 Tamin Ortiz-Gómez1
Tamin Ortiz-Gómez1 Andrea C. Gomez2
Andrea C. Gomez2 Brigitte Chuima1
Brigitte Chuima1 Alejandra Zevallos3Karen Ocampo1
Alejandra Zevallos3Karen Ocampo1 Diana Torres1,4
Diana Torres1,4 Joseph A. Pinto2*
Joseph A. Pinto2*- 1Laboratorios AUNA, Área de Biología Molecular, Lima, Peru
- 2Centro de Investigación Básica y Translacional, AUNA IDEAS, Lima, Peru
- 3Escuela Profesional de Medicina Humana, Universidad Privada San Juan Bautista, Lima, Peru
- 4Escuela Profesional de Medicina Humana, Universidad Privada Norbert Wiener, Lima, Peru
Introduction: In Peru, on 11 February 2023, the Ministry of Health registered 4 million patients infected with COVID-19 and around 219,260 deaths. In 2020, the SARS-CoV-2 virus was acquiring mutations that impacted the properties of transmissibility, infectivity, and immune evasion, leading to new lineages. In the present study, the frequency of COVID-19 variants was determined during 2021 and 2022 in patients treated in the AUNA healthcare network.
Methods: The methodology used to detect mutations and identify variants was the Allplex™ SARS-CoV-2 Variants Assay I, II, and VII kit RT-PCR. The frequency of variants was presented by epidemiological weeks.
Results: In total, 544 positive samples were evaluated, where the Delta, Omicron, and Gamma variants were identified. The Delta variant was found in 242 (44.5%) patients between epidemiological weeks 39 and 52 in 2021. In the case of Gamma, it was observed in 8 (1.5%) patients at weeks 39, 41, 43, 45, and 46 of 2021. The Omicron variant was the most frequent with 289 (53.1%) patients during weeks 49 to 52 of 2021 and 1 to 22 of 2022. During weeks 1 through 22 of 2022, it was possible to discriminate between BA. 1 (n = 32) and BA.2 (n = 82).
Conclusion: The rapid identification of COVID-19 variants through the RT-PCR methodology contributes to timely epidemiological surveillance, as well as appropriate patient management.
Introduction
SARS-CoV-2 is an emerging virus that made its first appearance in the Chinese province of Wuhan in November 2019 (1). It is alarming that the World Health Organization (WHO) declared it a global pandemic (2). In Peru, on 5 March 2020, the first case of COVID-19 was reported. Today, more than 4 million cases of COVID-19 have been confirmed in Peru and approximately 219,587 deaths were registered (3).
SARS-CoV-2 has constantly changed, this caused the virus to acquire mutations in the spike protein gene (S-gene) giving new lineages of origin of SARS-CoV-2. These mutations have an impact on the properties of the virus, such as transmissibility, immune response, infectivity, and disease severity (4). WHO and the Center for Disease Control and Prevention (CDC) of the United States classified these variants as Variant of concern (VOC): Alpha, Beta, Gamma, Delta, and the currently circulating variant of concern Omicron and Variants of interest (VOI): Iota, Eta, Kappa, Epsilon, Lambda, and Zeta (5).
The SARS-CoV-2 lineages have been determined by whole genome sequencing (WGS). This test has been used since the start of the pandemic to gather essential information for public health. WGS requires high-complexity laboratories, highly qualified staff, expensive resources, and a long time for analysis (6). The implementation of real-time PCR in laboratories became a great alternative for monitoring circulating variants because it can be used as a rapid screening for epidemiological surveillance (7, 8). Additionally, real-time PCR has advantages such as the rapid process time, the affordable price, and the easy implementation in a molecular biology laboratory. In the present study, we describe the frequency of SARS-CoV-2 variants in the Auna healthcare network from Peru determined by real-time identification of the S-gene mutation.
Materials and methods
Samples and selection criteria
Genetic materials were obtained from nasopharyngeal swabs from September to December (39 to 52 epidemiological weeks) in 2021 and from January to May (1 to 22 epidemiological weeks) in 2022, which were previously tested for SARS-CoV-2 by reverse transcription PCR (RT-PCR) (9, 10). We stored remnant RNA at −80°C from positive samples with a cycle threshold (CT) value less than 30. All procedures were performed in the Molecular Biology area of the Auna Laboratory.
Real-time PCR for variant determination
The identification of the variants was performed with real-time PCR using a commercial kit. The Allplex™ SARS-CoV-2 Variants I Assay detects and identifies the HV69/70 deletion, E484K and N501Y mutations of the S gene and the Allplex™ SARS-CoV-2 Variants II Assay detects the mutations: L452R, W152C, K417T, and K417N. Together, this allows the identification of the VOC: Alpha, Beta, Gamma, Delta, and Omicron (11, 12). The differentiation between the lineages of Omicron BA.1 and BA.2 was determined using the Novaplex™ SARS-CoV-2 Variants VII Assay. This assay detects mutations: N501Y, E484A and HV69/70 deletion (13).
Whole genome sequencing
The national programme for genomic surveillance of the SARS-CoV-2 virus in Peru is directed by the National Institute of Health (NIH) with the objective of developing adequate genomic surveillance of the circulation of variants of SARS-CoV-2. As an authorised laboratory, we participated in the analytical surveillance programme, which allowed us to know the exact lineage of some samples with the methodology of whole genome sequencing. A total of 49 samples were derived from the INS Genomic Laboratory of the INS; these results were compared with those obtained using the real-time PCR methodology for VOC identification.
Statistical analysis
The data analysis of the multiplex real-time PCR was developed using the automated software Seegene viewer. This allows identification and differentiation for both the Ct value and multiple targets in a single channel. The information for this epidemiological study was collected from the laboratory software Enterprise. The data was analysed in R studio and presented in graphs and tables.
Results
The sampling was carried out in the Auna clinic network from September to December 2021 and from January to May 2022. During this time, around 31,375 samples were analysed, reaching 50% positivity during the third wave in Peru between December 2021 and February 2022 (Figure 1).
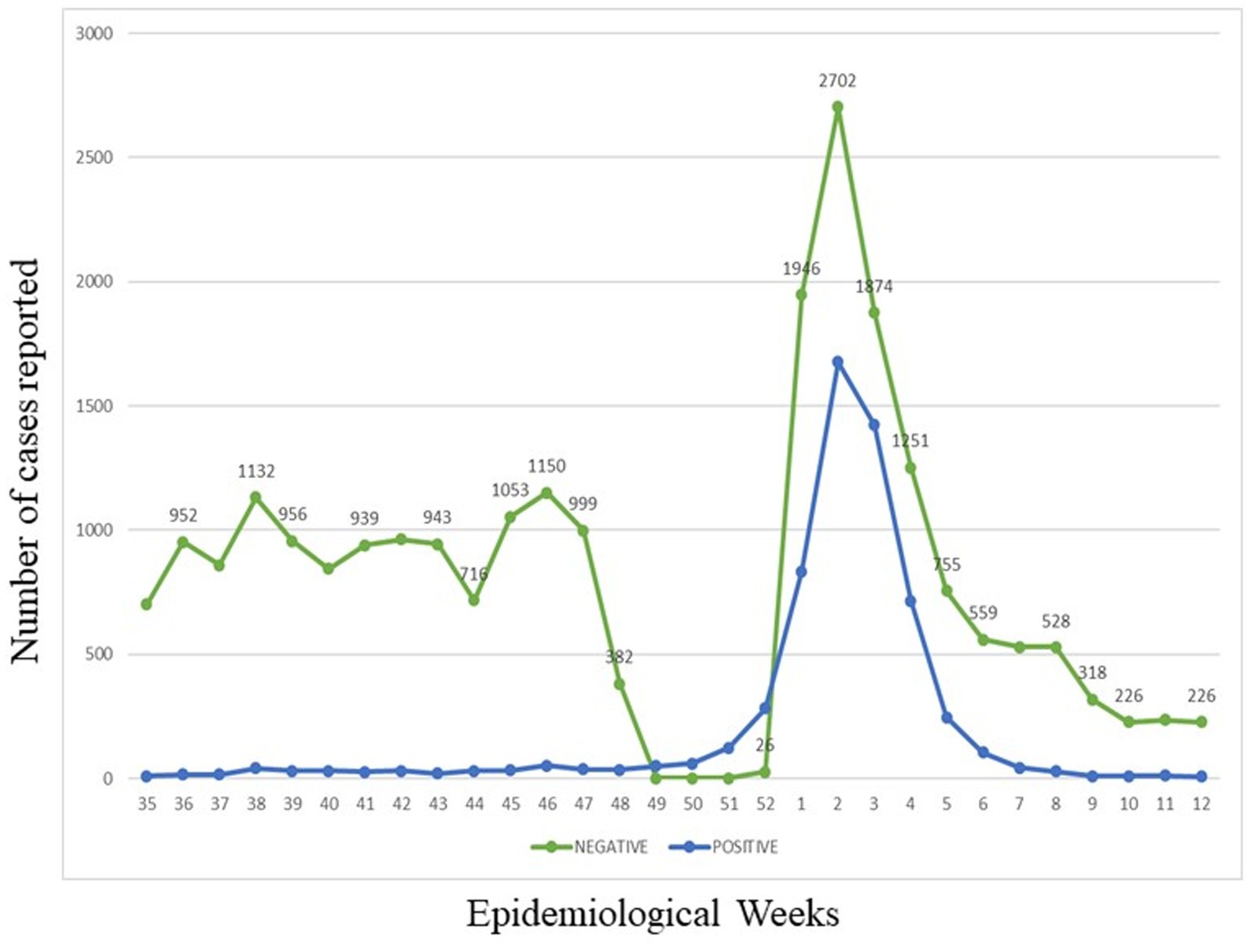
Figure 1. Evolution over the time of all samples processed from September to December 2021 and January to May 2022. The green line reports the COMD-19 negative cases. The blue line reports the COMD-19 positive cases.
A total of 544 samples with CT values less than 30 were selected, of which 432 ARN samples were tested with Allplex™ MC SARS-CoV-2 Variants I and II and 112 ARN samples were tested with Novaplex™ MC SARS-CoV-2 Variants VII (Tables 1, 2). As shown in Figure 2, the Delta variant was found during 39 to 52 weeks in 2021 with 242 (44.5%) positive samples. The Omicron variant was found in both years, 49 to 22 epidemiological weeks in 2021 and 1 to 22 epidemiological weeks in 2022. Overall, there were 289 samples with Omicron (53.1%). Gamma was the variant with the lowest frequency with 8 (1.5%) positive samples. Our data showed that in five samples, we were unable to identify the variant.
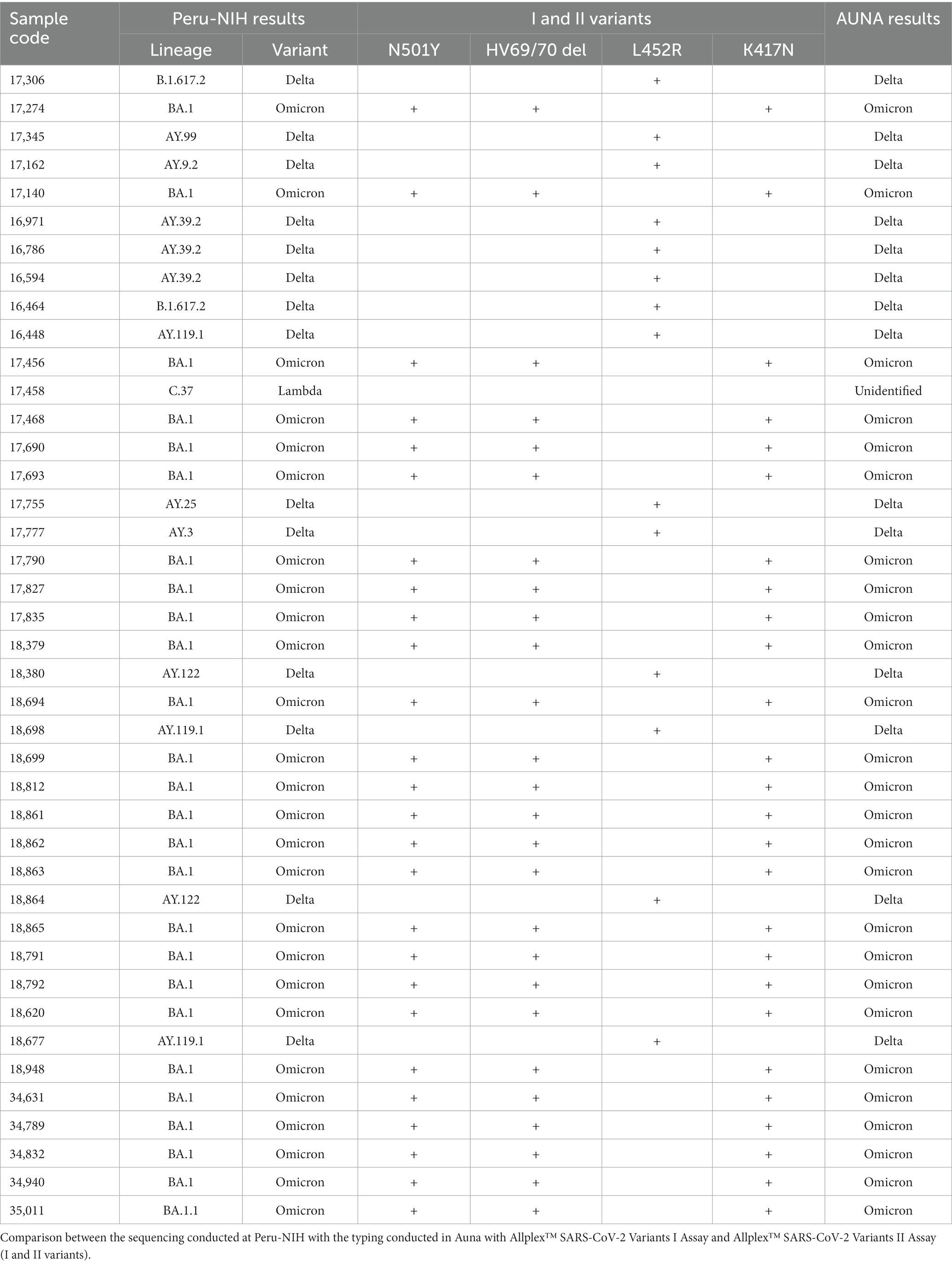
Table 1. Analysis of SARS-CoV-2 variants in samples obtained from AUNA patients.
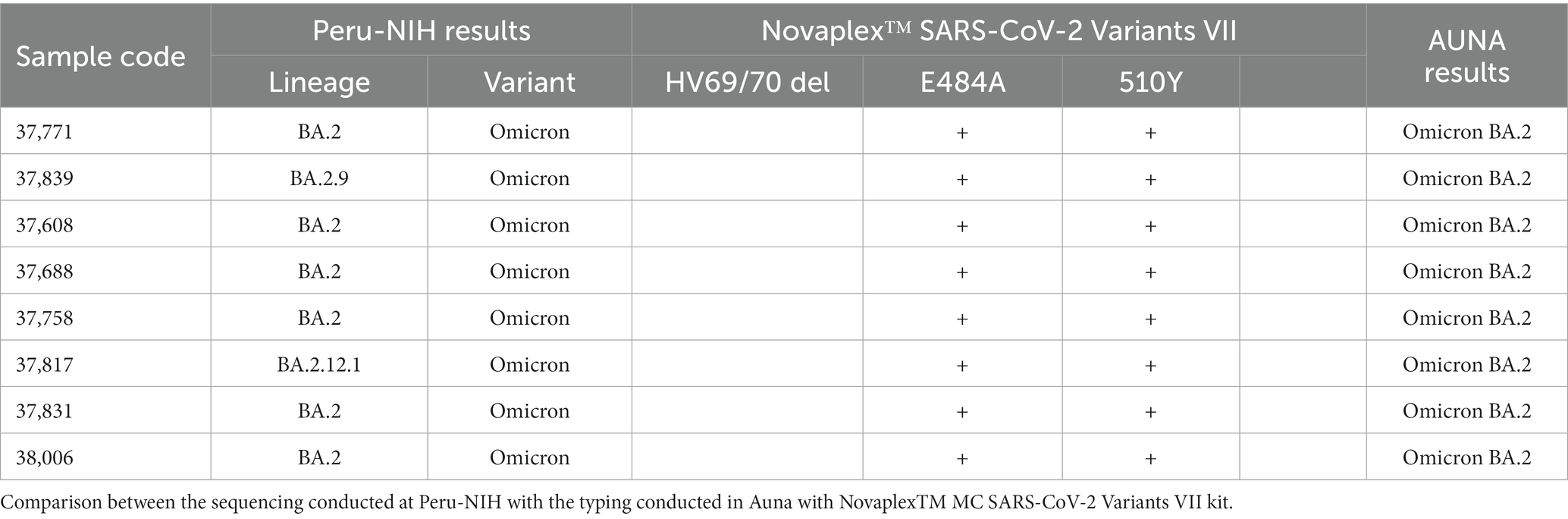
Table 2. Analysis of SARS-CoV-2 variants in samples obtained from AUNA patients.
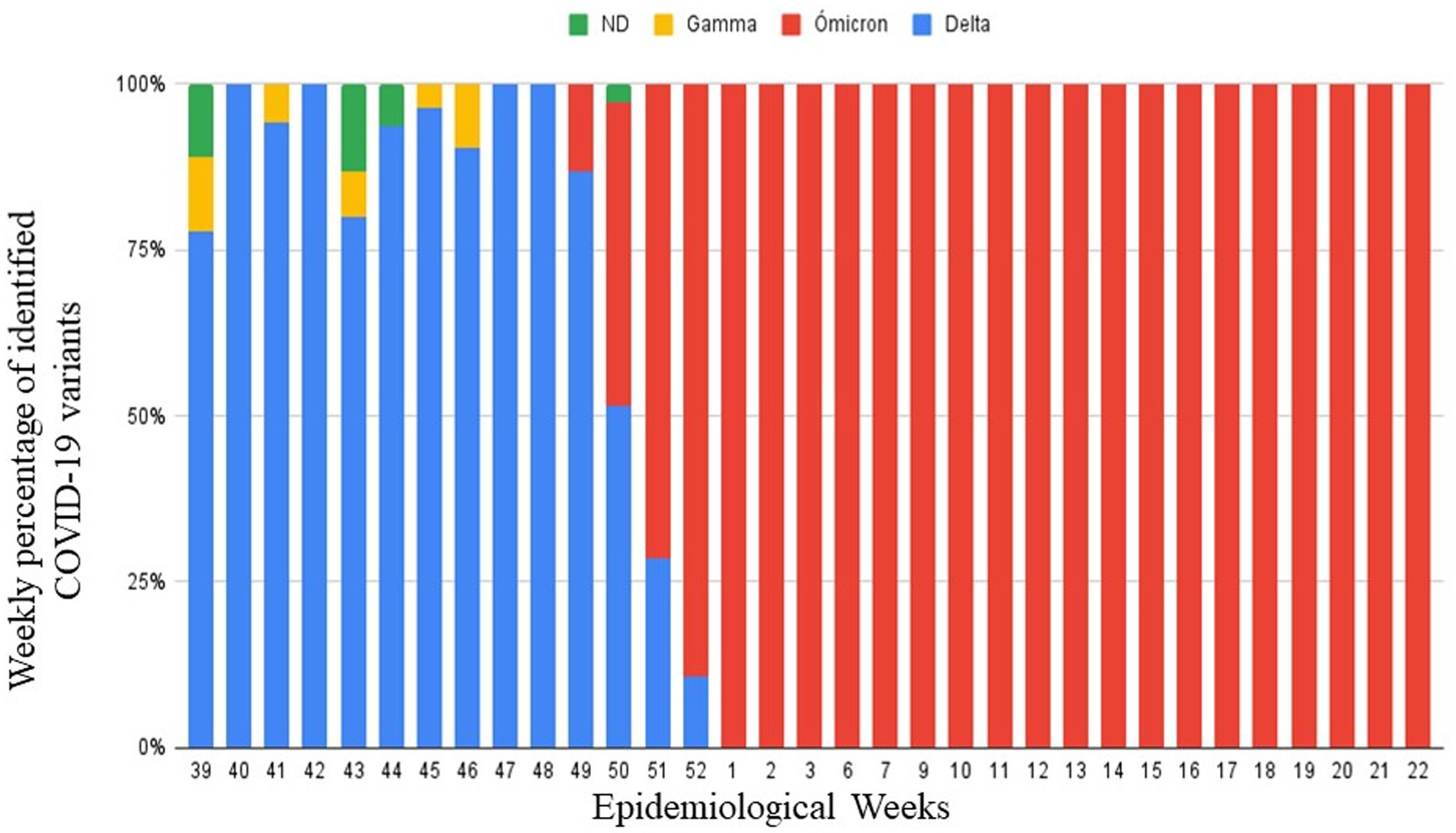
Figure 2. Identified variants by real-time PCR during epidemiological weeks 39–52 in 2021 and epidemiological weeks 1–22 in 2022.
The Omicron variant was identified between BA.1 and BA.2 at weeks 9 to 22 of 2022. BA.2 was the most frequent, with 80 (71.4%) samples identified. Unlike BA.1, with 32 (28.6%) positive samples. As shown in Figure 3, in the last weeks, BA.2 was the most frequent.
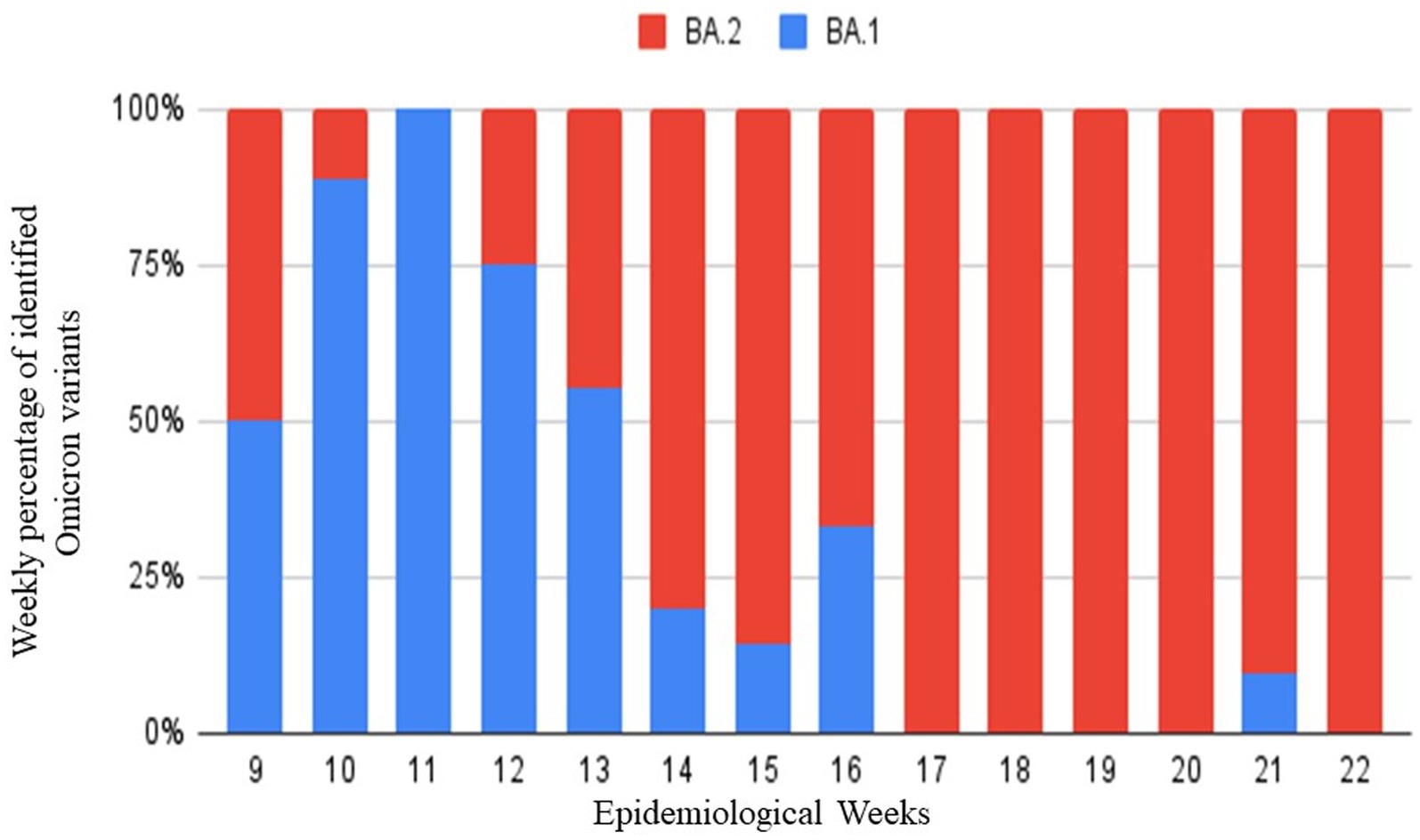
Figure 3. Identified Omicron variants during epidemiological weeks 9 to 22 of 2022 by real-time PCR with Novap1ex™ SARS-CoV-2 Variants VII Assay. In red BA.2 variant and in Blue BA.I variant.
As part of the COVID-19 surveillance in Peru, the National Institute of Health (NIH) requested samples from positive patients from laboratories that performed COVID-19 tests. Tables 1, 2 show the samples sent from 2021 to 2022 to the NIH. Only one sample could not be identified by real-time PCR used in the Auna laboratory. However, the NIH identified it as the Lambda variant by WGS. Furthermore, in the Supplementary Table S1, it can be seen that in all other samples Auna achieved the same diagnosis as the NIH.
Discussion
During the pandemic, COVID-19 developed different variants that caused worldwide concern. In Peru, the third wave of COVID-19 was declared in the 49 and 50 epidemiological weeks in 2021, increasing to more than 50% of positive cases (14, 15). In our study, Figure 1, we found an increasing number of positive cases of COVID-19 in December 2021 and January 2022, which were the months with the highest positive cases.
In Figure 2, we show the circulating variants in our area during the last trimester of 2021 and the first semester of 2022. The results obtained during 39 to 49 weeks were consistent with the end of the second wave in Peru, which had a predominance of delta variants. Also, it can be seen that from week 50 of 2021, Omicron began to appear in patients. However, from week 52 of 2021 to week 22 of 2022, Omicron shows a rapid progression that becomes predominant in all the cases. In Figure 3, from weeks 9 to 22 of 2022, Omicron began to be identified between its appearances BA.1 and BA.2 appearances, where it is evident that BA.2 had the highest prevalence. These changes are based on the local epidemiology of Peru and the recovered collected data for the INS that make Omicron responsible for the third wave (16, 17).
According to the NGS results shown in Table 1, using both Seegene Variants I and II assays allowed to identify VOC in all cases. However, these assays do not identify VOI as in the case of lambda (12, 17). Our study shows five cases with a nonidentified result; those cases are presumptive other variants different from VOC. This amount represents the 0.9% of samples analysed. In addition to that, with the emergence of Omicron subvariants, the Variants I and II assays do not discriminate between Omicron BA.1 and BA.2. The transition from BA.1 to BA.2 could be detected using the Variant VII Assay during weeks 9 to 22 of 2022.
Different assays were evaluated to identify VOC and VIC during the COVID-19 pandemic. The Allplex Seegene Variants kits showed concordance rates with WGS between 96.4 and 98.10% (18). Additionally, the Thermo Fisher TaqPath COVID-19 PCR assay achieved a 98.2% success rate in variant identification (19). The TaqPath methodology provides the advantage of identifying multiple mutations based on the current context, unrestricted to a specific kit. The high mutation rate of SARS-CoV-2 have led to the implementation of a surveillance programme in Peru to identify variants responsible for each wave. Gamma, Lambda and Delta variants principally detected during the second wave, and Omicron variant responsible for the third wave. Similar scenarios have been observed worldwide, but the timing and number of waves vary across regions (20–22). Peru has experienced diverse circulating variants, including native variants like Lambda, considered endemic to our territory (23, 24).
On the other hand, as the population immunity to SARS-CoV-2 increases, a variety of mutations have been identified that enhance replication fitness and have given rise to the VOCs. First, D614G spike protein mutation is in the C-terminal region of S1 domain related to S2. This mutation provokes a rapidly spread, higher transmissibility and more pathogenicity (25, 26). N501Y mutation enhances ACE2 proximity, it is on the RBD increasing the affinity to host cell receptor and increasing the transmission (Alpha variant) (27, 28). E484K mutation is involved in the initiation of the viral entry process and occurs at critical sites in the receptor binding motif of RBD. This mutation can escape from neutralization that affects the antibody-based measuring the monoclonal antibodies and vaccines (Beta variant) (28). On the other hand, NTD mutations has a deletion at 69–70 position that has shown a higher viral replication (29, 30). At the position 141–146 and 242–244, this deletion causes the neutralization of NTD antibodies. The reduction of the susceptibility to NTD neutralizing antibodies is produced by L18F, D253Y and other NTD mutilations, such the case of Gamma variant (29, 31). Non-spike mutations have been observed to enhance the transitivity of the virus host cells (32).
Aditionally, the multiple variants of SARS-CoV-2 that have surfaced recently have created uncertainty regarding the disease and its effects on vaccination programs. According to clinical trial evidence, vaccines currently available against the alpha variant (B.1.1.7) are highly effective (33–37). In the case of beta variants (B.1.351), some vaccines have shown reduced efficacy and effectiveness against symptomatic disease (38–41). Similarly, the effectiveness and efficacy of some vaccines have been reduced against delta variants (B.1.617.2) (42, 43). However, they have remained effective against severe disease and hospitalization (44–48). According to data on the effectiveness of vector-based vaccines against omicron variant (B.1.1.529), primary vaccine regimes fail to provide adequate protection (49). Likewise, primary mRNA vaccination regimens provide insufficient protection (50). However, it is important to highlight that vaccines remain effective against severe disease and hospitalization caused by the omicron variant, with initial data indicating 90% effectiveness against hospitalization from the United Kingdom (51, 52). Finally, it is noteworthy to mention that in the case of vaccine variants that do not have immune escape capability, a high-efficacy vaccine may only need a booster dose, whereas a lower-efficacy vaccine may need to be adapted. Thus, it is possible that all vaccines will require adaptation for variants with a significant immune escape ability, such as the Omicron variant. Equally, it is noteworthy to mention that artificial intelligence and big data have great potential for COVID-19 and other emergencies surveillance, and their roles are expected to expand over the next few years. Using AI and Big Data, public health interventions can be planned and organized based on the spread of the virus, their effectiveness monitored, old compounds can be repurposed and new drugs discovered, vaccine candidates can be identified, and communities and territories can be better prepared for the outbreak. Currently, a few studies have shown that AI-assisted methods distinguish accurately between different viral strains, aiding targeted interventions and surveillance (53–57). However, For AI-assisted methods to be effective in real world situations, more work should be done on strengthening the representativeness of data, improving predictive capabilities, and integrating AI-assisted methods into existing public health settings.
This study presents some limitations. First, the small number of samples collected during the selection of the third wave. Second, the high impact in the positive cases and the storage capacity of the laboratory complicated the recollection of ARN. However, the results obtained are based on local epidemiology during this time. Third, the kits Allplex™ SARS-CoV-2 Variants I and II assay were limited to the detection of Gamma, Beta, Delta, and Omicron that were considered VOCs (11, 12, 18). Since the SARS-CoV-2 virus is constantly mutational, these essays could quickly become out of date. For this reason, RT-PCR methods must be in permanent actualization (20). Finally, RT-PCR kits focus on a select group of mutations that identify a variant using an interpretative algorithm. Additional information like lineage, genomic diversity, and genotyping must be obtained by WGS (21).
In the present study, data from the official epidemiological surveillance issued by the NIH are correlated with national data obtained during the epidemiological weeks monitored. The data obtained during the study helped to observe the evolution of the mutations present in the second and third waves in our country. On the other hand, the kits used for RT-PCR identification have 98% reproducible genomic sequencing. Furthermore, the kits allowed us to identify variants of COVID-19 at a much lower cost and with much less equipment than the NGS method.
In conclusion, our data show the landscape of variant transitions in a private clinic where the omicron variant eventually replaced all circulating SARS-CoV-2 variants. In our experience, although with limited data, the determination of SARS-CoV-2 variants through RT-PCR assays was reliable and useful in routine.
Data availability statement
The datasets presented in this study can be found in the Figshare repository https://figshare.com/s/9e8295978679d692a711.
Ethics statement
The studies involving humans were approved by the IRB of the Universidad Privada San Juan Bautista (Approval: 0600-2023-CIEI-UPSJB), which waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because a database was used with patients’ personal information codified. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
TO-G: design of the study, laboratory analysis, data creation, writing draft, and review and editing. AG: formal analysis, data curation, writing draft, and review and editing. BC: design of the study, laboratory analysis, and review and editing. AZ: ethics committee approval procedures, writing draft, and review and editing. KO: laboratory analysis, data creation, and review and editing. DT: laboratory analysis, data creation, and review and editing. JP: design of the study, formal analysis, writing draft, and review and editing. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2023.1244662/full#supplementary-material
References
1. Huang, C, Wang, Y, Li, X, Ren, L, Zhao, J, Hu, Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
2. World Health Organization. WHO director-General's opening remarks at the media briefing on COVID-19. (2020). Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (Accessed May 9, 2023).
3. Ministry of Health, Peru. Sala COVID-19. (2023). Available at: https://www.dge.gob.pe/covid19.html (Accessed May 9, 2023).
4. Volz, E, Hill, V, McCrone, JT, Price, A, Jorgensen, D, O'Toole, Á, et al. Evaluating the effects of SARS-CoV-2 spike mutation D614G on transmissibility and pathogenicity. Cells. (2021) 184:64–75.e11. doi: 10.1016/j.cell.2020.11.020
5. Centers for Disease Control and Prevention. Clasificaciones y definiciones de las variantes del SARS-CoV-2. (2023). Available at: https://espanol.cdc.gov/coronavirus/2019-ncov/variants/variant-classifications.html (Accessed May 9, 2023).
6. Greninger, AL, Dien Bard, J, Colgrove, RC, Graf, EH, Hanson, KE, Hayden, MK, et al. Clinical and infection prevention applications of severe acute respiratory syndrome coronavirus 2 genotyping: an Infectious Diseases Society of America/American Society for Microbiology consensus review document. J Clin Microbiol. (2022) 60:e0165921. doi: 10.1128/JCM.01659-21
7. Neopane, P, Nypaver, J, Shrestha, R, and Beqaj, SS. SARS-CoV-2 variants detection using TaqMan SARS-CoV-2 mutation panel molecular genotyping assays. Infect Drug Resist. (2021) 14:4471–9. doi: 10.2147/IDR.S335583
8. Borillo, GA, Kagan, RM, and Marlowe, EM. Rapid and accurate identification of SARS-CoV-2 variants using real time PCR assays. Front Cell Infect Microbiol. (2022) 12:894613. doi: 10.3389/fcimb.2022.894613
9. Sule, WF, and Oluwayelu, DO. Real-time RT-PCR for COVID-19 diagnosis: challenges and prospects. Pan Afr Med J. (2020) 35:121. doi: 10.11604/pamj.supp.2020.35.24258
10. Rahbari, R, Moradi, N, and Abdi, M. rRT-PCR for SARS-CoV-2: analytical considerations. Clin Chim Acta. (2021) 516:1–7. doi: 10.1016/j.cca.2021.01.011
11. Fu, JYL, Chong, YM, Sam, IC, and Chan, YF. SARS-CoV-2 multiplex RT-PCR to detect variants of concern (VOCs) in Malaysia, between January to may 2021. J Virol Methods. (2022) 301:114462. doi: 10.1016/j.jviromet.2022.114462
12. Umunnakwe, CN, Makatini, ZN, Maphanga, M, Mdunyelwa, A, Mlambo, KM, Manyaka, P, et al. Evaluation of a commercial SARS-CoV-2 multiplex PCR genotyping assay for variant identification in resource-scarce settings. PLoS One. (2022) 17:e0269071. doi: 10.1371/journal.pone.0269071
13. Ministry of Health, Peru. Minsa confirma tercera ola ante incremento de casos de contagio por la COVID-19. (2022). Available at: https://www.gob.pe/institucion/minsa/noticias/574040-minsa-confirma-tercera-ola-ante-incremento-de-casos-de-contagio-por-la-covid-19 (Accessed April 27, 2023).
14. National Hospital Daniel Alcides Carrion. Tercera ola de la COVID-19 inició en el Perú. (2022). Available at: https://www.hndac.gob.pe/tercera-ola-de-la-covid-19-inicio-en-el-peru/#:~:text=Ante%20esto%2C%20el%20titular%20de,seguridad%20dentro%20de%20nuestro%20nosocomio (Accessed April 27, 2023).
15. Essalud. EsSalud: Conoce las variantes causantes del Covid-19 en Perú. Available at: http://noticias.essalud.gob.pe/?inno-noticia=essalud-conoce-las-variantes-causantes-del-covid-19-en-peru#:~:text=Actualmente%2C%20ómicron%20es%20la%20cepa,tercera%20ola%20de%20la%20pandemia (Accessed April 27, 2023).
16. Ministry of Health, Peru. Coronavirus: variantes de la COVID-19 detectadas en el Perú. (2023). Available at: https://www.gob.pe/12548-coronavirus-variantes-de-la-covid-19-detectadas-en-el-peru (Accessed May 9, 2023).
17. Seegene. Novaplex™ SARS-CoV-2 variants VII assay. (2023). Available at: https://www.seegene.de/assays/novaplex_sars-cov-2_variants_vii_assay (Accessed May 9, 2023).
18. Caza, M, Hogan, CA, Jassem, A, Prystajecky, N, Hadzic, A, and Wilmer, A. Evaluation of the clinical and analytical performance of the Seegene allplex™ SARS-CoV-2 variants I assay for the detection of variants of concern (VOC) and variants of interests (VOI). J Clin Virol. (2021) 144:104996. doi: 10.1016/j.jcv.2021.104996
19. Vogels, CBF, Breban, MI, Ott, IM, Alpert, T, Petrone, ME, Watkins, AE, et al. Multiplex qPCR discriminates variants of concern to enhance global surveillance of SARS-CoV-2. PLoS Biol. (2021) 19:e3001236. doi: 10.1371/journal.pbio.3001236
20. Padane, A, Diedhiou, CK, Gueye, K, Ndiour, S, Diagne, ND, Mboup, A, et al. Dynamics of variants of concern (VOC) of SARS-CoV-2 during the different waves of COVID-19 in Senegal. COVID. (2022) 2:691–702. doi: 10.3390/covid2060052
21. Liotti, FM, De Maio, F, Ippoliti, C, Santarelli, G, Monzo, FR, Sali, M, et al. Two-period study results from a large Italian hospital laboratory attesting SARS-CoV-2 variant PCR assay evolution. Microbiol Spectr. (2022) 10:e0292222. doi: 10.1128/spectrum.02922-22
22. Wei, Y, Guan, J, Ning, X, Li, Y, Wei, L, Shen, S, et al. Global COVID-19 pandemic waves: limited lessons learned worldwide over the past year. Engineering (Beijing). (2022) 13:91–8. doi: 10.1016/j.eng.2021.07.015
23. Justo Arevalo, S, Uribe Calampa, CS, Jimenez Silva, C, Quiñones Aguilar, M, Bouckaert, R, and Rebello Pinho, JR. Phylodynamic of SARS-CoV-2 during the second wave of COVID-19 in Peru. Nat Commun. (2023) 14:3557. doi: 10.1038/s41467-023-39216-8
24. Padilla-Rojas, C, Jimenez-Vasquez, V, Hurtado, V, Mestanza, O, Molina, IS, Barcena, L, et al. Genomic analysis reveals a rapid spread and predominance of lambda (C.37) SARS-COV-2 lineage in Peru despite circulation of variants of concern. J Med Virol. (2021) 93:6845–9. doi: 10.1002/jmv.27261
25. Becerra-Flores, M, and Cardozo, T. SARSCoV-2 viral spike G614 mutation exhibits higher case fatality rate. Int J Clin Pract. (2020) 74:e13525. doi: 10.1111/ijcp.13525
26. Korber, B, Fischer, WM, Gnanakaran, S, Yoon, H, Theiler, J, Abfalterer, W, et al. Tracking changes in SARS-CoV-2 spike: evidence that D614G increases infectivity of the COVID-19 virus. Cells. (2020) 182:812–827.e19. doi: 10.1016/j.cell.2020.06.043
27. Zhu, X, Mannar, D, Srivastava, SS, Berezuk, AM, Demers, JP, Saville, JW, et al. Cryo-electron microscopy structures of the N501Y SARS-CoV-2 spike protein in complex with ACE2 and 2 potent neutralizing antibodies. PLoS Biol. (2021) 19:e3001237. doi: 10.1371/journal.pbio.3001237
28. Tegally, H, Wilkinson, E, Giovanetti, M, Iranzadeh, A, Fonseca, V, Giandhari, J, et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature. (2021) 592:438–43. doi: 10.1038/s41586-021-03402-9
29. Tao, K, Tzou, PL, Nouhin, J, Gupta, RK, de Oliveira, T, Kosakovsky Pond, SL, et al. The biological and clinical significance of emerging SARS-CoV-2 variants. Nat Rev Genet. (2021) 22:757–73. doi: 10.1038/s41576-021-00408-x
30. Choi, B, Choudhary, MC, Regan, J, Sparks, JA, Padera, RF, Qiu, X, et al. Persistence and evolution of SARS-CoV-2 in an immunocompromised host. N Engl J Med. (2020) 383:2291–3. doi: 10.1056/NEJMc2031364
31. Gangavarapu, K, Latiff, AA, Mullen, JL, Alkuzweny, M, Hufbauer, E, Tsueng, G, et al. Outbreak. Info genomic reports: scalable and dynamic surveillance of SARS-CoV-2 variants and mutations. Nat Methods. (2023) 20:512–522. doi: 10.1101/2022.01.27.22269965
32. Hodcroft, EB, Domman, DB, Snyder, DJ, Oguntuyo, KY, van Diest, M, Densmore, KH, et al. Emergence in late 2020 of multiple lineages of SARS-CoV-2 spike protein variants affecting amino acid position 677. medRxiv. (2021). doi: 10.1101/2021.02.12.21251658
33. Emary, KRW, Golubchik, T, Aley, PK, Ariani, CV, Angus, B, Bibi, S, et al. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): an exploratory analysis of a randomised controlled trial. Lancet. (2021) 397:1351–62. doi: 10.1016/S0140-6736(21)00628-0
34. Heath, PT, Galiza, EP, Baxter, DN, Boffito, M, Browne, D, Burns, F, et al. Safety and efficacy of NVX-CoV2373 Covid-19 vaccine. N Engl J Med. (2021) 385:1172–83. doi: 10.1056/NEJMoa2107659
35. Dagan, N, Barda, N, Kepten, E, Miron, O, Perchik, S, Katz, MA, et al. BNT162b2 mRNA Covid-19 vaccine in a nationwide mass vaccination setting. N Engl J Med. (2021) 384:1412–23. doi: 10.1056/NEJMoa2101765
36. Katz, MA, Harlev, EB, Chazan, B, Chowers, M, Greenberg, D, Peretz, A, et al. Early effectiveness of BNT162b2 Covid-19 vaccine in preventing SARS-CoV-2 infection in healthcare personnel in six Israeli hospitals (CoVEHPI). Vaccine. (2022) 40:512–20. doi: 10.1016/j.vaccine.2021.11.092
37. Nasreen, S, Chung, H, He, S, Brown, KA, Gubbay, JB, Buchan, SA, et al. Effectiveness of COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario. Nat Microbiol. (2022) 7:379–85. doi: 10.1038/s41564-021-01053-0
38. Madhi, SA, Baillie, V, Cutland, CL, Voysey, M, Koen, AL, Fairlie, L, et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. (2021) 384:1885–98. doi: 10.1056/NEJMoa2102214
39. Shinde, V, Bhikha, S, Hoosain, Z, Archary, M, Bhorat, Q, Fairlie, L, et al. Efficacy of NVX-CoV2373 Covid-19 vaccine against the B.1.351 variant. N Engl J Med. (2021) 384:1899–909. doi: 10.1056/NEJMoa2103055
40. Johnson & Johnson. (2021). Johnson & Johnson announces single-shot Janssen COVID-19 vaccine candidate met primary endpoints in interim analysis of its phase 3 ENSEMBLE trial. Available at: https://www.jnj.com/johnson-and-johnson-announces-single-shot-janssen-covid-19-vaccine-candidate-met-primary-endpoints-in-interim-analysis-of-its-phase-3-ensemble-trial (Accessed September 23, 2023).
41. Abu-Raddad, LJ, Chemaitelly, H, and Butt, AA. National Study Group for Covid-vaccination. Effectiveness of the BNT162b2 Covid-19 vaccine against the B.1.1.7 and B.1.351 variants. N Engl J Med. (2021) 385:187–9. doi: 10.1056/NEJMc2104974
42. Israel Ministry of Health. (2021). Decline in vaccine effectiveness against infection and symptomatic illness. Available at: https://www.gov.il/en/departments/news/05072021-03 (Accessed September 20, 2023.
43. Tartof, SY, Slezak, JM, Heidi, F, Hong, V, Ackerson, BK, Ranasinghe, ON, et al. Six-month effectiveness of BNT162b2 mRNA COVID-19 vaccine in a large US integrated health system: a retrospective cohort study. Lancet. (2021) 398:1407–16. doi: 10.1016/S0140-6736(21)02183-8
44. Pfizer, BioNTech. (2021). Pfizer and BioNTech announce phase 3 trial data showing high efficacy of a booster dose of their COVID-19 vaccine. Available at: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-phase-3-trial-data-showing (Accessed September 18, 2023).
45. Sheikh, A, McMenamin, J, Taylor, B, and Robertson, CPublic Health Scotland and the EAVE II Collaborators. SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness. Lancet. (2021) 397:2461–2. doi: 10.1016/S0140-6736(21)01358-1
46. Lopez Bernal, J, Andrews, N, Gower, C, Gallagher, E, Simmons, R, Thelwall, S, et al. Effectiveness of Covid-19 vaccines against the B.1.617.2 (Delta) Variant. N Engl J Med. (2021) 385:585–94. doi: 10.1056/NEJMoa2108891
47. Pouwels, KB, Pritchard, E, Matthews, PC, Stoesser, N, Eyre, DW, Vihta, K-D, et al. Effect of Delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. Nat Med. (2021) 27:2127–35. doi: 10.1038/s41591-021-01548-7
48. Grannis, SJ, Rowley, EA, Ong, TC, Stenehjem, E, Klein, NP, DeSilva, MB, et al. Interim estimates of COVID-19 vaccine effectiveness against COVID-19-associated emergency department or urgent care clinic encounters and hospitalizations among adults during SARS-CoV-2 B.1.617.2 (Delta) variant predominance – nine states, June-august 2021. MMWR Morb Mortal Wkly Rep. (2021) 70:1291–3. doi: 10.15585/mmwr.mm7037e2
49. Andrews, N, Stowe, J, Kirsebom, F, Toffa, S, Rickeard, T, Gallagher, E, et al. Effectiveness of COVID-19 vaccines against the omicron (B.1.1.529) variant of concern. N Engl J Med. (2022) 386:1532–46. doi: 10.1056/NEJMoa2119451
50. Gram, MA, Emborg, H-D, Schelde, AB, Friis, NU, Nielsen, KF, Moustsen-Helms, IR, et al. Vaccine effectiveness against SARS-CoV-2 infection or COVID-19 hospitalization with the Alpha, Delta, or Omicron SARS-CoV-2 variant: A nationwide Danish cohort study. PLoS Med. (2022) 19:e1003992. doi: 10.1371/journal.pmed.1003992
51. UK Health Security Agency. (2021). Effectiveness of 3 doses of COVID-19 vaccines against symptomatic COVID-19 and hospitalization in adults aged 65 years and older. UK: Department of Public Health.
52. Public Health England. (2021). SARS-CoV-2 variants of concern and variants under investigation in England: technical briefing: update on hospitalization and vaccine effectiveness for omicron VOC-21NOV-01 (B.1.1.529). UK: Department of Public Health.
53. Promja, S, Puenpa, J, Achakulvisut, T, Poovorawan, Y, Lee, SY, Athamanolap, P, et al. Machine learning-assisted real-time polymerase chain reaction and high-resolution melt analysis for SARS-CoV-2 variant identification. Anal Chem. (2023) 95:2102–9. doi: 10.1021/acs.analchem.2c05112
54. Beguir, K, Skwark, MJ, Fu, Y, Pierrot, T, Carranza, NL, Laterre, A, et al. Early computational detection of potential high-risk SARS-CoV-2 variants. Comput Biol Med. (2023) 155:106618. doi: 10.1016/j.compbiomed.2023.106618
55. Togrul, M, and Arslan, H. Detection of SARS-CoV-2 Main Variants of Concerns using Deep Learning 2022. Innovations in intelligent systems and applications conference (ASYU), Antalya, Turkey, 2022, pp. 1–5.
56. Perez-Romero, CA, Mendoza-Maldonado, L, Tonda, A, Coz, E, Tabeling, P, Vanhomwegen, J, et al. An innovative AI-based primer design tool for precise and accurate detection of SARS-CoV-2 variants of concern. Sci Rep. (2023) 13:15782. doi: 10.1038/s41598-023-42348-y
Keywords: SARS-CoV-2 variants, surveillance & forecast system, epidemiological monitoring, RT-PCR method, COVID-19
Citation: Ortiz-Gómez T, Gomez AC, Chuima B, Zevallos A, Ocampo K, Torres D and Pinto JA (2024) Frequency of SARS-CoV-2 variants identified by real-time PCR in the AUNA healthcare network, Peru. Front. Public Health. 11:1244662. doi: 10.3389/fpubh.2023.1244662
Edited by:
Zhimin Tao, Jiangsu University, ChinaReviewed by:
Marianna Scrima, BioGeM Institute, ItalyHong Peng, Sun Yat-sen University, Shenzhen Campus, China
Copyright © 2024 Ortiz-Gómez, Gomez, Chuima, Zevallos, Ocampo, Torres and Pinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph A. Pinto, am9zZXBoLnBpbnRvQGF1bmEtaWRlYXMub3Jn