 Marisa Lourenço
Marisa Lourenço Tânia Gomes2
Tânia Gomes2 Filipa Ventura
Filipa Ventura Rosa Silva
Rosa Silva- 1Nursing School of Porto, Center for Health Technology and Services Research (CINTESIS), Porto, Portugal
- 2Urology Department - Santo António University Hospital Center, Porto, Portugal
- 3The Health Sciences Research Unit: Nursing (UICISA: E), Nursing School of Coimbra, Coimbra, Portugal
- 4Centre for Evidence Based Practice: A JBI Centre of Excellence (PCEBP), Coimbra, Portugal
Introduction: Many of the essential practices in palliative care (PC) had to be adapted to the COVID-19 pandemic. This global spread of the infectious respiratory disease, caused by SARS-CoV-2, created unprecedented obstacles. The aim of this research was to comprehensively assess the experiences and perceptions of healthcare professionals, individuals, and families in palliative and end-of-life situations during the COVID-19 pandemic.
Methods: A scoping review was conducted using the databases CINAHL Complete, MEDLINE, Scopus, SciELO, Cochrane Central Register of Controlled Trials, Psychology and Behavioral Sciences, MEDIClatina, and Portugal’s Open Access Scientific Repository. The review followed the JBI® methodological approach for scoping reviews.
Results: Out of the initially identified 999 articles, 22 studies were included for analysis. The deprivation of relationships due to the safety protocols required to control the spread of COVID-19 was a universally perceived experience by healthcare professionals, individuals in PC, and their families. Social isolation, with significant psychological impact, including depersonalization and despair, was among the most frequently reported experiences by individuals in palliative situation. Despite healthcare professionals’ efforts to mitigate the lack of relationships, the families of these individuals emphasized the irreplaceability of in-person bedside contact.
Systematic review registration: https://osf.io/xmpf2/.
1 Introduction
Advancements in science and technology have contributed to an augmentation in life expectancy and the management of numerous severe pathologies, yielding substantial enhancements in the quality of life. Nevertheless, this extension of lifespan poses the challenge of contending with progressive and advanced chronic illnesses, frequently precipitating frailty and reliance on assistance for daily activities. Within this framework, palliative care (PC) assumes an exceedingly critical role, furnishing assistance not solely on a physical plane, but also addressing emotional and spiritual needs, thereby assisting in the preservation of dignity and quality of life until the final moments. The terminal phase of existence is characterized by the encounter with myriad losses across pivotal spheres of the human condition, spanning physical, psychological, social, and spiritual dimensions. This revelation further underscores the indispensability of PC as a requisite response to the intricacy and varied needs encountered by individuals at this juncture of life (1, 3).
PC services are comprehensive and holistic, delivered by specialized teams to individuals of all ages experiencing suffering due to incurable or severe illness, in advanced and progressive stages, as well as to their families. These services are offered across various healthcare settings. The primary objective of PC is to enhance well-being and quality of life by preventing and alleviating physical, psychological, social, and spiritual distress (4). A person in an end-of-life situation is considered to have an estimated prognosis of 12 months, while a person in a terminal phase is typically considered as having an expected prognosis of 3–6 months (4).
PC is a demanding form of care that combines science and humanism. It emphasizes early identification of the person’s needs, rigorous control of suffering and distress, and the promotion of autonomy, up to the last days of life. PC advocates for quality of life and dignity throughout the process of dying and in death (5). It is a global imperative for health and equity and is universally regarded as a basic human right (6). PC chooses active interventions in various dimensions of suffering to prevent it from becoming disruptive for the person in extreme end-of-life circumstances. It strives for person-centered care and support to the family, aiming to enhance life, optimize human well-being, and maximize the dignity of care (7).
PC practitioners establish their actions upon a model of technical and humanized approach to care, which is necessarily personalized and primarily rooted in four fundamental pillars: (i) stringent control of symptoms, employing both pharmacological and non-pharmacological measures; and (ii) appropriate communication with the individual and their family, utilizing active listening strategies, approaches to promote dignity, and assisting in finding meaning for the remaining life, with emphasis on the significance of non-verbal communication (i.e., gaze, touch, facial expression, and hand placement); (iii) supporting the family, identifying their needs, mobilizing their potential, and aiding them in coping with the various losses before and after the patient’s death; (iv) interdisciplinary teamwork, integrating the contributions of different professionals adequately trained to address the diverse needs of the individual and their family (8).
On March 11, 2020, the World Health Organization (WHO) declared the status of a global pandemic due to the spread of COVID-19, a respiratory infectious disease caused by the SARS-CoV-2 virus (9). The global population faced intense and unprecedented challenges, leading to economic shifts, humanitarian crises, and new social interaction norms (10). The pandemic brought about abrupt and stringent changes in people’s lives, resulting in significant personal, psychological, professional, social, and familial impacts within a timeframe that, even today, remains poorly defined (11).
The overall circumstances experienced during 2020–2022 due to the COVID-19 pandemic, demanded a reevaluation of caring procedures, where a priority measure emerged: restricting contacts between individuals at the end of life, their families, and healthcare professionals. The need to prevent transmission both during hospitalization and at the home setting, significantly changed many aspects PC, especially concerning the doctor/professional/patient relationship (12). The use of masks and other personal protective equipment (PPE) substantially changed both verbal and non-verbal communication. The imposed physical distancing limited the possibility of providing a warm embrace or offering a comforting gesture (13). Consequently, facial expressions were also restricted, making the transmission of messages more challenging. Genuine and comprehensible communication relies heavily on facial expressions (14). Individuals in need of PC experienced long periods of solitude without the presence of their family members. Despite the fear of transmission and imposed isolation, these individuals managed to preserve their ability to communicate and interact, nearly until the moment of death (15). Since communication is an essential resource for high-quality PC, limitations in personal interaction among the individual, family, and healthcare providers significantly impacted the delivery of these services (15).
The information concerning the experiences perceived by healthcare professionals, individuals, and families regarding PC during the COVID-19 pandemic can provide significant insights about supporting strategies for PC practices in future pandemics. This information may also prove valuable during situations where healthcare decisions need to be made promptly.
This study aimed to map the experiences of healthcare professionals, individuals, and families in PC and end-of-life situations during the COVID-19 pandemic. An initial search in the JBI Evidence Synthesis, MEDLINE (PubMed), and CINAHL databases did not yield any scoping reviews addressing this objective.
The research questions guiding this study were as follows: (i) What are the experiences perceived by healthcare professionals in the practice of PC and end-of-life situations during the COVID-19 pandemic? (ii) What are the experiences perceived by the person in palliative or end-of-life situations during the provision of care in the context of the COVID-19 pandemic? (iii) What are the experiences perceived by the family of the person in palliative or end-of-life situations during the provision of care in the context of the COVID-19 pandemic? (iv) What strategies were employed by healthcare professionals during the COVID-19 pandemic in the practice of PC and end-of-life situations?
2 Method
The study followed the JBI® methodology for scoping reviews, which was considered the most appropriate method to explore and examine the experiences of healthcare professionals, individuals, and families in PC and end-of-life situations during the COVID-19 pandemic. Eligibility criteria were developed following the mnemonic P (participants), C (concept), and C (context) and with no deviations from the review protocol (16), with registration on the Open Science Framework.1
2.1 Eligibility criteria
Participants: studies that involved healthcare professionals from multidisciplinary teams providing PC and end-of-life care; individuals aged 18 and above and/or their families, who were in palliative and end-of-life situations, referred for PC.
Concept: studies that focused on the concept of experience and perception as encountered by individuals, families, and healthcare professionals regarding the provision of PC and end-of-life care during the COVID-19 pandemic. This also included studies referencing the strategies employed by healthcare professionals during the COVID-19 pandemic in the practice of PC and end-of-life care.
Regarding the Context, studies conducted in locations where PC and end-of-life care are provided were included. Studies published in English between 2019 and 2022 were incorporated, encompassing original research with various methodological approaches such as qualitative, quantitative, and mixed methods, as well as literature reviews, as outlined in the review protocol (16).
Literature that did not report on the SARS-COV-2 Pandemic period was excluded.
2.2 Search strategy
The research employed a comprehensive strategy to identify available literature regarding the experiences of healthcare professionals, individuals, and families in PC and end-of-life situations during the COVID-19 pandemic. An initial evidence search was conducted by one reviewer to determine key terms and develop the search strategy. This search was limited to MEDLINE (via PubMed) and CINAHL (via EBSCO). The search strategy was pilot tested in a database selected by the research team to ensure its robustness in capturing the necessary evidence before finalization. Text words found in the titles and abstracts of relevant articles, as well as indexing terms used to describe the articles, were used to develop a comprehensive search strategy in databases such as CINAHL Complete (via EBSCOhost), MEDLINE (via PubMed), Psychology, Mediclatina, and Cochrane Database of Systematic Reviews (via EBSCOhost). Grey literature was searched for in RCAAP (Repositório Científico de Acesso Aberto de Portugal). The search strategy incorporated all identified keywords and indexing terms, and the Boolean phrase was adapted for each included database. For additional information, please refer to Lourenço et al. (14). Reference lists of all selected studies were screened for additional relevant studies. The search strategy was developed by two researchers (17).
2.3 Study selection
The identified studies were retrieved and stored in Mendeley® V1.19.8 (Mendeley Ltd., Elsevier, Netherlands), and the duplicates were removed. Subsequently, the articles were imported into Rayyan QCRI (Qatar Computing Research Institute [Data Analytics], Doha, Qatar). Titles and abstracts were independently reviewed by two researchers to assess eligibility. The full texts of eligible documents were thoroughly examined by two independent reviewers based on the inclusion and exclusion criteria. Exclusion reasons for full-text articles that are documented in Figure 1. Discrepancies that emerged between reviewers during this stage of the selection process were solved through discussion with a third reviewer. The results of the search and the study inclusion process are reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (18).
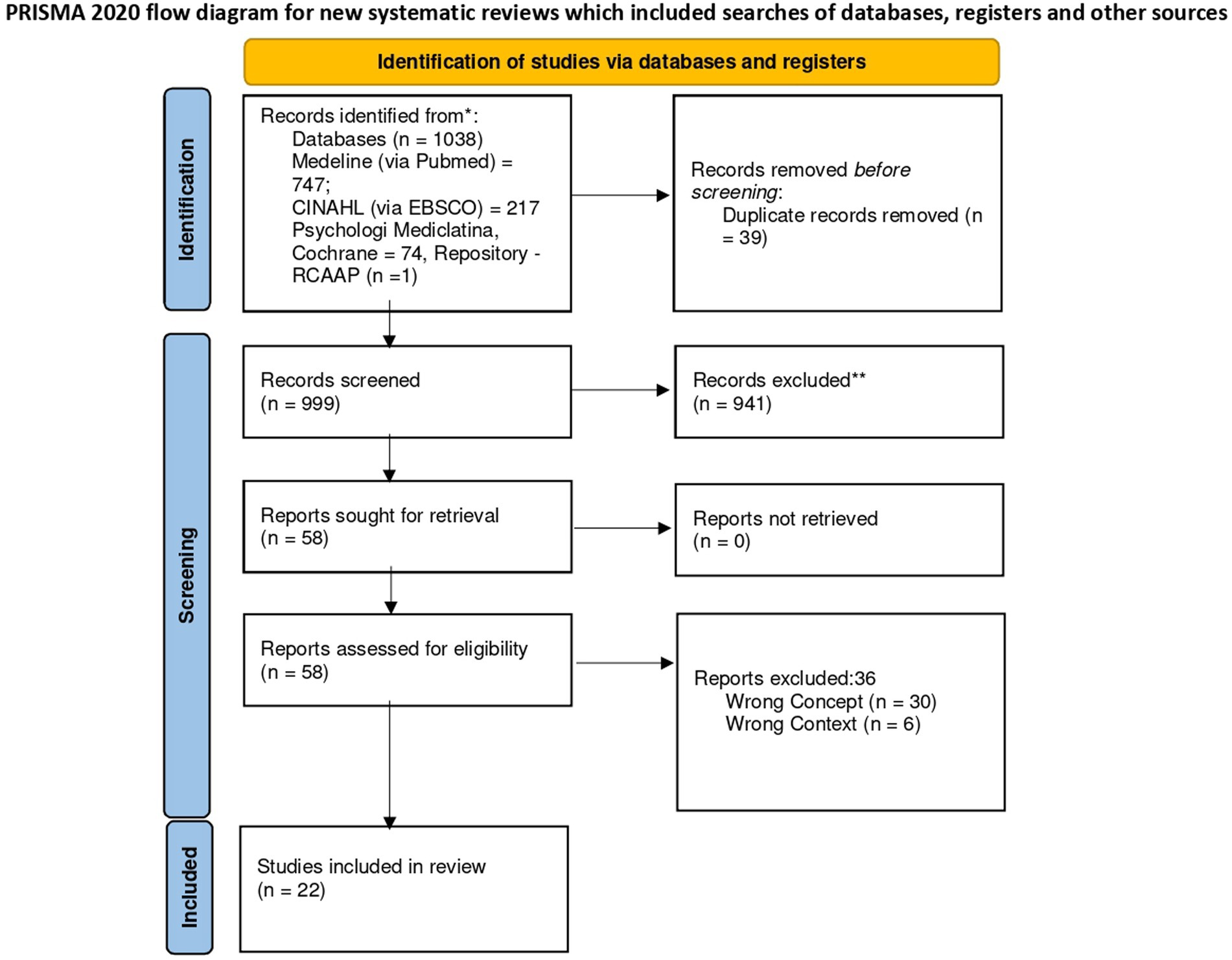
Figure 1. Search results and study selection and inclusion process (18).
2.4 Data extraction
Data were extracted from articles included in the scoping review by two independent reviewers using a data extraction tool developed by the reviewers and refined following piloting with a small number of studies, and subsequently applied to all included studies. The data extraction tool collected specific information about the population, context, geographical location, study methods, phenomena of interest relevant to the review objectives, and the type of sources. Discrepancies between the two reviewers were resolved through discussion or by involving a third reviewer. A reflective thematic analysis was conducted to extract findings related to common themes. The extracted data are presented in both tabular and diagrammatic formats. A narrative summary follows the tabulated results, according to JBI® recommendations (19), which align with the protocol planned for this study (16).
3 Results
3.1 Study inclusion
The research strategy yielded a total of 1,038 references, among which 39 were removed due to duplication, resulting in 999 articles for title and abstract screening. A total of 941 references were excluded during the title and abstract screening stage with a sample of 58 studies proceeding to full-text review. A sample of 22 references met the inclusion criteria, being the research sample of this scoping review. Figure 1 provides a concise overview of the article screening process for inclusion in the review, following the PRISMA flowchart (18).
3.2 Characteristics of included studies/reports
The characteristics of the studies included in this review are presented in Table 1. Among the 22 studies included in this scoping review, 21 were primary studies (2, 20–29, 31–39), and one was a narrative literature review (30). The studies originated from various countries: 9 from the USA, 3 from Germany, 3 from Italy, 2 from the UK, 1 from Australia, 1 from Brazil, 1 from Canada, 1 from Ireland, and 1 from Portugal. The majority (n = 12) employed qualitative approaches (2, 20, 22, 26–28, 33, 35–39), while the remaining ten were quantitative studies (21, 23–25, 29–32, 34, 37). Regarding study types, 15 were observational studies, of which 13 were descriptive studies (2, 21, 23, 24, 29, 31–39), and two were cross-sectional designs (25, 37). The remaining studies included three case studies (20, 22, 26), one narrative literature review (30), and three qualitative studies (27, 28, 39). These qualitative studies aimed to comprehend the grieving process (27), the changes and challenges in the daily work of healthcare professionals (39), and the impact of changes on individuals and caregivers in palliative and end-of-life situations (28), exploring the experiences of participants including bereaved family members, professionals, and patients/caregivers throughout the study duration.
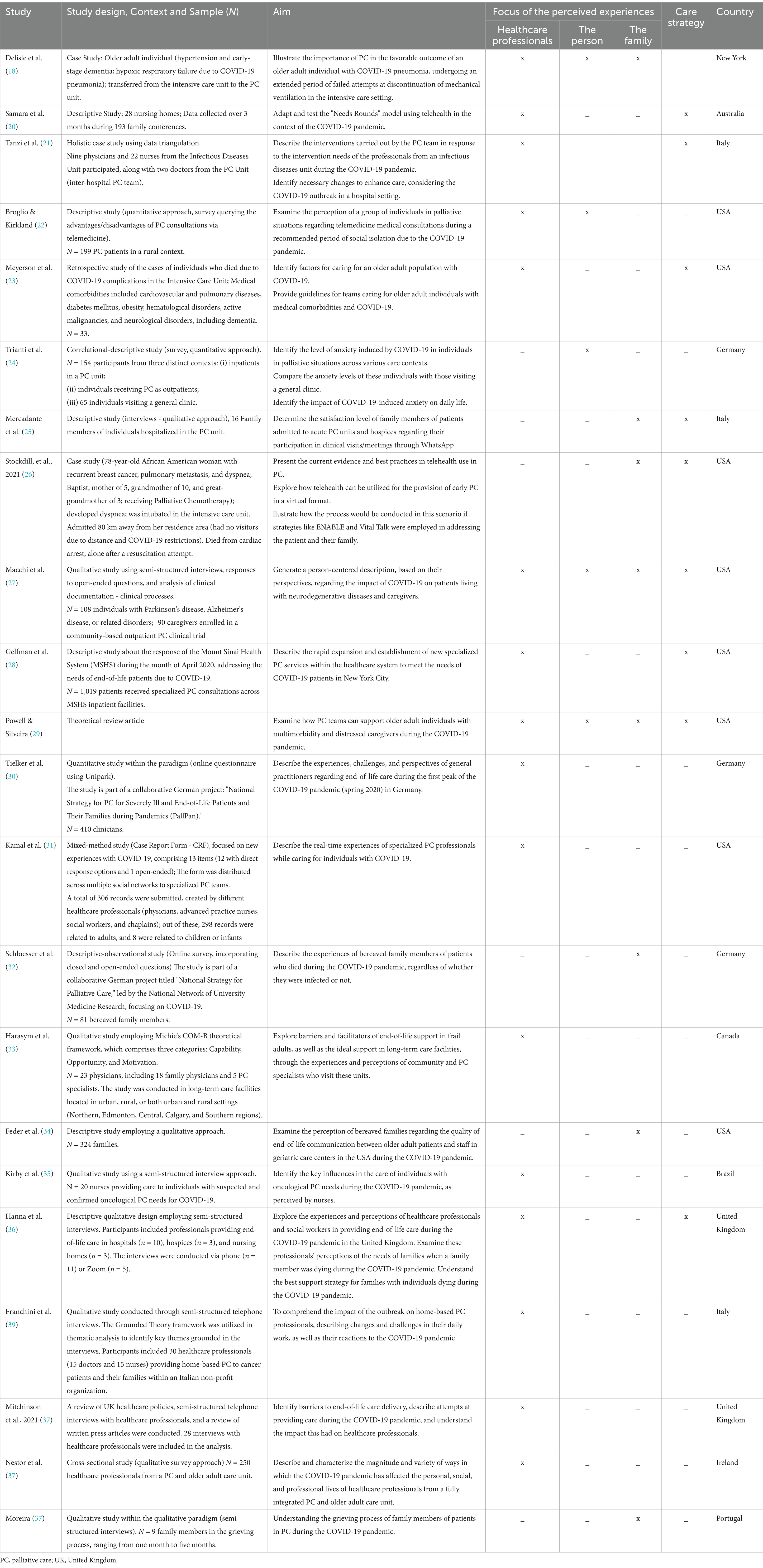
Table 1. Study characteristics concerning the country of origin, study design, number of participants, types of experiences perceived and described in the study, and care strategies.
Among the 22 studies included in this review, 12 focus on PC in a hospital setting (20, 22, 24, 26, 27, 29, 30, 32, 35–38). Two studies highlight long-term care (21, 34), two explore PC in a home-based context (23, 39), and two investigate PC in outpatient settings (28, 31). In the remaining four studies (2, 25, 33, 37), the samples included participants from diverse contexts.
As shown in Table 1, most of the studies predominantly report the experiences and perceptions of healthcare professionals working in PC during COVID-19 (2, 20–24, 28–32, 34, 36, 37, 39). The experiences and perceptions of the person in palliative situation during COVID-19, were described in 5 studies (20, 23, 25, 28, 30). Concerning, the experiences and perceptions of the family of the person in palliative situations during COVID-19 these were reflected in eight studies (20, 26–28, 30, 33, 35, 38).
3.3 Review findings
3.3.1 Theme 1: healthcare professionals’ experiences
Some of the experiences reported by healthcare professionals are described in Table 2. The theme of relationship and communication had the most significant impact. This care strategy was perceived differently by the PC team in relation to the person in a palliative and end-of-life situation (2, 22, 23, 30, 32, 37, 39) and the family (2, 21, 22, 28–32, 37, 39). The theme of relationship and communication was also evident between the multidisciplinary PC team and the frontline team caring for COVID-19 patients (22–24, 29, 30, 37, 39). Teams of professionals who provide PC have become managers in providing technical and instrumental support, in controlling complex symptoms, particularly in managing pain and dyspnea (2, 22, 24, 29, 30, 34, 39), in delicate end-of-life decisions and post-grief care (22, 24, 32), and in the emotional and psychosocial support provided to the frontline teams caring for COVID-19 patients (22, 24, 29, 30, 32). Other themes emerged in the practice of PC, such as procedures for caring for the person and the family in a palliative and end-of-life situation (31, 37, 39) and the impact on the well-being of the multidisciplinary PC team (2, 36, 37, 39) during the pandemic period, as presented in the data shown in Table 2.
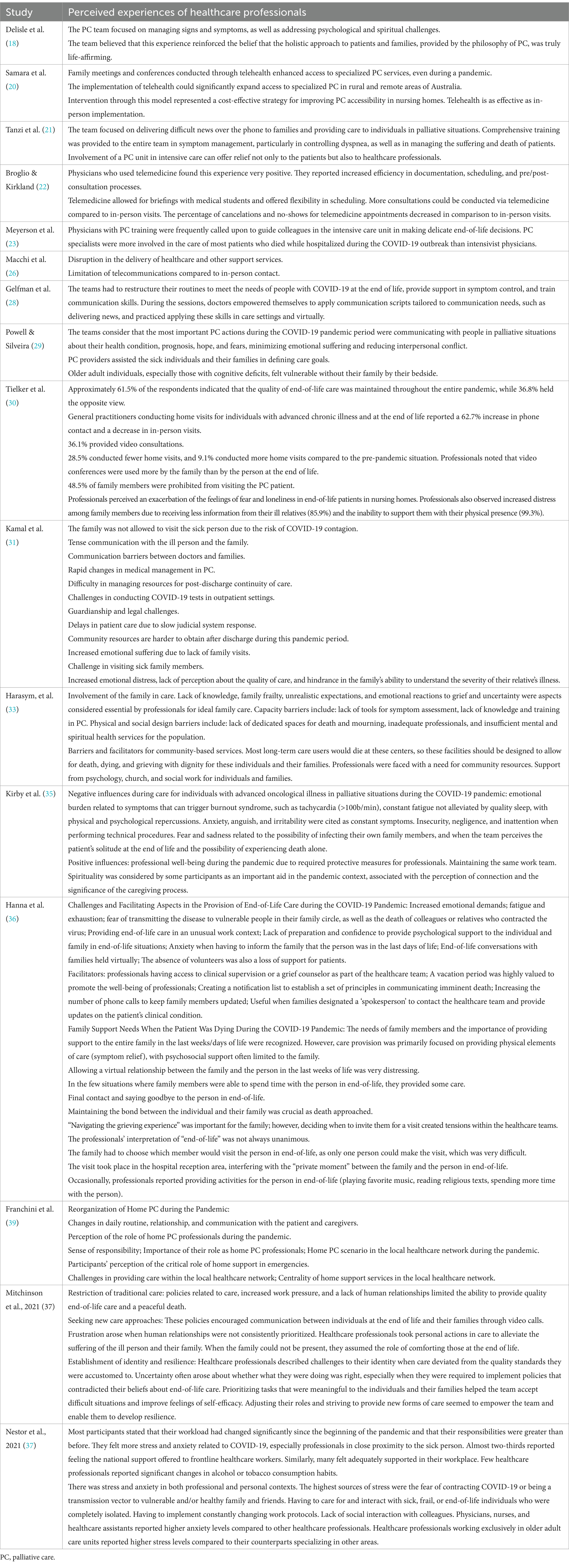
Table 2. Perceived experiences of healthcare professionals in the context of palliative and end-of-life care during the COVID-19 pandemic.
3.3.2 Theme 2: the person’s experiences
The perceptions experienced by individuals in palliative and end-of-life situations during the study period, due to the restrictions adopted by healthcare services associated with the risk of virus transmission, included: long periods of social isolation (20, 28, 30), which caused them negative psychological impact (20, 25, 28); and loss of dignity and insecurity (20) (for more details, see Table 3).
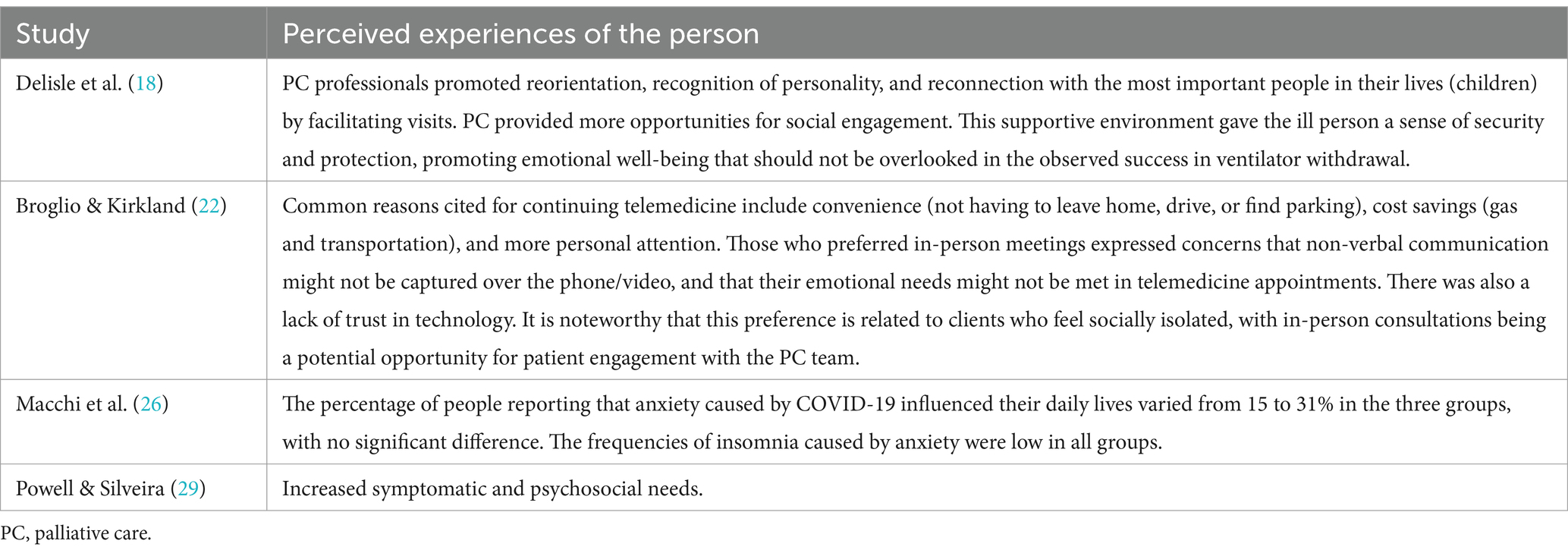
Table 3. Perceived experiences of the person in the context of palliative and end-of-life care during the COVID-19 pandemic.
3.3.3 Theme 3: the family experiences
Regarding the experiences reported by the family, the relationship and communication with the person in a palliative situation are highlighted (20, 26, 27, 33, 38), as well as the need to stay by the bedside of the ill person despite all implemented strategies, such as telemedicine, to overcome some of the difficulties in relationship and communication (25, 26, 27, 29, 32, 43, 40). Additionally, there is a perceived sense of gratitude from the family toward the palliative care team (20). Experiences reported by families caring for the person in a palliative situation at home during COVID-19 reflect higher levels of burden (28, 30). However, one of the studies does not support this finding, as bereaved family members who accompanied their loved one at home expressed lower burden compared to those whose family member died in a hospital setting (33) (for more details, see Table 4).
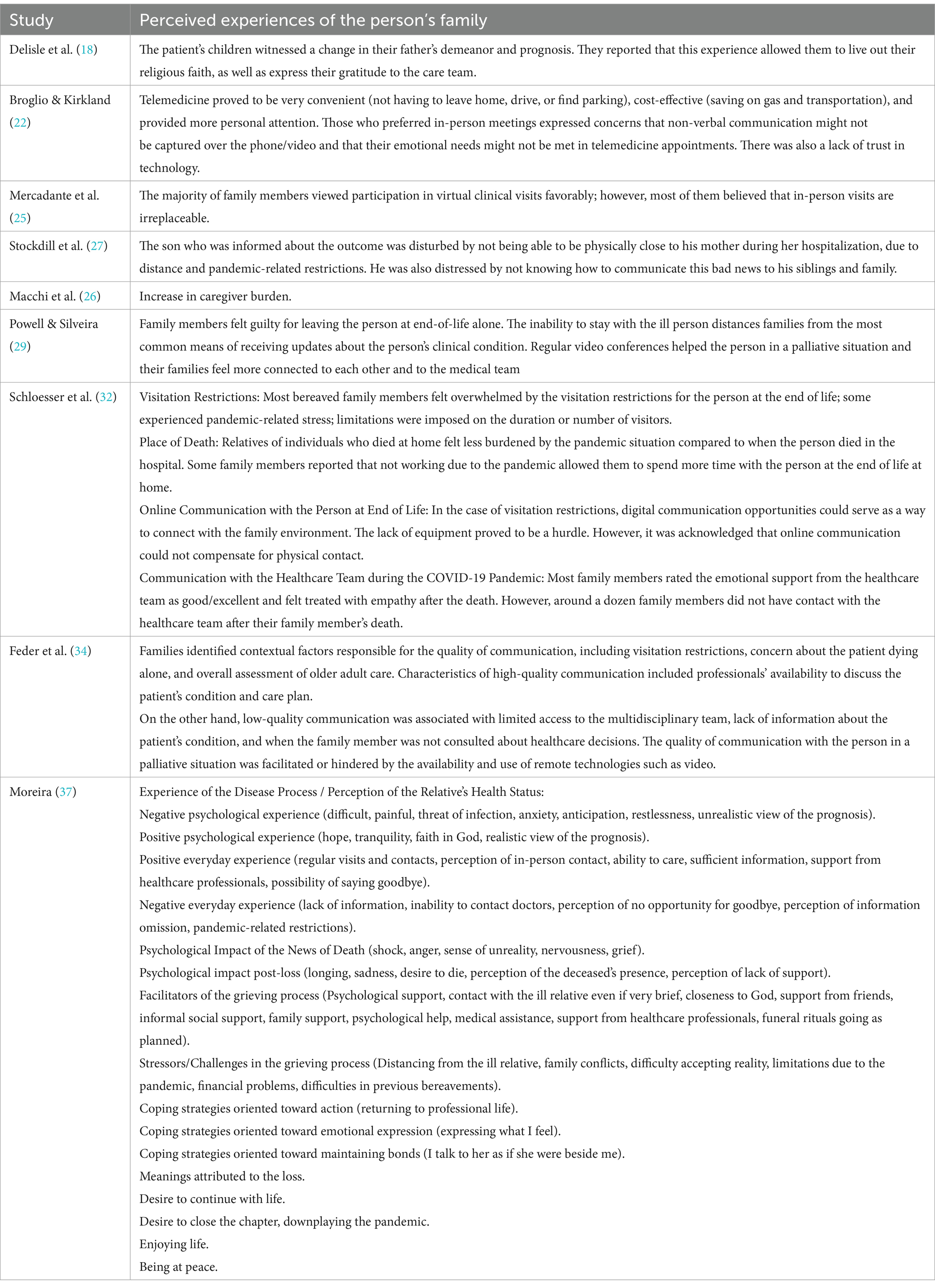
Table 4. Perceived experiences of the person’s family in the context of palliative and end-of-life care during the COVID-19 pandemic.
3.3.4 Theme 4: strategies used by healthcare professionals
Despite the constraints resulting from the pandemic process, it was considered relevant to gather information about new strategies used by healthcare professionals in the practice of PC during COVID-19. Some studies addressed the use of new technologies to mitigate social isolation caused by the restrictive measures adopted by healthcare institutions (21, 22, 26, 28–30, 32, 38). Others discuss new strategies to ensure a peaceful death within the hospital (22, 30). Two of the studies addressed the strategies used to ensure the safety of the multidisciplinary team in infection control (29, 37) (see Table 5).
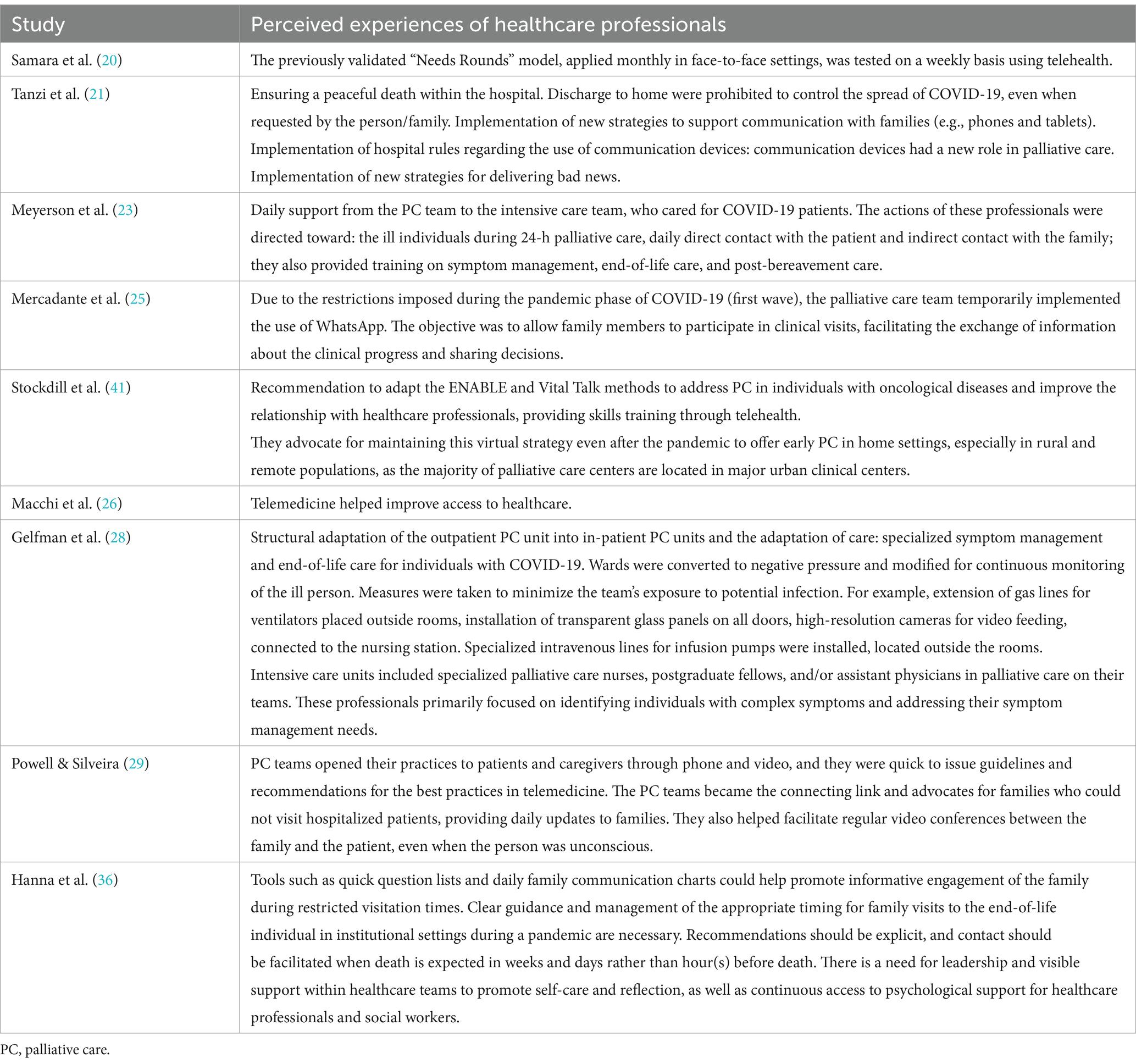
Table 5. Strategies used by healthcare professionals in the practice of palliative and end-of-life care during the COVID-19 pandemic.
4 Discussion
Regarding the characterization of the studies included in this review, a wide geographical distribution was observed, covering various continents, although with a predominance of European, n = 10 (Germany, Italy, UK, Ireland, and Portugal), and American (n = 9) studies. The worldwide spread of included studies, reflect the global spread of the disease across different continents which is aligns with the concept of pandemic attributed to COVID-19. In this sample of 22 studies, there was a predominance of representation of PC in the hospital setting compared to home and long-term care settings. This result can be explained by the fact that most of the studies collected data in 2020 (during the first and second waves of the pandemic) due to fear of the unknown, the high rate of hospitalization among the older adult population with a high burden of disease and frailty.
To address the guiding questions of the review, the discussion was organized by exploring the experiences/perceptions of each participant group: healthcare professionals, individuals, and families in palliative and end-of-life situations. The analyzed studies revealed that communication was a universally perceived experience among the participants. This perception emphasizes the idea that appropriate communication with the individual and the family is a fundamental pillar of PC. In other words, communication among healthcare professionals, the individual, and the family should be systematic, centered on promoting dignity, and helping find meaning in the remaining life (40). The lack of relationship and communication associated with the protective measures required to control COVID-19 transmission was felt by individuals in palliative and end-of-life situations, especially due to social isolation and separation from loved ones. Additionally, the use of personal protective equipment impacted communication and touch (20). To enhance the comfort of the individual and the family, healthcare professionals adopted new forms of communication through technologies such as video calls. However, they felt frustrated when human connections were not consistently prioritized (18). The various participants valued new technologies, although professionals placed greater importance on them compared to families. The latter group considered these technologies an alternative strategy to alleviate the feeling of separation, emphasizing that they do not substitute for physical presence.
Concerning the experiences/perceptions of healthcare professionals in PC during COVID-19, the findings highlighted the following themes: the PC team acting as managers in providing technical and instrumental support, especially in the management of complex symptoms, particularly pain and dyspnea, in delicate end-of-life decisions, and in emotional and psychosocial support for frontline teams caring for individuals with COVID-19. These teams are familiar with legal requirements for documenting advance care directives, as well as living wills and decisions regarding appropriate life-sustaining measures. PC teams made efforts to maintain a connection with families who could not visit their hospitalized loved ones and provided post-bereavement care. They sought to ensure that the wishes of individuals in palliative situations and their families were properly documented and communicated.
Some changes in the procedures for caring for individuals and families in palliative and end-of-life situations, implemented by healthcare management entities, significantly increased the workload and responsibilities compared to the pre-COVID-19 period, conflicting with the principles of palliative care. These factors had an impact on the well-being of the multidisciplinary team (36, 39). Conversely, the well-being of healthcare professionals was observed when they used the required personal protective measures and maintained the same team. Some participants regarded spirituality as a binding factor in the caregiving process (36).
The experiences/perceptions of individuals in PC and at the end of life during COVID-19 received less attention in scientific literature. Among the five articles in which the palliative individual participated, in addition to communication, the following themes were identified: social isolation, psychological impact, loss of dignity, and insecurity. This was experienced due to the inherent restrictions during the pandemic period, which overlapped with the core principles of PC that truly affirm life. The overwhelming majority of studies reported the social isolation of patients, which had a significant psychological impact, including feelings of depersonalization and despair.
The psychological impact of the COVID-19 pandemic on individuals in PC admitted to PC units seemed insignificant, given the imminent threat that terminal illness represents for these individuals, in contrast to individuals receiving outpatient palliative care, who exhibited higher levels of anxiety (25). COVID-19 added a new dimension of suffering to the experience of individuals transitioning to palliative and end-of-life situations due to the serious and irreversible nature of the disease. These mostly older individuals found themselves socially isolated for an extended period. They were cared for by healthcare professionals whose presence was obscured by layers of personal protective equipment, disruption of circadian rhythms, and within an intensive care context, despite their palliative condition. These aspects led to an end-of-life process marked by insecurity and a lack of dignity (20). This contradicts the principles in healthcare disciplines where dignity is considered a professional code and a care policy (20). The findings confirm that institutions that allowed palliative care teams to assume full responsibility for managing individuals at the end of life facilitated a more dignified dying process (31).
The experiences/perceptions of the family of individuals in PC and at the end of life during COVID-19 revealed two central themes: staying by the bedside and the burden of concerns. Indeed, family members valued virtual contacts with the healthcare team and their loved ones, both in virtual clinical visits to monitor the situation (38) and to feel more engaged (20, 30, 35). These contacts were also helpful in receiving emotional support from the PC team during the illness and post-death period (27, 33). Therefore, family members express a sense of gratitude toward the PC team (20). However, they emphasize that in-person contact by the bedside of the family member is irreplaceable (38, 40). Communication enables a connection between different elements, facilitating shared decision-making (41).
Caregivers of individuals in palliative care and at the end of life perceived an increased burden during the COVID-19 period (28, 30), especially during the first and second waves of the disease. The abrupt constraints and restrictions, fear, and insecurity about the unknown may justify the heightened perception of burden among family members, regardless of whether the individual in palliative care and at the end of life was in a home or hospital setting.
The results indicate an increased burden on family caregivers providing care to individuals in palliative care and at the end of life in a home setting. The lack of psychosocial support reduced home-based PC, worsening condition of their family member, and imposed changes for pandemic control might explain this intensified perception of burden (30). However, when comparing the burden between caregivers providing care at home and those for who the loved one passed away at a hospital setting, the findings revealed that the former experienced less burden by the pandemic situation compared to the latter. According to these family members, not being employed due to the pandemic allowed them to spend more time with their family member at the end of life (33).
The new strategies used by healthcare professionals in the practice of PC during COVID-19 include the use of information and communication technologies to address communication and care documentation deficits. There was a reorganization of services and restructuring of CP units to cope with the rapid and exponential increase in COVID-19 infected individuals. Information technologies used to meet the universal need for social isolation had two levels of acceptance. The convenience of not having to leave home, drive or park a car, cost reduction (gas and transportation), and the perception of personalized care were seen as advantages. On the other hand, those who preferred in-person meetings expressed concerns that non-verbal communication might not be captured in phone/video consultations, emotional needs might not be met in telemedicine appointments, and there was a general mistrust on technology. It is worth noting that this preference was related to individuals who experienced social isolation, with in-person consultations seen as a potential opportunity for patient engagement with the PC team (23).
Visitor restrictions were a practice implemented by healthcare institutions worldwide to mitigate the pandemic. PC teams became the link and advocates for families who could not visit their hospitalized loved ones. They facilitated and promoted regular video conferences between families and patients (even when the person was unconscious) and provided daily updates to families about the clinical status of their loved ones, significantly reducing levels of distress (30).
The reorganization of services and restructuring of PC units in response to a public health emergency caused by the COVID-19 pandemic forced PC teams to make rapid decisions and adapt care to the new needs of individuals and families. As a result, many of the golden rules of PC practice had to be adjusted to the current COVID-19 pandemic. Coordination of care could be improved when the whole healthcare team was involved (22).
4.1 Limitations
The high proportion of descriptive studies and case studies, which are methodologically weak and less robust in terms of the evidence produced, requires caution in interpreting the results of this review.
5 Conclusion
The pandemic caused by COVID-19 imposed implications on healthcare professionals, individuals, and families in PC and end-of-life situations. Apart from the risk of contracting the disease, there was a need to adopt isolation policies that ended up changing many PC and end-of-life practices. The fear of virus transmission and the isolation imposed by health regulatory authorities led the participants to new experiences. The central theme reported by the participants during the study period was relationships. This caregiving strategy was perceived differently by all participants. The restriction of visits was a practice implemented by healthcare institutions worldwide, aiming to control and mitigate the pandemic disease. However, PC teams became the link and advocates for families who could not visit hospitalized patients. They promoted and facilitated regular videoconferences between the family and the patient. Nevertheless, individuals and families emphasized that despite the benefits of new technologies, in PC, in-person contact by the bedside was irreplaceable. The restrictive measures inherent to the pandemic period conditioned feelings of social isolation, with negative psychological impact, loss of dignity, and insecurity, especially for the person in PC. These factors overshadowed the fundamentals of PC.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ML: Formal analysis, Writing – review & editing, Writing – original draft, Validation, Supervision, Project administration, Methodology, Investigation, Conceptualization. TG: Writing – original draft, Investigation, Conceptualization. FA: Project administration, Writing – review & editing, Supervision, Methodology. FV: Writing – review & editing. RS: Writing – review & editing, Methodology.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Amblàs-Novellas, J, Murray, SA, Espaulella, J, Martori, JC, Oller, R, Martinez-Muñoz, M, et al. Identifying patients with advanced chronic conditions for a progressive palliative care approach: a cross-sectional study of prognostic indicators related to end-of-life trajectories. BMJ Open. (2016) 6:e012340. doi: 10.1136/bmjopen-2016-012340
2. Hanna, JR, Rapa, E, Dalton, LJ, Hughes, R, Quarmby, LM, McGlinchey, T, et al. Health and social care professionals’ experiences of providing end of life care during the COVID-19 pandemic: a qualitative study. Palliat Med. (2021) 35:1249–57. doi: 10.1177/02692163211017808
3. Knaul, FM, Farmer, PE, Krakauer, EL, De Lima, L, Bhadelia, A, Kwete, XJ, et al. Alleviating the access abyss in palliative care and pain relief— an imperative of universal health coverage: the lancet commission report. Lancet. (2018) 391:1391–454. doi: 10.1016/S0140-6736(17)32513-8
4. Worldwide Palliative Care Alliance. Global atlas of palliative care at the end of life. London: Worldwide Palliative Care Alliance (2014).
5. Al-Mahrezi, A, and Al-Mandhari, Z. Palliative care: time for action. Oman Med J. (2016) 31:161–3. doi: 10.5001/omj.2016.32
6. Radbruch, L, De Lima, L, Lohmann, D, Gwyther, E, and Payne, S. The Prague charter: urging governments to relieve suffering and ensure the right to palliative care. Palliat Med. (2013) 27:101–2. doi: 10.1177/0269216312473058
7. Dakessian Sailian, S, Salifu, Y, Saad, R, and Preston, N. Dignidade de pacientes com necessidades paliativas no Oriente Médio: uma revisão integrativa. BMC Cuidados Paliativos. (2021) 20:112. Publicado em 2021 jul 16. doi: 10.1186/s12904-021-00791-
9. Centro Regional de Informação para a Europa Ocidental. (2020). United Nations: one year of combating the pandemic. Available at: https://unric.org/pt/
10. World Health Organization. (2022). Versão final da nova classificação internacional de doenças da OMS. Available at: https://www.paho.org/pt/noticias/11-2-2022-versao-final-da-nova-classificacao-internacional-doencas-da-oms-cid-11-e
11. Chochinov, HM, Bolton, J, and Sareen, J. Death, dying, and dignity in the time of the COVID-19 pandemic. J Palliat Med. (2020) 23:1294–5. doi: 10.1089/jpm.2020.0406
12. Back, A, Tulsky, JA, and Arnold, RM. Communication skills in the age of COVID-19. Ann Intern Med. (2020) 172:759–60. doi: 10.7326/M20-1376
13. Marra, A, Buonanno, P, Vargas, M, Iacovazzo, C, Ely, EW, and Servillo, G. How COVID-19 pandemic changed our communication with families: losing nonverbal cues. Crit Care. (2020) 24:297. Published 2020 Jun 5. doi: 10.1186/s13054-020-03035-w
14. Ersek, M, Smith, D, Griffin, H, Carpenter, JG, Feder, SL, Shreve, ST, et al. End-of-life Care in the Time of COVID-19: communication matters more than ever. J Pain Symptom Manag. (2021) 62:213–222.e2. doi: 10.1016/j.jpainsymman.2020.12.024
15. Chapman, M, Russell, B, and Philip, J. Systems of care in crisis: the changing nature of palliative care during COVID-19. J Bioeth Inq. (2020) 17:761–5. doi: 10.1007/s11673-020-10006-x
16. Lourenço, M, Gomes, T, Araujo, F, Ventura, F, and Silva, R. Challenges for palliative care in times of COVID-19: a scoping review protocol. Res Soc Develop. (2023) 12:e23012340640–16. doi: 10.33448/rsd-v12i3.40640
17. Peters, MDJ, Marnie, C, Tricco, AC, Pollock, D, Munn, Z, Alexander, L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI® evidence. Synthesis. (2020) 18:2119–26. doi: 10.11124/JBIES-20-00167
18. Peters, MD, Godfrey, C, McInerney, P, Munn, Z, Tricco, AC, and Khalil, H. Chapter 11: scoping reviews In: E Aromataris and Z Munn, editors. JBI manual for evidence synthesis. Adelaide: JBI (2020)
19. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
20. Delisle, S, Heller, FE, and Blinderman, CD. Prolonged critical illness and demoralization: curative factors in hospice Care in the age of COVID-19. J Hosp Palliat Nurs. (2020) 22:428–31. doi: 10.1097/NJH.0000000000000689
21. Samara, J, Liu, WM, Kroon, W, Harvie, B, Hingele, R, and Johnston, N. Telehealth palliative care needs rounds during a pandemic. J Nurse Pract. (2021) 17:335–8. doi: 10.1016/j.nurpra.2020.12.009
22. Tanzi, S, Alquati, S, Martucci, G, and De Panfilis, L. Learning a palliative care approach during the COVID-19 pandemic: a case study in an infectious diseases unit. Palliat Med. (2020) 34:1220–7. doi: 10.1177/0269216320947289
23. Broglio, K, and Kirkland, KB. Rural palliative care Patients' attitudes toward telemedicine visits during the COVID-19 pandemic: a descriptive study. J Palliat Med. (2021) 24:1126–7. doi: 10.1089/jpm.2021.0192
24. Meyerson, JL, McNamara, LA, Nathan, SN, and Skarf, LM. Complexities of Corona virus Disease-19: the role of palliative Care at a Veterans Affairs Hospital. J Palliat Med. (2021) 24:1375–8. doi: 10.1089/jpm.2021.0020
25. Trianti, SM, Soßalla, L, and Schmitzer, I. Anxiety due to COVID-19 in different palliative care settings in Germany. J Hosp Palliat Nurs. (2021) 23:135–9. doi: 10.1097/NJH.0000000000000719
26. Bakitas, MA, Dionne-Odom, JN, Ejem, DB, Wells, R, Azuero, A, Stockdill, ML, et al. Effect of an early palliative care telehealth intervention vs usual care on patients with heart failure: the ENABLE CHF-PC randomized clinical trial. JAMA Intern Med. (2020) 180:1203–13. doi: 10.1001/jamainternmed.2020.2861
27. Moreira, BS. O luto em tempos de covid 19: a Experiência dos familiares de Doentes em cuidados Paliativos [Dissertação de mestrado]. Porto: Universidade Católica Portuguesa. Faculdade de Educação e Psicologia (2021).
28. Macchi, ZA, Ayele, R, Dini, M, Lamira, J, Katz, M, Pantilat, SZ, et al. Kluger, B M lessons from the COVID-19 pandemic for improving outpatient neuropalliative care: a qualitative study of patient and caregiver perspectives. Palliat Med. (2021) 35:1258–66. doi: 10.1177/02692163211017383
29. Gelfman, LP, Morrison, RS, Moreno, J, and Chai, E. Palliative care as essential to a hospital System's pandemic preparedness planning: how to get ready for the next wave. J Palliat Med. (2021) 24:656–8. doi: 10.1089/jpm.2020.0670
30. Powell, VD, and Silveira, MJ. Palliative Care for Older Adults with multimorbidity in the time of COVID 19. J Aging Soc Policy. (2021) 33:500–8. doi: 10.1080/08959420.2020.1851436
31. Tielker, JM, Weber, JP, Simon, ST, Bausewein, C, Stiel, S, and Schneider, N. Experiences, challenges and perspectives for ensuring end-of-life patient care: a national online survey with general practitioners in Germany. PLoS One. (2021) 16:e0254056. doi: 10.1371/journal.pone.0254056
32. Kamal, AH, Thienprayoon, RM, Aldridge, M, Bull, J, Fazzalaro, K, Meier, DE, et al. Specialty palliative care in COVID-19: early experiences from the palliative care quality collaborative. J Palliat Med. (2021) 24:1689–96. doi: 10.1089/jpm.2020.0440
33. Schloesser, K, Simon, ST, Pauli, B, Voltz, R, Jung, N, Leisse, C, et al. “Saying goodbye all alone with no close support was difficult”- dying during the COVID-19 pandemic: an online survey among bereaved relatives about end-of-life care for patients with or without SARS-CoV2 infection. Schloesseret al. BMC Health Serv Res. (2021) 21:998. doi: 10.1186/s12913-021-06987-Z
34. Harasym, P, Brisbin, S, Afzaal, M, Sinnarajah, A, Venturato, L, Quail, P, et al. Barriers and facilitators to optimal supportive end-of-life palliative care in long-term care facilities: a qualitative descriptive study of community-based and specialist palliative care physicians' experiences, perceptions and perspectives. BMJ Open. (2020) 10:e037466. doi: 10.1136/bmjopen-2020-037466
35. Feder, S, Smith, D, Griffin, H, Shreve, ST, Kinder, D, Kutney-Lee, A, et al. "why Couldn't I go in to see him?" bereaved Families' perceptions of end-of-life communication during COVID-19. J Am Geriatr Soc. (2021) 69:587–92. doi: 10.1111/jgs.16993
36. Kirby, EEF, Siqueira, ASA, Cunha, DAO, Santiago, FB, Neves, LML, and Beserra, VS. COVID-19 and its psychic influences on the perception of the nursing team of oncologica palliative care. REME-Rev Min Enferm. (2021) 25:e-1355. doi: 10.5935/1415-2762-20210003
37. Nestor, S, Tuathaigh, C, and Brien, T. Assessing the impact of COVID-19 on healthcare staff at a combined elderly care and specialist palliative care facility: a cross-sectional study. Palliat Med. (2021) 35:1492–501. doi: 10.1177/02692163211028065
38. Mercadante, S, Adile, C, Ferrera, P, Giuliana, F, Terruso, L, and Piccione, T. Palliative Care in the Time of COVID-19. J Pain Symptom Manag. (2020) 60:e79–80. doi: 10.1016/j.jpainsymman.2020.04.025
39. Franchini, L, Varani, S, Ostan, R, Bocchi, I, Pannuti, R, Biasco, G, et al. Home palliative care professional’s perception of challenges during the COVID-19 outbreak: a qualitative study. Palliat Med. (2021) 35:862–74. doi: 10.1177/02692163211008732
40. Parola, V, Neves, H, Duque, FMB, Bernardes, RA, Cardoso, R, Mendes, CA, et al. Rehabilitation programs for bedridden patients with prolonged immobility: a scoping review protocol. Int J Environ Res Public Health. (2021) 18:12033. doi: 10.3390/ijerph182212033
Keywords: palliative care, end-of-life care, COVID-19, health personnel, family
Citation: Lourenço M, Gomes T, Araujo F, Ventura F and Silva R (2024) Challenges for palliative care in times of COVID-19: a scoping review. Front. Public Health. 12:1330370. doi: 10.3389/fpubh.2024.1330370
Edited by:
Vincenzo Auriemma, University of Salerno, ItalyReviewed by:
Daniele Battista, University of Salerno, ItalyValeria Saladino, University of Cassino, Italy
Copyright © 2024 Lourenço, Gomes, Araujo, Ventura and Silva. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marisa Lourenço, bWFyaXNhQGVzZW5mLnB0