 Paicheng Liu
Paicheng Liu Jianxin Cheng
Jianxin Cheng Yuxuan Yang
Yuxuan Yang Haipeng Zhu
Haipeng Zhu- 1Department of Orthopaedics, Guangdong Women and Children Hospital, Guangzhou, China
- 2School of Public Administration, Southwestern University of Finance and Economics, Chengdu, China
- 3School of Public Administration and Emergency Management, Jinan University, Guangzhou, China
- 4School of Government, Sun Yat-sen University, Guangzhou, China
Background: Orthopaedics have become the focus of research on patient safety due to the high incidence of medical errors. Previous studies were based on all orthopaedic patients and rarely conducted empirical analyses from the perspective of age. This study aimed to fill the academic gap in the age variable by comparing medical errors, affected sites, and adverse consequences in orthopaedic patients.
Methods: This retrospective study included 329 litigation claims against orthopaedists using data from China Judgments Online. First, we performed computer crawling and screened 5,237 litigation documents using keywords, including medical errors. Second, 2,536 samples were retained through systematic random sampling, and 549 irrelevant cases were deleted after manual reading. Finally, three clinicians from different medical departments selected 329 incidents related to orthopaedics for further analysis, according to the description of the lawsuits. Three other professional orthopaedists evaluated the patients’ ages, affected sites of medical errors, and adverse consequences.
Results: The greatest number of medical errors was observed in the joints (30.43%) for all orthopaedic patients. However, adult patients (aged 18–60 years) were most susceptible to errors in the extremities (30.42%). A higher rate of complications was associated with a higher rate of morbidity/mortality for the corresponding patients. Medical errors correlated with complications occurred in the following sites: joints (15.38%), extremities (12.50%), spine (16.95%), multiple sites (15.38%), and hands and feet (14.81%). In addition to surgical errors, over 10% of all orthopaedic patients experienced missed diagnoses. The incidence of insufficient adherence to informed consent obligations was 13.5% among adult patients and was much higher in paediatric and older adults patients. When orthopaedic patients suffered from medical technical errors, iatrogenic mortality/morbidity would decrease by 0.3% for one unit increase in age.
Conclusion: Dividing patients into different ages demonstrated diverse results in terms of medical errors and affected sites. Negligence in diagnosis and examination can be fatal factors that endanger safety, and complications may cause morbidity/mortality. When patients suffered from technical errors, age is inversely proportional to mortality/morbidity. Special attention needs to be paid to technical errors in the younger older adults population (60–64 years old), which has inspired implications in promoting aging and public health.
Introduction
As fears about the adverse impact of medical errors in the orthopaedic department grow, issues related to patient safety in surgical specialties have garnered international attention. Previous studies illustrated that the clinical departments with the most surgical accidents are trauma and orthopaedics, of which 30.1% of the incidents cause iatrogenic injuries to patients (1). In addition to higher morbidity and mortality, medical errors might lead to unnecessary health costs for patients (2), which induce increased medical litigation and insurance premiums in the orthopaedic department (3). The grim reality of the present includes the untoward search for insurance companies that are willing to take the risk of making monetary claims due to medical malpractice (4). Moreover, defensive medical behaviours are gradually increasing, and rising medical costs have resulted in the overuse of medical resources without benefiting patients (5). Hence, exploring the causes of medical errors in orthopaedic departments has become the focus of solving the aforementioned problems.
Most researchers blame surgery for medical errors in orthopaedic departments. At present, surgery has been categorized as a “very unsafe” industry, which could increase the hazard of adverse events in the clinical stage (6, 7). Meanwhile, other scholars subscribed to the view that failed teamwork in the operating theatre became an inevitable cause of medical errors (8). But some scholars hold different opinions that medical errors in the orthopaedic department may be related to humanistic factors including inadequate informed consent and invalid communication between physicians and patients during the preoperative period (9, 10). This leads us to question whether the medical errors in the orthopaedic department result from the surgeries, failure to embrace sufficient communication between physicians and patients, or a combination of both, which would further advance the preventive measures implemented in clinical practice. The aforementioned academic debates may reveal, to some extent, that research on patient safety in orthopaedic departments is still necessary.
Existing studies have preferred to regard orthopaedic patients as a whole and primarily concentrate on the adult population. Previous scholars have proven that the spine is the affected site with maximum errors (11). But according to a survey by the American Academy of Orthopaedic Surgeons (AAOS), the knees, fingers, and hands have the highest probability of medical errors, whereas the spine has the lowest probability (12). Despite wrong-site surgery being the error that elicited the most successful litigation (13), there are conspicuous disparities among different patient groups. A study of paediatric patients demonstrated that the most common reason for medical litigation was missed or incorrectly diagnosed injuries, and 44% of these were upper limb injuries, mainly fractures around the elbow (14). However, hip fractures are more severe in the older adults population, resulting in substantial morbidity and mortality (15). We believe that existing research lacks empirical analyses from the perspective of age, which may explain the paradoxical conclusions previously drawn by scholars. Further, if patients are not compared by different age groups, most countermeasures may be invalid in addressing adverse events, especially in the orthopaedic department.
To sum up, we proposed following research questions. What are the characteristics of orthopaedic patients in different age groups when suffering from medical errors? Which sites are more prone to be affected by medical errors among different age patients in the orthopaedic department? Have medical errors caused iatrogenic mortality or morbidity among orthopaedic patients? To answer these questions, we utilized the available medical litigation to systematically sort the medical errors, prone sites, and adverse consequences of suffering by paediatric, adult, and older adults patients in the orthopaedic department. This study contributes to the existing literature in three aspects. Firstly, the comparative analysis among patients can fill the academic gap in existing research to enrich the comprehension of orthopaedic medical errors. Secondly, grouping comparisons from an age perspective can provide orthopaedic practitioners with more targeted preventions. Third, grouping patients by age will provide more detailed comprehensions of medical errors in paediatric and older adults orthopaedic patients, which will play an imperative role in promoting aging and public health in particular.
Materials and methods
Study design and sample
Research on patient safety in China habitually lags behind that in other countries due to a lack of data, as the medical error collection system has not yet been constructed. However, China Judgments Online (CJO) provides a new approach to the study of medical errors. According to the provisions of the Supreme People’s Court of the People’s Republic of China, except for particular circumstances stipulated by the law, legally effective judgments, rulings, and decisions should generally be available on the CJO website. Hence, it is possible to retrieve litigation documents related to medical errors on the public CJO website for research without ethical approval. The Ethics Committee of Jinan University (NO. JNUKY-2021-035) approved this study and we confirm all methods were performed in accordance with the relevant guidelines and regulations.
The samples used in this study were selected in the four steps detailed in Figure 1. First, we utilized keywords with regard to medical errors and adverse events to computer crawl on the CJO website and retrieved a total of 5,237 litigation documents. Second, we eliminated 2,701 documents through systematic random sampling due to the limited research funding and the high cost of manual reading, including some samples with missing texts as well. Third, we removed 549 documents that were unrelated to medical errors through manual review. These unrelated documents do not cover the content of medical errors from orthopaedic department and are inconsistent with the subject of this study. Finally, we invited three clinical physicians to identify the medical errors and specialties in 1,987 litigation documents. We obtained 329 orthopaedic samples after removing 1,658 documents from other specialities.

Figure 1. Process of sample selection.
Data collection
For the coding of medical errors and departments, we referred to the definition and classification criteria in the existing literature. We defined medical error as an act of omission or commission in planning or executing that contributes or could contribute to an unintended result (16). Combing another study on medical errors in China (17), we identified the types of medical errors and the classification of medical departments. The specific classifications of the medical errors and departments are detailed in Appendix 1. Initially, two clinical physicians independently reviewed litigation documents and judged the medical errors and specialties involved. A third doctor reread any inconsistent results and determined a final judgment. We then retained 329 cases that appeared in the orthopaedic department for further coding. To obtain accurate data, we invited three professional orthopaedists with more than 10 years of clinical experience to conduct a second batch of coding. According to the text in the litigation documents, two orthopaedists coded the patient information, including sex, age, type of surgery, affected sites of medical error, mortality, morbidity, and complications.
To analyse the affected sites of medical errors among patients of different ages, we divided them into three groups according to age range: paediatric patients (aged ≤18 years), adult patients (aged 18–60 years), and older adults patients (aged ≥60 years). Based on whether the patients underwent surgery, we classified the surgery types into surgery and non-surgery groups and further divided surgery into emergency surgery and selective surgery. Combining the directories of orthopaedic subspecialties in Chinese clinical practice and the classification of orthopaedic surgical sites in existing literature (18), we grouped the sites affected by medical errors into the following seven categories: joints (excluding extremities and spine), spine, pelvis, hands and feet, limbs, multiple sites, and other. Finally, a third orthopaedist reviewed the disparate results and independently provided the final judgment. All information about the patients is anonymous.
We utilized LOGIT regression to investigate the association between the iatrogenic mortality/morbidity and the age of the patient. The independent variable was the age of the patient, which was extracted from the patient information in the litigation documents. The dependent variable was whether iatrogenic mortality/morbidity occurred. We assigned a value of “1” to iatrogenic mortality/morbidity, “0” to no iatrogenic mortality/morbidity. The control variables included gender, whether multiple departments were involved in treatment, hospital class, and affected site.
Results
In terms of the total patient population, the joints, extremities, and spine were the three sites with the highest rates of medical errors (Figure 2). However, there were apparent discrepancies in the affected sites after subdivision into different patient groups. For example, joints were the most frequently affected sites in paediatric and older adults patients, but adult patients were more prone to medical errors in the extremities. Although the incidence of medical errors in the spine increased with the age of the patients, the hands and feet showed diametrical results, as the proportion of medical errors was highest in paediatric patients.
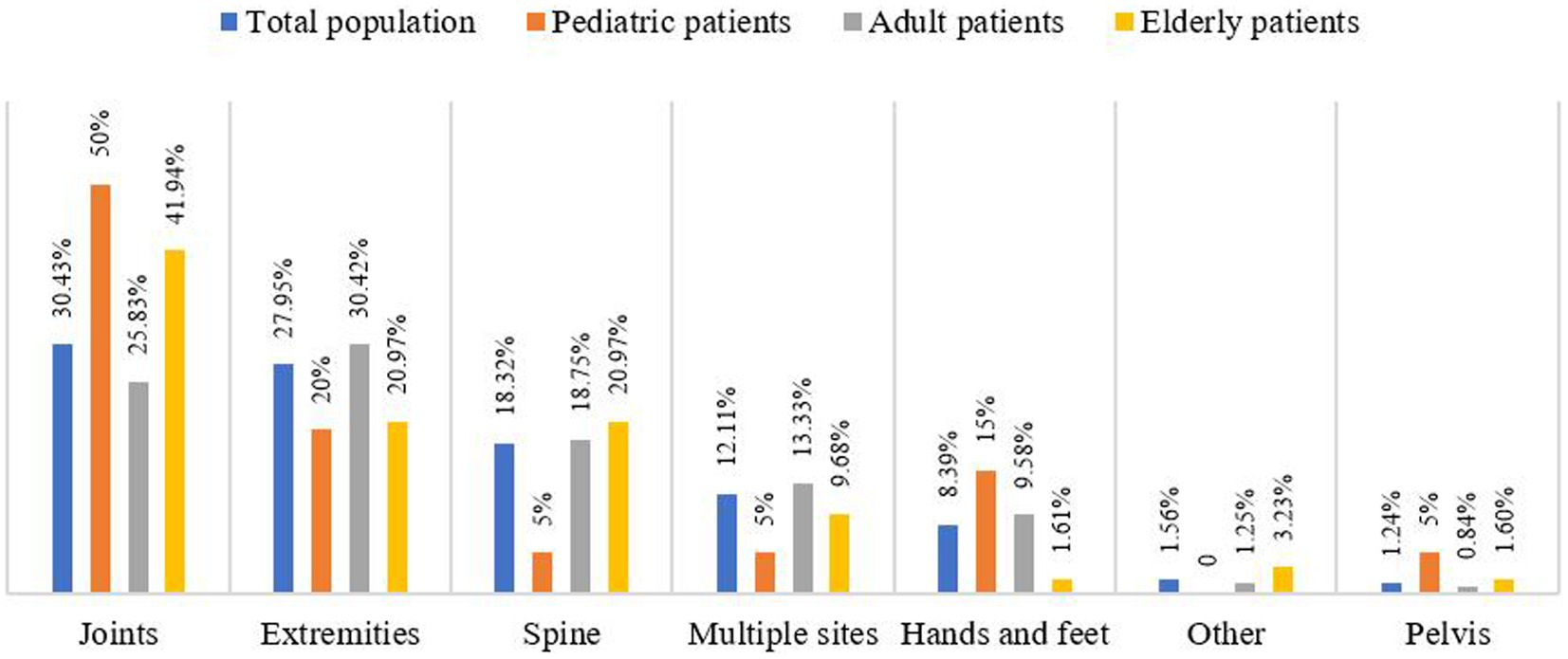
Figure 2. Affected sites of medical errors among different population.
As shown in Figure 3, different affected sites may cause different degrees of harm to patients in diverse groups. Furthermore, even though we cannot infer that complications were the fundamental reason for morbidity/mortality of patients, as 7.14% of paediatric patients had medical errors in the spine, but none suffered morbidity/mortality, we realized that there was a high association between complications and morbidity/mortality within different affected sites. Specifically, a higher incidence of complications was associated with a higher rate of morbidity/mortality in the corresponding patients. Half of the paediatric patients suffered from complications due to medical errors in the joints, and morbidity/mortality accounted for 53.85%. It is worth noting that similar circumstances appeared in adult patients with medical errors in the extremities and in older adults patients with medical errors in the joints.
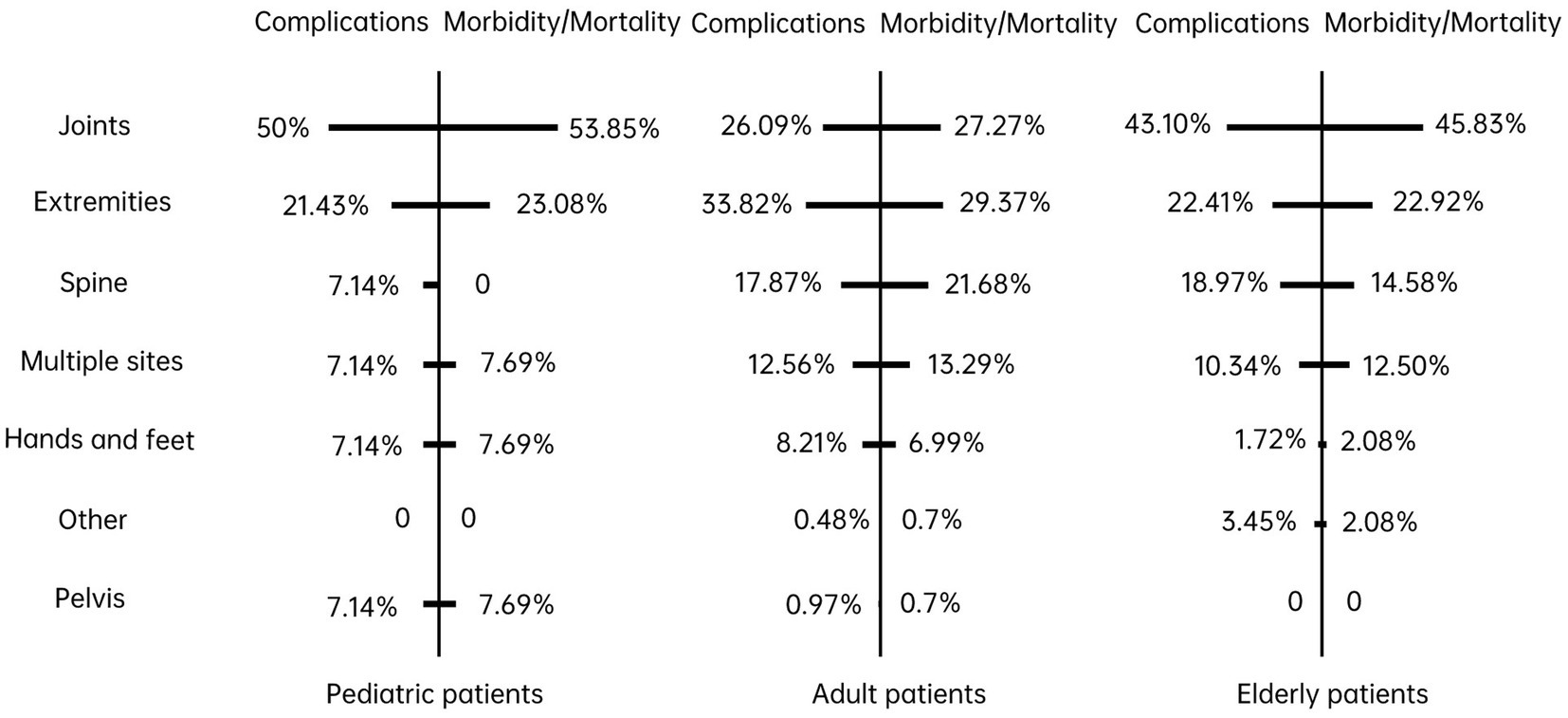
Figure 3. Complications and morbidity/mortality of affected sites among different patients.
To better understand the relationship between medical errors and affected sites, we calculated the three most frequent types of medical errors at different sites. The first column in Table 1 is the affected sites where medical errors occur, and the number in the brackets is the proportion of errors in each site. The results in Table 1 show that medical errors correlated with complications, especially post-operative complications, arose in all included sites: joints (12.77%), extremities (12.50%), spine (16.95%), hands and feet (14.81%), and multiple sites (15.38%). In addition, insufficient implementation of informed consent obligations attached to physician-patient communication was the foremost type of medical error in extremities (19.32%), and multiple sites (28.21%). Missed diagnoses were found in joints (9.57%), extremities (12.50%), spine (10.17%), and multiple sites (10.26%), compared with other sites. Although we cannot assert that there are causalities between missed diagnoses and the four aforementioned affected sites, missed diagnosis is still a vigilant signal.
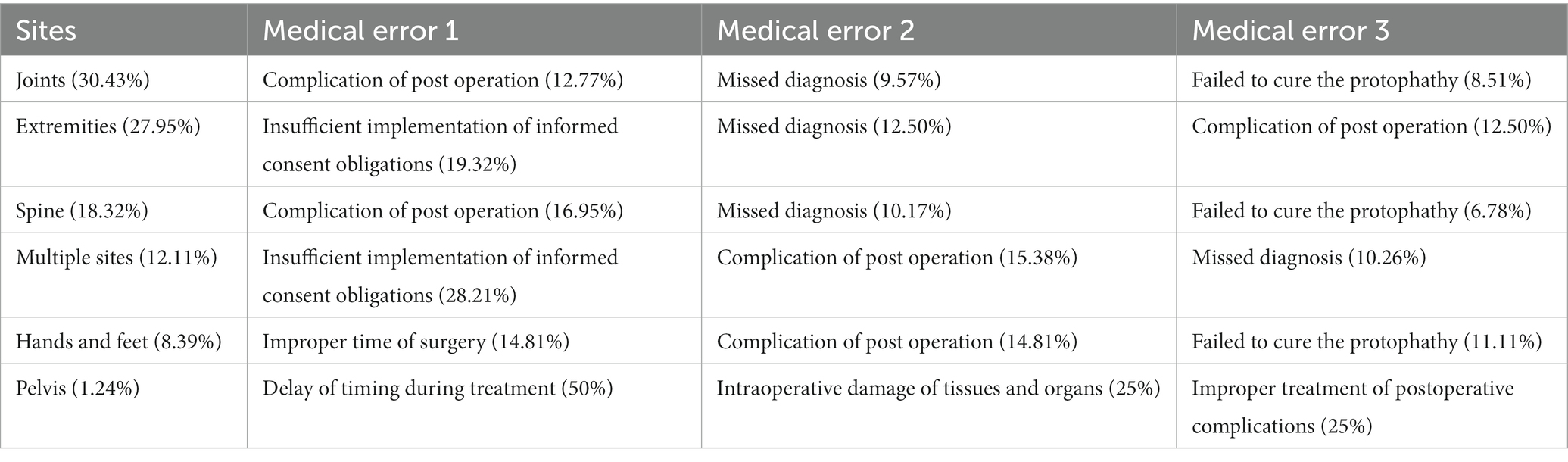
Table 1. Three most frequent medical errors in different sites.
All orthopaedic patients are susceptible to errors in medical technology; however, these errors are not restricted to surgery. Medical errors in diagnosis and examination also impair orthopaedic safety, especially in the paediatric population. As shown in Table 2, missed diagnosis (3103) was not the most continual error but was experienced by over 10% of all orthopaedic patients. Errors in the treatment plan (3303) severely impacted paediatric patients, and the incidence was four times higher than that of adults. The prevalence of post-operative complications (3609) in adult and older adults patients was 13.92 and 13.56%, respectively. However, among adult patients, the rate of insufficient implementation of informed consent obligations was 13.5%, which was much higher than that of paediatric and older adults patients.

Table 2. Top ten medical errors of patients in different age groups.
Additionally, 4.22% of adult patients challenged informal writing or modification of medical records (7103), which was remarkably different from the other two groups. Although the insufficient implementation of informed consent obligations correspondingly threatens the safety of older adults orthopaedic patients, insufficient inspection (3203) was nearly 3.3 times higher than that of adults. In summary, there are discrepancies in medical errors among different patients. Medical technical errors and medical humanistic errors are the two chief foundations of litigation in orthopaedic departments.
Given the disparities in the harm of medical technical errors and medical humanistic errors to different age groups of patients, we performed regression analysis for patient’s age and iatrogenic mortality/morbidity. As shown in Table 3, there is no significant relationship between age and the iatrogenic mortality/morbidity for medical humanistic errors. However, for medical technical errors, iatrogenic mortality/morbidity decreases with age. Specially, the iatrogenic mortality/morbidity decreased by 0.3% for every year increase in age. This finding reveals that as orthopaedic patient’s age increase, the damage caused by medical technical errors decreases.
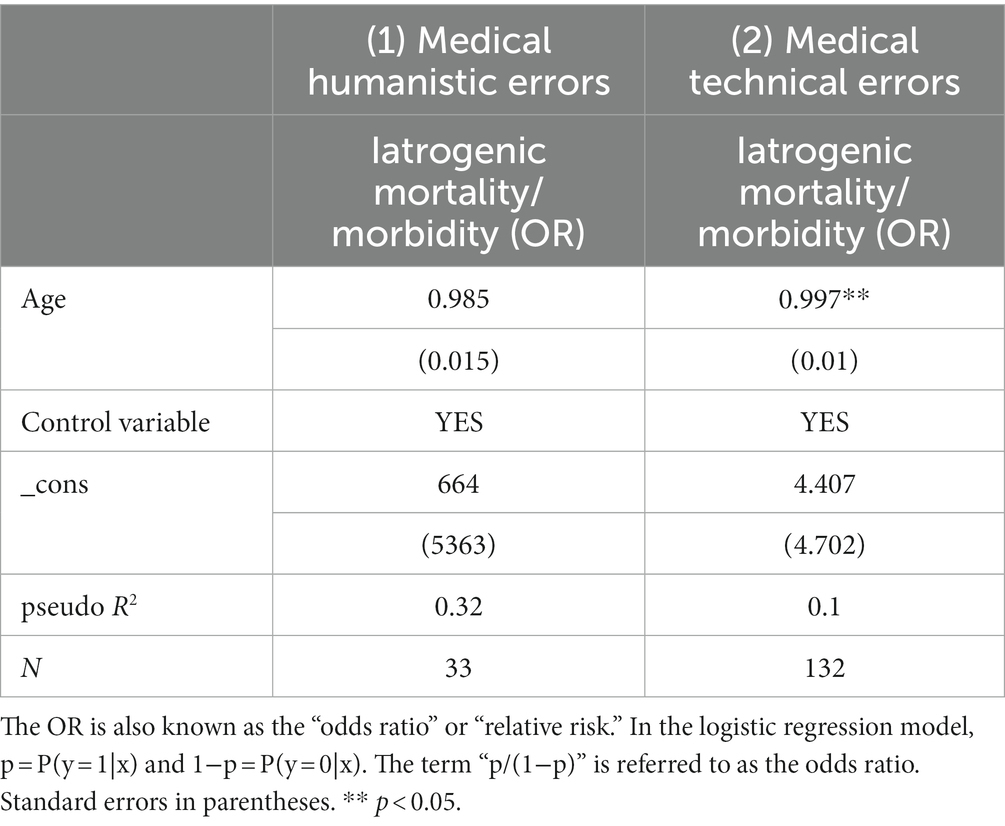
Table 3. Relationship between age of patient and iatrogenic mortality/morbidity.
Discussion
Through quantitative analysis of medical litigation documents, we concluded that the joint was the most prone to medical errors. However, after adding the variable of age, diverse patients manifested dissimilar characteristic trends in the affected sites. Previous findings have shown that the majority of deaths or severe permanent injuries coexist with the spine in all orthopaedic patients (18). But we recognized that paediatric and older adults patients were more likely to experience medical errors in the joints, which is akin to the previous conclusion that operative procedures on joints resulted in the most claims in paediatrics group (19). Hence, standardize care processes have been regarded as the best tool for implementing safety culture in paediatrics (20). While the extremities were the primary sites for medical errors in adult patients, revealing that affected sites with the most medical errors were different after dividing the patients into groups according to age. This discrepancy suggests that attention to certain medical error sites should be allocated separately to different groups rather than considering orthopaedic patients as a whole. This will not only provide more detailed countermeasures for preventing medical errors but will also effectively improve patient safety in different populations.
A broad consensus has been reached that surgical safety should be a substantial global public health issue (21), but it is worth considering the adverse consequences of medical errors in other clinical stages. Most medical errors are linked to medical technology (12, 22); however, medical errors in the diagnosis and examination stages seem to be neglected in the orthopaedic department. Diagnosis and examination are the two prerequisites for successful surgery, but existing studies have overemphasized improper procedures during surgery (22) while disregarding precise diagnosis and sufficient examination. We concluded that over 10% of orthopaedic patients suffered from inaccurate diagnosis, and the impact of errors in treatment plans for paediatric patients and insufficient inspection of older adults patients were more serious than those of adult patients, which may have been formerly overlooked by scholars. Although orthopaedists place more emphasis on surgery, accumulating rich expertise and developing skilful diagnostic abilities are imperative in practice (23), especially when providing clinical receptions for paediatric patients (24).
There are disparate emphases on how to rectify medical errors in orthopaedic departments. We are not opposed to the indispensable role of surgical checklists in promoting patient safety (25, 26). A free and simple intervention, such as a two-lesson training, significantly stimulated the correct use of the surgical safety checklist (27). Safety guidelines in anaesthesia and obstetric departments have successfully achieved the goal of promoting patient safety (28). The implementation and regular use of surgical checklists may also become important elements in orthopaedic safety programs (29). However, the surgical safety checklist has been finitely applied in orthopaedic departments in practice, with 65.3% of Brazilian orthopaedists unaware of this protocol (10). In addition, the FDA created an analogous program called MedWatch to aid healthcare professionals in reporting adverse events, which aimed to help orthopaedic surgeons protect their patients (30). Other scholars believe that shifting the culture surrounding medical errors from blame to understanding and prevention could accomplish mutual benefits for patients and surgeons in orthopaedic departments (31).
Additionally, it is equally vital to enhance physician-patient communication to prevent additional medical errors in the orthopaedic department. Generally speaking, verbal aggression toward the physicians or between patients has been the most reported events (32). Despite having identified the insufficient implementation of informed consent obligations as a challenge for orthopaedists (33), further analysis indicated that this challenge may be more frequent in adult and older adults patients, especially in the adult population. This academic contribution differs from existing conclusions. However, some countermeasures and suggestions provided by previous research seem to align with this study. Therefore, we emphasize that, in addition to the necessary attention given to the surgical stage, treatment, diagnosis, and physician-patient communication might equally require more consideration.
Finally, orthopaedists must be alert to medical errors associated with complications, which, in addition to leading to medical claims (34), may lead to further morbidity and mortality (35). Owing to the lack of rigorous experimental data, we cannot provide scientific answers to the causality between complications and morbidity/mortality. However, we observed positive correlations between complications and morbidity/mortality, which might provide innovative insights for promoting orthopaedic patient safety in the future. Most complications in orthopaedic surgery can be dealt with adequately, provided they are anticipated with implemented risk-reduction strategies (36). Hence, we should prioritize addressing medical errors by combining the age and affected sites of patients in clinical practice. Additionally, the COVID-19 pandemic has given to the spread of telemedicine in the orthopaedic field (37), which might be an effective approach to improve the patient safety in the orthopaedic specialty. Previous interventions might be less effective, as they are slightly generic and exceedingly concentrated on the operation stage.
Conclusion
Subdivision of orthopaedic patients into different groups based on age demonstrated entirely dissimilar results in both affected sites and medical errors. In addition to surgery, negligence in diagnosis and examination is also a fatal factor endangering patient safety. Complications may cause morbidity or mortality among different orthopaedic patient groups, but the underlying mechanism remains unclear. Patient age and affected sites should be integrated to discern the medical errors that may occur in the orthopaedic department and prevent adverse events in clinical practice accordingly. Additionally, special attention needs to be paid to medical technical errors in the younger older adults population because they have higher iatrogenic mortality/morbidity in comparison to senile patients (≥ 65 years old). This finding has inspired implications in promoting aging and public health.
Limitations of this study
Due to the limited samples of paediatric patients, the analysis seems to be insufficient for this population. More patient demographics were not included in the litigation documents; hence we were unable to perform more quantitative analysis in this dimension. Similarly, we were unable to explain the causal mechanism between complications and morbidity/mortality. However, the database in this study has been the best material to study patient safety in China so far. The conclusions could promote health for patients and guide clinical practice for medical staff as well.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the ethics committee of Jinan University waived the need of informed consent. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
PL: Conceptualization, Funding acquisition, Investigation, Writing – original draft. JC: Methodology, Resources, Writing – review & editing. YY: Data curation, Methodology, Software, Writing – original draft. HZ: Conceptualization, Data curation, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Fundamental Research Funds for the Central Universities (JBK2304133).
Acknowledgments
Thanks to the three physicians involved in this study for their dedication to error coding. They are Dr. Ren Chen (from the Department of Radiotherapy, Nanfang Hospital of Southern Medical University), Dr. Deng Jun (from the Department of Gastroenterology, Sixth Affiliated Hospital of Sun Yat-sen University), and Dr. Gao Wenjie (from the Department of Orthopaedics, Sun Yat-sen Memorial Hospital, Sun Yat-sen University).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1306215/full#supplementary-material
Abbreviations
AAOS, American Academy of Orthopaedic Surgeons; CJO, China Judgments Online.
References
1. Panesar, SS, Carson-Stevens, A, Salvilla, SA, Patel, B, Mirza, SB, and Mann, B. Patient safety in orthopedic surgery: prioritizing key areas of iatrogenic harm through an analysis of 48,095 incidents reported to a national database of errors. Drug Healthc Patient Saf. (2013) 5:57–65. doi: 10.2147/DHPS.S40887
2. Zhan, CL, and Miller, MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. (2003) 290:1868–74. doi: 10.1001/jama.290.14.1868
3. Aoki, UK, Ohta, S, Kiuchi, T, and Fukui, T. Impact of miscommunication in medical dispute cases in Japan. Int Qual Health Care. (2007) 20:358–62. doi: 10.1093/intqhc/mzn028
4. Traina, F. Medical malpractice: the experience in Italy. Clin Orthop Relat Res. (2009) 467:434–42. doi: 10.1007/s11999-008-0582-z
5. He, AJ. The doctor-patient relationship, defensive medicine and over-prescription in Chinese public hospitals: evidence from a cross-sectional survey in Shenzhen city. Soc Sci Med. (2014) 123:64–71. doi: 10.1016/j.socscimed.2014.10.055
6. Panesar, SS, Noble, DJ, Mirza, SB, Patel, B, Mann, B, Emerton, M, et al. Can the surgical checklist reduce the risk of wrong site surgery in orthopaedics? Can the checklist help? Supporting evidence from analysis of a national patient incident reporting system. J Orthop Surg Res. (2011) 6:18. doi: 10.1186/1749-799X-6-18
7. Amalberti, R, Auroy, Y, Berwick, D, and Barach, P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. (2005) 142:756–64. doi: 10.7326/0003-4819-142-9-200505030-00012
8. Emerton, M, Panesar, SS, and Forrest, K. Safer surgery: how a checklist can make orthopaedic surgery safer. Orthop Trauma. (2009) 23:377–80. doi: 10.1016/j.mporth.2009.08.004
9. Gould, MT, Langworthy, MJ, Santore, R, and Provencher, MT. An analysis of orthopaedic liability in the acute care setting. Clin Orthop Relat Res. (2003) 407:59–66. doi: 10.1097/00003086-200302000-00011
10. Motta Filho, GDR, Neves da Silva, LF, Ferracini, AM, and Bähr, GL. The WHO surgical safety checklist: knowledge and use by Brazilian orthopedists. Rev Bras Ortop. (2013) 48:554–62. doi: 10.1016/j.rbo.2013.08.002
11. Tarantino, U, Giai Via, A, Macrì, E, Eramo, A, Marino, V, and Marsella, LT. Professional liability in orthopaedics and traumatology in Italy. Clin Othop Relat Res. (2013) 471:3349–57. doi: 10.1007/s11999-013-3165-6
12. Wong, DA, Herndon, JH, Canale, ST, Brooks, RL, Hunt, TR, Epps, HR, et al. Medical errors in orthopaedics. Results of an AAOS member survey. J Bone Joint Surg Am. (2009) 91:547–57. doi: 10.2106/JBJS.G.01439
13. Harrison, WD, Narayan, B, Newton, AW, Banks, JV, and Cheung, G. Litigation costs of wrong-site surgery and other non-technical errors in orthopaedic operating theatres. Ann R Coll Surg Engl. (2015) 97:592–7. doi: 10.1308/rcsann.2015.0045
14. Atrey, A, Nicolaou, N, Katchburian, M, and Norman-Taylor, F. A review of reported litigation against English health trusts for the treatment of children in orthopaedics: present trends and suggestions to reduce mistakes. J Child Orthop. (2010) 4:471–6. doi: 10.1007/s11832-010-0276-4
15. Beaupre, LA, Cinats, JG, Senthilselvan, A, Lier, D, Jones, CA, Scharfenberger, A, et al. Reduced morbidity for elderly patients with a hip fracture after implementation of a perioperative evidence-based clinical pathway. Qual Saf Health Care. (2006) 15:375–9. doi: 10.1136/qshc.2005.017095
17. Liu, J, Liu, P, Gong, X, and Liang, F. Relating medical errors to medical specialties: a mixed analysis based on litigation documents and qualitative data. Risk Manag Healthc Policy. (2020) 13:335–45. doi: 10.2147/RMHP.S246452
18. Matsen, FA 3rd, Stephens, L, Jette, JL, Warme, WJ, and Posner, KL. Lessons regarding the safety of orthopaedic patient care: an analysis of four hundred and sixty-four closed malpractice claims. J Bone Joint Surg Am. (2013) 95:e201–8. doi: 10.2106/JBJS.K.01272
19. Jessica, B, Shrader, MW, Boan, C, and Belthur, M. Characteristics of medical professional liability claims in pediatric orthopedics. J Patient Saf. (2021) 17:e1088–96. doi: 10.1097/PTS.0000000000000484
20. Nicoi, S, Benevento, M, Ferorelli, D, Mandarelli, G, and Solarino, B. Little patients, large risks: an overview on patient safety management in pediatrics settings. Front Pediatr. (2022) 10:919710. doi: 10.3389/fped.2022.919710
21. Weiser, TG, Regenbogen, SE, Thompson, KD, Haynes, AB, Lipsitz, SR, Berry, WR, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. (2008) 372:139–44. doi: 10.1016/S0140-6736(08)60878-8
22. Casali, MB, Blandino, A, Del Sordo, S, Vignali, G, Novello, S, Travaini, G, et al. Alleged malpractice in orthopaedics. Analysis of a series of medmal insurance claims. J Orthop Traumatol. (2018) 19:7. doi: 10.1186/s10195-018-0500-4
23. Yamamoto, N, Watari, T, Shibata, A, Noda, T, and Ozaki, T. The impact of system and diagnostic errors for medical litigation outcomes in orthopedic surgery. J Orthop Sci. (2023) 28:484–9. doi: 10.1016/j.jos.2021.11.006
24. Conrad, VF, and Jane, GR. Strategies for the prevention of medical error in pediatrics. J Pediatr. (2003) 143:155–62. doi: 10.1067/S0022-3476(03)00244-0
25. Munigangaiah, S, Sayana, MK, and Lenehan, B. Relevance of World Health Organization surgical safety checklist to trauma and orthopaedic surgery. Acta Orthop Belg. (2012) 78:574–81.
26. Chandraharan, E. Clinical dashboards: do they actually work in practice? Three-year experience with the maternity dashboard. Clin Risk. (2010) 16:176–82. doi: 10.1258/cr.2010.010022
27. Ferorelli, D, Benevento, M, Vimercati, L, Spagnolo, L, De Maria, L, Caputi, A, et al. Improving healthcare workers’ adherence to surgical safety checklist: the impact of a short training. Front Public Health. (2022) 9:732707. doi: 10.3389/fpubh.2021.732707
28. Pegalis, SE, and Bal, BS. Closed medical negligence claims can drive patient safety and reduce litigation. Clin Orthop Relat Res. (2012) 470:1398–404. doi: 10.1007/s11999-012-2308-5
29. Kuo, CC, and Robb, WJ III. Critical roles of orthopaedic surgeon leadership in healthcare systems to improve orthopaedic surgical patient safety. Clin Orthop Relat Res. (2013) 471:1792–800. doi: 10.1007/s11999-012-2719-3
30. Mihalko, WM, Greenwald, AS, Lemons, J, and Kirkpatrick, J. Reporting and notification of adverse events in orthopaedics. J Am Acad Orthop Surg. (2010) 18:193–8. doi: 10.5435/00124635-201004000-00002
31. Panesar, SS, Shaerf, DA, Mann, BS, and Malik, AK. Patient safety in orthopaedics: state of the art. J Bone Joint Surg Br. (2012) 94-B:1595–7. doi: 10.1302/0301-620X.94B12.30217
32. Benevento, M, Nicoli, S, Mandarelli, G, Ferorelli, D, Cicolini, G, Marrone, M, et al. Strengths and weaknesses of the incident reporting system: an Italian experience. J Patient Saf Risk Manag. (2023) 28:15–20. doi: 10.1177/25160435221150568
33. Atrey, A, Gupte, CM, and Corbett, SA. Review of successful litigation against English health trusts in the treatment of adults with orthopaedic pathology: clinical governance lessons learned. J Bone Joint Surg Am. (2010) 92:e36. doi: 10.2106/JBJS.J.00277
34. Khan, IH, Jamil, W, Lynn, SM, and Khan, OH. Analysis of NHSLA claims in orthopedic surgery. Orthopedics. (2012) 35:e726–31. doi: 10.3928/01477447-20120426-28
35. Osler, T, Glance, LG, and Hosmer, DW. Complication-associated mortality following trauma: a population-based observational study. Arch Surg. (2021) 147:152–8. doi: 10.1001/archsurg.2011.888
36. Panesar, SS, Carson-Stevens, A, Mann, BS, Bhandari, M, and Madhok, R. Mortality as an indicator of patient safety in orthopaedics lessons from qualitative analysis of a database of medical errors. BMC Musculoskelet Disord. (2012) 13:93. doi: 10.1186/1471-2474-13-93
Keywords: adverse consequences, affected sites, aging and public health, medical errors, orthopaedic, patient safety
Citation: Liu P, Cheng J, Yang Y and Zhu H (2024) Medical errors, affected sites, and adverse consequences among patients in the orthopaedic department: Does age matter? Front. Public Health. 12:1306215. doi: 10.3389/fpubh.2024.1306215
Edited by:
Anees Ur Rehman, Bahauddin Zakariya University, PakistanReviewed by:
Marcello Benevento, University of Bari Aldo Moro, ItalySusan Elizabeth Esposito, Life University, United States
Copyright © 2024 Liu, Cheng, Yang and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuxuan Yang, eWFuZ3l1eHVhbnh1YW4xOTk0QDE2My5jb20=; Haipeng Zhu, emh1aHBAbWFpbDIuc3lzdS5lZHUuY24=
†These authors have contributed equally to this work