 JunCheng Zhao
JunCheng Zhao Xiaoyin Wang
Xiaoyin Wang Shiliang Xu2
Shiliang Xu2 Ming Hao
Ming Hao- 1School of Public Health and Health Management, Gannan Medical University, Ganzhou, China
- 2College of Electronics and Information Engineering, Liaoning Institute of Science and Technology, Benxi, Liaoning, China
Background: Depression rates among adolescents have risen dramatically over the past decade. Therefore, preventing depression among adolescents is particularly important. Differences in lifestyle habits may play a role in depression.
Purpose: This study aimed to explore the influence of living habits on depression levels among rural middle school students in Northeast China and to provide a theoretical basis for developing interventions to reduce depression levels in middle school students.
Methods: A total of 296 middle school students aged 13–15 years from Benxi City, Northeast China completed the anthropometric measurements, Physical Activity Scale-3 (PARS-3), and the Self-Rating Depression Scale (SDS). Their average screen time in the most recent week, parents' education level, and monthly family income were collected through a questionnaire.
Results: Females had higher depression scores than males (41.0 ± 6.9 vs. 37.9 ± 8.0). Physical activity (β = −0.38, t = −7.06, P < 0.01), family income (β = −0.20, t = −4.07, P < 0.01), screen time (β = 0.16, t = 3.34, P < 0.01), age (β = 0.15, t = 3.16, P < 0.01), sex (β = −0.13, t = −2.74, P < 0.01), and sleep quality (β = −0.08, t = −1.87, P < 0.01) are important factors related to depression levels.
Conclusion: The preliminary analysis results showed that among middle school students in rural Northeast China, the depression level of females was significantly higher than that of males. Poor quality sleep, low levels of physical activity, low household income, and long screen time were positively associated with depression. Therefore, strengthening physical activity, improving sleep quality, and reducing screen time are of clinical relevance in preventing and reducing depression.
1 Introduction
Currently, depression is the most common mental disorder worldwide (1). Between 1990 and 2018, there were 322 million cases of depression reported globally (2). It is estimated that depression will become the most burdensome disease worldwide by 2030 (3). A meta-analysis of 72 studies on the global prevalence of depression among adolescents showed that between 2010 and 2020, the prevalence of depressive symptoms among teenagers rose from 24 to 37% (4). Mental health problems are equally serious among Chinese adolescents. According to the results of China's 2022 National Depression Blue Book, children under the age of 18 years in China account for ~30.28% of the total number of people suffering from mental health problems, such as various emotional and behavioral disorders, and ~5.2% have obvious mental health problems. Depression is one of the most prevalent mental health disorders and can lead to anxiety, sleep disturbance, and other adverse outcomes. Patients with major depressive disorders may exhibit suicidal behaviors (5). Therefore, it is important to improve the depression conditions in adolescents, particularly as this is a period of rapid social, emotional, and cognitive development, as well as critical life transitions.
However, its pathogenesis remains unclear. For mild to moderate depression, there is no reliable evidence that any single treatment method has a prominent effect on improving depressive symptoms (6). Nevertheless, lifestyle habits play a crucial role in the emergence of depression (7, 8), and the importance of self-care behavior in preventing depression needs to be emphasized (9). Maintaining appropriate exercise and sufficient sleep are considered beneficial for improving and preventing depression.
Physical exercise has a positive impact on the prevention and treatment of depression (10). An exercise intervention study of 433 adolescents with depression showed that moderate- to high-intensity exercise had a significant therapeutic effect on adolescent depression and was significantly better than low-intensity exercise, in addition to the moderate and sustained positive effects of the exercise intervention on adolescent depression (11).
Sleep disturbance is also considered an important cause of depression in adolescents. Three quarters (76.5%) of the 28,135 teenagers did not get the necessary 8 h of sleep on a typical school night (12). The results of a cross-sectional study of the relationship between sleep duration and depression in rural areas of Northeast China showed that sleep duration was strongly associated with depression in a rural population in Liaoning Province. Inadequate sleep duration is a risk factor for depression. Therefore, optimizing sleep status may contribute to physical and mental health (13). Increasing use of electronic devices among students has been cited as a significant contributor to sleep disturbances and reduced average sleep duration. A study on the relationship between mobile phone addiction and the incidence of low and short sleep among 1,125 adolescent students in South Korea showed that the frequent use of mobile phones is a risk factor for sleep disorders in adolescents (14). Another study on the relationship between cell phone use and depressive symptoms, body aches and daytime sleepiness among secondary school students in Hong Kong showed that cell phone use was associated with a wide range of health problems, such as depression, sleep disorders, etc., and that secondary school students who had a higher demand for cell phones scored significantly higher in terms of depression severity and daytime sleepiness (15).
A study on the development and changes in depression during adolescence showed that middle and late adolescence (15–18 years old) is a critical period for susceptibility to depression because the incidence of depression is higher during this period (16). In a study of the impact of schooling on depressive symptoms in Chinese adolescents before the COVID-19 outbreak, it was found that the negative impact of schooling on the mental health of Chinese adolescents was even greater than that of the epidemic and home isolation, and that secondary school students were subjected to unprecedentedly high levels of pressure to advance to higher levels of schooling, which may have had a greater impact on the incidence of depression among secondary school students (17). In addition, in a study of 1,314 schoolchildren on the impact of poverty mediated by family social capital on children's anxiety and depression, it was shown that poverty had a significant direct impact on children's anxiety and depression (18).
This study aimed to investigate the status quo of depression levels of middle school students in rural areas of Northeast China, analyze the factors influencing their depression levels, explore the effects of lifestyle habits (physical activity, screen time, and sleep quality) on depression levels, and give a theoretical foundation for developing interventions to reduce the depression levels in middle school students.
2 Materials and methods
2.1 Participants
We have chosen the Rural Department of Mingshan District, Benxi City, Liaoning Province as the survey area. There are three middle schools in the local area, two of which have a total of <80 students and are no longer continuing to recruit new students. We selected the remaining middle school, which had the largest number of students among the three rural middle schools in the district. Schools in this area were suspended for ~1 month because of the COVID-19 pandemic in early 2020. No cluster epidemics occurred before September 2021, and the students attended classes normally. We held parent teacher meetings and required parents and children to sign informed consent forms and fill out survey questionnaires on site. In total, 318 students agreed to participate in the questionnaire survey, while parents provided guidance. Of the participants, 296 students (male: 158; female: 138) provided complete and valid data to be included in this study.
2.2 Physical activity score
The physical activity levels of rural children were investigated using the Physical Activity Scale-3 (PARS-3) (19). The scale consists of three questions examining the intensity, duration, and frequency of exercise. A five-level scoring method of 1–5 points was used for evaluation. The exercise intensity, time, and frequency were multiplied to determine the amount of exercise. Exercise volume ranged from 0 to 100 points, with higher scores indicating greater levels of exercise. Categories were defined as: light exercise: 0–19 points; moderate exercise: 20–42 points; and strenuous exercise: 43–100 points (19).
2.3 Screen time
Through a questionnaire, the students were asked to record their average screen time usage (min/day) in the most recent week. To estimate screen time, they were asked to separately report the time spent watching TV, using a computer, and playing video games.
2.4 Sleep quality score
We use the Pittsburgh Sleep Quality Index (PSQI) to evaluate the sleep status of students. The PSQI was compiled by Dr. Buysse, a psychiatrist at the University of Pittsburgh, in 1989 (20). This scale consists of seven components (sleep latency, duration, and disturbance, daytime dysfunction, habitual sleep efficiency, sleep medication, and overall sleep quality) and a total of 19 questions. The sum of the scores for the seven components is the PSQI score, and the higher the score, the worse the sleep quality (20).
2.5 Depression score
Depressive symptoms were assessed using the Self-Rating Depression Scale (SDS) (21), which is a self-reported measure of depression consisting of 20 items covering the emotional, psychological, and physical characteristics of depression. Each item is ranked from 1 to 4, with higher scores indicating greater levels of depressive symptoms, resulting in a total score of between 20 and 80. All participants were then divided into two groups: (1) a non-depressive symptom group (SDS < 40) and (2) a depressive symptom group (SDS ≥40) (21). Value cuts were established based on the SDS. The SDS has been developed and proven to be quantitatively suitable for the subjective perception of depression with good validity and reliability in China, with a Cronbach's alpha coefficient and a test-retest reliability of 0.862 and 0.820, respectively.
2.6 Parents' educational background and family monthly income
Parents' educational background and family monthly income were also surveyed through a questionnaire.
2.7 Statistical methods
A Chi square test was used to determine gender differences in the SDS. We used an independent sample t-test to verify physical activity score, sleep quality score, and gender differences in screen time. Multiple regression analysis was performed with the depression score as the dependent variable, with gender, age, family income, education level of parents, physical activity score, sleep quality score, and screen time as predictor variables. Variables were selected according to the stepwise increase and decrease method, and we used the likelihood ratio test method to calculate and set the threshold P-value as 0.20. P < 0.05 was considered statistically significant. We used JMP 20.0J for all statistical analyses and processing (SAS Institute Inc., Cary, NC).
2.8 Sample size estimation
The sample size for the study was determined using the G*Power calculator 3.1.9.7 (Franz Faul et al., Universität Kiel, Germany, http://www.gpower.hhu.de/). Considering an α = 0.05, 1-β = 0.90, the number of tested predictors = 3 (physical activity score, screen time, and sleep quality score), the number of covariates = 3 (family income, age, and sex), we calculated the sample size to be 33, 73, and 528, respectively if the effect size f2 equaled to 0.35 (large), 0.15 (medium) and 0.02 (small). Furtherly, a 20% dropout rate was assumed, and the total number was estimated as 42–660. The actual valid sample size was 298, which was much larger than the estimated size as large effect size f2.
2.9 Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All study participants provided informed consent, agreeing to the required measurement and survey completion procedures. This study was approved by the ethics committee of the Gannan Medical University, China, No: 2021110.
3 Results
The characteristics of the study participants are listed in Table 1. The participants' average age was 12.0 years. Their parents' education level was mostly high school and family income was mostly 3,001–5,000 yuan.
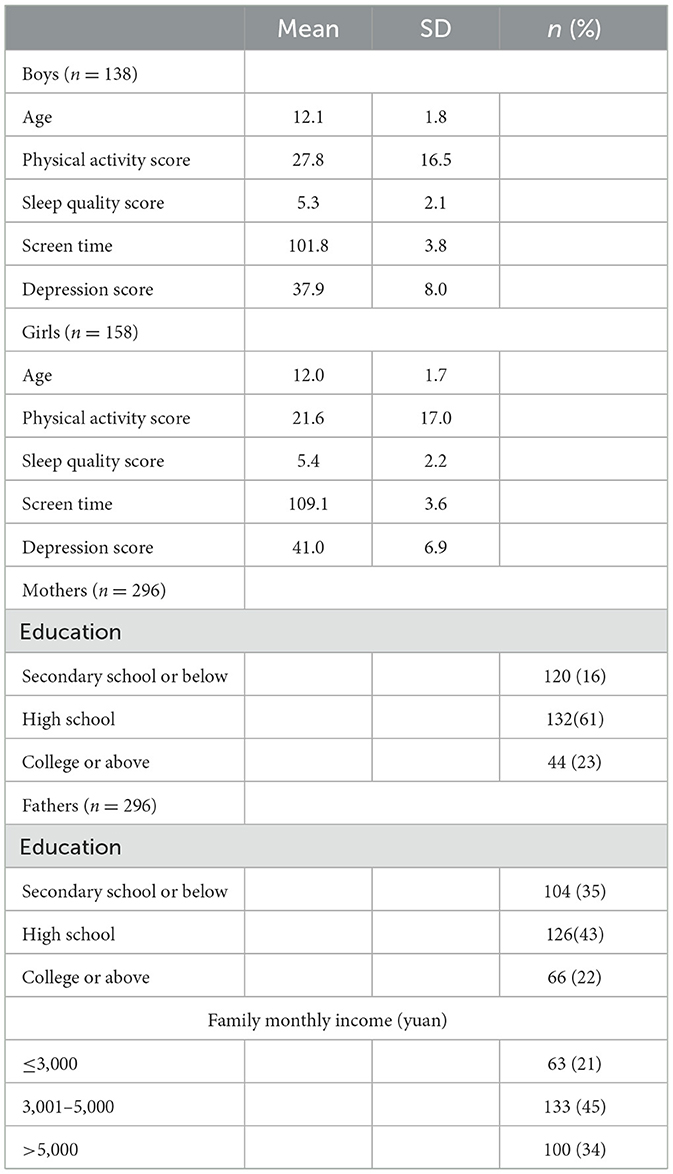
Table 1. Characteristics of the study subjects.
Table 2 shows the gender differences in lifestyle. Gender differences were found in exercise scores, but not in sleep time and screen time. In addition, we found that the proportion of females in the depression group is higher (Figure 1).
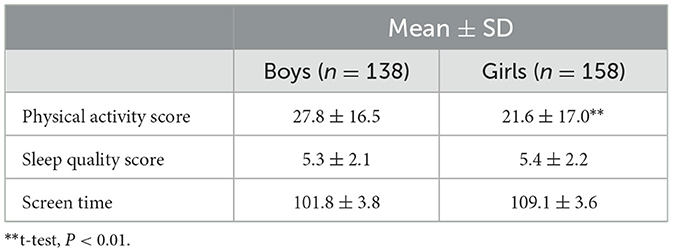
Table 2. Gender differences in lifestyle.
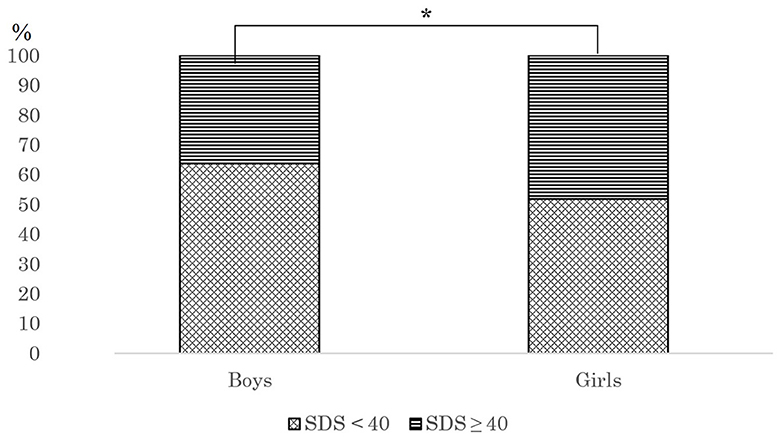
Figure 1. The percentage of boy and girls with SDS scores ≥40. *Chi square test, P < 0.05.
Table 3 shows the results of the multiple regression analysis of the factors affecting the SDS scores. The higher the R-squared score, the better the representativeness of the model. R-squared for the model in this study was 0.39, P < 0.01. The model in this study has a certain representativeness. According to the multiple linear regression equation standardized coefficient β, the intensity of the impact on SDS scores varies from high to low, as follows: physical activity (β = −0.38, t = −7.06, P < 0.01), family income (β = −0.20, t = −4.07, P < 0.01), screen time (β = 0.16, t = 3.34, P < 0.01), age (β = 0.15, t = 3.16, P < 0.01), sex (boy: 1; girl: 0; β = −0.13, t = −2.74, P < 0.01), and sleep quality (β = −0.08, t = −1.87, P < 0.01), and these were significant predictors of the SDS scores.
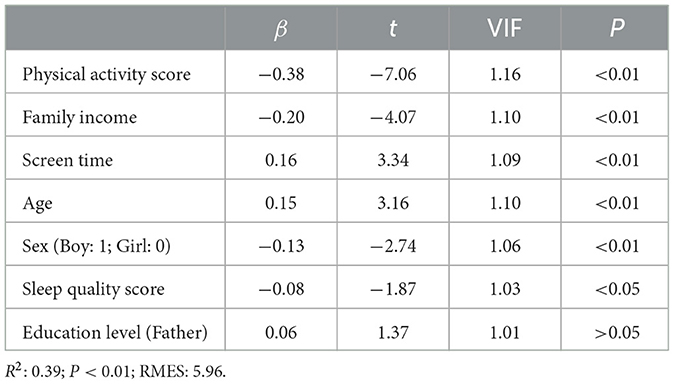
Table 3. Factors that contributed to depression level of children (n = 296).
4 Discussion
The depression levels of middle school students were similar to those of college students. A study on college students in southern China showed that the average SDS scores of male and female college students were 44.9 and 46.8, respectively (22). College students need to adapt to the increased independence and academic pressure of college life, making them prone to depression and other mental health problems (23). In China, college students have more free time to use the Internet compared to middle school students, and thus are at a higher risk of being exposed to cyberbullying behavior which can lead to depression (24). In addition, several studies have shown that impending adulthood is a period of emotional complexity during which one develops career and social orientations, enters into adult relationships, and faces potentially high levels of stress due to familial, financial, and professional obligations (25, 26) as well as frequently experiencing emotional turmoil (27). Indeed, the college years coincide with this period, thus leading to a potentially higher prevalence of depression. The findings of this study revealed that male and female middle school pupils had depression levels of 37.9 and 41.0, respectively, which is close to that of college students. However, compared to college students, middle school students have lower mental maturity and a higher possibility of extreme behavior. Studies have shown that depression may affect 2%−8% of children and adolescents; ~40% of affected children will have recurrent episodes, one-third of affected children will attempt suicide, and 3%−4% of children will die of suicide (28). It is particularly important to improve the current high depression levels among middle school students as soon as possible.
Girls had higher levels of depression than boys (Figure 1). A survey on the prevalence of depressed mood in ~12,000 Norwegian adolescents showed that girls had higher levels of depression than boys, and this difference persisted throughout adolescence (29). A screening of depressive symptoms among 4,100 adolescents in Wuhan, China, showed that the prevalence of high depressive symptoms in girls and boys was 38.9 and 30.2%, respectively, with prevalence higher for girls than boys (30). In addition, the results of a new descriptive analysis on the depression status of adolescents in Huangshi City, China, show that the prevalence of depression has been on the rise since 2018, especially in 2021, and the prevalence is higher among females than males (31). Another study on the relationship between non-educational electronic screen time and depressive symptoms among 27,070 seventh-grade middle school students in China showed that girls had a higher prevalence of depression than boys (27.6 vs. 17.7%) (32). This study supports the findings of a previous study (Figure 1). Previous studies have emphasized that physiological and psychological differences between boys and girls are important reasons for the difference in depression levels. According to epidemiological research, women are more likely than men to experience mental illnesses including anxiety and post-traumatic stress disorder, which may be associated with variations in gonadal hormone levels during stressful situations and differences in gender-specific brain regions (33). At the same time, compared with boys, girls are more susceptible to tension, more emotional, and more likely to have negative emotions, resulting in higher levels of depression (34). In addition, boys are often allowed to have more social and outdoor time, while girls are often restricted from going out and socializing (35, 36). This may further exacerbate gender differences in depression levels.
The results of this study emphasize that exercise level may be an important reason for the emergence of gender differences in depression levels among middle school students. Compared with girls, boys scored higher at the sports level (Table 2). Research has shown that physical activity can help prevent the onset and relapse of mild to moderate depression (37). In another study of the relationship between physical activity and mental disorders in U.S. adults, researchers used data from the National Comorbidity Survey (n = 8,089) to compare the prevalence of mental disorders among those who participated in regular physical activity and those who did not. Using multivariate logistic regression analysis, the study showed that physical activity was associated with lower levels of depression, and those who were physically active had lower levels of depression than those who did not participate in a daily exercise program (38). This study supports the findings of previous studies, confirming that higher physical activity scores are associated with lower levels of depression among middle school students in rural Northeast China (Table 3). Regular recreational exercise of any intensity could prevent future depression, according to a study of 33,908 adults in the Exercise and Depression Prevention Study (39). Therefore, it is important to reduce depression levels in middle school students, especially girls, by increasing the physical activity level of young people.
The sleep quality scores of males and females in this area were 5.3 ± 2.1 and 5.4 ± 2.2. A PSQI score >5 indicates poor sleep quality in middle school students. Sleep quality has a significant impact on mental health. Studies have shown that mental illnesses such as depression are often associated with the development of sleep problems (40). The findings of this study demonstrated a relationship between poorer sleep quality and higher levels of depression, supporting the findings of previous studies (Table 3). Studies have shown that sleep disturbance is a stand-alone risk factor for teen suicide and substance use; it is connected to depression and other psychiatric illnesses and increases the risk of suicidal behavior in depressed patients. Therefore, treating sleep disturbance in early adolescence may lower the chance of these negative results (41, 42). Data from another survey on the relationship between sleep disorders and depression in 4,175 young people aged 11–17 years showed that depression raises the likelihood of sleep loss, which in turn raises the likelihood of depression (43). Therefore, to reduce depression, it is particularly important to improve sleep in adolescents.
The results showed that the longer the use of screen time by middle school students, the higher their level of depression (Table 2). Numerous studies have demonstrated that screen time exerts a detrimental effect on depression. A study of 1,380 Egyptian college students showed that prolonged smartphone use may lead to depression (44). Another survey of 688 Lebanese university students found that mobile phone addicts were more likely to experience depression (45). Notably, previous studies have emphasized that the impact of screen time on depression results from excessive screen time encroaching on and affecting the duration and quality of sleep (46). However, the results of this study showed that compared with sleep quality, screen time has a stronger effect on depression (Table 2); even under the condition of sufficient sleep time, longer screen time itself may lead to higher depression levels. Therefore, to prevent and reduce depression levels in adolescents, screen time should be reasonably controlled even under the condition of sufficient sleep.
Findings from a previous study suggested that family income positively impacts children's emotional wellbeing (47). A study of 12,210 middle- and high-school adolescent students showed that low family income is an important factor affecting depression (48). Our results were consistent with previous findings. According to the preliminary analysis, the higher the family income of rural middle school students in Northeast China, the lower their level of depression (Table 3), which supports previous research. Although income is one of the most commonly used indicators of an individual or household's financial status, the relationship between income and depression remains unclear. Low income was not linked to depression in Spain, according to a Collaborative Research on Aging in Europe (COURAGE) study carried out in Finland, Poland, and Spain (49). Perhaps low income is not a primary risk factor associated with depression for Spaniards (50). It is possible that sunshine (51) and diet (52) play a mitigating role. Therefore, when other socioeconomic factors (such as education level and employment status) and health status are controlled for, this link is greatly reduced or even becomes insignificant (53, 54). The 2018 China Health and Retirement Longitudinal Study (CHARLS), a cross-sectional study of 16,545 individuals, showed that a higher level of economic development largely contributes to the alleviation of depression (55). A study on cognitive vulnerability to depression among Canadian and Chinese adolescents showed that Chinese adolescents had higher levels of depressive symptoms than Canadian adolescents due to differences in culture and beliefs (56). A substantial amount of research has examined the connection between socioeconomic position and mental health. There are some studies that suggest that the level of depression may vary due to cultural differences, different economic levels (55, 57), but we did not find similar results. This may be related to the concentration of regions we have chosen and the small sample size.
5 Limitations
Our study participants came from a single school in Benxi City. Therefore, it is difficult to generalize these results to other cities in the northeast region. As this was a cross-sectional study, we were unable to determine a causal relationship between depression levels and lifestyle habits among middle school students.
6 Conclusions
Among rural middle-school students in northeastern China, depression levels were much higher in girls than in boys. High sleep quality and high physical activity levels were negatively associated with depression, while low household income and high screen time were positively associated with depression. Therefore, factors such as strengthening physical activity, improving sleep quality, and reducing screen time can greatly help prevent and reduce depression.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of Gannan Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JZ: Writing—original draft, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing—review & editing. XW: Software, Writing—review & editing. SX: Software, Writing—review & editing. WY: Project administration, Writing—review & editing. JW: Validation, Writing—review & editing. EW: Software, Writing—review & editing. TL: Data curation, Writing—review & editing. MH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Starting Research Fund from the Gannan Medical University.
Acknowledgments
We would like to express our appreciation to all the participants.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Clarke DM, Currie KC. Depression, anxiety and their relationship with chronic diseases: a review of the epidemiology, risk and treatment evidence. Med J Aust. (2009) 190:54–60. doi: 10.5694/j.1326-5377.2009.tb02471.x
2. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J, et al. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res. (2020) 126:134–40. doi: 10.1016/j.jpsychires.2019.08.002
3. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
4. Shorey S, Ng ED, Wong CHJ. Global prevalence of depression and elevated depressive symptoms among adolescents: a systematic review and meta-analysis. Br J Clin Psychol. (2021) 61:287–305. doi: 10.1111/bjc.12333
5. Liu C, Pan W, Zhu D, Meng F, Tian T, Li L, et al. Factors of suicidal behavior among inpatients with major depressive disorder: a retrospective case series. Front Psychiatry. (2022) 13:996402. doi: 10.3389/fpsyt.2022.996402
6. Cipriani A, Barbui C, Butler R, Hatcher S, Geddes J. Depression in adults: drug and physical treatments. BMJ Clin Evid. (2011) 2011:1003.
7. Taheri M. Comparative study of the long-term impact of the COVID-19 pandemic on mental health and nutritional practices among international elite and sub-elite athletes: a sample of 1420 participants from 14 countries. Sports Med-Open. (2023) 9:104. doi: 10.1186/s40798-023-00653-w
8. Pranoto NW. The effects of inactivity during the COVID-19 pandemic on the psychomotor skills of kindergarten students. Ann Appl Sport Sci. (2023). doi: 10.52547/aassjournal.1162
9. Afshar-Zanjani H, Khalifesoltani F, Hajializadeh K, Ahadi H. Comparison of the effectiveness of self-efficacy-based training and compassion-focused therapy on depression, self-care behaviors, and quality of life of patients with irritable bowel syndrome. Int J Body Mind Cult. (2021) 8. doi: 10.22122/ijbmc.v8i1.287
10. Choi KW, Chen CY, Stein MB, Klimentidis YC, Wang MJ, Koenen KC, et al. Assessment of bidirectional relationships between physical activity and depression among adults: a 2-sample Mendelian Randomization Study. JAMA Psychiatry. (2019) 76:399–408. doi: 10.1001/jamapsychiatry.2018.4175
11. Zhang CS, Cheng L, Chen X, Wang Y, Wei S, Sun J, et al. The strategies of exercise intervention for adolescent depression: a meta-analysis of randomized controlled trials. Front Psychol. (2022) 13:974382. doi: 10.3389/fpsyg.2022.974382
12. Baiden P, Spoor SP, Nicholas JK, Brown FA. LaBrenz, CA, Spadola, C. Association between use of electronic vaping products and insufficient sleep among adolescents: findings from the 2017 and 2019 YRBS. Sleep Med. (2023) 101:19–27. doi: 10.1016/j.sleep.2022.10.005
13. Mohan J, Xiaofan G, Yingxian S. Association between sleep time and depression: a cross-sectional study from countries in rural Northeastern China. J Int Med Res. (2017) 45:984–92. doi: 10.1177/0300060517701034
14. Lee JE, Jang SI, Ju YJ, Kim W, Lee HJ, Park EC, et al. Relationship between mobile phone addiction and the incidence of poor and short sleep among Korean Adolescents: a Longitudinal Study of the Korean Children and Youth Panel Survey. J Korean Med Sci. (2017) 32:1166–72. doi: 10.3346/jkms.2017.32.7.1166
15. Ng KC, Wu LH, Lam HY, Lam LK, Nip PY, Ng CM, et al. The relationships between mobile phone use and depressive symptoms, bodily pain, and daytime sleepiness in Hong Kong secondary school students. Addict Behav. (2020) 101:105975. doi: 10.1016/j.addbeh.2019.04.033
16. Hankin BL, Abramson LY, Moffitt TE, Silva PA, McGee R, Angell KE, et al. Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. J Abnorm Psychol. (1998) 107:128–40. doi: 10.1037//0021-843X.107.1.128
17. Qu M, Yang K, Ren H, Wen L, Tan S, Xiu M, et al. The impact of school education on depressive symptoms in Chinese adolescents: a prospective longitudinal study. Int J Ment Health Addict. (2022) 1–15. doi: 10.1007/s11469-022-00944-5
18. Li C, Liang Z, Yin X, Zhang Q. Family social capital mediates the effect of poverty on children's anxiety and depression. J Community Psychol. (2018) 46:983–95. doi: 10.1002/jcop.22086
19. Yang G, Li Y, Liu S. Physical activity influences the mobile phone addiction among Chinese undergraduates: the moderating effect of exercise type. J Behav Addict. (2021) 10:799–810. doi: 10.1556/2006.2021.00059
20. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
21. Zung WWA. self-rating depression scale. Arch Gen Psychiatry. (1965) 12:63–70. doi: 10.1001/archpsyc.1965.01720310065008
22. Wu C, Hao M, Liu X, Yang D, Liu B, Yan W, et al. The effects of body dissatisfaction and depression levels on the dietary habits of university students in southern China during COVID-19. Front Nutr. (2023) 10:1103724. doi: 10.3389/fnut.2023.1103724
23. Hao M, Liu X, Wang Y, Wu Q, Yan W, Hao Y, et al. The associations between body dissatisfaction, exercise intensity, sleep quality, and depression in university students in southern China. Front Psychiatry. (2023) 14:1118855. doi: 10.3389/fpsyt.2023.1118855
24. Wang W, Xie X, Wang X. Cyberbullying and depression among Chinese college students: a moderated mediation model of social anxiety and neuroticism. J Affect Disord. (2019) 256:54–61. doi: 10.1016/j.jad.2019.05.061
25. Huang Y, Heflin CM, Validova A. Material hardship, perceived stress, and health in early adulthood. Ann Epidemiol. (2021) 53:69–75.e3. doi: 10.1016/j.annepidem.2020.08.017
26. Fenzel LM, Richardson KD. The stress process among emerging adults: spirituality, mindfulness, resilience, and self-compassion as predictors of life satisfaction and depressive symptoms. J Adult Dev. (2022) 29:1–15. doi: 10.1007/s10804-021-09384-2
27. Feldt R, Bejar M, Lee J, Louison R. Vocational identity resources in emerging adulthood: associations with facets of dispositional mindfulness. Career Dev Q. (2021) 69:2–18. doi: 10.1002/cdq.12245
29. Wichstrøm L. The emergence of gender difference in depressed mood during adolescence: the role of intensified gender socialization. Dev Psychol. (1999) 35:232–45. doi: 10.1037/0012-1649.35.1.232
30. Sun W, Mei J, Wang Y, Zhao X, Zhu Z, Zhang C, et al. Psycho-social factors associated with high depressive symptomatology in female adolescents and gender difference in adolescent depression: an epidemiological survey in China's Hubei Province. BMC Psychiatry. (2021) 21:168. doi: 10.1186/s12888-021-03165-7
31. Zhang X, Yan Y, Ye Z, Xie J. Descriptive analysis of depression among adolescents in Huangshi, China. BMC Psychiatry. (2023) 23:176. doi: 10.1186/s12888-023-04682-3
32. Wang H, Bragg F, Guan Y, Zhong J, Li N, Pan J, et al. Association between duration of electronic screen use for non-educational purposes and depression symptoms among middle and high school students: a cross-sectional study in Zhejiang Province, China. Front Public Health. (2023) 11:1138152. doi: 10.3389/fpubh.2023.1138152
33. Maeng LY, Milad MR. Sex differences in anxiety disorders: interactions between fear, stress, and gonadal hormones. Horm Behav. (2015) 76:106–17. doi: 10.1016/j.yhbeh.2015.04.002
34. Hankin BL, Abramson LY. Development of gender differences in depression: description and possible explanations. Ann Med. (1999) 31:372–9. doi: 10.3109/07853899908998794
35. Ninsiima AB, Leye E, Michielsen K. “Girls have more challenges; they need to be locked up”: a qualitative study of gender norms and the sexuality of young adolescents in Uganda. Int J Environ Res Public Health. (2018) 15:193. doi: 10.3390/ijerph15020193
36. Fang P, Sun L, Shi SS. Influencing factors related to female sports participation under the implementation of chinese government interventions: an analysis based on the China family panel studies. Front Public Health. (2022) 10:875373. doi: 10.3389/fpubh.2022.875373
37. Andersson E, Hovland A, Kjellman B, Taube J, Martinsen E. Physical activity is just as good as CBT or drugs for depression. Lakartidningen. (2015) 112:DP4E.
38. Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. (2003) 36:698–703. doi: 10.1016/S0091-7435(03)00042-2
39. Harvey SB, Øverland S, Hatch SL, Wessely S, Mykletun A, Hotopf M, et al. Exercise and the prevention of depression: results of the HUNT Cohort Study. Am J Psychiatry. (2018) 175:28–36. doi: 10.1176/appi.ajp.2017.16111223
40. Nunes ML, Bruni O. Insomnia in childhood and adolescence: clinical aspects, diagnosis, and therapeutic approach. J Pediatr. (2015) 91:26–35. doi: 10.1016/j.jped.2015.08.006
41. de Zambotti M, Goldstone A, Colrain IM, Baker, FC. Insomnia disorder in adolescence: diagnosis, impact, and treatment. Sleep Med Rev. (2018) 39:12–24. doi: 10.1016/j.smrv.2017.06.009
42. Wang X, Cheng S, Xu H. Systematic review and meta-analysis of the relationship between sleep disorders and suicidal behaviour in patients with depression. BMC Psychiatry. (2019) 19:303. doi: 10.1186/s12888-019-2302-5
43. Roberts RE, Duong HT. The prospective association between sleep deprivation and depression among adolescents. Sleep. (2014) 37:239–44. doi: 10.5665/sleep.3388
44. Okasha T, Saad A, Ibrahim I, Elhabiby M, Khalil S, Morsy M, et al. Prevalence of smartphone addiction and its correlates in a sample of Egyptian university students. Int J Soc Psychiatry. (2021) 68:1580–8. doi: 10.1177/00207640211042917
45. Matar Boumosleh J, Jaalouk D. Depression, anxiety, and smartphone addiction in university students- a cross sectional study. PLoS ONE. (2017) 12:e0182239. doi: 10.1371/journal.pone.0182239
46. Wang W, Du X, Guo Y, Li W, Zhang S, Zhang W, et al. Associations among screen time, sleep duration and depressive symptoms among Chinese adolescents. J Affect Disord. (2021) 284:69–74. doi: 10.1016/j.jad.2021.01.082
47. Qi D, Wu Y. Family income and children's emotional wellbeing: the mediational role of parents' life satisfaction and emotional wellbeing in China. Int J Environ Res Public Health. (2020) 17:7573. doi: 10.3390/ijerph17207573
48. Lin HC, Tang TC, Yen JY, Ko CH, Huang CF, Liu SC, et al. Depression and its association with self-esteem, family, peer and school factors in a population of 9586 adolescents in southern Taiwan. Psychiatry Clin Neurosci. (2008) 62:412–20. doi: 10.1111/j.1440-1819.2008.01820.x
49. Freeman A, Tyrovolas S, Koyanagi A, Chatterji S, Leonardi M, Ayuso-Mateos JL, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health. (2016) 16:1098. doi: 10.1186/s12889-016-3638-0
50. Tuesca-Molina R, Fierro Herrera N, Molinares Sosa A, Oviedo Martínez F, Polo Arjona Y, Polo Cueto J, et al. Socializing groups as protective factor against depression in elderly people: Barranquilla, Colombia. Rev Esp Salud Publica. (2003) 77:595–604. doi: 10.1590/S1135-57272003000500008
51. Kent ST, McClure LA, Crosson WL, Arnett DK, Wadley VG, Sathiakumar N, et al. Effect of sunlight exposure on cognitive function among depressed and non-depressed participants: a REGARDS cross-sectional study. Environ Health. (2009) 8:34. doi: 10.1186/1476-069X-8-34
52. Virtanen M, Koskinen S, Kivimäki M, Honkonen T, Vahtera J, Ahola K, et al. Contribution of non-work and work-related risk factors to the association between income and mental disorders in a working population: the Health 2000 Study. Occup Environ Med. (2008) 65:171–8. doi: 10.1136/oem.2007.033159
53. Skarupski KA, Tangney CC, Li H, Evans DA, Morris MC. Mediterranean diet and depressive symptoms among older adults over time. J Nutr Health Aging. (2013) 17:441–5. doi: 10.1007/s12603-012-0437-x
54. Martikainen P, Adda J, Ferrie JE, Davey Smith G, Marmot M. Effects of income and wealth on GHQ depression and poor self rated health in white collar women and men in the Whitehall II study. J Epidemiol Community Health. (2003) 57:718–23. doi: 10.1136/jech.57.9.718
55. Wang J, Zhang J, Lin H, Han Y, Tu J, Nie X, et al. Economic development, weak ties, and depression: evidence from China. J Affect Disord. (2023) 334:246–57. doi: 10.1016/j.jad.2023.04.097
56. Auerbach RP, Eberhart NK, Abela JR. Cognitive vulnerability to depression in Canadian and Chinese adolescents. J Abnorm Child Psychol. (2010) 38:57–68. doi: 10.1007/s10802-009-9344-y
Keywords: depression, physical activity, sleep quality, screen time, household income
Citation: Zhao J, Wang X, Xu S, Yan W, Wang J, Wang E, Liu T and Hao M (2024) The influence of lifestyle habits on levels of depression among rural middle school students in Northeastern China. Front. Public Health 12:1293445. doi: 10.3389/fpubh.2024.1293445
Received: 13 September 2023; Accepted: 15 January 2024;
Published: 29 January 2024.
Edited by:
Wulf Rössler, Charité University Medicine Berlin, GermanyCopyright © 2024 Zhao, Wang, Xu, Yan, Wang, Wang, Liu and Hao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Hao, aG00ODkyMjIwMEB5YWhvby5jby5qcA==