 Yang Zhao
Yang Zhao Shenglan Tang
Shenglan Tang Wenhui Mao1
Wenhui Mao1 Tomi Akinyemiju
Tomi Akinyemiju- 1Duke Global Health Institute, Duke University, Durham, NC, United States
- 2Global Health Research Center, Duke Kunshan University, Kunshan, China
- 3The George Institute for Global Health at Peking University Health Science Center, Beijing, China
- 4Department of Population Health Sciences, Duke University School of Medicine, Durham, NC, United States
- 5Duke Cancer Institute, Duke University, Durham, NC, United States
Objective: In China, cancer accounts for one-fifth of all deaths, and exerts a heavy toll on patients, families, healthcare systems, and society as a whole. This study aims to examine the temporal trends in socio-economic and rural-urban differences in treatment, healthcare service utilization and catastrophic health expenditure (CHE) among adult cancer patients in China. We also investigate the relationship between different types of treatment and healthcare service utilization, as well as the incidence of CHE.
Materials and Methods: We analyzed data from the 2011 and 2015 China Health and Retirement Longitudinal Study, a nationally representative survey including 17,224 participants (234 individuals with cancer) in 2011 and 19,569 participants (368 individuals with cancer) in 2015. The study includes six different types of cancer treatments: Chinese traditional medication (TCM); western modern medication (excluding TCM and chemotherapy medications); a combination of TCM & western medication; surgery; chemotherapy; and radiation therapy. Multivariable regression models were performed to investigate the association between cancer treatments and healthcare service utilization and CHE.
Results: The age-adjusted prevalence of cancer increased from 1.37% to 1.84% between 2011 and 2015. More urban patients (54%) received cancer treatment than rural patients (46%) in 2015. Patients with high socio-economic status (SES) received a higher proportion of surgical and chemotherapy treatments compared to patients with low SES in 2015. Incidence of CHE declined by 22% in urban areas but increased by 31% in rural areas. We found a positive relationship between cancer treatment and outpatient visits (OR = 2.098, 95% CI = 1.453, 3.029), hospital admission (OR = 1.961, 95% CI = 1.346, 2.857) and CHE (OR = 1.796, 95% CI = 1.231, 2.620). Chemotherapy and surgery were each associated with a 2-fold increased risk of CHE.
Conclusions: Significant improvements in health insurance benefit packages are necessary to ensure universal, affordable and patient-centered health coverage for cancer patients in China.
Introduction
Non-communicable diseases are the leading cause of death and disability worldwide, and cancer is one of the most common. In China, there were an estimated 4 million new cancer cases, and 3 million cancer deaths in 2018, which accounted for a high percentage of total cancer cases (about 23%) and deaths (30%) worldwide (1). In China, cancer accounts for one-fifth of all deaths, and exerts a heavy toll on patients, families and the whole healthcare system.
To mitigate the healthcare and financial burden of non-communicable diseases including cancers, the Chinese central government launched a new round of comprehensive healthcare system reforms in 2009, focusing on healthcare delivery, essential medicines and financial protection. Most of the reform measures were designed to improve access to good quality and affordable care for patients with non-communicable diseases (2, 3). In 2015, the Urban Residents Basic Medical Insurance and New Rural Cooperative Medical System were integrated into one urban–rural resident health insurance scheme, which improved financial risk protection for cancer patients (4, 5). Additionally, the Critical Illness Health Insurance, supplementary medical insurance program, and the consolidation of medical institutions were designed to provide better benefits packages to citizens with severe chronic diseases (6).
We hypothesize that reforms in health insurance and healthcare delivery systems could further reduce catastrophic health expenditures (CHE) among cancer patients in both rural and urban regions of China. In this study, CHE is defined as the point at which annual household healthcare expenses exceed 40% of non-food household expenditure. Although a new round of health reforms have been implemented at the national level, it may take time for their impact to materialize across populations with different SES (7).
Previous research (including research in China) has shown that higher SES is associated with a greater likelihood of routine cancer screening, incidence of cancer, treatment utilization as well as better outcomes in cancer patients (8–13). Other studies in China have found a higher incidence of common cancers in men than women in most age groups (14, 15). Previous research has explored the socio-economic differences among patients with non-communicable diseases, such as hypertension, diabetes, stroke, chronic obstructive pulmonary disease, and patients with multiple chronic diseases (16–21). However, there is limited research on the financial burden caused by cancer on different socio-economic groups in China (22). Furthermore, few studies have evaluated whether CHE varies by treatment type (e.g., Chinese traditional or western medicine), or estimated the impact of the 2009 health reforms on health service utilization among cancer patients (23–26).
Our research aims include: (1) investigating temporal changes in the financial burden of treatment and CHE among Chinese adults with cancer between 2011 and 2015; (2) assessing differences in cancer treatment, health service utilization and CHE between patients of different SES and rural-urban residences; and (3) examining relationships between different types of cancer treatments and healthcare service utilization and CHE.
Materials and Methods
Data Source
Data were obtained from the China Health and Retirement Longitudinal Study (CHARLS) in 2011 and 2015. The CHARLS is a biennial survey, aimed to be representative of Chinese adults aged 45 years and above. The CHARLS study design is similar to the Health and Retirement Study (HRS) and other established aging-related surveys (27). Study questionnaires collect information on demographics, functional health status, healthcare and insurance, household income and expenditure, and clinical risk factors (such as blood pressure). Further details of the study methodology are published elsewhere (27).
To ensure ample representativeness at the national level, CHARLS sampled 150 counties and 450 villages/urban communities across 28 provinces, using multi-stage stratified probability-proportionate-to-size sampling. A total of 17,708 individuals were interviewed in 2011 (baseline) and 21,097 in 2015 (3rd wave). Final data were available for 17,224 participants in 2011 and 19,569 participants in 2015, after excluding participants with missing values. A total of 234 individuals (in 2011) and 368 (in 2015) self-reported having clinically-diagnosed cancer.
Cancer Care Indicators
We identified six types of cancer treatments: Chinese traditional medication (TCM); western modern medication (taking western medication excluding TCM and chemotherapy medications for cancer treatment); a combination of TCM & western medication; surgery; chemotherapy; and radiation therapy. Overall, treatment was defined as the receipt of any TCM or western medical treatment (having one or more of the six therapies). In terms of health service utilization, this study included:(1) outpatient care (participants were asked whether they had received any outpatient care during the last month); (2) inpatient care (participants were asked whether they were hospitalized and for how many nights during the last year). Information on medical expenditures was also collected, including: total health expenditure; reimbursement; and out-of-pocket spending on outpatient services in the past month and for inpatient services in the past year.
We used CHE to measure the financial risk or economic burden on households with a family member diagnosed with cancer. There were two common criteria to meet the definition of CHE: (1) out-of-pocket expenditure (OOPE) over 40% of the household's income after paying essential living expenses (using household expenditure on non-food consumption as proxy); and (2) over 10% of total household income/expenditure (28–30). The OOPE health expenditure and household expenditure on non-food consumption were considered as the numerator and denominator, respectively.
SES was assessed using the Socio-economic Index score, and calculated based on educational attainment, occupation, and household consumption expenditure. Li's scale for Chinese residents (version 2010) (31) was used as a standard scale. This scale, commonly used in social science research in China (32–35), was modified based on a scale first proposed by Duncan (36). Education level, occupation, and household consumption expenditure were classified to assign scores, and then summarized as a comprehensive Socio-economic Index score. Based on the Socio-economic Index scores, all subjects were classified as being of either low (<10 score) or high SES (≥10 score).
Statistical Analysis
This study applied Chi-square tests to examine the SES differences in types of cancer treatment, outpatient and inpatient service utilization, as well as incidence of CHE. For continuous variables including nights of hospitalization and OOPE, we used non-parametric tests to analyze SES group differences. Based on the pooled two-wave data of cancer patients, we performed multivariable logistic regressions to investigate the association between cancer treatment with outpatient visits, hospitalization, and incidence of CHE, adjusting for socio-demographic factors. Covariates in the regression analyses included gender, age, marital status, location of residence, region in China, and enrollment in social health insurance.
To explore differential relationships across the SES groups, we conducted subgroup analyses with logistic regression models stratified by the SES Index. The adjusted odds ratio (OR) and 95% confidence intervals (CI) were reported for the logistic regression analyses in this study. The weighted prevalence of cancers was also reported considering nonresponse data and the complex, multistage design of the CHARLS study. P-values less than 0.1 were considered as statistically significant. Statistical analyses were conducted using STATA software (version 15.0; StataCorp LLC College Station, Texas, United States).
Results
Table 1 presents the socio-demographic characteristics of participants and cancer patients among individuals aged 45 years and older in 2011 and 2015. The prevalence of cancer increased from 1.36% (234 of 17,224) in 2011 to 1.88% (368 of 19,569) in 2015. The age-adjusted prevalence of cancer was 1.37% in 2011 and 1.84% in 2015. The prevalence of cancer was higher in individuals who were female, had social health insurance, were located in the eastern region, and unemployed; compared with participants who were male, did not have health insurance, lived in the western region, and were employed.

Table 1. The prevalence of cancer among Chinese adults in 2011 and 2015.
Overall, approximately half of the cancer patients utilized treatment, with a higher proportion of urban residents (54%) than rural residents (46%) receiving treatment in 2015. In addition, a higher proportion of high vs. low SES patients utilized treatment. Western medication and surgery were the two main types of treatment. People with a high SES level received more western medication treatment, surgery, and chemotherapy than low SES patients (Table 2).
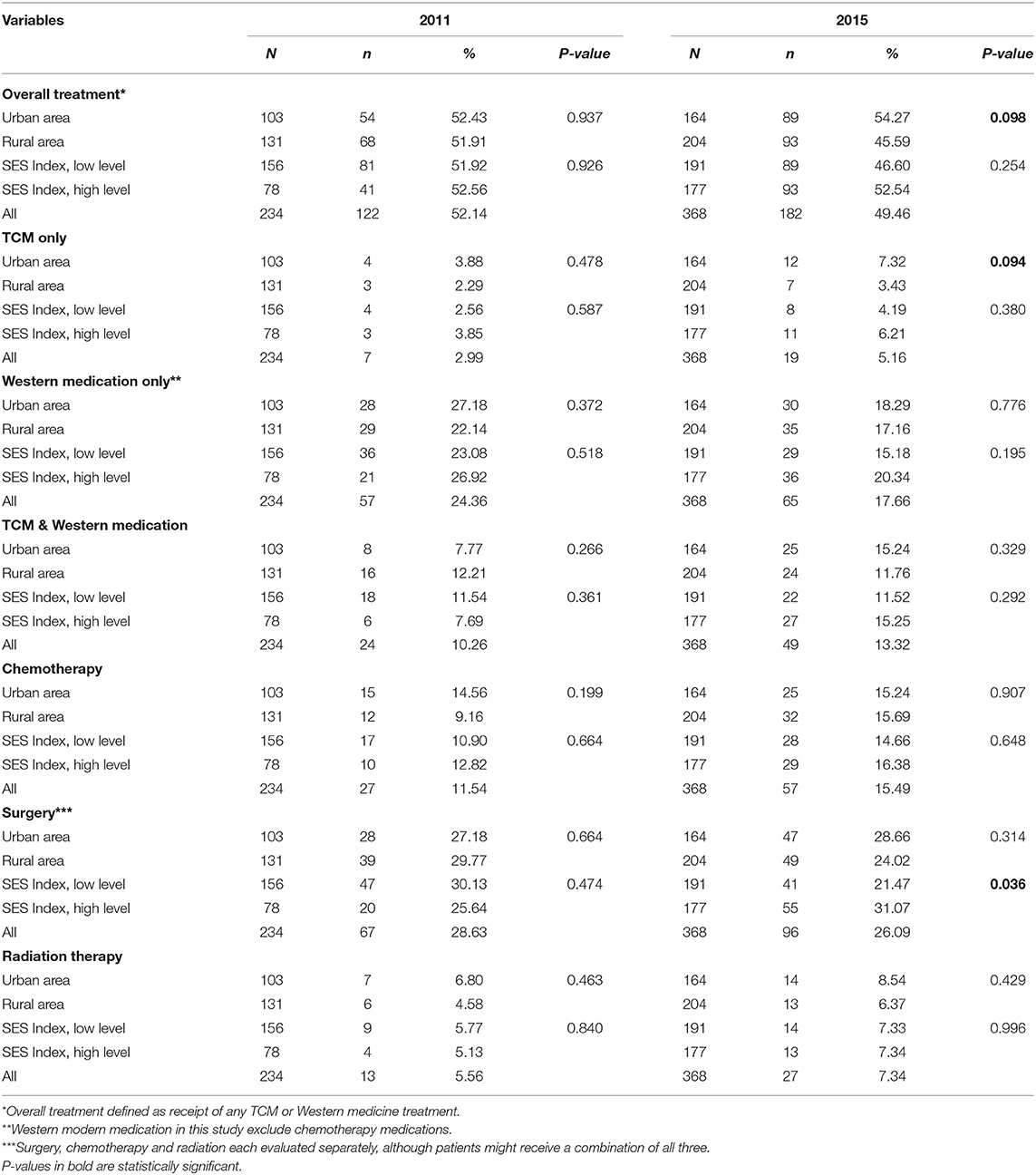
Table 2. The proportion of cancer treatment in China, by the socioeconomic group.
There was increasing health service utilization among cancer patients in China from 2011 to 2015 (outpatient visit, 26 to 30%; admission rate, 23 to 30%; average nights of hospitalization, 3.41 to 3.81). In 2011, residents living in rural areas had a higher proportion of outpatient visits but less OOPE for outpatient care than urban residents. However, by 2015, this gap had narrowed and the OOPE for outpatient care had more than tripled in rural areas, and declined significantly in urban areas. Between 2011 and 2015, CHE declined by 22% in urban areas (25% in 2011 and 19% in 2015) but increased by 31% in rural areas (25% in 2011 to 33% in 2015). In 2011, low SES cancer patients had significantly lower OOPE for inpatient care compared with high SES patients. However, by 2015 this gap had narrowed and was no longer significant (Table 3).
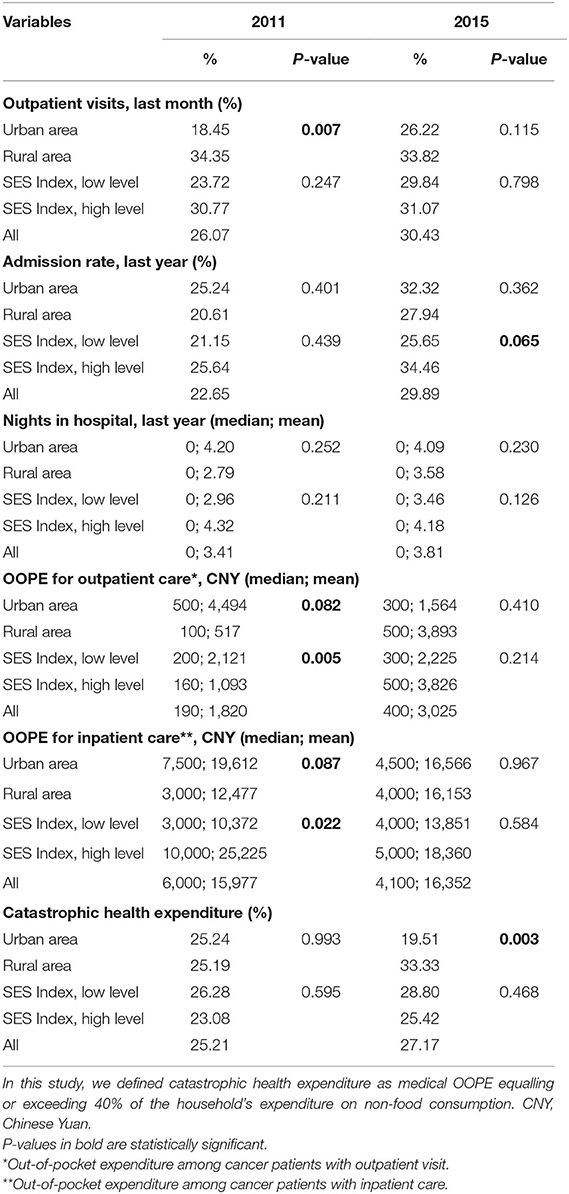
Table 3. Health service utilization and health spending among cancer patients in China, by the socioeconomic group.
The multivariable regression analyses suggest positive relationships between cancer treatment and outpatient visits (OR = 2.098, 95% CI =1.453, 3.029), admission to hospital (OR = 1.961, 95% CI = 1.346, 2.857) and CHE (OR = 1.796, 95% CI =1.231, 2.620). Chemotherapy (OR = 2.53, 95% CI: 1.55, 4.12) and surgery (surgery: OR = 2.15, 95% CI: 1.44, 3.20) were each associated with a 2-fold increased risk of CHE, after controlling for all socio-demographic covariates. This association was stronger among high SES groups (chemotherapy OR = 3.16, 95% CI: 1.44, 6.90; surgery: OR = 2.36, 95% CI: 1.24, 4.49) compared with low SES groups (chemotherapy OR = 2.77, 95% CI: 1.41, 5.41; surgery OR = 2.07, 95% CI: 1.22, 3.51). There were no significant associations observed for TCM with CHE overall or by SES (Table 4).
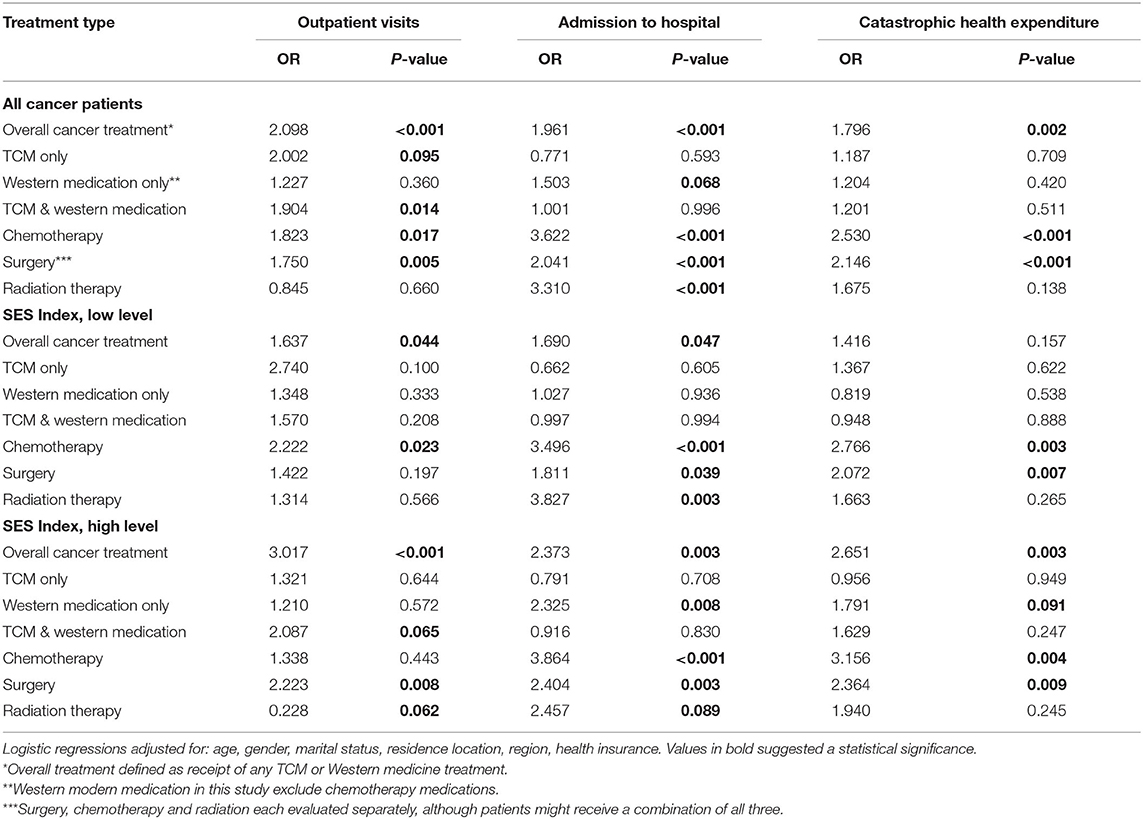
Table 4. Differential impacts of the cancer treatment on health service use and catastrophic health expenditure.
Discussion
As this nationally representative study indicated, there were increasing trends in the prevalence of cancer, and healthcare service utilization among adults with cancer from 2011 to 2015. The results suggest socio-economic and rural-urban differences impact cancer treatment in China. For example, about half of cancer patients in urban areas utilized cancer treatment in 2015, a higher proportion than rural residents. Patients with high SES received a higher proportion of surgery and chemotherapy treatment compared to those with low SES in 2015. Moreover, there was a substantial increase in CHE among rural patients between 2011 and 2015, but a substantial decrease among urban patients in during the same time period. Regression analyses revealed that the cost of chemotherapy and surgery appeared to drive the CHE increase, regardless of SES.
There are likely several factors contributing to the observed urban-rural differences in cancer treatment that need to be addressed in order to improve equitable access to healthcare. First, cancer treatment is a specialized service, and generally only secondary or higher levels hospitals have the capacity to provide it. Therefore, rural residents have less geographic access to treatment compared with urban areas. Additionally, some rural patients require extended travel and incur additional expenses to receive treatment in urban areas (37).
Second, previous studies have documented the disparities in access to healthcare between urban and rural areas in China (38, 39). Rural areas are less likely to have access to the same quality of healthcare services as urban areas due to differences in economic development (38, 40). Rural areas are more likely to have a shortage of healthcare service providers and lack of social support services (41–43). Previous research found that the number of licensed doctors and nurses, medical-technical personnel, and beds per 1,000 population increased more in Chinese urban areas than in rural areas from 2005 to 2017 (44). There were 2.57 more registered doctors per thousand people in urban areas than in rural areas in China in 2015 (45). As a result cancer patients in rural areas may prefer to use services in nearby urban areas despite the higher financial burden.
Third, patients in rural areas potentially face more financial barriers in accessing cancer treatment compared with patients in urban areas. This is likely due to the fact that rural areas have more barriers in physical access to healthcare services, and high per-capita payment for cancer treatment. Social medical insurance also likely contributes to the urban-rural disparity in CHE due to gaps in coverage and benefit packages (46). While over 95% of the Chinese population are covered by basic medical insurance, the benefits packages vary significantly (5, 6, 13). For example, in 2015 the per-capita fund for Urban Employee Basic Medical Insurance was US$424.7, whereas it was only $61.2 for New Rural Cooperative Medical System (15). The co-payment rate for the New Rural Cooperative Medical System (73.4%) was higher than the Urban Employee Basic Medical Insurance (36.8%) and Urban Residents Basic Medical Insurance (50.7%) in 2008 (47). Cancer patients in rural regions receive lower reimbursement rates and have lower annual maximum payments from insurance. Additionally, patients that seek treatment outside of their residential location usually receive lower reimbursement rates. For example, if cancer patients from rural areas utilize cancer treatment from another city, they have to pay a higher proportion of their bill out-of-pocket. Such a heavy financial burden likely prohibits low SES and rural patients seeking cancer treatment, possibly explaining the large urban-rural disparity in inpatient care compared to outpatient visits. More attention should be given to the financial implications caused by out of pocket expenses for cancer treatment across the different health insurance schemes in future.
Finally, while the expenditure for cancer treatment is increasing in both rural and urban areas, unequal economic development and the low amount of disposable income available to rural residents may further contribute to the urban-rural disparities. In 2015, the disposable income of urban citizens was 31,195 CNY per capita, three times higher than that of residents living in rural areas (11,422 CNY) (48). Medical expenditure due to cancer treatment, specifically surgery and chemotherapy, is likely to have significantly greater impact on rural patients, leading to increased risk of CHE and impoverishment (48). In addition, since the New Rural Cooperative Medical System and the Urban Residents Basic Medical Insurance were mainly financed by local county-level governments at the early stage of China's health system reform, the quality of benefit packages likely depends on the strength of the local economy (45).
We observed that cancer patients with high SES were less likely to experience CHE than those with low SES, and by 2015, rural cancer patients had almost double the prevalence of CHE compared with urban cancer patients, suggesting that a potential unintended consequence of the health reform is the widening of rural-urban disparities in CHE. The findings are consistent with previous research on financial burden among residents with non-communicable diseases in China (15, 49). Recent studies have documented a rapid rise in healthcare costs for cancer patients in China. However, data on the population-level economic burden of cancer is limited and the reported expenditure per patient may be underestimated (50–56). For example, a systematic review of the economic burden of liver cancer shows an increase in expenditure indicators (direct medical expenditure, annual expenditure per visit and annual expenditure per diem) from 1996 to 2015, with medication costs accounting for more than half of overall expenditure (56. 6%) (53). For colorectal cancer, the annual growth rate for medical expenditure per patient, per visit and per day increased from 6.9 to 7.8% from 1996 to 2015, respectively (54).
Policy Implications
The health insurance programs in China have had some positive impact on healthcare utilization. For instance, we observed that outpatient visits and admissions increased between 2011 and 2015 in all socio-demographic groups. However, challenges remain. Overall, the burden of cancer among adults in China is increasing, and about one-fourth of cancer patients experienced CHE. Yet disparities among urban-rural areas, and across different SES still exist, even after the implementation of the national health insurance scheme.
To reduce financial burden of cancer and bridge the SES gap, comprehensive changes to health insurance benefit packages and healthcare resource allocation are needed to ensure universal, affordable and patient-centered health coverage. First, the Urban Residents Basic Medical Insurance and the New Rural Cooperative Medical System need to be further integrated to provide similar contributions, benefit packages, as well as financial risk protection to accelerate the equitable access to health services in both urban and rural areas. Secondly, social health insurance benefit packages need to be expanded. Health services that have proven cost-effective (including medicines) should be added to the National Insurance Reimbursable List. For instance, 17 and 22 anti-cancer medications were added to the National Insurance Reimbursable List in 2018 and 2019 respectively. This allowed for a significant price cut and helped to reduce the financial burden on cancer patients. (57). Thirdly, while the National Health Insurance provides financial protection for essential care, the Critical Illness Medical Insurance should play an increasing role in providing financial support for catastrophic expenses, including cancer treatment. In particular, the current Critical Illness Medical Insurance in most regions followed the National Insurance Reimbursable List which prioritizes essential care (58). To provide better protection against catastrophic expenses, Critical Illness Medical Insurance should explore additional coverage on other treatments with proven health benefits. Furthermore, enhancing the capacity of the National Public Health Initiative would increase cancer prevention strategies such as routine screening and case management. This might lead to early detection, reduced financial burden and improved cancer outcomes. This approach is especially critical given the healthcare disruptions caused by the COVID-19 pandemic.
Strengths and Limitations
This research utilized data from a nationally representative study to investigate the trends and disparities in cancer treatment, healthcare service utilization and CHE from 2011 to 2015. Our study contributes to a deeper understanding of the socio-economic and rural-urban disparities in cancer treatment, health service utilization and expenditure. There are several significant limitations. This study used self-reported data on cancer diagnosis, treatment type and healthcare service utilization. Self-reported information could result in underestimated figures as a result of recall bias (53). Medical information regarding cancer severity was not collected. Using the indicator of CHE to measure the financial burden might ignore a part of patients not seeking health care because of economic restraints who could be even more vulnerable, while the CHARLS data showed that only a very small proportion of patients with cancer in China did not seek medical treatment due to economic restraints. The CHARLS survey only included middle-aged and elderly members of the population. Future research should also focus on younger adults. Moreover, about 20% of participants in the CHARLS survey had missing values for some key variables.
In conclusion, the burden of cancer among Chinese adults is increasing. Socio-economic and urban-rural disparities in cancer treatment and health service utilization were largely determined by patient financial capability. The current social health insurance schemes are insufficient to address these disparities. A comprehensive health insurance policy with expanded benefit packages and a stronger Public Medical Assistance System, are essential to providing adequate and equitable cancer treatment in China.
Data Availability Statement
The datasets generated and analyzed during the current study are available in the China Health and Retirement Longitudinal Study repository; http://charls.pku.edu.cn/pages/data/111/en.html.
Ethics Statement
The studies involving human participants were reviewed and approved by the Biomedical Ethics Review Committee of Peking University approved the CHARLS study, and all interviewees were required to provide informed consent. The ethical approval number was IRB00001052–11015. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YZ and ST conceived and designed the study. YZ carried out the initial analysis. YZ, ST, and TA interpreted the data. WM and YZ analyzed the literature. YZ and WM wrote the first draft of the paper. TA, ST, and WM provided guidance on the first draft and provided feedback on intellectual content. All authors reviewed and had final approval of the submitted and published versions.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We gratefully acknowledge the China Health and Retirement Longitudinal Study team for providing data and training in use of the datasets. We are grateful to the students who participated in the survey for their cooperation. The authors thank all volunteers and staff involved in this research.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.779285/full#supplementary-material
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
2. Fang H, Eggleston K, Hanson K, Wu M. Enhancing financial protection under China's social health insurance to achieve universal health coverage. BMJ. (2019) 365:l2378. doi: 10.1136/bmj.l2378
3. Liu H, Gao S, Rizzo J. The expansion of public health insurance and the demand for private health insurance in rural China. China Econ Rev. (2011) 22:28–41. doi: 10.1016/j.chieco.2010.08.006
4. Mao W, Tang S, Zhu Y, Xie Z, Chen W. Financial burden of healthcare for cancer patients with social medical insurance: a multi-centered study in urban China. Int J Equity Health. (2017) 16:180. doi: 10.1186/s12939-017-0675-y
5. Meng Q, Xu L, Zhang Y, Qian J, Cai M, Xin Y, et al. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. Lancet. (2012) 379:805–14. doi: 10.1016/S0140-6736(12)60278-5
6. Meng Q, Fang H, Liu X, Yuan B, Xu J. Consolidating the social health insurance schemes in China: towards an equitable and efficient health system. Lancet. (2015) 386:1484–92. doi: 10.1016/S0140-6736(15)00342-6
7. Chatfield M. Primary health care: the Chinese experience. Health Care Manag Rev. (1984) 9:82. doi: 10.1097/00004010-198400920-00013
8. Kumachev A, Trudeau ME, Chan KKW. Associations among socioeconomic status, patterns of care, and outcomes in breast cancer patients in a universal health care system: Ontario's experience. Cancer. (2016) 122:893–8. doi: 10.1002/cncr.29838
9. Aileen T, Rachael GH, Linda S. “It's at a Time in Your Life When You Are Most Vulnerable”: A Qualitative Exploration of the Financial Impact of a Cancer Diagnosis and Implications for Financial Protection in Health. PLoS ONE. (2013) 8:e77549. doi: 10.1371/journal.pone.0077549
10. Derouen MC, Parsons HM, Kent EE, Pollock BH, Keegan THM. Sociodemographic disparities in survival for adolescents and young adults with cancer differ by health insurance status. Cancer Causes Control. (2017) 28:841–51. doi: 10.1007/s10552-017-0914-y
11. Penson DF, Stoddard ML, Pasta DJ, Lubeck DP, Flanders SC, Litwin MS. The association between socioeconomic status, health insurance coverage, and quality of life in men with prostate cancer. J Clin Epidemiol. (2001) 54:350–8. doi: 10.1016/S0895-4356(00)00312-7
12. Fei X, Wu J, Kong Z, Christakos G. Urban-rural disparity of breast cancer and socioeconomic risk factors in China. PLoS ONE. (2015) 10:e0117572. doi: 10.1371/journal.pone.0117572
13. Yang L, Zhang X, Yang X, Yang J, Wang Z, Chen H, et al. Lung cancer treatment disparities in China: A question in need of an answer. Oncologist. (2014) 19:1084–90. doi: 10.1634/theoncologist.2014-0007
14. Xia C, Ding C, Zheng R, Zhang S, Zeng H, Wang J, et al. Trends in geographical disparities for cervical cancer mortality in China from 1973 to 2013: a subnational spatio-temporal study. Chin J Cancer Res. (2017) 29:487–95. doi: 10.21147/j.issn.1000-9604.2017.06.03
15. Jiang X, Cai S, Hu Y, Ye D, Li Q, Chen K, et al. Sex disparities in cancer incidence in Jiashan County, China, 1995–2014. Cancer Epidemiol. (2017) 50:46–52. doi: 10.1016/j.canep.2017.07.013
16. Zhao Y, Oldenburg B, Mahal A, Haregu T, Katar A, Zhang L. Trends and inequalities in the health care and hypertension outcomes in China, 2011 to 2015. Int J Environ Res Public Health. (2019) 16:4578. doi: 10.3390/ijerph16224578
17. Liu X, Sun X, Zhao Y, Meng Q. Financial protection of rural health insurance for patients with hypertension and diabetes: repeated cross-sectional surveys in rural China. BMC Health Serv Res. (2016) 16:481. doi: 10.1186/s12913-016-1735-5
18. Zhao Y, Oldenburg B, Zhao S, Haregu T, Zhang L. Temporal trends and geographic disparity in hypertension care in China. J Epidemiol. (2019) 30:29. doi: 10.2188/jea.JE20190029
19. Zhao Y, Oldenburg B, Mahal A, Lin Y, Tang S, Liu X. Trends and socioeconomic disparities in catastrophic health expenditure and health impoverishment in China: 2010 to 2016. Trop Med Int Health. (2019) 24:236–47. doi: 10.1111/tmi.13344
20. Yin P, Zhang M, Li Y, Jiang Y, Zhao W. Prevalence of COPD and its association with socioeconomic status in China: findings from China Chronic Disease Risk Factor Surveillance 2007. BMC Public Health. (2011) 11:586. doi: 10.1186/1471-2458-11-586
21. Zhao Y, Atun R, Oldenburg B, McPake B, Tang S, Mercer S, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Global Health. (2020) 8:e840–9. doi: 10.1016/S2214-109X(20)30127-3
22. Yao N, Wang J, Cai Y, Yuan J, Wang H, Gong J, et al. Patterns of cancer screening, incidence and treatment disparities in China: protocol for a population-based study. BMJ Open. (2016) 6:e012028. doi: 10.1136/bmjopen-2016-012028
23. Zhang Y, Bu Y, Gao H. Rural–urban disparities of breast cancer patients in China. Med Oncol. (2012) 30:387. doi: 10.1007/s12032-012-0387-5
24. Wen D, Wen X, Yang Y, Chen Y, Wei L, He Y, et al. Urban rural disparity in female breast cancer incidence rate in China and the increasing trend in parallel with socioeconomic development and urbanization in a rural setting. Thorac Cancer. (2017) 9:262–72. doi: 10.1111/1759-7714.12575
25. Wen X, Wen D, Yang Y, Chen Y, Wang G, Shan B. Urban-rural disparity in helicobacter pylori infection-related upper gastrointestinal cancer in China and the decreasing trend in parallel with socioeconomic development and urbanization in an endemic area. Ann Glob Health. (2017) 83:444–62. doi: 10.1016/j.aogh.2017.09.004
26. Wen D, Zou W, Wen X, Yang Y, Chen Y, He Y, et al. Urban–rural disparity in colorectal cancer incidence and increasing trend in relation to socioeconomic development and urbanization in China. J Int Med Res. (2018) 46:4181–96. doi: 10.1177/0300060518791090
27. Zhao Y, Hu Y, Smith J, Strauss J, Yang G. Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. (2012) 43:61–8. doi: 10.1093/ije/dys203
28. Raban M, Dandona R, Dandona L. Variations in catastrophic health expenditure estimates from household surveys in India. Bull World Health Organ. (2013) 91:726–35. doi: 10.2471/BLT.12.113100
29. Brinda E, Kowal P, Attermann J, Enemark U. Health service use, out-of-pocket payments and catastrophic health expenditure among older people in India: the WHO Study on global AGEing and adult health (SAGE). J Epidemiol Community Health. (2015) 69:489–94. doi: 10.1136/jech-2014-204960
30. Ranson MK. Reduction of catastrophic health care expenditures by a community-based health insurance scheme in Gujarat, India: current experiences and challenges. Bull World Health Organ. (2002) 80:613–21.
31. Li Q. Social Class in Current China: Measurement and Analysis. Beijing: Beijing Normal University Press (2010) (in Chinese).
32. Liu H. Research on English learning motivation: a social class perspective. J Northeast Norm Univ. (2014) 5:256–61. Available online at: https://d.wanfangdata.com.cn/periodical/dbsdxb-zxsh201405049
33. Xu H, Guo Y, Shi S. The impact of farmer differentiation on the willingness of farmland transfer of the households: based on structural equation model. China Land Sci. (2012) 26:74–9. doi: 10.3969/j.issn.1001-8158.2012.08.012. (in Chinese).
34. Zhang J, Liu Y, Du Q. Comparing sport consumer behaviors across social strata. Consumer Econ. (2012) 28:81–5. (in Chinese)
35. Mingling C, Yikang W, Hiroto N, Wang C, Luo J, Zhao G, et al. Socioeconomic status and physical activity in Chinese adults: a report from a community-based survey in Jiaxing, China. PLoS ONE. (2015) 10:e0132918. doi: 10.1371/journal.pone.0132918
36. Duncan OD. A Socioeconomic Index for All Occupations. In: Reiss AJ, editor. New York, NY: Free Press (1961). p. 109–38.
37. Li J, Shi L, Liang L, Ding G, Xu L. Urban-Rural disparities in health care utilization among Chinese adults from 1993 to 2011. BMC Health Serv Res. (2018) 18:102. doi: 10.1186/s12913-018-2905-4
38. Chen Y, Yin Z, Xie Q. Suggestions to ameliorate the inequity in urban/rural allocation of healthcare resources in China. Int J Equity Health. (2014) 13:34. doi: 10.1186/1475-9276-13-34
39. Shi LY. Health-care in China - a rural-Urban comparison after the socioeconomic reforms. Bull World Health Organ. (1993) 71:723–36.
40. Wu RX, Cai Y, Lan L, Fan ZW, Xue M. Trend analysis on the allocation of primary health care resources between urban and rural areas in China from 2008 to 2015. Chin Health Resour. (2017) 3:20–3. doi: 10.13688/j.cnki.chr.2017.17042
41. Weaver KE, Geiger AM, Lu L, Case LD. Rural-urban disparities in health status among US cancer survivors. Cancer. (2013) 119:1050–7. doi: 10.1002/cncr.27840
42. Kroneman M, Verheij R, Tacken M, van der Zee J. Urban-rural health differences: primary care data and self reported data render different results. Health Place. (2010) 16:893–902. doi: 10.1016/j.healthplace.2010.04.015
43. Sibley LM, Weiner JP. An evaluation of access to health care services along the rural-urban continuum in Canada. BMC Health Serv Res. (2011) 11:20. doi: 10.1186/1472-6963-11-20
44. Tao W, Zeng Z, Dang H, Li P, Kominski G. Towards universal health coverage: achievements and challenges of 10 years of healthcare reform in china. Brit Med J Glob Health. (2020) 5:e002087. doi: 10.1136/bmjgh-2019-002087
45. China NHaFPCo. Health and Family Planning Statistics Yearbook. Beijing: China Union Medical University Press (2015).
46. Yongjian X, Jie M, Na W, Wu N, Fan X, Zhang T, et al. Catastrophic health expenditure in households with chronic disease patients: a pre-post comparison of the New Health Care Reform in Shaanxi Province, China. PLoS ONE. (2018) 13:e0194539. doi: 10.1371/journal.pone.0194539
47. Li X, Zhang W. The impacts of health insurance on health care utilization among the older people in China. Soc Sci Med. (2013) 85(Complete):59–65. doi: 10.1016/j.socscimed.2013.02.037
48. Shen Lamson L. Inequities in access: the impact of a segmented health insurance system on physician visits and hospital admissions among older adults in the 2014 China Family Panel Studies. Int J Health Serv. (2019) 50:1–27. doi: 10.1177/0020731419867529
49. Gwatidzo SD, Stewart Williams J. Diabetes mellitus medication use and catastrophic healthcare expenditure among adults aged 50+ years in China and India: results from the WHO study on global AGEing and adult health (SAGE). BMC Geriatr. (2017) 17:1–15. doi: 10.1186/s12877-016-0408-x
50. Yao F, Shi CL, Liu CC, Wang L, Song SM, Ren JS, et al. Economic burden of stomach cancer in China during 1996-2015: a systematic review. Zhonghua Yu Fang Yi Xue Za Zhi. (2017) 51:756–62. doi: 10.3760/cma.j.issn.0253-9624.2017.08.018
51. Cai Y, Yan B, Zhou G. Analysis of direct economic burden and average hospitalization cost of lung cancer in China in 2011-2015. Chin J Health Statist. (2018) 35:16–9.
52. Guo LW, Shi CL, Huang HY, Wang L, Shi JF. Economic burden of esophageal cancer in China from 1996 to 2015: a systematic review. Zhong hua Liu xing bing xue Za zhi. (2017) 38:102–9. doi: 10.3760/cma.j.issn.0254-6450.2017.01.020
53. Jun Y, Le W, Chunlei S, Huiyao H, Yuting W, Jiang L, Jianjun Z, et al. Economic burden of liver cancer in China during 1996-2015: a systematic review. Chin J Dis Control Prevent. (2017) 21:835–40. doi: 10.16462/j.cnki.zhjbkz.2017.08.020
54. Liu C, Huang H, Shi J. Economic burden of colorectal cancer in China from 1996 to 2015: a systematic review. China Cancer. (2017) 26:859–67. doi: 10.11735/j.issn.1004-0242.2017.11.A005
55. Le W, Xinpei Y, Jufang S, Shijiao H, Juan Z, Chunlei S, et al. Economic burden of breast cancer in China in the past two decades. Chin J Dis Control Prevent. (2017) 25:143–6. doi: 10.16386/j.cjpccd.issn.1004-6194.2017.02.019
56. Shi J, Shi C, Yue X, Huang H, Wang L, Li J, et al. Economic burden of cancer in China during 1996-2014: a systematic review. Chin J Oncol. (2016) 38:929–41. doi: 10.3760/cma.j.issn.0253-3766.2016.12.010
57. The State Council of the People's Republic of China. Including 22 Anticancer Drugs and 14 Chronic Disease Drugs into the “National Basic Medical Insurance Drug Catalogue. Available online at: http://www.gov.cn/xinwen/2019-12/17/content_5461773.htm (accessed December 17, 2019).
Keywords: cancer study, healthcare, health expenditure, rural-urban difference, China
Citation: Zhao Y, Tang S, Mao W and Akinyemiju T (2022) Socio-Economic and Rural-Urban Differences in Healthcare and Catastrophic Health Expenditure Among Cancer Patients in China: Analysis of the China Health and Retirement Longitudinal Study. Front. Public Health 9:779285. doi: 10.3389/fpubh.2021.779285
Received: 18 September 2021; Accepted: 15 December 2021;
Published: 11 January 2022.
Edited by:
Amelia Kekeletso Ranotsi, Maluti Adventist College, LesothoReviewed by:
Lan Hoang Nguyen, Hue University, VietnamMarte Karoline Råberg Kjøllesdal, Norwegian Institute of Public Health (NIPH), Norway
Copyright © 2022 Zhao, Tang, Mao and Akinyemiju. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yang Zhao, d3poYW9AZ2VvcmdlaW5zdGl0dXRlLm9yZy5jbg==; eGl5dW5qdXNoaUAxNjMuY29t