 Mathieu Jendly1
Mathieu Jendly1 Valérie Santschi2
Valérie Santschi2 Stefano Tancredi1
Stefano Tancredi1 Isabelle Konzelmann3
Isabelle Konzelmann3 Leila Raboud3
Leila Raboud3 Arnaud Chiolero1,3,4,5*
Arnaud Chiolero1,3,4,5*- 1Population Health Laboratory (#PopHealthLab), University of Fribourg, Fribourg, Switzerland
- 2La Source, School of Nursing Sciences, HES-SO University of Applied Sciences and Arts Western Switzerland, Lausanne, Switzerland
- 3Observatoire Valaisan de la Santé (OVS), Sion, Switzerland
- 4School of Population and Global Health, McGill University, Montreal, QC, Canada
- 5Institute of Primary Health Care (BIHAM), University of Bern, Bern, Switzerland
Background: Digital health technology can be useful to improve the health of patients with diabetes and to support patient-centered care and self-management. In this cross-sectional study, we described the eHealth profile of patients with diabetes, based on their use of digital health technology, and its association with sociodemographic characteristics.
Methods: We used data from the “Qualité Diabète Valais” cohort study, conducted in one region of Switzerland (Canton Valais) since 2019. Participants with type 1 or type 2 diabetes completed questionnaires on sociodemographic characteristics and on the use of digital health technology. We defined eHealth profiles based on three features, i.e., ownership or use of (1) internet-connected devices (smartphone, tablet, or computer), (2) mHealth applications, and (3) connected health tools (activity sensor, smart weight scale, or connected blood glucose meter). We assessed the association between sociodemographic characteristics and participants’ eHealth profiles using stratified analyses and logistic regression models.
Results: Some 398 participants (38% women) with a mean age of 65 years (min: 25, max: 92) were included. The vast majority (94%) were Swiss citizens or bi-national and 68% were economically inactive; 14% had a primary level education, 51% a secondary level, and 32% a tertiary level. Some 75% of participants had type 2 diabetes. Some 90% of the participants owned internet-connected devices, 43% used mHealth applications, and 44% owned a connected health tool. Older age and a lower educational level were associated with lower odds of all features of the eHealth profile. To a lesser extent, having type 2 diabetes or not being a Swiss citizen were also associated with a lower use of digital health technology. There was no association with sex.
Conclusion: While most participants owned internet-connected devices, only about half of them used mHealth applications or owned connected health tools. Older participants and those with a lower educational level were less likely to use digital health technology. eHealth implementation strategies need to consider these sociodemographic patterns among patients with diabetes.
1. Background
Diabetes is a major burden on the healthcare system and can have a major impact on patients’ quality of life (1). The risk of developing diabetes and its complications increases with age and lower levels of education (2). Within a patient-centered, evidence-based, and data-informed framework (3), improving the quality of care of patients with diabetes requires a multidisciplinary team of healthcare professionals, including physicians, pharmacists, or nurses (4, 5). Digital health technology, also known as eHealth, could help improve diabetes management by facilitating data exchange between patients and healthcare professionals, thus improving care practice and coordination. Within the field of eHealth, a distinction is made between mHealth (which refers to mobile health via applications on smartphones) and connected health tools (to measure and analyze health data) (6). For example, applications to monitor diet or exercise are considered as mHealth and digital blood glucose meters are connected health tools.
While there is no consensus on the effectiveness of eHealth in improving health outcomes, mounting evidence suggests that it could help, including among patients with diabetes (7). Hence, studies have shown that the use of digital health technology and mobile devices could help improve diabetes management, e.g., to reach lower level of glycated hemoglobin (HbA1c) or blood pressure (8, 9) as well as to improve psychosocial and physical well-being (10). It could also enable patient empowerment by allowing them to play an active role in the management of their disease (11). eHealth also has a positive impact on medication adherence (12) and in the management of polypharmacy (13), which is a major challenge among patients with chronic diseases like diabetes (14, 15).
Several factors however constrain eHealth tools implementation. Not all healthcare professionals are comfortable with digital health technology (16). Hence, they often have a poor digital health literacy and are not yet sufficiently trained to use these tools. The absence of strong evidence on their beneficial use, the ever-changing market of eHealth tools, and their cost are also limiting factors (17, 18). Furthermore, several barriers at the patient level hinder the use of eHealth tools, including socioeconomic and demographic factors (17). Indeed, there is a socioeconomic divide in digital health, with patients of lower socioeconomic status having lower digital literacy and limited access to digital health tools (19, 20). A scoping review on the factors influencing the digital divide identified age, ethnicity, and education, together with health status and eHealth literacy, as factors influencing the use of digital health technologies (21). A recent example that highlighted the lack of equity in digital health was the COVID-19 pandemic, where populations with the lowest socioeconomic status were less likely to integrate digital health innovations into their daily lives or usual care (22). Socio-patterns of eHealth use need to be better understood if policymakers are to design equitable strategies to promote digital health (23), including among patients with diabetes.
Our aim was, therefore, to evaluate the eHealth profile of patients with diabetes, based on their use of digital health technology, and assess its association with sociodemographic characteristics.
2. Participants and methods
2.1. Study design
We used data from a prospective cohort study (“Qualité Diabète Valais”) conducted by the Observatoire Valaisan de la Santé (OVS1) which aims to evaluate the quality of care and the quality of life of patients with diabetes in the canton of Valais, Switzerland (24, 25). For the current study, we performed a cross-sectional analysis of the data collected at baseline. Ethical approval was obtained to conduct the cohort study (ethics committee “Commission cantonale d’éthique de la recherche sur l’être humain CER-VD,” file number 2019–01668).
2.2. Participants
Participants were recruited in collaboration with several institutions and healthcare professionals in the Canton of Valais. Eligible patients were informed about the objectives of the study and the possibility of participating in the cohort. Volunteers were enrolled after a telephone interview with the OVS between December 2019 and December 2022. During the interview, detailed information about the study was provided and inclusion and exclusion criteria were reviewed. To be included in the study, participants had to meet the following inclusion criteria: (1) be 25 years or older; (2) have a physician-confirmed diagnosis of type 1 or 2 diabetes; (3) residency in Valais (Switzerland); (4) be able to take informed decisions. Exclusion criteria were: (1) gestational diabetes; (2) corticoid-induced diabetes; (3) severe cognitive impairment or other illness that prevented understanding the content of the information sheet; (4) insufficient knowledge of the French or German language (24). All participants signed an informed consent form.
2.3. Data collection and measurement
At baseline, participants completed a self-administered questionnaire to assess their sociodemographic characteristics, health status, quality of care, use of the health care system, health behaviors, quality of life and use of digital health technology.
For the current analysis, we used the following sociodemographic data and participants’ characteristics: age, sex, citizenship (Swiss or bi-national, non-Swiss), type of diabetes (type 1 or 2), marital status (single, in a relationship), household type (living alone, living in a couple), occupational status (active, inactive) and highest education level attained (primary, secondary, tertiary). Eight participants reported not knowing their type of diabetes. Type 2 diabetes is much more frequent in the population and type 1 diabetes requires greater patient involvement, making them more aware of the diagnosis. Furthermore, these participants were diagnosed at an old age. They were therefore assigned to the “type 2″ group. To describe the participants’ eHealth profile, we used the following information on digital health technology use: (1) ownership of an internet-connected device (smartphone, tablet, or computer); (2) use of a mHealth application (such as diet or exercise applications) and reasons for not using mHealth applications; (3) ownership of a connected health tool (activity sensor, smart weight scale, or connected blood glucose meter). We did not have information on the type of mHealth applications used by participants.
2.4. Statistical analysis
We presented descriptive statistics of the participants’ characteristics and their eHealth profile. We examined the association between participants’ characteristics and participants’ eHealth profile using stratified analyses and logistic regression models. Two models fitted to estimate the odds ratios: a model 1 unadjusted and a model 2 adjusted for age, sex, citizenship, type of diabetes, marital status, household type, occupational status, and highest education level attained. Statistical analyses were performed using Stata 17 software (Stata Corp, TX, 2021).
3. Results
The characteristics of the 398 participants recruited between December 2019 and December 2022 are shown in Table 1. The mean age was 65 years (min: 25, max: 92) and 38% were women. The majority were Swiss citizens or bi-national (94%) and economically inactive (68%). Some 14% had a primary level education, 51% a secondary level, and 32% a tertiary level. Most of the participants (75%) had type 2 diabetes.
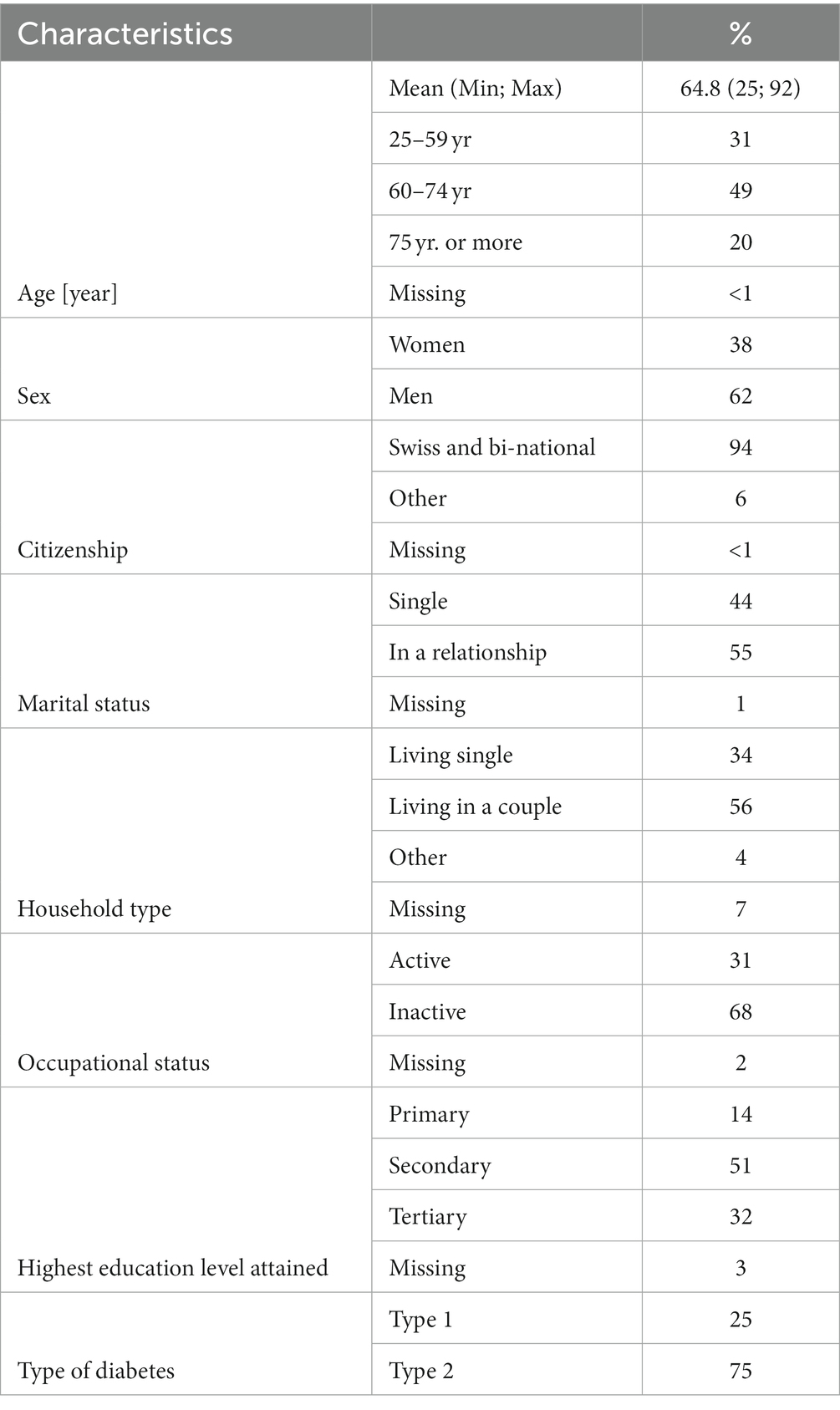
Table 1. Characteristics of participants (N = 398).
Descriptive statistics of the participants’ eHealth profile are shown in Table 2. Some 90% of the participants owned an internet-connected device (smartphone, tablet, or computer), and 43% reported using mHealth. When asked about the reasons for not using mHealth, the most common responses were that they did not need it (45%), that it was too complicated (34%), that they did not find the application relevant to their health problem (14%). Only 2% said that it was too expensive. Some 44% of participants owned a connected health tool, the most common being connected blood glucose meters (31%) and activity sensors (25%).
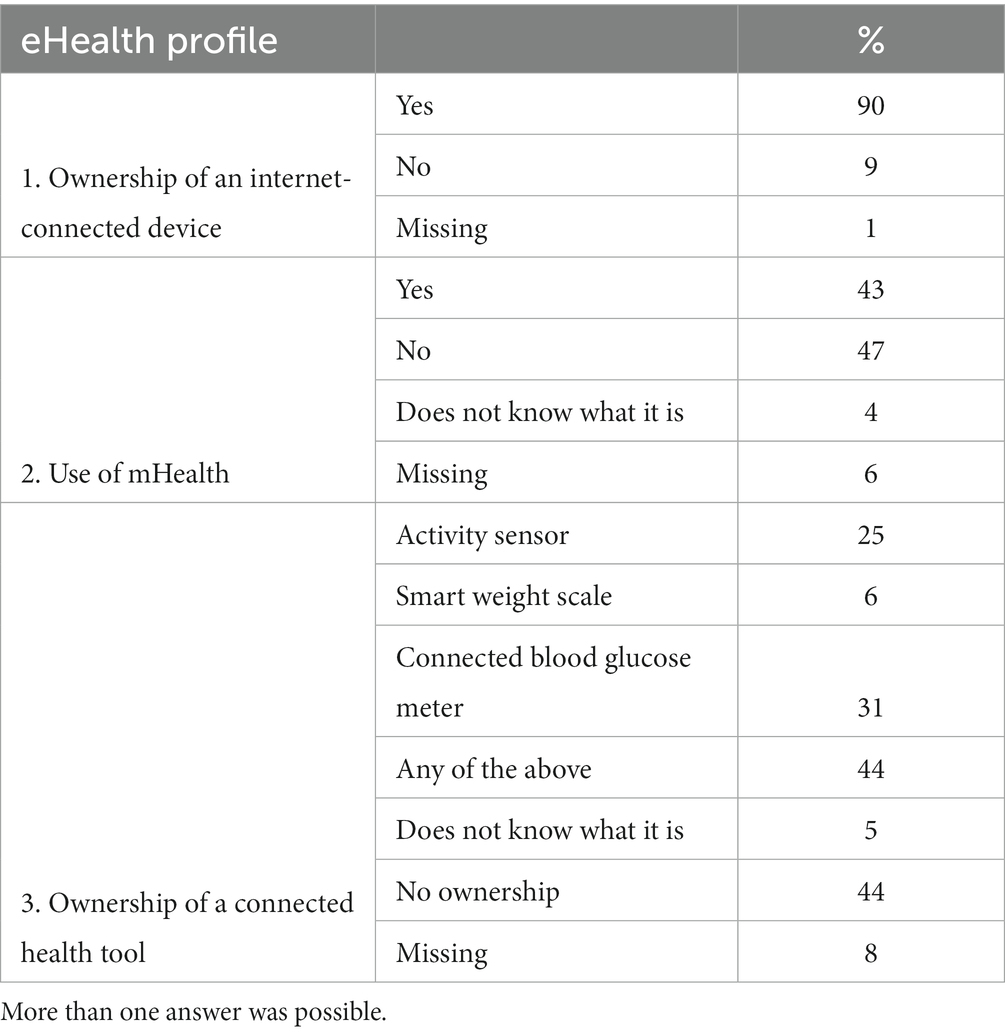
Table 2. eHealth profile of participants (N = 398).
The eHealth profile of participants according to their characteristics is shown in Supplementary Table S1 and Figure 1. All features of eHealth profile were related to age and to level of education. The higher the age and the lower the educational level, the less likely participants were to own internet-connected devices, to use mHealth applications, and to own connected health tools (Figure 1).
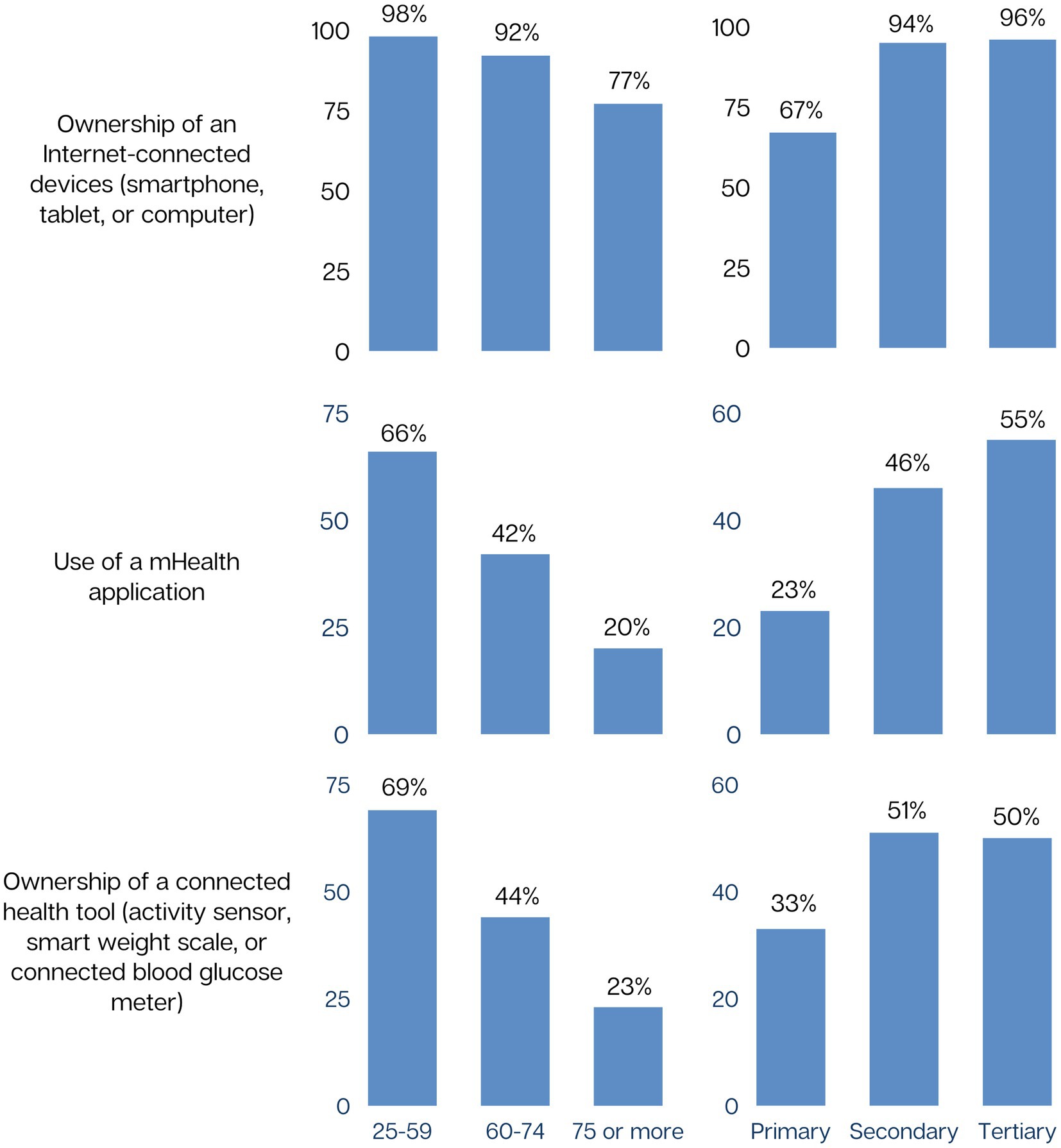
Figure 1. eHealth profile by age and education (N = 398).
After adjusting for participants’ characteristics, age and education remained associated with owning an internet-connected device (Table 3), using mHealth applications (Table 4), and owning connected health tools (Table 5). Use of mHealth and ownership of connected health tools were less frequent among Non-Swiss and type 2 diabetes patients. Features of the eHealth profile were not associated with sex, marital status, occupational status, or household type.
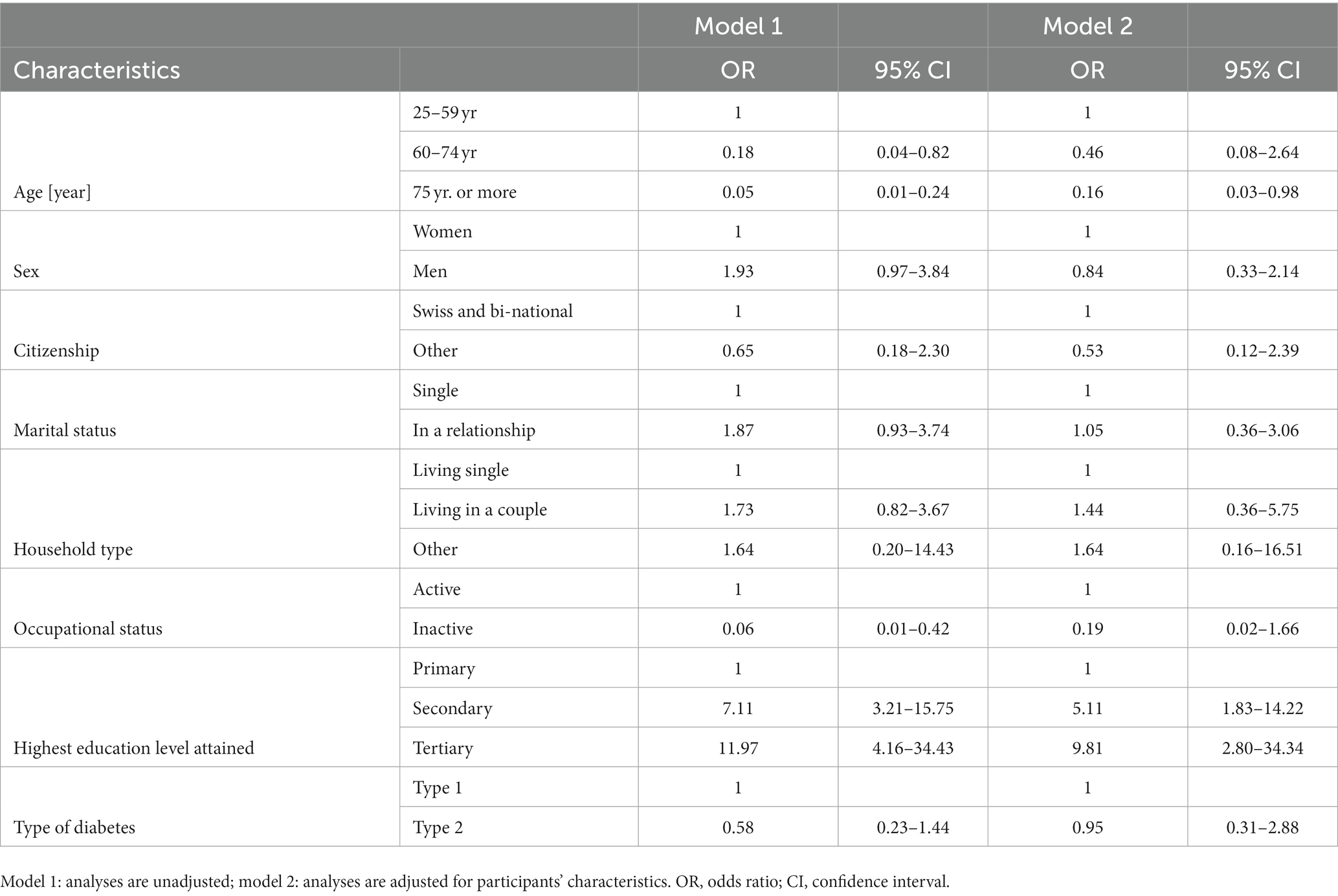
Table 3. Association between participants’ characteristics and ownership of an internet-connected device (N = 398).
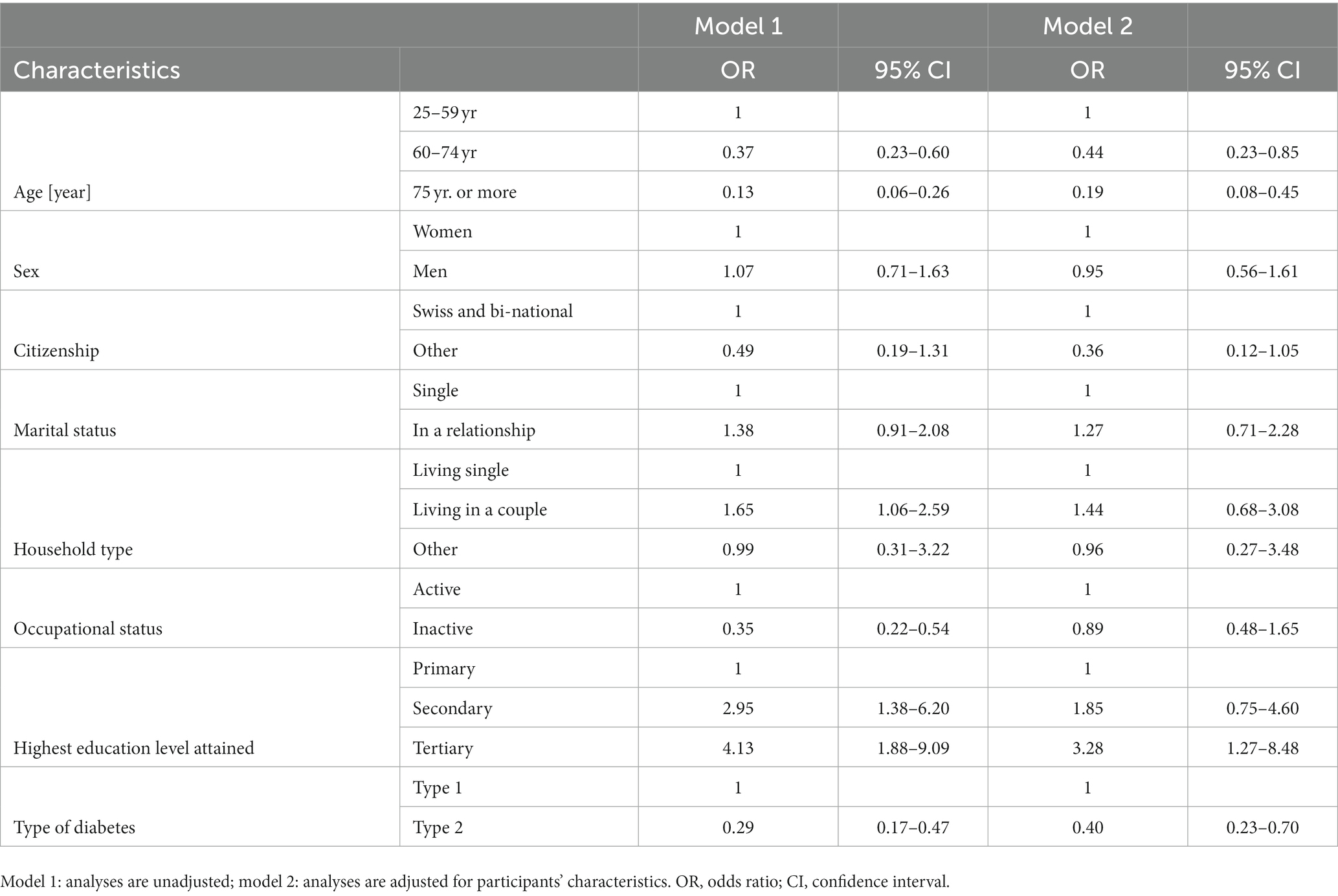
Table 4. Association between participants’ characteristics and use of mHealth (N = 398).
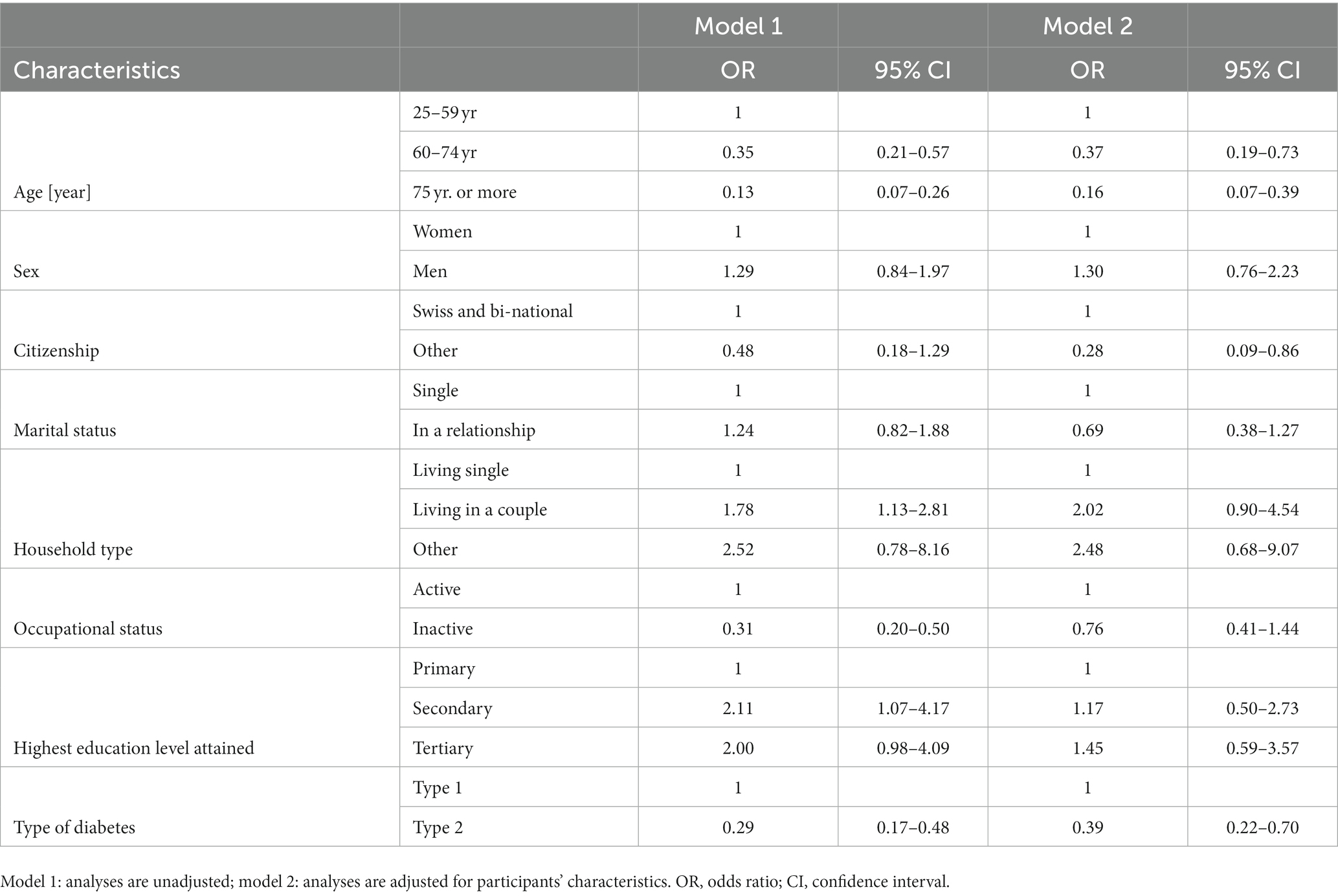
Table 5. Association between participants’ characteristics and ownership of a connected health tool (N = 398).
4. Discussion
The aim of this study was to describe the eHealth profile of patients with diabetes in one region of Switzerland, and its relationship with sociodemographic factors. We found that most participants owned an internet-connected device (smartphone, computer, or tablet) and that about half of them used mHealth applications and owned connected health tools, especially connected blood glucose meters and activity sensors. Older age and a lower educational level were associated with lower odds of all features of the eHealth profile. To a lesser extent, having type 2 diabetes was also associated with a lower use of digital health technology. This could be due to differences in treatment approaches for type 1 and type 2 diabetes, as type 1 diabetes is treated with insulin and requires strict glucose monitoring before insulin administration, and type 2 diabetes is often treated with metformin, without the need to measure glucose levels beforehand. Not being a Swiss or bi-national citizen was also associated with a lower use of digital health technology. There was no association between sex and the features of the eHealth profile.
A survey conducted in Switzerland in 2022 found that around half of the Swiss population used digital health tools (mHealth and connected health tools combined). Greater use was associated with younger age, higher education, higher income, and greater digital health literacy (26). Our findings are also consistent with some other studies on eHealth use in patients with diabetes or other chronic diseases. For example, a 2019 literature review investigating socio-demographic factors influencing eHealth use in patients with chronic diseases found that “higher age and lower income, lower education, living alone, and living in rural areas were […] associated with lower eHealth use” (27). In another study conducted in Australia, several factors were associated with a lower likelihood of access to eHealth: higher age, lower education, low digital literacy, low socioeconomic status, and living in remote areas (28). In addition, one study found that the same factors-older age, ethnic minority, and lower education-were associated with less readiness to use areas of eHealth such as teleconsultation and digital prescribing. Patients with diabetes were also less ready for eHealth than the general population (29).
While this study focuses only on personal characteristics of patients associated with eHealth use, the acceptability of eHealth to healthcare professionals is also another important determinant of eHealth use. In an umbrella review, it was found that positive attitudes of healthcare professionals toward eHealth (such as beliefs that the new systems would benefit patients, interest in the technologies, usefulness, and motivation in working with the systems) increase its acceptance and implementation, while negative attitudes (beliefs that electronic systems would disrupt the delivery of care; doubts that these systems can improve patient care, clinical outcomes or the quality of medical practices; and distrust in the systems as well as a more general staff resistance to change) decrease it (30). The current study shows that the use of eHealth by patients with diabetes is quite high, and that should drive health professionals to give more interest in the use of this technology in usual clinical activity.
This study has a few limitations. First, the sample size was relatively small. Second, we recruited participants on a voluntary basis, implying that our sample is only partly representative of the population of patients with diabetes. For example, the proportion of participants with type 1 diabetes (25%) was much higher than in the general population, where type 1 diabetes accounts for approximately 5–10% of all diagnosed cases of diabetes (31). Moreover, recruiting only voluntary participants might have introduced a “healthy user bias,” participants probably being better informed and having a higher health and digital health literacy compared to usual patients with diabetes. Third, information bias is also possible because the information collected by the questionnaire was self-reported. Fourth, we had no information on why patients were using eHealth tools. Finally, participants were relatively old and we could not accurately assess the eHealth profile of young participants with diabetes. More research is needed to further investigate the use of eHealth in younger patients with diabetes.
Our results suggest that older patients of relatively low educational level, who are the patients with the highest diabetes related morbidity and mortality rates, are also the least likely to use eHealth. If the benefits of eHealth are confirmed, it means that policy for its implementation should target these groups to have their access to eHealth strengthened. The Organization for Economic Co-operation and Development (OECD) has published a report suggesting that in order to implement eHealth in clinical practice, governments need to meet three objectives: increase the confidence of healthcare workers and patients in the benefits of digital transformation, increase the knowledge and skills needed to use digital health technologies effectively, and adapt the organization of healthcare services and the legal and financial operating frameworks (32).
In conclusion, while most patients with diabetes owned internet-connected devices such as smartphones, tablets, or computers, only about half of them used mHealth applications or owned connected health tools. The oldest participants and those with lower educational levels were the least likely to use eHealth, despite being the groups that could benefit the most from it.
Data availability statement
Datasets are available upon request to the corresponding author.
Ethics statement
The studies involving humans were approved by ethics committee “Commission cantonale d’éthique de la recherche sur l’être humain CER-VD,” file number 2019-01668. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants.
Author contributions
AC, IK, and LR designed the “Qualité Diabète” study. MJ, VS, and ST wrote the protocol for the current analysis. IK and LR recruited participants and managed data necessary for this study. MJ analyzed the data under the guidance of ST and drafted the manuscript with contributions of VS, ST, and AC. All authors revised and approved the final version of the manuscript before submission.
Funding
The “Qualité Diabète” project is financed by the canton of Valais and the Valais diabetes associations via the “Action Diabète” project supported by Promotion Santé Suisse. There is no specific funding for this analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1240879/full#supplementary-material
Footnotes
1. ^www.ovs.ch
References
1. Björk, S. The cost of diabetes and diabetes care. Diabetes Res Clin Pract. (2001) 54:13–8. doi: 10.1016/S0168-8227(01)00304-7
2. Hill-Briggs, F, Adler, NE, Berkowitz, SA, Chin, MH, Gary-Webb, TL, Navas-Acien, A, et al. Social determinants of health and diabetes: a scientific review. Diabetes Care. (2021) 44:258–79. doi: 10.2337/dci20-0053
3. Chiolero, A, Rodondi, N, and Santschi, V. High-value, data-informed, and team-based care for multimorbidity. Lancet Public Health. (2020) 5:e84. doi: 10.1016/S2468-2667(20)30007-4
4. Santschi, V, Chiolero, A, Paradis, G, Colosimo, AL, and Burnand, B. Pharmacist interventions to improve cardiovascular disease risk factors in diabetes. Diabetes Care. (2012) 35:2706–17. doi: 10.2337/dc12-0369
5. Huber, CA, Schwenkglenks, M, Rapold, R, and Reich, O. Epidemiology and costs of diabetes mellitus in Switzerland: an analysis of health care claims data, 2006 and 2011. BMC Endocr Disord. (2014) 14:44. doi: 10.1186/1472-6823-14-44
6. Pais, B, and Buluschek, DP. De nouvelles technologies au service du maintien à domicile des personnes âgées. Rev Med Suisse. (2019) 15:1407–11. doi: 10.53738/REVMED.2019.15.658.1407
7. Elbert, NJ, van Os-Medendorp, H, van Renselaar, W, Ekeland, AG, Hakkaart-van Roijen, L, Raat, H, et al. Effectiveness and cost-effectiveness of eHealth interventions in somatic diseases: a systematic review of systematic reviews and meta-analyses. J Med Internet Res. (2014) 16:e110. doi: 10.2196/jmir.2790
8. Wu, X, Guo, X, and Zhang, Z. The efficacy of Mobile phone apps for lifestyle modification in diabetes: systematic review and meta-analysis. JMIR Mhealth Uhealth. (2019) 7:e12297. doi: 10.2196/12297
9. Shan, R, Sarkar, S, and Martin, SS. Digital health technology and mobile devices for the management of diabetes mellitus: state of the art. Diabetologia. (2019) 62:877–87. doi: 10.1007/s00125-019-4864-7
10. Bassi, G, Mancinelli, E, Dell’Arciprete, G, Rizzi, S, Gabrielli, S, and Salcuni, S. Efficacy of eHealth interventions for adults with diabetes: a systematic review and meta-analysis. Int J Environ Res Public Health. (2021) 1:1–2. doi: 10.3390/ijerph2004010001
11. Ashrafzadeh, S, and Hamdy, O. Patient-driven diabetes care of the future in the technology era. Cell Metab. (2019) 29:564–75. doi: 10.1016/j.cmet.2018.09.005
12. Pouls, BPH, Vriezekolk, JE, Bekker, CL, Linn, AJ, Van Onzenoort, HAW, Vervloet, M, et al. Effect of interactive eHealth interventions on improving medication adherence in adults with long-term medication: systematic review. J Med Internet Res. (2021) 23:e18901. doi: 10.2196/18901
13. Santschi, V, Rodondi, N, Bugnon, O, and Burnier, M. Impact of electronic monitoring of drug adherence on blood pressure control in primary care: a cluster 12-month randomised controlled study. Eur J Intern Med. (2008) 19:427–34. doi: 10.1016/j.ejim.2007.12.007
14. Markovič, R, Grubelnik, V, Vošner, HB, Kokol, P, Završnik, M, Janša, K, et al. Age-related changes in lipid and glucose levels associated with drug use and mortality: an observational study. JPM. (2022) 12:280. doi: 10.3390/jpm12020280
15. Markovič, R, Grubelnik, V, Završnik, T, Blažun Vošner, H, Kokol, P, Perc, M, et al. Profiling of patients with type 2 diabetes based on medication adherence data. Front Public Health. (2023) 11:1209809. doi: 10.3389/fpubh.2023.1209809
16. Levine, BJ, Close, KL, and Gabbay, RA. Reviewing U.S. connected diabetes care: the newest member of the team. Diabetes Technol Ther. (2020) 22:1–9. doi: 10.1089/dia.2019.0273
17. Schreiweis, B, Pobiruchin, M, Strotbaum, V, Suleder, J, Wiesner, M, and Bergh, B. Barriers and facilitators to the implementation of eHealth services: systematic literature analysis. J Med Internet Res. (2019) 21:e14197. doi: 10.2196/14197
18. Pais, B, Buluschek, P, DuPasquier, G, Nef, T, Schütz, N, Saner, H, et al. Evaluation of 1-year in-home monitoring technology by home-dwelling older adults, family caregivers, and nurses. Front Public Health. (2020) 8:8. doi: 10.3389/fpubh.2020.518957
19. Rodriguez, JA, Clark, CR, and Bates, DW. Digital health equity as a necessity in the 21st century cures act era. JAMA. (2020) 323:2381. doi: 10.1001/jama.2020.7858
20. Lyles, CR, Wachter, RM, and Sarkar, U. Focusing on digital health equity. JAMA. (2021) 326:1795. doi: 10.1001/jama.2021.18459
21. Yao, R, Zhang, W, Evans, R, Cao, G, Rui, T, and Shen, L. Inequities in health care services caused by the adoption of digital health technologies: scoping review. J Med Internet Res. (2022) 24:e34144. doi: 10.2196/34144
22. Shaw, J, Brewer, LC, and Veinot, T. Recommendations for health equity and virtual care arising from the COVID-19 pandemic: narrative review. JMIR Form Res. (2021) 5:e23233. doi: 10.2196/23233
23. Richardson, S, Lawrence, K, Schoenthaler, AM, and Mann, D. A framework for digital health equity. NPJ Digital Med. (2022) 5:119. doi: 10.1038/s41746-022-00663-0
24. Qualité Diabète Valais-OVS. (2020). Available at: https://www.ovs.ch/diabete/ (Accessed July 19, 2023).
25. Association Valaisannes du Diabète. Action Diabète Valais. (2021). Available at: https://www.actiondiabete.ch/home/ (Accessed May 13, 2023).
26. Sternberg, J. A Swiss digital healthcare system: what the population thinks. digitalswitzerland. (2022). Available at: https://digitalswitzerland.com/digital-health-study/ (Accessed July 19, 2023).
27. Reiners, F, Sturm, J, Bouw, LJW, and Wouters, EJM. Sociodemographic factors influencing the use of eHealth in people with chronic diseases. Int J Environ Res Public Health. (2019) 16:645. doi: 10.3390/ijerph16040645
28. Alam, K, Mahumud, RA, Alam, F, Keramat, SA, Erdiaw-Kwasie, MO, and Sarker, AR. Determinants of access to eHealth services in regional Australia. Int J Med Inform. (2019) 131:103960. doi: 10.1016/j.ijmedinf.2019.103960
29. AshaRani, P, Jue Hua, L, Roystonn, K, Siva Kumar, FD, Peizhi, W, Ying Jie, S, et al. Readiness and acceptance of eHealth services for diabetes care in the general population: cross-sectional study. J Med Internet Res. (2021) 23:e26881. doi: 10.2196/26881
30. Ross, J, Stevenson, F, Lau, R, and Murray, E. Factors that influence the implementation of e-health: a systematic review of systematic reviews (an update). Implementation Sci. (2016) 11:146. doi: 10.1186/s13012-016-0510-7
31. Centers for Disease Control and Prevention (CDC). Diabetes fast facts. (2023). Available at: https://www.cdc.gov/diabetes/basics/quick-facts.html (Accessed May 13, 2023).
Keywords: eHealth, mHealth, diabetes, quality of care, digital health technology, self-management, equity
Citation: Jendly M, Santschi V, Tancredi S, Konzelmann I, Raboud L and Chiolero A (2023) eHealth profile of patients with diabetes. Front. Public Health. 11:1240879. doi: 10.3389/fpubh.2023.1240879
Edited by:
Peter Kokol, University of Maribor, SloveniaReviewed by:
Rene Markovič, University of Maribor, SloveniaPedro Elkind Velmovitsky, University of Waterloo, Canada
Copyright © 2023 Jendly, Santschi, Tancredi, Konzelmann, Raboud and Chiolero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Arnaud Chiolero, YXJuYXVkLmNoaW9sZXJvQHVuaWZyLmNo