 Mona Alhasani
Mona Alhasani Dinesh Mulchandani1
Dinesh Mulchandani1 Oladapo Oyebode
Oladapo Oyebode Nilufar Baghaei
Nilufar Baghaei Rita Orji
Rita Orji- 1Faculty of Computer Science, Dalhousie University, Halifax, NS, Canada
- 2Games and Extended Reality Lab, Massey University, Auckland, New Zealand
Stress is one of the significant triggers of several physiological and psychological illnesses. Mobile health apps have been used to deliver various stress management interventions and coping strategies over the years. However, little work exists on persuasive strategies employed in stress management apps to promote behavior change. To address this gap, we review 150 stress management apps on both Google Play and Apple's App Store in three stages. First, we deconstruct and compare the persuasive/behavior change strategies operationalized in the apps using the Persuasive Systems Design (PSD) framework and Cialdini's Principles of Persuasion. Our results show that the most frequently employed strategies are personalization, followed by self-monitoring, and trustworthiness, while social support strategies such as competition, cooperation and social comparison are the least employed. Second, we compare our findings within the stress management domain with those from other mental health domains to uncover further insights. Finally, we reflect on our findings and offer eight design recommendations to improve the effectiveness of stress management apps and foster future research.
Introduction
Stress is a common and continuous phenomenon that poses mild to serious physical and mental health risks to individuals (1). Stress is in various forms such as routine stress (i.e., pressures from work, family, school, and other daily activities), traumatic stress (caused by events such as accidents, war, harassment or assault, natural disasters, disease outbreak, etc.), and others such as stress due to sudden negative events like divorce, sickness, and job loss (2). Stress can be short-term (acute stress) or repeatedly occur over a long term (chronic stress). Evidence shows that more than three-quarters of adults in the United States report physical or emotional stress symptoms including headache, tiredness, and sleep disorders in 2019 (3). Moreover, stress has been linked to coronary heart disease (4), Type 2 diabetes (5), cardiovascular disease (6–9), childhood asthma, and wheezing due to maternal stress during pregnancy (10), osteoporosis (11), miscarriage (12), menstrual problems (13), acne (14), obesity (15), autoimmune disease (16), and Alzheimer's disease (17). The mental health consequences of stress (e.g., anxiety, depression, panic attacks, sleep disorders, and low cognitive performance) have also been documented (18–22). In addition, maternal stress during pregnancy has been shown to negatively affect offspring's neuro and cognitive development, triggering negative affectivity, difficult temperament, and psychiatric disorders (23). Stress can be reduced or managed through mindfulness and meditation (24–32), music (33), and nature relatedness (34, 35), cognitive-behavioral therapy (36–38), stress-reduction programs (31, 39), and structured counseling (40, 41).
In recent years, stress management interventions have been delivered to target audiences through mobile health (mHealth) apps due to the proliferation of smartphones (42) and advancements in smartphone technology. These apps are capable of detecting stress through continuous monitoring of heart rate variability (43, 44) using smartphone sensors (e.g., photoplethysmography) or wearable devices such as heart-rate chest strap and electrocardiography (45). In addition, mHealth apps can detect stress through skin conductance (46) or self-reports (such as daily mood logs) (47). Furthermore, mHealth apps can deliver real-time stress relief or relaxation features (such as breathing sessions, mindfulness and meditation practice, emotion regulation programs, etc.) using biofeedback techniques (48–50), conversational coaches (51), gamification, videos, etc. Evidence shows people's willingness to adopt mHealth apps for their stress relief needs (52). Research also indicates that mHealth apps are effective in reducing stress and improving users' wellbeing over time (53, 54). To promote continuous engagement with stress management apps, designers/developers operationalized various persuasive or behavior change strategies, whether consciously or unconsciously, to help users deal with their stress. Although systematic reviews of persuasive health apps exist in the literature (55–57), little is known about the persuasive strategies employed in stress management apps to motivate behavior change, to the best of our knowledge.
In this paper, we reviewed and analyzed 150 stress management apps on both Google Play and App Store with the aim of deconstructing the persuasive and behavior change techniques they employed using the Persuasive Systems Design (PSD) framework (58) and Cialdini's Principles of Persuasion (CPP) (59) which are two widely employed frameworks in persuasive and behavior change systems design. Specifically, we address the following research questions:
RQ1: What are the most and least employed strategies in stress management apps?
RQ2: How are the strategies operationalized or implemented in these apps?
RQ3: How do stress management apps compare with apps in other mental health domains in terms of the persuasive strategies employed?
Background
Persuasive Strategies and Persuasion Frameworks
Fogg et al. defined persuasive technology as “interactive computing systems designed to change people's attitudes and behaviors” (60). Similarly, Oinas-Kukkonen et al. defined persuasive systems as “computerized software or information systems designed to reinforce, change or shape attitudes or behaviors or both without using coercion or deception” (61). Both Fogg and Oinas-Kukkonen proposed persuasion frameworks that are useful in analyzing and designing persuasive technologies—the Fogg Behavior Model (FBM) (62) and Persuasive Systems Design (PSD) framework (58), respectively. The FBM posits that a person must meet three conditions to perform a target behavior: (i) be sufficiently motivated, (ii) possess the ability to perform the behavior, (iii) receive the trigger to perform the behavior. Hence, behavior is a combination of three factors that must occur at the same time: motivation, ability, and triggers. The PSD framework builds upon the FBM to describe how to inject persuasive features that motivate behavior change into systems during the design process. The PSD framework comprises 28 persuasive strategies grouped into four categories—primary task support, dialogue support, system credibility support, and social support. The primary task support category comprises persuasive strategies that support users in carrying out their primary task. In contrast, the dialogue support category includes persuasive strategies that provide some degree of system feedback to users. The system credibility support category comprises persuasive strategies that support designing a system that it is more credible and thus more persuasive. The social support category includes persuasive strategies that enable system users to interact or socialize with others. Table 1 shows the four categories and their respective persuasive strategies, as well as a description of each strategy according to (58).
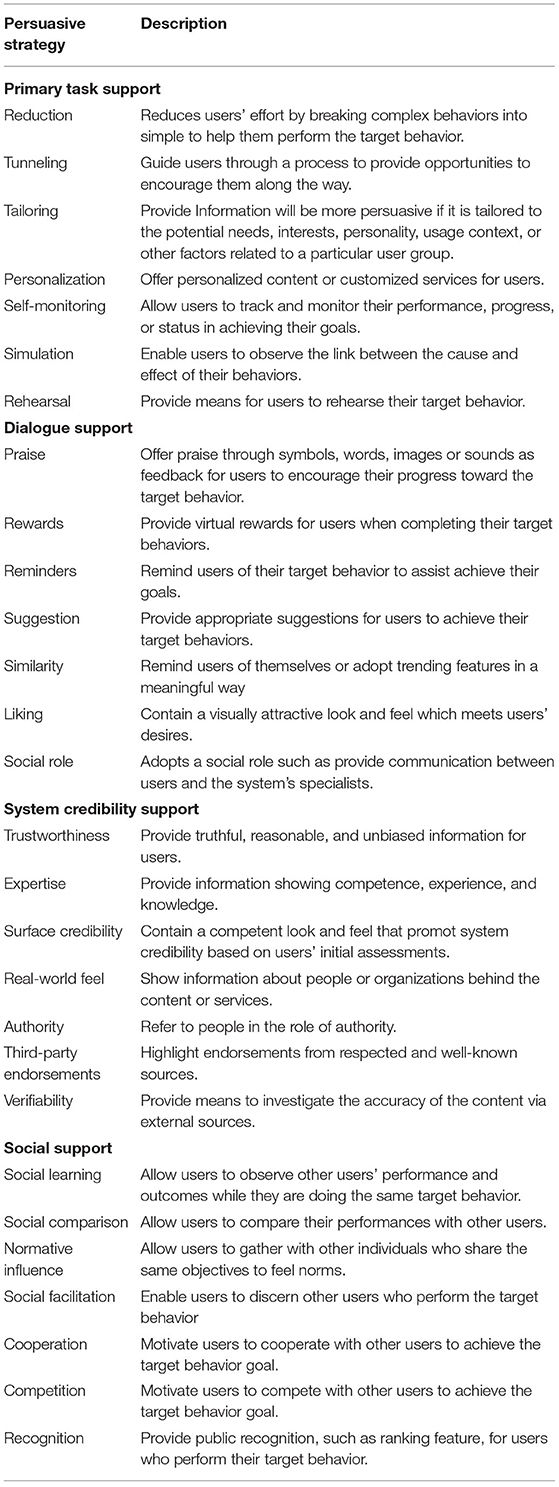
Table 1. Twenty-eight persuasive strategies in the Persuasive Systems Design (PSD) framework.
Additional frameworks have emerged over the years, such as Cialdini's Principles of Persuasion (CPP) (59). CPP comprises six (6) persuasive strategies described below:
• Reciprocity: give gifts or freebies to users, and they will repay in kind
• Social Proof: use peer power whenever it is available
• Liking: uncover real similarities and offer genuine praise
• Consistency/commitment: make user commitments active, public, and voluntary
• Authority: demonstrate expertise, and
• Scarcity: highlight unique benefits and exclusive information.
Although the PSD framework is comprehensive and widely used to extract persuasive strategies implemented in mobile apps, the framework did not capture strategies such as reciprocity, consistency/commitment, and scarcity which are commonly implemented in apps for behavior change (57). In addition, social proof, liking, and authority strategies in CPP are similar to social facilitation, liking, and authority strategies in PSD. Hence, in this study, we focused on reciprocity, consistency/commitment, and scarcity from CPP in addition to the PSD strategies.
Persuasive Strategies Employed in Mobile Health (mHealth) Apps
Previous research has investigated the persuasiveness of apps targeting various domains, including health, using the PSD framework only or in conjunction with other persuasion frameworks.
In the general area of health and wellness, Langrial et al. (63) reviewed 12 healthcare apps to identify the PSD framework's persuasive strategies. Their findings revealed that strategies in the primary task support category (especially self-monitoring, reduction, and personalization) were relatively broadly utilized, while dialogue support strategies were largely underutilized. In addition, the implementation of social support strategies was found to be shallow. Similarly, Oyebode et al. (57) conducted a comparative analysis of 80 health and wellness apps to evaluate the persuasive features implemented using the PSD and CPP frameworks. Their findings revealed that personalization, self-monitoring, suggestion, trustworthiness, surface credibility, and liking are the dominant persuasive strategies under the PSD framework, while consistency/commitment is the dominant strategy under CPP. In addition, persuasive strategies under the social support category were generally underutilized. To investigate the effectiveness of persuasive technologies for health and wellness, Orji and Moffatt (64) conducted a literature search and found that persuasive technologies effectively promote healthy behaviors, with 92% of reviewed articles reporting positive outcomes. Similarly, Hamari et al. (65) conducted empirical research on persuasive technologies (95 articles), and the results show that 92.6% of the reviewed articles reported positive outcomes.
In the area of mental health, Alqahtani et al. (55) analyzed 103 mental health apps to determine their persuasiveness using the PSD framework and Behavior Change Techniques (BCTs). Their results revealed that self-monitoring is the most frequently employed persuasive strategy, followed by personalization, reminder, and rewards. Similarly, Chang et al. (66) analyzed 12 mental health apps using the PSD framework and Goal-setting theory. Their findings showed that persuasive strategies in the primary task support categories, including goal setting, are the most employed, while social support strategies were the least employed.
In the domain of disease management, Geuens et al. (67) reviewed 28 mobile apps for managing chronic arthritis using the PSD framework and BCTs. Their results revealed that persuasive strategies in the system credibility support are the most employed, followed by strategies in the primary task support, dialogue support, and social support categories in decreasing order of utility. Similarly, Fadhil and Wang (68) investigated the persuasiveness of 19 diabetes management apps and coded them using the PSD framework and BCTs. Based on their findings, persuasive strategies in the primary task support category (especially personalization, self-monitoring, and tailoring) and system credibility support (especially expertise and trustworthiness) are the most employed. In contrast, dialogue support and social support strategies are the least employed.
Furthermore, Win et al. (69) examined the persuasive features employed in medication management apps retrieved from 13 research articles using the PSD framework. Based on their findings, persuasive strategies in the primary task support and dialogue support categories (such as tailoring, self-monitoring, and reminders) were widely employed in the apps, while those in the social support category were the least utilized. Furthermore, Lehto et al. applied the PSD framework to identify and analyze persuasive strategies in web-based alcohol and smoking interventions retrieved from 23 articles. Their findings showed that primary task support strategies (especially reduction, self-monitoring, simulation, and personalization) were relatively widely utilized, while persuasive strategies in the social support category were moderately utilized. In addition, dialogue support strategies were generally found to be underutilized.
In the physical activity domain, Matthews et al. (70) reviewed fitness apps from 20 research articles using the PSD framework. Their findings revealed that self-monitoring is the most widely represented strategy in the primary task support category, followed by personalization and tunneling, while suggestion is the most common dialogue support persuasive strategy. Almutari and Orji (71) focused on identifying social support strategies employed by physical activity apps in 32 studies using the PSD framework. They found that majority of the apps employed the competition persuasive strategy to promote social interaction, followed by the cooperation and social comparison strategies.
In summary, the literature review above shows that the dominance of the strategy utilization in persuasive and behavior change app design varies; however, there is no analysis targeting the stress management domain and how the results compare with other areas of mental health. Therefore, this paper utilized the PSD and CPP frameworks to deconstruct the persuasive strategies implemented in 150 stress management apps. We conducted a comparative analysis to understand the persuasive strategies employed in the apps and uncover new insights that drive future research.
Methods
In this section, we discuss the app selection criteria and coding process.
Selection of Stress Management Apps
Apps were extracted from Google Play and Apple's App Store automatically using a script that we developed using JavaScript and Node.js runtime. Search keywords were formulated by combining the term “stress” with each of the following terms: management, monitoring, support, detection, mindfulness, meditation, breathing, relief , relaxation, curbing, prevention, and treatment. The search was conducted in February 2020 and produced 4,375 apps in total (3,308 apps from App store and 1,067 from Google Play). For analysis, the inclusion criteria were: (1) apps must have more than four user comments, (2) apps must be related to stress, and (3) apps must be free or free with in-app purchases (free/free*). The apps that did not meet all of these criteria were excluded. To avoid duplication, any app that appeared on both platforms were considered as one. Information like app name, platform (i.e., iOS, Android, or both), developer name, free/free* were collected. We randomly selected 150 out of the 318 eligible apps for review (see Figure 1). One hundred fifty is a good number for generalizable results.
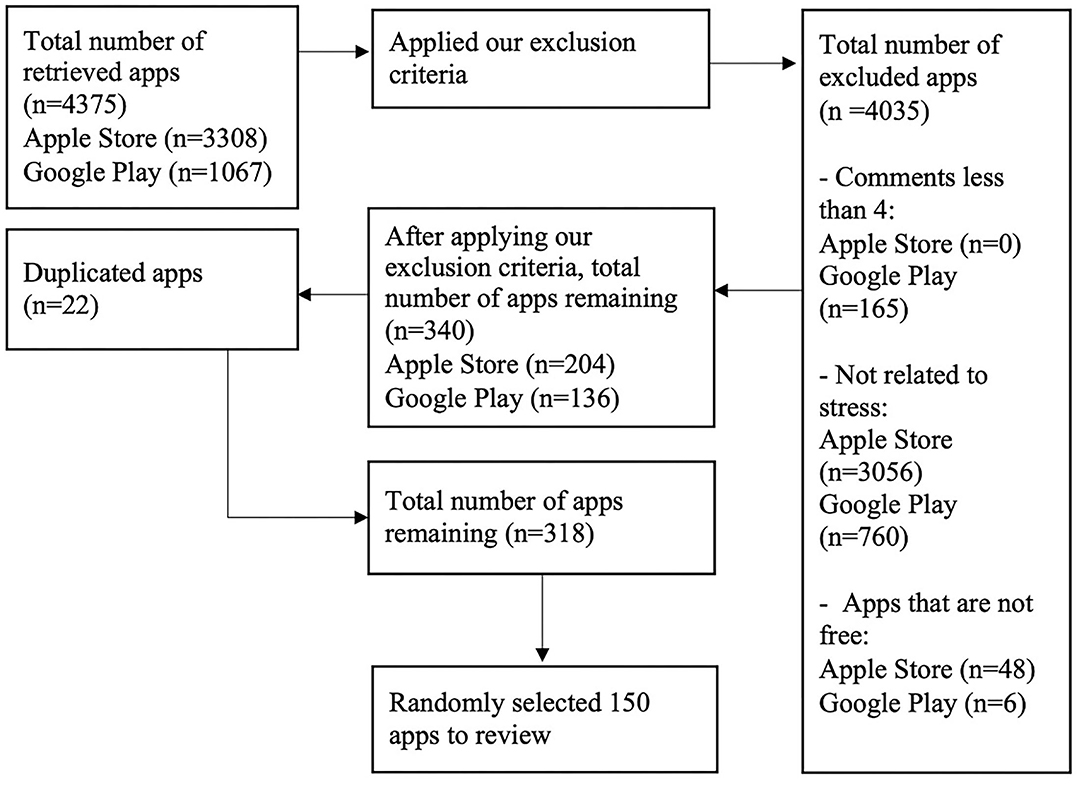
Figure 1. App selection process (150 apps selected).
Process of Coding Apps for Persuasive Strategies
The purpose of coding the apps in our research is to evaluate the number and type of persuasive strategies employed in mental health apps specifically related to stress. We collected 150 apps and deconstructed the persuasive strategies employed using the PSD and CPP frameworks. We combined both frameworks to boost the coverage of our coding process. Two persuasive technology researchers coded the apps after installing them and performing various tasks using the apps' features. For apps with in-app purchases, researchers accepted the free trial to enable examination of all persuasive strategies employed in the apps. The interrater agreement score for each strategy was computed after coding. Finally, a third expert reviewer was involved in resolving any disagreement for strategies having agreement score <100%. Figure 2 shows the steps of coding the apps. Appendices A, B present the summary of the apps evaluated and the persuasive strategies employed in the apps.
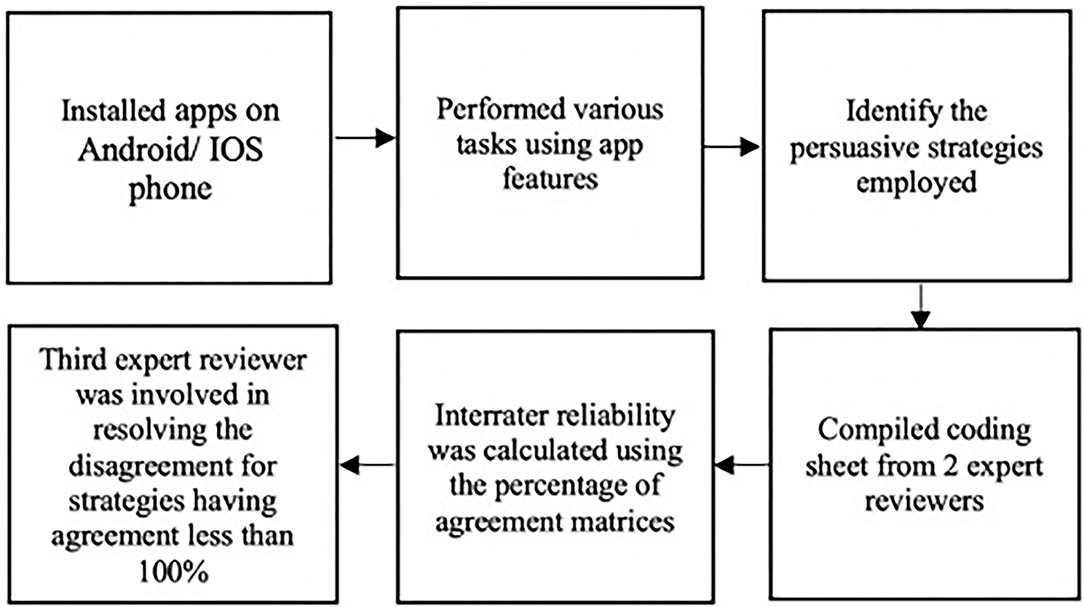
Figure 2. Process of coding apps.
Agreement
The interrater reliability for the coded apps was measured using the percentage of agreement metric (6), as shown in Table 2. Agreement occurs when both researchers indicate the presence or absence of a persuasive strategy in an app. Disagreement occurs if one reviewer indicates the presence of a strategy and the second reviewer indicates an absence. Reliability values range between 85.7 and 100% agreement depending on the persuasive strategy. The strategy with the lowest interrater reliability (85.7%) is social role, while 27 out of the 31 strategies obtained perfect agreement scores. Overall, all intercoder reliability scores are within the acceptable range [i.e., > 60% (72)].
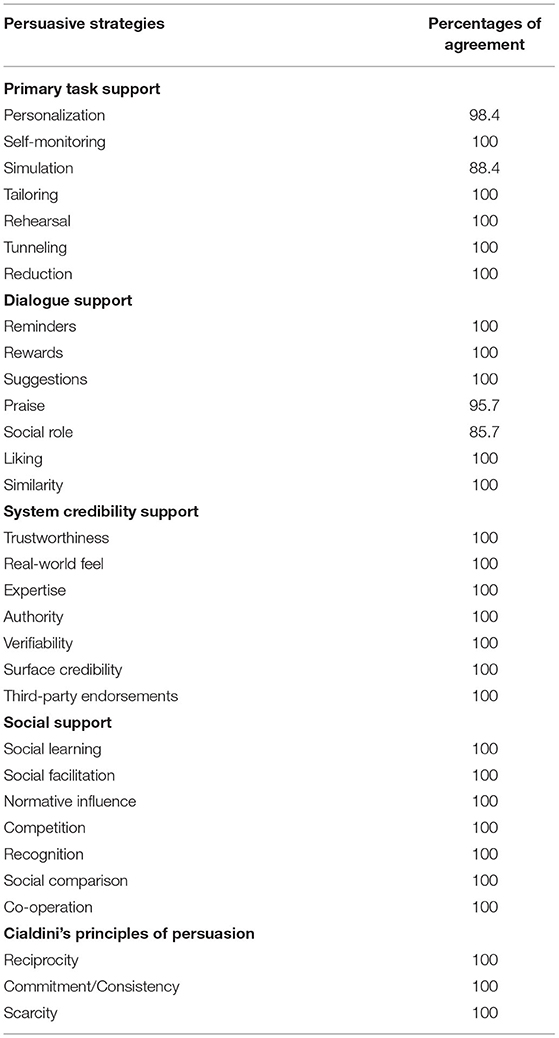
Table 2. Agreement percentage of persuasive strategies.
Categories of Stress Management Apps Based on Their Purpose
We classified apps into three categories, as shown in Figure 3, based on the purpose intended by the app. Most apps were designed to provide different sets of interventions to help users relieve and cope with stress. For example, apps provide different relaxation sessions or a list of games to help reduce stress levels. However, some apps were developed to monitor or track users' stress levels by allowing them to record their feelings either manually or by capturing their stress in real-time via sensors. Few apps combined both stress monitoring (tracking) and intervention by detecting users' stress levels and providing interventions such as meditation and relaxation sessions.
Figure 3. Stress management apps categorized according to their purpose.
Results
This section describes the results of our analysis, including information about the apps reviewed, implementation of the persuasive strategies employed, and comparison between the different categories of persuasive strategies.
Information on Selected Apps
Table 3 presents a summary of the reviewed apps.
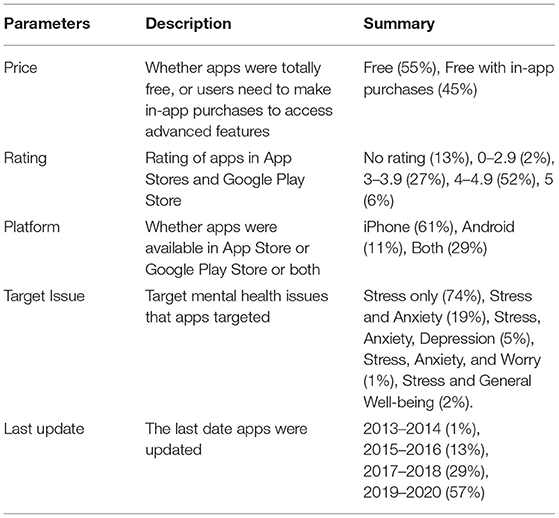
Table 3. Summary of the selected stress management apps.
Persuasive Strategies and Their Implementation
To answer our second research question (RQ2), we identified how each persuasive strategy is operationalized or implemented in all 150 stress management apps. We discuss these implementations in the following subsections.
Primary Task Support Strategies and Their Implementation
Figure 4 illustrates the frequency of the primary task support strategies in the reviewed apps. Among the seven (7) strategies in primary task support, we observed that personalization (n = 121) is the most employed strategy, followed by self-monitoring (n = 77), simulation (n = 43), tailoring (n = 32), rehearsal (n = 14), and reduction (n = 12). However, tunneling (n = 11) is the least employed strategy in the primary task support category.
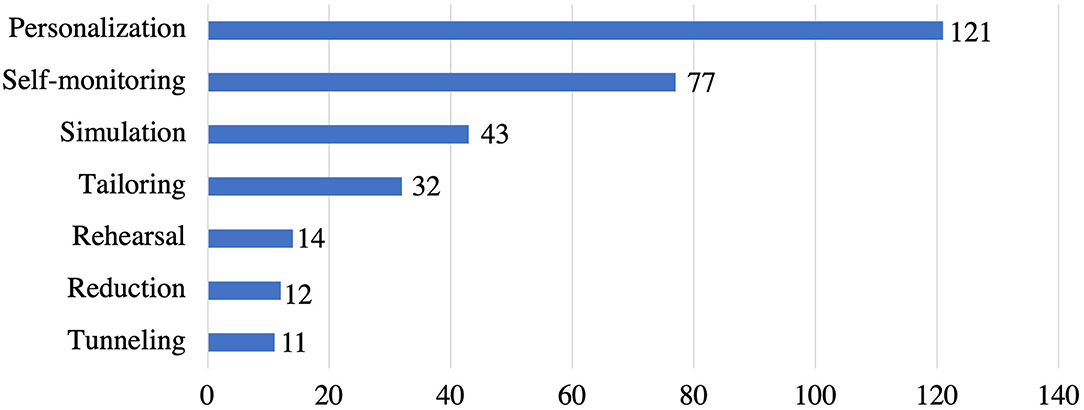
Figure 4. Persuasive strategies under primary task support category and the corresponding number of apps that implemented individual strategies.
Each strategy was operationalized in multiple ways, as shown in Table 4. For example, personalization strategy was implemented via individualized pre-assessments (24 apps), personalized app content based on user's preferences (7 apps), personalized avatar (2 apps), or offering customization features (88 apps). Among the 77 apps that implemented self-monitoring, 17 apps utilized self-report method for recording stress and anxiety levels (using responses from pre and post-assessment questions), 33 apps provide automatic logging of stress levels using chatbots, and remaining 27 apps provided manual journaling feature to record own thoughts about your mood, stress, anxiety, etc. within the app. In addition, all the 77 apps provided some sort of visualization for users to monitor their progress using graphs/charts. Furthermore, 43 apps that implemented simulation strategy used the following: stress relief games (28 apps), observing stress and anxiety levels with real-time sensors (9 apps), and synchronizing activity progress to tree/flower growth (6 apps). Besides, tailoring was employed in a total of 32 apps, out of which 16 apps provided the option to switch languages, and the remaining 16 apps offered tailored app content based on user type and age group. On the other hand, rehearsal was implemented by 14 apps allowing users to practice interaction for capturing stress and anxiety levels using heart rate sensors (6 apps) and training the user about the gestures to play stress relief games (8 apps). Furthermore, 12 apps implemented reduction strategy by allowing users to use hashtags for quick journaling (9 apps) and a search bar option to search for specific sessions and navigate through fast (3 apps). Finally, only 11 apps implemented tunneling strategy by offering step-by-step weekly or daily sessions.
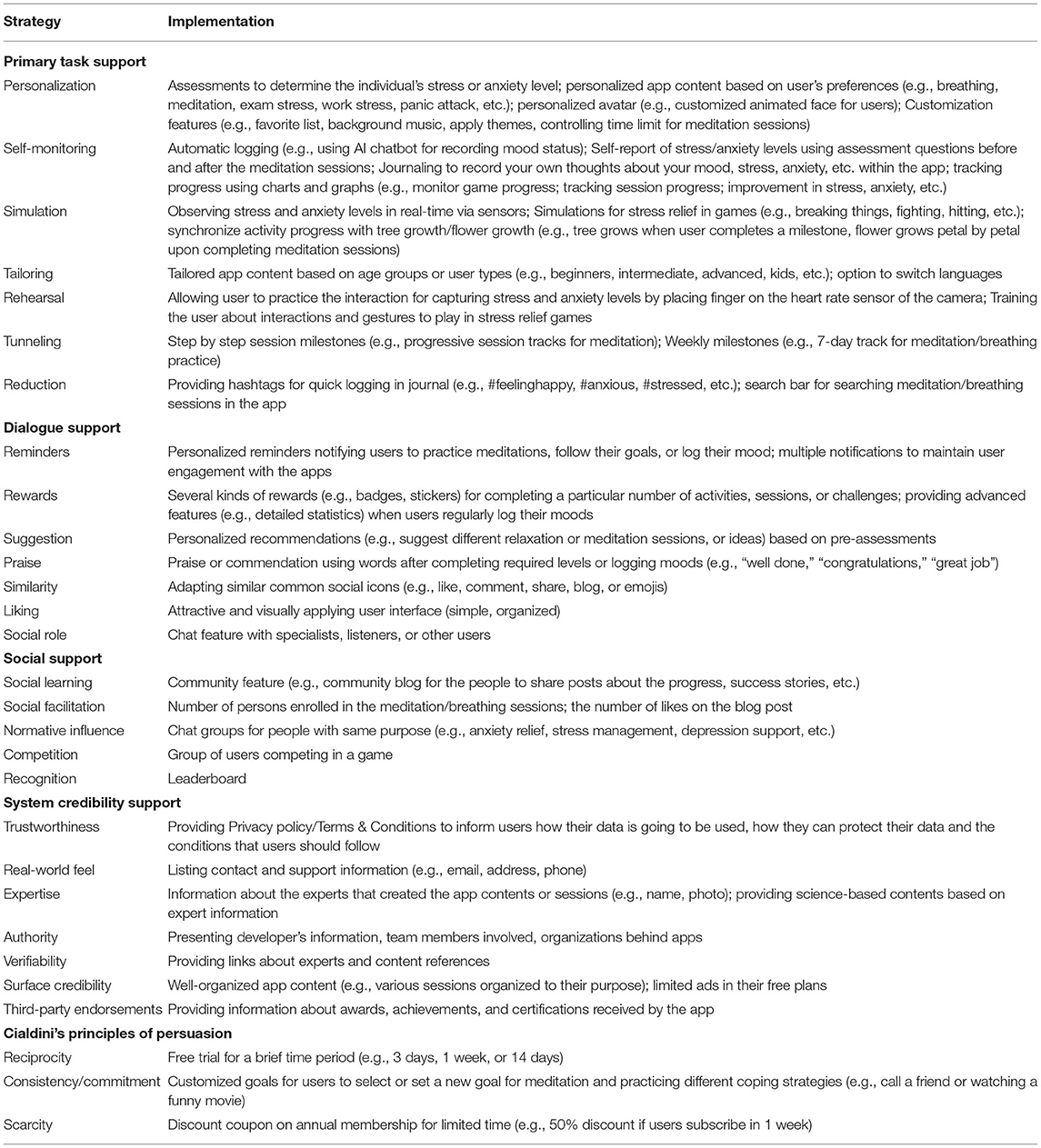
Table 4. Summary of persuasive strategies and how they are implemented in the apps.
Dialogue Support Strategies and Their Implementation
Figure 5 shows the dialogue support strategies employed in the reviewed apps. We found that reminders strategy (n = 54) is the most commonly employed strategy, followed by rewards (n = 35), suggestion (n = 31), and praise (n = 23). However, social role (n = 14), liking (n = 10), and similarity (n = 6) are the least employed dialogue support strategies in stress management apps.
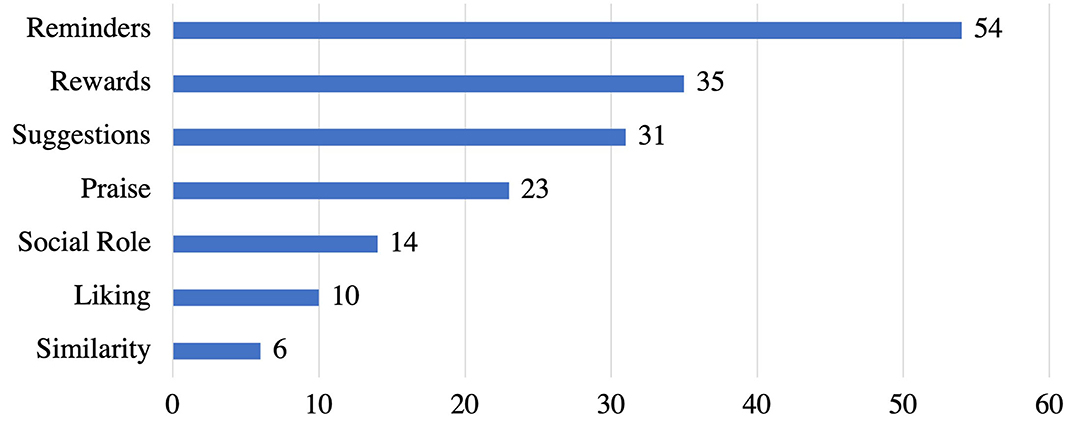
Figure 5. Persuasive strategies under dialogue support category and the corresponding number of apps that implemented individual strategies.
Each strategy has one or more different implementations, as presented in Table 4. Out of the 54 apps that implemented the reminders strategy, 46 apps provide personalized reminders. Users can set times, days, and how often they want to be notified to practice meditations, follow their goals, or log their mood. Only 8 apps did not make the reminder/notification feature customizable. Furthermore, 35 apps implemented the rewards strategy as badges, stickers or unlock advanced features. Besides, suggestion was implemented as personalized recommendations in 31 apps based on the result of in-app assessments (such as questions for assessing user moods and needs). Also, 23 apps implemented praise as words of commendation for completing required levels or logging moods. On the other hand, social role, was implemented as a chat feature in 14 apps. Also, 10 apps implemented the liking strategy by presenting an attractive or visually appealing user interface to users. Finally, only 6 apps implemented similarity strategy by providing features or icons (such as emojis) that depict users' current mood.
Social Support Strategies and Their Implementation
Figure 6 illustrates the frequency of employing the social support strategies in the reviewed apps. Among the seven strategies in social support category, we uncovered that social learning (n = 9) is the most employed strategy, followed by social facilitation (n = 8), and normative influence (n = 4). Yet, recognition (n = 3) and competition (n = 2) are the least implemented strategies. While co-operation and social comparison were not implemented in any of the stress management apps reviewed.
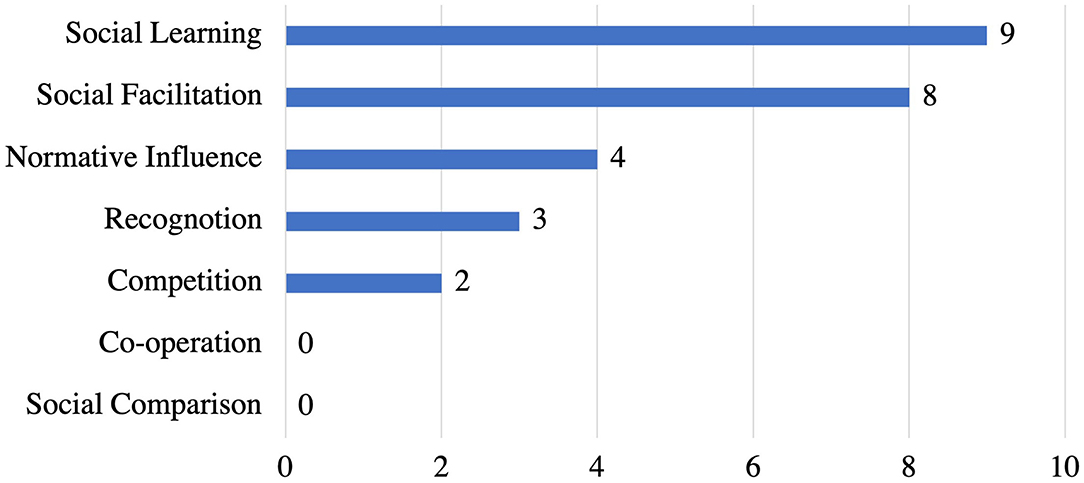
Figure 6. Persuasive strategies under social support category and the corresponding number of apps that implemented individual strategies.
Table 4 shows the implementations for social support strategies in the reviewed apps. social learning strategy was employed by 9 apps as providing users with the community blog feature for sharing their success stories so that other people can learn from them. A total of 8 apps implemented the social facilitation strategy by highlighting the number of enrolled users in a meditation session or the number of likes on the blog post. Normative influence was implemented in 4 apps as chat groups. On the other hand, recognition and competition were implemented in 3 apps (as leaderboard ranking) and 2 apps (as group of users competing in a game), respectively.
System Credibility Support Strategies and Their Implementation
Figure 7 presents the system credibility support strategies implemented in the reviewed apps. Trustworthiness (n = 59) is the most employed strategy, followed by real-world feel (n = 58), expertise (n = 39), authority (n = 17), and verifiability (n = 14). Yet, surface credibility (n = 9) and third-party endorsements (n = 6) are the least employed strategies in stress management apps.
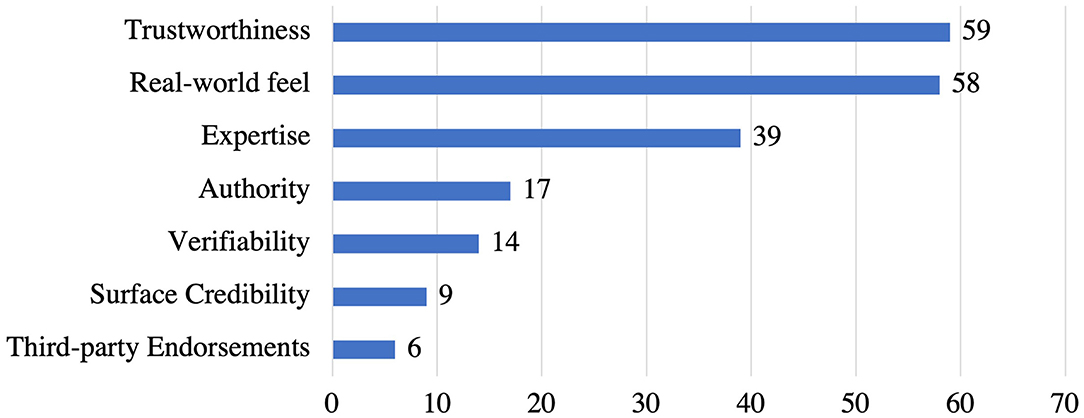
Figure 7. Persuasive strategies under system credibility category and the corresponding number of apps that implemented individual strategies.
Most system credibility support strategies were identified to have a single implementation, as showed in Table 4. For trustworthiness strategy, 59 apps provide both privacy policy and terms/conditions to explain to users how their data is going to be utilized, information about the secure data transmission to third party entities and maintaining the confidentiality of the users as a way to gain users' trust. Besides, real-world feel (n = 58) strategy was implemented by including different contact information such as e-mails, phone numbers, addresses that allow users to reach people behind the apps for providing feedback or answering their concerns. Moreover, 26 out of 39 apps implemented the expertise strategy by showing names, brief information, and/or photos of expertise behind the app contents or meditation sessions while 13 apps present science-based contents based on expert information. Also, 17 apps employed authority strategy by listing names of developers, team members involved, and the organizations such as universities behind the apps. Furthermore, 14 apps implemented verifiability strategy as links that show more details about experts in the app and references to verify apps' content (reference list). However, 9 apps implemented surface credibility strategy by presenting well-organized content according to the purpose of the apps and limited ads in their free plans. Lastly, only 6 apps implemented third-party endorsements strategy by showing awards, achievements, or certifications received by the app from external people or agencies.
CPP Persuasive Strategies and Their Implementations
Figure 8 shows CPP strategies employed in the reviewed apps. Reciprocity (n = 21) is the most commonly employed strategy, followed by consistency/commitment (n = 14). On the other hand, scarcity (n = 13) emerged as the least implemented strategy in stress apps.
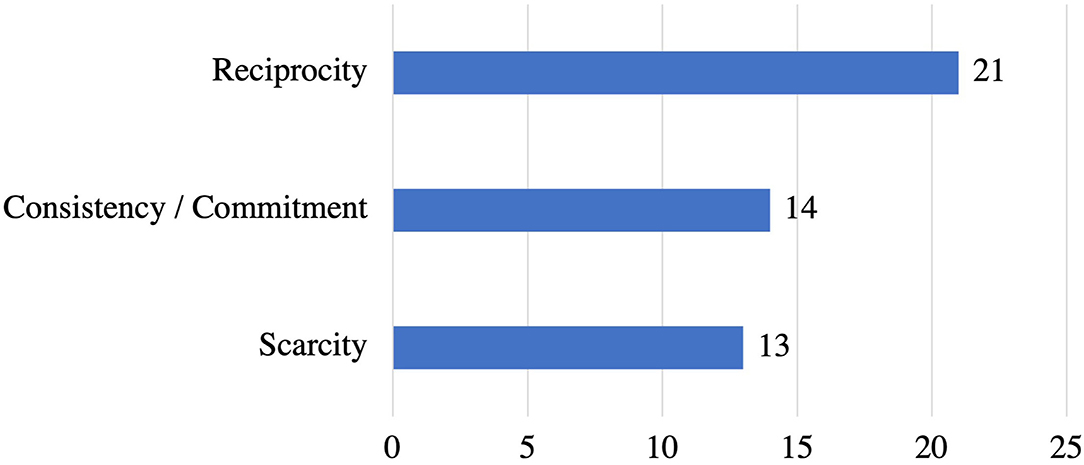
Figure 8. Persuasive strategies under CPP and the corresponding number of apps that implemented individual strategies.
Table 4 presents ways of implementation for each strategy. Reciprocity strategy was implemented in 21 apps by offering a free trial for a brief period such as 7 days free trial to try all advanced features in the app. Moreover, 14 apps employed consistency/commitment strategy by allowing users to customize their goals based on their preferences, such as setting a goal to practice specific meditation or relaxation sessions for a week. Also, users can select different goals to help them cope with their stress, such as calling a friend, watching a funny movie, or writing a letter for a family member, etc. Finally, scarcity is the least employed strategy, implemented in 12 apps as discount coupons on annual membership for a limited time.
Summary of the Study Findings
Figure 9 shows the comparison between different categories of PSD and CPP frameworks regarding the number of persuasive strategies employed in the reviewed apps. Our findings showed that primary task support strategies of the PSD model are the most commonly employed in the reviewed apps, followed by system credibility support, dialogue support strategies, and the CPP strategies. However, we found that social support strategies are least employed overall. This answered our first research question (RQ1).
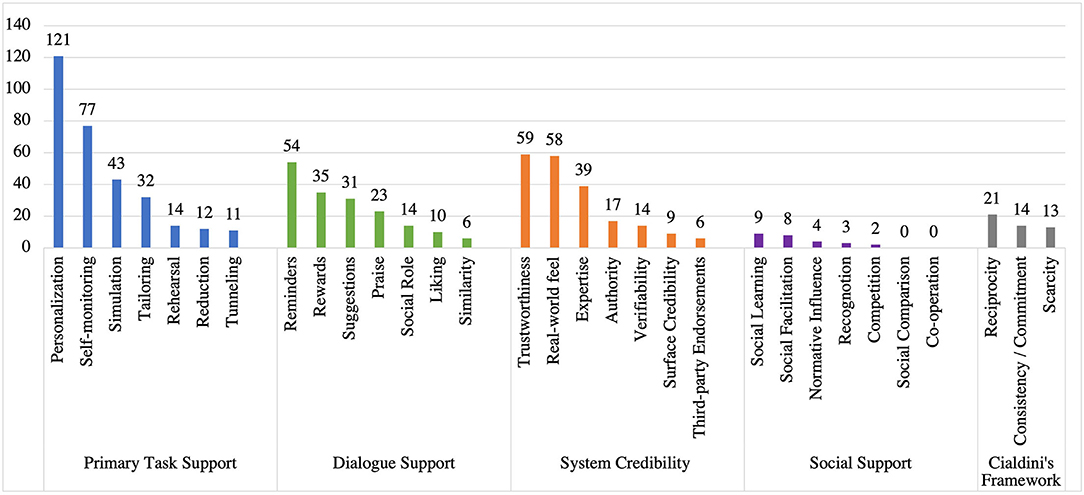
Figure 9. Summary of persuasive strategies employed in stress management apps.
Comparing Strategies Employed in Stress Management Apps With Other Mental Health Domains
In this section, we compare our findings of persuasive strategies in stress management apps to an existing systematic review of apps in other mental health domains including anxiety, depression, fears and worries, and mood disorder (55). As shown in Figure 10, personalization is the most commonly implemented strategy followed by self-monitoring and reminders in anxiety apps. Similarly, personalization is the most frequently employed strategy, followed by reminders and self-monitoring in depression apps. Personalization and self-monitoring strategies are equally implemented in apps targeting fear and worry, followed by reminders, tunneling, and praise strategies. However, in mood disorders apps, self-monitoring is the most employed strategy, followed by reminders and personalization. Furthermore, rehearsal, authority, verifiability, and social learning are the least employed strategies in anxiety apps. Similarly, the least implemented strategies in depression apps are social role, praise, verifiability, and social learning. However, the least employed strategies in mood disorder are reminders, rewards, real-world feel, and third-party endorsements.
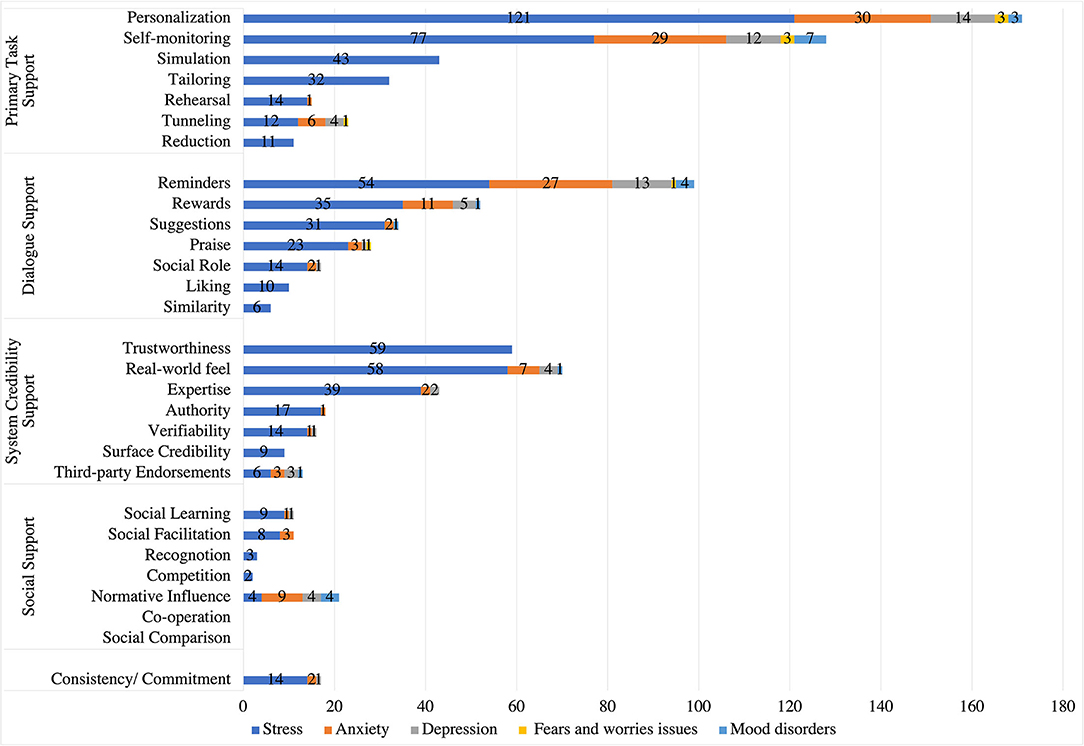
Figure 10. Comparing persuasive strategies in stress management apps with those in other mental health domains.
Interestingly, our findings shows that tailoring, simulation, reduction, similarity, trustworthiness, and surface credibility were not employed in any other mental health apps. This distinguishes stress-related apps from other mental health apps with respect to the strategies employed in their designs. Our finding confirms that personalization and self-monitoring are the most frequently implemented persuasive strategies in stress management and other mental health apps. On the other hand, our results show that simulation, trustworthiness, real-world feel, and expertise strategies are commonly employed in stress management apps, compared to other mental health apps. This answered our third research question (RQ3).
Discussion
The goal of this review was to determine which persuasive strategies were employed in apps for managing stress. The following sub-sections discuss our findings based on PSD and CPP frameworks.
Primary Support Strategies
Majority of the apps that were coded (94%) employed the personalization strategy to deliver content and interventions personalized to individual users based on their profiles (such as demographics, medical history, etc.) and activities within the app (i.e., behavioral patterns). Evidence already affirms the global shift from standard healthcare to personalized healthcare to enhance patient experience and significantly improve their health and wellbeing (73–75). Hence, it is unsurprising that mobile health (mHealth) apps that offer personalized content or services were found to be effective by target users (76–79), including apps for managing stress (80).
Self-monitoring is the next commonly used persuasive strategy after personalization. Our results show that 59% of the analyzed apps employed self-monitoring to deliver features that enable users to record their activities manually or automatically and track progress toward set goals over time. This strategy is crucial for apps that support self-management of health-related issues by enhancing users' insights into the state of their health and motivating them to take charge and seek medical attention where necessary. For example, data captured through self-monitoring can be used to track the risk of mild or chronic health conditions [including mental health issues, such as mood disorder (81), depression (82), stress (44), and others (83)] in real-time, and then trigger interventions to mitigate the risk. Interestingly, research has also found personalization and self-monitoring as dominant strategies in other mental health-related apps (55) since user activity data (or behavioral data) can be used to offer personalized services or interventions that will improve users' health and wellbeing.
Moreover, the simulation strategy which allows users to observe the cause and effect of their behavior was found in 34% of the analyzed apps. For example, some apps use tree and flower metaphors such as petal growth in the flower or more leaves on the tree to show the influence of completing meditation sessions on health. Research has shown that simulation can yield positive outcomes in patients experiencing stress (43, 84).
Furthermore, tailoring strategy offers similar content to users who share common interests and rehearsal strategy that allows users to rehearse a target behavior found in 21% of the coded apps. However, tunneling and reduction persuasive strategies were found in only 9 and 6% of the stress management apps, which is surprising since mental health patients are usually advised to avoid stressful situations and complex activities that can increase their stress levels. In addition, users can get frustrated easily if in-app support or guidance is missing in mental apps (85, 86).
Dialogue Support Strategies
In the dialogue support category, reminders strategy is the most commonly employed strategy, followed by rewards and suggestion. Reminders strategy is the top strategy possibly because it keeps users focused on their intended tasks. For instance, users are usually reminded or notified at specific intervals to meditate, check their heart rate, or log their activities. The suggestion strategy offers personalized tips or recommendations as push notifications (or pop-up messages) that draw users closer to their goals. Majority of the apps that implemented the suggestion made it customizable such that users can enable/disable or change the timing/frequency of the notifications. This improves the users' feeling of agency and sense of control (87, 88), which can increase their motivation.
Rewards strategy is another motivating factor since users tend to intensify their actions if incentives are attached (89). However, offering tangible rewards to people who are already motivated could confuse them about the real motives (90) and benefits of adopting a healthy behavior (91). Social role is the least employed strategy based on our findings and this may reflect users' concern about privacy and trust if they share sensitive information about their mental health issues (such as stress) with conversational/virtual agents or human specialists via apps (92–94). This also mirrors research evidence that patients are generally less willing to share or engage in most personal communication while using mental health apps due to trust and privacy concerns, among other issues (95).
System Credibility Support Strategies
Based on our findings, system credibility persuasive strategies are the second most employed strategies in stress management apps. Our results showed that trustworthiness strategy (39%) is the most implemented strategy followed by real-world feel (38% of the coded apps) and expertise (26% of the coded apps) in the system credibility support category of the PSD framework. From our results, we also found that trustworthiness was operationalized using privacy statements and informing the user about the terms and conditions for handling the collected data, which is in line with the previous research (96, 97) which shows that trustworthiness is an essential factor for increasing user engagement and safety of the personal data in the mHealth apps. In addition, (86) affirms that users using mental health apps are more concerned about their data privacy, information sharing, and data handling transparency. This explains why trustworthiness is the most implemented system credibility strategy in stress management apps.
According to (86), users prefer to use apps that are aesthetically pleasing (surface credibility) with interventions that are clinically validated (expertise and third-party endorsements) for their mental health needs. Prior research also indicates that using strategies from the system credibility category is essential for improving the overall credibility of the mHealth apps (70). In addition, apps implementing trustworthiness, expertise, and authority strategies have greater chances of persuading users to complete their target behavior (98). However, surface credibility and third-party endorsements are the least implemented strategies in the system credibility category, based on our findings. This is a call to action for app designers aiming to motivate behavior change and increase engagement in the area of stress management.
Social Support Strategies
Although socially-driven persuasive strategies are the most frequently employed strategies in health technologies and other online support systems (64, 91, 99), we found that social support strategies are the least implemented persuasive strategies in stress management apps, as well as apps in other mental health domains (55). Most people are silent about their mental health issues possibly because they are afraid of being stigmatized if they openly discuss their health challenges (100). Consequently, they tend to withdraw from social interactions (100). Moreover, previous research has stated that it could be inappropriate to incorporate social comparison and competition in a mental health apps, particularly for stressed users since competition could induce unhealthy stress levels and discourage some people. Additionally, a positive correlation has been found between high levels of perceived competition and other mental health issues such as depression and anxiety (101). Therefore, applying social comparison and competition strategies in stress management apps could negatively impact users' stress levels.
Furthermore, literature shows that there is a relationship between cooperation and stress. According to Yuebing (102), individuals under stress worry about being exploited. Hence, they are less likely to cooperate, with tendencies to have negative expectations about their partners' behavior (102). As a result, stress may obstruct cooperation. However, incorporating social learning, social facilitation, and normative influence strategies in stress management apps could help stressed individuals to decrease the feeling of being alone, isolated, or stigmatized. Evidence shows that forums that provide peer support may foster social inclusion in unexpected and new ways and should be a core element of recovery-oriented mental health policy (103). In addition, peer support is a primary part of helping many people experiencing mental ill-health in their recovery journeys (104).
CPP Strategies
Based on our findings, reciprocity is the most implemented strategy (21 apps), followed by commitment (14 apps) and scarcity (13 apps). This aligns with the research evidence which found reciprocity as the most implemented strategy in emotional and mental health apps (57). According to (105), if people receive something valuable in advance (such as gifts) before completing a task, they are encouraged to perform the target behavior since they feel indebted. Commitment is the second most commonly implemented strategy in emotional and mental health apps based on our findings and in alignment with (57). Employing commitment in stress management apps would motivate users to commit to their daily, weekly, or monthly goals and work consistently toward achieving them.
Comparative Analysis
Table 5 shows the most and least dominant persuasive strategies for app category. Every individual faces a different kind of stress and the level of stress also varies from person to person. Therefore, it is not surprising that personalization is the most dominant in both “Stress Intervention Only” and “Stress Intervention and Monitoring” categories. Self-monitoring is essential for tracking users' stress levels and helps them visualize their progress over time. Some of the apps do not track stress levels directly, but they do track user activity, which is indirectly related to stress levels (e.g., number of meditation sessions completed by the user). This explains why the self-monitoring strategy is most dominant in the “Stress Monitoring Only” category.
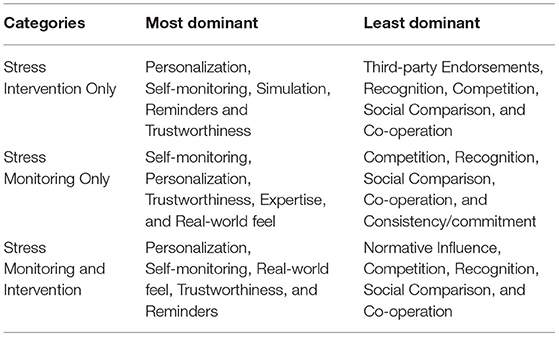
Table 5. Comparative analysis of persuasive strategies across app categories (Strategies are presented in descending order of prevalence or dominance).
Trustworthiness is another important strategy for stress management apps. Users tend to use mHealth apps that clearly specifies how their data will be stored and protected in the app. On the other hand, social support strategies (e.g., social comparison, recognition, competition, co-operation, etc.) are the least dominant, as the users experiencing stress are hesitant and less likely to compete with others in order to improve their stress, and most would like to keep it private to avoid stigmatization.
Furthermore, our findings revealed six (6) strategies (i.e., tailoring, simulation, reduction, similarity, trustworthiness, and surface credibility) implemented in stress management apps but not in other mental health apps. This could be due to several reasons. First, stress management apps usually tailor educational and interactive modules to users based on established various intervention techniques, including mindfulness, meditation, or breathing exercises (106–108). Intervention modules for stress reduction could also be tailored based on user groups such as general military members or combat-injured patients (109). Second, decreasing the complexity and steps users need to perform the target behavior (reduction strategy) could reduce negative emotions that contribute to high-stress levels. Third, surface credibility is essential for stress management apps since organized, efficient, and ads-free content could contribute to stress reduction (110). Fourth, privacy and trust concerns surrounding mental health apps, including stress (111), tend to be a major factor influencing designers' implementation of trustworthiness strategy in stress management apps. Finally, simulation strategy is widely used as a technique for stress relief such that users can see the cause and effect of their behavior. For instance, recent research, informed by Laughter therapy, implemented flower blooms at a certain point based on users' laugh energy (112). Another app encourages users to practice relaxation training that would help reduce their stress when users' stress level is balanced; a tree grows up strong and healthy when users' stress level is balanced or normal (113).
Design Recommendations
In this section, we offer a set of design guidelines based on our review findings.
Provide Personalized Stress Interventions
Everyone experiences varying stress levels at different times; hence, coping intervention can only produce the desired outcome if it fits each target user's current stress level. Hence, designers of stress management apps should leverage sensors data, in addition to self-reports where available, to detect stress levels in real-time using machine learning (ML) models and then offer personalized interventions that relieve the stress detected. Stress interventions can be personalized based on users' preferences through a pre-survey that introduces a list of recommended interventions, in which users can choose the interventions that work in reducing their stress—for example, practicing meditation or getting social support. In addition, users' past preferences can also be fed into ML models to determine the most suitable intervention. As a result, users will find the apps effective for managing their stress on an ongoing basis, thereby boosting user motivation and engagement/adoption in both the short and long term.
Reduce Task Complexity and Provide In-app Support
Most reviewed stress management apps lack in-app support and fail to simplify tasks users are expected to perform. App designers should reduce tasks into simpler steps (reduction) and offer contextual guidance (tunneling) until the tasks are successfully completed to avoid raising the stress levels of their users (114). Simplifying tasks and minimizing user efforts through providing templates for journaling which users can easily fill or change as necessary. Since feeling stressed may affect users' choices, the system should automatically arrange and present interventions based on users' needs/type (tailoring) and support their adoption of the target intervention.
Provide Clear Privacy Policies to Address Data Privacy Concerns
Data privacy and transparency are important factors to ensure the trustworthiness of stress-based apps (96, 97) due to the sensitive nature of the data collected. Users of mental health apps usually have privacy and trust concerns that affect their decision to use such apps (111). To establish the users' trust, designers should provide the app's clear privacy policies and clear information about the data storage. Additionally, they should also provide steps for secure data transmission to third-party entities, how the user's data is stored and utilized, and steps taken to ensure users' anonymity. This information should be presented to the user in concise and plain language, and consent obtained prior to collecting any personal data (trustworthiness).
Create Apps Using Evidence-Based or Clinically Proven Techniques for Handling Stress
To improve system credibility, designers should use evidence-based or clinically-validated stress relief techniques that are proven to be effective for a larger group of audience in the design of their apps. These techniques can be in the form of daily or weekly psychoeducation materials (e.g., stress reduction, mindfulness skills, and well-being enhancement) developed by health professionals or taken from valid sources with proper references included or approved by top health authorities (e.g., World Health Organization, Public Health Agency of Canada, United States Department of Health and Human Services, etc.). Evidence-based contents or interventions delivered through mobile apps have been shown to be effective in reducing stress and improving mental wellbeing (108).
Deliver Stable, Functional, and Professionally Looking Interfaces in the Apps
The usability of stress management apps is crucial for continuous engagement. Research has shown that aesthetically pleasing and stable user interfaces are more likely to be used by the users (86). Therefore, designers should make their apps visually attractive and have a consistent interface in terms of color, layout, and graphics. In addition, designers should ensure that the app's interface is simple, organized, easy to use/understand, and void of ambiguous and unstable functionalities (surface credibility). These practices will ensure that stress management apps are appealing, credible, and motivating to users.
Make Premium Features for Stress Intervention Accessible
Designers should provide a free trial upon user registration to allow them to use the premium features in the app. This can be achieved by offering a free trial for an initial period (e.g., 30 days) or linking the premium features to achievement of behavior change milestones (Scarcity). As a result, users will get the required experience to practice different stress management techniques and encourage them to continue using the app. Moreover, apps designed for stressed individuals should reduce distractions induced through in-app advertisements or ads (110).
Allow Users to Set and Track Their Goals
Designers should provide users with an option to select their daily, weekly, or monthly goals for performing their target behavior, e.g., practicing breathing exercises or journaling their feeling/mood. In addition, designers should provide users with an activity dashboard to view progress and visualize how far they are from their defined goal. Moreover, the app should observe and monitor users' stress levels and recommend a set of specific goals to follow based on users' behavior or preferences. Research has shown that goal-setting, self-monitoring and feedback on users' performance are essential behavior change techniques (115).
Incorporate an Online Community
Designers should include community, forum, or blog features to promote social or peer support as it is essential to overcoming stress (104, 116). Incorporating an online community will enable stressed individuals to get emotional support through empathy and other positive feelings from peers during stressful periods. Besides, users can get help or support from stress reduction techniques, advice, and suggestions shared on such in-app social settings. Therefore, accessing such social support will help users disconnect from stress by learning from other users' experiences and success stories (social learning).
Limitations
This study only targeted apps developed in English languages. Also, the 150 apps analyzed were randomly selected from the pool of stress management apps extracted from both Google Play and App Store. As a result, selected apps were not uniformly distributed into the various app categories (i.e., stress monitoring only, stress intervention only, and stress monitoring and intervention). Therefore, our results may not generalize to all stress management apps but still comprehensive considering the relatively large number of apps analyzed.
Conclusion and Future Work
In this paper, we conducted a comprehensive and comparative review of 150 stress management apps to deconstruct the persuasive strategies employed in each of them and how they were implemented. Specifically, we categorized the apps based on their purpose into three main categories: “stress intervention only,” “stress monitoring only,” and “stress intervention and monitoring.” Next, we utilized the PSD and CPP frameworks to deconstruct the persuasive or behavior change strategies utilized in each app. Our results revealed that primary task support strategies (especially personalization and self-monitoring) of the PSD model are the most commonly employed, followed by system credibility support (such as trustworthiness and real-world feel), dialogue support strategies (e.g., reminders and rewards), and the CPP strategies (e.g., reciprocity and commitment/consistency). Social support strategies are the least employed overall. We also compared stress management apps with those targeting other mental health apps to uncover further insights. Our findings revealed six (6) persuasive strategies that were solely implemented in stress management apps: tailoring, simulation, reduction, similarity, trustworthiness, and surface credibility. Finally, we offered a set of design recommendations that would inform effective, usable, engaging, and motivating apps for managing stress.
As part of future work, we will explore the strategies employed in stress management apps using additional frameworks such as the Theory of Reasoned Action/Planned Behavior and Health Belief Model. We will also examine the effectiveness of the apps based on user reviews using natural language processing and machine learning techniques.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
MA designed the study, coded apps, analyzed the data and wrote parts of the results, discussion, and design recommendation sections. DM reviewed and coded the app, generated figures, wrote the methodology, and parts in the results section. OO validated the coding sheet of the apps, performed the statistical analysis, contributed to writing the introduction, and related work sections. NB reviewed and edited the manuscripts and contributed to writing the design recommendation section. RO guided the team through different stages of the research, reviewed and edited the manuscripts, and contributed to the writing of the discussion section. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program. We acknowledge the support of the Natural Sciences and Engineering Research Council of Canada (NSERC) through the Discovery Grant.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.777567/full#supplementary-material
References
1. Larzelere MM, Jones GN. Stress and health. Primary Care. (2008) 35:839–56. doi: 10.1016/j.pop.2008.07.011
2. The National Institute of Mental Health (NIMH). The National Institute of Mental Health (NIMH). 5 Things You Should Know About Stress. Malibu, CA (2020).
3. American Psychological Association. Stress. (2020). Available online at: https://www.apa.org/topics/stress/
4. Wirtz PH, Känel RV. Psychological stress, inflammation, and coronary heart disease. Curr Cardiol Rep. (2017) 19:1–10. doi: 10.1007/s11886-017-0919-x
5. Hackett RA, Steptoe A. Type 2 diabetes mellitus and psychological stress — a modifiable risk factor. Nat Rev Endocrinol. (2017) 13:547–60. doi: 10.1038/nrendo.2017.64
6. Albert MA, Durazo EM, Slopen N, Zaslavsky AM, Buring JE, Silva T, et al. Cumulative psychological stress and cardiovascular disease risk in middle aged and older women: rationale, design, and baseline characteristics. Am Heart J. (2017) 192:1–12. doi: 10.1016/j.ahj.2017.06.012
7. Gianaros PJ, Jennings JR. Host in the machine: a neurobiological perspective on psychological stress and cardiovascular disease. Am Psychol. (2018) 73:1031–44. doi: 10.1037/amp0000232
8. Ginty AT, Kraynak TE, Fisher JP, Gianaros PJ. Cardiovascular and autonomic reactivity to psychological stress: neurophysiological substrates and links to cardiovascular disease. Auton Neurosci. (2017) 207:2–9. doi: 10.1016/j.autneu.2017.03.003
9. Kivimäki M, Steptoe A. Effects of stress on the development and progression of cardiovascular disease. Nat Rev Cardiol. (2017) 15:215–29. doi: 10.1038/nrcardio.2017.189
10. Loo KFEVD, Gelder MHJV, Roukema J, Roeleveld N, Merkus PJFM, Verhaak CM. Prenatal maternal psychological stress and childhood asthma and wheezing: a meta-analysis. Europ Respir J. (2016) 47:133–46. doi: 10.1183/13993003.00299-2015
11. Kelly RR, McDonald LT, Jensen NR, Sidles SJ, LaRue AC. Impacts of psychological stress on osteoporosis: clinical implications and treatment interactions. Front Psychiatry. (2019) 10:200. doi: 10.3389/fpsyt.2019.00200
12. Qu F, Wu Y, Zhu YH, Barry J, Ding T, Baio G, et al. The association between psychological stress and miscarriage: a systematic review and meta-analysis. Sci Rep. (2017) 7:1731. doi: 10.1038/s41598-017-01792-3
13. Rafique N, Al-Sheikh MH. Prevalence of menstrual problems and their association with psychological stress in young female students studying health sciences. Saudi Med J. (2018) 39:67–73. doi: 10.15537/smj.2018.1.21438
14. Jović A, Marinović B, Kostović K, Ceović R, Basta-Juzbašić A, Mokos ZB. The impact of psychological stress on acne. Acta Dermatovenerol Croatica. (2017) 25:133.
15. Tomiyama AJ. Stress and obesity. Ann Rev Psychol. (2019) 70:703–18. doi: 10.1146/annurev-psych-010418-102936
16. Song H, Fang F, Tomasson G, Arnberg FK, Mataix-Cols D, Cruz LFDL, et al. Association of stress-related disorders with subsequent autoimmune disease. JAMA. (2018) 319:2388–400. doi: 10.1001/jama.2018.7028
17. Caruso A, Nicoletti F, Mango D, Saidi A, Orlando R, Scaccianoce S. Stress as risk factor for Alzheimer's disease. Pharmacol Res. (2018) 132:130–4. doi: 10.1016/j.phrs.2018.04.017
18. Hollifield M, Warner T, Krakow B, Westermeyer J. Mental health effects of stress over the life span of refugees. J Clin Med. (2018) 7:25. doi: 10.3390/jcm7020025
19. Kuiper NA, Olinger LJ, Lyons LM. Global perceived stress level as a moderator of the relationship between negative life events and depression. J Human Stress. (1986) 12:149–53. doi: 10.1080/0097840X.1986.9936781
20. Pascoe MC, Hetrick SE, Parker AG. The impact of stress on students in secondary school and higher education. Int J Adolesc Youth. (2020) 25:104–12. doi: 10.1080/02673843.2019.1596823
21. Schönfeld P, Brailovskaia J, Bieda A, Zhang XC, Margraf J. The effects of daily stress on positive and negative mental health: mediation through self-efficacy. Int J Clin Health Psychol. (2016) 16:1–10. doi: 10.1016/j.ijchp.2015.08.005
22. Shankar NL, Park CL. Effects of stress on students' physical and mental health and academic success. Int J Schl Educ Psychol. (2016) 4:5–9. doi: 10.1080/21683603.2016.1130532
23. Bergh BRHVd, Heuvel MIvd, Lahti M, Braeken M, Rooij SRd, Entringer S, et al. Prenatal developmental origins of behavior and mental health: the influence of maternal stress in pregnancy. Neurosci Biobehav Rev. (2017) 117:26–64. doi: 10.1016/j.neubiorev.2017.07.003
24. Breedvelt JJF, Amanvermez Y, Harrer M, Karyotaki E, Gilbody S, Bockting CLH, et al. The effects of meditation, yoga, and mindfulness on depression, anxiety, and stress in tertiary education students: a meta-analysis. Front Psychiatry. (2019) 10:193. doi: 10.3389/fpsyt.2019.00193
25. Chiesa A, Serretti A. Mindfulness-based stress reduction for stress management in healthy people: a review and meta-analysis. J Alter Complement Med. (2009) 15:593–600. doi: 10.1089/acm.2008.0495
26. Chin B, Slutsky J, Raye J, Creswell JD. Mindfulness training reduces stress at work: a randomized controlled trial. Mindfulness. (2019) 10:627–38. doi: 10.1007/s12671-018-1022-0
27. Eby LT, Allen TD, Conley KM, Williamson RL, Henderson TG, Mancini VS. Mindfulness-based training interventions for employees: a qualitative review of the literature. Human Resour Manage Rev. (2019) 29:156–78. doi: 10.1016/j.hrmr.2017.03.004
28. Fortney L, Mssw CL, Ma LZ, Rakel D, Zgierska A. Primary care for primary care clinicians : a pilot study of an abbreviated mindfulness intervention on measures of job satisfaction, quality of life, and compassion. Ann Fam Med. (2013) 11:412–20. doi: 10.1370/afm.1511
29. Hazlett-Stevens H, Singer J, Chong A. Mindfulness-based stress reduction and mindfulness-based cognitive therapy with older adults: a qualitative review of randomized controlled outcome research. Clin Gerontol. (2019) 42:347–58. doi: 10.1080/07317115.2018.1518282
30. Hwang WC, Chan CP. Compassionate meditation to heal from race-related stress: a pilot study with Asian Americans. Am J Orthopsychiatry. (2019) 89:482–92. doi: 10.1037/ort0000372
31. Premnath A, Sivan S, Velayudhan R, MS S, TM R. Effect of a stress reduction programme on academic stress and coping skills of first year medical students. Kerala J Psychiatry. (2020) 33:27–33. doi: 10.30834/KJP.33.1.2020.187
32. Wetherell JL, Hershey T, Hickman S, Tate SR, Dixon D, Bower ES, et al. Mindfulness-based stress reduction for older adults with stress disorders and neurocognitive difficulties: a randomized controlled trial. J Clin Psychiatry. (2017) 78:e736–43. doi: 10.4088/JCP.16m10947
33. Witte Md, Spruit A, Hooren Sv, Moonen X, Stams GJ. Effects of music interventions on stress-related outcomes: a systematic review and two meta-analyses. Health Psychol Rev. (2019) 21:1–31. doi: 10.1080/17437199.2020.1846580
34. Corazon SS, Sidenius U, Poulsen DV, Gramkow MC, Stigsdotter UK. Psycho-physiological stress recovery in outdoor nature-based interventions: a systematic review of the past eight years of research. Int J Environ Res Public Health. (2019) 16:10. doi: 10.3390/ijerph16101711
35. Podszus R. Nature Relatedness as a Facilitator to Utilizing the Natural World as a Coping Strategy to Reduce Stress. (2017). Retrieved from: https://research.libraries.wsu.edu:8443/xmlui/handle/2376/11903 (accessed June 27, 2020)
36. Beanlands H, McCay E, Fredericks S, Newman K, Rose D, Mina ES, et al. Decreasing stress and supporting emotional well-being among senior nursing students: a pilot test of an evidence-based intervention. Nurse Educ Today. (2019) 76:222–7. doi: 10.1016/j.nedt.2019.02.009
37. Gardiner M, Kearns H, Tiggemann M. Effectiveness of cognitive behavioural coaching in improving the well-being and retention of rural general practitioners. Austr J Rural Health. (2013) 21:183–89. doi: 10.1111/ajr.12033
38. Sood A, Sharma V, Schroeder DR, Gorman B. Stress Management and Resiliency Training (SMART) program among department of radiology faculty: a pilot randomized clinical trial. Explore. (2014) 10:358–63. doi: 10.1016/j.explore.2014.08.002
39. Park JM, Choi IR. The effect of K-MBSR program on stress, stress coping style, depression, anger and sleep of middle aged women. J Korean Acad Nurs. (2016) 46:194–206. doi: 10.4040/jkan.2016.46.2.194
40. Ro KEI, Tyssen R, Hoffart A, Sexton H, Aasland OG, Gude T. A three-year cohort study of the relationships between coping, job stress and burnout after a counselling intervention for help-seeking physicians. BMC Public Health. (2010) 10:213. doi: 10.1186/1471-2458-10-213
41. Mccue JD, Sachs CL. A stress management workshop improves residents' coping skills. Arch Intern Med. (1991) 151:12273–7. doi: 10.1001/archinte.1991.00400110117023
42. O'Dea S. Smartphone Users Worldwide. (2020). Retrieved from: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (accessed April 21, 2020)
43. Osman HA, Dong H, Saddik AE. Ubiquitous biofeedback serious game for stress management. IEEE Access. (2016) 4:1274–86. doi: 10.1109/ACCESS.2016.2548980
44. Reimer U, Maier E, Ulmer T. SmartCoping: A mobile solution for recognizing stress coping with it. In: Wickramasinghe N, Bodendorf F, editors. Healthcare Delivery in the Information Age. Cham: Springer (2020). p. 119–43. doi: 10.1007/978-3-030-17347-0_6
45. Plews DJ, Scott B, Altini M, Wood M, Kilding AE, Laursen PB. Comparison of heart-rate-variability recording with smartphone photoplethysmography, polar H7 chest strap, and electrocardiography. Int J Sports Physiol Perform. (2017) 12:1324–8. doi: 10.1123/ijspp.2016-0668
46. Wang Y, Fischer N, Bry F. Pervasive persuasion for stress self-regulation. 2019. In: IEEE International Conference on Pervasive Computing and Communications Workshops, PerCom Workshops. Kyoto (2019). p. 724–30. doi: 10.1109/PERCOMW.2019.8730850
47. Visuri A, Poguntke R, Kuosmanen E. Proposing design recommendations for an intelligent recommender system logging stress. In: ACM International Conference Proceeding Series. New York, NY (2018). p. 411–7. doi: 10.1145/3282894.3289733
48. Dillon A, Kelly M, Robertson IH, Robertson DA. Smartphone applications utilizing biofeedback can aid stress reduction. Front Psychol. (2016) 7:832. doi: 10.3389/fpsyg.2016.00832
49. Harris J, Vance S, Fernandes O, Parnandi A, Gutierrez-Osuna R. Sonic respiration : controlling respiration rate through auditory biofeedback. In: Proceedings of the Extended Abstracts of the 32nd Annual ACM Conference on Human Factors in Computing Systems (CHI EA'14). Toronto, ON (2014). p. 2383–8. doi: 10.1145/2559206.2581233
50. Jonckheere JD, Ibarissene I, Flocteil M, Logier R. A smartphone based cardiac coherence biofeedback system. In: 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC 2014. Chicago, IL (2014). p. 4791–4. doi: 10.1109/EMBC.2014.6944695
51. Martin JC, Lescanff C, Rosset S, Walker M, Whittaker S. How to personalize conversational coaches for stress management? In: UbiComp/ISWC 2018 - Adjunct Proceedings of the 2018. ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2018. ACM International Symposium on Wearable Computers. New York, NY (2018). p. 718–21. doi: 10.1145/3267305.3267698
52. Apolinário-Hagen J, Hennemann S, Fritsche L, Drüge M, Breil B. Determinant factors of public acceptance of stress management apps: survey study. J Med Internet Res. (2019) 21:11. doi: 10.2196/preprints.15373
53. Ly KH, Asplund K, Andersson G. Stress management for middle managers via an acceptance and commitment-based smartphone application: a randomized controlled trial. Internet Interv. (2014) 1:95–101. doi: 10.1016/j.invent.2014.06.003
54. Weber S, Lorenz C, Hemmings N. Improving stress and positive mental health at work via an app-based intervention: a large-scale multi-center randomized control trial. Front Psychol. (2019) 10:2745. doi: 10.3389/fpsyg.2019.02745
55. Alqahtani F, Khalifah GA, Oyebode O, Orji R. Apps for mental health : an evaluation of behavior change strategies and recommendations for future development. Front Artif Intell. (2019) 2:30. doi: 10.3389/frai.2019.00030
56. Nurcan A, Duygu F-C. Use of Persuasion Strategies in Mobile Health Applications. Cham: Springer (2018).
57. Oyebode O, Ndulue C, Alhasani M, Orji R. Persuasive mobile apps for health and wellness : a comparative systematic review. In: International Conference on Persuasive Technology. Aalborg (2020). p. 1–12. doi: 10.1007/978-3-030-45712-9_13
58. Oinas-Kukkonen H, Harjumaa M. Persuasive systems design: key issues, process model, and system features. Commun Assoc Inform Syst. (2009) 24:96. doi: 10.17705/1CAIS.02428
59. Cialdini RB. Harnessing the science of persuasion. Harv Bus Rev. (2001) 79:72–81. doi: 10.1038/scientificamerican0201-76
60. Fogg BJ, Fogg GE. Persuasive Technology: Using Computers to Change What We Think Do. San Francisco, CA: Morgan Kaufmann (2003). doi: 10.1016/B978-155860643-2/50011-1
61. Oinas-Kukkonen H, Harjumaa M. Towards deeper understanding of persuasion in software and information systems. In: Proceedings of the 1st International Conference on Advances in Computer-Human Interaction, ACHI 2008. Sainte-Luce (2008). p. 200–5. doi: 10.1109/ACHI.2008.31
62. Fogg B. A behavior model for persuasive design. In: Proceedings of the 4th International Conference on Persuasive Technology. (2009). p. 7. doi: 10.1145/1541948.1541999
63. Langrial S, Lehto T, Oinas-Kukkonen H, Harjumaa M, Karppinen P. Native mobile applications for personal well- being: a persuasive systems design evaluation. In: PACIS 2012 Proceedings. (2012). Retrieved from: http://aisel.aisnet.org/pacis2012 (accessed March 22, 2020).
64. Orji R, Moffatt K. Persuasive technology for health and wellness: State-of-the-art and emerging trends. Health Informatics J. (2018) 24:66–91. doi: 10.1177/1460458216650979
65. Hamari J, Koivisto J, Pakkanen T. Do persuasive technologies persuade? - A review of empirical studies. In: International Conference on Persuasive Technology (PERSUASIVE 2014). Padua (2014). p. 118–36. doi: 10.1007/978-3-319-07127-5_11
66. Chang TR, Kaasinen E, Kaipainen K. Persuasive design in mobile applications for mental well-being: multidisciplinary expert review. In: International Conference on Wireless Mobile Communication and Healthcare. Washington, DC (2013). p. 154–62. doi: 10.1007/978-3-642-37893-5_18
67. Geuens J, Swinnen TW, Westhovens R, Vlam Kd, Geurts L, Abeele VV. A review of persuasive principles in mobile apps for chronic arthritis patients: opportunities for improvement. JMIR mHealth uHealth. (2016) 4:e118. doi: 10.2196/mhealth.6286
68. Fadhil A, Wang Y. Health Behaviour Change Techniques in Diabetes Management Applications: A Systematic Review. (2019). Retrieved from: http://arxiv.org/abs/1904.09884 (accessed June 13, 2021).
69. Win KT, Mullan J, Howard S, Oinas-Kukkonen H. Persuasive Systems Design features in Promoting Medication Management for consumers. In: Proceedings of the 50th Hawaii International Conference on System Sciences. Waikoloa Village, HI (2017). p. 3326–35. doi: 10.24251/HICSS.2017.403
70. Matthews J, Win KT, Oinas-Kukkonen H, Freeman M. Persuasive technology in mobile applications promoting physical activity: a systematic review. J Med Syst. (2016) 40:1–13. doi: 10.1007/s10916-015-0425-x
71. Almutari N, Orji R. How effective are social influence strategies in persuasive apps for promoting physical activity? A systematic review. In: ACM UMAP 2019. Adjunct - Adjunct Publication of the 27th Conference on User Modeling, Adaptation and Personalization. Larnaca (2019). p. 167–72. doi: 10.1145/3314183.3323855
72. Lombard M, Snyder-Duch J, Bracken CC. Content analysis in mass communication: assessment and reporting of intercoder reliability. Hum Commun Res. (2002) 28:587–604. doi: 10.1111/j.1468-2958.2002.tb00826.x
73. Berrouiguet S, Perez-Rodriguez MM, Larsen M, Baca-García E, Courtet P, Oquendo M. From eHealth to iHealth: transitiaon to participatory and personalized medicine in mental health. J Med Internet Res. (2018) 20:e2. doi: 10.2196/jmir.7412
74. Snowdon AW, Alessi C, Bassi H, DeForge RT, Schnarr K. Enhancing patient experience through personalization of health services. Healthcare Manage Forum. (2015) 28:5:182–5. doi: 10.1177/0840470415588656
75. Swan M. Health 2050: the realization of personalized medicine through Crowdsourcing, the Quantified Self, and the Participatory Biocitizen. J Personal Med. (2012) 2:93–118. doi: 10.3390/jpm2030093
76. Iacoviello BM, Steinerman JR, Klein DB, Silver TL, Berger AG, Luo SX, et al. Clickotine, a personalized smartphone app for smoking cessation: initial evaluation. JMIR mHealth uHealth. (2017) 5:e56. doi: 10.2196/mhealth.7226
77. Martin CK, Gilmore LA, Apolzan JW, Myers CA, Thomas DM, Redman LM. Smartloss: a personalized mobile health intervention for weight management and health promotion. JMIR mHealth uHealth. (2016) 4:e18. doi: 10.2196/mhealth.5027
78. Rabbi M, Pfammatter A, Zhang M, Spring B, Choudhury T. Automated personalized feedback for physical activity and dietary behavior change with mobile phones: a randomized controlled trial on adults. JMIR mHealth uHealth. (2015) 3:e42. doi: 10.2196/mhealth.4160
79. Zhou M, Fukuoka Y, Mintz Y, Goldberg K, Kaminsky P, Flowers E, et al. Evaluating machine learning–based automated personalized daily step goals delivered through a mobile phone app: Randomized controlled trial. JMIR mHealth uHealth. (2018) 6:e28. doi: 10.2196/mhealth.9117
80. Paredes P, Gilad-Bachrach R, Czerwinski M, Roseway A, Rowan K, Hernandez J. PopTherapy: coping with stress through pop-culture. In: Proceedings - PERVASIVEHEALTH 2014:8th International Conference on Pervasive Computing Technologies for Healthcare. (2014). p. 109–17. doi: 10.4108/icst.pervasivehealth.2014.255070
81. Rickard N, Arjmand H-A, Bakker D, Seabrook E. Development of a mobile phone app to support self-monitoring of emotional well-being: a mental health digital innovation. JMIR Mental Health. (2016) 3:e49. doi: 10.2196/mental.6202
82. Kauer SD, Reid SC, Crooke AHD, Khor A, Hearps SJC, Jorm AF, et al. Self-monitoring using mobile phones in the early stages of adolescent depression: randomized controlled trial. J Med Internet Res. (2012) 14:1–17. doi: 10.2196/jmir.1858
83. Torous J, Friedman R, Keshvan M. Smartphone ownership and interest in mobile applications to monitor symptoms of mental health conditions. J Med Internet Res. (2014) 16:1–8. doi: 10.2196/mhealth.2994
84. Yu B, Hu J, Funk M, Feijs L. DeLight: biofeedback through ambient light for stress intervention and relaxation assistance. Personal Ubiquitous Comput. (2018) 22:787–805. doi: 10.1007/s00779-018-1141-6
85. Alqahtani F, Orji R. Usability issues in mental health applications. In: Adjunct Publication of the 27th Conference on User Modeling, Adaptation and Personalization - UMAP'19 Adjunct, Larnaca (2019). p. 343–8. doi: 10.1145/3314183.3323676
86. Oyebode O, Alqahtani F, Orji R. Using machine learning and thematic analysis methods to evaluate mental health apps based on user reviews. IEEE Access. (2020) 8:111141–58. doi: 10.1109/ACCESS.2020.3002176
87. Marathe S, Sundar SS. What drives customization? Control or identity? In: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems - CHI'11. Vancouver, BC (2011). p. 781–90. doi: 10.1145/1978942.1979056
88. Sundar SS, Oh J, Bellur S, Jia H, Kim HS. Interactivity as self-expression: a field experiment with customization and blogging. In: Conference on Human Factors in Computing Systems - Proceedings. Montreal, QC (2012). p. 395–404. doi: 10.1145/2207676.2207731
89. Lemola S, Gkiouleka A, Read B, Realo A, Walasek L, Tang NKY, et al. Can a ‘rewards-for-exercise app' increase physical activity, subjective well-being and sleep quality? An open-label single-arm trial among university staff with low to moderate physical activity levels. BMC Public Health. (2021) 21:782. doi: 10.1186/s12889-021-10794-w
90. Cherubini M, Villalobos-Zuñiga G, Boldi M-O, Bonazzi R. The unexpected downside of paying or sending messages to people to make them walk. ACM Trans Computer-Human Interact (TOCHI). (2020) 27:1–44. doi: 10.1145/3365665
91. Orji R, Vassileva J, Mandryk RL. Modeling the efficacy of persuasive strategies for different gamer types in serious games for health. User Model User-adapt Interact. (2014) 24:453–98. doi: 10.1007/s11257-014-9149-8
92. Kretzschmar K, Tyroll H, Pavarini G, Manzini A, Singh I, Group NYPA. Can your phone be your therapist? Young people's ethical perspectives on the use of fully automated conversational agents (Chatbots) in mental health support. Biomed Inform Insights. (2019) 11:1178222619829083. doi: 10.1177/1178222619829083
93. Liao Y, He J. Racial mirroring effects on human-agent interaction in psychotherapeutic conversations. In: International Conference on Intelligent User Interfaces, Proceedings IUI. Cagliari (2020). p. 430–42. doi: 10.1145/3377325.3377488
94. Martinez-Martin N, Kreitmair K. Ethical issues for direct-to-consumer digital psychotherapy apps: addressing accountability, data protection, and consent. JMIR Ment Health. (2018) 5:e9423. doi: 10.2196/mental.9423
95. Torous J, Nicholas J, Larsen ME, Firth J, Christensen H. Clinical review of user engagement with mental health smartphone apps: evidence, theory and improvements. Evid Based Ment Health. (2018) 21:116–9. doi: 10.1136/eb-2018-102891
96. Chang TR, Kaasinen E, Kaipainen K. What influences users' decisions to take apps into use? A framework for evaluating persuasive and engaging design in mobile apps for well-being. In: Proceedings of the 11th International Conference on Mobile and Ubiquitous Multimedia - MUM. Ulm (2012). p. 1–10. doi: 10.1145/2406367.2406370
97. Chen T-W, Sundar SS. “This App Would Like to Use Your Current Location to Better Serve You”: importance of user assent and system transparency in personalized mobile services. In: Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems. Montreal, QC (2018). p. 1–13. doi: 10.1145/3173574.3174111
98. Fogg BJ. Computers as persuasive social actors. In: Drew J, editor. Persuasive Technology. Morgan Kaufmann Publishers (2003). p. 89–20. doi: 10.1016/B978-155860643-2/50007-X
99. Lehto T, Oinas-Kukkonen H. Persuasive features in web-based alcohol and smoking interventions: a systematic review of the literature. J Med Internet Res. (2011) 13:e46. doi: 10.2196/jmir.1559
100. Leff J, Richard W. Social Inclusion of People with Mental Illnesstle. London: Cambridge University Press (2006). doi: 10.1017/CBO9780511543937
101. Dqg G, Ri L, Dgglwlrqdo RU, Derxw L, Duwlfoh W, Posselt JR, et al. Competition, Anxiety, and Depression in the College Classroom : Variations by Student Identity and Field of Study. Baltimore, MD (2016).
103. Smith-merry J, Goggin G, Campbell A, Mckenzie K, Ridout B. Social connection and online engagement : insights from interviews with users of a mental health online forum. JMIR Ment Health. (2019) 6:e11084. doi: 10.2196/11084
104. Balani S, Choudhury MD. Detecting and characterizing mental health related self-disclosure in social media. In: CHI EA '15: Proceedings of the 33rd Annual ACM Conference Extended Abstracts on Human Factors in Computing Systems. New York, NY (2015). p. 1373–8. doi: 10.1145/2702613.2732733
105. Gamberini L, Petrucci G, Spoto A, Anna S. Embedded persuasive strategies to obtain visitors' data: comparing reward and reciprocity in an amateur, knowledge-based website. In: International Conference on Persuasive Technology. Stanford (2007). p. 4744. doi: 10.1007/978-3-540-77006-0_24
106. Allexandre D, Bernstein AM, Walker E, Hunter J, Roizen MF, Morledge TJ. A web-based mindfulness stress management program in a corporate call center. J Occup Environ Med. (2016) 58:254–64. doi: 10.1097/JOM.0000000000000680
107. Bostock S, Crosswell AD, Prather AA, Steptoe A. Mindfulness on-the-go: effects of a mindfulness meditation app on work stress and well-being. J Occup Health Psychol. (2019) 24:127–38. doi: 10.1037/ocp0000118
108. Fuller-Tyszkiewicz M, Richardson B, Little K, Teague S, Hartley-Clark L, Capic T, et al. Efficacy of a smartphone app intervention for reducing caregiver stress: Randomized controlled trial. JMIR Mental Health. (2020) 7:e17541. doi: 10.2196/17541
109. Williams RA, Gatien G, Hagerty B. Design element alternatives for stress-management intervention websites. Nurs Outlook. (2011) 59:5:286–291.e3. doi: 10.1016/j.outlook.2011.03.009
111. Proudfoot J, Parker G, Pavlovic DH, Manicavasagar V, Adler E, Whitton A. Community attitudes to the appropriation of mobile phones for monitoring and managing depression, anxiety, and stress. J Med Internet Res. (2010) 12:5:1–13. doi: 10.2196/jmir.1475
112. Deshpande G, Chanda S. Laughter as a controller in a stress buster game. PervasiveHealth. (2020). p. 316–24. doi: 10.1145/3421937.3421984
113. Yu B, Funk M, Hu J, Feijs L. StressTree: a Metaphorical Visualization for Biofeedback- assisted Stress Management Bin. Edinburgh: DIS (2017).
114. Jeronimus BF, Laceulle OM. Frustration. In: Virgil Zeigler-Hill Todd K, Shackelford, editor. Encyclopedia of Personality Individual Differences (1st ed.). New York, NY: Springer (2017). p. 1–8. doi: 10.1007/978-3-319-28099-8_815-1
115. Gardner B, Wardle J, Poston L, Croker H. Changing diet and physical activity to reduce gestational weight gain: a meta-analysis. Obesity Rev. (2011) 12:12–4. doi: 10.1111/j.1467-789X.2011.00884.x
Keywords: stress management, persuasive technology, persuasive strategies, systematic review, design recommendations, mobile health apps, mental health
Citation: Alhasani M, Mulchandani D, Oyebode O, Baghaei N and Orji R (2022) A Systematic and Comparative Review of Behavior Change Strategies in Stress Management Apps: Opportunities for Improvement. Front. Public Health 10:777567. doi: 10.3389/fpubh.2022.777567
Received: 17 November 2021; Accepted: 03 January 2022;
Published: 24 February 2022.
Edited by:
Khin Wee Lai, University of Malaya, MalaysiaReviewed by:
Yan Chai Hum, Tunku Abdul Rahman University, MalaysiaDeborah Richards, Macquarie University, Australia
Copyright © 2022 Alhasani, Mulchandani, Oyebode, Baghaei and Orji. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mona Alhasani, bW9uYS5hbGhhc2FuaUBkYWwuY2E=