 Delia Lilian Martínez Rodríguez1,2Tonatiuh González Vázquez3*Margarita Márquez Serrano3Mary de Groot4
Delia Lilian Martínez Rodríguez1,2Tonatiuh González Vázquez3*Margarita Márquez Serrano3Mary de Groot4 Alicia Fernandez5
Alicia Fernandez5 Ines Gonzalez Casanova6,7*
Ines Gonzalez Casanova6,7*- 1School of Public Health of Mexico, National Institute of Public Health, Cuernavaca, Mexico
- 2Oaxaca Health Services, Oaxaca, Mexico
- 3Center for Health Systems Research, National Institute of Public Health, Cuernavaca, Mexico
- 4Indiana University School of Medicine, Indianapolis, IN, United States
- 5Department of Medicine, San Francisco School of Medicine, University of California, San Francisco, San Francisco, CA, United States
- 6Department of Applied Health Science, Indiana University Bloomington School of Public Health, Bloomington, IN, United States
- 7Hubert Department of Global Health, School of Public Health, Emory University, Atlanta, GA, United States
Background: Mexican immigrants in the United States face mental health challenges, disparities, and limited access to healthcare; however, mental health promotion efforts specifically targeting this population have been insufficient. The objective of this study was to develop and test a mental health promotion intervention based on protective mental health factors and coping strategies for Mexican immigrants recruited through a free, consulate-based program in Atlanta.
Material and Methods: Working with the Ventanilla de Salud program, we conducted a longitudinal study in three phases: formative research and design, pre-intervention assessment and post-implementation evaluation. The intervention was designed based on the health promotion model and interviews with stakeholders. Qualitative information was collected by semi-structured interviews with participants before and after the intervention. Quantitative outcomes were knowledge about protective factors and coping mechanisms, and psychosocial distress. Differences were assessed using the Wilcoxon non-parametrical test. Intent-to-treat analysis was conducted with all participants who signed the informed consent (carrying last observation forward), and a complete case analysis was conducted with those who attended at least 70% of the sessions and completed the post- implementation evaluation.
Results: Twenty-five participants were enrolled in the intervention. Mean age was 38 years, and the majority were women. Only nine participants attended at least 70% of the sessions and completed the final evaluation. Men, those who did not complete high school, and workers in service or construction jobs were more likely to drop out. Knowledge about protective factors [pre- vs. post-intervention median (inter-quartile range) = 111 (100, 120) vs. 115 (100, 124)] and coping mechanisms [96 (85, 104) vs. 99 (90, 110)], as well as psychosocial distress [3 (2, 3) vs. 2 (2, 3)] improved after the intervention in both intent-to treat and complete case analyses (p < 0.05). Qualitative results also support improvements in targeted protective factors.
Discussion: The intervention was successful in improving psychological distress among Mexican immigrants. These results support the implementation of evidence-based mental health promotion interventions among Mexican immigrants via free and familiar programs. A limitation was the high attrition; future studies should explore approaches to improve retention in this population.
Introduction
Mexicans are the second largest migrant group in the world and the largest immigrant group in the United States, where there were ~12.3 million in 2019 (1). This population faces migration-related mental health challenges, socioeconomic disparities, and limited access to healthcare (2). It is estimated that, in 2019, 5.6 million Mexican immigrants in the US were undocumented, 20% lived in poverty and ~38% did not have access to health insurance (3). This makes linking Mexican immigrants to preventive services or healthcare very challenging, and often results in an accelerated deterioration of the health and wellbeing of this population, which translates into human and economic losses.
Latin American immigrants, including Mexicans, are at high risk of psychological distress and mental illness. A study of mental health among recently arrived Latino immigrants found a prevalence of depression of 26%—three times that of the US population (4). Similarly, migration-related loss and distress were present in all participants in a recent study of undocumented immigrants from Mexico (5). A political climate in the US that emphasized prosecution of undocumented immigrants, fear of being deported, language barriers, and socioeconomic challenges also has impacted the mental health of recent Mexican immigrants. Depression, anxiety, stress, addictions, gender violence, acculturative stress, and Immigrant Syndrome of Chronic and Multiple Stress (also known as Ulises Syndrome) have all been associated with the process of migration (6–8).
Interventions that support the development of coping strategies have been successful in improving mental health and preventing depression and anxiety symptoms in minoritized populations (9, 10). Coping strategies have been defined as group or individual decisions that support adaptation, managing new situations, problem solving, and emotional regulation when dealing with loss or stress. These strategies are the foundations for protective factors including adaptability, social support, and healthy habits (11). Mental health promotion interventions based on coping strategies could be especially important for Mexican immigrants; however, reaching this population can be challenging, and the lack of culturally tailored interventions has made addressing mental health risk factors in this group particularly difficult. Perhaps because of this, there are limited examples in the literature of mental health promotion interventions for Mexican immigrants in the United States (12–15). Most of these efforts have focused on screening and referrals rather than on education or training in mental health coping skills. In this study, we took advantage of a Ventanilla de Salud (VDS) which allowed us to reach Mexican immigrants through a free and familiar program, and design to design and test an evidence-based intervention with the potential to be scaled up through the VDS program.
The VDS program is a health promotion initiative offered through the fifty General Consulates of Mexico in the United States. A very large program, estimated to interact with over one million immigrants per year (16), it plays an important role providing preventive services and linkage to healthcare for Mexican immigrants and could provide an opportunity to address the gap in mental health promotion services among immigrants. Accordingly, as part of a thesis project (17), we developed a mental health promotion intervention based on coping strategies and protective factors and pilot-tested it among Mexican immigrants recruited through the VDS program in Atlanta, which provides preventive services and health education to Mexican immigrants in the Southeast of the United States.
Methods
Overview and Theoretical Framework
We conducted a longitudinal study in three phases: formative research and design, pre-intervention assessment and post implementation evaluation. We used a mixed methods approach based on the health promotion model that conceptualizes health as a positive state and aims to improve individuals' wellbeing. This model focuses on individual experiences, behavior-related cognitions and affect, and behavioral outcomes (18). Quantitative and qualitative information was collected in these domains.
For the development of the intervention, we followed the World Health Organization's recommendations for mental health promotion that identifies protective and risk factors (19). Protective factors of mental health refer to conditions that improve people's resilience to risk factors and disorders. They have been defined as those factors that modify, ameliorate, or alter a person's response to some environmental hazard that predisposes to a maladaptive outcome. Risk factors are associated with an increased probability of onset, greater severity and longer duration of major mental health problems (20, 21). In this case, we considered social support networks, adaptability, positive mental health habits, and coping mechanisms, including emotional regulation and stress management when faced with problems, as target protective factors for the intervention.
The educational sessions of the intervention were based on emotional education, which has been previously applied with adults for health purposes (22, 23) and is defined as an educational process, continuous and permanent, whose objective is to promote emotional development as a complement to cognitive development, for the development of a holistic personality. To do this, emotional education promotes the development of knowledge and skills about emotions in order to enable the individual to better face the challenges that arise in daily life (24). Objectives of emotional education are to acquire a better knowledge of one's own emotions, identify the emotions of others, develop the ability to regulate one's own emotions, prevent the harmful effects of negative emotions, develop the ability to generate positive emotions and the ability to positively relate emotionally with others (25).
Setting
The General Consulate of Mexico in Atlanta serves primarily Mexicans living in the states of Georgia, Alabama, and Tennessee. Within this consulate, the VDS Atlanta offers preventive services and health promotion through education, glucose, weight and hypertension screenings, and referrals to community clinics and low-cost services. In 2019, the VDS Atlanta was funded through a partnership between the Mexican Government and Emory University's School of Public Health and provided services to ~30,000 people.
Formative Research
The formative research consisted in non-participatory ethnographic observation of the functioning, practices and services provided at the VDS Atlanta, three semi-structured interviews with VDS personnel, and a group interview with three VDS clients. The interviews were conducted by the team psychologist (DLMR) and lasted ~30 min. The topics covered in the interviews were activities and programs conducted by the VDS, barriers to mental health care and prevention, and mental health challenges faced by Mexicans living in the Southeast of the US. Information was summarized into a report highlighting recommendations and potential challenges to implement a mental health intervention. The content of the intervention was adjusted based on results from this phase.
Design and Implementation
The design and implementation of the mental health intervention at the General Consulate of Mexico in Atlanta is summarized in Figure 1 and a detailed description is presented next.
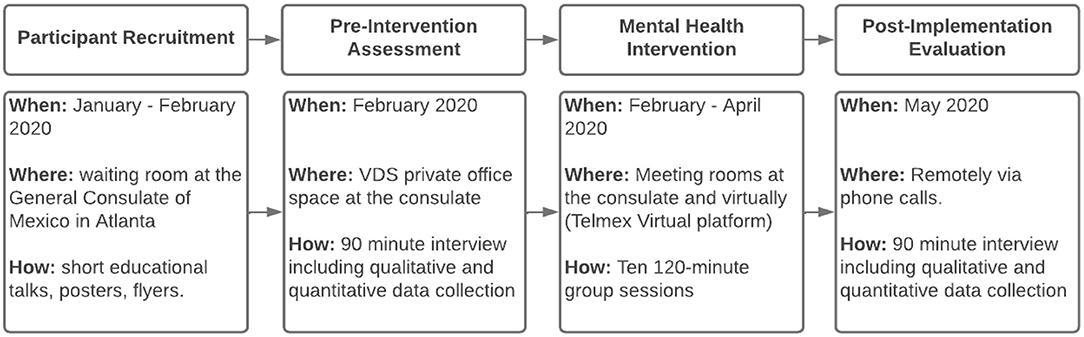
Figure 1. Intervention flowchart.
Participant Recruitment
Participant recruitment was conducted in person at the General Consulate of Mexico in Atlanta between December 2019 and February 2020. The team psychologist (LM) conducted 5–15 min health education talks for Mexicans in the waiting room of the consulate while their documents were being processed and invited them to participate in the intervention; additionally, posters and promotional materials were posted at the consulate, and an invitation to participate in the intervention was posted on the VDS Atlanta Facebook page. Interested participants received a screening and were enrolled in the study if they met the inclusion and exclusion criteria and provided written informed consent to participate in the study. The study was a project to obtain a master's degree in public health (17) approved by Ethics Board of the Mexican National Institute of Public Health (534-R71) and by Emory University Institutional Review Board (IRB00114514).
Inclusion criteria included: age 18 years or older, expressing need or interest in improving their mental health during their visit to the VDS, having an electronic device with internet connection, and being able to read and write. Exclusion criteria included: presence of a severe mental illness that required acute clinical care or having a visual, auditive, or cognitive impairment that impeded their participation in the sessions or in the evaluation.
Intervention Design
This pre-post single arm intervention consisted of ten 120-min group sessions that covered protective factors (social networks, healthy mental health habits, adaptability) and coping strategies (emotional regulation, stress management, and tools to deal with anxiety).
The intervention was conducted between February and May 2020. For the first three sessions, in-person and online options were provided; the remaining sessions were online only. The online component was planned in response to the formative research phase based on concerns related to participants traveling to the consulate on a weekly basis, and on the location of the team psychologist who is based in Mexico. The intervention period also coincided with the COVID-19 pandemic, limiting travel. The online sessions were conducted synchronically through the Virtual platform; they were also recorded and posted on the closed Facebook group that was created for the intervention participants. The closed Facebook group was used as an additional tool to reinforce the session content and was used by the team psychologist to provide instructions and additional material on a weekly basis. Links to the weekly synchronous meetings and pre-post evaluation surveys were posted on this page.
Participants also were given the opportunity of up to two one-on-one meetings with the team psychologist after sessions 5 and 8. The objective of these sessions was to reinforce the material that was being covered during the sessions, to discuss individual progress and challenges, and to address any concerns or issues being faced by the participants. These sessions lasted 45–60 min. Throughout the intervention, the psychologist observed participants to see if there was additional need of emotional support through community referrals.
Evaluation
The evaluation included a quantitative and a qualitative component before and after the intervention (pre-intervention assessment and post-implementation evaluation), and a process evaluation.
The pre- intervention assessment was conducted in person at the General Consulate of Mexico in Atlanta. It had an average duration of 90 min including the qualitative and quantitative components. The process evaluation was conducted during the third and seventh session to assess the method, materials, logistics, activities, and tools; it had the goal of identifying salient issues and improving the remaining sessions. The post-implementation survey and interview evaluation was conducted remotely a month after the last session.
Quantitative Data Collection
Knowledge
This questionnaire measured knowledge about mental health protective factors, based on the Mental Health and Coping Skills of College Students, and knowledge about coping skills based on the Nursing professional coping attitudes questionnaire, which was used in Hispanic populations (26), and was adapted and pilot tested for this study with returning migrants in Mexico These questionnaires have 38 and 30 questions, respectively, follow a Likert scale, and took ~20 min to complete. The mental health protective factors knowledge questionnaire can be categorized to assess the level of knowledge into “very low” (1–47), “low” (48–95), “medium” (96–142) and “high” (143–190), it has high validity (p < 0.01) and reliability (α = 0.93) (26). The coping skills questionnaire can be categorized into “deficient” (1–37), “low” (38–75), “medium” (76–112), and “high” (113–150) and also had high validity (p = 0.02) and reliability (α = 0.70) (27).
Psychological Distress
We used the Kessler Psychological Distress Scale (20), a 10-item questionnaire designed to provide a global measure of distress based on questions about anxiety and depressive symptoms. It uses a Likert Scale and provides an assessment of psychosocial distress: “low” (10–15), “moderate” (16–21), “high” (22–29) and “very high” (≥30) (28, 29).
Qualitative Data Collection
Semi-structured Interviews
Semi-structured interviews were conducted during the pre and the post evaluation. The pre- intervention interview was conducted in person in the Ventanilla de Salud private office space at the consulate and lasted ~45–60 min. The topics covered included sociodemographic information, family and individual mental health history, current mental health, effects of migration on mental health, protective factors and coping mechanisms. People with severe mental illness were excluded from the study and referred to local community resources.
The post- interviews were conducted remotely a month after the last session, they also had a duration of 45–60 min and included the following themes: current mental health status, protective factors and coping skills.
Data Analysis
Quantitative
Data collected using the questionnaires were entered into an Excel (v16.3) dataset. Likert scales were converted into numerical values going from 1 to 5. To assess changes in pre- and post-values we used the Wilcoxon non-parametric test, this was selected due to the small sample size and because the data did not meet the normality assumption. Following analysis recommendations for pre-post designs (30), the intent-to-treat analysis included all participants with pre-intervention information and complete case analysis was restricted to participants who attended at least 70% of the sessions and had post-implementation information. The process evaluation data were entered into a Google Form and then descriptive statistics were used to analyze them. All quantitative analyses were conducted using STATA v.15.
Qualitative
Interview data were transcribed into a Microsoft Word (v16.3) document and content matrices were created manually. These were analyzed using deductive codes based on the theoretical framework and the themes that were pre-specified during the development of the interview guides. This was further complemented using inductive coding, incorporating themes that had not been considered a priori.
Quantitative and qualitative data was triangulated for the final intervention evaluation report.
Results
Baseline Characteristics
Thirty-four participants expressed interest in participating, met the inclusion criteria, and were invited to the complete the pre-evaluation and participate in the sessions. Twenty-five participants signed the informed consent, completed the pre-evaluation, and were added to the Facebook group. Nine attended at least 70% of the sessions and completed the post-evaluation (Figure 2). The average attendance per session was of eleven people, with a minimum attendance of eight and a maximum of thirteen. Most participants who were lost to follow up did not show up to any session. The main reported reasons for not showing up were technical challenges using the platform (n = 6), time constraints (n = 4), unexpected circumstances such as change of job (n = 3), fear of legal consequences as an undocumented immigrant (n = 2), and shame of speaking in front of other participants (n = 1).
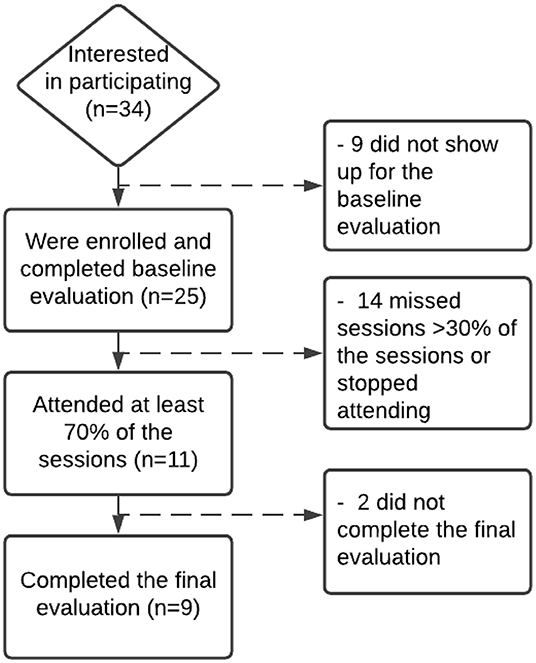
Figure 2. Participant flowchart.
Sociodemographic Characteristics of Study Participants
Participants were on average 39.8 (SD = 9.5) years and the majority (89%) were women. In general, participants that were included in the intervention were similar to those who were excluded from the pre-post evaluation due to missing sessions or not completing the post-evaluation. The main differences between these two groups were that workers in construction, cleaning, or cooking, and participants located outside of Georgia were more likely to not participate in 70% of sessions (Table 1).

Table 1. Sociodemographic characteristics of participants included (n = 9) and excluded (n = 16) from the pre-post evaluation.
Group Characteristics From Qualitative Pre-intervention Evaluation (n = 25)
Five topics related to the characteristics of the group were identified in the semi-structured interviews implemented during the pre-evaluation: reasons for migration, immigration experience, physical and mental health, risk factors for mental health, and challenges accessing mental health services.
Reasons for Migration
Participants mentioned being encouraged by others as important reasons to migrate to the US. Some had been brought by their parents when they were still underage. Women mentioned traditional gender roles as the reason to come to the US following their husbands or sons. Economic factors also influenced this decision, some participants mentioned that their parents or partners suggested that they migrate to improve their socioeconomic status.
Migration Experience
Participants discussed their experiences with migration in terms of time in the US and the experience evolved as they spent more years in the country. Most came to the US without migratory documents, but many were able to normalize their status with time. The main problems highlighted by the participants were feeling discriminated, judged or rejected by the new environment, challenges learning English, and lack of documentation which, in some cases, resulted in abuse by policemen, and feelings of fear, loneliness, and difficulty adapting to a new country. Participants said these situations directly impacted their mental health.
Physical and Mental Health
Participants expressed that they did not feel that their physical health had been affected by living in the US. However, they considered that living in the US had negatively impacted their mental health. They again identified being undocumented, as well as long work days, having left family behind in Mexico, language barriers, and feeling unable to adapt to the new country as factors affecting their mental health. They expressed that these situations left them feeling frustration, sadness, anxiety, stress, fear, depression, desperation, and like they do not belong in either Mexico or the US. Some women also mentioned problems in the current relationship with their partners as a factor affecting their mental health, which they said generated emotional distress and poor interactions with their social support networks.
Implementation and Process Evaluation
The ten virtual sessions were implemented as planned and had an average duration of 50 min. After the first in-person session in February 2020, participants had difficulty traveling to the Consulate and all sessions were then conducted virtually.
The two process evaluations yielded perfect satisfaction scores with all participants strongly agreeing that they were satisfied with the helpfulness of the topics, quality and clarity of the materials, the virtual platform, and the skills of the team psychologist conducting the sessions (using clear language, being respectful, etc.). There was 10% dissatisfaction with two sessions due to excessive duration (data not shown).
Pre- and Post-evaluation
Quantitative Results
Participants significantly increased their scores on knowledge of protective factors and coping skills, and had lower scores in the Kessler Scale of Psychological Distress (all p < 0.05) (Table 2).

Table 2. Pre- and post-evaluation scores for protective factors and coping mechanisms knowledge, and psychological distress among Mexican immigrants who participated in a mental health promotion intervention (n = 9).
Qualitative Results
Based on the theoretical framework, the intervention curriculum and the pre- and post-semi-structured interviews, the themes identified in the qualitative analysis were social support networks, adaptability, positive mental health habits, emotional regulation, stress management when facing a problem, and the role of the intervention during the COVID-19 pandemic. Many participants reported progress in the areas covered by the intervention and described using some of the techniques that were recommended during the sessions. They also identified some challenges applying the new knowledge and reported that they continue to work on those areas (Table 3).
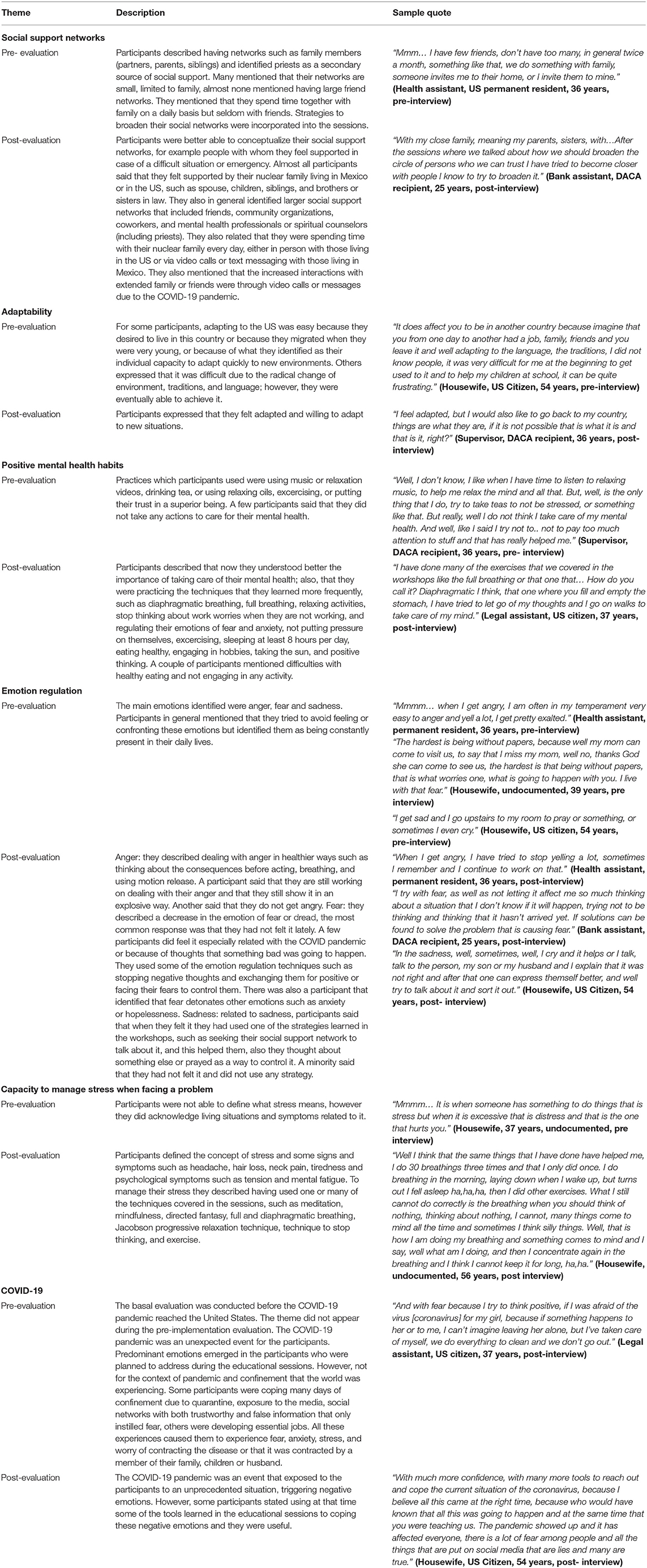
Table 3. Qualitative results for pre- post- evaluation of a mental health promotion intervention for Mexican immigrants.
Discussion
Despite their large numbers and high levels of emotional distress and mental health problems, reaching the Mexican immigrant population through mental health interventions has been very challenging. Little research has addressed this problem. We leveraged the reach and access of the VDS Atlanta to design and pilot a mental health promotion intervention for Mexican immigrants that was successful in improving psychological distress and knowledge among participants who attended at least 70% of the sessions. These results are encouraging and suggest that efforts to support protective mental health factors and teach coping strategies in groups has the potential to improve mental health outcomes in a distressed population.
This is the first study reporting on a mental health promotion intervention for Mexican immigrants implemented through a VDS; however, other similar preventive interventions have been conducted with ethnic and racial minority groups in the US. Most have focused on mental health assessments and referrals (12). Raval et al. (13) conducted a mental health promotion intervention and were successful improving internalizing and externalizing behaviors among minority youth in New York City. Blumenthal et al. used community based participatory research to develop mental health promotion interventions for African Americans and Latinos that resulted in better self-reported physical health and a decrease in depression symptoms (14). Another commonly-used approach among community-based mental health initiatives has been through promotoras (12). The Promotoras Model, where community health workers receive basic training to provide health education or promotion in their communities, has been used successfully in many areas of health and is increasingly used for group or individual mental health promotion interventions. The ALMA (Amigas Latinas Motivando el Alma/Latina Friends Motivating the Soul) pilot intervention used this model for a peer- support and education intervention was successful improving depression symptoms, acculturative stress and coping mechanisms among Latina immigrants in North Carolina (15). This is consistent with our findings and highlights the potential impact of community health promotion interventions to improve the health of Latino immigrants in the US. Further, the fact that our study is imbedded into an ongoing, national project that already conducts some screening and referrals could contribute to scaling up improved versions of this intervention.
An important finding of this study was high levels of attrition. High attrition and underrepresentation of Latinos and other racial and ethnic minorities have been important challenges in health research (31). In this study, through the VDS, we were able to reach and enroll a sample of Mexican immigrants, a population that based on the various societal, cultural and economic challenges has been difficult to include in health interventions, but several factors limited the retention of more than half of the sample. The main impediment for participants to join the sessions was problems with technology or signing into the virtual platform. In this sense, technological advances provide an opportunity to deliver health interventions, including in the mental health field, however, a digital divide has been identified where minoritized populations tend to have less access to technological resources (32). If this divide is not addressed, technology could exacerbate disparities in health promotion and care, which is a particular concern after the COVID-19 pandemic increased the need for remote and online interventions (33). A lesson-learned from this pilot-intervention was the need to address technological barriers before the start of the program. Additionally, some participants reported dissatisfaction with session length, and it is possible that 10 session was excessive; future program iterations should assess the feasibility and impact of delivering the program in shorter and fewer sessions.
Fear and anxiety were reported by participants both as barriers to attend the sessions and as one of the main emotions affecting their mental wellbeing. Participants identified being undocumented, working conditions, distance from family, language barriers, and adaptation challenges as factors leading to these emotions. This is consistent with other studies that have identified migration and socio-cultural factors as specific barriers affecting the mental health of Latino immigrants in the US (34). Others have also identified fear and anxiety as factors related to attrition (29), highlighting the importance of addressing these factors as part of health interventions, especially those targeting immigrants and racial or ethnic minorities; this could potentially improve retention and translate into better mental health outcomes (35). Further research is needed to identify potential approaches to address these factors and increase the reach of mental health promotion interventions in this population.
The small sample size was another limitation of this study besides attrition; however, we were still able to detect differences in the sample that completed the final evaluation, supporting the efficacy of the intervention. The COVID-19 pandemic was a challenge that made it even harder for some participants to attend the sessions, but the importance of having this form of support during the beginning of the pandemic was highlighted by participants in the final evaluation. Strengths of this study include the formative research that allowed us to design a culturally-relevant intervention and to take advantage of the community networks and programs of the VDS; the use of theoretical frameworks that incorporate protective factors, coping skills and emotional education for mental health promotion in marginalized populations; and the mixed methods evaluation that allowed us to assess the impact and also understand the psychosocial factors around attrition and effectiveness.
In conclusion, we developed and implemented a mental health promotion intervention for Mexican Immigrants through the VDS program in Atlanta that resulted in increased knowledge and lower distress among those who attended at least 70% of the sessions. The impact of this results was attenuated by high attrition that resulted from technological challenges and psychosocial barriers associated with migration and other socio-economic factors. In order to achieve health equity, particularly in mental health, it is important to continue to implement and study culturally relevant mental health promotion interventions for Latino immigrants and other racial and ethnic minorities that address the particular challenges faced by these populations.
Data Availability Statement
The datasets presented in this article are not readily available because of the small number of participants and the sensitive nature of this data. Requests to access the datasets should be directed to IG, aW5lZ29uemFAaXUuZWR1.
Ethics Statement
The studies involving human participants were reviewed and approved by National Institute of Public Health Ethics Review Board. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
DM, TG, MM, and IG contributed to conception and design of the study. DM conducted the data collection, implemented the pilot intervention, and analyzed the data. TG, MM, and IG guided the analysis of the data. MG and AF contributed to the interpretation of the data and wrote sections of the manuscript. DM and IG wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The Ventanilla de Salud Atlanta at the time of the study was funded through a shared cost agreement between Emory University and Mexico's Secretary of Health (SSA) and Institute for the Mexicans in the Exterior (IME). The intervention was funded through funds that were destined for mental health promotion by SSA and IME in 2019. IG received funds from the National Heart, Lung and Blood Institute as part of UCSF's Research in Implementation Science for Equity small research project (5R25HL126146).
Conflict of Interest
IG served as Emory University's director of the Ventanilla de Salud Atlanta program at the time of the implementation of the study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Migration Report. Geneva, Switzerland: International Organization for Migration, United Nations (2020).
2. Alonso AD. Mexicans in the United States. In Pursuit of Inclusion. Current History. (2016) 115:305–11. doi: 10.1525/curh.2016.115.784.305
3. Israel E, Batalova J. Mexican Immigrants in the United States. Migration Information Source (2020).
4. Shobe MA, Coffman MJ, Dmochowski J. Achieving the American dream: facilitators and barriers to health and mental health for Latino immigrants. J Evid Based Soc Work. (2009) 6:92–110. doi: 10.1080/15433710802633601
5. Garcini LM, Galvan T, Peña JM, Klonoff EA, Parra-Medina D, Ziauddin K, et al. “A high price paid”: migration-related loss and distress among undocumented Mexican immigrants. J Latinx Psychol. (2019) 7:245–55. doi: 10.1037/lat0000127
6. Orozco Vargas AE. Migración y estrés aculturativo: una perspectiva teórica sobre aspectos psicológicos y sociales presentes en los migrantes latinos en Estados Unidos. Norteamérica. (2013) 8:7–44. doi: 10.20999/nam.2013.a001
7. Moya EM, Chávez Baray SM, Esparza ÓA, Calderón Chelius L, Castañeda E, Villalobos G, et al. El Síndrome de Ulises en inmigrantes económicos y políticos en México y Estados Unidos. EHQUIDAD Revista Internacional de Políticas de Bienestar y Trabajo Social. (2017) 0:11–50. doi: 10.15257/ehquidad.2016.0001
8. Ornelas IJ, Perreira KM. The role of migration in the development of depressive symptoms among Latino immigrant parents in the USA. Soc Sci Med. (2011) 73:1169–77. doi: 10.1016/j.socscimed.2011.07.002
9. Greer TM. Coping strategies as moderators of the relation between individual race-related stress and mental health symptoms for African American women. Psychol Women Q. (2011) 35:215–26. doi: 10.1177/0361684311399388
10. Addressing the Mental Health Needs of Racial and Ethnic Minority Youth - A Guide for Practitioners. Washington, DC: American Psychological Association (2017).
11. Min J-A, Lee C-U, Lee C. Mental health promotion and illness prevention: a challenge for psychiatrists. Psychiatry Investig. (2013) 10:307–16. doi: 10.4306/pi.2013.10.4.307
12. Stacciarini JM, Shattell MM, Coady M, Wiens B. Review: community-based participatory research approach to address mental health in minority populations. Community Ment Health J. (2011) 47:489–97. doi: 10.1007/s10597-010-9319-z
13. Raval G, Montañez E, Meyer D, Berger-Jenkins E. School-based mental health promotion and prevention program “turn 2 us” reduces mental health risk behaviors in urban, minority youth. J School Health. (2019) 89:662–8. doi: 10.1111/josh.12805
14. Bluthenthal RN, Jones L, Fackler-Lowrie N, Ellison M, Booker T, Jones F, et al. Witness for wellness: preliminary findings from a community-academic participatory research mental health initiative. Ethn Dis. (2006) 16 (1 Suppl. 1):S18–34.
15. Tran AN, Ornelas IJ, Kim M, Perez G, Green M, Lyn MJ, et al. Results from a pilot promotora program to reduce depression and stress among immigrant Latinas. Health Promot Pract. (2014) 15:365–72. doi: 10.1177/1524839913511635
16. Rangel Gomez MG, Tonda J, Zapata GR, Flynn M, Gany F, Lara J, et al. Ventanillas de Salud: a collaborative and binational health access and preventive care program. Front Public Health. (2017) 5:151. doi: 10.3389/fpubh.2017.00151
17. Martinez Rodriguez DL. El uso de e-Health con usuarios de la ventanilla de salud del consulado de Atlanta, EEUU. para el fomento de factores protectores de salud mental en migrantes mexicanos. Cuernavaca, Mexico: Instituto Nacional de Salud Publica (2020).
18. Kobau R, Seligman MEP, Peterson C, Diener E, Zack MM, Chapman D, et al. Mental health promotion in public health: perspectives and strategies from positive psychology. Am J Public Health. (2011) 101:e1–e9. doi: 10.2105/AJPH.2010.300083
19. World Health Organization. Prevention of Mental Disorders: Effective Interventions and Policy Options: Summary Report/A Report of the World Health Organization Dept. of Mental Health and Substance Abuse; in Collaboration With the Prevention Research Centre of the Universities of Nijmegen and Maastricht. Geneva: World Health Organization (2004).
20. Coie JD, Watt NF, West SG, Hawkins JD, Asarnow JR, Markman HJ, et al. The science of prevention. A conceptual framework and some directions for a national research program. Am Psychol. (1993) 48:1013–22. doi: 10.1037/0003-066X.48.10.1013
21. Saxena S, Jané-Llopis E, Hosman C. Prevention of mental and behavioural disorders: implications for policy and practice. World Psychiatry. (2006) 5:5–14.
22. Guerrero AB, Gutierrez AC. Elements for the emotional learning in adults. Int J Learn. (2008) 15:89–94. doi: 10.18848/1447-9494/CGP/v15i02/45632
23. Ferrer RA, Fisher JD, Buck R, Amico KR. Pilot test of an emotional education intervention component for sexual risk reduction. Health Psychol. (2011) 30:656–60. doi: 10.1037/a0023438
24. Góralska R. Emotional education discourses: between developing competences and deepening emotional (co-) understanding. Qual Sociol Rev. (2020) 16:110–25. doi: 10.18778/1733-8077.16.1.08
25. Saini IK. Strengthening life skills through emotional intelligence education. Educ Quest. (2016) 7:5–11. doi: 10.5958/2230-7311.2016.00011.8
26. Fernández-Castillo E, Molerio-Pérez O, Herrera-Jiménez LF, Grau R. Validity and reliability of a questionnaire in exploring the protective factors of mental health in Cuban university students. Actualidades en Psicologia. (2017) 31:103–17. doi: 10.15517/ap.v31i122.24584
27. Peña Chagua MA, Gomez Perez KK. Estrés laboral y actitud de afrontamiento del profesional de enfermería del servicio de emergencia del hospital docente clínico quirúrgico Daniel Alcides Carrión, Huancayo−2017. Peru: Universidad Nacional del Callao (2018).
28. Valencia-Garcia D, Bi X, Ayón C. Sensitivity and specificity in three measures of depression among Mexican American women. J Immigr Minor Health. (2017) 19:562–71. doi: 10.1007/s10903-016-0512-1
29. Vargas Terrez BE, Villamil Salcedo V, Rodríguez Estrada C, Pérez Romero J, Cortés Sotres JJ. Validación de la escala Kessler 10 (K-10) en la detección de depresión y ansiedad en el primer nivel de atención. Propiedades psicométricas. (2011) 34:323–31.
30. Xi W, Pennell ML, Andridge RR, Paskett ED. Comparison of intent-to-treat analysis strategies for pre-post studies with loss to follow-up. Contemp Clin Trials Commun. (2018) 11:20–9. doi: 10.1016/j.conctc.2018.05.008
31. Yu Z, Kowalkowski J, Roll AE, Lor M. Engaging underrepresented communities in health research: lessons learned. West J Nurs Res. (2021) 43:915–23. doi: 10.1177/0193945920987999
32. Ramos G, Chavira DA. Use of technology to provide mental health care for racial and ethnic minorities: evidence, promise, and challenges. Cogn Behav Pract. (2019) 29:15–40. doi: 10.1016/j.cbpra.2019.10.004
33. Ojha R, Syed S. Challenges faced by mental health providers and patients during the coronavirus 2019 pandemic due to technological barriers. Internet Interv. (2020) 21:100330. doi: 10.1016/j.invent.2020.100330
34. Fortuna LR, Álvarez K, Ramos Ortiz Z, Wang Y, Mozo Alegría X, Cook BL, Alegría M. Mental health, migration stressors and suicidal ideation among Latino immigrants in Spain and the United States. Eur Psychiatry. (2016) 36:15–22. doi: 10.1016/j.eurpsy.2016.03.001
Keywords: mental health, health promotion, Mexican immigrants in the United States, community based mental health, protective factors, coping strategies
Citation: Martínez Rodríguez DL, González Vázquez T, Márquez Serrano M, Groot Md, Fernandez A and Gonzalez Casanova I (2022) A Window Into Mental Health: Developing and Pilot-Testing a Mental Health Promotion Intervention for Mexican Immigrants Through the Ventanilla de Salud Program. Front. Public Health 10:877465. doi: 10.3389/fpubh.2022.877465
Received: 16 February 2022; Accepted: 24 March 2022;
Published: 15 April 2022.
Edited by:
Yuka Kotozaki, Iwate Medical University, JapanCopyright © 2022 Martínez Rodríguez, González Vázquez, Márquez Serrano, Groot, Fernandez and Gonzalez Casanova. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tonatiuh González Vázquez, dG9uYXRpdWguZ29uemFsZXpAaW5zcC5teA==; Ines Gonzalez Casanova, aW5lZ29uemFAaXUuZWR1