 Katia Iskandar1,2,3,4*†
Katia Iskandar1,2,3,4*† Deema Rahme2,5†
Deema Rahme2,5† Pascale Salameh2,6,7,8†
Pascale Salameh2,6,7,8† Chadia Haddad2,7,9†
Chadia Haddad2,7,9† Hala Sacre2,10,11†
Hala Sacre2,10,11† Mohamed Bahlol12
Mohamed Bahlol12 Rula M. Darwish13
Rula M. Darwish13 Sarah El Khatib2,3†
Sarah El Khatib2,3† Jihan Safwan1,2†
Jihan Safwan1,2† Fouad Sakr1,2,13,14Mohamad Rahhal1Hassan Hosseini15,16†
Fouad Sakr1,2,13,14Mohamad Rahhal1Hassan Hosseini15,16† Michelle Cherfane2,7,17†
Michelle Cherfane2,7,17†- 1School of Pharmacy, Lebanese International University, Beirut, Lebanon
- 2INSPECT-LB (Institut National de Santé Publique, d’Épidémiologie Clinique et de Toxicologie-Liban), Beirut, Lebanon
- 3Department of Health and Social Work, School of Public Health, Lebanese University, Fanar, Lebanon
- 4Higher Institute of Public Health (ISSP), Saint Joseph University of Beirut, Beirut, Lebanon
- 5Department of Pharmacy Practice, School of Pharmacy, Beirut Arab University, Beirut, Beirut, Lebanon
- 6Department of Primary Care and Population Health, University of Nicosia Medical School, Nicosia, Cyprus
- 7Gilbert and Rose-Marie Chagoury School of Medicine, Lebanese American University, Byblos, Lebanon
- 8Faculty of Pharmacy, Lebanese University, Hadat, Lebanon
- 9Research Department, Psychiatric Hospital of the Cross, Jal Eddib, Lebanon
- 10Drug Information Center, Order of Pharmacists of Lebanon, Beirut, Egypt
- 11Department of Pharmaceutical management and economics, Department Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, Egyptian Russian University, Badr city, Cairo governorate, Egypt
- 12Department of Pharmaceutics and Pharmaceutical Technology, School of Pharmacy, The University of Jordan, Amman, Jordan
- 13École Doctorale Sciences de la Vie et de la Santé, Université Paris-Est Créteil, Paris, France
- 14UMR U955 INSERM, Institut Mondor de Recherche Biomédicale, Université Paris-Est Créteil, Paris, France
- 15INSERM U955-E01, IMRB, Henri Mondor Hospital, Créteil, France
- 16Department of Neurology, Henri Mondor Hospital, AP-HP, Créteil, France
- 17Environmental and Public Health Department, College of Health Sciences, Abu Dhabi University, Abu Dhabi, United Arab Emirates
Introduction: Studies from developed and developing countries showed that the knowledge levels of stroke need improvement. Educational campaigns varied and were of limited influence predominantly because of their short duration and the need for financial support. The study aims to test the impact of a 3-min online video on the knowledge of stroke and factors influencing the knowledge score in four Arab countries.
Methods: A cross-sectional web-based pre-post study was conducted in Egypt, Jordan, Lebanon, and the United Arab Emirates. The data were collected using the snowball technique. Participants were adults aged 18 years and above. The questionnaire sequence was conducting a pretest, followed by the educational video explaining stroke occurrence, types, risks, warning signs, preventive measures, and treatment, and finally, a posttest to evaluate the differences in knowledge from baseline. Statistical analysis included paired t-tests comparing pre-post-education stroke knowledge scores, while repeated measures ANOVA, adjusting for covariates, assessed mean changes.
Results: The total number of participants was 2,721, mainly younger than 55 years. The majority had a university degree and were not healthcare professionals. A significant improvement was noted in the total knowledge score in all countries from a mean average (Mpretest = 21.11; Mposttest = 23.70) with p < 0.001. Identification of the stroke risks (Mpretest = 7.40; Mposttest = 8.75) and warning signs (Mpretest = 4.19; Mposttest = 4.94), understanding the preventive measures (Mpretest = 5.27; Mposttest = 5.39) and the importance of acting fast (Mpretest = 0.82; Mposttest = 0.85) improved from baseline with (p < 0.001) for all score components.
Conclusion: The educational tool successfully enhanced public understanding of stroke risks, the identification of stroke signs, and the critical need for emergency action. The advantages of this video include its short length, free online access, use of evidence-based content in lay language, and reflective images. The ultimate goal remains the long-term improvement of sustainability by mandating full-scale trials.
Introduction
Stroke is the second leading cause of morbidity and mortality worldwide (1). The number of deaths due to stroke was 6.6 million in 2020, a figure projected to increase by at least 50% by 2050 (1). The burden of disability linked with disease complications is also on the rise, with an estimated increase from 144.8 million disability-adjusted life-years (DALYs) in 2020 to 189.3 million DALYs by 2050 (1). Previous data on the incidence and deaths due to stroke have been markedly and rapidly increasing since the 1990s, predominantly in low- and middle-income countries (LMICs) (1). The recent alarming findings are the higher incidence of stroke in young individuals (18–50 years) (2, 3). Stroke is also associated with high economic impact, with estimated costs of treatment, rehabilitation, and loss of productivity exceeding US$891 billion per year globally (1). Evidence-based solutions have been proposed to reduce the global incidence of stroke based on the following four pillars: surveillance, prevention, acute care, and rehabilitation (1). Primordial prevention of stroke meets the sustainable development goals (4), including (1) reducing poverty, (2) improving socioeconomic conditions, (3) universal health coverage, (4) health equity, (5) reducing air pollution, (6) healthy lifestyle, (7) building healthy cities and homes, (8) and public health campaigns to raise awareness about stroke and stroke risk factors (1).
The World Health Organization and the Lancet Neurology Commission surveyed 84 LMICs and high-income countries (HICs) to compare the status of stroke services. The results showed numerous deficiencies, including a lack of public education in many countries (5). The scope of this study is primordial community education as a preventive measure of stroke occurrence and recurrence (6). Primordial stroke prevention consists of activities to avoid stroke risk factors, whereas primary prevention aims to limit or manage exposure to risk factors for stroke (6). Research showed that the community knowledge of stroke symptoms, prevention measures, and the urgency of hospitalization in case of an event is poor or lacking in both LMICs and HICs (7–9).
Educational campaigns, including mass media (10), and digital platforms such as mobile applications [e.g., the PreventS-MD web app (PreventS-MD) (11) and stroke riskometer (12)], text messages to mobile health telemedicine (12), computer and web-based technologies, including artificial intelligence, are adapted tools to support stroke knowledge, awareness, and management (6). A systematic review and meta-analysis found that public stroke campaigns significantly influence the identification of stroke symptoms and the urgency for hospital transfer (13). The study stressed the accessibility and affordability of the digital technologies used by lay individuals for primary stroke prevention and considered that evidence-based content improves physician–patient communication and healthcare provision (13). Educating young adults about stroke was found beneficial in spreading awareness among families, raising the alarms about harmful health behaviors, and adapting preventive measures to reduce the burden of stroke in adult life (14). Numerous studies have demonstrated the effectiveness of educational campaigns and other digital tools in enhancing public knowledge of stroke to modify health behaviors and minimize delays in emergency transfer of a patient experiencing stroke (15–17). In this study, a 3-min educational video was built based on the American Stroke Association online awareness materials (18), the BE-FAST algorithm (19), and the Stroke Foundation New Zealand (20). The BE-FAST algorithm allows the identification of persons experiencing an ischemic stroke episode (18) to act fast and avoid delays in seeking emergency care. This study aims to test the impact of the budget-free short educational online video on public knowledge in Arab countries about stroke and factors influencing stroke knowledge scores.
Materials and methods
Study design
A cross-sectional population-based interventional study was conducted from 1 July 2022 to September 2022. The research proposal was sent to international research groups in Arab countries to invite interested parties to join the study. Researchers from Egypt, Jordan, Lebanon, and the United Arab Emirates (UAE) agreed to join the project. Google Forms, a cloud-based survey powered by Google, was used to create the online survey, which included a 3-min educational video based on the BE-FAST algorithm (19). Data were collected using the snowball sampling technique (21) by asking university students to share the link to the online survey with their families and social networks using various social media platforms (WhatsApp, Facebook, Instagram, and LinkedIn).
Participants
Eligible participants were adults 18 years of age or older, with internet access, and residing in the participating countries. The first contact with participants was made through university students in their respective countries who were trained and informed about the content and aim of the survey. The total number of respondents from the four participating countries was 2,721, including 1,414 from Egypt, 215 from Jordan, 685 from Lebanon, and 407 from the UAE.
Sample size calculation
The minimum sample size was calculated using the G-Power software, version 3.0.10. Taking into consideration that a stratified analysis per country applies, the minimum sample size calculation was determined as follows: the calculated effect size was 0.11 (small effect size), based on an expected squared multiple correlation of 0.1 (R2 deviation from 0) related to the omnibus test of multiple regression. The minimum sample required was n = 205 from each country, considering an alpha error of 5%, a power of 80%, and allowing 20 predictors in the model.
Questionnaire/educational video
The video was 3 min in length, and the evidence-based content was presented in lay language with images reflective of the content. The online video was piloted among the researcher’s network to test the acceptance and understanding of the content. Expert opinions of healthcare professionals provided insights about the relevance of the content. The purpose of the questionnaire/video was to educate participants about stroke, including its occurrence, risk factors, alarming signs, treatment, and prevention measures. Pretests and posttests included the same questions to evaluate baseline participant knowledge about the material in the video and evaluate acquired knowledge post-video. The online survey is translated from English to Arabic according to the WHO translational guidelines1. The translated version was then back-translated to English again. English versions were compared, with minor discrepancies corrected by consensus between the translators and the principal investigator in each country.
The questionnaire consisted of three main parts sequenced as follows: pretest, 3-min educational video, and posttest. It included closed-ended questions and encompassed the following four sections:
1. Participants’ sociodemographic characteristics, health status, and lifestyle. A healthy lifestyle index was set as any individual with normal-range body mass index (BMI), exercising regularly (mild, moderate, or intense), non-smoker or currently non-smoker, not drinking alcohol, eating fruits and vegetables, and drinking enough fluids (22).
2. A pretest that assesses the respondent’s baseline knowledge of stroke: (a) occurrence site, (b) risk factors (i.e., uncontrolled hypertension, diabetes, arrhythmias, dyslipidemia, transient ischemic attack, previous or family history of stroke, stress, obesity, smoking, alcohol consumption, aging, and poor diet), (c) alarming signs (i.e., sudden onset of weakness or numbness on one side of the body, sudden speech difficulty or confusion, sudden difficulty seeing in one or both eyes, and sudden severe headache with unknown cause), (d) preventive measures (i.e., keeping a healthy body weight, quit smoking and stop drinking alcohol, regular exercise, eating a healthy diet, reducing stress, and regular use of prescribed medications to treat underlying diabetes and cardiovascular diseases, including control of blood pressure), and (e) calling the ambulance. The pretest questions were based on the risks and warning signs established by the American Stroke Association (18) and the National Institute of Neurological Disorders and Stroke (23).
3. A 3-min online educational video: “Think and Act Fast to Save a Life” (English Version: https://youtu.be/uzN-Q5SUKmA; Arabic Version: https://youtu.be/yEvvQlX37gs).
4. A posttest, including the same set of questions as the pretest.
Reliability and validity testing of the questionnaire
A factor analysis was conducted on responses from 250 participants to explore stroke knowledge. The Kaiser–Meyer–Olkin measure indicated excellent sampling adequacy (KMO = 0.960), and Bartlett’s test supported the factorability of the correlation matrix (χ2 = 1502.45, df = 300, p < 0.001). Principal component analysis with Promax rotation extracted four factors, explaining 56.74% of the variance. Factors included prevention measures, risk of stroke, warning signs and treatment, and general knowledge and type of stroke. Reliability analysis yielded Cronbach’s alpha of 0.945. The scales used were of appropriate validity and reliability (Table 1).
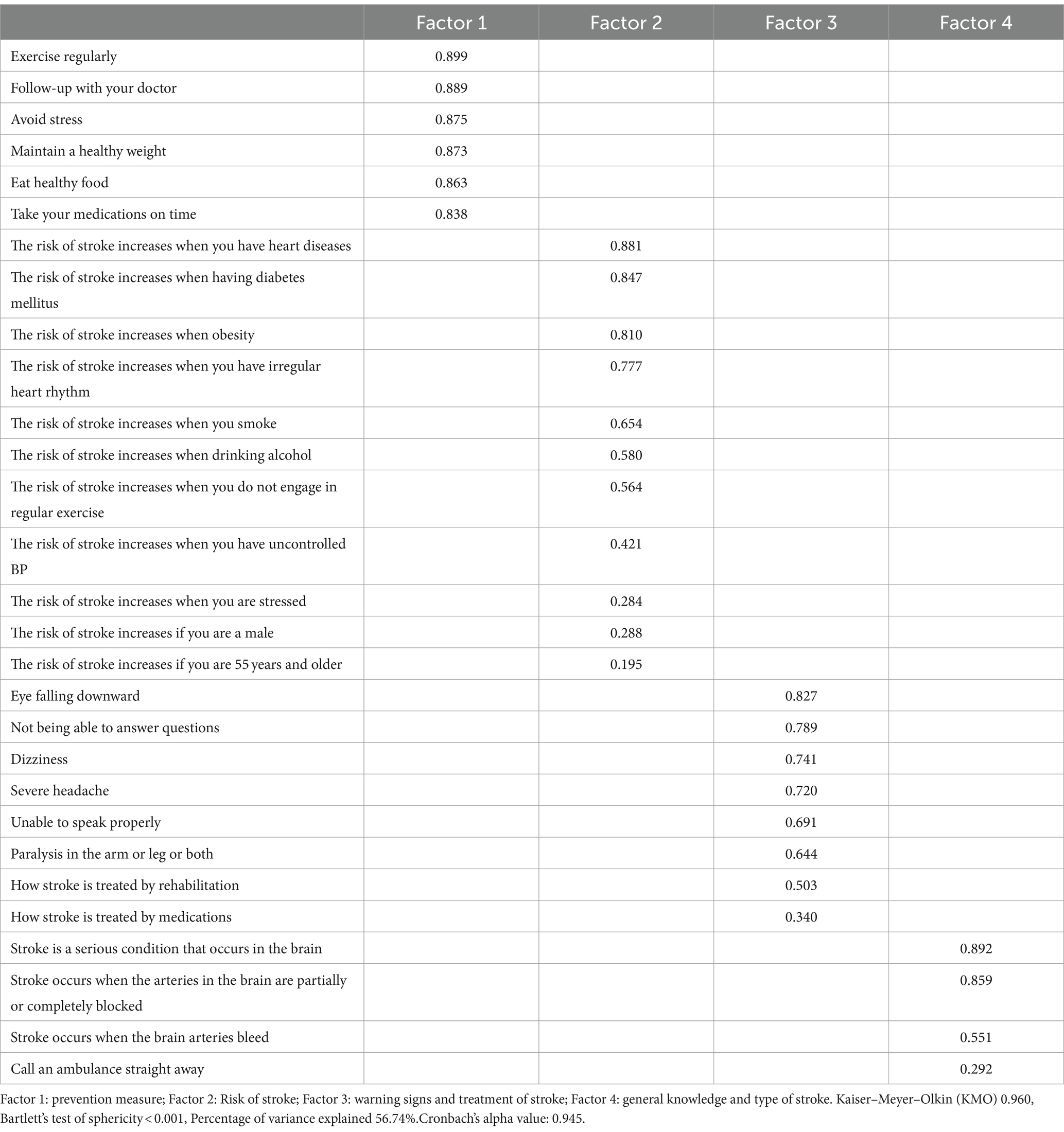
Table 1. Factor analysis of the knowledge of stroke (Promax rotated component matrix).
Ethical approval
The Institutional Review Board at Abu Dhabi University approved this study under the code number CoHS – 22-05-00018 on 16 May 2022. The study complies with the Declaration of Helsinki (24). Before filling out the online survey, participants were informed about the study objectives and the freedom to withdraw at any time. They also were informed that their participation is anonymous and voluntary. All participants filled out informed consent included at the beginning of the survey forms to enable proceeding with the survey. Participants did not receive any financial reward in exchange for their participation.
Statistical analysis
Data were analyzed using SPSS software version 25. The descriptive analysis used absolute frequencies and percentages for categorical variables and means and standard deviations (SD) for quantitative measures. As the skewness and kurtosis values of the dependent variables (knowledge total score) were under the acceptable range − 2 and + 2, so the data were considered normally distributed.
The paired sample t-test compared the stroke knowledge score before and after the education session. A repeated measures ANOVA evaluated the mean change of the stroke total knowledge before and after the educational video tool adjusted for covariates (age, gender, marital status, smoking, alcohol, education level, healthy lifestyle, having a stroke, family history of stroke, and having any medical illness). A bivariate analysis was conducted, taking the knowledge total score (pre, post, and the difference) as the dependent variables. Student’s T-test and ANOVA test were used in the bivariate analysis to compare two or more than three means. Cohen’s d effect size was calculated using the Psychometrica tool2. According to the effect size classification, a small effect was found for d = 0.2, medium d = 0.5, and large d ≥ 0.8. The post-hoc power was calculated using the G Power software. A p-value < 0.05 was considered significant.
Results
Demographic characteristics
A total of 2,721 participants were enrolled in the study from four Arab countries (Lebanon, UAE, Jordan, and Egypt). In Egypt and the UAE, sex-disaggregated responses are more balanced (approximately 50% women) than in Jordan and Lebanon, where the majority of respondents were women (≥63%). Nearly half or more of the participants were young, aged between 25 and 34 years, and almost all were highly educated (≥88%) but predominantly not healthcare providers (>66%) (Table 2).
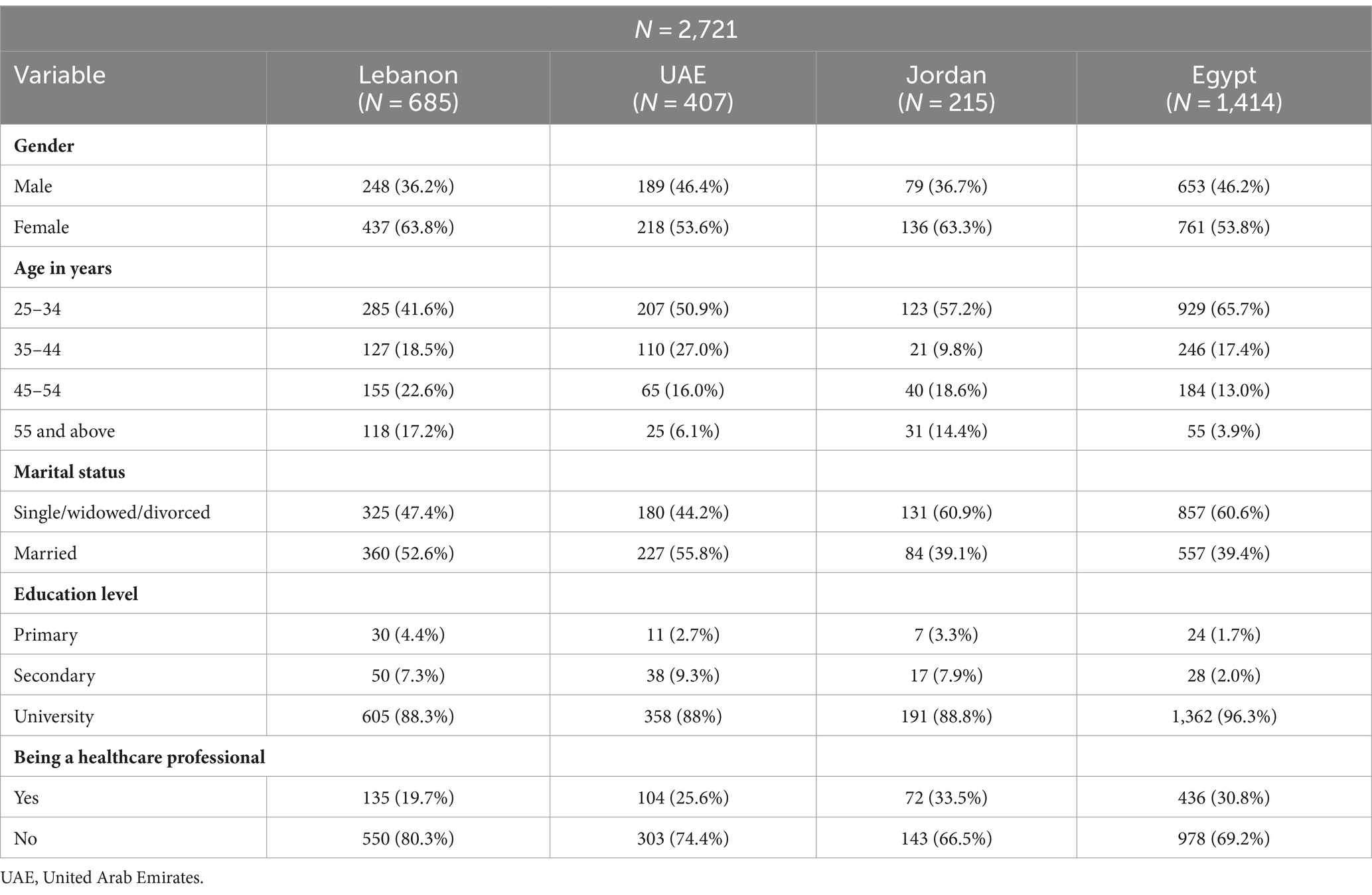
Table 2. Demographic characteristics of the participants.
Risks of stroke among participants
The majority of respondents were not at risk of developing stroke. They did not have a family history of stroke (>64%) or a previous stroke history (>96%). The majority of the participants were non-smokers and did not consume alcohol except 46.3% in Lebanon versus more than 84.8% in other countries. Nearly half of the people surveyed engage in mild physical activity and are either overweight or obese. Participants most frequently reported experiencing severe headaches, elevated cholesterol, and a family history of myocardial infarction (Table 3).
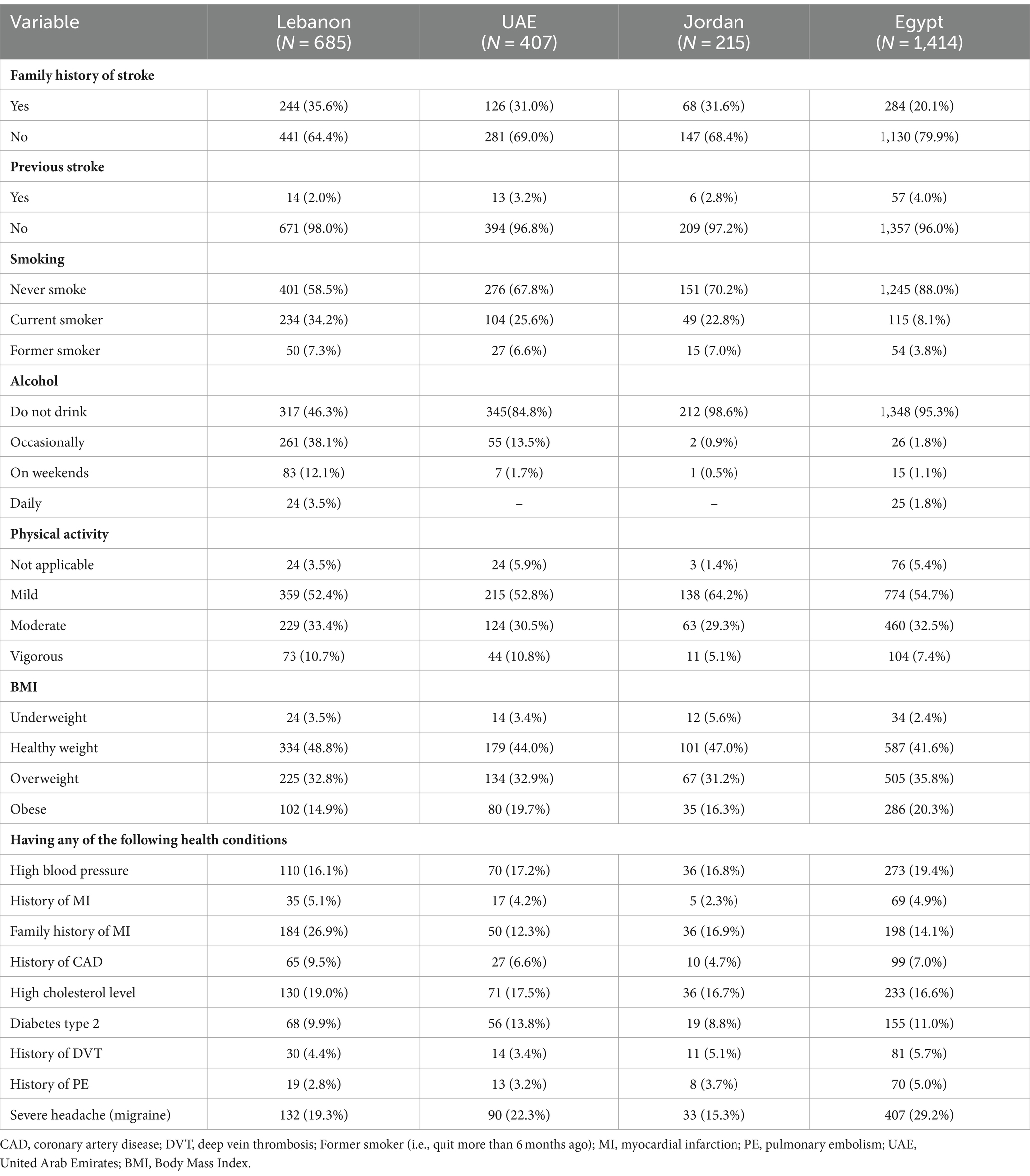
Table 3. Stroke risk factors among participants.
Comparison of stroke knowledge pretest and posttest
A significant increase was found post-education in the total knowledge score and among all knowledge items (p < 0.001), including stroke site of occurrence, types, risks, warning signs, prevention measures, treatment, and acting fast to save life (Table 4).

Table 4. Variation of the stroke knowledge pre- and post-education session.
Figure 1 shows the means of the knowledge total score before and after the educational session, after adjustment over age, gender, marital status, smoking, alcohol, education level, healthy lifestyle, having a stroke, a family history of stroke, and any medical illness. A significantly higher increase in the total knowledge score was found post-education in all countries (p < 0.05).
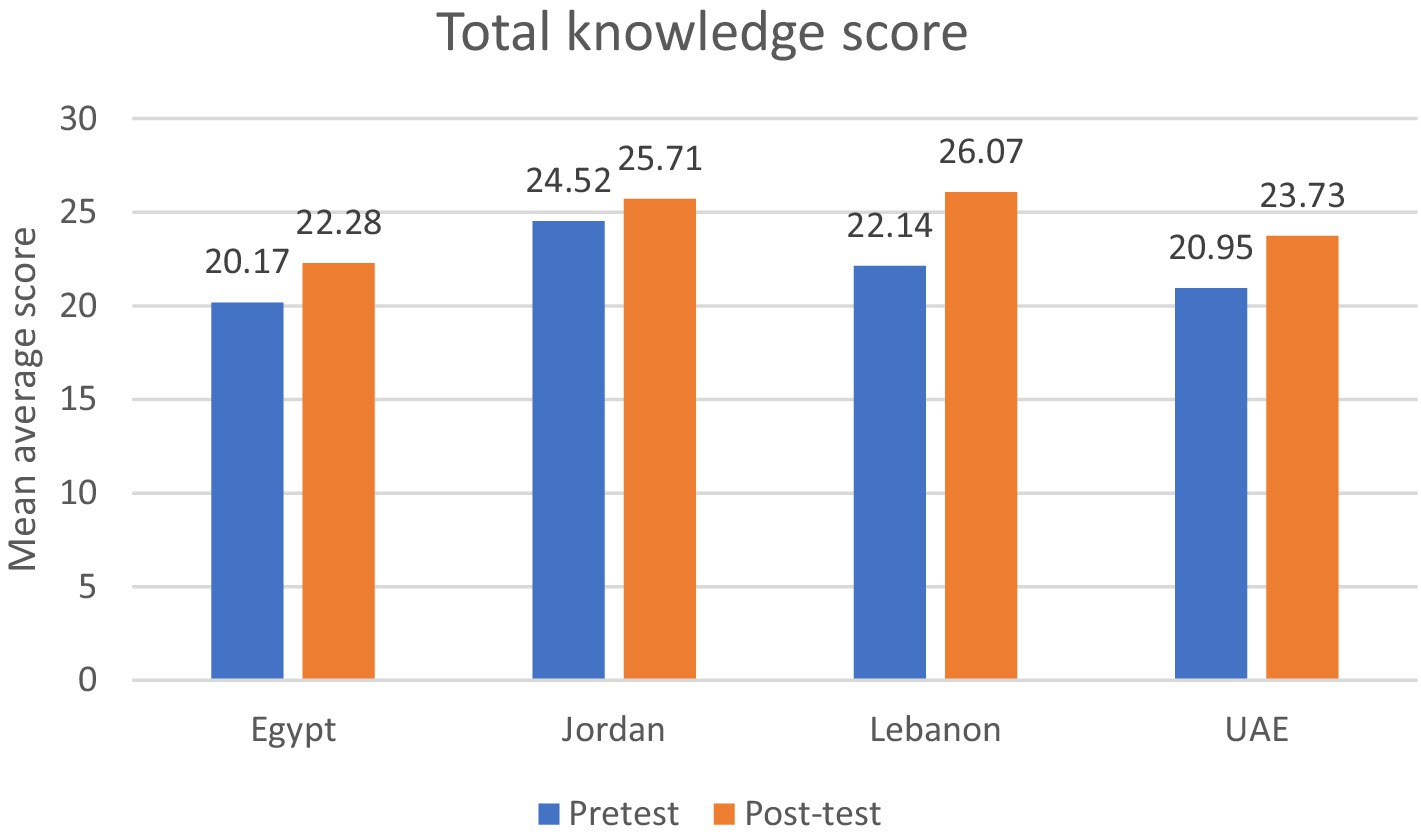
Figure 1. Differences in total knowledge pre-education and post-education scores among participating countries.
Bivariate analysis
The highest baseline mean knowledge score about stroke was found in Jordan (24.84 ± 4.55), followed by Lebanon (M = 22.26; SD = 6.22). The difference between the pre- and posttest was significant in all countries (p < 0.001). Although women had a higher baseline score (M = 21.67; SD = 7.15), the differences between pre and posttest were not significant for either gender (p = 0.353). The youngest participants (25–34 years) had a significantly lower mean knowledge score at baseline (M = 20.74; SD = 8.18) than participants 55 years and older (22.46 ± 6.00). There was no significant difference in the mean knowledge score between participants with and without a university degree, although highly educated participants had a higher baseline score (p = 0.425). Results showed that individuals who consumed alcohol had higher mean score differences (M = 3.12; SD = 5.21), while those with a low healthy lifestyle index had significantly higher knowledge scores (M = 2.68; SD = 5.40) (Table 5).
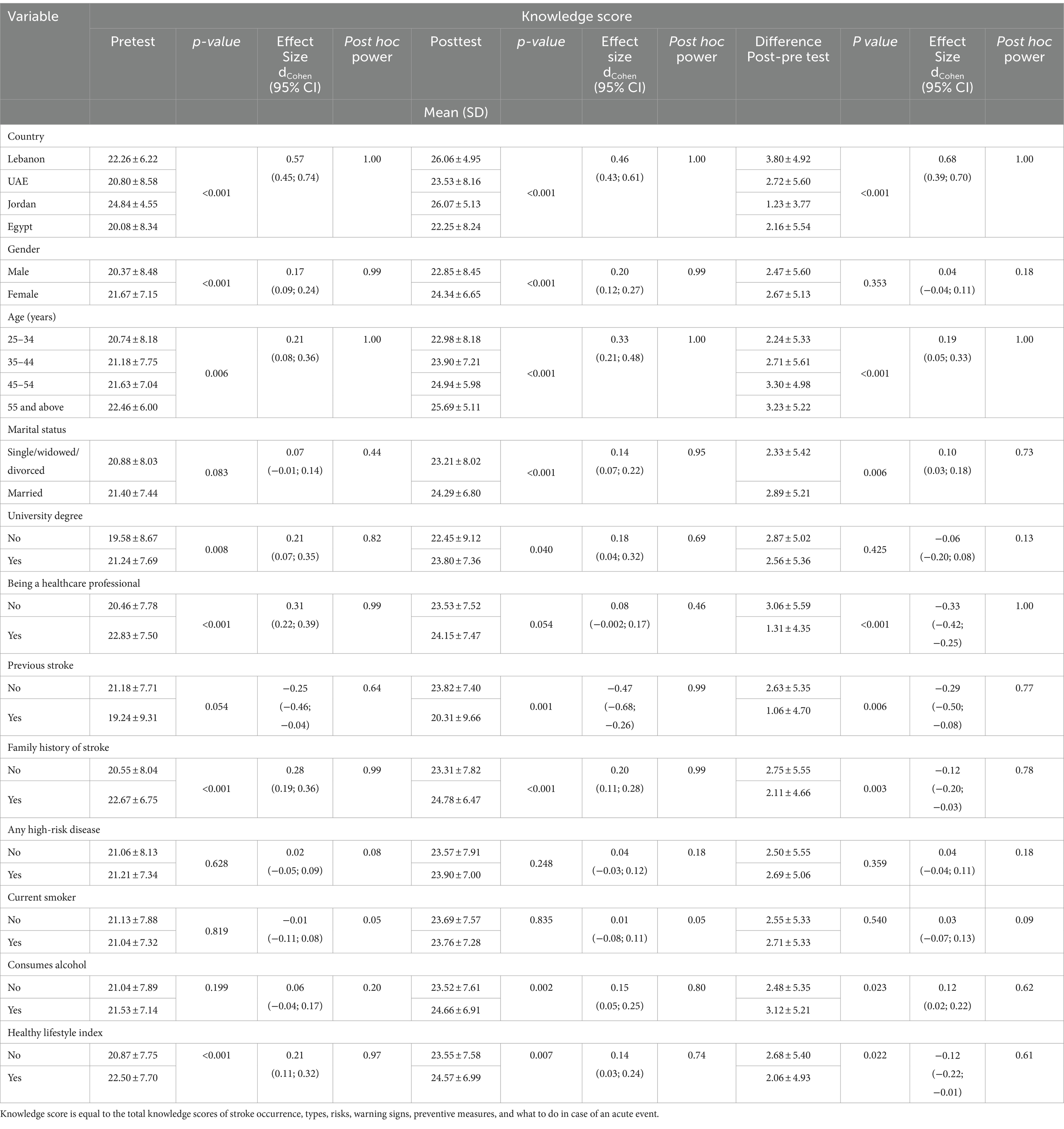
Table 5. Factors affecting the knowledge score.
Discussion
In this study, the educational video successfully improved stroke knowledge among highly educated participants from different age groups and Arab countries. The predominant originality includes its brevity (which maintains audience focus), evidence-based content (18–20, 23), and availability online free of charge in English and Arabic. The educational tool effectively delivered relevant information about stroke occurrence sites, types, risk factors, warnings, signs, preventive measures, and appropriate behavior in emergencies, as evidenced by the significant improvement in all knowledge scores. The use of lay language and suggestive images made the content easily understood by the public and healthcare professionals. Improving knowledge, especially at a young age, is crucial to raising awareness of inappropriate health behaviors that may increase the risk of stroke. It could also help save lives by identifying alarming signs in case of an event and understanding the importance of seeking emergency care.
The pretest knowledge scores varied across countries, with Jordan exhibiting the highest scores, followed by Lebanon, while Egypt and UAE had comparable knowledge. Previous research in Jordan had categorized the level of knowledge and awareness regarding stroke as good, particularly among those with a higher level of education (25). Conversely, studies conducted in Lebanon have reported poor knowledge in the general population, but not among participants with a university degree (26), a trend also observed among older adults (24). Similarly, in the present study, 88.3% of the Lebanese participants had a university degree. Unfortunately, campaigns intended to educate the general population are limited and lacking in Lebanon. Public education about stroke currently relies on academia and the scientific communities’ efforts (27, 28). Since awareness campaigns need general budgeting and planning, the main barriers in Lebanon are the ongoing economic downturn, the health system collapse, and the political crisis (29). In Egypt, a low level of stroke knowledge was reported across four governorates (30), with participants from urban areas demonstrating better knowledge than their rural counterparts (31). Egypt and the UAE have established strategies to manage, prevent, and improve awareness of stroke (32–34) (35–39). In Egypt, accredited stroke centers, including tele-stroke units and training and education centers, have been established in collaboration with the Wings of Angels initiative (32, 40). While the UAE is engaged in multiple awareness campaigns about stroke and is invested in stroke management and prevention plans through partnerships (33) and the implementation of centers for excellence (34), stroke knowledge was better among educated individuals than the general public (41).
The baseline knowledge of stroke varied across different age groups, with participants aged 55 years and above scoring the highest (M = 22.46; SD = 6.00) compared to those aged 25–34 years (M = 20.74; SD = 8.18). According to the World Health Organization (WHO), stroke is the second leading cause of death in individuals aged >60 years and the fifth in people aged 15–59 years (42). The youngest age group (25–34 years) may not be aware of the high incidence of stroke reported at this age, which can explain the lower scores compared with older adults. In the last decade, stroke has been increasingly documented in young adults (1, 2, 42), potentially due to higher incidences of preventable risk factors, such as smoking, obesity, hypertension, and dyslipidemia (2, 4). Therefore, there is a critical need for educating young adults about the risks associated with stroke and the importance of preventive measures.
The baseline knowledge scores were lower among non-healthcare professionals, participants who did not have a family history of stroke, and those who consumed alcohol or did not maintain a healthy lifestyle. Interestingly, the difference between the pretest and posttest scores was significantly higher. These results indicate that the 3-min educational video succeeded in capturing the attention of susceptible individuals and those who may not have prior knowledge of this topic.
Educational campaigns have consistently demonstrated a significant improvement in stroke knowledge, awareness, and appropriate emergency response behaviors (14, 15, 43). In addition to educational lectures (44), these campaigns have used various tools, including mass media (18–20, 44–46), social media platforms (44, 47), mobile applications (14, 15), pharmacy flyers (47), readings in schools and high schools (44), and advertisement in public transportation spots (48). Notably, mobile applications were well-received by healthcare professionals and individuals at risk of stroke (14, 15). In Western Norway, mass media intervention effectively enhanced awareness about acute stroke onset, as indicated by the increase in the number of admissions to the emergency room (35). However, sustaining this improvement necessitated repeated campaigns beyond the initial 6 months allocated (35). Similarly, regular mass media coverage was recommended in Hungary to educate the public about stroke instead of a 1-day campaign (36). The Stroke Foundation in Australia conducted annual paid advertisements from 2004 to 2014 using the FAST campaign to promote the need for emergency medical services, resulting in improved public awareness and behaviors (37). Similar positive effects were observed in New Zealand with the implementation of these campaigns (38). Worldwide national campaigns among the general public significantly improved knowledge of stroke (39, 43, 45, 46) and emergency response behaviors (10, 43). These campaigns varied in duration, from 1-week campaigns per year for 4 years to 50-month initiatives (31).
The design and implementation of educational campaigns for stroke vary based on the sustainability of financial support and the intended audience’s demographics, including age, sex, cultural background, level of education, and stroke risks (43, 48–51). Reading was the preferred way to acquire information in schools (44). In some cultures, social networking may be a way of communicating and enhancing awareness about the topic (49). Television remains a widely accepted and efficient means of education and communication, reaching a vast audience. Nevertheless, it is time-limited and requires repetition to convey the message and a dedicated budget for sustained campaigns (44, 45, 50, 51). Social media platforms offer enhanced communication and interaction among healthcare professionals and the community (47). Blogs, infographics, and videos shared on social media can reach a vast audience (47). However, the proliferation of infodemics and misinformation on social media can have adverse effects on individuals’ health-related behaviors (52, 53).
Finally, the main challenges in stroke education campaigns include the need for short-term non-repetitive campaigns, sustainable financial support, and an adequate educational approach tailored to the cultural background, age, sex, and level of education of the target audience. Educating children in schools and colleges is crucial to preparing a knowledgeable society for the future and influencing the parents’ behaviors. Engaging students in academic activities allows them to undertake periodic educational campaigns within their community as part of extra-curricular public health initiatives. This bundle of initiatives may be effective even without a budget or financial support.
Limitations
The limitations of the study are mainly the population distribution. Participants had predominantly a university degree, were 55 years and younger, and were women. Other limitations inherent to the study design include response bias and concerns related to data validity, as participants can get the information from another source, so the presence of an interviewer is preferable. The study design can also introduce selection bias, addressing the need to conduct randomized controlled trials to allow the generalizability of data findings. In addition, a comparison between intervention and control groups was not undertaken due to the study design limitations, lack of funding, and time constraints. Additional limitations include the short-term impact of this study, while detection of the tool’s long-term effectiveness in reducing disability, morbidity, and mortality and improving overall outcomes of stroke mandate a full-scale trial. Other limitations include a lack of long-term follow-up to verify the sustainability of the knowledge gained about stroke follow-up.
Practical implications
The educational video in this study showed how academia can play a crucial role in public health education without the need for a high budget. There is room for improvement if the government, professional societies, healthcare professionals, social workers, academia, students, and the community engage in awareness campaigns. If a budget is available, television and advertisements in public transportation, flyers distribution in pharmacies, stroke screening, and educational campaigns have proven effective. Regardless of budget constraints, school education and the role of academia, professional societies, and international organizations can secure a sustainable impact for a healthy society.
Conclusion
Educating the public about stroke has proven effective in enhancing knowledge and adapting appropriate behavior in case of an emergency. The main goal of this educational video in the short term is to improve community knowledge about stroke and the impact of inappropriate health behaviors, the identification of stroke signs, and action taken in case of an event. The mainstays are predominantly the sustainability and long-term effectiveness of this improvement in modifying inappropriate health behaviors and decreasing the risk of stroke morbidity and mortality. There is a need to capitalize on the strengths of this video and tailor its content to different cultural and educational backgrounds to reach all age groups. This tool can be part of a bundle of evidence-based interventions planned and implemented in collaboration with healthcare providers, the academic sector, governments, non-healthcare providers, and community engagement.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://doi.org/10.6084/m9.figshare.24551878.v2.
Ethics statement
The studies involving humans were approved by the institutional Review Board at Abu Dhabi University approved this study under the code number CoHS – 22-05-00018. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KI: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. DR: Validation, Writing – original draft. PS: Data curation, Formal analysis, Software, Validation, Writing – review & editing. CH: Data curation, Formal analysis, Software, Visualization, Writing – review & editing. HS: Writing – review & editing. MB: Investigation, Writing – review & editing. RD: Investigation, Writing – review & editing. SE: Investigation, Writing – review & editing. JS: Investigation, Writing – review & editing. FS: Investigation, Writing – review & editing. MR: Conceptualization, Validation, Writing – review & editing. HH: Conceptualization, Validation, Writing – review & editing. MC: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article from the University of Abu Dhabi, Abu Dhabi, United Arab Emirates.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^https://terrance.who.int/mediacentre/data/WHODAS/Guidelines/WHODAS%202.0%20Translation%20guidelines.pdf
References
1. Feigin, VL, Owolabi, MO, Feigin, VL, Abd-Allah, F, Akinyemi, RO, Bhattacharjee, NV, et al. Pragmatic solutions to reduce the global burden of stroke: a world stroke organization–lancet neurology commission. Lancet Neurol. (2023) 22:1160–206. doi: 10.1016/S1474-4422(23)00277-6
2. George, MG, Tong, X, and Bowman, BA. Prevalence of cardiovascular risk factors and strokes in younger adults. JAMA Neurol. (2017) 74:695–703. doi: 10.1001/jamaneurol.2017.0020
3. Ekker, MS, Boot, EM, Singhal, AB, Tan, KS, Debette, S, Tuladhar, AM, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol. (2018) 17:790–801. doi: 10.1016/S1474-4422(18)30233-3
4. Norrving, B, Davis, SM, Feigin, VL, Mensah, GA, Sacco, RL, and Varghese, C. Stroke prevention worldwide - what could make it work. Neuroepidemiology. (2015) 45:215–20. doi: 10.1159/000441104
5. Owolabi, MO, Thrift, AG, Martins, S, Johnson, W, Pandian, J, Abd-Allah, F, et al. The state of stroke services across the globe: report of world stroke organization–World Health Organization surveys. Int J Stroke. (2021) 16:889–901. doi: 10.1177/17474930211019568
6. Feigin, VL, Owolabi, M, Hankey, GJ, Pandian, J, and Martins, SC. Digital health in primordial and primary stroke prevention: a systematic review. Stroke. (2022) 53:1008–19. doi: 10.1161/STROKEAHA.121.036400
7. Stack, K, Robertson, W, and Blackburn, C. Does socioeconomic position affect knowledge of the risk factors and warning signs of stroke in the WHO European region? A systematic literature review. BMC Public Health. (2020) 20:1473. doi: 10.1186/s12889-020-09580-x
8. Patel, A. Awareness of stroke signs and symptoms and calling 9-1-1 among US adults: National Health Interview Survey, 2009 and 2014. Prev Chronic Dis. (2019) 16:E78. doi: 10.5888/pcd16.180564
9. Kharbach, A, Obtel, M, Achbani, A, Bouchriti, Y, Hassouni, K, Lahlou, L, et al. Level of knowledge on stroke and associated factors: a cross-sectional study at primary health care centers in Morocco. Ann Glob Health. (2020) 86:83. doi: 10.5334/aogh.2885
10. Lecouturier, J, Rodgers, H, Murtagh, MJ, White, M, Ford, GA, and Thomson, RG. Systematic review of mass media interventions designed to improve public recognition of stroke symptoms, emergency response and early treatment. BMC Public Health. (2010) 10:784. doi: 10.1186/1471-2458-10-784
11. Feigin, VL, Krishnamurthi, R, Medvedev, O, Merkin, A, Nair, B, Kravchenko, M, et al. Usability and feasibility of PreventS-MD web app for stroke prevention. Int J Stroke. (2024) 19:94–104. doi: 10.1177/17474930231190745
12. Medvedev, O, Truong, QC, Merkin, A, Borotkanics, R, Krishnamurthi, R, and Feigin, V. Cross-cultural validation of the stroke riskometer using generalizability theory. Sci Rep. (2021) 11:19064. doi: 10.1038/s41598-021-98591-8
13. Tan, J, Ramazanu, S, Liaw, SY, and Chua, WL. Effectiveness of public education campaigns for stroke symptom recognition and response in non-elderly adults: A systematic review and Meta-analysis. J Stroke Cerebrovasc Dis. (2022) 31:106207. doi: 10.1016/j.jstrokecerebrovasdis.2021.106207
14. Di Carlo, A, Baldereschi, M, Bovis, F, Piccardi, B, Linoli, G, Orlandi, G, et al. Effect of an educational intervention to increase stroke awareness among Italian high school students: A prospective study in Tuscany. Eur Stroke J. (2023) 8:769–76. doi: 10.1177/23969873231175405
15. Caminiti, C, Schulz, P, Marcomini, B, Iezzi, E, Riva, S, Scoditti, U, et al. Development of an education campaign to reduce delays in pre-hospital response to stroke. BMC Emerg Med. (2017) 17:20. doi: 10.1186/s12873-017-0130-9
16. Van Der, MJ, Tsakpounidou, K, Baskini, M, Webb, C, Keramydas, C, Martins, SCO, et al. Continuity and change in baseline stroke knowledge across the world: second wave of FAST heroes campaign implementation. J Stroke Cerebrovasc Dis. (2023) 32:107426. doi: 10.1016/j.jstrokecerebrovasdis.2023.107426
17. Oostema, JA, Chassee, T, Baer, W, Edberg, A, and Reeves, MJ. Brief educational intervention improves emergency medical services stroke recognition. Stroke. (2019) 50:1193–200. doi: 10.1161/STROKEAHA.118.023885
18. American Stroke Association. Community Stroke Prevention Toolkit. Stroke (2023). Available at: https://www.stroke.org/en/help-and-support/resource-library/prevention-toolkit (Accessed March 27, 2024)
19. Aroor, S, Singh, R, and Goldstein, LB. BE-FAST (balance, eyes, face, arm, speech, time). Stroke. (2017) 48:479–81. doi: 10.1161/STROKEAHA.116.015169
20. Stroke Foundation New Zealand. Think F.A.S.T., act fast. Stroke Foundation New Zealand. Available at: https://www.stroke.org.nz/think-fast-act-fast (Accessed March 27, 2024)
22. Fukunaga, A, Inoue, Y, Chandraratne, N, Yamaguchi, M, Kuwahara, K, Indrawansa, S, et al. Healthy lifestyle index and its association with hypertension among community adults in Sri Lanka: A cross-sectional study. PLoS One. (2020) 15:e0226773. doi: 10.1371/journal.pone.0226773
23. National Institute of Neurological Disorders and Stroke. Stroke. NINDS. Available at: https://www.ninds.nih.gov/health-information/disorders/stroke (Accessed March 27, 2024)
24. Khalil, HM, and Lahoud, N. Knowledge of stroke warning signs, risk factors, and response to stroke among Lebanese older adults in Beirut. J Stroke Cerebrovasc Dis. (2020) 29:104716. doi: 10.1016/j.jstrokecerebrovasdis.2020.104716
25. Barakat, M, AlSalamat, H, Jirjees, F, al-Obaidi, H, Hussain, Z, el Hadidi, S, et al. Factors associated with knowledge and awareness of stroke among the Jordanian population: a cross-sectional study. F1000Res. (2022) 10:1242. doi: 10.12688/f1000research.74492.2
26. Saade, S, Hallit, S, Salameh, P, and Hosseini, H. Knowledge and response to stroke among Lebanese adults: a population-based survey. Front Public Health. (2022) 10:891073. doi: 10.3389/fpubh.2022.891073
27. Malaeb, D, Dia, N, Haddad, C, Hallit, S, Sacre, H, Barakat, M, et al. Factors associated with knowledge and awareness of stroke among the Lebanese population: A cross-sectional study. F1000Res. (2022) 11:425. doi: 10.12688/f1000research.108734.2
28. Batakji, R. World stroke day 2021: Act FAST, treat and prevent. LAU (2021). Available at: https://news.lau.edu.lb/2021/world-stroke-day-2021-act-fast-treat-and-prevent.php (Accessed March 27, 2024)
29. Akar, B. LCPS - higher education in Lebanon: Struggling to survive in times of crises. The Lebanese Center for Policy Studies (2023). Available at: https://www.lcps-lebanon.org/articles/details/4784/higher-education-in-lebanon-struggling-to-survive-in-times-of-crises (Accessed March 27, 2024)
30. Farrag, MA, Oraby, MI, Ghali, AA, Ragab, OA, Nasreldein, A, Shehata, GA, et al. Public stroke knowledge, awareness, and response to acute stroke: multi-center study from 4 Egyptian governorates. J Neurol Sci. (2018) 384:46–9. doi: 10.1016/j.jns.2017.11.003
31. Elhassanien, MEM, Ghali, AA, Shaheen, AK, Ali, DA, Sabra, HK, Motawea, SH, et al. Public stroke awareness among Gharbia governorate inhabitants: a cross-sectional study. Egypt J Neurol Psychiatry Neurosurg. (2023) 59:27. doi: 10.1186/s41983-023-00629-3
32. Aref, H, Zakaria, M, Shokri, H, Roushdy, T, El Basiouny, A, and El Nahas, N. Changing the landscape of stroke in Egypt. Cerebrovascular Diseases Extra. (2021) 11:155–9. doi: 10.1159/000521271
33. Release, P. Dubai children to become FAST heroes as part of a global stroke awareness initiative (2021). Available at: https://www.zawya.com/en/press-release/dubai-children-to-become-fast-heroes-as-part-of-a-global-stroke-awareness-initiative-e7ykpkh5 (Accessed March 27, 2024)
34. Kumar, A. UAE: Two hospitals designated as stroke centres of excellence in Abu Dhabi. Khaleej Times (2023). Available at: https://www.khaleejtimes.com/lifestyle/health/uae-two-hospitals-designated-as-stroke-centres-of-excellence-in-abu-dhabi (Accessed March 27, 2024)
35. Advani, R, Naess, H, and Kurz, M. Mass media intervention in Western Norway aimed at improving public recognition of stroke, emergency response, and acute treatment. J Stroke Cerebrovasc Dis. (2016) 25:1467–72. doi: 10.1016/j.jstrokecerebrovasdis.2016.02.026
36. Folyovich, A, Biczó, D, Béres-Molnár, KA, and Toldi, G. Assessment of the efficiency of stroke awareness campaigns in Hungary. J Stroke Cerebrovasc Dis. (2018) 27:1770–4. doi: 10.1016/j.jstrokecerebrovasdis.2018.02.006
37. Bray, JE, Finn, J, Cameron, P, Smith, K, Straney, L, Cartledge, S, et al. Temporal trends in emergency medical services and general practitioner use for acute stroke after Australian public education campaigns. Stroke. (2018) 49:3078–80. doi: 10.1161/STROKEAHA.118.023263
38. Gordon, C, Bell, R, and Ranta, A. Impact of the national public “FAST” campaigns. N Z Med J. (2019) 132:48–56. Available at: https://global-uploads.webflow.com/5e332a62c703f653182faf47/5e332a62c703f639082fdc20_NZMJ%201507%20FINAL.pdf
39. Haesebaert, J, Laude, C, Termoz, A, Bravant, E, Perreton, N, Bony, T, et al. Impact of a theory-informed and user-centered stroke information campaign on the public’s behaviors, attitudes, and knowledge when facing acute stroke: a controlled before-and-after study. BMC Public Health. (2020) 20:1712. doi: 10.1186/s12889-020-09795-y
40. Hacke, W, Caso, V, Esagunde, RU, Aref, H, Martins, SCO, and Mikulik, R. Stroke care taking flight with the wings of ANGELS (2021). Available at: https://www.oruen.com/, https://www.oruen.com/neurology/stroke/stroke-care-taking-flight-with-the-wings-of-angels, https://www.oruen.com/neurology/stroke/stroke-care-taking-flight-with-the-wings-of-angels (Accessed March 27, 2024)
41. Jirjees, F, Al-Obaidi, H, Barakat, M, Kharaba, Z, AlSalamat, H, Khidhair, Z, et al. Knowledge and awareness of stroke in the United Arab Emirates: a cross-sectional study of the general population. F1000Res. (2023) 12:1112. doi: 10.12688/f1000research.134328.2
42. World Health Organization. The top 10 causes of death (2020). Available at: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (Accessed March 27, 2024)
43. Hickey, A, Mellon, L, Williams, D, Shelley, E, and Conroy, RM. Does stroke health promotion increase awareness of appropriate behavioural response? Impact of the face, arm, speech and time (FAST) campaign on population knowledge of stroke risk factors, warning signs and emergency response. Eur Stroke J. (2018) 3:117–25. doi: 10.1177/2396987317753453
44. Khan, F, Gaowgzeh, RAM, Saif, AA, Chevidikunnan, MF, Soman, A, Mazi, A, et al. Effect of community education program on stroke symptoms and treatment on school and college students from South India: a longitudinal observational study. Healthcare. (2021) 9:1637. doi: 10.3390/healthcare9121637
45. Hodgson, C, Lindsay, P, and Rubini, F. Can mass media influence emergency department visits for stroke? Stroke. (2007) 38:2115–22. doi: 10.1161/STROKEAHA.107.484071
46. Komolafe, MA, Obembe, AO, Olaogun, MO, Adebiyi, AM, Ugalahi, T, Dada, O, et al. Awareness of stroke risk factors and warning signs in Nigerian adolescents compared with adults. J Stroke Cerebrovasc Dis. (2015) 24:687–93. doi: 10.1016/j.jstrokecerebrovasdis.2014.11.013
47. Cabrera-Maqueda, JM, and Minhas, JS. New horizons for stroke medicine: understanding the value of social media. Stroke. (2018) 49:e25–7. doi: 10.1161/STROKEAHA.117.020068
48. Worthmann, H, Schwartz, A, Heidenreich, F, Sindern, E, Lorenz, R, Adams, H-A, et al. Educational campaign on stroke in an urban population in northern Germany: influence on public stroke awareness and knowledge. Int J Stroke. (2013) 8:286–92. doi: 10.1111/j.1747-4949.2012.00809.x
49. Pandian, JD, Jaison, A, Deepak, SS, Kalra, G, Shamsher, S, Lincoln, DJ, et al. Public awareness of warning symptoms, risk factors, and treatment of stroke in Northwest India. Stroke. (2005) 36:644–8. doi: 10.1161/01.STR.0000154876.08468.a0
50. Alaqeel, A, AlAmmari, A, AlSyefi, N, Al-Hussain, F, and Mohammad, Y. Stroke awareness in the Saudi community living in Riyadh: prompt public health measures must be implemented. J Stroke Cerebrovasc Dis. (2014) 23:500–4. doi: 10.1016/j.jstrokecerebrovasdis.2013.04.011
51. Silver, FL, Rubini, F, Black, D, and Hodgson, CS. Advertising strategies to increase public knowledge of the warning signs of stroke. Stroke. (2003) 34:1965–8. doi: 10.1161/01.STR.0000083175.01126.62
52. World Health Organization. Infodemics and misinformation negatively affect people’s health behaviours, new WHO review finds. WHO News (2022). Available at: https://www.who.int/europe/news/item/01-09-2022-infodemics-and-misinformation-negatively-affect-people-s-health-behaviours--new-who-review-finds (Accessed March 27, 2024).
Keywords: stroke, knowledge, video, educational tool, Arab countries
Citation: Iskandar K, Rahme D, Salameh P, Haddad C, Sacre H, Bahlol M, Darwish RM, El Khatib S, Safwan J, Sakr F, Rahhal M, Hosseini H and Cherfane M (2024) Evaluating the influence of a 3-min online video on the community knowledge of stroke in four Arab countries. Front. Public Health. 12:1342490. doi: 10.3389/fpubh.2024.1342490
Edited by:
Mohan Bairwa, All India Institute of Medical Sciences, IndiaReviewed by:
Abolfazl Avan, Western University, CanadaIntan Idiana Hassan, Universiti Sains Malaysia Health Campus, Malaysia
Ahmed Kharbach, Mohammed V University at Souissi, Morocco
Copyright © 2024 Iskandar, Rahme, Salameh, Haddad, Sacre, Bahlol, Darwish, El Khatib, Safwan, Sakr, Rahhal, Hosseini and Cherfane. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katia Iskandar, a2F0aWFfaXNrYW5kYXJAaG90bWFpbC5jb20=
†ORCID: Katia Iskandar, https://orcid.org/0000-0001-5544-6681
Deema Rahme, https://orcid.org/0000-0003-4245-9699
Pascale Salameh, https://orcid.org/0000-0002-4780-0772
Chadia Haddad, https://orcid.org/0000-0002-6438-0159
Hala Sacre, https://orcid.org/0000-0003-2413-2684
Sarah El Khatib, https://orcid.org/0000-0001-6547-6251
Jihan Safwan, https://orcid.org/0000-0001-8599-1103
Hassan Hosseini, https://orcid.org/0000-0002-8602-1042
Michelle Cherfane, https://orcid.org/0000-0002-2169-3788