 Chiara Lorini1,2
Chiara Lorini1,2 Giuseppe Cavallo1,2*
Giuseppe Cavallo1,2* Virginia Vettori1,2Primo Buscemi3Giulia Ciardi3
Virginia Vettori1,2Primo Buscemi3Giulia Ciardi3 Patrizio Zanobini1,2
Patrizio Zanobini1,2 Orkan Okan4
Orkan Okan4 Kevin Dadaczynski5,6
Kevin Dadaczynski5,6 Vieri Lastrucci1,7
Vieri Lastrucci1,7 Guglielmo Bonaccorsi1,2
Guglielmo Bonaccorsi1,2- 1Department of Health Science, University of Florence, Florence, Italy
- 2Health Literacy Laboratory, Department of Health Science, University of Florence, Florence, Italy
- 3School of Specialization in Public Health, University of Florence, Florence, Italy
- 4Department of Sport and Health Sciences, Technical University Munich, Uptown München-Campus D, Munich, Germany
- 5Department of Health Science, Fulda University of Applied Sciences, Fulda, Germany
- 6Center for Applied Health Sciences, Leuphana Universitat Lüneburg, Lüneburg, Germany
- 7Epidemiology Unit, Meyer Children’s University Hospital, Florence, Italy
The pandemic deeply changed young adults’ life. Lockdown period and the social restrictions dramatically affected university students’ mental health. The aim of our cross-sectional study was to describe psychological well-being, future anxiety (FA), and health complaints (HCs) in a sample of 3,001 students of the University of Florence in the middle of the first two pandemic waves. We assessed the role of subjective social status, chronic diseases, sense of coherence (SoC), and digital health literacy (DHL) as predictors of psychological well-being, FA, and HCs. Students expressed high levels of FA and reported being disturbed by not being able to achieve their desired future goals. About 40% reported a low or a very low well-being and 19.1% experienced two or more subjective health complaints more than once a week. The likelihood of having a better mental health status significantly increased with increasing SoC and among males. Subjective Social Status proved to be a predictor for FA. Enhancing SoC could improve the health status of the university students during the pandemic and beyond.
Introduction
Italy was the first European country to be severely affected by a high incidence of COVID-19 cases (1, 2). During the first wave, from 1st March to 31 May 2020, Italy registered 227,972 cases and 34,079 deaths (3). All non-essential services and activities (including schools and universities) were suspended, and a “stay-at-home” order was imposed. The pandemic has profoundly changed everyone’s lives and young adults in particularly have suffered severe consequences because they have been unable to maintain social contacts and activities during the crucial phase of their lives. In this context, people with chronic diseases or physical impairments could have been more affected, due to their more vulnerability.
Like many other Universities worldwide, the University of Florence – the setting of the present study - rapidly adapted its organizational processes by adopting distance learning, library closures, virtual dissertation, and a strict application of anti-contagion measures. Recent literature shows that the lockdown period and the other social restrictions dramatically affected university students’ mental health (4). Many studies conducted worldwide presented consistent results showing increasing prevalence of suicidal thoughts, severe distress, perceived stress, depressive symptoms, anxiety, concentration disorders, and psycho-somatization (5–11).
This could be considered because of the syndemic – that is the biological and social interactions between conditions and states, interactions that increase a person’s susceptibility to harm or worsen their health outcomes. In fact, a combined effect of the pandemic and the infodemic has been observed, where the damages caused by SARS-CoV-2 are to be attributed not only to the direct effects on health, but also to the plethora of information produced, part of which unintentionally – misinformation - or deliberately - disinformation – false. In addition to the impact on mental health, Savage et al. (4) observed an increase in sedentary behavior and, in line with another research (12), a reduction in time spent with and level of energy expenditure due to physical activity, especially in males. In summary, although the pandemic was handled differently around the world and the epidemic situation differed across countries, some common patterns in the way the pandemic has impacted health outcomes and behaviors in university students have emerged in the literature.
Nonetheless, to the best of our knowledge, to date just a few studies have investigated the predictors of well-being, anxiety and health complains among university students during the COVID-19 pandemic, although such information would be useful to manage similar situations that may arise again in the future. Since the infodemic increased the state of uncertainty and fear (13) and negatively affected the strategies adopted to contain the contagion, the role of health literacy (HL), particularly of digital health literacy (DHL), has become crucial. DHL has been defined as a set of skills needed by the individuals to search health information on the Internet, and to understand and apply them to increase awareness and responsibility for one’s own health (14). The Internet and the social networks are often used by university students as a primary source of health information (15, 16). However, they frequently have problems in finding the appropriate information on a particular health-related topic and difficulties in assessing the quality and reliability of the information found (17, 18). Moreover, people with chronic diseases seem to be less satisfied with information during the infodemic than those without such health problems, and they pay much more attention to information about COVID-19 because of their higher risks (18).
Another factor that supports individuals in coping with difficulties while maintaining a good physical and mental quality of life is the sense of coherence (SoC). SoC is an important concept of the Salutogenesis theory and according to Antonovsk (19), SoC reflects a persons’ ability and coping capability to respond to stressful situations (20). In this sense, it is a global orientation to see life as structured, manageable, and meaningful (20). On this topic, Leung et al. (21) conducted a study with older adults during the COVID-19 pandemic that showed how SoC directly affected anxiety. Moreover, in this cross-sectional study, the level of DHL was closely related to that of SoC, suggesting that promoting HL, especially its digital component, may be key to improving SoC. Regarding university students, Chu et al. (22) examined the level of SoC and found a positive association with health awareness. and negative links with higher levels of stress and poor financial status (22).
The aim of our study is to describe psychological well-being, future anxiety, and health complaints (HCs) in a sample of students enrolled at the University of Florence, between the first and the second pandemic wave of COVID-19, and to assess the role of subjective social status, chronic diseases, SoC and DHL as their predictors.
Materials and methods
Study participation was voluntary. Data was collected using an online questionnaire developed by Dadaczynski et al. (17). The Italian version of the questionnaire was developed using a standard procedure of translation and back-translation (23) and includes scales or parts of scales already validated at the national or international level to collect data regarding sociodemographic condition, life situation, future anxiety, DHL and information seeking behaviors, personal health situation (17). The materials and methods are reported in Table 1.
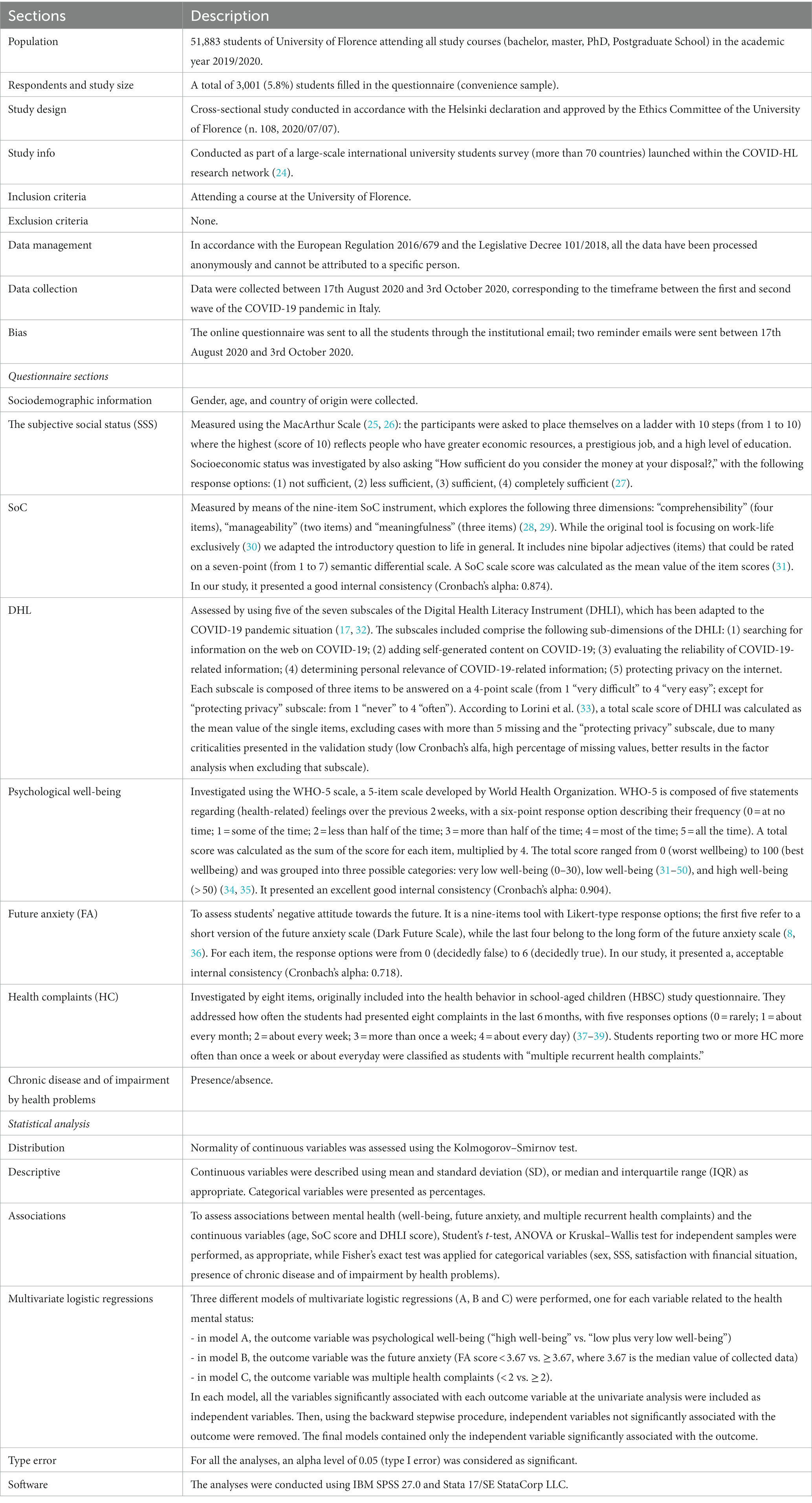
Table 1. Materials and methods used for this study.
Results
Description of the sample
A total of N = 3,001 undergraduate students participated in the study. The majority was pursuing a bachelor’s degree (62%), while 37% were in a master’s degree programe and a small percentage (1%) were in other courses (PhD, Post-graduate School). Twenty-three percent were enrolled in Humanities and Education degree, 15% in Human Health Sciences, 13% in Engineering, 11% in Mathematical, Physical and Natural Sciences, 10% in Architecture, and another 10% in Economics. The remaining 18% were enrolled in Political Science, Law, Agriculture, and Psychology. About 68% (67.9%) were female and 92.5% were born in Italy. The median age was 22 (IQR: 20–24, range: 18–70 years). About 14% of the subjects (N = 408; 13.6%) reported a low SSS, 69% (N = 2,072) a medium SSS, and 17.4% (N = 521) a high SSS. Moreover, 18.9% were completely sufficient with the money at their disposal, 50.8% sufficient, 24.3% less than sufficient, and 6% not sufficient. The median SoC score was 3.67 (IQR: 2.89–4.44). The median of the total DHLI score was 2.83 (IQR: 2.58–3.17). At least one chronic disease affected 14.7% (N = 440) of the respondents and 8.7% (N = 262) had functional limitations in daily activities.
Well-being, future anxiety, and health complaints: general findings
Concerning the results derived from the WHO-5 scale, 60.8% of the respondents had a high well-being, while 24.5% showed a low well-being and 14.7% a very low well-being. In particular, the highest criticality was observed for the item 4 (“I woke up feeling fresh and rested”), with 10.8% responding with “at no time” and 15.2% with “some of the time” (Figure 1A). The median score at the WHO-5 scale was 56 (IQR: 40–72), with a mean of 55.23 ± 21.9. Future anxiety were mainly related to the possibility that changes in the economic and political situation would threaten students’ future (50.9% of “decidedly true” response) and by the thought that in the future they would not be able to realize their goals (54.4% of “decidedly true” response; Figure 1B). The median score at the FA scale was 3.67 (IQR: 2.67–4.33), while the mean 3.53 ± 1.24. Concerning health complaints, 19.9% reported headache about every day or more than once a week, 12.5% feeling low about every day, and 15% difficulties in getting sleep about every day (Figure 1C). Considering multiple recurrent health complaints, 19.1% experienced two or more subjective health complaints more than once a week or more often.
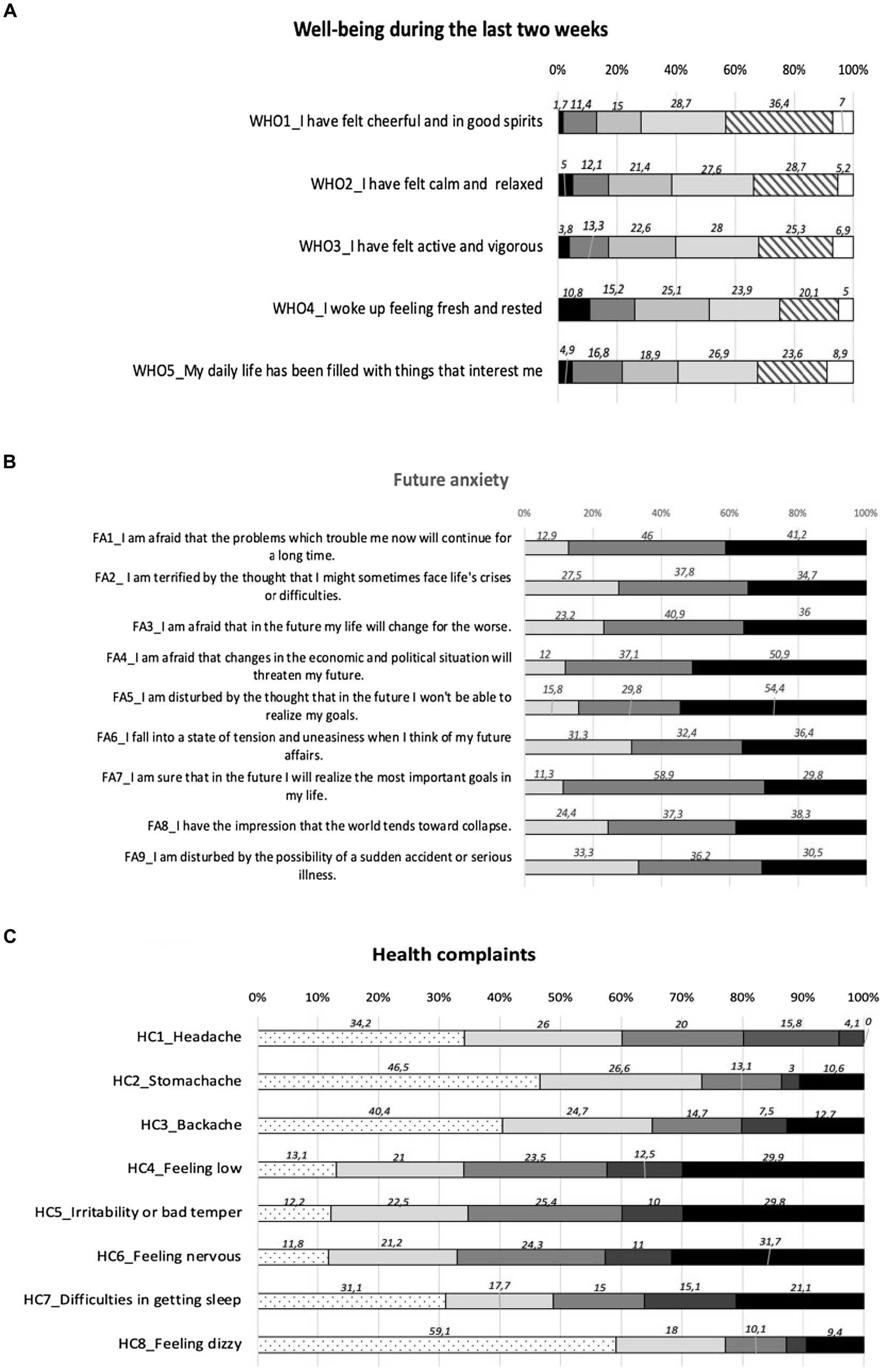
Figure 1. (A) Well-being: items responses.  At no time;
At no time;  some of the time;
some of the time;  less than half of the time;
less than half of the time;  more than half of the time;
more than half of the time;  most of the time;
most of the time;  all of the time. (B) Future anxiety: items responses.
all of the time. (B) Future anxiety: items responses.  Decidedly false;
Decidedly false;  hard of say;
hard of say;  decidedly true. (C) Health complaints: items responses.
decidedly true. (C) Health complaints: items responses.  Rarely or never;
Rarely or never;  about every month;
about every month;  about every week;
about every week;  more than once a week;
more than once a week;  about every day;
about every day;  missing.
missing.
Well-being, future anxiety, and multiple recurrent health complaints: predictors
Table 2 reports the descriptive analysis of sex, age, SoC, SSS, DHL, satisfaction of the financial situation, presence of chronic diseases, and impairment by health problems, well-being, future anxiety, and multiple health complaints. Age distribution was not significantly associated with any health outcomes. SoC score was significantly higher with increasing well-being (median values: from 2.67 for “very low well- being” to 4.11 for “high well-being”), decreasing future anxiety (median values: from 4.22 for FA scores lower than 3.67 to 3.22 for FA scores higher than 3.67), and for students with less than two recurrent health complaints (median values: from 3.89 for those reported less than two recurrent health complaints to 2.89 for those with two or more recurrent health complaints). The distribution of DHLI score showed similar results: significantly higher scores could be found with increasing well-being (median values: from 2.83 for “very low well- being” to 2.92 for “high well-being”), decreasing future anxiety (median values: from 2.92 for FA scores lower than 3.67 to 2.83 for FA scores higher than 3.67), and for students with less than two recurrent health complaints (median values: from 2.92 for those reported less than two recurrent health complaints to 2.78 for those with two or more recurrent health complaints). Considering the categorical variables (Table 2), females were identified to have a lower mental health (lower well-being, higher FA, more frequently multiple recurrent health complaints) compared with male respondents. The same could be found for those with lower socioeconomic condition (all indicators), and for those reporting a chronic disease and accompanied impairments.
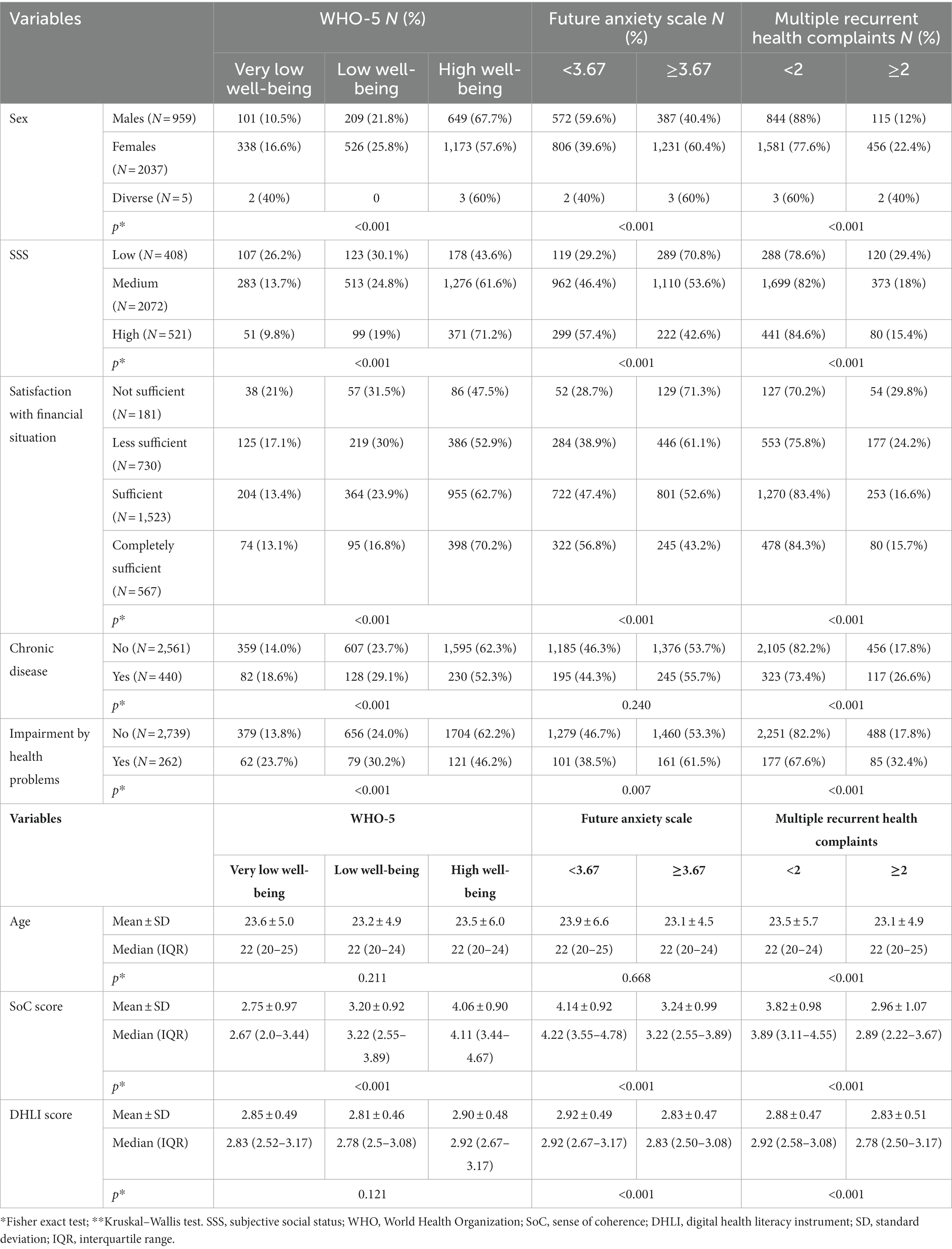
Table 2. Descriptive analysis of sex, SSS, satisfaction with current financial situation, presence of chronic diseases and impairment by health problems, by well-being, future anxiety, and multiple recurrent health complaints, and descriptive analysis of age, SoC and DHLI scores by well-being, future anxiety, and health complaints.
Finally, Table 3 reports the results of multivariate logistic analyses (models A, B, and C, one for each outcome variable). Sex was a significant predictor of all the outcome variables: female students indicated a higher likelihood of poorer mental health. On the other hand, for all the outcome variables, the likelihood of reporting a better mental health status significantly increased with increasing SoC score. Conversely, socioeconomic status, either measured using SSS or satisfaction with financial situation, was excluded from the final models for well-being and multiple health complaints as not significant associations could be found. Only high SSS maintained a significant predictor for FA (OR: 1.39 of FA score lower than 3.67 with respect to equal or higher than 3.67). Moreover, the presence of an impairment by health problems emerged as another significant predictor of low or very low well-being and for two or more recurrent health complaints at least once a week.
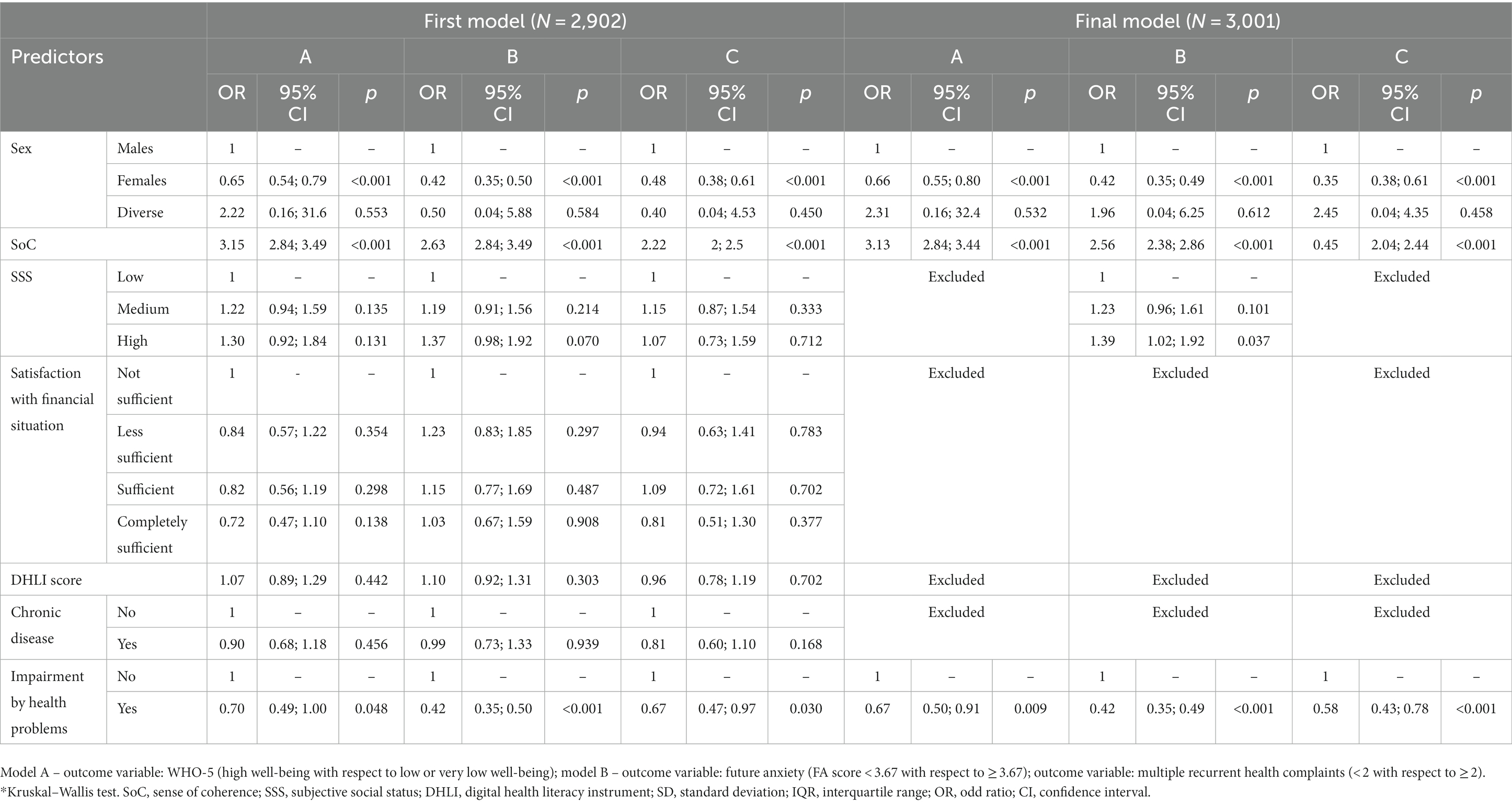
Table 3. Multivariate logistic regression analysis – first and final models.
Discussion
Main finding of this study
The COVID-19 pandemic has strongly affected – and is still affecting – people’s life. University students have been overwhelmed by both the effects of social restriction and lockdowns, as well as by the uncertainty related to the socio-economic consequences of the pandemic on the medium and long-term. In this context, our study aims at describing psychological well-being, future anxiety, and health complaints in a sample of students attending the University of Florence, between the first and the second pandemic wave of COVID-19, and to assess the role of socioeconomic condition, chronic diseases, SoC and DHL as their predictors. Considering the results, it emerged that students feel threatened by economic and political situations and disturbed by not being able to achieve their goals in their future. About 40% of the students reported a low or very low well-being, and 19.1% experienced two or more subjective health complaints more than once a week or about every day. Some variables emerged as predictors of the outcome variables: sex (females presented worse condition), SoC (the higher the SoC, the better the health condition), subjective social status (the higher the SoC, the lower the anxiety for the future), chronic diseases (better condition are reported among students who did not suffer from chronic diseases). On the contrary, DHL did not predict the outcome variables.
What is already known on this topic
Studies conducted on previous pandemics occurred over the last 60 years - the Asian flu (1956–1957), SARS (2002–2003), H1N1 flu (2009–2010), Ebola (2013–2014) - gave useful elements to evaluate the psychological reactions resulting from these public health emergencies (40). Such reactions include maladaptive behaviors, emotional distress, and defensive responses. In fact, both during and after the pandemic period, individuals had an increased likelihood of mental health problems including insomnia, anger, fear of illness, increased health risk behaviors, such as psychotropic substance use and social isolation, onset of mental disorders, such as anxiety, depression, somatization and decreased perceived health (41). Differently from the previous ones, the COVID-19 pandemic is occurring in the digital and social media era, resulting in enormous mediatic visibility and in generating an infodemic, and this could further lead to uncertainties, distress, and difficulties in making appropriate health decisions. In this perspective, DHL is a fundamental skill during the COVID-19 pandemic, that could influence mental well-being. For these reasons, our study, as part of an international project, investigated DHL, future life perspectives, health-related outcomes in a sample of university students (42). Surprisingly, in our sample, DHL does not affect well-being, FA and HCs.
Our findings in several aspects – such as in terms of demographics, SoC and DHLI scores - are comparable to the many studies published from COVID-HL network (8, 13, 17, 18, 31, 43–48). Also considering the health-related outcomes, Florentine university students presented conditions in line with the other studies. Regarding health complaints, more than half of our students suffered from an HC at least once a week in the last 6 months, in line with Dadaczynski et al. (31). On the other hand, the reported level of well-being varies, probably due to the different waves of the pandemic during which the surveys were conducted, as well as due to the different restriction measures adopted at the national or local levels and to the to the cultural differences of each country (8, 46, 48). As far as FA score is concerned, our findings are similar to what emerged from the Australian study by Dodd et al. (8), and higher than that measured in the German sample by Dadaczynski et al. (31).
According to our results, sex and SoC emerged as consistent predictors of all the investigated outcomes, also in the multivariate analysis: while females presented worse health status, the higher the SoC, the better the health condition. SoC is a resource to cope with physical isolation and social distancing and can help students to avoid or contain healthcare problems, particularly in the mental dimension. In fact, as evidenced by some studies (49–52), subjects with high SoC experience symptoms of stress less frequently and cope with stressful situations more efficiently. The potential of SoC to promote mental health during stressful situations is supported by previous studies across different populations: university students (22), adolescents (53) disadvantaged women (54), caregivers of older adults and hospital patients (55), and older adults (21). In fact, higher SOC could enable persons to perceive stressful situation, like the first phases of the pandemic, as not too bad and manageable by utilizing available resources, thereby reducing the fear of the unknown.
The role of female sex as risk condition for depression, anxiety, and stress is consistent with the studies conducted by Dodd (8), Dadaczynski et al. (31), Debowska et al. (56), and Hou et al. (57). In particular, in the face of a greater comprehensibility shown by males about the epidemic, there is a greater FA by females (31). Moreover, males tend to have higher SoC and well-being than females (58).
As for DHL and satisfaction of current economic situation, although at the bivariate analysis significant associations were found with all the health-related outcomes, their role as predictors were lost at the multivariate analysis. Also, for chronic conditions, significant associations were not confirmed at the multivariate analysis. These results seem different with respect to those reported by other Authors. In particular, some studies have described that having sufficient financial resources could also play a role in addressing people’s anxiety during the COVID-19 pandemic (59, 60). Moreover, some studies have reported that students with high levels of DHL were those who reported low levels of anxiety about the future and less somatization symptoms (8, 19, 31, 54, 55). Considering the predictors of SoC described in other studies (8, 61) as well as the parallelism between competences, skills and abilities of health literacy with respect to the three dimensions of SoC (62) we can suppose that DHL and socioeconomic condition have to be considered mostly as predictors of SoC, instead of strong and direct predictors of students’ health. This aspect emerged also by a mediation analysis performed in a sample of older people during the current pandemic, in which SoC had a direct, negative effect on anxiety and mediated the relationships between anxiety and DHL/financial satisfaction (21). A similar connection can also be supposed for chronic conditions: for people with these characteristics, the relationships between anxiety, well-being, health complaints, SoC, DHL and economic status could be complex, multiple, and non-linear. Future studies will be useful to deepen – and eventually confirm - these relationships also among university students.
What this study adds
This study adds new elements regarding the predictors of well-being, FA and HCs of university students during the COVID-19 pandemic. In particular, to the best of our knowledge, this is the first study conducted in Italy investigating a wide range of health-related outcomes and potential predictors, by using validated scales. Because this study was conducted within an international network, our results contribute to investigate country-specific characteristics related to the impact of the COVID-19 pandemic on university students.
Limitation of this study
This study presents some limitations. First, the participation was voluntary, and only about 6% of the students joined it. Moreover, all the information was self-reported, so underestimation or overestimation of health conditions or health-related outcomes were possible. Finally, the cross-sectional design does not allow to assess causal relationship between potential predictors and health-related outcomes.
Generalizability
Participation was voluntary, so the study was conducted using a convenience sample, in so limiting the generalizability of the results to the entire population of students at the University of Florence.
Conclusion
SoC and sex resulted strong predictors of well-being, multiple recurrent health complaints and future anxiety. In this perspective, health promoting interventions devoted to enhancing SoC should be conducted, in order to improve the health status of the university students, particularly in mitigating the negative consequences on mental health caused by the many stressful factors produced by the pandemic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by the Ethics Committee of the University of Florence (n. 108, 2020/07/07). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. All patients provided their written informed consent to participate in this study.
Author contributions
OO and KD: conceptualization. OO, KD, CL, and GB: methodology. CL, GB, PB, GCa, and VV: formal analysis and investigation. CL, GCa, VV, PB, and GCi: writing – original draft preparation. CL, GCa, VL, and GB: writing – review and editing. GB: resources. GB, CL, GCa, VL, and PZ: supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cerqua, A, and Di Stefano, R. When did coronavirus arrive in Europe? Stat Methods Appt. (2022) 31:181–95. doi: 10.1007/s10260-021-00568-4
2. Baccini, M, Cereda, G, and Viscardi, C. The first wave of the SARS-CoV-2 epidemic in Tuscany (Italy): a SI2R2D compartmental model with uncertainty evaluation. PLoS One. (2021) 16:e0250029. doi: 10.1371/journal.pone.0250029
3. ISTAT. (2021). Available at: https://www.istat.it/it/files//2021/03/Report_ISS_Istat_2020_5_marzo.pdf (Accessed July 04, 2022).
4. Savage, MJ, Hennis, PJ, Magistro, D, Donaldson, J, Healy, LC, and James, RM. Nine months into the COVID-19 pandemic: a longitudinal study showing mental health and movement behaviours are impaired in UK students. Int J Environ Res Public Health. (2021) 18:2930. doi: 10.3390/ijerph18062930
5. Wathelet, M, Duhem, S, Vaiva, G, Baubet, T, Habran, E, Veerapa, E, et al. Factors associated with mental health disorders among university students in France confined during the COVID-19 pandemic. JAMA Netw Open. (2020) 3:e2025591. doi: 10.1001/jamanetworkopen.2020.25591
6. Ma, Z, Zhao, J, Li, Y, Chen, D, Wang, T, Zhang, Z, et al. Mental health problems and correlates among 746 217 college students during the coronavirus disease 2019 outbreak in China. Epidemiol Psychiatr Sci. (2020) 29:e181. doi: 10.1017/S2045796020000931
7. Wang, X, Hegde, S, Son, C, Keller, B, Smith, A, and Sasangohar, F. Investigating mental health of US College students during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. (2020) 22:e22817. doi: 10.2196/22817
8. Dodd, RH, Dadaczynski, K, Okan, O, McCaffery, KJ, and Pickles, K. Psychological wellbeing and academic experience of university students in Australia during COVID-19. Int J Environ Res Public Health. (2021) 18:866. doi: 10.3390/ijerph18030866
9. Villani, L, Pastorino, R, Molinari, E, Anelli, F, Ricciardi, W, Graffigna, G, et al. Impact of the COVID-19 pandemic on psychological well-being of students in an Italian university: a web-based cross-sectional survey. Glob Health. (2021) 17:39. doi: 10.1186/s12992-021-00680-w
10. Romeo, A, Benfante, A, Castelli, L, and Di Tella, M. Psychological distress among Italian university students compared to general workers during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:2503. doi: 10.3390/ijerph18052503
11. Savarese, G, Curcio, L, D'Elia, D, Fasano, O, and Pecoraro, N. Online university counselling services and psychological problems among Italian students in lockdown due to Covid-19. Healthcare (Basel). (2020) 8:440. doi: 10.3390/healthcare8040440
12. Giustino, V, Parroco, AM, Gennaro, A, Musumeci, G, Palma, A, and Battaglia, G. Physical activity levels and related energy expenditure during COVID-19 quarantine among the Sicilian active population: a cross-sectional online survey study. Sustainability. (2020) 12:4356. doi: 10.3390/su12114356
13. Patil, U, Kostareva, U, Hadley, M, Manganello, JA, Okan, O, Dadaczynski, K, et al. Health literacy, digital health literacy, and COVID-19 pandemic attitudes and behaviors in U.S. college students: implications for interventions. Int J Environ Res Public Health. (2021) 18:3301. doi: 10.3390/ijerph18063301
14. Broucke, SVD, Levin-Zamir, D, Schaeffer, D, Pettersen, K, Guttersrud, O, Finbraten, H, et al. Digital health literacy in general populations – an international comparison. Eur J Pub Health. (2020) 2020:5. doi: 10.1093/eurpub/ckaa165.124
15. Stellefson, M, Hanik, B, Chaney, B, Chaney, D, Tennant, B, and Chavarria, EA. eHealth literacy among college students: a systematic review with implications for eHealth education. J Med Internet Res. (2011) 13:e102. doi: 10.2196/jmir.1703
16. Escoffery, C, Miner, KR, Adame, DD, Butler, S, McCormick, L, and Mendell, E. Internet use for health information among college students. J Am Coll Heal. (2005) 53:183–8. doi: 10.3200/JACH.53.4.183-188
17. Dadaczynski, K, Okan, O, Messer, M, Leung, AYM, Rosário, R, Darlington, E, et al. Digital health literacy and web-based information-seeking behaviors of university students in Germany during the COVID-19 pandemic: cross-sectional survey study. J Med Internet Res. (2021) 23:e24097. doi: 10.2196/24097
18. Zakar, R, Iqbal, S, Zakar, MZ, and Fischer, F. COVID-19 and health information seeking behavior: digital health literacy survey amongst university students in Pakistan. Int J Environ Res Public Health. (2021) 18:4009. doi: 10.3390/ijerph18084009
19. Eriksson, M, and Lindström, B. Antonovsky's sense of coherence scale and the relation with health: a systematic review. J Epidemiol Community Health. (2006) 60:376–81. doi: 10.1136/jech.2005.041616
20. Mittelmark, MB, Bauer, GF, Vaandrager, L, Pelikan, JM, Sagy, S, Eriksson, M, et al. eds. The Handbook of Salutogenesis. 2nd ed. Cham (CH): Springer (2022).
21. Leung, AYM, Parial, LL, Tolabing, MC, Sim, T, Mo, P, Okan, O, et al. Sense of coherence mediates the relationship between digital health literacy and anxiety about the future in aging population during the COVID-19 pandemic: a path analysis. Aging Ment Health. (2022) 26:544–53. doi: 10.1080/13607863.2020.1870206
22. Chu, JJ, Khan, MH, Jahn, HJ, and Kraemer, A. Sense of coherence and associated factors among university students in China: cross-sectional evidence. BMC Public Health. (2016) 16:336. doi: 10.1186/s12889-016-3003-3
23. Streiner, D, Norman, G, and Cairney, J. Health measurement scales: a practical guide to their development and use (5th edition). Aust N Z J Public Health. (2016) 40:294–5. doi: 10.1111/1753-6405.12484
24. COVID-HL. (2021). Available at: https://covid-hl.eu (Accessed March 13, 2022).
25. Adler, NE, Epel, ES, Castellazzo, G, and Ickovics, JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol. (2000) 19:586–92. doi: 10.1037//0278-6133.19.6.586
26. Hoebel, J, Müters, S, Kuntz, B, Lange, C, and Lampert, T. Messung des subjektiven sozialen status in der Gesundheitsforschung mit einer deutschen version der MacArthur scale [measuring subjective social status in health research with a German version of the MacArthur scale]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2015) 58:749–57. doi: 10.1007/s00103-015-2166-x
27. Health Survey among University Students in North Rhine-Westphalia/Germany: Questionnaire. (2019) Available at: https://tinyurl.com/qkxxwuz
28. Bauer, GF, Vogt, K, Inauen, A, and Jenny, GJ. Work-SoC– entwicklung und validierung einer skala zur erfassung des arbeitsbezogenen kohärenzgefühls [Work-SoC—Development and validation of a scale measuring work-related sense of coherence]. Zeitschrift für Gesundheitspsychologie. (2015) 23:20–30. doi: 10.1026/0943-8149/a000132
29. Vogt, K, Jenny, GJ, Füllemann, D, Inauen, A, and Bauer, GF, Work-Related Sense of Coherence as a Higher-Order Indicator of Salutogenic Working Conditions. (2012). Paper Presented at Health Promotion Research - An International Forum, Trondheim, Norway.
30. Vogt, K, Jenny, GJ, and Bauer, GF. Comprehensibility, manageability and meaningfulness at work: constructvalidity of a scale measuring work-related sense of coherence. SA J Ind Psychol. (2013) 39:1–8. doi: 10.4102/sajip.v39i1.1111
31. Dadaczynski, K, Okan, O, Messer, M, and Rathmann, K. University students' sense of coherence, future worries and mental health: findings from the German COVID-HL-survey. Health Promot Int. (2022) 37:daab070. doi: 10.1093/heapro/daab070
32. van der Vaart, R, and Drossaert, C. Development of the digital health literacy instrument: measuring a broad Spectrum of health 1.0 and health 2.0 skills. J Med Internet Res. (2017) 19:e27. doi: 10.2196/jmir.6709
33. Lorini, C, Velasco, V, Bonaccorsi, G, Dadaczynski, K, Okan, O, Zanobini, P, et al. Validation of the COVID-19 digital health literacy instrument in the Italian language: a cross-sectional study of Italian university students. Int J Environ Res Public Health. (2022) 19:6247. doi: 10.3390/ijerph19106247
34. Topp, CW, Østergaard, SD, Søndergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
35. Bech, P. Measuring the dimension of psychological general well-being by the WHO-5 119. Qual. Life Newsl. (2004) 32:15–6.
36. Zaleski, Z, Sobol-Kwapinska, M, Przepiorka, A, and Meisner, M. Development and validation of the dark future scale. Time Soc. (2019) 28:107–23. doi: 10.1177/0961463X16678257
37. Haugland, S, and Wold, B. Subjective health complaints in adolescence--reliability and validity of survey methods. J Adolesc. (2001) 24:611–24. doi: 10.1006/jado.2000.0393
38. Haugland, S, Wold, B, Stevenson, J, Aaroe, LE, and Woynarowska, B. Subjective health complaints in adolescence. A cross-national comparison of prevalence and dimensionality. Eur J Pub Health. (2001) 11:4–10. doi: 10.1093/eurpub/11.1.4
39. Hetland, J, Torsheim, T, and Aarø, LE. Subjective health complaints in adolescence: dimensional structure and variation across gender and age. Scand J Public Health. (2002) 30:223–30. doi: 10.1080/140349402320290953
40. Wang, Z, and Wang, D. The influence and enlightenment of five public health emergencies on public psychology since new century: a systematic review. Int J Soc Psychiatry. (2021) 67:878–91. doi: 10.1177/00207640211002222
41. Shigemura, J, Ursano, RJ, Morganstein, JC, Kurosawa, M, and Benedek, DM. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry Clin Neurosci. (2020) 74:281–2. doi: 10.1111/pcn.12988
42. Dadaczynski, K, Okan, O, and Rathmann, K. COVID-19 Health Literacy Survey: University Students (COVID-HL-Survey). Questionnaire and Scale Documentation Version 1. Bielefeld/Fulda: Bielefeld University, Interdisciplinary Centre for Health Literacy Research and Fulda University of Applied Sciences, Public Health Centre (2020).
43. Silva, AND, Guedes, CR, Santos-Pinto, CDB, Miranda, ES, Ferreira, LM, and Vettore, MV. Demographics, socioeconomic status, social distancing, psychosocial factors and psychological well-being among undergraduate students during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:7215. doi: 10.3390/ijerph18147215
44. Rosário, R, Martins, MRO, Augusto, C, Silva, MJ, Martins, S, Duarte, A, et al. Associations between COVID-19-related digital health literacy and online information-seeking behavior among Portuguese university students. Int J Environ Res Public Health. (2020) 17:8987. doi: 10.3390/ijerph17238987
45. Li, M, Xu, Z, He, X, Zhang, J, Song, R, Duan, W, et al. Sense of coherence and mental health in college students after returning to school during COVID-19: the moderating role of media exposure. Front Psychol. (2021) 12:687928. doi: 10.3389/fpsyg.2021.687928
46. Nguyen, LHT, Vo, MTH, Tran, LTM, Dadaczynski, K, Okan, O, Murray, L, et al. Digital health literacy about COVID-19 as a factor mediating the association between the importance of online information search and subjective well-being among university students in Vietnam. Front Digit Health. (2021) 3:739476. doi: 10.3389/fdgth.2021.739476
47. Vrdelja, M, Vrbovšek, S, Klopčič, V, Dadaczynski, K, and Okan, O. Facing the growing COVID-19 Infodemic: digital health literacy and information-seeking behaviour of university students in Slovenia. Int J Environ Res Public Health. (2021) 18:8507. doi: 10.3390/ijerph18168507
48. Amoah, PA, Leung, AYM, Parial, LL, Poon, ACY, Tong, HH, Ng, WI, et al. Digital health literacy and health-related well-being amid the COVID-19 pandemic: the role of socioeconomic status among university students in Hong Kong and Macao. Asia Pac J Public Health. (2021) 33:613–6. doi: 10.1177/10105395211012230
49. Rossi, R, Socci, V, Talevi, D, Mensi, S, Niolu, C, Pacitti, F, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Psych. (2020) 11:790. doi: 10.3389/fpsyt.2020.00790
50. Wang, C, Pan, R, Wan, X, Tan, Y, Xu, L, Ho, CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
51. Hochwälder, J, and Saied, V. The relation between sense of coherence and daily hassles among university students. Health Psychol Behav Med. (2018) 6:329–39. doi: 10.1080/21642850.2018.1538802
52. Albertsen, K, Nielsen, ML, and Borg, V. The Danish psychosocial work environment and symptoms of stress: the main, mediating and moderating role of sense of coherence. Work Stress. (2001) 15:241–53. doi: 10.1080/02678370110066562
53. Moksnes, UK, and Espnes, GA. Sense of coherence in association with stress experience and health in adolescents. Int J Environ Res Public Health. (2020) 17:3003. doi: 10.3390/ijerph17093003
54. Remes, O, Wainwright, N, Surtees, P, Lafortune, L, Khaw, KT, and Brayne, C. A strong sense of coherence associated with reduced risk of anxiety disorder among women in disadvantaged circumstances: British population study. BMJ Open. (2018) 8:e018501. doi: 10.1136/bmjopen-2017-018501
55. Li, W, Leonhart, R, Schaefert, R, Zhao, X, Zhang, L, Wei, J, et al. Sense of coherence contributes to physical and mental health in general hospital patients in China. Psychol Health Med. (2015) 20:614–22. doi: 10.1080/13548506.2014.952644
56. Debowska, A, Horeczy, B, Boduszek, D, and Dolinski, D. A repeated cross-sectional survey assessing university students' stress, depression, anxiety, and suicidality in the early stages of the COVID-19 pandemic in Poland. Psychol Med. (2020) 52:3744–7. doi: 10.1017/S003329172000392X
57. Hou, F, Bi, F, Jiao, R, Luo, D, and Song, K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China:a cross-sectional study. BMC Public Health. (2020) 20:1648. doi: 10.1186/s12889-020-09738-7
58. Nilsson, KW, Leppert, J, Simonsson, B, and Starrin, B. Sense of coherence and psychological well-being: improvement with age. J Epidemiol Community Health. (2010) 64:347–52. doi: 10.1136/jech.2008.081174
59. Bareket-Bojmel, L, Shahar, G, and Margalit, M. COVID-19-related economic anxiety is as high as health anxiety: findings from the USA, the UK, and Israel. Int J Cogn Ther. (2021) 14:566–74. doi: 10.1007/s41811-020-00078-3
60. Agberotimi, SF, Akinsola, OS, Oguntayo, R, and Olaseni, AO. Interactions between socioeconomic status and mental health outcomes in the Nigerian context amid COVID-19 pandemic: a comparative study. Front Psychol. (2020) 11:559819. doi: 10.3389/fpsyg.2020.559819
61. Togari, T, Inoue, Y, Oshima, G, Abe, S, Hosokawa, R, and Takaku, Y. Socioeconomic status and the sense of coherence among Japanese people living with HIV. Int J Environ Res Public Health. (2022) 19:7673.
Keywords: psychological determinants, well-being, socioeconomic determinants, university students, SOC, cross-sectional study
Citation: Lorini C, Cavallo G, Vettori V, Buscemi P, Ciardi G, Zanobini P, Okan O, Dadaczynski K, Lastrucci V and Bonaccorsi G (2023) Predictors of well-being, future anxiety, and multiple recurrent health complaints among university students during the COVID-19 pandemic: the role of socioeconomic determinants, sense of coherence, and digital health literacy. An Italian cross-sectional study. Front. Public Health. 11:1210327. doi: 10.3389/fpubh.2023.1210327
Edited by:
Ashwani Kumar Mishra, All India Institute of Medical Sciences, IndiaReviewed by:
Assis Kamu, Universiti Malaysia Sabah, MalaysiaSergio López García, Pontifical University of Salamanca, Spain
Copyright © 2023 Lorini, Cavallo, Vettori, Buscemi, Ciardi, Zanobini, Okan, Dadaczynski, Lastrucci and Bonaccorsi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giuseppe Cavallo, Z2l1c2VwcGUuY2F2YWxsb0B1bmlmaS5pdA==