 Zhaoya Fan
Zhaoya Fan Yuanlin Mou
Yuanlin Mou Rui Cheng
Rui Cheng Yong Zhao
Yong Zhao Fan Zhang
Fan Zhang- School of Public Health and Management, Research Center for Medicine and Social Development, Collaborative Innovation Center of Social Risks Governance in Health, Chongqing Medical University, Chongqing, China
Background: Since the outbreak of the coronavirus disease 2019 (COVID-19) world pandemic, it has had a significant negative impact on the economy and employment. The orderly resumption of work and production is an important factor in reducing the impact of the COVID-19 and an important guarantee of social and economic stability. The study aimed to investigate the knowledge, attitudes, and practice (KAP) of people returning to work about personal protection under the COVID-19 world pandemic.
Methods: During March 2020, based on WeChat, QQ and other internet platforms, online questionnaire survey was conducted by the convenience sampling method. SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA) was used for statistics analysis. Descriptive statistics and multiple linear regression analyses were conducted to analyze the data.
Results: A total of 302 valid questionnaires was collected, and the valid response rate was 86.7%. About knowledge, people who return to work had the highest awareness rate of safe communication distance and the lowest awareness rate of exposure risk levels in different workplaces. The average scores of respondents in different occupations were higher than 95 in terms of personal protective attitude. In terms of practice, the average scores of respondents in different occupations were higher than 90 points. Multiple linear regression results showed that education and place of residence were the influencing factors of knowledge, while gender was the influencing factor of practice.
Conclusion: The awareness of prevention and control among the 302 participants was good. There were differences in personal protection knowledge among different occupational groups, but there were no differences in attitude and practice. Our findings were of great significance to improve the pertinence of COVID-19 prevention programs.
Introduction
Since the end of December 2019, coronavirus disease (COVID-19) has spread rapidly in various regions of the world, and has become an issue of concern (1, 2). On January 30, 2020, the World Health Organization (WHO) announced that the world pandemic was listed as a public health emergency of international concern and called on all countries to fight against the epidemic (3, 4). The disease has high infectiousness, and its main clinical symptoms include fever, dry cough, fatigue, muscle pain and dyspnea (2). As of April 13, 2021, 221 countries around the world have reported 137,265,460 confirmed cases and 2,958,863 confirmed deaths from COVID-19 (5). The world pandemic has disrupted the daily work and life of the public, and the global economy has been severely damaged. It is clear that COVID-19 has become a global public health issue. In order to reduce the impact of COVID-19 outbreak, China has actively adopted medical measures and social evacuation. For example, all staff except necessary occupations should stop working before February 9, 2020 to avoid population gathering due to work (6). This measure greatly curbed the spread of the virus (7). Studies have shown that, in the environment outside the hospital, the workplace may be the best breeding ground for the virus (8). Preventive measures in the workplace can have a significant impact on the spread of a pandemic disease (9). However, studies predicted that the best time to resume work in China would be in early April. If the restrictions were lifted earlier might lead to an earlier and higher second peak (10). Therefore, in the face of the severity of the world pandemic, it is important to take relevant protective measures for those who return to work in February and March. On March 5, news.cn/worldpro/ issued a series of guidelines related to returning to work: indoor ventilation and disinfection should be done well in the workplace; employers should establish health records of employees and do not discriminate against employees confirmed or suspected of being infected with COVID-19; employees should insist on wearing masks and keeping a safe distance from colleagues, etc. (11). Specifically, farmers can carry out agricultural activities on a staggered peak and time sharing to avoid unnecessary gathering and contact. For the general staff, try not to take public transport when going out, consciously accept temperature monitoring when entering the unit, and keep the office clean and hygienic. If conditions permit, the company can allow employees to telecommute from home to avoid the risks brought by commuting, and at the same time pay close attention to their daily physical conditions. It is more important for high-risk medical workers to do a good job of self-protection. At ordinary times, it is necessary to strengthen the disinfection of the environment, prevent nosocomial infection, establish a strict ward management system, control the entry and exit of irrelevant personnel, reduce the frequency and time of family visits, wear protective clothing, goggles and gloves correctly during work (12, 13). In addition, special attention should be paid to the adjustment of negative emotions. Studies have shown that medical workers are more likely to have psychological problems (14, 15).
So far, the global epidemic prevention and control is still in a critical period, and some areas have been in a state of resumption of work. It is worth noting that during the period of resuming work and increasing production, the effect of prevention and control of pneumonia is greatly affected by the knowledge, attitudes and practices (KAP) of the people returning to work. The level of knowledge of a disease can affect people's attitudes and practices, on the other hand, negative attitudes and practices can increase the risk of death from disease (16, 17). Therefore, the purpose of this study is to assess the KAP status quo and explore the possible influencing factors of different occupational groups, so as to provide valuable information for countries and regions that have returned to work or are ready to return to work.
Materials and Methods
Study Design and Sampling
This cross-sectional study was conducted on a professional questionnaire survey platform (https://www.wenjuan.com) from March 23 to April 8, 2020. Convenience sampling method was used to select participants. According to the Kendall sample estimation method for multivariate analysis, the sample size was required to be 5–10 times the number of variables (18). In our survey, a total of 6 basic information items and 41 questionnaire dimensions were covered, therefore the minimum sample size of this survey was 235–470. Those returning to work who can understand the contents of the questionnaire and can access to the internet were eligible to participate. Finally, 348 people completed the online questionnaire, 302 of which were valid. We also performed post hoc power analysis using G-power 3.1.9.7 (Kiel University, Kiel, Germany) software to test the power of our study. The power (1-β) was determined to be 0.996, based on an error probability (significance level) of 0.05, and total sample size of 302.
Measures and Analysis
Instrument
The questionnaire was designed on the basis of guidelines for COVID-19 prevention and control issued by the WHO (19), the National Health Commission of the People's Republic China (20), the Chinese Center for Disease Control and Prevention (21). The relevant experts were invited to discuss the questionnaire to make the questions and options as accurate and comprehensive as possible. Cronbach's alpha for the questionnaire total was 0.951 which indicated that the internal consistency of the questionnaire was good. The questionnaire was a voluntary and anonymous survey. No private information and sensitive language. The questionnaire consisted of four sections: demographic variables, knowledge, attitudes and practices with respect to COVID-19.
Demographic variables (six items): age, gender, education, occupation, etc. For occupations, it involved more than a dozen industries. In order to avoid too few people in each category, we divided the occupations into four groups: (1) white-collar workers (including officials, public servants, managers, office clerks, etc.); (2) professionals (including doctors, nurses, teachers, reporters, lawyers, etc.); (3) blue-collar workers (including mill workers, waiters, salespeople, etc.); (4) self-employments (including contractors, freelancers, farmers, herdsmen, fishermen, etc.). As for the self-filled occupation questionnaires, we classified them into the above four categories according to the Code of Occupational Classification of the People's Republic of China (2015 Edition).
Knowledge of personal protection (10 items): infectious disease classification, measures to inactivate the virus, the source of infection, the main route of transmission, susceptible population, daily protection knowledge, safe communication distance, risk of infection in different workplaces, mask selection, anti-virus measures after going home. There were three options for each item, one point was given for a correct answer. The higher the score, the better the knowledge.
Attitude of personal protection (seven items): actively guard against virus, attitude toward confirmed cases around them, cooperate with the protective measures of the work unit, etc. Each item used the Likert scale to assess the degree of agreement with the statement, with options ranging from 1 (strongly disagree) to 5 (strongly agree). The total score was converted into a percentage system, the higher the score, the more positive attitude.
Practice of personal protection (24 items): pay attention to world pandemic information, wear masks, avoid crowds gathering, keep the indoor ventilation, etc. It involved the protective practice in four aspects: at home, commuting, working and dining behavior. Each item used the Likert scale to assess the degree of agreement with the statement, with options ranging from 1 (strongly disagree) to 5 (strongly agree). The total score was converted into a percentage system, with higher scores indicating better practice.
Data Analysis
We described the characteristics of participants based on four groups according to their occupations, the results were presented as frequencies and percentages. The KAP scores of different occupational groups were presented as means and interquartile rage. Mann-Whitney U test and Kruskal–Wallis H test were used to analyze the differences of KAP among different occupational groups. A multiple linear regression model was used to identify factors associated with KAP. P < 0.05 (two-tailed) was considered statistically significant. All statistics analyses were performed with SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA).
Results
Basic Characteristics of the Respondents
Table 1 presented the basic characteristics in the whole sample. A total of 348 questionnaires was collected in this survey. After excluding duplicate and invalid questionnaires, 302 were enrolled, and the effective response rate was 86.7%. Most of the respondents were female (56.1%), urban residents (97.6%), with an educational level of undergraduate or junior college (74.4%). Among those who returned to work in different occupations, white-collar workers, professionals, blue-collar workers and self-employments were 82 (27.2%), 113 (37.4%), 46 (15.2%), and 61 (20.2%), respectively.
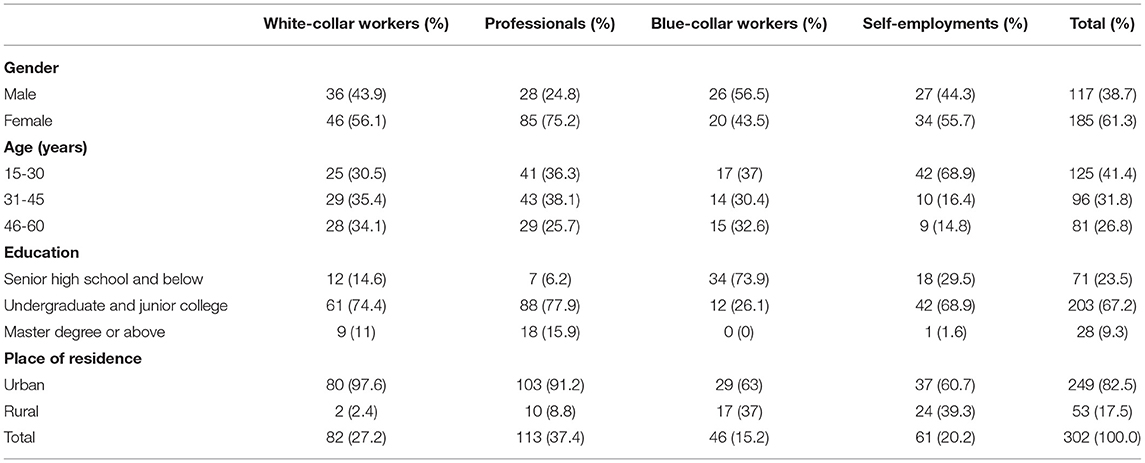
Table 1. Demographic characteristics of respondents.
COVID-19 Knowledge
Table 2 showed the options and responses for each question, of the 302 respondents, measures to inactivate the virus (96.4%), susceptible population (90.1%), and anti-virus measures after going home (94.7%) had a higher scoring rate. However, the scoring rates of infectious disease classification (45.0%), route of transmission (56.3%), and mask selection (47.0%) were lower. The highest (safe communication distance) and lowest (risk of infection in different workplaces) item scoring rates were 99.0 and 10.9%, respectively. Among those who answered correctly, the chi-square test was used to compare what aspects of knowledge were different among people returning to work in different occupations, and the results showed that there were statistical differences in infectious disease classification (χ2 = 53.658, P < 0.001), the source of infection (χ2 = 23.883, P < 0.001), the route of transmission (χ2 = 14.282, P = 0.003), the risk level of the workplace (χ2 = 8.986, P = 0.029) and the choice of masks (χ2 = 12.405, P = 0.006). More details were shown in Table 3.
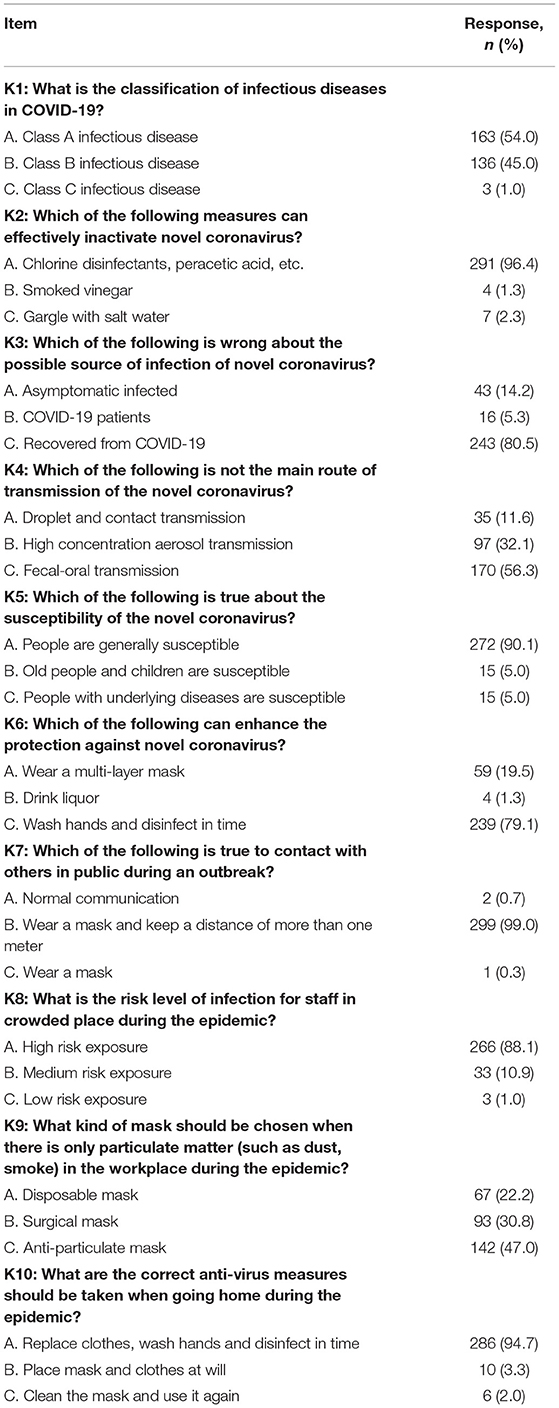
Table 2. Responses to knowledge of COVID-19 among people returning to work in different occupations.
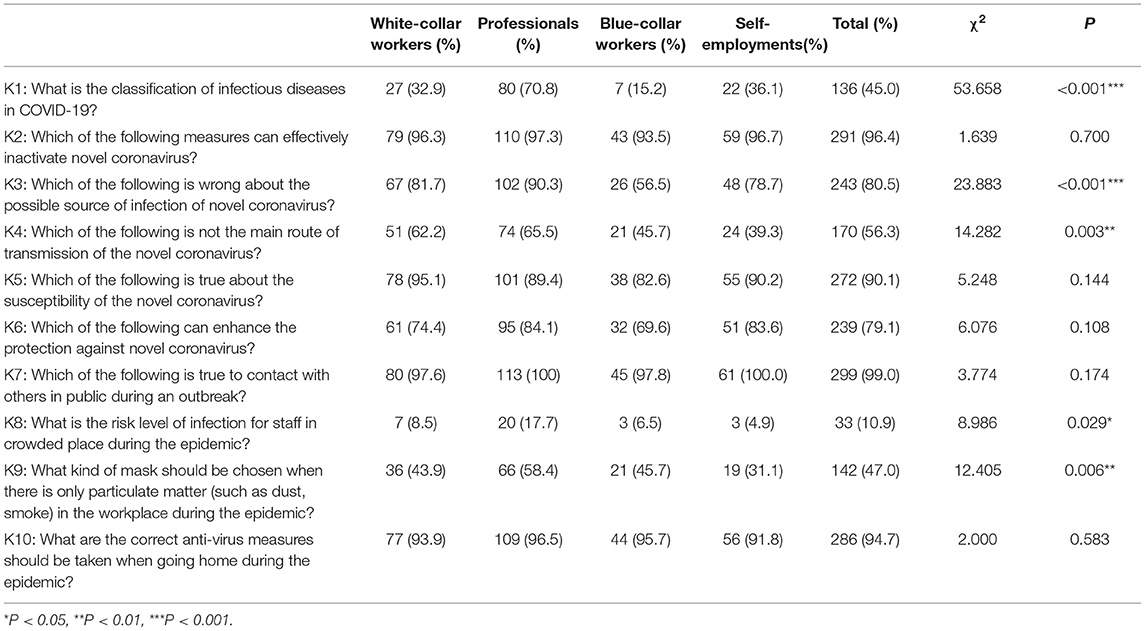
Table 3. Comparison of knowledge level of people returning to work in different occupations regarding COVID-19.
COVID-19 Attitude and Practice
The attitude scores of different occupational groups were all higher than 95, and practice scores were all higher than 90. For people of different occupations, the influencing factors of KAP were different. Education level was the influencing factor of white-collar workers practice, residence was the influencing factor of blue-collar attitude, and gender was the influencing factor of professional attitude and practice. The results of Kruskal–Wallis H test showed that there were differences in knowledge among people of different occupations, but not in attitudes and practices. More details were shown in Table 4.
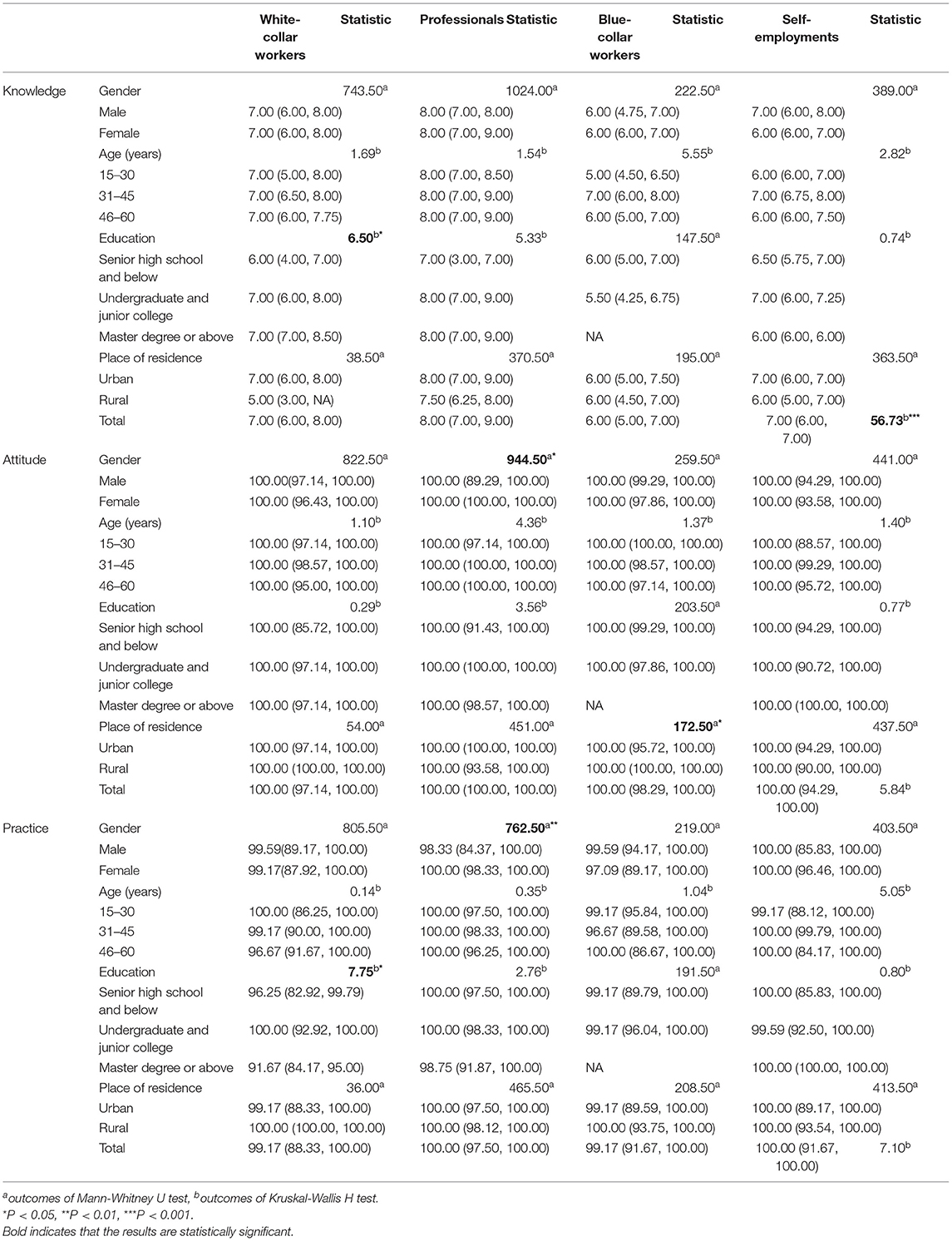
Table 4. Univariate analysis of factors associated with KAP.
Multiple Linear Regression Analysis of the Factors Influencing KAP
Knowledge score was taken as the dependent variable, gender (male = 1, female = 2), age (15–30 years old = 1, 31–45 years old = 2, 46–60 years old = 3), education (senior high school and below = 1, undergraduate and junior college = 2, master degree or above = 3), place of residence (urban = 1, rural = 2), occupation (white-collar workers = 1, professionals = 2, blue-collar workers = 3, self-employments = 4), were the five independent variables. Multiple linear regression was conducted by the forced entry method to quantify the independent contributions of the above variables to knowledge. The same two models were built using the scores of attitude and practice as dependent variables. After adjusting for demographic variables, we found that the factors influencing knowledge were the level of education and place of residence, specifically reflected in living in the urban, the higher the level of education, the higher the level of knowledge. Gender was a predictor for practice, and females might have a better personal protective practice than males. More details were shown in Table 5.
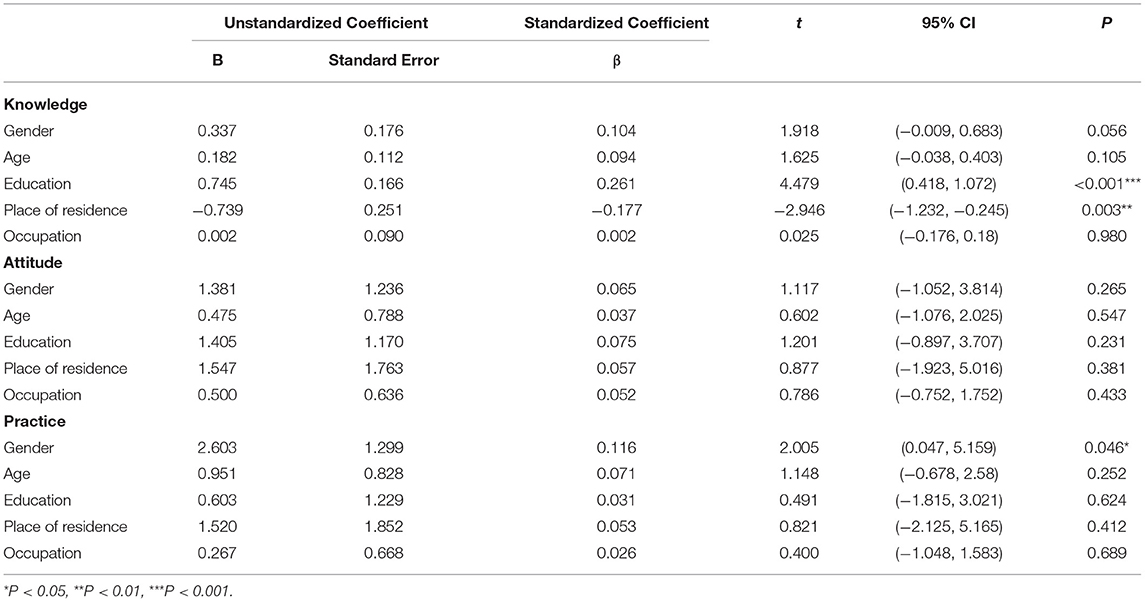
Table 5. Multiple linear regression analysis of the factors influencing KAP.
Discussion
Since the discovery of novel coronavirus, COVID-19 has had a destructive impact on the world. Health departments must formulate effective strategies to educate and manage the public. It is particularly important to timely grasp the current status and influencing factors of workers' KAP on epidemic prevention and control in the process of resuming work and production. Therefore, the purpose of this study was to compare the KAP regarding to COVID-19 among people returning to work in different occupations in China, which provides a theoretical reference for strengthening society-wide efforts to prevent and control the world pandemic. In this study, there were great differences in knowledge scoring rates in different aspects. Some professional issues such as risk of infection in different workplaces (K8:10.9%), infectious disease classification (K1: 45%) and mask selection in different places (K9: 47%) had low scores, suggesting these are the weak areas to be strengthened. This was different from the results of Zhong et al. (the overall correct rate of the knowledge questionnaire was 90%) (22). The reason might be that Zhong's survey area was mainly Wuhan city (where the first confirmed case was found in China), and most of the people surveyed were well-educated people (82.4% held an associate's degree or higher, and 56.2% engaged in mental labor). For the attitudes and practices about prevention and control of COVID-19 of the returning workers, with COVID-19 spread rapidly from a single city to the whole country, the vast of majority of respondents showed a high degree of compliance. The scores of attitude and practice were all higher than 95 and 90 respectively. According to the WHO, social distancing/self-isolation and lockdown were two crucial nationwide social measures during a public health crisis (23). After COVID-19 broke out across the country, the Chinese government took unprecedented measures to control the world pandemic, including quarantine and isolation, strict management of working and living spaces and the Examine and Approve Policy on the resumption of work. All occupations expressed high support for the measures taken by the government, health institutions and communities prevent and control the world pandemic.
Our study found that individual demographic characteristics had an impact on their KAP, which is consistent with previous studies (24–26). Educational level and place of residence were the influencing factors of respondents' knowledge, which was also in line with the law of low educational level in rural areas. The results suggested that people living in rural areas with a low level of education also had a lower level of knowledge. This may be due to residents in rural areas have limited availability to the internet and online health information resources and they are more likely to have poor knowledge about COVID-19. Less educated residents may be more likely to receive visual media rather than textual official documents. We suggest that more targeted health education should be carried out. For villages and towns to increase broadcasting and other more acceptable publicity methods, for people with low educational level to use more easy-to-understand popular science means such as simple cartoons. For people of different occupations, the knowledge score of professional personnel was generally higher than that of other types of workers, probably because they have received more training, have stronger learning ability, and easier to master COVID-19 's prevention and control knowledge. We also found that gender was a factor affecting practice. Females showed better protective practice, consistent with the results of a study in Vietnam (27), which may be related to the fact that males were more likely to engage in risk-taking behavior (28). Knowledge is the basis for establishing correct attitudes to change practice, while the attitude is the driving force of practice change. People's practice is influenced by their own knowledge and attitude (29). The KAP theoretical model is helpful for public health policy makers and health workers to identify the target population of COVID-19's prevention and health education.
During the outbreak of infectious diseases, timely understand the public's KAP of the epidemic and the needs of health education, and carry out effective risk communication with the public, so as to take health education measures and strategies for different groups of people. So as to control the spread of virus in the population in a timely manner. This can effectively reduce the negative psychological reaction caused by the outbreak of the world pandemic, eliminate public panic, prevent the spread of virus, which is conducive to the prevention and control of the epidemic (30). This study conducted a rapid evaluation of public KAP in the rising phase of COVID-19, which can provide a basis for the government to formulate targeted health education and behavior intervention strategies.
This study also has some limitations. Although we have designed the questionnaire according to the official guidance manual and the latest literature, the depth of the survey may be limited. Second, this study is a web-based survey, which will result in the loss of some respondents (those who do not know how to use the internet or cannot use the internet or smart phones due to restrictions), and overestimate the KAP level of those who return to work to a certain extent. Third, there may be a recall bias because the data are collected through participants' self-reports.
Conclusion
This study preliminarily explored the KAP and influencing factors of people returning to work in different occupations on the prevention and control of COVID-19. Overall, these workers in our survey showed positive attitude and appropriate practice toward COVID-19 during the world pandemic, which are significant factors to limit the spread of the virus. The results of this survey can provide a reference for the subsequent improvement of COVID-19's prevention publicity and health education. Due to the sample limitation, more extensive studies are needed in the future to support our conclusions.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
The manuscript writing for the original draft and data analysis were completed by ZYF. YLM collaborated in data extraction and gave the paper revision and format adjustment work. FZ and YZ gave the entire process technical and paper writing guidance support. All authors read and approved the final manuscript.
Funding
This research was funded by Chongqing Medical University School of Public Health and Management, Research Center for Medicine and Social Development, COVID-19 Prevention, and Control Emergency Research (Management) Project.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in wuhan, china, of novel coronavirus-infected pneumonia. New Engl J Med. (2020) 382:1199–207. doi: 10.1056/NEJMoa2001316
2. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
3. World Health Organization (WHO). WHO Director-General's statement on IHR Emergency Committee on Novel Coronavirus (2019-nCoV). (2021). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus-2019-ncov (accessed March 12, 2021).
4. Dousari AS, Moghadam MT, Satarzadeh N. COVID-19 (Coronavirus Disease 2019): a new coronavirus disease. Infect Drug Resist. (2020) 13:2819–28. doi: 10.2147/IDR.S259279
5. Worldmeter. COVID-19 Update (Live). (2020). Available online at: https://www.worldometers.info/coronavirus/ (accessed March 12, 2021).
6. Fong MW, Gao H, Wong JY, Xiao J, Shiu EYC, Ryu S, et al. Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings-social distancing measures. Emerg Infect Dis. (2020) 26:976–84. doi: 10.3201/eid2605.190995
7. Ahmed F, Zviedrite N, Uzicanin A. Effectiveness of workplace social distancing measures in reducing influenza transmission: a systematic review. BMC Public Health. (2018) 18:518. doi: 10.1186/s12889-018-5446-1
8. Tan W, Hao F, McIntyre RS, Jiang L, Jiang X, Zhang L, et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav Immun. (2020) 87:84–92. doi: 10.1016/j.bbi.2020.04.055
9. Ferguson NM, Cummings DAT, Fraser C, Cajka JC, Cooley PC, Burke DS. Strategies for mitigating an influenza pandemic. Nature. (2006) 442:448–52. doi: 10.1038/nature04795
10. Prem K, Liu Y, Russell TW, Kucharski AJ, Eggo RM, Davies N. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. (2020) 5:e261–70. doi: 10.1016/S2468-2667(20)30073-6
11. Xinhua. State Council's tips on workplace COVID-19 prevention, control. (2020). Available online at: http://www.china.org.cn/china/2020-03/05/content_75776272.htm (accessed March 12, 2021).
12. The State Council. Notice on prevention and control measures of resuming work and production. (2020). Available online at: http://www.gov.cn/zhengce/content/2020-02/22/content_5482025.htm (accessed April 10, 2021).
13. Qu J, Lv X. The Response Measures to the Coronavirus Disease 2019 Outbreak in China. Open Forum Infect Dis. (2021) 8:ofab14. doi: 10.1093/ofid/ofab014
14. Liang Y, Wu K, Zhou Y, Huang X, Zhou Y, Liu Z. Mental health in frontline medical workers during the 2019 novel coronavirus disease epidemic in china: a comparison with the general population. Int J Environ Res Public Health. (2020) 17:6550. doi: 10.3390/ijerph17186550
15. Moghadam MT, Taati B, Ardakani SMP, Suzuki K. Ramadan fasting during the COVID-19 pandemic; observance of health, nutrition and exercise criteria for improving the immune system. Front Nutr. (2021) 7:570235. doi: 10.3389/fnut.2020.570235
16. Saadatjoo S, Miri M, Hassanipour S, Ameri H, Arab-Zozani M. Knowledge, attitudes, and practices of the general population about Coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis with policy recommendations [published online ahead of print]. Public Health. (2021). doi: 10.1016/j.puhe.2021.03.005
17. Moghadam MT, Babakhani S, Rajabi S, Baravati FB, Raeisi M, Dousari AS. Does stress and anxiety contribute to COVID-19? Iran J Psychiatry Behav Sci. (2020) 15:e106041. doi: 10.5812/ijpbs.106041
18. Chen B. Sample size methodology for multivariate analysis—synthetic estimate method for sample size in multivariate analysis. Injury Med (Electronic Edition). (2012) 1:58–60. doi: 10.3868/j.issn.2095-1566.2012.04.012
19. World Health Organization (WHO). Q&As on COVID-19 and related health topics. Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub (accessed March 12, 2021).
20. National Health Commission of the People's Republic China (NHC). Knowledge on prevention and control of COVID-19. (2020). Available online at: http://www.nhc.gov.cn/xcs/kpzs/list_gzbd.shtml (accessed March 12, 2021).
21. Chinese Center for Disease Control and Prevention (CDC). Knowledge world. (2020). Available online at: http://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/jszl_2275/ (accessed March 12, 2021).
22. Zhong B, Luo W, Li H, Zhang Q, Liu X, Li W, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. (2020) 16:1745–52. doi: 10.7150/ijbs.45221
23. World Health Organization (WHO). WHO Director-General's opening remarks at the media briefing on COVID-19—March 11, 2020. (2020). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020 (accessed March 12, 2021).
24. Gao H, Hu R, Yin L, Yuan X, Tang H, Luo L, et al. Knowledge, attitudes and practices of the Chinese public with respect to coronavirus disease (COVID-19): an online cross-sectional survey. BMC Public Health. (2020) 20:1816. doi: 10.1186/s12889-020-09961-2
25. Chen Y, Zhou R, Chen B, Chen H, Li Y, Chen Z, et al. Knowledge, perceived beliefs, and preventive behaviors related to COVID-19 among chinese older adults: cross-sectional web-based survey. J Med Internet Res. (2020) 22:e23729. doi: 10.2196/23729
26. Lau LL, Hung N, Go DJ, Ferma J, Choi M, Dodd W, et al. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: a cross-sectional study. J Glob Health. (2020) 10:11007. doi: 10.7189/jogh.10.011007
27. Van Nhu H, Tuyet-Hanh TT, Van NTA, Linh TNQ, Tien TQ. Knowledge, attitudes, and practices of the vietnamese as key factors in controlling COVID-19. J Community Health. (2020) 45:1263–69. doi: 10.1007/s10900-020-00919-4
28. Yang K, Liu H, Li H, Wang S, Tian Y, Zhang F, et al. Knowledge, attitude and practice of residents in the prevention and control of COVID-19: an online questionnaire survey. J Adv Nurs. (2020) 77:1839–55. doi: 10.1111/jan.14718
Keywords: COVID-19, knowledge, attitudes, practices, personal protection
Citation: Fan ZY, Mou YL, Cheng R, Zhao Y and Zhang F (2021) Investigation of Knowledge, Attitude and Practice of Personal Protection Among Different Types of Workers Returning to Work Under COVID-19 Epidemic. Front. Public Health 9:679699. doi: 10.3389/fpubh.2021.679699
Received: 12 March 2021; Accepted: 19 April 2021;
Published: 17 May 2021.
Edited by:
Atefeh Abedini, Shahid Beheshti University of Medical Sciences, IranReviewed by:
Majid Taati Moghadam, Iran University of Medical Sciences, IranHosein Ameri, Shahid Sadoughi University of Medical Sciences and Health Services, Iran
Waquar Ahsan, Jazan University, Saudi Arabia
Copyright © 2021 Fan, Mou, Cheng, Zhao and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fan Zhang, ZXBpY3FtdUAxNjMuY29t; Yong Zhao, emhhb3lvbmdAY3FtdS5lZHUuY24=