 Anne Geweniger1*
Anne Geweniger1* Michael Barth2
Michael Barth2 Anneke Haddad2Henriette Högl3Shrabon Insan1Annette Mund3
Anneke Haddad2Henriette Högl3Shrabon Insan1Annette Mund3 Thorsten Langer1
Thorsten Langer1- 1Department of Neuropediatrics and Muscle Disease, Center for Pediatrics, Medical Center—University of Freiburg, Freiburg, Germany
- 2Department of General Pediatrics, Adolescent Medicine and Neonatology, Center for Pediatrics, Medical Center—University of Freiburg, Freiburg, Germany
- 3Kindernetzwerk e.V., Mainaschaff, Germany
Background: Children with special healthcare needs (CSHCN) require more support than the average of their peers. Support systems for CSHCN were particularly affected by pandemic control measures. Perceived social support is a resource for health and wellbeing for CSHCN and their families. Associations of social support, mental health and socioeconomic status (SES) have been described. This study aims to (1) assess perceived social support in families with and without CSHCN; (2) describe structure and types of social networks of families with and without CSHCN; and (3) explore associations between perceived social support, disease complexity, child and caregiver mental health, and SES.
Methods: This is the third of a sequential series of cross-sectional online surveys conducted among caregivers of children ≤ 18 years in Germany since the beginning of the COVID-19 pandemic, administered between 1st December 2022 and 10 March 2023. The Brief Social Support Scale (BS6) assessed perceived social support. Child and parental mental health were assessed using the Strengths and Difficulties Questionnaire (SDQ) and WHO-5 Wellbeing index. The CSHCN-Screener identified CSHCN. Descriptive statistics and linear regression modeling assessed associations between perceived social support, parent-reported child mental health problems, disease complexity, caregiver mental wellbeing and SES.
Results: The final sample included 381 participants, among them 76.6% (n = 292) CSHCN. 46.2% (n = 176) of caregivers reported moderate, i.e., at least occasional social support. Social support was largely provided by informal social networks consisting of partners, relatives and neighbors/friends. Linear regression modeling revealed associations of lower perceived social support with higher disease complexity of the child, lower caregiver mental wellbeing, lower SES and increasing caregiver age.
Conclusion: The results of this study describe inequalities in perceived social support according to disease complexity of the child, caregiver mental health and socioeconomic status. They highlight the importance of social support and support networks as a resource for wellbeing of caregivers and CSHCN. Moving on from the COVID-19 pandemic, recovery strategies should focus on low-threshold interventions based in the community to improve social support for families with CSHCN and actively involve caregivers in identifying needs and co-creating new approaches.
1 Introduction
Children with special healthcare needs (CSHCN) have chronic health conditions which require more support than the average of their peers (1). Their families face multiple demands relating to the physical and mental wellbeing of the affected child, management of limited resources and to family functioning (2, 3). As a result, caregivers of CSHCN are more likely to be affected by low levels of mental wellbeing, increased levels of stress, financial difficulties, social isolation and difficulties in accessing community resources (2–4). A growing body of research highlights the complex and multi-faceted impact of the COVID-19 pandemic on families with CSHCN. Suspension or reduction in frequency of health care services provision led to an increase in care responsibilities with parents trying to maintain therapies and surveilling their child’s health status at home. Rehabilitation services for CSHCN are often school-based, and thus school closures affected these children’s access not only to education, but also to therapies crucial for their physical health. In addition, respite services as a source of short-term relief to families with CSHCN were mostly suspended (5–7). Social distancing measures led to a loss of family and social support networks. As a result, worsening caregiver and child mental health, increasing stress and financial insecurities due to job loss or part-time work have been reported (3, 4, 8–10).
The first case of COVID-19 in Germany was reported on 27 January 2020. The first national lockdown lasted from 22nd March until 4 May 2020, followed by periods of stronger restrictions and distancing measures such as nightly curfews in November 2020 to January 2021, April 2021, and December 2021 to February 2022. Schools closed completely from about the middle of March until 4 May 2020 and patterns of (partial) reopening mostly coincided with periods of easing pandemic control measures; precise dates of school closure varied slightly by federal state. All pandemic measures were lifted by February 2023 (11).
Social support is a widely acknowledged resource for health and wellbeing, and an important coping resource for families with CSHCN in particular. Social support can arise both from social contacts and social networks and perceived social support may be as important as actual support provided (2, 12). Different conceptualizations of social support exist. Functional support describes the extent to which relationships serve particular functions and provide resources. It can be further categorized as tangible support (e.g., practical help, financial support); emotional support (e.g., empathy, companionship); appraisal support (e.g., help in decision-making processes) and informational support (e.g., provision of advice or information relating to particular needs). Structural support describes size and types of social networks, frequency of contacts and existence of relationships (13–15).
To our knowledge, there has been limited research focusing on social support of families with CSHCN during the COVID-19 pandemic. A Brazilian study highlights the relevance of perceived social support for quality of life, caregiver burden and stress of caregivers of CSHCN, but no differences in perceived social support between families with and without CSHCN during the COVID-19 pandemic were found (16). In our previous two surveys among families with and without CSHCN in Germany during the COVID-19 pandemic we described associations of parent-reported child mental health problems with increasing disease complexity of the child, low caregiver mental wellbeing, low SES, and inadequate social support reported by caregivers (17, 18).
The importance of social support in this context is further emphasized by the potential long-term impact of the COVID-19 pandemic on CSHCN due to persisting unequal access to treatment (e.g., financial barriers in accessing telehealth), associated poor health outcomes such as developmental delays or delays in diagnosis and treatment, and dependence on multidisciplinary support. These indirect impacts of the pandemic in turn increase the vulnerability of an already particularly vulnerable group leading to calls that “inequities and prior disadvantage […] [be] addressed in current policies regarding the recovery of healthcare services” (19) (p. 18).
Based on the findings outlined above, the goal of our study in a phase of pandemic recovery is to examine dimensions of social support and support networks of families with and without CSHCN with a focus on implications for health and care service provision post COVID-19. In particular, this study aims to
1. Assess perceived social support in families with and without CSHCN.
2. Describe structure and types of social networks of families with and without CSHCN.
3. Explore associations between perceived social support, disease complexity, child and caregiver mental health, and socioeconomic status (SES).
2 Methods
2.1 Study design
This study is the third of a sequential series of cross-sectional online surveys since the onset of the pandemic: the first survey was conducted from August–October 2020 (18), the second from December 2020–March 2021 (17). This third survey was initiated in December 2022 when most pandemic restrictions and social distancing measures in Germany had been relaxed or abolished. It was administered via REDcap©, an online survey platform, between 1st December 2022 and 10 March 2023.
Caregivers of children ≤ 18 years who gave informed consent were included in the study. Participants were recruited through convenience and non-probabilistic snowball sampling, study promotion via partner organizations, social and public media, and through free access websites. Representatives of the Kindernetzwerk e.V., a large German patient organization for families with children with chronic disease and disabilities, were involved in the survey design, study promotion and disseminated study results to their members through newsletters and free access websites. The study is registered with the German Registry for Clinical Studies (DRKS00022868). Ethics approval was granted by the ethics committee of Freiburg University (Approval number 377/20).
2.2 Measures
2.2.1 Brief Social Support Scale (BS6)
The Brief Social Support Scale (BS6) is a bi-factorial questionnaire assessing overall perceived social support as well as both emotional-informational and tangible support. It was developed based on the MOS Social support survey (20). Three items assess tangible and emotional-informational support, respectively, on a 4-point Likert Scale. A sum score for perceived social support ranging from 6 to 24 can be calculated as well as sum scores for each of the two subscales ranging from 3 to 12. The authors suggest a stratification of the overall score of perceived social support into low (6–11), moderate (12–17; at least occasional support), high (18–23; at least mostly supported) and very high (24; always supported). The BS6 was validated in a population-based sample of 15,010 participants in an existing German cohort study and showed good reliability with Cronbach’s alpha α = 0.86 for overall perceived social support (20). For the purpose of this study, the wording of the items on the tangible support scale was slightly adapted to be suitable to the situation of families with children.
2.2.2 Social support networks
Drawing on an assessment of support networks for families in pediatric oncology included in the Psychosocial Assessment Tool (PAT) (21, 22), six items eliciting support networks for tangible, informational, appraisal and emotional support were developed. For each area of support, participants were asked who provided this kind of support. Multiple answers were possible. Response options included both informal support provided by partners, grandparents or relatives, neighbors or friends; and formal support provided by volunteers, family support services, home care services or others.
Unmet support needs were assessed by seven newly developed items which were created in a collaborative process together with representatives of the patient organization Kindernetzwerk e.V. Each item mentioned a potential area of unmet support, e.g., “Everyday tasks in the household” and participants were asked whether they agreed, disagreed or if the item did not apply.
2.2.3 Socioeconomic status
As outlined in the National Health Interview and Examination Survey for Children and Adolescents (KiGGS) in Germany (23), an index measuring SES was constructed as the sum of three indicators: household net equivalent income, parental education and parental occupation. Household net equivalent income was calculated as the monthly net family income adjusted for household size using a modified scale proposed by the Organisation for Economic Cooperation and Development (OECD) (23). Weights were assigned to the household head (=1), any additional adult living in the same household (=0.5) and children (=0.3). The monthly net family income was divided by the sum of weights per household. For parental education and occupation, the respective higher level of each parent was assigned to each household. Each of the three dimensions of the SES index takes values of 1–7 and the final SES index ranges from 3 to 21, with lower values indicating a lower socioeconomic status.
2.2.4 Children with special health care needs
The Children with Special Healthcare Needs Screener (CSHCN Screener) is a five-item parent-reported screening instrument which aims to identify children with chronic physical, mental, behavioral or other conditions who require more health and related services than the average of their peers (1). Higher scores indicate higher disease complexity and healthcare needs (24). We stratified children into three groups (25): no special healthcare needs (CSHCN score = 0), chronic conditions (CSHCN score ≤ 2) and complex chronic conditions (CSHCN score ≥ 3) (24).
2.2.5 Strengths and Difficulties Questionnaire (SDQ)
The Strengths and Difficulties Questionnaire (SDQ) is an established and validated screening instrument for mental health problems in children and adolescents. It relates to child or adolescent behavior during the previous 6 months. The standard parent-reported version of the SDQ applies to children aged 4–16 years, with a preschool version differing in three items (26, 27). The Total Difficulties score covers four subscales (hyperactivity/inattention, emotional symptoms, conduct problems, peer problems) and ranges from 0 to 40, with higher scores indicating more serious mental health problems. Both the German standard parent-report version and the preschool version are valid and reliable instruments (28, 29). We used age-appropriate versions of the SDQ for caregivers of children older than 2 years and a cut-off of 13 or higher on the Total Difficulties Score (30, 31).
2.2.6 WHO-5 Wellbeing Index
The WHO-5 Wellbeing Index (WHO-5) is a 5-question screening tool for mental health with good validity and reliability (32). The final score ranges between 0 and 100, with 100 representing the best imaginable mental wellbeing. The cut-off point for depression screening is 50 (32).
2.2.7 Sociodemographic measures
Included age and gender, relationship status, education, occupation, monthly household income, household size, area of residence and country of birth. Caregiver education was categorized according to the international CASMIN classification (33).
2.3 Statistical methods
Participants with no more than three missing values in any of the following key variables were included in the analysis: BS6 total score, SDQ total score, WHO-5 total score, CSHCN Screener score and SES variables (monthly household income, occupation and education). Missing values for household net income (10.6%) were replaced by multiple imputation. Analyses involving the SDQ were restricted to children older than 2 years of age. Descriptive statistics comprised frequencies for social support network structures, comparisons of means for BS6 total score between families with and without CSHCN by independent t-tests and by Chi-Square test for the stratified BS6 total score. Homogeneity of variance was assessed by Levene’s Test for Equality of Variances. Simple linear regression modeling was performed for BS6 total score on CSHCN total score.
Multiple linear regression modeling was performed on complete datasets (n = 327; 86% of total sample size) to assess associations of perceived social support (BS6 total score) with disease complexity, child mental health, caregiver mental health and SES. Analyses were adjusted for age and gender. Sensitivity analyses were performed for tangible and emotional-informational support subscales, respectively. Multicollinearity between exposure variables was assessed by calculating the variance inflation factor (VIF). Analysis was performed using IBM SPSS Version 27.0.
3 Results
3.1 Sociodemographic characteristics
Of 478 persons accessing the survey, 425 fulfilled the inclusion criteria. Among these, 381 met the criteria for missing data in key variables as outlined above and were thus included in the final sample. Participants were mostly female, lived with their partner in the same household and had on average two children. Of all participants, 39.4% had already participated in the first and second round of this sequential survey. Further sociodemographic characteristics are displayed in Table 1.
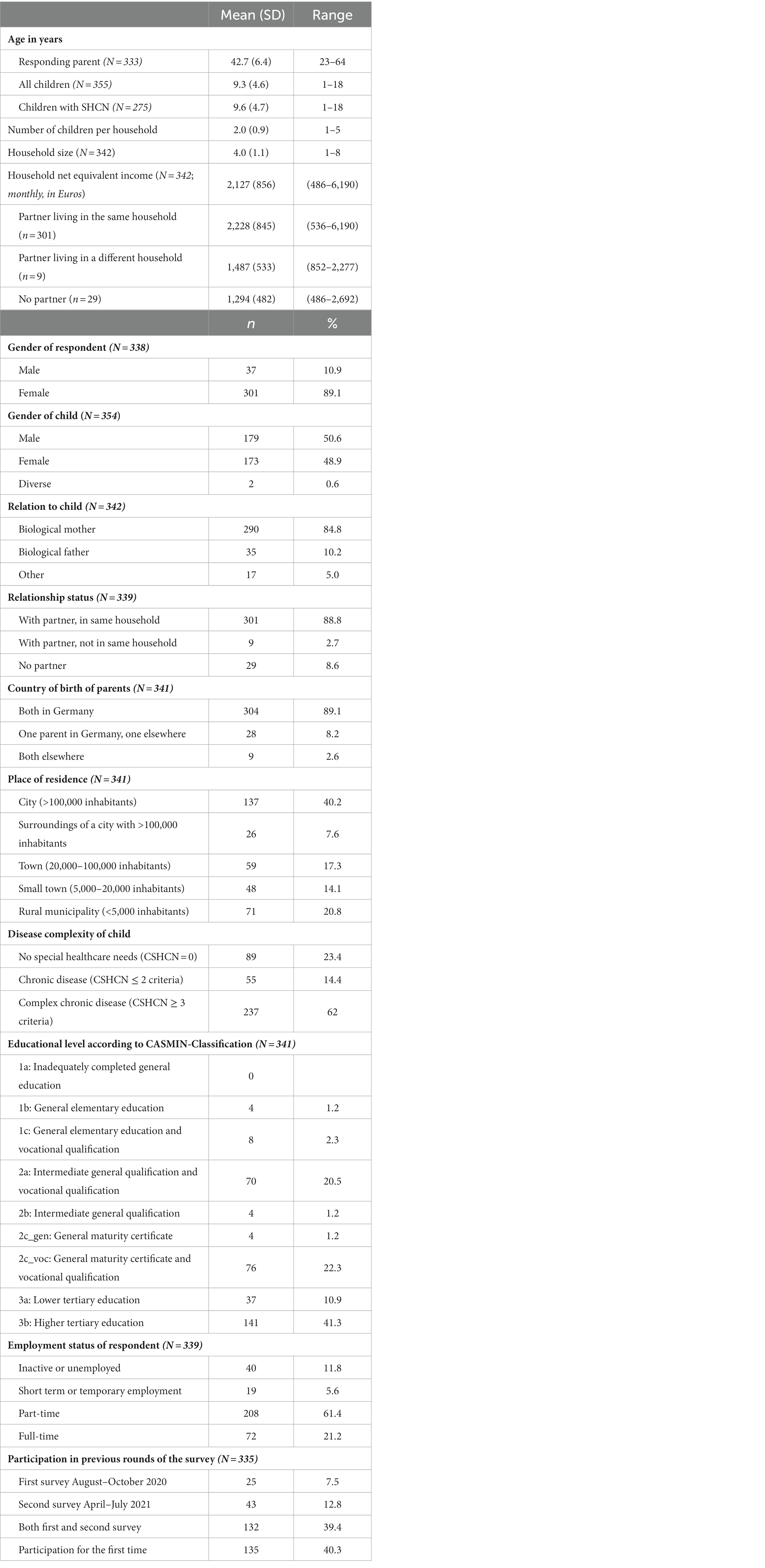
Table 1. Sociodemographic characteristics (N = 381).
Among all children, 76.6% (n = 292) had special healthcare needs. Of these, 78.8% (n = 230) had a physical impairment, 73.6% (n = 215) a behavioral or sensory impairment and 55.1% (n = 161) had impaired speech or understanding.
3.2 Perceived social support
The mean score for perceived social support was 13.4 (SD 4.1) for the total score, 5.7 (SD 2.2) and 7.8 (SD 2.6) for tangible and emotional-informational subscales, respectively. Stratification of the total score revealed that 46.2% (n = 176) of caregivers reported moderate, i.e., at least occasional social support (Table 2). There was strong evidence that caregivers of CSHCN (12.7; SD 3.8) perceived lower social support than caregivers without CSHCN (16.0; SD 3.8) (t[379] = 7.16, p < 0.001) with a difference of 3.3 points on the BS6 scale (95% CI 2.4; 4.2). When stratifying the total social support score, 44.5% (n = 130) caregivers of CSHCN reported low perceived social support compared to 9.0% (n = 8) caregivers of children without SHCN (χ2[df = 2] = 39.78, p < 0.001; Table 2).
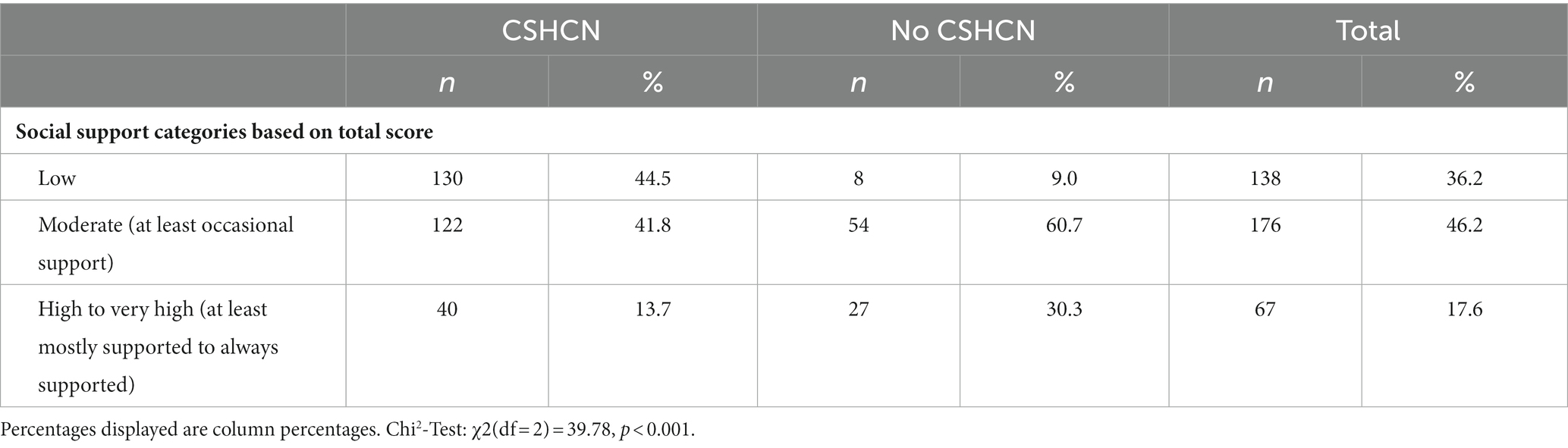
Table 2. Perceived social support (Brief Social Support Scale BS6, N = 381).
Simple linear regression showed strong evidence for an association between perceived social support and disease complexity. BS6 total scores decreased with increasing CSHCN total score (Supplementary Table S1).
3.3 Support networks
Results are displayed in Supplementary Table S2. Among all participants, support by a partner constituted the largest share of support provided for all items. In addition, grandparents or relatives mostly supported everyday childcare and childcare during holidays. Neighbors or friends were important sources of emotional and informational support or advice. Formal support provided by family support services or home care services only constituted a small share in the whole study population. Among families with CSHCN, family support services and home care services provided between 3.8% and 4.9% of support in childcare, everyday tasks and informational support compared to none for families without CSHCN (Figures 1, 2; Supplementary Tables S3, S4). However, support networks of both families with and without CSHCN were largely informal with support provided by a partner, grandparents or relatives and neighbors or friends.
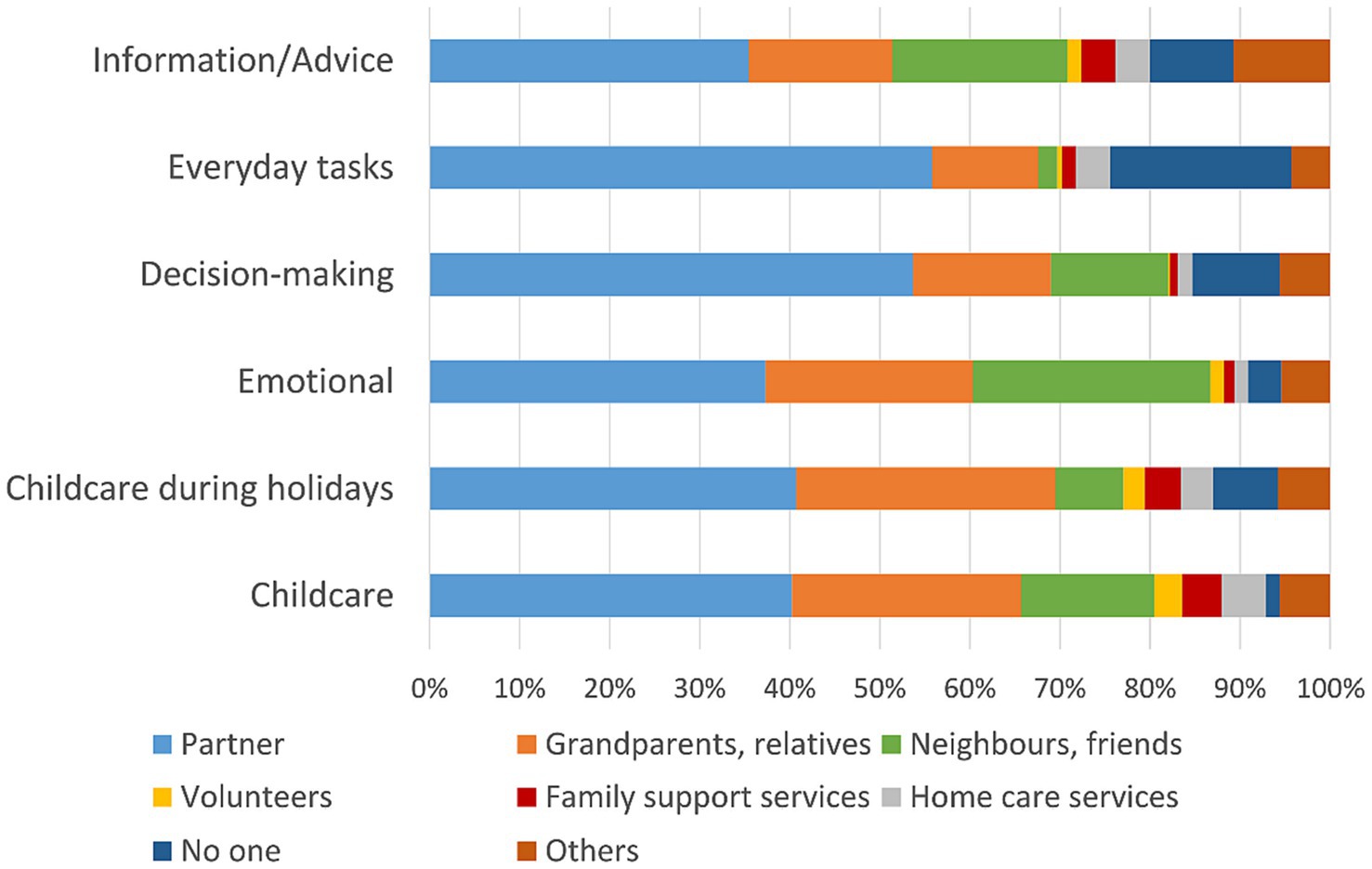
Figure 1. Support networks of families with CSHCN.
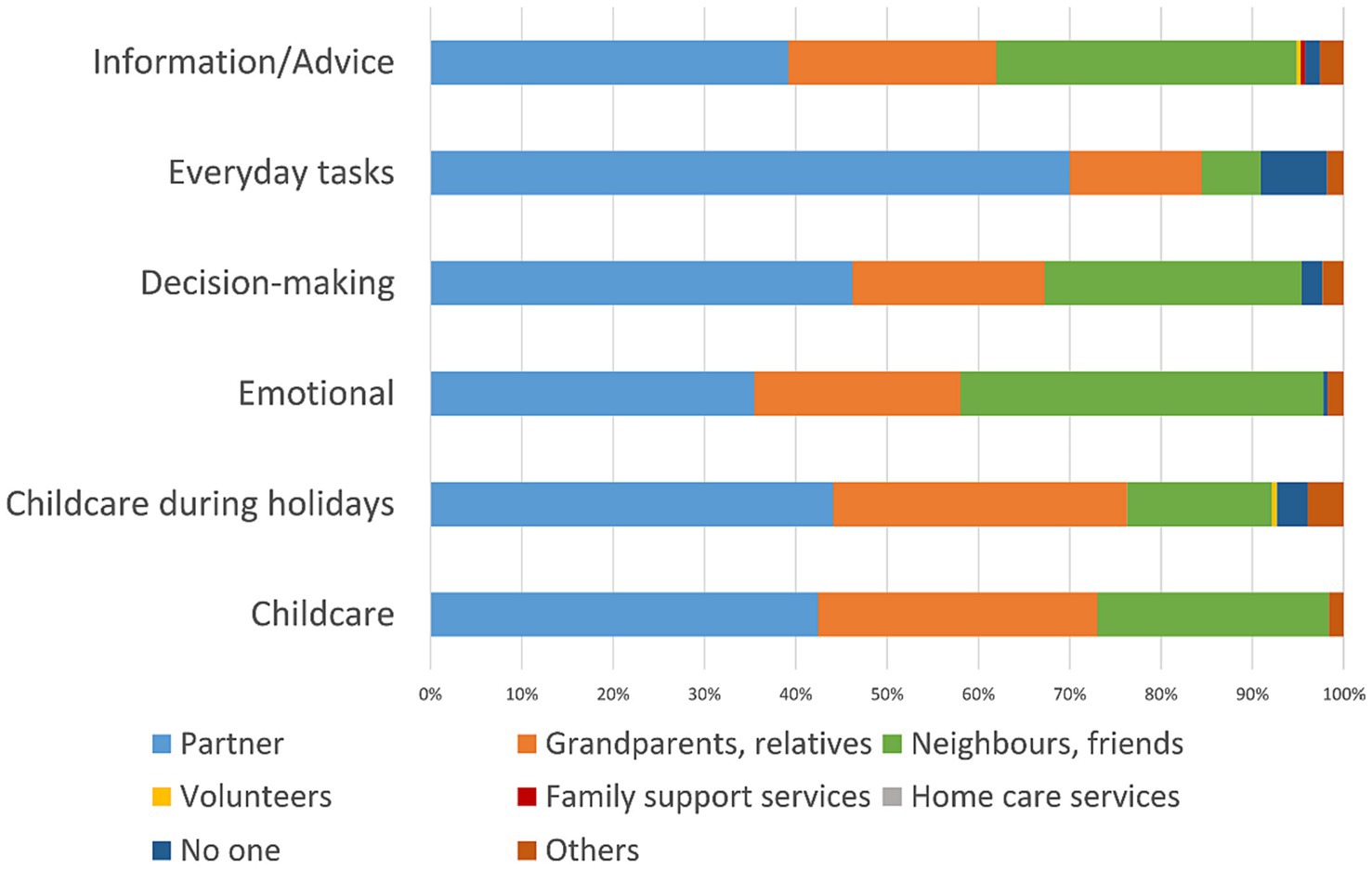
Figure 2. Support networks of families without CSHCN.
Table 3 shows areas of unmet support needs of families with CSHCN. Support needs were highest for childcare outside school or nursery opening times (61%), everyday tasks in the household (60.1%) and support of the child in nursery or school (59.9%). Support needs were lowest for nursing or caring for a child with special healthcare needs, however this was still a relevant unmet need for more than one third of parents (36.4%). Stratified analysis revealed strong evidence for higher unmet needs among families with children with complex chronic disease compared to families with children with chronic disease for all items but financial support (results not displayed).
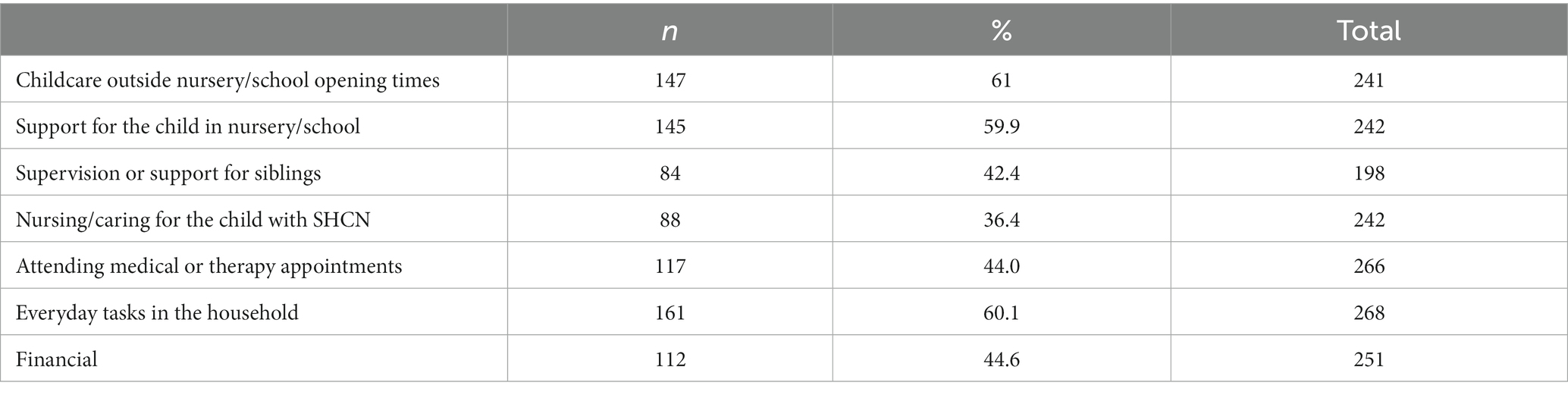
Table 3. Areas of unmet support needs of families with CSHCN.
3.4 Associations of perceived social support, disease complexity, child and caregiver mental health, and socioeconomic status
Results of the multiple linear regression modeling are displayed in Table 4. There was strong evidence of an association of perceived social support as measured by the BS6 total score, disease complexity, caregiver mental health, SES and age of caregiver. Perceived social support decreased with increasing disease complexity (CSHCN total score), decreasing caregiver mental wellbeing (WHO-5 score), decreasing SES and increasing caregiver age. After controlling for confounding effects of age, gender and disease complexity, there was no evidence of an association of perceived social support and parent-reported child mental health problems as measured by the SDQ total score. Overall, the model explained 22% of variance in perceived social support.
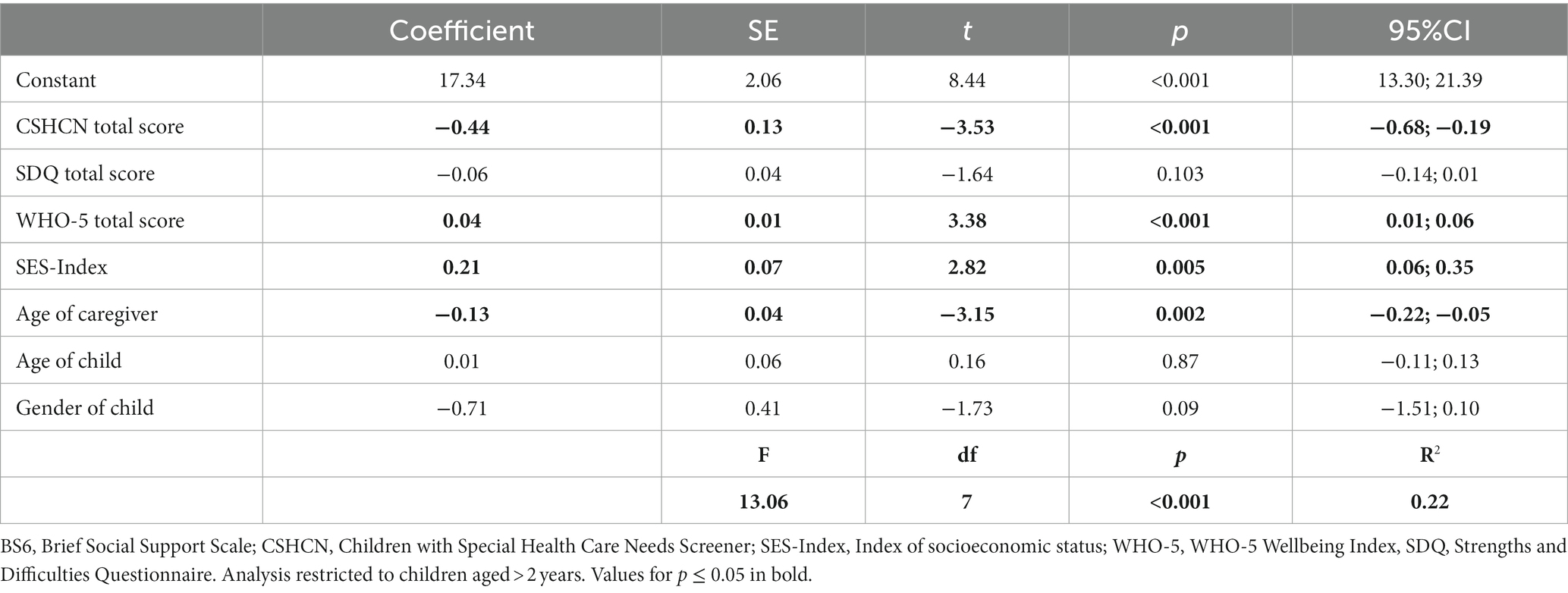
Table 4. Multiple linear regression modeling of BS6 total score on CSHCN total score, SDQ, WHO-5 and SES-Index (N = 327).
Sensitivity analyses were performed for perceived tangible and emotional-informational support, respectively (Table 5). For perceived tangible support, there was strong evidence of an association with disease complexity, SES and caregiver age. Regarding perceived emotional-informational support, there was strong evidence for an association with disease complexity, caregiver mental health and caregiver age.
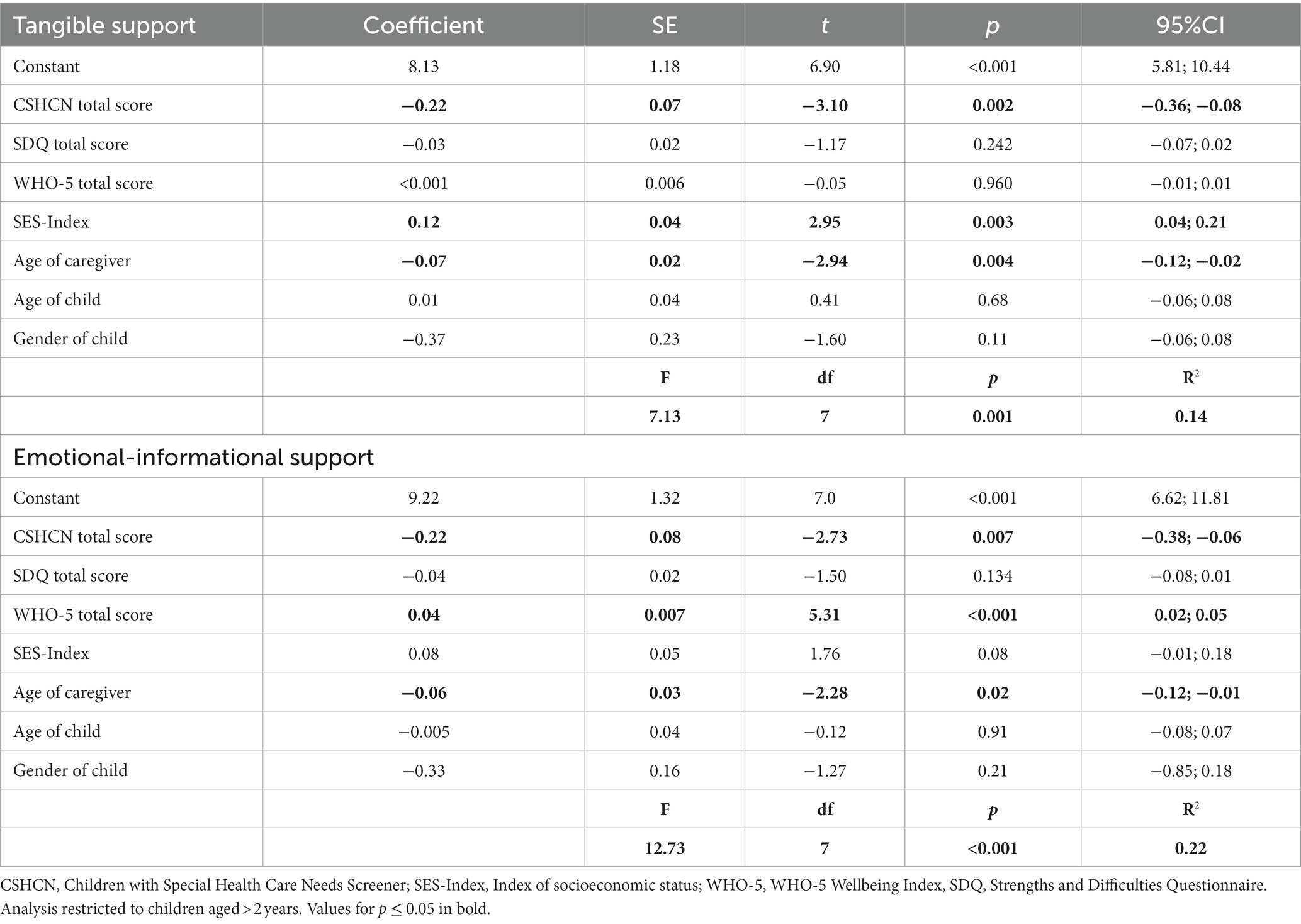
Table 5. Multiple linear regression modeling for tangible and emotional-informational support subscales (N = 327).
There was no evidence for multicollinearity between independent variables included in the regression modeling.
4 Discussion
This study reports low to moderate levels of perceived social support in a sample of 381 families with and without CSHCN in Germany following the COVID-19 pandemic. Lower perceived social support was associated with higher disease complexity of the child, lower caregiver mental wellbeing, lower SES and increasing caregiver age. Social support was largely provided by informal social networks consisting of partners, relatives and neighbors or friends.
Perceived social support was lower in caregivers of CSHCN and associated with disease complexity of the child. Families of CSHCN face multiple responsibilities related to their child’s complex medical and psychosocial needs, and particularly rely on broad support networks (2). Studies conducted during the COVID-19 pandemic report a disintegration of family, peer and community support networks of caregivers of CSHCN (10, 34, 35). Caregivers of children with complex chronic disease were additionally affected by a lack of respite often provided through these networks (4, 9, 10, 35). However, a Brazilian study conducted during the first year of the pandemic did not find a difference in perceived social support between caregivers of children with and without developmental disabilities. The authors concluded that this was most likely due to social support being less available for everyone as pandemic restrictions affected all families (16). Barriers in accessing community support for families with CSHCN have been described prior to the COVID-19 pandemic (3). It remains open whether our results still reflect the impact of the pandemic years on perceived social support of caregivers of CSHCN and future studies are thus needed as we move beyond pandemic recovery.
In addition to the association of perceived social support and disease complexity, our study demonstrates that perceived social support decreased with lower caregiver mental wellbeing and lower SES. Financial stress and low SES have been described as associated with lower levels of perceived social support in adult populations (12, 20). Families with CSHCN are particularly at risk of financial difficulties due to part-time work and resulting income loss, and an association of chronic disease and disability with low SES has been widely described (3, 18, 36). It is crucial that efforts to strengthen social support focus on this vulnerable group and aim to remove barriers to accessing support systems.
Higher levels of psychological distress and mental health problems during the pandemic compared to pre-pandemic data have been reported for mothers in particular (17, 18, 37–39). Higher levels of depression in caregivers of CSHCN during the COVID-19 pandemic have been described for younger age, those being single or living alone, which might in addition point toward the importance of social support for caregiver mental wellbeing (40). However, our results indicated that decreasing perceived social support was associated not only with decreasing caregiver mental wellbeing but also with increasing caregiver age. This is contrary to results reported in a general population sample showing no relationship between perceived social support and age (20). Our finding may suggest that younger caregivers were better able to access social support during the COVID-19 pandemic, which warrants further exploration.
For families with and without CSHCN, social support constitutes a resource for lowering caregiver’s psychological distress and higher levels of emotional support showed positive effects on caregiver wellbeing (41). According to Wade et al., caregiver wellbeing is the central element in a family stress model and positively impacts children via changes in family processes, structure and organization (39). The most recent results of the representative German longitudinal COPSY study on youth mental health during the pandemic similarly describes a 4–14 times higher chance of better mental health outcomes in children with high social and family support (42). Accordingly, strengthening social support for families with and without CSHCN is an important mechanism for achieving both caregiver and child wellbeing.
In our study population, families largely relied on informal support networks. For families with CSHCN this might still be a reflection on reduced access to formal support services during the pandemic (8). However, those results highlight the importance of strengthening informal social support networks and increasing the availability of low-threshold support systems. Peer support interventions have the potential to act as egalitarian interventions without a power imbalance of the kind that exists, for example, between a formal service provider and the recipient. A recent Cochrane review on peer interventions for parents and carers of children with complex needs by Sartore et al. did not find clear evidence of an effect of the interventions on caregiver outcomes (2). However, this was mostly due to poor quality and heterogeneity of available studies. The authors still concluded that peer support might be equally effective as more intensive, standard interventions such as psychoeducation and stress management. Community health approaches such as neighborhood support programs can support families with CSHCN in everyday household tasks, attending medical appointments or providing childcare after school. Given that these programs are a valuable resource, patient organizations in Germany demand that they be strengthened (43). Further promising approaches include family guides for accessing community based social support and care coordination to enhance integration of medical and community-based supports for CSHCN (44, 45).
5 Limitations
The results of this study are limited by its design and recruitment process. The cross-sectional design does not allow inference of causality in the associations between social support, disease complexity, mental health and SES. Furthermore, the non-representative nature of the sample limits the generalizability of our study results. The recruitment process is likely to have encouraged a self-selection of participants, resulting in a sample with a high educational level. Participants from lower educational and occupational levels, those from a minority or ethnic background and families without CSHCN are underrepresented. Also, the survey delivery online might have excluded those from a low SES who lacked appropriate technology to access the survey. Associations described between perceived social support and low SES might thus still be underestimated. Similarly, differences in perceived social support between families with and without CSHCN might be either over- or underestimated.
6 Conclusion
The results presented here highlight the importance of social support and support networks as a resource for wellbeing of caregivers and children with special healthcare needs. Following the COVID-19 pandemic, we describe marked inequalities in perceived social support according to disease complexity, caregiver mental health and socioeconomic status. Recovery strategies and healthcare reform should focus on low-threshold interventions based in the community to improve social support for families with CSHCN, and actively involve caregivers in identifying needs and co-creating new approaches.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Freiburg University (Approval number 377/20). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. MB: Conceptualization, Writing – review & editing. AH: Conceptualization, Methodology, Supervision, Writing – review & editing. HH: Resources, Writing – review & editing. SI: Data curation, Writing – review & editing. AM: Resources, Writing – review & editing. TL: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Volkswagen Foundation, grant number Az 990622. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Acknowledgments
The authors would like to thank Kathrin Jackel-Neusser and other members of the steering committee of the Kindernetzwerk e.V. for their support in the recruitment process and their valuable contributions to the survey development.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1322185/full#supplementary-material
References
1. Bethell, CD, Read, D, Stein, REK, Blumberg, SJ, Wells, N, and Newacheck, PW. Identifying children with special health care needs: development and evaluation of a short screening instrument. Ambul Pediatr. (2002) 2:38–48. doi: 10.1367/1539-4409(2002)002<0038:ICWSHC>2.0.CO;2
2. Sartore, GM, Pourliakas, A, and Lagioia, V. Peer support interventions for parents and carers of children with complex needs. Cochrane Database Syst Rev. (2021) 2021:CD010618. doi: 10.1002/14651858.CD010618.pub2
3. Smiley, Y, Silberholz, E, Bekele, ES, and Brodie, N. Caregiver stress and social determinants of health in key populations: immigrant parents, parents of children with medical complexity, and adolescent parents. Curr Opin Pediatr. (2022) 34:521–30. doi: 10.1097/MOP.0000000000001163
4. Fortin-Bédard, N, Ladry, NJ, Routhier, F, Lettre, J, Bouchard, D, Ouellet, B, et al. Being a parent of children with disabilities during the COVID-19 pandemic: multi-method study of health, social life, and occupational situation. Int J Environ Res Public Health. (2023) 20:3110. doi: 10.3390/ijerph20043110
5. Michaud, M, and Dietz, IC. The effects of the SARS-CoV-2 pandemic on children and youth with special health care needs. Front Pediatr. (2023) 10:70. doi: 10.3389/fped.2022.1007770
6. Diskin, C, Buchanan, F, Cohen, E, Dewan, T, Diaczun, T, Gordon, M, et al. The impact of the COVID-19 pandemic on children with medical complexity. BMC Pediatr. (2022) 22:496. doi: 10.1186/s12887-022-03549-y
7. Cohen, SS, Toly, VB, Lerret, SM, and Sawin, KJ. The impact of COVID-19 on Systems of Care for children and youth with special health care needs. J Pediatr Health Care. (2023) 37:106–16. doi: 10.1016/j.pedhc.2022.09.009
8. Merrick, H, Driver, H, Main, C, Kenny, RPW, Richmond, C, Allard, A, et al. Impacts of health care service changes implemented due to COVID-19 on children and young people with long-term disability: a mapping review. Dev Med Child Neurol. (2023) 65:885–99. doi: 10.1111/dmcn.15503
9. Arichi, T, Cadwgan, J, McDonald, A, Patel, A, Turner, S, Barkey, S, et al. Neurodisability care in the time of COVID-19. Child Care Health Dev. (2022) 48:901–5. doi: 10.1111/cch.13015
10. Cadwgan, J, Goodwin, J, Arichi, T, Patel, A, Turner, S, Barkey, S, et al. Care in COVID: a qualitative analysis of the impact of COVID-19 on the health and care of children and young people with severe physical neurodisability and their families. Child Care Health Dev. (2022) 48:924–34. doi: 10.1111/cch.12925
11. Tagesschau.de. Drei Jahre Pandemie: Als plötzlich nichts mehr normal war. (2023). Available at: https://www.tagesschau.de/inland/gesellschaft/corona-pandemie-rueckblick-101.html (Accessed 26 January 2024).
12. Borgmann, LS, Rattay, P, and Lampert, T. Social support as a health resource in Germany. J Health Monit. (2017) 2:110–5. doi: 10.17886/RKI-GBE-2017-131
13. Kocalevent, RD, Berg, L, Beutel, ME, Hinz, A, Zenger, M, Härter, M, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. (2018) 6:31. doi: 10.1186/s40359-018-0249-9
14. Cohen, S, and Wills, TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
15. Berkman, LF, Glass, T, Brissette, I, and Seeman, TE. From social integration to health: Durkheim in the new millennium. Soc Sci Med. (2000) 51:843–57. doi: 10.1016/S0277-9536(00)00065-4
16. Da Costa, IGR, Brugnaro, BH, Lima, CRG, Kraus de Camargo, O, Fumincelli, L, Pavão, SL, et al. Perceived social support and quality of life of children with and without developmental disabilities and their caregivers during the COVID-19 pandemic in Brazil: a cross-sectional study. Int J Environ Res Public Health. (2023) 20:4449. doi: 10.3390/ijerph20054449
17. Geweniger, A, Haddad, A, Barth, M, Högl, H, Mund, A, Insan, S, et al. Mental health of children with and without special healthcare needs and of their caregivers during COVID-19: a cross-sectional study. BMJ Paediatr Open. (2022) 6:1–9. doi: 10.1136/bmjpo-2022-001509
18. Geweniger, A, Barth, M, Haddad, AD, Högl, H, Insan, S, Mund, A, et al. Impact of the COVID-19 pandemic on mental health outcomes of healthy children, children with special health care needs and their caregivers – results of a cross-sectional study. Front Pediatr. (2022) 10:1–11. doi: 10.3389/fped.2022.759066
19. Lignou, S, and Sheehan, M. Children with medical complexities: their distinct vulnerability in health systems’ Covid-19 response and their claims of justice in the recovery phase. Med Health Care Philos. (2023) 26:13–20. doi: 10.1007/s11019-022-10119-7
20. Beutel, ME, Brähler, E, Wiltink, J, Michal, M, Klein, EM, Jünger, C, et al. Emotional and tangible social support in a German population-based sample: development and validation of the brief social support scale (BS6). PLoS One. (2017) 12:e0186516. doi: 10.1371/journal.pone.0186516
21. Kazak, AE, Hwang, WT, Fang Chen, F, Askins, MA, Carlson, O, Argueta-Ortiz, F, et al. Screening for family psychosocial risk in pediatric cancer: validation of the psychosocial assessment tool (PAT) version 3. J Pediatr Psychol. (2018) 43:737–48. doi: 10.1093/jpepsy/jsy012
22. Pai, ALH, Patiño-Fernández, AM, McSherry, M, Beele, D, Alderfer, MA, Reilly, AT, et al. The psychosocial assessment tool (PAT2.0): psychometric properties of a screener for psychosocial distress in families of children newly diagnosed with cancer. J Pediatr Psychol. (2008) 33:50–62. doi: 10.1093/jpepsy/jsm053
23. Lampert, T, Hoebel, J, Kuntz, B, Müters, S, and Kroll, LE. Messung des sozioökonomischen Status und des subjektiven sozialen Status in KiGGS Welle 2. J Health Monit. (2018) 3:114–33. doi: 10.17886/RKI-GBE-2018-016
24. Bethell, CD, Blumberg, SJ, Stein, REK, Strickland, B, Robertson, J, and Newacheck, PW. Taking stock of the CSHCN screener: a review of common questions and current reflections. Acad Pediatr. (2015) 15:165–76. doi: 10.1016/j.acap.2014.10.003
25. Matiz, LA, Robbins-Milne, L, and Rausch, JA. EMR adaptations to support the identification and risk stratification of children with special health care needs in the medical home. Matern Child Health J. (2019) 23:919–24. doi: 10.1007/s10995-018-02718-9
26. Goodman, R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry Allied Discip. (1997) 38:581–6. doi: 10.1111/j.1469-7610.1997.tb01545.x
27. Croft, S, Stride, C, Maughan, B, and Rowe, R. Validity of the strengths and difficulties questionnaire in preschool-aged children. Pediatrics. (2015) 135:e1210–9. doi: 10.1542/peds.2014-2920
28. Klein, AM, Otto, Y, Fuchs, S, Zenger, M, and Von Klitzing, K. Psychometric properties of the parent-rated SDQ in preschoolers. Eur J Psychol Assess. (2013) 29:96–104. doi: 10.1027/1015-5759/a000129
29. Woerner, W, Becker, A, and Rothenberger, A. Normative data and scale properties of the German parent SDQ. Eur Child Adolesc Psychiatry. (2004) 13:II3–10. doi: 10.1007/s00787-004-2002-6
30. Kuntz, B, Rattay, P, Poethko-Müller, C, Thamm, R, Hölling, H, et al. Soziale Unterschiede im Gesundheitszustand von Kindern und Jugendlichen in Deutschland – Querschnittergebnisse aus KiGGS Welle 2. Health Monit. (2018) 3:9–36.
31. Rothenberger, A, Becker, A, Erhart, M, Wille, N, and Ravens-Sieberer, U. Psychometric properties of the parent strengths and difficulties questionnaire in the general population of German children and adolescents: results of the BELLA study. Eur Child Adolesc Psychiatry. (2008) 17:99–105. doi: 10.1007/s00787-008-1011-2
32. Winther Topp, C, Østergaard, SD, Søndergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
33. Brauns, H, and Steinmann, S. Educational reform in France, West-Germany and the United Kingdom: updating the CASMIN educational classification. ZUMA Nachrichten. (1999) 23:7–44.
34. McLoone, J, Wakefield, CE, Marshall, GM, Pierce, K, Jaffe, A, Bye, A, et al. It’s made a really hard situation even more difficult: the impact of COVID-19 on families of children with chronic illness. PLoS One. (2022) 17:e0273622. doi: 10.1371/journal.pone.0273622
35. Currie, G, Finlay, B, Seth, A, Roth, C, Elsabbagh, M, Hudon, A, et al. Mental health challenges during COVID-19: perspectives from parents with children with neurodevelopmental disabilities. Int J Qual Stud Health Well-Being. (2022) 17:6090. doi: 10.1080/17482631.2022.2136090
36. Spencer, NJ, Blackburn, CM, and Read, JM. Disabling chronic conditions in childhood and socioeconomic disadvantage: a systematic review and meta-analyses of observational studies. BMJ Open. (2015) 5:e007062. doi: 10.1136/bmjopen-2014-007062
37. Racine, N, Hetherington, E, McArthur, BA, McDonald, S, Edwards, S, Tough, S, et al. Maternal depressive and anxiety symptoms before and during the COVID-19 pandemic in Canada: a longitudinal analysis. Lancet Psychiatry. (2021) 8:405–15. doi: 10.1016/S2215-0366(21)00074-2
38. Dickerson, J, Kelly, B, Lockyer, B, Bridges, S, Cartwright, C, Willan, K, et al. When will this end? Will it end?’ The impact of the march-June 2020 UK COVID-19 lockdown response on mental health: a longitudinal survey of mothers in the born in Bradford study. BMJ Open. (2022) 12:e047748. doi: 10.1136/bmjopen-2020-047748
39. Wade, M, Prime, H, Johnson, D, May, SS, Jenkins, JM, and Browne, DT. The disparate impact of COVID-19 on the mental health of female and male caregivers. Soc Sci Med. (2021) 275:113801. doi: 10.1016/j.socscimed.2021.113801
40. Wauters, A, Vervoort, T, Dhondt, K, Soenens, B, Vansteenkiste, M, Morbée, S, et al. Mental health outcomes among parents of children with a chronic disease during the COVID-19 pandemic: the role of parental burn-out. J Pediatr Psychol. (2022) 47:420–31. PMID:34915562. doi: 10.1093/jpepsy/jsab129
41. Liu, S, Lombardi, J, and Fisher, PA. The COVID-19 pandemic impact on households of young children with special healthcare needs. J Pediatr Psychol. (2021) 47:158–70. doi: 10.1093/jpepsy/jsab135
42. Ravens-Sieberer, U, Devine, J, Napp, AK, Kaman, A, Saftig, L, Gilbert, M, et al. Three years into the pandemic: results of the longitudinal German COPSY study on youth mental health and health-related quality of life. Front Public Health. (2023) 11:1129073:73. doi: 10.3389/fpubh.2023.1129073
43. Kindernetzwerk. Der Berliner Appell (2023). Available at: https://www.kindernetzwerk.de/de/agenda/News/2023/Pressekonferenz-Der-Berliner-Appell.php
44. Currie, G, Materula, D, Gall, N, Lachuk, G, Richard, C, Yohemas, M, et al. Care coordination of children with neurodevelopmental disabilities and medical complexity during the COVID-19 pandemic: caregiver experiences. Child Care Health Dev. (2023) 49:834–45. doi: 10.1111/cch.13149
Keywords: social support, support networks, children with special healthcare needs, caregivers, pandemic, Covid-19, children with chronic disease, inequalities
Citation: Geweniger A, Barth M, Haddad A, Högl H, Insan S, Mund A and Langer T (2024) Perceived social support and characteristics of social networks of families with children with special healthcare needs following the COVID-19 pandemic. Front. Public Health. 12:1322185. doi: 10.3389/fpubh.2024.1322185
Edited by:
David Pérez-Jorge, University of La Laguna, SpainReviewed by:
Hannah Merrick, Newcastle University, United KingdomJose Luis Ramos Sanchez, Universidad de Extremadura, Spain
Copyright © 2024 Geweniger, Barth, Haddad, Högl, Insan, Mund and Langer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne Geweniger, YW5uZS5nZXdlbmlnZXJAdW5pa2xpbmlrLWZyZWlidXJnLmRl