosenthal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashlinn K. Quinn, YXNobGlubi5xdWlubkBuaWguZ292