 Lemessa Debel1*
Lemessa Debel1* Jemal Ayalew2
Jemal Ayalew2 Saro Abdella1
Saro Abdella1 Jaleta Bulti1Birra Bejiga1
Jaleta Bulti1Birra Bejiga1 Fayiso Bati Wariso1Wudinesh Belete1Abebe Habtesilase1Silesh Lulseged3
Fayiso Bati Wariso1Wudinesh Belete1Abebe Habtesilase1Silesh Lulseged3- 1Ethiopian Public Health Institute, HIV/TB Research Directorate, Addis Ababa, Ethiopia
- 2Department of Statistics, Wollo University, College of Natural Science, Dessie, Ethiopia
- 3Addis Ababa University, Faculty of Medicine, College of Health Sciences, Addis Ababa, Ethiopia
Background: Gender-based violence (GBV) is usually defined as unequal power relations between men and women, which poses a widespread public health problem. The study evaluated the prevalence and factors associated with GBV among female sex workers (FSWs) in Ethiopia.
Method: We used cross-sectional bio-behavioral data collected using respondent-driven sampling (RDS) in 2020 from 16 towns in Ethiopia. Descriptive statistics was analyzed to summarize the study population characteristics and prevalence of GBV, and a multilevel logistic regression model was applied to identify associated factors for GBV. A p-value of ≤0.05 was used as a threshold for statistical significance.
Result: Of 6,085 participants, 28.1% had experienced GBV during the last 12 months, among which 12.7% and 22.3% experienced physical and sexual violence, respectively. FSWs aged 15–24, and 25–34 than those 35 years or more, had a non-paying than paying partners, had 31–60, 61–90, and over 91 than those had less than 30 paying partners, ever had anal sex than those not, condom failure than those not, mobile female sex workers when compared with those not mobile at different town; 3–5 and ≥ 6 years than those less than 3 years stayed in selling sex, street-based, and multiple places selling sex than those used other venues were significantly associated with GBV.
Conclusion: Gender-based violence is a substantial problem among FSWs in Ethiopia, with significant implications for program planning on prevention and response to mitigate the occurrence and impact of GBV among FSWs.
Background
The United Nations defines GBV as any act of violence that results in or is likely to result in physical, sexual, or psychological harm or suffering to women, including threats of such acts, coercion, or arbitrary deprivation of liberty, whether occurring in public or in private life (1). The definition emphasizes that violence is a manifestation of historically unequal power relations between men and women, which have led to the domination over and discrimination against women by men that causes various health problems.
Female sex workers are at heightened risk for GBV (2, 3). Gender-based violence among female sex workers may cause a widespread public health problem including the acquisition of HIV and other sexually transmitted infections (STIs) through unprotected sex and forced sex, physical injury, and psychological trauma. An increasing body of evidence suggests that sexual violence among FSWs may be associated with individual and interpersonal characteristics and a broad range of environmental factors (4–6).
Reports indicate that the prevalence of GBV at the workplace among FSWs varies from 14 to 54% globally (3, 4, 6). Sexual and/or physical GBV was 75% in Latin America and the Caribbean (7), whereas GBV among mobile FSWs in India was 30.5% (8). Physical violence was reported in 65% of some studies (5, 7, 9). A study from South India indicated that the overall GBV among FSWs was 24%, of which 33% and 7% were exposed to physical and sexual violence, respectively (8). In comparison, sexual violence was reported to be 16.9% in Iran (9). Different reports from five Southern African countries show that physical and sexual violence among FSWs in the past 12 months was as high as 70% (10). This figure was 87%, 82%, and 40% in Kenya, Uganda, and Tanzania, respectively (11–13). In Ethiopia, the studies conducted in specific areas indicated that the overall workplace sexual violence was 28%, and the highest prevalence of 75.6% was reported at Mekele town among this population group (14, 15).
Female sex workers use different settings and venues for selling sex where GBV could be committed. The most common settings reported include homes, workplaces such as bars, and on the street (5, 16). The perpetrators of GBV vary by their type of relationship and setting, which was approximately 63.8% with clients in the Caribbean and 18.7% with brothel management in Nigeria (17). The other different factors such as migration to meet new clients (18, 19), stigma, discrimination, or harassment, and changes in work environments increase the exposure of FSWs to GBV (18–21).
Indeed, the majority of these studies identified that individual-level risk factors associated with physical or sexual violence among FSWs were limited to small geographic areas and did not take into account interpersonal and environmental factors beyond individual control that may play significant roles in GBV. Therefore, this study aimed to determine the magnitude of GBV and associated factors related to individual, interpersonal, and environmental factors by considering the cluster effect across towns in Ethiopia.
Materials and methods
A cross-sectional survey using a respondent-driven sampling process was conducted from 2019 to 2020 to identify the prevalence of HIV and other STIs, and GBV among FSWs in 16 cities and towns of Ethiopia. The study population was FSWs who had had sex for money or goods in the capital cities (Addis Ababa, Hawassa, Bahir Dar, Harar, Gambella, and Dire Dawa) of six administrative regions and ten sub-national major towns (Adama, Jimma, Nekemte, and Shashemane; Arba Minch, Dilla, and Mizan; Gondar and Kombolcha; and Logia), which could represent the population groups in Ethiopia.
Sampling procedures
The sample size was determined by a single population proportion formula, assuming a 95% confidence interval, α = 0.05, margin of error (d) = 35%, and proportion (p) = 2% (22), and a design effect of 1.5 with a replacement for non-responders was used. The minimum desired sample size of FSWs in the 6 regional capitals and 10 major towns with a 10% contingency was 6,085 FSWs. This was allocated to the 16 sites proportionate to population size (Table 1).
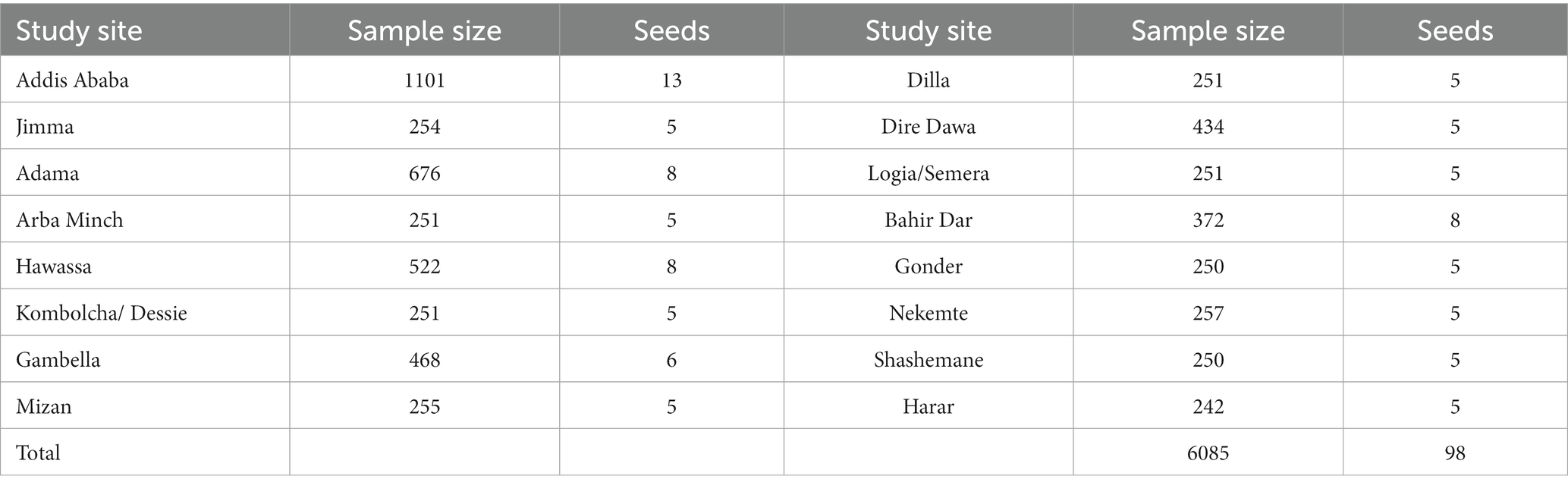
Table 1. Sample sizes and seed distribution by study sites and the National HIV and Other STI Bio-Behavioral Survey, Ethiopia, 2019–2020 (N = 6,085).
The participants were included in the study by respondent-driven sampling (RDS) method. The RDS technique was started by identifying seeds or initial participants. The “seeds” were selected based on the type of sex worker, age category, and geographic location. The number of seeds for each site was determined based on the result of the formative assessment. Accordingly, five seeds for each site that had less than 450 sample sizes, 6–8 seeds for each site that had between 450 and 900 sample sizes, and 12 for 1,250 sample sizes were recruited. Then, FSWs with a known social network were given three coupons so that they could invite their friends or other FSW contacts that were in their network. The coupon was active from the day the coupon was given by the potential recruiter and expired after 2 weeks or when the study was completed. Coupons that were damaged, not readable, photocopied, had no seal/stamp on them, or were not the original ones were declared not valid to avoid desirability bias. Each participant who visited the study site brought the coupon that was identified by number and by who referred them. Based on these criteria, each new participant was given coupons and asked to recruit three additional acquaintances. This process continued until the desired sample size was achieved and the RDS equilibrium was attained. The respondents gave their informed consent to participate in the study. A total of 98 seeds were used for the enrollment of a total of 6,085 FSWs from the 16 study sites, and all 6,085 participated in the study. The majority of the study participants were recruited from seeds that generated two to six waves. A maximum of 16 waves were attained.
Inclusion criteria
Across all 16 study sites, participants were eligible for the study if they were 15 years or older, reported having sex in exchange for money, goods, services, or drugs with more than one client within 12 months before the interviews, and lived or worked in the city/town where the study was conducted.
Definitions of terms
Khat is a shrub (Catha edulis) of the staff-tree family that is cultivated in the Middle East and Africa for its leaves and buds which are the source of a habituating stimulant when chewed or used as a tea (23).
Condom failure is the situation when the condom tears off or partially or completely slips off the penis or is removed from the penis during sexual intercourse (24).
Study variables
The outcome (dependent) variable was GBV experienced by FSWs. The independent variables were individual [(socio-demographic factors: age, educational status, marital status, income, and residence), alcohol consumption, chewing khat, and duration since engagement in sex work], interpersonal with partners (number and type of partner, ever had anal sex, and condom failure), and environmental (change of place in the last 6 months, number of cities FSWs practiced selling sex and practiced venue, FSWs’ mobility, and place of sex work).
Data collection
A standard National HIV and other STIs Bio-Behavioral Survey (NHSBS) questionnaire includes questions on demographic characteristics, history of sexual and other risk behaviors, and GBV (25). A response plan was made to refer FSWs who reported recent GBV victims to the concerned body to get the necessary counseling and support services. The data were collected using the Open Data Kit (ODK) software on a tablet.
Data analysis
The RDS recruitment process (tree of recruitment), evaluation of the RDS assumptions, and generation of weights were all done using R statistical software. The entire dataset was combined with the RDS weights using the RDS-II function before being exported for additional analysis. The frequency in their raw, median, inter-quartile range (IQR), and RDS-adjusted forms was computed using STATA software. The ODK software’s data were exported to MS Excel, cleaned up, and then imported into STATA Verssion16 for analysis.
Owing to the different geographic areas, GBV prevalence and the associated factors could be influenced by the differences in site (city/town)-level factors. A multilevel logistic regression analysis was considered to assess for variation by town and identify their association with the independent variables. This analysis used a two-level multilevel fixed-effect logistic regression model. Level 1 variables were all the independent variables categorized as individual-level variables and level 2 variables were the towns. To measure the impact of the level 2 variables (town) in the multilevel regression model, we used intra-class correlation (ICC), and the between-town variation accounted for a portion of the total variation in the response variable. The effects of individual-level predictors were quantified by the estimates from the fixed-effect part of the model with a p-value less than 0.05 at 95% CI that did not include one.
Ethical considerations
The study protocol and procedures were approved by the Research Ethics Committee of the Ethiopian Public Health Institute (Ethics reference number: EPHI-IRB-108-2018). FSWs were invited to participate in the study after receiving a brief introduction to the aims of the study and the potential risks and benefits of participating in the study. Those who provided verbal informed consent were interviewed one-on-one in a private room by trained interviewers. The collected data were kept confidentially and secured in the Ethiopian Public Health Institute’s database.
Results
Socio-demographic and other related characteristics
In total, 6,085 FSWs were recruited from the 16 survey sites. The median age of participants was 25.0 IQR of ±8 years [22, 30]. More than four-fifths (82.7%) of them were literate (attended primary school and above). A majority (85%) consumed alcohol, and approximately 62.9% of them chewed Catha edulis (khat) (Table 1). Nearly two-thirds (61.5%) of them had up to 60 paying partners in the last 6 months, and most (81%) stayed in the same town in the past 12 months before the survey (Table 2).
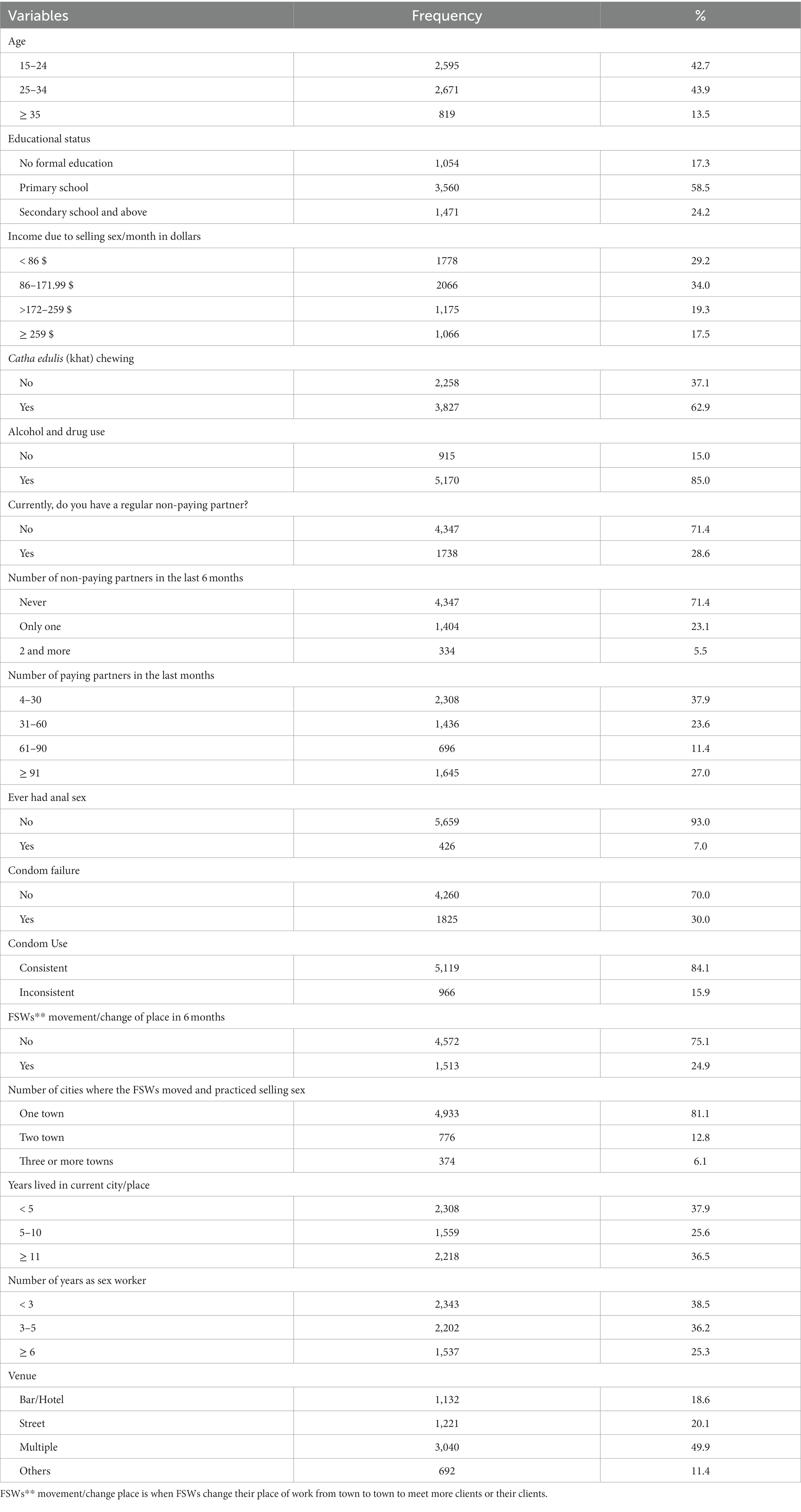
Table 2. Socio-demographics and other related characteristics of female sex workers in Ethiopia (N = 6,085).
Prevalence of types of gender-based violence
Among the 6,085 FSWs aged 15 years and above who participated in the study, over a quarter (1710) [28.1%; 95% CI (26.99, 29.25)] had experienced physical or sexual violence or both types in the last 12 months before the survey, of which 1,354 [22.3%; 95% CI (21.23, 23.31)] and 771 [12.7%; 95% CI (11.86, 13.53)] experienced physical violence and sexual violence, respectively (Table 3).
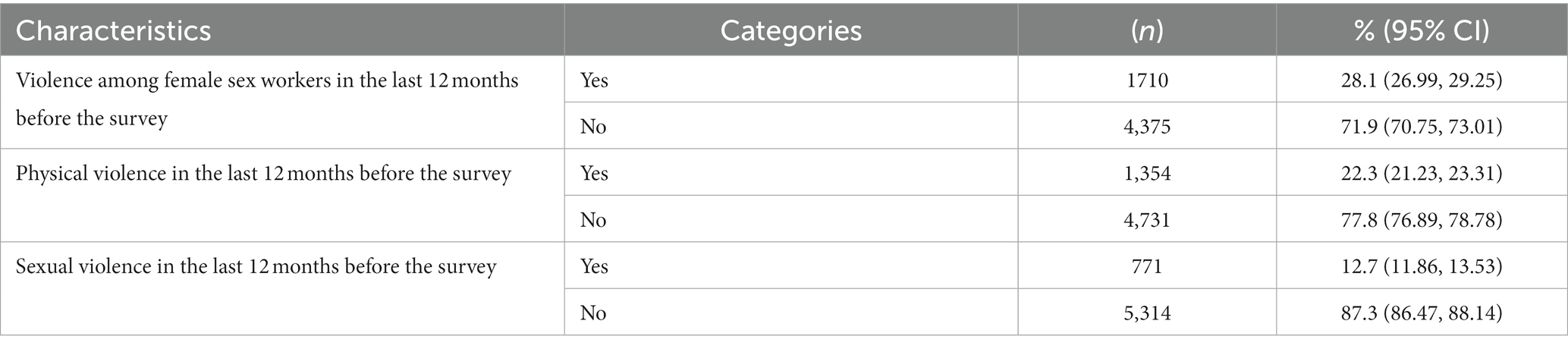
Table 3. Prevalence and types of violence among female sex workers in Ethiopia (N = 6,085).
Gender-based violence perpetrators and victims reported to the police
Nearly four-fifth (77.9%) of the perpetrators who committed GBV were paying partners followed by non-paying partners other than regular non-paying partners (10.5%) (Figure 1). Only 20% of the victims reported to the police (Figure 2).
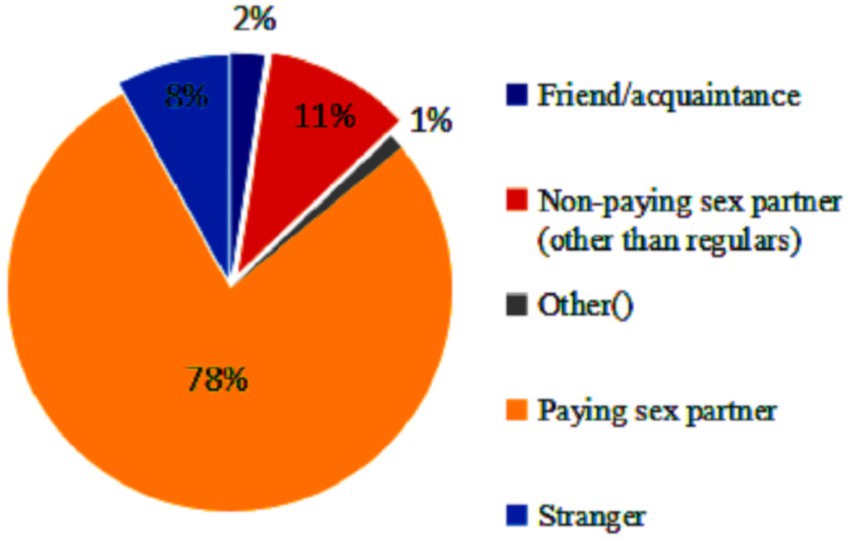
Figure 1. Perpetrators of violence.
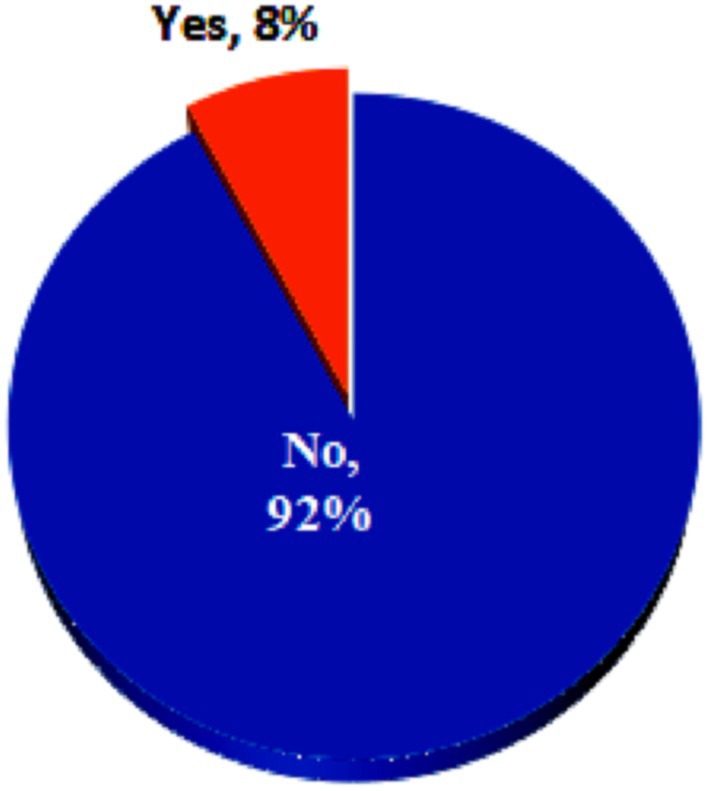
Figure 2. Victims reported to the police.
Gender-based violence and associated factors
The results on the multilevel fixed-effect logistic regression model diagnosis show that the model fitted well for the data over the standard logistic regression to assess determinants for GBV ( ). The results of the ICC of the two multilevel models revealed that approximately 8.0% of the variations in the likelihood of GBV were explained by the variation among the towns in Ethiopia. As we can see from the 95% CI [0.04, 0.15], the variation among the towns was statistically significant, and hence any estimation without considering this effect will result in a biased estimate (Table 4).
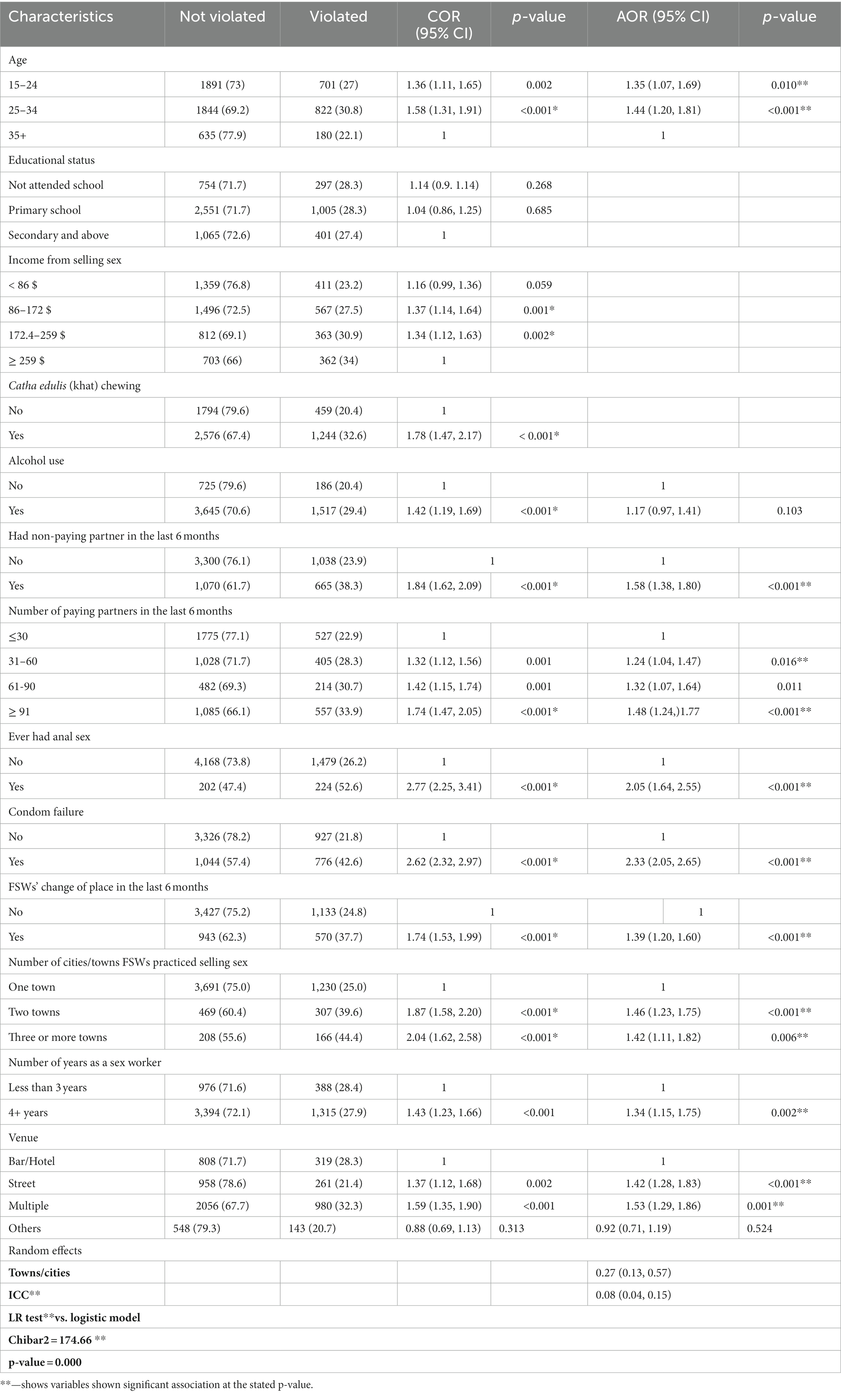
Table 4. Bivariate and multivariate logistic regression analyses of gender-based violence and associated factors among female sex workers.
The fixed effect of the multilevel logistic regression analysis indicated that age groups 5–24 and 25–34 years [AOR = 1.35; 95% (1.07, 1.69); p = 0.01] and [AOR = 1.44; 95% CI (1.20, 1.81); p < 0.001] than age group 35 years or more have shown an association with GBV among FSWs. Concerning partners’ characteristics; having a non-paying partner [AOR = 1.58; 95% CI (1.38, 1.80); p < 0.001] than paying; number of paying partners having 31–60, 61–90; and ≥ 91 which were [AOR = 1.24; 95% CI (1.04, 1.47); p = 0.016], [AOR = 1.32; 95% CI (1.07, 1.64); p = 0.011)], and [AOR = 1.48; 95% CI (1.24, 1.77); p < 0.001] than with less than 30, respectively, have shown association with GBV among FSWs. It also indicated that the trend of GBV among FSWs increased with an increase in the number of paying partners. Related to sexual act, those FSWs who ever had on the other side, sexual acts ever had anal sex [AOR = 2.05; 95% CI (1.64, 2.55); p < 0.001] than those not; condom failure [AOR = 2.33; 95% CI (2.05, 2.65); p < 0.001] than those not, and number of years 3–5, and 6 years or more [AOR = 1.21; 95% CI (1.05, 1.41)] and [AOR = 1.34; 95% CI (1.15, 1.75); p = 0.002) than those stayed less than 3 years in selling sex, respectively, were associated with FSWs GBV.
Regarding the environment in which FSWs reside and sell sex; changing place or mobile than those not in the last 6 months [AOR = 1.39; 95% CI (1.20, 1.60); p < 0.001]; the number of cities two and three or more FSWs stayed and selling sex [AOR = 1.46; 95% CI (1.23, 1.75); p < 0.00] and [AOR = 1.42; 95% CI (1.11, 1.82); p = 0.006], respectively, than those stayed at one town/city, sex work in the street and multiple places [AOR = 1.42; 95% CI (1.28, 1.83); p < 0.001] and [AOR = 1.53 95% CI (1.29, 1.86); p = 0.001] than those use other venue, respectively, were associated with GBV among FSWs.
Discussion
The overall prevalence of GBV experienced among FSWs in our study was 28.1%, which falls within the range of globally reported GBV prevalence among this population group (4). The prevalence of GBV among FSWs by our study was approximately a third of that reported by studies conducted in Mombasa, Kampala, and Mekele (11, 12, 15) and less than half of that reported from Latin America and the Caribbean, Nigeria, Zambia, and Tanzania (7, 12, 13, 17). On the other hand, our finding was almost similar to what had been reported from south India (30.5%) and the finding from a meta-analysis of isolated studies in Ethiopia (16), while it was higher than what was reported by a study in Iran and the Middle East (6). These variations could be due to the variations in sociocultural differences between the countries and/or the continents.
The physical violence and the sexual violence among FSWs in our study were 22.3% and 12.8%, respectively. The prevalence of physical violence among FSWs was similar to what had been reported by the study conducted in Mombasa, Kenya, but was two times more than the finding from South India (8, 11), three times more than the prevalence reported by Tanzania (13), and two times less than what was reported by the study from Nigeria (17). On the other hand, sexual violence in our study showed a similar finding to the study conducted in South India among mobile FSWs but three times less than the findings from Nigeria and Tanzania and five times less than what was reported from North Karnataka in South India (9, 13, 17).
The wide variation in the prevalence and type of gender-based violence among FSWs across countries indicates specific individual characteristics and contextual factors need to be understood to design prevention and response interventions. Among the FSWs in the study, we documented that age, having non-paying partners and number of paying partners in the 6 months preceding data collection, having ever had anal sex, mobility of FSWs, number of towns where they practiced selling sex, number of years the FSWs stayed in selling sex, and the venue at which selling sex was practiced were associated with violence.
Our finding on prevalence and predictors of sexual violence among FSWs concurs with the report from a study conducted in Northern Ethiopia, which showed that FSWs in the younger age group had a higher rate of violence than the older age category (15). In contrast, a study in Nigeria identified more violence among older FSWs than the younger age group (17). This might be explained as the older age group FSWs could have more awareness of it and experience in escaping from perpetrators, while the differences could be due to sociocultural and other drivers of GBV among FSWs in the two countries. Among other factors associated with FSWs, GBV in our study was having non-paying partners in the last 6 months. This was similar to the findings from North Karnataka in South India, which examined determinants of GBV among FSWs in an intimate partner relationship (9). Similar to the study conducted in Zambia, our study showed that the number of paying partners in the last 6 months was associated with GBV among FSWs, while having more than nine paying partner by our study has half less GBV among FSWs than the finding from Zambia (12).
We also found that FSWs who ever practiced anal sex experienced GBV more often than their counterparts, which was similar to what was reported by the African Sex Work Alliance among FSWs in Nairobi but two times more than that was reported by the study conducted at Kampala (12). Regarding FSW mobility and the number of cities and towns where they practiced selling sex in association with GBV, the finding from our study was similar to the findings from the study conducted in India and Northern Vietnam (20, 21).
This study also identified an association between GBV and the number of years of selling sex (more than 3 years) sex by FSWs. This finding corroborated the similarity with the finding from a study conducted in Northern Ethiopia (19). Concurring with the findings from the Ethiopia National Survey on FSWs (16), the venue type where the FSWs used to sell sex was significantly associated with violence in our study. This indicated that there are still similarities in trends of venues where FSWs used to pickup their partners. Unlike previous studies (14–16), other socio-demographic and individual factors including educational status, income, and chewing Catha edulis (khat) were not associated with GBV among FSWSs in our study.
Limitations
As the findings from this study relied on self-reported measures, there might be social desirability and recall biases. These need to be considered in the interpretation of the results as well. The strength of the study was the nationally representative number of FSWs from cities and towns that participated, the respondent-driven sampling method (RDS) including eligible participants, and the multilevel logistic regression analysis that was applied to manage the individual level and intra-class correlation (ICC) between-town variation.
Conclusion and recommendation
The findings from this study revealed that violence among FSWs is high in Ethiopia. It also indicated that GBV among FSWs in Ethiopia is associated with socio-demographic factors, partner characteristics, and the environment where they practice sex selling. The study results have important implications for policy and program planning, prevention, and response to mitigate the occurrence and impact of GBV among FSWs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethiopian Public Health Institute IRB. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LN developed the concept of the study and contributed to the analysis, manuscript development, and submission. JA contributed to data analysis. SA was involved in manuscript development and review. JB, BB, FW, WB, and AH participated in manuscript development. SL carried out the manuscript review. All authors contributed to the article and approved the submitted version.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to acknowledge data collectors and supervisors, other stakeholders, the District Health Offices, and health facilities for their collaboration during the data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
FSW, female sex worker; GBV, gender-based violence; HIV, human immunodeficiency virus; NHSBS, National HIV and other STIs Bio-Behavioral Survey; RDS, respondent-driven sampling; STI, sexually transmitted disease; SNNPR, south nations and nationalities people region.
References
1. United Nations declaration on the elimination of violence against women, (1993); A/RES/48/104. 4. Available at:https://www.un.org/en/genocideprevention/documents/atrocity-crimes/Doc.21_declaration%20elimination%20vaw.pdf
2. Shannon, K, Goldenberg, SM, Deering, KN, and Strathdee, SA. HIV infection among female sex workers in concentrated and high prevalence epidemics: why a structural determinants framework is needed. Curr Opin HIV AIDS. (2014) 9:174–82. doi: 10.1097/COH.0000000000000042
3. Deering, KN, Amin, A, Shoveller, J, Nesbitt, A, Garcia-Moreno, C, Duff, P, et al. A systematic review of the correlates of violence against sex workers. Am J Public Health. (2014) 104:e42. doi: 10.2105/AJPH.2014.301909
4. Violence against women and HIV/AIDS: Critical inter-sections. Violence against sex workers and HIV prevention. World Health Organization. (2005). Available at: https://www.who.int/gender-equity-rights/knowledge/sexworkers.pdf?
5. Heylen, E, Shamban, E, Steward, WT, Krishnan, G, Solomon, R, Srikrishnan, AK, et al. Alcohol use and experiences of partner violence among female sex Workers in Coastal Andhra Pradesh, India. Violence Against Women. (2019) 25:251–73. doi: 10.1177/1077801218778384
6. Hosseini-Hooshyar, S, Mirzazadeh, A, Karamouzian, M, Sharifi, H, Khajehkazemi, R, Haghdoost, AA, et al. Prevalence and correlates of sexual violence experienced by female sex Workers in Iran: results from a national HIV bio-behavioral surveillance survey. Violence Against Women. (2022) 28:872–89. doi: 10.1177/10778012211008992
7. Evens, E, Lanham, M, Santi, K, Cooke, J, Ridgeway, K, Morales, G, et al. Experiences of gender-based violence among female sex workers, men who have sex with men, and transgender women in Latin America and the Caribbean: a qualitative study to inform HIV programming. BMC Int Health Hum Rights. (2019) 19:9. doi: 10.1186/s12914-019-0187-5
8. Swain, SN, Saggurti, N, Battala, M, Verma, RK, and Jain, AK. Experience of violence and adverse reproductive health outcomes, HIV risks among mobile female sex workers in India. BMC Public Health. (2011) 11:357. doi: 10.1186/1471-2458-11-357
9. Javalkar, P, Platt, L, Prakash, R, Beattie, T, Bhattacharjee, P, Thalinja, R, et al. What determines violence among female sex workers in an intimate partner relationship? Findings from North Karnataka, South India. BMC Public Health. (2019) 19:350. doi: 10.1186/s12889-019-6673-9
10. Hendriks, S, and Woensdregt, L. Sex Work and Violence in Southern Africa. A participatory research in Botswana, Mozambique, Namibia, South Africa and Zimbabwe. AIDS Fonds. (2018) 36. Available at: https://aidsfonds.org/assets/resource/file/Research%20report%20Handsoff%20Southern%20Africa.pdf.
11. Roberts, ST, Flaherty, BP, Deya, R, Masese, L, Ngina, J, McClelland, RS, et al. Patterns of gender-based violence and associations with mental health and HIV risk behavior among female sex Workers in Mombasa, Kenya: a latent class analysis. AIDS Behav. (2018) 22:3273–86. doi: 10.1007/s10461-018-2107-4
12. African Sex Worker Alliance. Every sex worker has got a story to tell about violence: Violence against sex workers in Africa. Nairobi: Kenyans’ Sex work association. (2019). Available at: https://keswa-kenya.org/assets/publications/visible-scars-brief.pdf.
13. Hendrickson, ZM, Leddy, AM, Galai, N, Mbwambo, JK, Likindikoki, S, and Kerrigan, DL. Work-related mobility and experiences of gender-based violence among female sex workers in Iringa, Tanzania: a cross-sectional analysis of baseline data from project Shikamana. BMJ Open. (2018) 8:e022621. doi: 10.1136/bmjopen-2018-022621
14. Worke, MD, Koricha, ZB, and Debelew, GT. Prevalence of sexual violence in Ethiopian workplaces: systematic review and meta-analysis. Reprod Health. (2020) 17:195. doi: 10.1186/s12978-020-01050-2
15. Alemayehu, M, Yohannes, G, Damte, A, Fantahun, A, Gebrekirstos, K, Tsegay, R, et al. Prevalence and predictors of sexual violence among commercial sex workers in northern Ethiopia, Alemayehu. Reprod Health. (2015) 12:47. doi: 10.1186/s12978-015-0036-5
16. Amogne, MD, Balcha, TT, and Agardh, A. Prevalence and correlates of physical violence and rape among female sex workers in Ethiopia: a cross-sectional study with respondent-driven sampling from 11 major towns. BMJ Open. (2019) 9:e028247. doi: 10.1136/bmjopen-2018-028247
17. Prevalence and correlates of violence against female sex workers in Abuja. Nigeria, Fawole Olufunmilayo I, Dagunduro Abosede T. Epidemiology and medical statistics, Faculty of Public Health, College of Medicine University of Ibadan, Nigeria. Afr Health Sci. (2014) 14:299–313. doi: 10.4314/ahs.v14i2.4
18. Scorgie, F, Chersich, MF, Ntaganira, I, Gerbase, A, Lule, F, and Lo, YR. Socio-demographic characteristics and behavioral risk factors of female sex workers in sub-Saharan Africa: a systematic review. AIDS Behav. (2012) 16:920–33. doi: 10.1007/s10461-011-9985-z
19. Van Blerk, L. AIDS, mobility and commercial sex in Ethiopia: Implications for policy In: Contested bodies of childhood and youth, vol. 4. Berlin: Springer (2010). 232–46.
20. Rushing, R, Watts, C, and Rushing, S. Living the reality of forced sex work: perspectives from young migrant women sex workers in northern Vietnam. J Midwifery Womens Health. (2005) 50:e41–4. doi: 10.1016/j.jmwh.2005.03.008
21. Ramesh, S, Ganju, D, Mahapatra, B, Mishra, RM, and Saggurti, N. Relationship between mobility, violence and HIV/STI among female sex workers in Andhra Pradesh, India. BMC Int Health Hum Rights. (2012) 12:764. doi: 10.1186/1471-2458-12-764
22. Ethiopian Public Health Institute (EPHI). Ethiopia population-based HIV impact assessment (EPHIA) 2017-2018: final report. Addis Ababa: EPHI; August 2020.
23. Merriam-Webster dictionary thesaurus., Available at: https://www.merriam-webster.com/
24. The health encyclopedia general information. Available at: https://en.wikipedia.org/wiki/Medical_encyclopedia
25. UNAIDS. The joint United Nations program on HIV/AIDS, brings together the efforts and resources of ten UN system organizations to the global AIDS response. Available at: https://data.unaids.org/pub/epislides/2007/2007_epiupdate_en.pdf.
Keywords: female sex workers, gender-based violence, sexual violence, physical violence, Perpetrators and victims
Citation: Debel L, Ayalew J, Abdella S, Bulti J, Bejiga B, Wariso FB, Belete W, Habtesilase A and Lulseged S (2024) Gender-based violence and associated factors among female sex workers in Ethiopia. Evidence from The National Bio-behavioral Survey, 2020. Front. Public Health. 11:1213725. doi: 10.3389/fpubh.2023.1213725
Edited by:
Aswathy Sreedevi, Amrita Vishwa Vidyapeetham University, IndiaReviewed by:
Sathish Thirunavukkarasu, Emory University, United StatesP. S. Rakesh, The Union South East Asia Office, India
Copyright © 2024 Debel, Ayalew, Abdella, Bulti, Bejiga, Wariso, Belete, Habtesilase and Lulseged. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lemessa Debel, bmxlbWVzc2FAZ21haWwuY29t