 Shuanghu Fang
Shuanghu Fang Dongyan Ding
Dongyan Ding Ru Zhang
Ru Zhang Mingjie Huang
Mingjie Huang- School of Educational Science, Anhui Normal University, Wuhu, China
Hoarding is a common problem behavior worldwide and is detrimental to the physical and mental health of individuals and groups. Currently, effective interventions for hoarding are cognitive-behavioral therapies, but their post-intervention efficacy is questionable, and the available research does not examine the mediating variables of the effects of interventions on clinical outcomes. Moreover, current research on hoarding has focused on Western countries. Therefore, there is a need to investigate the efficacy of other forms of cognitive behavioral therapy on hoarding as well as other psychological outcomes related to hoarding and mediating variables that contribute to its effectiveness in different cultural contexts. One hundred thirty-nine college students with higher hoarding behaviors were randomly divided into three groups: 45 in the Acceptance and Commitment Therapy (ACT) group, 47 in the Rational Emotive Behavior Therapy (REBT) group, and 47 in the control group. They completed the Saving Inventory-Revised (SI-R), Obsessive-Compulsive Symptom Scale (OCSS), Difficulties in Emotion Regulation Scale (DERS), Experiences in Close Relationships Inventory-Attachment Anxiety Subscale (ECR), Depression Anxiety Stress Scales (DASS-21), Acceptance and Action Questionnaire II (AAQ-II), and Cognitive Fusion Questionnaire (CFQ) before and immediately after the intervention. The results showed that ACT and REBT improved individuals' psychological flexibility, cognitive fusion, acquisition-difficulty discarding, clutter, negative affect (anxiety, depression, stress), attachment anxiety, obsessive-compulsive disorder, and difficulty in emotion regulation compared to the control group. In addition, ACT was more effective than REBT in improving psychological flexibility and reducing hoarding, cognitive fusion, depression, stress, and obsessive-compulsive disorder; there were no significant differences between the two in anxiety and emotion regulation difficulties. Furthermore, psychological flexibility is a mediator of the effect of ACT and REBT on some behavioral and psychological outcomes (hoarding, negative affect, attachment anxiety). Limitations were discussed.
Introduction
Hoarding disorder has been considered a subtype of obsessive-compulsive disorder (OCD) and obsessive-compulsive personality disorder (OCPD) (1). Hoarding is characterized by severe difficulties in discarding possessions, resulting in a cluttered living space that cannot be used for its intended purpose (2, 3). Frost and Hartl (3) identified hoarding as consisting of the following key elements: the acquisition of a large number of possessions, the subsequent failure to discard the possessions, and the clutter that results in a living space that cannot be used in the manner for which it was designed. Studies have shown that up to 5.8% of the population has a hoarding disorder (4). Due to cultural differences, in China, hoarding may be considered a good virtue of “frugality” and “thriftiness”. As a result, hoarding is common in China. Previous research has shown that ~51.8% of college students reported hoarding behaviors, but only about 4.22% met the DSM-5 diagnostic criteria for hoarding disorder (5). Severe hoarding behaviors can even lead to community health and safety problems, such as falls, fires, and death (6). Additionally, hoarding is an important mental health problem that can lead to severe personal distress and may result in impairment of social skills, occupational abilities, and family functions (7, 8). Individuals with higher hoarding behaviors have poorer information processing skills (9, 10) and may also have problems with attention and memory (11–13).
Research has shown that individuals with higher attachment anxiety often exhibit higher hoarding (14, 15), which is consistent with insecure attachment (16). Attachment theory suggests that the severe difficulty of discarding possessions in hoarding may be an attempt to compensate for loneliness and lack of emotional connection with people (17, 18). Emotional over-attachment to objects appears to be one of the distinguishing features of hoarding behaviors, with possessions often seen as an extension of the self (19). Attachment anxiety is a significant predictor of hoarding behavior (20, 21). It has been suggested that intolerance of uncertainty and experiential avoidance exerted sequential mediating effects on the association of attachment anxiety with hoarding behavior, i.e., attachment anxiety could influence hoarding behavior, which in turn affected intolerance of uncertainty and experiential avoidance and then impacted hoarding behavior (22). Therefore, examining the mechanism of attachment anxiety on hoarding behavior from the perspective of cognitive and coping means has implications for the prevention and intervention of hoarding behavior.
Many theoretical models have integrated emotional regulation and emotional responses into the onset and maintenance of psychological symptoms (23, 24). Individuals with hoarding experience difficulties with emotional regulation (13), and they also have higher levels of experiential avoidance and emotion regulation difficulties than healthy individuals (25). Systematic reviews and meta-analyses suggested that emotion dysregulation had a medium to strong association with hoarding (26, 27). Hoarding disorder is considered a subtype of OCD, and the cognitive model of OCD suggests that OCD is influenced by emotion regulation difficulties and consistently implicates the nonacceptance of emotions and difficulties engaging in goal-directed behavior when distressed (28). Some researchers have suggested that emotion regulation can play an important role in understanding OCD and in improving treatment, as well as improving the tolerability of treatment for individuals with this debilitating disorder (28). Emotional reactions also play a key role in the onset and maintenance of hoarding (26). Hoarding is closely related to the experience of negative emotions (29, 30). Previous research reported that people with higher levels of hoarding may also suffer from negative affect (e.g., depression, anxiety, stress) (13, 30). The cognitive-behavioral model of hoarding highlights the role of strong negative emotional responses (e.g., sadness, anxiety, depression) in stimulating hoarding behaviors (3, 24). Some research has argued that stronger negative emotions after viewing emotional movies were associated with more severe hoarding symptoms (24, 31). Some studies have suggested that it is appropriate to examine whether emotional responses should be the target of behavioral interventions for hoarding (24).
Hoarding could be influenced by psychological flexibility. As a core component of acceptance and commitment therapy (ACT), psychological flexibility can be divided into six core processes: acceptance, cognitive defusion, engagement with the present moment, self as context, values, and committed action (32–34). Psychological flexibility can assist individuals in consciously accepting adverse life events and adversities with an open mindset and help people persist and act on their value-consistent goals (35, 36). Existing meta-analyses suggest that psychological flexibility is positively related to individuals' mental health and adaptive behaviors and negatively related to individuals' negative emotional affect and problematic behaviors (37–39). Psychological flexibility has been found to be significantly associated with hoarding behaviors (40). It was found that the lower the degree of psychological flexibility, the higher the hoarding behaviors (31). There was also a significant negative association between psychological flexibility and difficulty discarding and over-acquisition in a clinical sample (41). Some researchers believed that the symptoms of hoarding (e.g., acquisition and clutter) stem from a variety of avoidance behaviors designed to avoid the pain of making poor decisions about possessions (3). Researchers have observed a pattern of behavioral avoidance in most hoarders (3, 25). Experienced avoidance is a subcomponent of psychological inflexibility (33). Psychological inflexibility may manifest as a confusion of thoughts with reality, leading to hoarding (42). Cognitive fusion, as one factor of psychological inflexibility, may further contribute to hoarding (43). If individuals are filled with thoughts about their possessions, such as “I cannot get rid of this,” they may build a narrow repertoire of options for saving or acquiring. The role of cognitive fusion may be related to the emergence of hoarding-related thoughts (43).
Most current interventions for hoarding behaviors are less effective or even ineffective, but many kinds of cognitive behavioral therapy (CBT) have shown definite effectiveness in reducing hoarding disorders (44, 45). However, a meta-analysis indicated that in most cases, patients continue to have significant hoarding symptoms after treatment with CBT (46). CBT has gone through several different eras, generations, or waves. Traditional CBT focuses on modifying maladaptive thought and cognitive distortion patterns in emotions and behaviors, training adaptive thinking, and engaging in enjoyable activities (47, 48). Third-wave CBT is based on the concept of context and focuses more on the person's relationship with thoughts and emotions than on the content of cognitions (47). Therefore, it is necessary to explore the role of other forms of CBT that are more effective for treating hoarding behaviors and related outcomes.
Rational Emotive Behavior Therapy (REBT) is one kind of traditional CBT, but there is little empirical evidence on the efficacy of REBT for hoarding. The theoretical basis of REBT is the ABC theory of emotions (49, 50). In the ABC model, A represents the activating event, B represents rational or irrational beliefs, and C represents emotional, cognitive, and behavioral consequences (49). According to the ABC model, when the reality of a situation contradicts our needs, we transform our rational needs into inflexible desires, and therefore we become emotionally upset (51). One of the core principles of REBT is that these evaluative beliefs influence people's perceptions of events and then affect their emotions, behaviors, and reactions to those events (52). The primary goal of REBT is to change irrational beliefs through cognitive restructuring and to foster rational beliefs to promote mental health and wellbeing (49, 52). A systematic review and meta-analysis summarized the effectiveness and efficacy of 50 years of REBT and concluded that REBT has a medium effect size compared to other interventions on irrational beliefs and different types of outcomes (e.g., emotional outcomes, behavioral outcomes, cognition outcomes, and health outcomes) (53). Currently, REBT has been used with good results in the treatment of psychological disorders, such as depression (54) and social phobia (55). However, no studies have explored the utility of REBT for hoarding. Hoarding is a subtype of OCD (1). A case study of schizophrenia and OCD in China concluded that REBT has an ameliorative effect on OCD (56). REBT specializes in helping clients unconditionally self-accept their OCD suffering, as well as increasing their frustration tolerance about affiliation (57). Therefore, we hypothesized that REBT may be effective in alleviating hoarding behaviors.
According to the cognitive model of hoarding, the manifestation of hoarding (e.g., difficulty discarding, clutter, and acquiring) stems from a variety of avoidance behaviors aiming to avoid distress (3). Acceptance commitment therapy, as a third-wave CBT, can reduce experiential avoidance by increasing psychological flexibility while encouraging participants to make behavioral changes consistent with their values (35, 58). Hoarding behaviors are considered lifelong, and therefore, treatment should focus on symptom improvement rather than complete remission (46, 59), which is consistent with the notion of not changing symptoms but only the relationship with distress in the ACT. Some meta-analyses and reviews have found that ACT has efficacy for improving mental health and reducing behavioral disorders in adults and children (60–62), such as decreasing anxiety, depression, stress, eating disorders (63), obsessive-compulsive disorder (64), and smoking (65). A recent intervention trial with six individuals revealed the effectiveness of ACT for reducing hoarding symptoms (66), but the participants in this trial were all white women. One of the authors of this study explored the efficacy of an ACT self-help program on hoarding (67) and concluded that ACT has an ameliorative effect on hoarding. However, to date, the efficacy of ACT on hoarding in China has not yet been explored.
Currently, the vast majority of ACT research or psychological flexibility studies have been conducted in Western countries and in English. In addition, contemporary research on hoarding has also focused on Western countries, and there is a lack of research on the effects of ACT on hoarding behaviors in different cultural contexts. Moreover, some studies focusing on mechanisms of change have suggested that the effect of ACT or CBT on outcome variables (e.g., depression, pain interference, and OCD) is mediated by its impact on psychological flexibility or cognitive fusion (68–70). However, previous studies on the effects of CBT on hoarding have failed to examine the possible mediating role of psychological flexibility or cognitive fusion as a process variable. A test of mediating effects would be helpful in understanding the mechanisms of CBT in non-Western countries and the role of psychological flexibility and cognitive fusion in individual psychological and behavioral changes.
According to the aforementioned, hoarding can be accompanied by attachment anxiety, difficulties with emotion regulation, and negative emotions. Therefore, the main purpose of this study was to investigate the efficacy of ACT and REBT on hoarding among Chinese college students and to explore whether psychological flexibility or cognitive fusion mediates the effect of ACT/REBT on the outcome variables (i.e., hoarding behaviors, difficulties in emotion regulation, and attachment anxiety).
Methods
Participants
This study was approved by the Ethical Committee of Anhui Normal University. A total of 1,620 questionnaires were distributed to university students, and 14,78 valid questionnaires were returned (91.2% effective rate). Among the 1,478 surveys, 533 college students had high hoarding problems (total score of Saving Inventory-Revised above the cutoff of 42). Participants in this study were recruited from these 533 university students. The inclusion criteria of the intervention group were being aged 18 years or older and having a self-reported total score on the Saving Inventory-Revised above the cutoff of 42. Exclusion criteria assessed via self-report measures and one-on-one online semistructured interviews with a trained research assistant were suicidal intentions, use of psychiatric medicines, receiving psychological counseling or other treatment, and not being willing to undergo the intervention. In this way, we recruited 144 participants. They were randomly divided into three groups: the ACT group, REBT group, and control group, with 48 participants in each group (see Figure 1). It is necessary to note that these students did not participate in other interventions or take medication to alleviate their symptoms. Informed consent was obtained from all students. Five participants withdrew from the intervention for personal reasons (i.e., no time to complete all intervention programs or questionnaires) in the process, resulting in a total sample of N = 139, of which 66 (48.2%) were male and 73 (51.8%) were female, with a mean age of 19.65 ± 1.46 years. There were 45 participants in the ACT group, including 22 males and 23 females, with a mean age of 19.71 ± 1.56 years; 47 participants in the REBT group, including 23 males and 24 females, with a mean age of 19.72 ± 1.49 years; and 47 participants in the control group, including 21 males and 26 females, with a mean age of 19.53 ± 1.37 years.
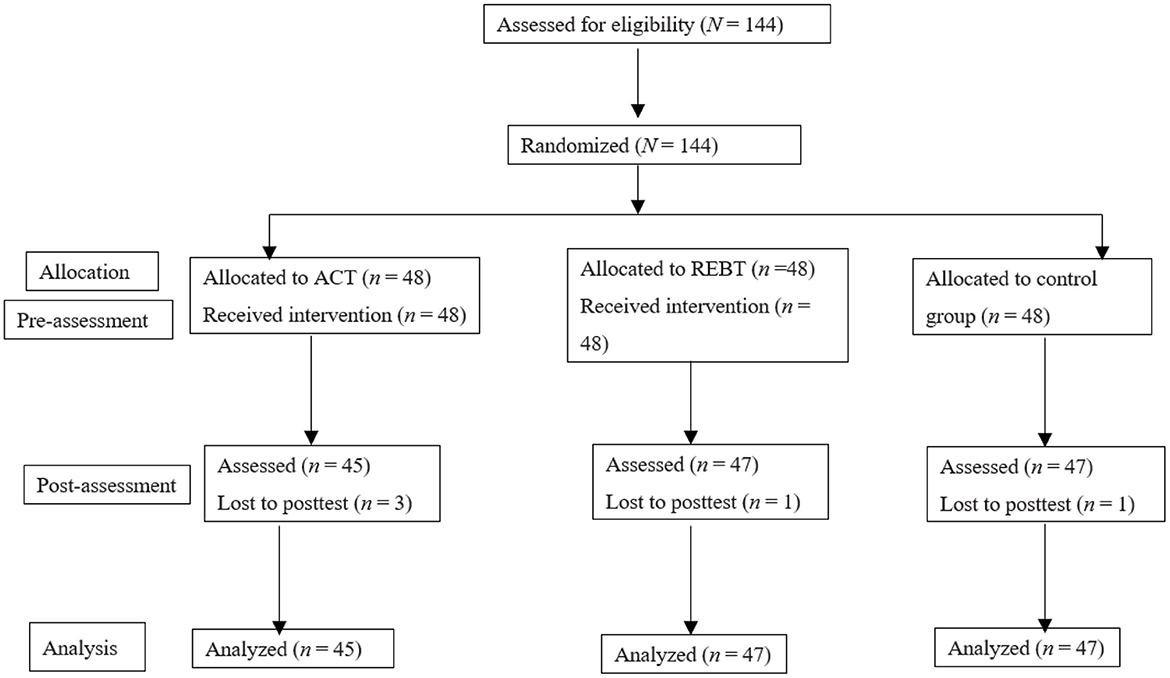
Figure 1. Flowchart of participants.
To test the reasonableness of the sample size, statistical power was calculated using G*Power 3.1 software (71). Referring to the parameter settings in previous studies (72), the covariance analysis was chosen with an effect size of 0.4, a significance level of 0.05, a sample size of 139, a group size of 3, and a covariate of 1. The statistical power was 0.99, which exceeded the basic level of 0.80, so the sample size of this study met the requirements.
Procedure
This study was a three-group randomized controlled trial. Participants were randomly assigned to one of the three groups. The ACT group was given acceptance commitment therapy group counseling, the REBT group was given rational emotional behavior therapy group counseling, and the control group was left untreated. The ACT, REBT, and control groups were pre-tested before the beginning of group counseling and post-tested after the completion of group counseling.
Interventions
Group interventions for both groups were conducted once a week for 1.5 h for 8 weeks. The group intervention protocols were designed by two professionally trained psychology graduate students supervised by the first author of this paper, who is the President of the China chapter of Association for Contextual Behavioral Science and is a professionally trained and certified counselor, trainer, and supervisor. The intervention protocols were revised and refined based on the suggestions of the relevant counselors and supervisors. Before each intervention, the first author explained and illustrated the intervention protocol and intervention points and led the interventionists to discuss the intervention process and intervention methods together. After each intervention, the interventionists reported to the first author of this paper, who provided supervision. The entire process of the group intervention was completed under the supervision of the first author.
ACT condition
The intervention content for the ACT group was based on the psychological flexibility model, with reference to the book Acceptance and commitment therapy: The process and practice of mindful change (73), and Act in practice: Case Conceptualization in Acceptance and Commitment Therapy (74). 8-week intervention programs were designed. See Table 1 for the specific intervention programs.
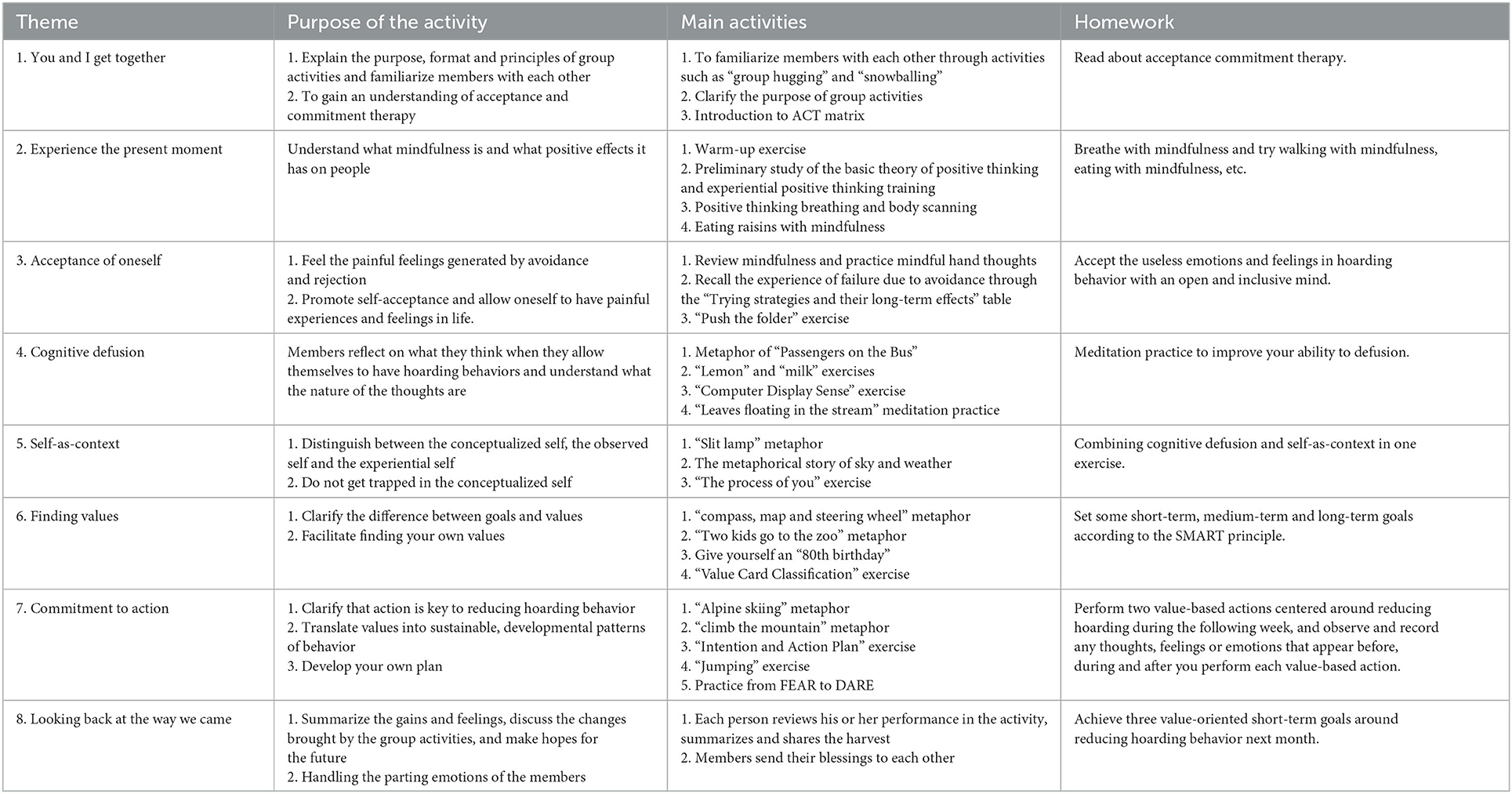
Table 1. Acceptance and commitment therapy intervention program.
REBT condition
The intervention program was based on ABC theory, with reference to the book How to make yourself happy and remarkably less disturbable (75) and Rational Emotive Behavior Therapy (76). A total of 8 weeks of intervention programs were designed. See Table 2 for the specific intervention items.
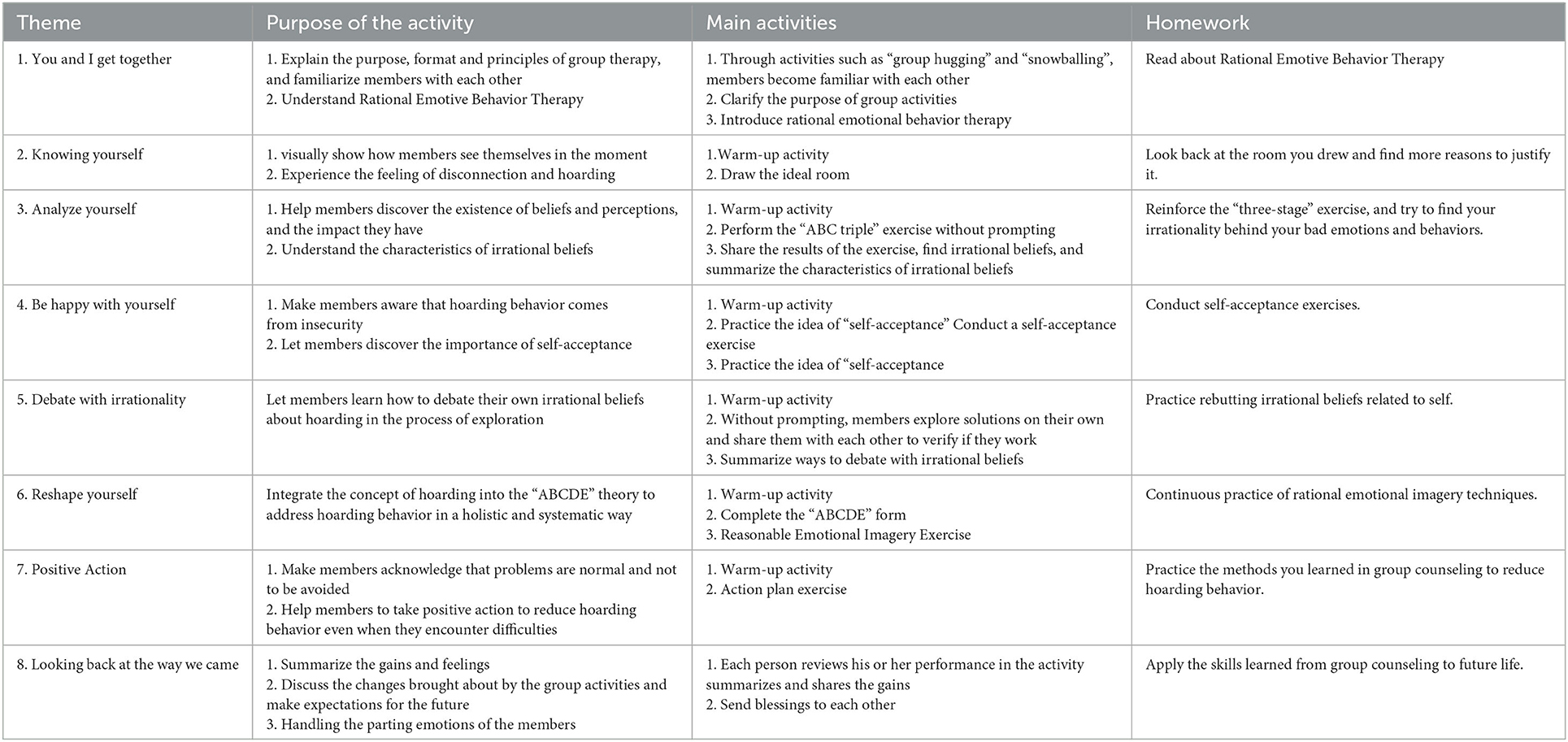
Table 2. Rational emotive behavior therapy intervention program.
Measures
Primary outcome measure
Saving inventory-revised (SI-R)
This study used the Chinese SI-R to measure hoarding (77, 78). The scale consists of 21 items (e.g., “How distressing do you find the task of throwing things away”) and is scored on a 5-point scale from 0 (not at all) to 4 (very much so). The scale includes two dimensions: acquisition-difficulty discarding and clutter. Total sum scores and the score of each dimension were calculated. The Cronbach's α for this study was 0.95.
Secondary outcome measures
Obsessive-compulsive symptom scale (OCSS)
As hoarding has been considered a subtype of OCD (1), obsessive-compulsive symptoms were measured as a secondary outcome. The OCSS is a Chinese scale (79) with 18 items (e.g., “Washing hands frequently and more often and for a longer time than the average person.”) and is scored on a 5-point scale from 1 (not at all) to 5 (always). Total sum scores were used. The Cronbach's alpha coefficient for this study was 0.85.
Difficulties in emotion regulation scale (DERS)
The Chinese version of the DERS (80, 81) was used to measure individuals' difficulties in emotion regulation. The scale has 27 items (e.g., “When I'm upset, I feel guilty for feeling that way”) and is scored on a 4-point scale from 1 (not at all) to 4 (largely). Total sum scores were used. The Cronbach's alpha coefficient for this study was 0.86.
Experiences in close relationships inventory-attachment anxiety subscale (ECR)
The Chinese version of the ECR (82) was used to measure individuals' attachment anxiety for their relationship with their father, mother, best friend and romantic partner. The scale has 18 items (e.g., “I'm a little worried about losing my lover”) and is scored on a 7-point scale from 1 (strongly disagree) to 7 (strongly agree). Total sum scores were used. The Cronbach's alpha coefficient for this study was 0.94.
Depression anxiety stress scales (DASS-21)
The DASS-21 was designed to measure individual psychological distress, i.e., depression, anxiety, and stress (83). The revised Chinese version was applied in this study, with twenty-one items and three dimensions (84). A 4-point scale ranging from 0 (“did not apply to me”) to 3 (“applied to me very much”) is presented to each item, with higher scores indicating severe psychological distress. Total sum scores and the score of each dimension were calculated. Cronbach's alpha for the total scale and its subscales, i.e., depression, anxiety, and stress, were 0.84, 0.91, 0.85, and 0.82, respectively.
Process outcome measures
Acceptance and action questionnaire II (AAQ-II)
Psychological flexibility was assessed using the Chinese AAQ-II (85). This questionnaire included seven items (e.g., “I worry that I can't control my worries and feelings”) and was rated on a 7-point Likert scale ranging from 1 (never) to 7 (always). The scale has shown good reliability and validity in China (36). Higher AAQ scores indicate lower levels of psychological flexibility or higher levels of experienced avoidance. Total sum scores were used. In the present study, Cronbach's α was 0.89.
Cognitive fusion questionnaire (CFQ)
The CFQ is a 9-item scale that assesses cognitive confusion (86). The revised Chinese version with 9 items (e.g., “I tend to get very entangled in my thoughts”) was used in this study (87). The scale presents a 7-point response scale from 1 (never true) to 7 (always true). Higher scores indicate higher levels of cognitive confusion. Total sum scores were used. In this study, Cronbach's alpha was 0.96.
Statistical analyses
Data entry and statistical analysis were performed using SPSS 22.0. The success of the randomization process was first tested by running a one-way ANOVA to test for differences in pre-measure across the three groups (ACT group, REBT group, and control group). Then, analysis of covariance and Bonferroni post hoc comparisons were applied to determine the differences in post-measure across the three groups. Effect size was reported as η2 (0.04 = small effect; 0.25 = medium effect; 0.64 = large effect (88).
Simple mediation models were performed with psychological flexibility or cognitive fusion as the mediator, group condition (ACT/REBT vs. control) as the independent variable, baseline values of the outcome and mediator as covariates, and post-intervention values of the primary or secondary variable as the dependent variable. Mediation was examined with a bootstrapping method and the PROCESS macro for SPSS (89). Parameter estimates were based on 5,000 resamples, and 95% bias-corrected confidence intervals were computed to determine the statistical significance of indirect effects.
Results
One-way ANOVA results showed that there were no significant differences between the three groups on pre-measures regarding hoarding behaviors, psychological flexibility, cognitive fusion, OCD, negative affect, attachment anxiety, and difficulty in emotion regulation. However, each variable in the three groups differed significantly on the post-measures. For more details, they can be seen in Table 3.
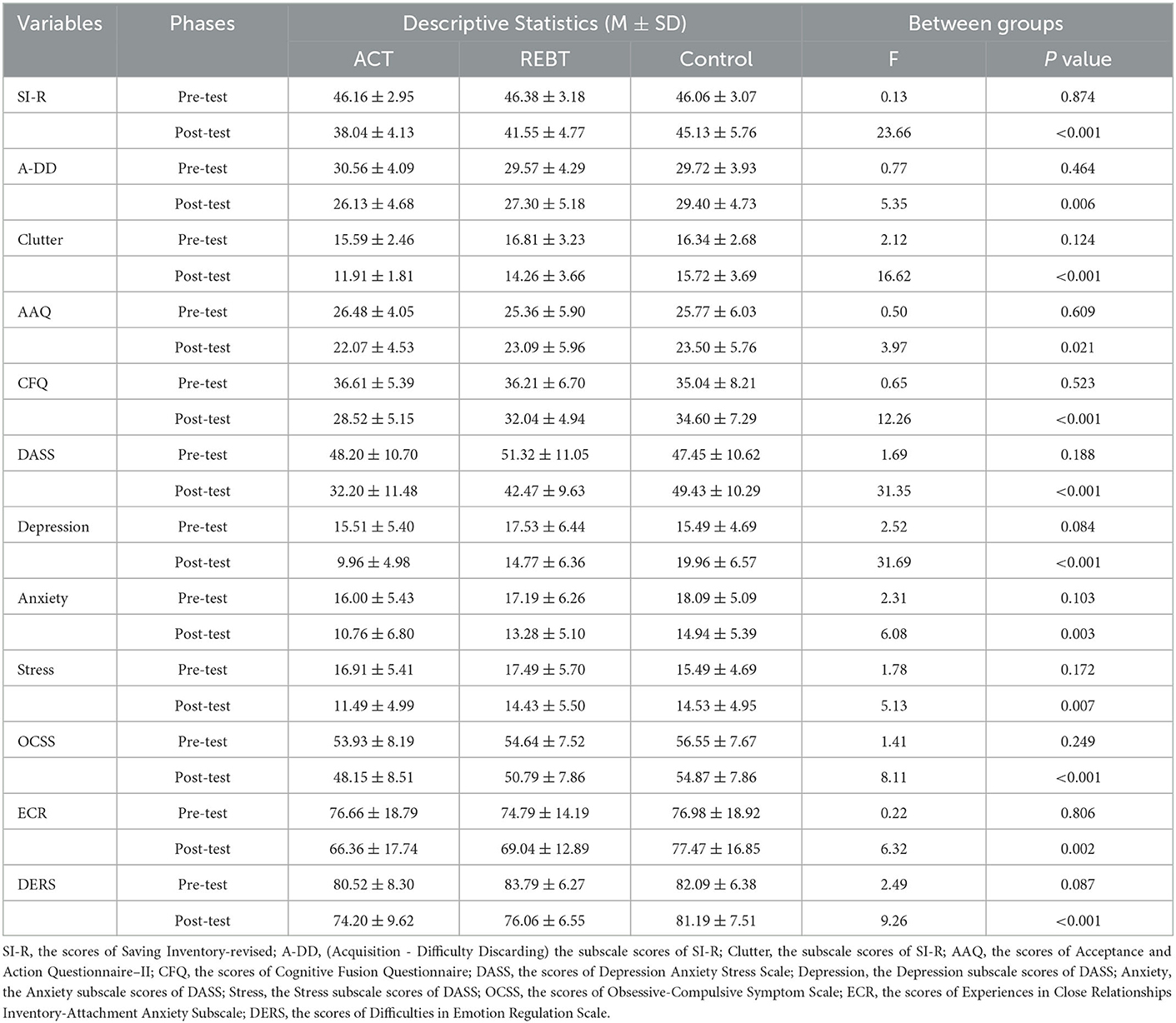
Table 3. Descriptive statistics and one-way ANOVA.
To accurately test and compare the differences in post-intervention between the three groups, posttest scores for each variable were used as the dependent variable, pretest scores were used as covariates, and the group was used as the independent variable for analysis of covariance and Bonferroni post-hoc comparisons. None of the interactions between the independent variables and the pretest scores of each outcome variable were significant, which satisfied the conditions of the analysis of covariance. The results indicated that hoarding behaviors, psychological flexibility, cognitive fusion, negative affect (depression, anxiety, and stress), OCD, attachment anxiety, and difficulties in emotion regulation differed significantly in all three groups, as shown in Table 4.
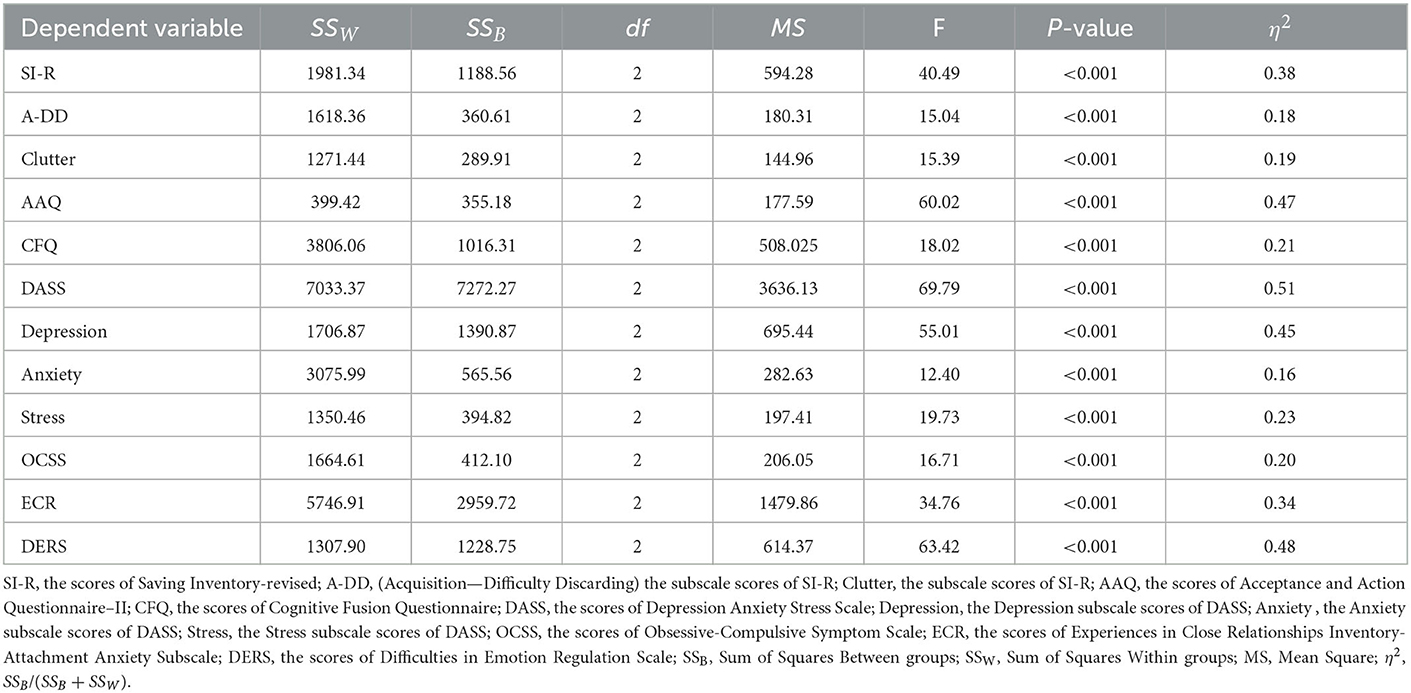
Table 4. The results of one-way ANCOVA.
Figures 2, 3 show the results of the Bonferroni post-hoc test for each outcome variable in the three groups. This result shows that after controlling for baseline levels of each variable, participants who received the ACT intervention and the REBT intervention showed significantly greater improvements in each outcome than those in the control group. In addition, the ACT group was significantly better than the REBT group in improving psychological flexibility and reducing hoarding (acquisition-difficulty discarding, clutter), cognitive fusion, negative affect (depression and stress), and OCD. However, for Anxiety (ACT vs. REBT, p = 0.220) and ECR-AA (ACT vs. REBT, p = 0.062), there was no significant difference in the effects of the two interventions.
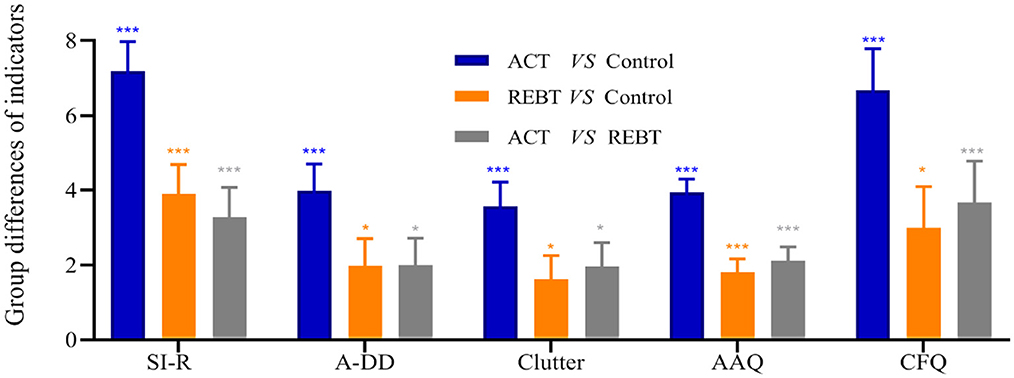
Figure 2. The results of Bonferroni's post hoc comparison (SI-R, A-DD, Clutter, AAQ, and CFQ). *p < 0.05; ***p < 0.001; Blue bar, Difference between ACT group and Control group; Orange bar, Difference between REBT group and Control group; Gray bar, Difference between ACT group and REBT group. SI-R, the scores of Saving Inventory-revised; A-DD, (Acquisition-Difficulty Discarding) the subscale scores of SI-R; Clutter, the subscale scores of SI-R; AAQ, the scores of Acceptance and Action Questionnaire–II; CFQ, the scores of Cognitive Fusion Questionnaire.
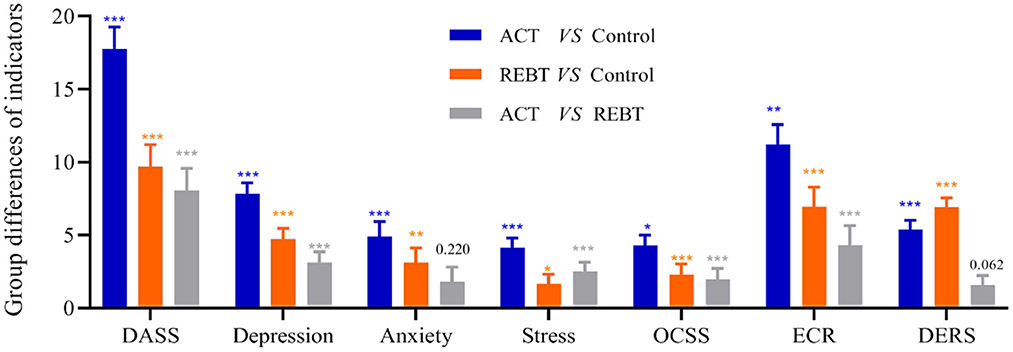
Figure 3. The results of Bonferroni's post hoc comparison (DASS, Depression, Anxiety, Stress, OCSS, ECR, and DERS). *p < 0.05; **p < 0.01; ***p < 0.001; DASS, the scores of Depression Anxiety Stress Scale; Depression, the Depression subscale scores of DASS; Anxiety, the Anxiety subscale scores of DASS; Stress, the Stress subscale scores of DASS; OCSS, the scores of Obsessive-Compulsive Symptom Scale; ECR, the scores of Experiences in Close Relationships Inventory-Attachment Anxiety Subscale; DERS, the scores of Difficulties in Emotion Regulation Scale.
The results of the mediation analyses showed that the treatment condition indirectly influenced hoarding behaviors (SI-R), negative affect (DASS), and attachment anxiety (ECR-AA) through its effect on psychological flexibility (AAQ-II) but not through the cognitive fusion change process (CFQ). As seen in Table 5, however, psychological flexibility does not mediate the effect of treatment conditions on OCD and difficulties in emotion regulation. The indirect effect of treatment condition on hoarding behaviors, negative affect, and attachment anxiety through AAQ-II was, respectively estimated as −1.48 (SE = 0.63, 95% CI: −2.84 −0.37), −3.49 (SE = 1.16, 95% CI: −6.14, −1.62),−2.16 (SE = 0.82, 95% CI: −3.98, −0.83), indicating that hoarding behaviors, negative affect, and attachment anxiety among participants in ACT/REBT were, on average, 1.48, 3.49, and 2.16 units lower than that of participants in the control group as a result of the indirect effect through psychological flexibility. The bias-corrected bootstrap confidence intervals for the indirect effects of psychological flexibility based on 5,000 bootstrap samples did not contain zero, suggesting that these effects were significant.
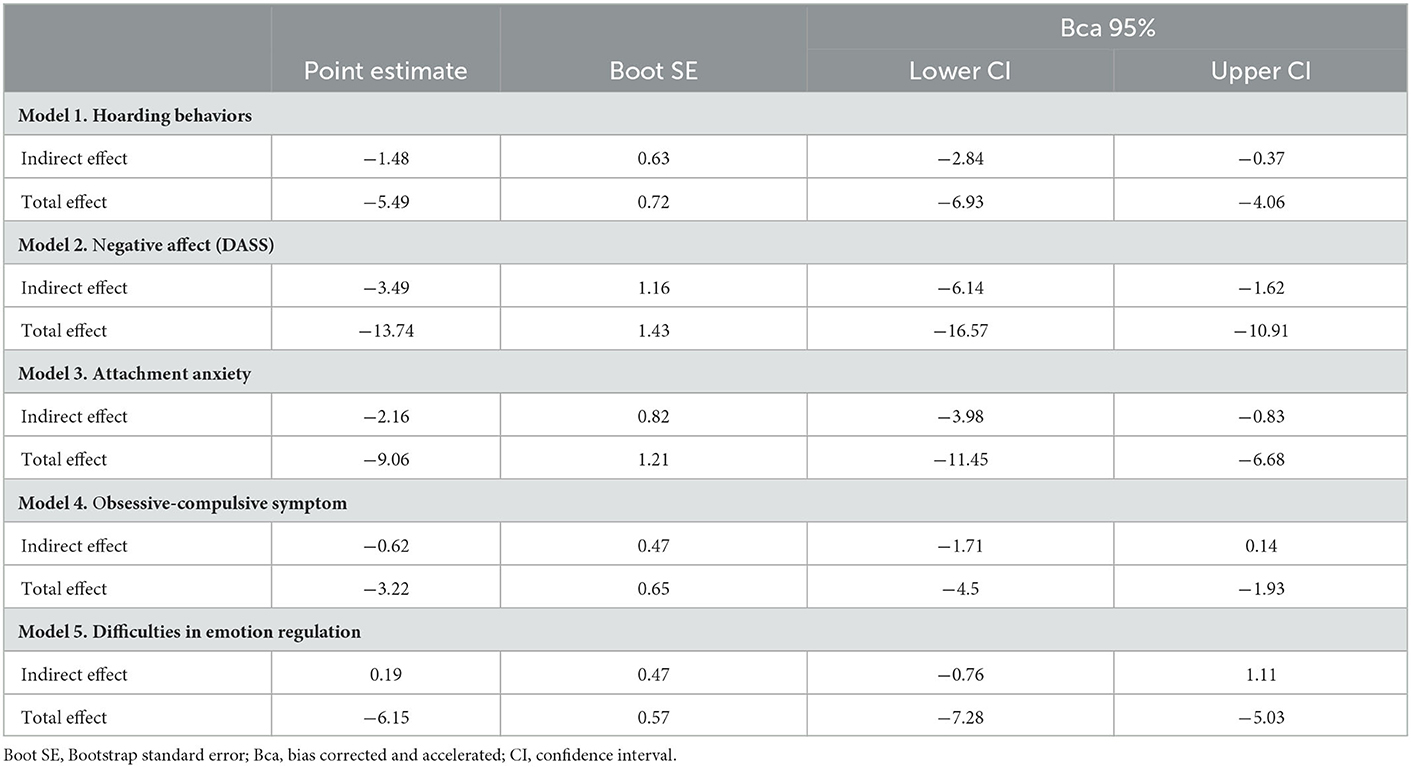
Table 5. The specific indirect effects of the intervention on each outcome measure through changes in psychological flexibility.
Discussion
In this study, ACT and REBT were found to reduce hoarding compared to the control group. Specifically, ACT and REBT improved individuals' psychological flexibility and reduced cognitive fusion, acquisition-difficulty discarding, clutter, negative affect (anxiety, depression, stress), attachment anxiety, obsessive-compulsive disorder, and difficulty in emotion regulation. In addition, ACT was more effective than REBT in improving psychological flexibility and reducing hoarding, cognitive fusion, depression, stress, and obsessive-compulsive disorder; there were no significant differences between the two in anxiety and emotion regulation difficulties. Finally, psychological flexibility is a mediator of the effect of ACT and REBT on some behavioral and psychological outcomes (hoarding behaviors, negative affect, attachment anxiety).
ACT has been found to alleviate individuals' OCD (90, 91), negative affect (92–94), hoarding (66, 67), difficulties with emotion regulation (95, 96), and attachment anxiety (97), which are consistent with the findings of the present study. According to the cognitive model of hoarding, the performance of hoarding stems from various avoidance behaviors (3, 30). Patterns of behavioral avoidance have been observed in most hoarding patients (25, 98). Additionally, the primary goal of ACT is to reduce cognitive fusion and experiential avoidance and increase psychological flexibility so that individuals can reduce their avoidance behaviors and act in accordance with their values (32, 36, 58).
Previous studies have suggested that other therapies can also affect psychological flexibility, including other forms of CBT, such as exposure and response/or ritual prevention (99, 100), which is also consistent with our study. The present study found that REBT, as a form of CBT, can increase psychological flexibility and reduce cognitive fusion. Theoretical studies of hoarding have found that irrational perceptions of possessions are an important cause of hoarding (3). REBT focuses on a person's irrational beliefs, which is consistent with the mechanisms that produce hoarding. The most distinctive feature of REBT is that it helps individuals change their rigid and extreme beliefs to flexible and non-extreme beliefs (101) with various cognitive skills (49, 52). However, cognitive skills need to be practiced continuously (102, 103). People may be negligent in performing cognitive practice, making it less useful than ACT for improving psychological flexibility. This may explain why ACT is more effective in improving psychological flexibility and reducing hoarding, cognitive fusion, depression, stress, and OCD.
Additionally, some studies focusing on mechanisms of change have suggested that the effect of ACT or CBT on outcome variables is mediated by its impact on psychological flexibility (68–70, 104). The present study also found that psychological flexibility played a mediating role in the efficacy of ACT/REBT on the outcome variables (i.e., hoarding behaviors, negative affect, and attachment anxiety). Psychological flexibility, as a fundamental aspect of health, is a cornerstone of healthy personal and social functioning and one of the foremost goals of human existence (105). Empirical research has shown that psychological flexibility is implicated in a variety of psychopathological and functional outcomes (106). Models of developmental psychopathology (107) and theories of mechanisms of change in psychotherapy (108) conclude that psychological flexibility in emotion, behavior, and cognition predicts successful psychosocial adjustment and treatment (106). Therefore, enhancing psychological flexibility is a primary mechanism by which evidence-based psychotherapies produce adaptive behavioral change and related outcomes (39, 109, 110).
The present study did not find a mediating role of cognitive fusion. Future research should explore the possible mediating roles of other process variables in the effects of various forms of CBT on psychological and behavioral outcomes related to hoarding. Such process-based research may be better able to distill potent components from ACT and other formats of CBT to develop a coherent intervention framework for hoarding in the service of streamlining treatment development, dissemination, and implementation (66, 111).
There are some limitations in this study. The present study did not carry out follow-up measures to examine the durability of the effects of the intervention study, and there is a lack of follow-up studies on the stability of the intervention effect. Second, this study measured psychological flexibility using the Acceptance and Action Questionnaire II (AAQ-II), which measures only one dimension of psychological flexibility (112, 113). In addition, all studies were based on self-reported data. Given these limitations, the findings from this study should be interpreted with caution. Because of the theoretical importance of hoarding behaviors in current psychological models, further research is needed to reveal neural mechanisms associated with the cognitive representation of hoarding behaviors pre- and post-interventions. Future research is needed to explore the effects of other forms of CBT-based group interventions (e.g., mindfulness-based stress reduction, mindfulness-based cognitive therapy or dialectical behavioral therapy) on hoarding behaviors and the neural mechanisms involved.
Overall, current findings provide preliminary support for the efficacy of ACT and REBT for hoarding and associated impairment in China. We found that ACT was more effective than REBT in improving psychological flexibility and reducing hoarding, cognitive fusion, depression, stress, and obsessive-compulsive disorder. Furthermore, this study examined the mediating role of psychological flexibility as a process variable. A test of mediating effects would be helpful in understanding the mechanisms of CBT in non-Western countries and the role of psychological flexibility in individual psychological and behavioral changes.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Anhui Normal University. The participants provided their written informed consent to participate in this study.
Author contributions
SF: conceptualization, methodology, supervision, design experiments, validation, data collection, data curation, formal analysis, visualization, writing—original draft, writing—review and editing, and project administration. DD: design experiments, formal analysis, writing—original draft, and writing—review and editing. RZ: design experiments, implementation of experiments, data collection, data curation, formal analysis, and writing—original draft. MH: design experiments, implementation of experiments, data collection, data curation, formal analysis, visualization, and writing—original draft. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by Philosophy and Social Science Planning Key Project of Anhui Province (grant number AHSKZ2020D37).
Acknowledgments
We would like to thank the support of Anhui Provincial Women's Federation and Anhui Provincial Department of Education 2022 Annual Women's Theory Research Key Project (2022-FNYJ-002), Open Fund Project of Key Laboratory of Philosophy and Social Science of Anhui Province on Adolescent Mental Health and Crisis Intelligence Intervention, The University Synergy Innovation Program of Anhui Province (GXXT-2022-101), and Anhui Topnotch Talents of Disciplines in Universities and colleges (SF).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wheaton MG. Understanding and treating hoarding disorder: a review of cognitive-behavioral models and treatment. J Obses Compuls Relat Disord. (2016) 9:43–50. doi: 10.1016/j.jocrd.2016.02.006
2. APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed. Arlington, VA: American Psychiatric Publishing, Inc (2013).
3. Frost RO, Hartl TL. A cognitive-behavioral model of compulsive hoarding. Behav Res Ther. (1996) 34:341–50. doi: 10.1016/0005-7967(95)00071-2
4. Nordsletten AE, Reichenberg A, Hatch SL, de la Cruz LF, Pertusa A, Hotopf M, et al. Epidemiology of hoarding disorder. Br J Psychiatry. (2013) 203:445–52. doi: 10.1192/bjp.bp.113.130195
5. Zheng Y, Liu D. A survey of hoarding phenomenon and its influencing factors among Chinese college students. Chin J Public Health. (2020) 36:1474–7. doi: 10.11847/zgggws1124563
6. Frost RO, Steketee G, Williams L. Hoarding: a community health problem. Health Soc Care Commun. (2000) 8:229–34. doi: 10.1046/j.1365-2524.2000.00245.x
7. Drury H, Ajmi S, Fernandez, de la Cruz L, Nordsletten AE, Mataix-Cols D. Caregiver burden, family accommodation, health, and well-being in relatives of individuals with hoarding disorder. J Affect Disord. (2014) 159:7–14. doi: 10.1016/j.jad.2014.01.023
8. Tolin DF, Frost RO, Steketee G, Gray KD, Fitch KE. The economic and social burden of compulsive hoarding. Psychiatry Res. (2008) 160:200–11. doi: 10.1016/j.psychres.2007.08.008
9. Blom RM, Samuels JF, Grados MA, Chen Y, Bienvenu J, Riddle MA, et al. Cognitive functioning in compulsive hoarding. J Anx Disord. (2011) 25:1139–44. doi: 10.1016/j.janxdis.2011.08.005
10. Mackin RS, Vigil O, Insel P, Kivowitz A, Kupferman E, Hough CM, et al. Patterns of clinically significant cognitive impairment in hoarding disorder. Depress Anx. (2016) 33:211–8. doi: 10.1002/da.22439
11. Ayers CR, Dozier ME, Wetherell JL, Twamley EW, Schiehser DM. Executive functioning in participants over age of 50 with hoarding disorder. Am J Geriat Psychiatry. (2016) 24:342–49. doi: 10.1016/j.jagp.2015.10.009
12. Steketee G, Frost R. Compulsive hoarding: current status of the research. Clin Psychol Rev. (2003) 23:905–27. doi: 10.1016/j.cpr.2003.08.002
13. Tolin DF, Levy HC, Wootton BM, Hallion LS, Stevens MC. Hoarding disorder and difficulties in emotion regulation. J Obsessive Compuls Relat Disord. (2018) 16:98–103. doi: 10.1016/j.jocrd.2018.01.006
14. Grisham JR, Martyn C, Kerin F, Baldwin PA, Norberg MM. Interpersonal functioning in hoarding disorder: an examination of attachment styles and emotion regulation in response to interpersonal stress. J Obses Compul Relat Disord. (2018) 16:43–9. doi: 10.1016/j.jocrd.2017.12.001
15. Medard E, Kellett S. The role of adult attachment and social support in hoarding disorder. Behav Cogn Psychother. (2013) 42:629–33. doi: 10.1017/S1352465813000659
16. Yap K, Grisham JR. Object attachment and emotions in hoarding disorder. Compr Psychiatry. (2020) 100:152179. doi: 10.1016/j.comppsych.2020.152179
17. Yap K, Eppingstall J, Brennan C, Le B, Grisham JR. Emotional attachment to objects mediates the relationship between loneliness and hoarding symptoms. J Obsessive Compuls Relat Disord. (2020) 24:100487. doi: 10.1016/j.jocrd.2019.100487
18. Grisham JR, Barlow DH. Compulsive hoarding: current research and theory. J Psychopathol Behav Assess. (2005) 27:45–52. doi: 10.1007/s10862-005-3265-z
19. Dozier M, Bernard K. Attachment and Biobehavioral Catch-up: addressing the needs of infants and toddlers exposed to inadequate or problematic caregiving. Curr Opinion Psychol. (2017) 15:111–7. doi: 10.1016/j.copsyc.2017.03.003
20. Neave N, Tyson H, McInnes L, Hamilton C. The role of attachment style and anthropomorphism in predicting hoarding behaviors in a non-clinical sample. Personal Individ Diff . (2016) 99:33–7. doi: 10.1016/j.paid.2016.04.067
21. Liu X, Cai Y, Tao Y, Hou W, Niu H, Liu X, et al. Association between attachment and hoarding behavior: Mediation of anthropomorphism and moderation of hoarding beliefs among Chinese adolescents. Psych J. (2022) 3:610. doi: 10.1002./pchj.610
22. Jia Y, Zhang S, Jin T, Zhang L, Zhao S, Li Q, et al. Effect of attachment anxiety on hoarding behaviour of college students: mediating role of intolerance of uncertainty and experiential avoidance. Psychol Develop Educ. (2019) 35:393–400. doi: 10.16187/j.cnki.issn1001-4918.2019.04.02
23. Jazaieri H, Morrison AS, Goldin PR, Gross JJ. The role of emotion and emotion regulation in social anxiety disorder. Curr Psychiatry Rep. (2014) 17:531. doi: 10.1007/s11920-014-0531-3
24. Shaw AM, Timpano KR, Steketee G, Tolin DF, Frost RO. Hoarding and emotional reactivity: the link between negative emotional reactions and hoarding symptomatology. J Psychiatr Res. (2015) 63:84–90. doi: 10.1016/j.jpsychires.2015.02.009
25. Fernández de la, Cruz L, Landau D, Iervolino AC, Santo S, Pertusa A, et al. Experiential avoidance and emotion regulation difficulties in hoarding disorder. J Anxiety Disord. (2013) 27:204–9. doi: 10.1016/j.janxdis.2013.01.004
26. Akbari M, Seydavi M, Mohammadkhani S, Turchmanovych N, Chasson GS, Majlesi N, et al. Emotion dysregulation and hoarding symptoms: a systematic review and meta-analysis [Review]. J Clin Psychol. (2022) 78:1341–53. doi: 10.1002/jclp.23318
27. Barton ALJ, Johns L, Salkovskis P. Are self-reported difficulties in emotional regulation associated with hoarding? a systematic review. J Obsess Compul Relat Disord. (2021) 30:100660. doi: 10.1016/j.jocrd.2021.100660
28. Yap K, Mogan C, Moriarty A, Dowling N, Blair-West S, Gelgec C, et al. Emotion regulation difficulties in obsessive-compulsive disorder. J Clin Psychol. (2018) 74:695–709. doi: 10.1002/jclp.22553
29. Raines AM, Boffa JW, Allan NP, Short NA, Schmidt NB. Hoarding and eating pathology: the mediating role of emotion regulation. Compr Psychiatry. (2015) 57:29–35. doi: 10.1016/j.comppsych.2014.11.005
30. Frost RO, Steketee G, Tolin DF. Comorbidity in hoarding disorder. Depress Anxiety. (2011) 28:876–84. doi: 10.1002/da.20861
31. Timpano KR, Shaw AM, Cougle JR, Fitch KE. A multifaceted assessment of emotional tolerance and intensity in hoarding. Behav Ther. (2014) 45:690–9. doi: 10.1016/j.beth.2014.04.002
32. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Therapy. (2006) 44:1–25. doi: 10.1016/j.brat.2005.06.006
33. Hayes SC, Pistorello J, Levin ME. Acceptance and commitment therapy as a unified model of behavior change. Counsel Psychol. (2012) 40:976–1002. doi: 10.1177/0011000012460836
34. Levin ME, Luoma JB, Vilardaga R, Lillis J, Nobles R, Hayes SC, et al. Examining the role of psychological inflexibility, perspective taking, and empathic concern in generalized prejudice. J Appl Soc Psychol. (2016) 46:180–91. doi: 10.1111/jasp.12355
35. Hayes SC. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies—Republished article. Behav Therapy. (2016) 47:869–85. doi: 10.1016/j.beth.2016.11.006
36. Fang S, Ding D. The efficacy of group-based acceptance and commitment therapy on psychological capital and school engagement: a pilot study among Chinese adolescents. J Context Behav Sci. (2020) 16:134–43. doi: 10.1016/j.jcbs.2020.04.005
37. Daks JS, Rogge RD. Examining the correlates of psychological flexibility in romantic relationship and family dynamics: a meta-analysis. J Context Behav Scie. (2020) 18:214–38. doi: 10.1016/j.jcbs.2020.09.010
38. Garner EV, Golijani-Moghaddam N. Relationship between psychological flexibility and work-related quality of life for healthcare professionals: a systematic review and meta-analysis. J Context Behav Sci. (2021) 21:98–112. doi: 10.1016/j.jcbs.2021.06.007
39. Fang S, Ding D. Which outcome variables are associated with psychological inflexibility/flexibility for chronic pain patients? A three level meta-analysis. Front Psychol. (2022) 13:1069748. doi: 10.3389/fpsyg.2022.1069748
40. Timpano KR, Buckner JD, Richey JA, Murphy DL, Schmidt NB. Exploration of anxiety sensitivity and distress tolerance as vulnerability factors for hoarding behaviors. Depress Anxiety. (2009) 26:343–53. doi: 10.1002/da.20469
41. Ayers CR, Castriotta N, Dozier ME, Espejo EP, Porter B. Behavioral and experiential avoidance in patients with hoarding disorder. J Behav Ther Exp Psychiatry. (2014) 45:408–14. doi: 10.1016/j.jbtep.2014.04.005
42. Krafft J, Ong CW, Twohig MP, Levin ME. Assessing psychological inflexibility in hoarding: the acceptance and action questionnaire for hoarding (AAQH). Journal of Context Behav Scie. (2019) 12:234–42. doi: 10.1016/j.jcbs.2018.08.003
43. Ong CW, Krafft J, Levin ME, Twohig MP. An examination of the role of psychological inflexibility in hoarding using multiple mediator models. J Cogn Psychother. (2018) 32:97–111. doi: 10.1891/0889-8391.32.2.97
44. Bodryzlova Y, Audet JS, Bergeron K, O'Connor K. Group cognitive-behavioral therapy for hoarding disorder: systematic review and meta-analysis. Health Soc Care Commun. (2019) 27:517–30. doi: 10.1111/hsc.12598
45. Rodgers N, McDonald S, Wootton BM. Cognitive behavioral therapy for hoarding disorder: An updated meta-analysis. J Affect Disord. (2021) 290:128–35. doi: 10.1016/j.jad.2021.04.067
46. Tolin DF, Frost RO, Steketee G, Muroff J. Cognitive behavioral therapy for hoarding disorder: a meta-analysis. Depress Anxiety. (2015) 32:158–66. doi: 10.1002/da.22327
47. Hayes SC, Hofmann SG. The third wave of CBT and the rise of process based care. World Psychiatry. (2017) 16:245–6. doi: 10.1002/wps.20442
48. Márquez-González M, Romero-Moreno R, Cabrera I, Olmos R, Pérez-Miguel A, Losada A, et al. Tailored vs. manualized interventions for dementia caregivers: the functional analysis-guided modular intervention. Psychol Aging. (2020) 35:41–54. doi: 10.1037/pag0000412
49. Ellis A. Can rational emotive behavior therapy (REBT) be effectively used with people who have devout beliefs in God and religion? Prof Psychol Res Pract. (2000) 31:29–33. doi: 10.1037/0735-7028.31.1.29
51. Outar L, Turner MJ, Wood AG, Lowry R. “I need to go to the gym”: exploring the use of rational emotive behavior therapy upon exercise addiction, irrational and rational beliefs. Perform Enhanc Health. (2018) 6:82-93. doi: 10.1016/j.peh.2018.05.001
52. MacInnes D. The theories underpinning rational emotive behavior therapy: where's the supportive evidence? Int J Nurs Stud. (2004) 41:685–95. doi: 10.1016/j.ijnurstu.2004.02.004
53. David D, Cotet C, Matu S, Mogoase C, Stefan S. 50 years of rational-emotive and cognitive-behavioral therapy: a systematic review and meta-analysis. J Clin Psychol. (2018) 74:304–18. doi: 10.1002/jclp.22514
54. Iftene F, Predescu E, Stefan S, David D. Rational-emotive and cognitive-behavior therapy (REBT/CBT) vs. pharmacotherapy vs. REBT/CBT plus pharmacotherapy in the treatment of major depressive disorder in youth; a randomized clinical trial. Psychiatry Res. (2015) 225:687–94. doi: 10.1016/j.psychres.2014.11.021
55. Mersch PPA. The treatment of social phobia: The differential effectiveness of exposure in vivo and an integration of exposure in vivo, rational emotive therapy, and social skills training. Behav Res Ther. (1995) 33:259–69. doi: 10.1016/0005-7967(94)00038-L
56. Yu HW, Huang YJ, Ma WF. Nursing experience with reconstructing self-control using rational-emotive behavior therapy on a patient with schizophrenia and obsessive-compulsive symptoms. Hu li za zhi J Nurs. (2018) 65:112–119. doi: 10.6224/jn.201810_65(5).14
57. Ellis A. Rational emotive behavior therapy approaches to obsessive-compulsive disorder (OCD). J Rat Emot Cognit Behav Therapy. (1994) 12:121–41. doi: 10.1007/BF02354608
58. Fang S, Ding D, Ji P, Huang M, Hu K. Cognitive defusion and psychological flexibility predict negative body image in the chinese college students: evidence from acceptance and commitment therapy. Int J Environ Res Public Health. (2022) 19:16519. doi: 10.3390/ijerph192416519
59. Mathews CA, Uhm S, Chan J, Gause M, Franklin J, Plumadore J, et al. Treating hoarding disorder in a real-world setting: results from the mental health association of San Francisco. Psychiatry Res. (2016) 237:331–8. doi: 10.1016/j.psychres.2016.01.019
60. A-Tjak JGL, Davis ML, Morina N, Powers MB, Smits JA, Emmelkamp PMG. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychotherapy Psychosomat. (2015) 84:30–6. doi: 10.1159/000365764
61. Fang S, Ding D. A meta-analysis of the efficacy of acceptance and commitment therapy for children. J Context Behav Sci. (2020) 15:225–34. doi: 10.1016/j.jcbs.2020.01.007
62. Wang J, Fang S. Effects of internet-based acceptance and commitment therapy (IACT) on adolescents: a systematic review and meta-analysis. Int J Mental Health Promot. (2023):25304. doi: 10.32604/ijmhp.2023.025304
63. Juarascio A, Shaw J, Forman E, Timko CA, Herbert J, Butryn M, et al. Acceptance and commitment therapy as a novel treatment for eating disorders:an initial test of efficacy and mediation. Behav Modif. (2013) 37:459–89. doi: 10.1177/0145445513478633
64. Twohig MP. The application of acceptance and commitment therapy to obsessive-compulsive disorder. Cognit Behav Pract. (2009) 16:18–28. doi: 10.1016/j.cbpra.2008.02.008
65. Heffner JL, McClure JB, Mull KE, Anthenelli RM, Bricker JB. Acceptance and commitment therapy and nicotine patch for smokers with bipolar disorder: preliminary evaluation of in-person and telephone-delivered treatment. Bipolar Disord. (2015) 17:560–6. doi: 10.1111/bdi.12300
66. Ong CW, Krafft J, Panoussi F, Petersen JM, Levin ME, Twohig MP, et al. In-person and online-delivered acceptance and commitment therapy for hoarding disorder: a multiple baseline study. J Context Behav Sci. (2021) 20:108–17. doi: 10.1016/j.jcbs.2021.02.001
67. Krafft J. Testing an Acceptance and Commitment Therapy Website for Hoarding: A Randomized Waitlist-Controlled Trial [Doctoral dissertation, Utah State University]. (2021). Available inline at: https://digitalcommons.usu.edu/etd/8188
68. Åkerblom S, Perrin S, Rivano Fischer M, McCracken LM. Predictors and mediators of outcome in cognitive behavioral therapy for chronic pain: the contributions of psychological flexibility. J Behav Med. (2021) 44:111–22. doi: 10.1007/s10865-020-00168-9
69. Larsson A, Hartley S, McHugh L. A randomised controlled trial of brief web-based acceptance and commitment therapy on the general mental health, depression, anxiety and stress of college Students. J Context Behav Sci. (2022) 24:10–7. doi: 10.1016/j.jcbs.2022.02.005
70. Ruiz FJ. A review of Acceptance and Commitment Therapy (ACT) empirical evidence: Correlational, experimental psychopathology, component and outcome studies. Int J Psychol Psychol Therapy. (2010) 10:125–62.
71. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences [journal article]. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
72. Zhang L, Bao Q, Chen L, Liang Y. Dynamic adaptation of the Inventory of Piaget's Developmental task (IPDT) and the application for children with low socioeconomic status. Acta Psychol Sin. (2021) 53:960–75. doi: 10.3724/SP.J.1041.2021.00960
73. Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, 2nd ed. New York, NY: Guilford Press. (2012).
74. Fang S, Wang W. Act in practice: Case Conceptualization in Acceptance and Commitment Therapy. Chongqing: Chongqing University Press (2011).
75. Ellis A. How to Make Yourself Happy and Remarkably Less Disturbable. Beijing: China Renmin University Press (2010).
77. Frost RO, Steketee G, Grisham J. Measurement of compulsive hoarding: saving inventory-revised. Behav Res Ther. (2004) 42:1163–82. doi: 10.1016/j.brat.2003.07.006
78. Tang T, Wang J, Tang S, Zhao L. Psychometric properties of the saving inventory-revised in Chinese university students sample. Chin J Clin Psychol. (2012) 20:21–4. doi: 10.16128/j.cnki.1005-3611.2012.01.006
79. Qi X, Wu M, Yang J, Fang G, Luo Q, Chen L. Analysis of obsessive-compulsive symptom of fresh men scale. Chin J Clin Psychol. (2005) 13:25–7. doi: 10.16128/j.cnki.1005-3611.2005.01.007
80. Gratz KL, Roemer L. multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. (2004) 26:41–54. doi: 10.1023/B:JOBA.0000007455.08539.94
81. Feng Y. The Relation of Adolecents' Self-Harm Behaviors, Individual Emotion Characteristics and Family Environment Factors [Master degree, Central China Normal University] (2008).
82. Li T, Kato K. Measuring adult attachment: chinese adaptation of the ECR Scale. Acta Psychol Sin. (2006) 38:399–406.
83. Antony MM, Bieling PJ, Cox, BJ, Enns MW, Swinson RP. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol Assess. (1998) 10:176–181. doi: 10.1037/1040-3590.10.2.176
84. Gong X, Xie X, Rui X, Yue-Jia L. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chin J Clin Psychol. (2010) 18:443–7. doi: 10.16128/j.cnki.1005-3611.2010.04.020
85. Cao J, Ji Y, Zhu Z. Reliability and validity of the chinese version of the acceptance and action questionnaire-second edition (AAQ-II) in college students. Chin Ment Health J. (2013) 27:873–7. doi: 10.3969/j.issn.1000-6729.2013.11.014
86. Gillanders DT, Bolderston H, Bond FW, Dempster M, Flaxman PE, Campbell L, et al. The development and initial validation of the cognitive fusion questionnaire. Behav Ther. (2014) 45:83–101. doi: 10.1016/j.beth.2013.09.001
87. Zhang W, Ji Y, Li X, Guo H, Zhu Z. Reliability and validity of the chinese version of the cognitive fusion questionnaire. Chin Ment Health J. (2014) 28:40–6. doi: 10.3969/j.issn.1000-6729.2014.01.007
88. Ferguson CJ. An effect size primer: a guide for clinicians and researchers. Profess Psychol Res Practice. (2009) 40:532–8. doi: 10.1037/a0015808
89. Hayes AF. Process: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling [White paper]. (2012). Available online at: http://www.afhayes.com/public/process2012.pdf
90. Twohig MP, Hayes SC, Masuda A. Increasing willingness to experience obsessions: acceptance and commitment therapy as a treatment for obsessive-compulsive disorder. Behav Ther. (2006) 37:3–13. doi: 10.1016/j.beth.2005.02.001
91. Twohig MP, Hayes SC, Plumb JC, Pruitt LD, Collins AB, Hazlett-Stevens H, et al. A randomized clinical trial of acceptance and commitment therapy vs. progressive relaxation training for obsessive-compulsive disorder. J Consult Clin Psychol. (2010) 78:705–16. doi: 10.1037/a0020508
92. French K, Golijani-Moghaddam N, Schröder T. What is the evidence for the efficacy of self-help acceptance and commitment therapy? A systematic review and meta-analysis. J Contex Behav Sci. (2017) 6:360–74. doi: 10.1016/j.jcbs.2017.08.002
93. Lønfeldt NN, Silverman WK, Esbjørn BH. A systematic review and meta-analysis of the association between third-wave cognitive constructs and youth anxiety. Int J Cogn Therapy. (2017) 10:115–37. doi: 10.1521/ijct.2017.10.2.115
94. Haller H, Breilmann P, Schroter M, Dobos G, Cramer H. A systematic review and meta-analysis of acceptance- and mindfulness-based interventions for DSM-5 anxiety disorders. Sci Rep. (2021) 11:20385. doi: 10.1038./s41598-021-99882-w
95. Amirian K, Mami S, Ahmadi V, Mohamadzadeh J. Effectiveness of group psychotherapy based on acceptance and commitment therapy on difficultes emotion regulation and distress tolerance in substance abusers. J Edu Commun Health. (2018) 5:53–61. doi: 10.21859/jech.5.2.53
96. Joda A, Saed O, Mohammadi bytamar J, Zenoozian S, Fayegh Y. The efficacy of group acceptance and commitment therapy on reducing academic procrastination and improving difficulty in emotion regulation: a randomized clinical trial. Scien J Kurdistan Univ Med Sci. (2018) 23:66–78.
97. A-Tjak JGL, Morina N, Boendermaker WJ, Topper M, Emmelkamp PM. Explicit and implicit attachment and the outcomes of acceptance and commitment therapy and cognitive behavioral therapy for depression. BMC Psychiatry. (2020) 20:155. doi: 10.1186./s12888-020-02547-7
98. Frost RO, Steketee G. Issues in the treatment of compulsive hoarding. Cogn Behav Pract. (1999) 6:397–407. doi: 10.1016/S1077-7229(99)80058-3
99. Thompson BL, Twohig MP, Luoma JB. Psychological flexibility as shared process of change in acceptance and commitment therapy and exposure and response prevention for obsessive-compulsive disorder: a single case design study. Behav Ther. (2021) 52:286–97. doi: 10.1016/j.beth.2020.04.011
100. Twohig MP, Abramowitz JS, Smith BM, Fabricant LE, Jacoby RJ, Morrison KL, et al. Adding acceptance and commitment therapy to exposure and response prevention for obsessive-compulsive disorder: a randomized controlled trial. Behav Res Ther. (2018) 108:1–9. doi: 10.1016/j.brat.2018.06.005
101. Dryden, W. The Distinctive Features of Rational Emotive Behavior Therapy. In M. E. Bernard and W. Dryden (Eds.), Advances in REBT: Theory, Practice, Research, Measurement, Prevention and Promotion. Springer International Publishing (2019) (pp. 23-46). doi: 10.1007./978-3-319-93118-0_2
102. Gunzenhauser C, Nuckles M. Training executive functions to improve academic achievement: tackling avenues to far transfer. Front Psychol. (2021) 12:624008. doi: 10.3389/fpsyg.2021.624008
103. Renkl A, Mandl H, Gruber H. Inert knowledge: analyses and remedies. Educ Psychol. (1996) 31:115–21. doi: 10.1207/s15326985ep3102_3
104. Stockton D, Kellett S, Berrios R, Sirois F, Wilkinson N, Miles G, et al. Identifying the underlying mechanisms of change during acceptance and commitment therapy (ACT): a systematic review of contemporary mediation studies. Behav Cogn Psychother. (2019) 47:332–62. doi: 10.1017/S1352465818000553
105. Kashdan TB, Rottenberg J. Psychological flexibility as a fundamental aspect of health. Clin Psychol Rev. (2010) 30:865–78. doi: 10.1016/j.cpr.2010.03.001
106. Cherry KM, Hoeven EV, Patterson TS, Lumley MN. Defining and measuring “psychological flexibility”: a narrative scoping review of diverse flexibility and rigidity constructs and perspectives. Clin Psychol Rev. (2021) 84:101973. doi: 10.1016/j.cpr.2021.101973
107. Cole PM, Michel MK, Laureen O'Donnell T. The development of emotion regulation and dysregulation: a clinical perspective. Monographs Soc Res Child Develop. (1994) 59:73–100. doi: 10.2307/1166139
108. Greenberg L, Safran J. Emotion in psychotherapy. Am Psychol. (1989) 44:19–29. doi: 10.1037/0003-066X.44.1.19
109. Kashdan TB, Disabato DJ, Goodman FR, Doorley JD, McKnight PE. Understanding psychological flexibility: a multimethod exploration of pursuing valued goals despite the presence of distress. Psychol Assess. (2020) 32:829–50. doi: 10.1037/pas0000834
110. Watts R, Luoma JB. The use of the psychological flexibility model to support psychedelic assisted therapy. J Context Behav Sci. (2020) 15:92–102. doi: 10.1016/j.jcbs.2019.12.004
111. Hofmann SG, Hayes SC. The future of intervention science: process-based therapy. Clin Psychol Sci. (2019) 7:37–50. doi: 10.1177/2167702618772296
112. Fang S, Huang M. Reliability and validity of the chinese version of multidimensional psychological inflexibility scale in college students. Chin J Clin Psychol. (2022) 30:1367–70. doi: 10.16128/j.cnki.1005-3611.2022.06.021
Keywords: acceptance and commitment therapy, rational emotive behavior therapy, hoarding, psychological flexibility, mediation
Citation: Fang S, Ding D, Zhang R and Huang M (2023) Psychological mechanism of acceptance and commitment therapy and rational emotive behavior therapy for treating hoarding: Evidence from randomized controlled trials. Front. Public Health 11:1084467. doi: 10.3389/fpubh.2023.1084467
Received: 30 October 2022; Accepted: 16 January 2023;
Published: 10 February 2023.
Edited by:
Keong Yap, Australian Catholic University, AustraliaReviewed by:
Junhui Wu, Institute of Psychology (CAS), ChinaHui Zhang, Nanjing Normal University, China
Copyright © 2023 Fang, Ding, Zhang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuanghu Fang,  ZnNoOTA3NUAxNjMuY29t
ZnNoOTA3NUAxNjMuY29t