 Alexander Avian
Alexander Avian Clemens Könczöl2
Clemens Könczöl2 Bettina Kubicek
Bettina Kubicek Ulrike Spary-Kainz
Ulrike Spary-Kainz- 1Institute for Medical Informatics, and Statistics and Documentation, Medical University of Graz, Graz, Austria
- 2Institute of Psychology, University of Graz, Graz, Austria
- 3Institute of General Practice and Evidence-based Health Services Research, Medical University of Graz, Graz, Austria
- 4Institute of General Practice, Goethe University Frankfurt, Frankfurt am Main, Germany
Background: Since the beginning of the pandemic in December 2019, Coronavirus disease 2019 (COVID-19) has been a significant challenge to health care systems throughout the world. The introduction of measures to reduce the incidence of infection had a significant impact on the workplace. Overall, companies played a key and adaptive role in coping with the pandemic.
Methods: Cross-sectional data from an online-survey of 1,183 employees conducted during the COVID-19 pandemic in spring 2021 in Austria were used in the analyses. The influence of health beliefs (e.g., perceived severity), modifying factors (e.g., age) and time-dependent factors (e.g., corona fatigue) on individual adherence were evaluated. The conception of the questionnaire was based on the health belief model.
Results: The majority of respondents were female (58.3%), worked in companies with more than 250 employees (56.6%) and had been to an academic secondary school or had a university degree (58.3%). Overall, employees were adherent to most of the measures at their company (>80%), except for wearing FFP-2 masks when they were travelling in a car with coworkers (59.3, 95%CI 51.3–66.7%). Overall adherence was associated with high ratings for the meaningfulness of testing (OR: 2.06 95%CI: 1.00–4.22; p = 0.049), the extent to which social norms govern behavior (OR: 6.61 95%CI: 4.66–9.36; p < 0.001), lower perceived difficulties associated with the adoption of health-promoting measures (OR: 0.37 95%CI: 0.16–0.82; p = 0.015) and lower corona fatigue (OR: 0.23 95%CI: 0.10–0.52; p < 0.001). Adherence to four single measures was influenced by different predictors. The most important predictors (important for the adherence to three out of four single measures) were social norms and corona fatigue.
Conclusion: The importance attached to testing and social norms, as well as lower perceived barriers to health-promoting measures and low levels of corona fatigue all increase overall adherence to Covid-19 protective measures in companies. Strategies to improve adherence should be adapted depending on the aim (to raise overall adherence or adherence to individual measures) and on the group of persons that is being targeted.
1 Introduction
Since the beginning of the pandemic in December 2019, Coronavirus disease 2019 (COVID-19) has been a significant challenge to health care systems throughout the world (1–9). To slow down transmission rates, almost all governments developed a prevention strategy of some kind, as recommended by the World Health Organization (WHO) (10).
The corona pandemic and associated measures have become a global public health issue and have disrupted people’s daily lives and work, and severely damaged the global economy (11, 12). Companies were faced with such hitherto unknown challenges as the requirement to close down facilities, deal with greater numbers of employees off sick (13), and further health-promoting measures such as short-time work, teleworking (14), and personal protection (e.g., wearing masks, testing, distancing). As early as March 2020, the WHO issued simple recommendations to employers that were aimed at preventing the spread of Covid-19 (15), and other organizations such as the International Labor Organization followed suit with additional guidance for employers on how to protect their employees from infection in the workplace (16, 17).
The introduction of measures to reduce the incidence of infection had a significant impact on the workplace. While the closure of enterprises had a direct economic affect, the wearing of masks, the introduction of tests and the opportunity to work from home at least enabled enterprises to continue operating at reduced risk of infection for employees. A rapid review and meta-analyses published by Ingram provided evidence that a combination of SARS-CoV-2 infection prevention and control measures resulted in fewer Covid-19 infections among employees, especially when timely and widespread contact tracing and isolation was combined with smaller worker cohorts and adequate personal protective equipment (18).
Overall, companies played a key and adaptive role in coping with the pandemic. One longitudinal study of full-time employees in Japan showed that the implementation of health-promoting measures in companies varied over time, with an increase in the first phase in spring 2020 (19), steady rates during the summer, and a decrease in preventive measures between summer and November 2020 (20). We also know that adherence to some measures in the general population steadily decreased towards the end of the pandemic (21–23). Already at the beginning of the pandemic from April to May 2020 adherence decreased from 66%% to 33–38% in a Norwegian cohort (23). In a Spanish cohort, it could be shown that less people showed preventing behavior like disinfecting surfaces (42% vs. 55%) and washing hands often with soap and water (81% vs. 85%) in the end of 2020 compared to 2 months before (22). Adherence data from employees at work are rare, but a huge study of over 50,000 people performed in the UK showed that low rates of teleworking were associated with lower than average compliance, and high rates of teleworking with higher than average compliance with preventive measures (24).
The health belief model (25) offers one way to explain individual health behavior like adherence to measures. This model includes factors such as perceived susceptibility, perceived severity, perceived benefits, perceived barriers and cues to action, has often been used to explain differences in adherence. Zewdie et al. (26) concluded in their review that the health belief model can explain a large part of the variation in people’s behavior regarding COVID-19 preventive behavior with perceived benefit being the most important predictor, followed by self efficacy. Looking on specific behaviors Limbu et al. (27) showed in their review, that COVID-19 vaccine hesitancy reinforced by perceived barriers and mitigated by perceived benefits, perceived severity. Conflicting results were found for perceived susceptibility. Self-efficacy has only rarely been studied and has also shown an mitigated effect. Regarding modifying variables female sex was found to increase vaccine hesitancy. Other modifying factors have rarely been examined (e.g., social norms) or shown conflicting results (income). Liang et al. (28) investigated in their review different behaviors (hand hygiene, face mask wearing, physical distancing) and found that knowledge, positive attitudes and perceived norms increased adherent behavior for all three examined behaviors. Perceived susceptibility showed no effect, perceived severity and perceived control mixed effects. Self-efficacy (increased adherent behavior) and negative attitudes (no effect) were only investigated for hand hygiene and physical distancing. Aside from these population-wide studies, there are less studies that explicitly address the workplace and these mostly relate to the medical sector [(e.g., 29–31)] or students [(e.g., 32, 33)]. This study is based on the adapted health belief model (34) and aims to confirm known and identify new factors influencing adherence at the workplace among employees in Austria.
2 Methods
Cross-sectional data from an online-survey of 1,183 employees conducted during the COVID-19 pandemic in spring 2021 in Austria were used in the analyses. The questionnaire was based on the health belief model (HBM) and adapted for use in COVID-19 research by Hsing et al. (35) and Siebenhofer et al. (34). In the present version, health behavior (e.g., adherent behavior) is explained by health beliefs beliefs (e.g., perceived severity), modifying factors (e.g., age) and time-dependent factors (e.g., corona fatigue). According to national legislation and institutional requirements, no ethical approval was required for this study.
2.1 Questionnaire
The final questionnaire consisted of general items to be answered by all participants and items to which responses were only required from those that had given certain answers to the general questions. All employees were asked about their perceived susceptibility (1 item), perceived severity (3 items), corona fatigue (6 items) (36), meaningfulness of measures (7 items), information and participation at their company (2 items) (34), specific measures (8 items), social norms (1 item), and company support (1 item), as well as their individual work situation (e.g., whether an employee worked in the same room as others, dealt directly with customers etc.). Employees from which more detail was required were asked further questions about perceived barriers (12 items), social norms (4 items), company support (2 items), and specific measures (13 items). A translated version of the German questionnaire can be found in the Supplement. Explorative factor analysis (VARIMAX rotation) was carried out separately for all aspects apart from sociodemographic variables and aspects about which only one question was asked. Internal consistency (Cronbach’s alpha) was calculated for each factor.
2.1.1 Adherence
Since the working situation differed between respondents and therefore involved different measures, respondents’ adherence also varied. Employees’ responses varied between 0 measures (9 employees) and 7 (1 employee). Most employees reported 2 (n = 434) or 3 (n = 433) measures. Since it made little sense to add up these responses to provide an overall score, employees were divided into two groups. The first group consisted of employees that were adherent to all measures that were relevant to them, while employees that did not follow all relevant measures were assigned to the other group (non-adherent).
2.1.2 Health beliefs
Ten items were used to assess three aspects of the adapted health belief model (perceived severity, perceived susceptibility, perceived barriers). To assess perceived severity, respondents were first asked to compare COVID-19 to influenza (response format: harmless / comparable / more dangerous), and then to assess their personal health risk and the economic risk resulting from measures to combat the coronavirus on a 5-point Likert type response scale. No satisfactory result could be achieved in the factor analysis of perceived severity. The three perceived severity items were therefore analyzed separately.
Perceived susceptibility was assessed using a single item (response format: not at all / slightly / high). To evaluate perceived barriers due to health-promoting measures, respondents were asked whether they were required to adhere to specific measures (e.g., testing themselves before coming to work; checking whether customers had a negative corona test; wearing FFP-2 masks when driving with others; wearing FFP-2 masks at work). If a respondent was expected to carry out at least one of these measures, one of them was randomly chosen and he or she was asked whether they thought the measures were annoying, unnecessarily strict, would prevent the virus from spreading, had been scientifically proven to be effective, violated legal regulations, and were feasible in reality (response format: yes / partly / no). The first four items could be assigned to one factor (Cronbach’s α =0.855). The other two items were assigned to another (practicability of health-promoting measures), whereby the latter had too little internal consistency (α = 0.343) to be considered in the further analysis.
2.1.3 Modifying factors
The following demographic variables were assessed: age (years), gender (female, male, other), educational levels (EL1: compulsory education including those with no school leaving certificate, EL2: apprenticeship, EL3: higher vocational education, EL4: academic secondary school, EL5: university) and number of employees at the company [less than 10 (micro companies) – 10 to 49 (small companies) – 50 to 249 (medium-sized companies) – 250 and more (large companies)].
2.1.4 Time-dependent factors
The corona fatigue aspect contained all six items from Lilleholt’s corona fatigue questionnaire (36) and has a two-dimensional structure (information fatigue, behavioral fatigue). Since this survey was part of a bigger project involving an additional telephone survey, the response formats were adapted to make responses to a telephone survey easier. In this study, the response format was simplified to: agree / partly agree / do not agree. Since the factors proposed by Lilleholt et al. (36) only had an internal consistency of α = 0.717 (information fatigue) and α = 0.695 (behavioral fatigue), exploratory factor analysis was also used to analyze the six items. This resulted in a one-factor model (α = 0.811).
2.2 Survey
The questionnaire was transferred to SurveyMonkey. Potential respondents came from one Austrian state (Vorarlberg), whereby smaller companies were selected by the Chamber of Commerce (membership mandatory for all companies) and Chamber of Labor (membership mandatory for all employees) and the Vorarlberg Society for General Practice, and larger companies by members of the works council and the staff manager. The cooperating institutions contacted the potential respondents independently. Therefore, on the one hand, there could have been multiple contacts with the same person through different institutions. On the other hand, it may also be that certain groups of people were not contacted. Furthermore we had no control whether or not reminders were send to potential respondents. Media channels (newspapers and television) were also used for promoting the study. Potential respondents answered the survey from June 1 to June 27, 2021. The online-survey was conducted by a professional research center (L&R Sozialforschung).
2.3 Statistics
Baseline characteristics (demographic variables) are presented as mean ± SD or median (IQR), as appropriate. Categorical variables are provided as absolute and relative numbers. In order to identify independent predictors for adherent behavior (outcome of interest) respondents were grouped into an “adherent group” and a “non adherent group.” The adherent group consisted of employees that were adherent to all measures that were relevant to them, while employees that did not follow all relevant measures were assigned to the non-adherent group. In a first step, univariate logistic regression analysis was performed, with adherence serving as the outcome (adherent group vs. not adherent group). Predictors were the factors and the single-item aspects described above, along with sociodemographic variables. To enhance comparability, all dichotomous factors and single-item aspects apart from age were transformed to fit into a range of 0 to 1. To ensure the resulting betas were comparable, the age variable was therefore divided by 100. Significant univariate predictors were checked for multicollinearity (variance inflation factor < 2.5). Remaining variables were included in a multivariate regression analysis (backwards selection). Exploratory also the influence of the predictors on each individual measure (logistic regression analysis: Model 1: outcome: testing for work; model 2: outcome: wearing of FFP2 masks; model 3: outcome: treatment of customers; model 4: outcome: social distancing). For this analysis, significant univariate predictors were also checked for multicollinearity (variance inflation factor < 2.5). The remaining variables were subjected to multivariate logistic regression analysis (backwards selection). SPSS 26 was used in data analysis (IBM Corp, 2019), and a value of p < 0.05 was considered significant.
3 Results
3.1 Demographics
Overall 1,183 employees answered the survey. The majority of respondents were female (n = 690, 58.3%), worked in companies with more than 250 employees (n = 669, 56.6%) and had been to an academic secondary school or had a university degree (n = 690, 58.3%). Detailed demographic information is provided in Table 1.
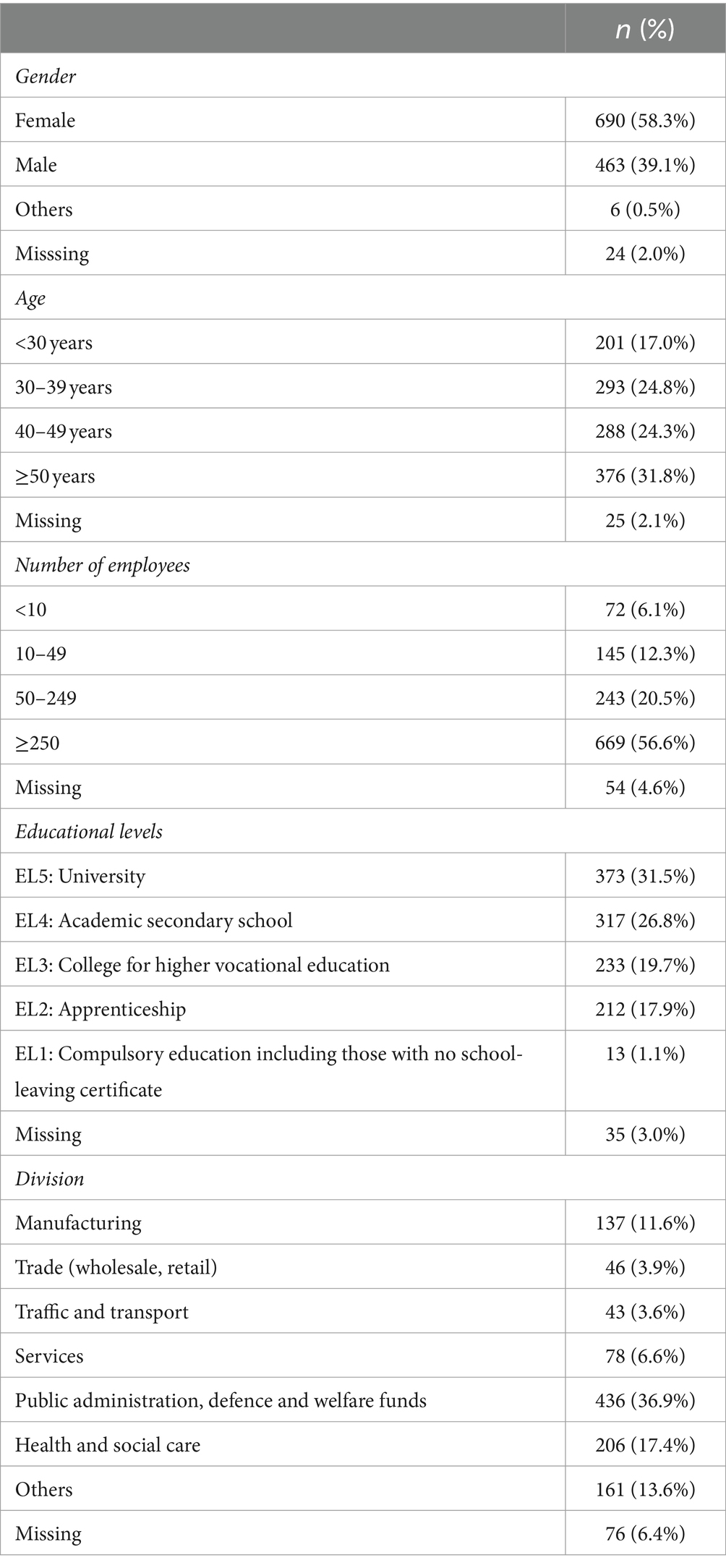
Table 1. Baseline characteristics of responders (n = 1,183).
Overall, employees were adherent to most of the measures at their company, except for wearing FFP-2 masks when they were travelling in a car with coworkers (in a car during worktime: 59.3, 95%CI 51.3–66.7%; in a car on the way to work: 54.6, 95%CI: 44.5–63.0%). The other measures were adhered to by more than 80% of employees (Figure 1). Furthermore 60.4% (95%CI: 57.4–63.2%) said their co-workers adhered to the measures at their company.
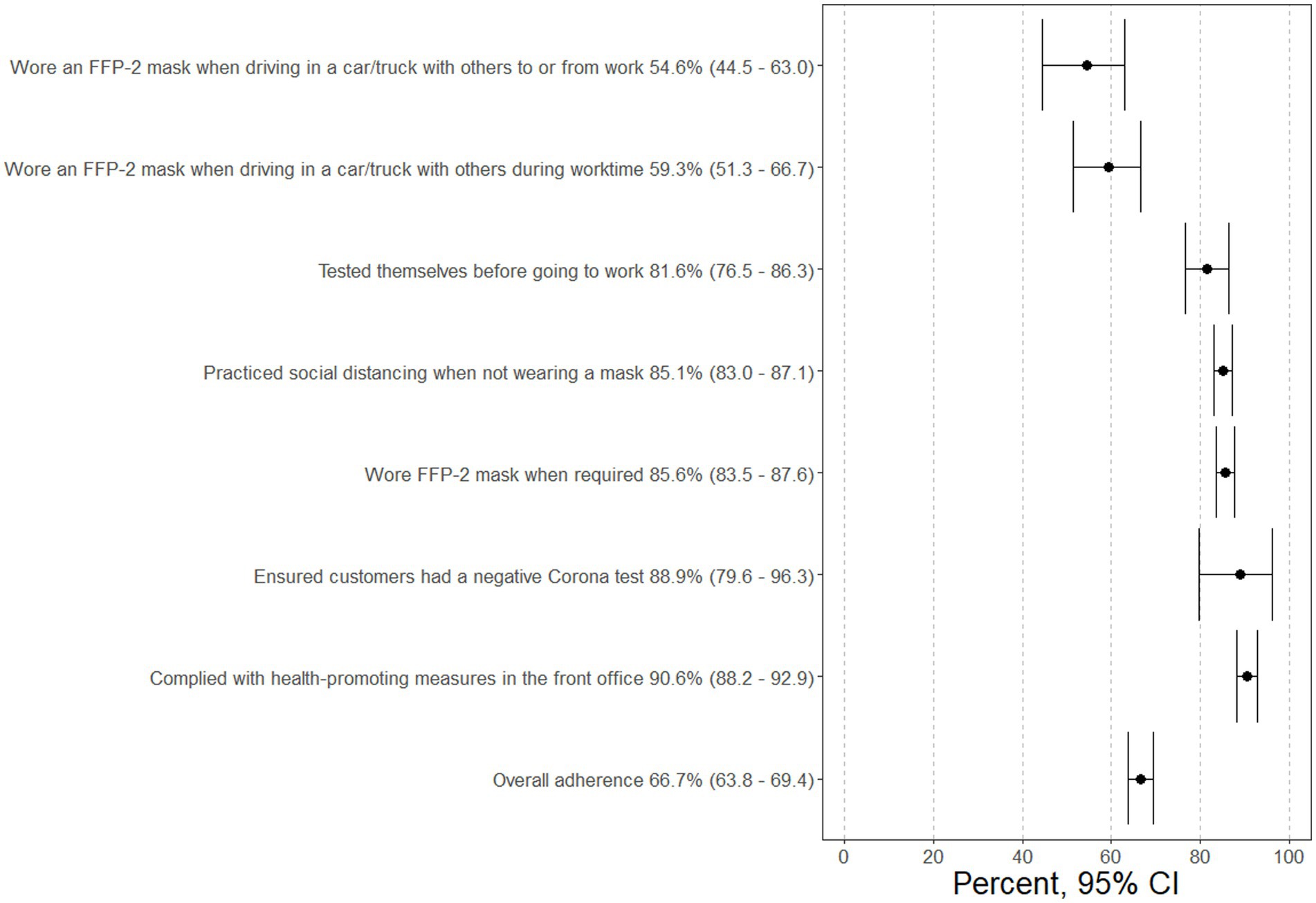
Figure 1. Percentage of people adherent to individual measures.
The majority of the employees rated a COVID-19 infection as more dangerous than an influenza infection (more dangerous: 69.7%, comparable 25.3%, harmless 1.4%). We also measured personal health risk (9.0% very high, 21.0% high, 45.7% moderate, 16.4% low, 5.2% very low), economic risk stemming from measures to combat the coronavirus (15.0% very high, 25.0% high, 30.7% moderate, 16.8% low, 10.1% very low) and perceived susceptibility (high 15.6%, slight: 69.7%, non-existent: 13.3%). Overall employees rated perceived barriers due to health-promoting measures as low (median 0.25, IQR: 0.10–0.50) and their corona fatigue as moderate (0.50, 0.33–0.67). While testing for the coronavirus was considered important (median 0.83, IQR: 0.67–1.00) wearing FFP-2 masks was rated as moderately important (0.50, 0.17–0.83).
3.2 Influence on adherence
In a first step, the following variables were significant univariate predictors of adherence to company-specific health-promoting behaviors: age, gender, and responses to all three perceived severity items (comparison to influenza, personal health risk, economic risk), perceived susceptibility, perceived barriers due to health-promoting measures, social norms, corona fatigue, meaningfulness of wearing FFP-2 masks, meaningfulness of testing, number of employees at the company, company support to help employees follow the measures, and the provision of information by the company (Supplementary Figure S1; Supplementary Table S1).
In a second step, multivariate regression analysis indicated that four independent predictors explained 31% of the variation in adherence (R2Nagelkerke = 0.308). Increased health-promoting behaviors were also associated with high ratings for the meaningfulness of testing (OR: 2.06 95%CI: 1.00–4.22; p = 0.049), the extent to which social norms govern behavior (OR: 6.61 95%CI: 4.66–9.36; p < 0.001), lower perceived difficulties associated with the adoption of health-promoting measures (OR: 0.37 95%CI: 0.16–0.82; p = 0.015) and lower corona fatigue (OR: 0.23 95%CI: 0.10–0.52; p < 0.001) (Figure 2).
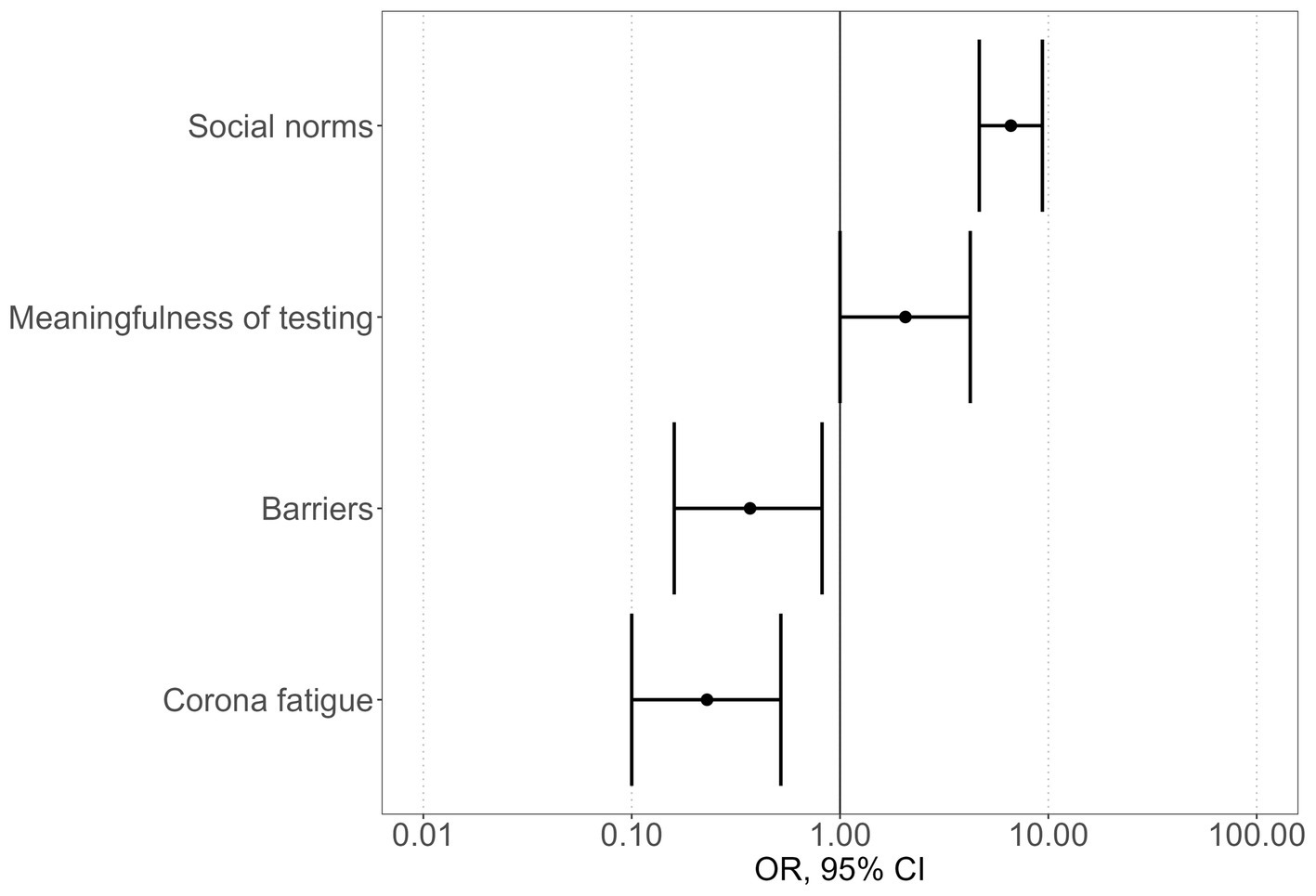
Figure 2. Independent multivariate predictors of adherent behavior.
3.3 Influence on single measures of adherence
Multivariate regression analysis of individual measures indicated that two to four independent predictors explained 9 to 50% of variance. Seven different predictors were included in the final four models. No predictor was included in all the final models. The predictors that were most often included were social norms (three times) and corona fatigue (three times) (Table 2; Supplementary Figure S2).
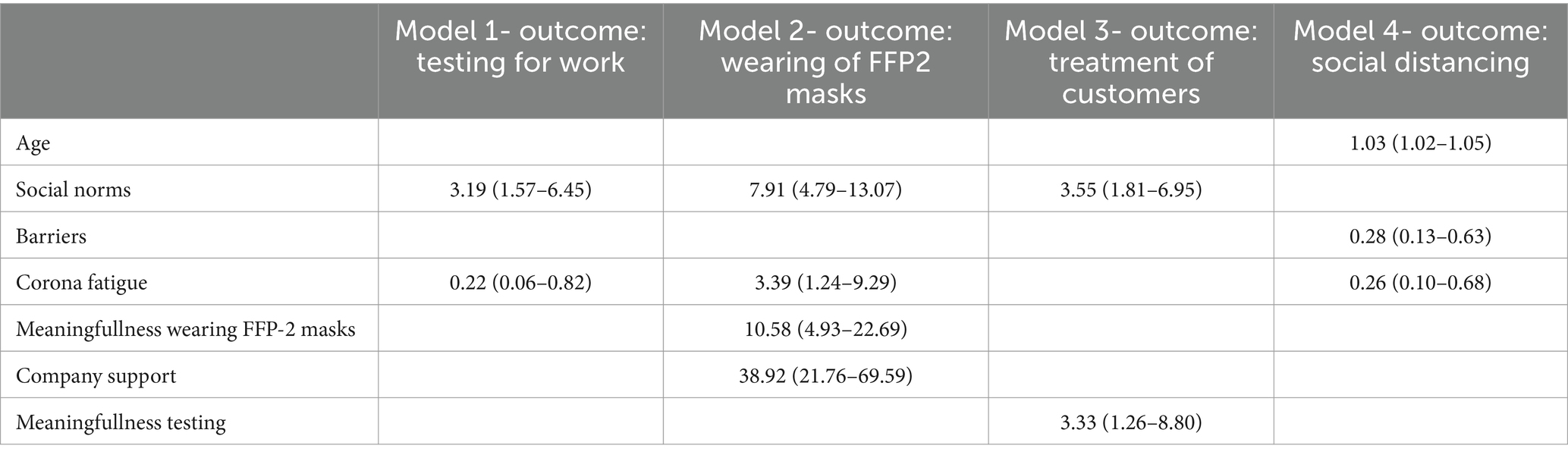
Table 2. Independent multivariate predictors of adherence to various measures (OR and 95%CIs are provided in parentheses).
4 Discussion
This cross-sectional online survey of 1,183 people working in Vorarlberg, Austria, during the COVID-19 pandemic in spring 2021 showed that social norms and corona fatigue were independent predictors of greater adherence in general and adherence to most of the investigated behaviors in particular. Further independent predictors of general adherence were higher perceived meaningfulness of testing and lower perceived barriers due to health-promoting measures. Depending on which Covid-19 protective measure in companies is considered, additional factors such as age, meaningfulness for wearing FFP2-masks and company support may also be relevant for individual measures.
4.1 Social norms
In our study, social norms – the informal rules that govern behavior in groups and societies and hence concern that individuals or groups may disapprove of one’s conduct (37) – were strong predictors of generally adherent behavior during the COVID-19 pandemic. They specifically influenced testing behavior, mask wearing and treatment of customers, but had no impact on social distancing in the work environment. These results generally agree with various other studies in the health sector [e.g., McEachan et al. (38)], as well as with studies on COVID-19 in particular [e.g., Shanka and Gebremariam Kotecho (39)]. Studies on adherence to COVID-19 measures have shown that adherence decreases when others are seen not wearing a mask and when people are heard speaking disparagingly about wearing one (40). Furthermore it has been reported that social norms influence social distancing (41), hand washing (42) and both vaccine hesitancy (43) and actual vaccinations (44) in the general population. Furthermore, professional behaviors such as the use of personal protective equipment is influenced by social norms (45).
With regard to prescribed COVID-19 measures, reactance phenomena may have encouraged the formation of social norms in specific groups (40). Reactance refers to an unintended behavioral reaction to a stimulus that occurs because an individual’s sense of behavioral freedom is threatened (e.g., decrease in adherence after the introduction of new measures). Since reactance to COVID-19 measures is associated with political discontent (46), groups that are opposed to the political authorities in their country and the measures they introduce tend to show reactance, thus reinforcing their own social norms. As concluded by Resnicow et al. (47), a subgroup’s general propensity to defy authority or oppose any laws or public health advice on the basis that it impinges upon personal rights will automatically lead to a rejection of, for example, COVID-19 protective practices. Reactance is therefore a reflection of the social norms in this subgroup of the population.
An important example of how social norms can affect adherence is the way in which social norms predict individuals’ information avoidance (48). Information avoidance is influenced by subjective norms (what people important to me think I should do), descriptive norms on a personal level (what people important to me are doing), injunctive norms on a personal level (what people important to me think should be done) and injunctive norms on a societal level (what the majority of people think should be done) but not descriptive norms on a societal level (what the majority of people actually do) (49). In addition to the norm itself, the origin of information about the behavior of relevant groups and their expectations, as well as information about the pandemic in general, also plays a role. In a meta-analysis, Li (50) showed that channel belief (perceived trustworthiness and usefulness of information) was most responsible for explaining information avoidance. Depending on the groups that are relevant to an individual, specific sources of information are trusted and therefore sought out, while others are rejected, or discussion partners are avoided or preferred. Furthermore, it can be observed that when information is sought in a targeted manner (intentional exposure), e.g., using a trusted channel, people are more likely to believe it than when they come across it by accident (incidental exposure) (51).
Interestingly, the effect of social norms can change over time. Zhou et al. (52) showed that social norms had more influence on individual behavior during the first and second waves of COVID-19 than on later waves. In their study, social norms were defined as the assumed behavior of neighbors, which would seem to imply that the reference group (neighbors) was more important at the beginning of the pandemic than later, when other groups may have established themselves as references. Borkowska and Laurence (53) had similar results and were able to show that for certain groups (certain ethnic minority groups, lower-skilled) perceived cohesion in the neighborhood decreased during the pandemic, apparently indicating that the neighborhood had lost importance as a reference group for social norms.
4.2 Corona fatigue
Another important factor determining the level of adherence in a population is so-called corona fatigue, which was associated with decreased adherence to health-promoting measures in our study. According to the World Health Organization (WHO) definition, coronavirus fatigue is the emotional exhaustion caused by feeling distressed or frustrated by the pandemic and “sustained and unresolved adversity” (54). Such emotional exhaustion corresponds more or less with items assessing behavioral fatigue. Studies have shown that adherence is negatively influenced by information fatigue (55, 56), behavioral fatigue (34) and pandemic fatigue in general (57).
In addition to the influence of corona fatigue on adherence behavior, corona fatigue also appears to increase over time. A sharp increase in corona fatigue (58) was particularly marked following the launch of the vaccination program. However, it may be short-sighted to regard this particular increase as a sign of fatigue, as, for example, there are indications that interest in finding out more about the pandemic did not decrease overall, but the focus shifted from scientific to political topics (59). Another aspect is also the coverage of this topic within medias. The topic of corona fatigue is therefore accompanied by the so-called “issue fatigue.” This means that a topic that is very prominent in the media is replaced after a while by other, more important topics. As the media competes for attention, they adapt to the mood and report less or differently on topics in which society has lost interest. Changes during the pandemic have an impact on the attention the pandemic receives from media and therefore issue fatigue contribute to the pandemic’s decreased newsworthiness (60). The interaction between issue fatigue and corona fatigue is described very well in a study of young adults (61). While the beginning of the pandemic was characterized by frequent press conferences and a daily update of COVID-19 cases, which was experienced as a phase of shock by young adults, corona fatigue later emerged. In this phase, the information was dosed. Due to emotional and informational overload, the young adults tried to regain control of their lives by determining how much information they consumed. Over time, the media began to focus more on other topics and young adults began to consume more news. This phase was referred to as “back to normal.” In addition to the effect that less news is consumed due to corona fatigue, the risk of misinformation acceptance also increases (62).
It is also important to mention that different groups were not affected by pandemic fatigue to the same extent. In the literature, female gender, younger age, economic inactivity, a low level of education, lower resilience and poorer coping abilities, greater fear/anxiety in connection with COVID-19, and poorer health were found to increase pandemic fatigue (63–69). For one group, the changes in their work and especially in the appreciation of their work were particularly dramatic. While at the beginning of the pandemic the work of medical staff, and especially nurses, was viewed as very valuable, this appreciation was often not reflected in their salaries. In this group, the corona fatigue was accompanied by exhaustion, disappointment and sometimes defeatist behavior (70).
4.3 Strengths and limitations
Although some studies have evaluated psychological factors in companies during the pandemic, our study is different in that it evaluates adherence in companies on the basis of the health belief model (25). One study performed in German companies showed that as compared to men, female employees were particularly exhausted during the pandemic (71). Another study conducted in China and based on interviews with 700 employees revealed that employees in the 30–40 age group were particularly exhausted, as were employees with a higher level of education and those with a relatively low family income (72). A longitudinal study of 419 workers in the USA demonstrated that economic vulnerability did not affect adherence to Covid-19 infection protection measures recommended in guidelines. However, cognitive attitudes were strong predictors of compliance with protective measures in the most economically secure class, while worry was a significantly stronger predictor of compliance in the most vulnerable group (73).
Our study has several limitations. The questionnaire was broadly distributed by the office of the Vorarlberg Provincial Government, the Chambers of Commerce and Labor and further groups we contacted such as work councils, personnel managers, safety experts and the Society of General Practice. Nonetheless, selection bias cannot be ruled out. Furthermore, as this was an online survey and only persons willing to participate answered our questionnaire voluntarily, the generalizability of our findings to employees as a whole may be limited. Another limitation is that it cannot be ruled out that other aspects (e.g., trust in state authorities) that could have an influence on behavior were not surveyed and therefore their influence was not examined.
5 Conclusion
The results of this Austrian cross-sectional online survey of employees show that combining the health belief model with aspects that vary over time provides useful information on why adherence varies among company employees. The importance attached to testing and social norms, as well as lower perceived barriers to health-promoting measures and low levels of corona fatigue all increase overall adherence to Covid-19 protective measures in companies.
Adherence to individual measures was also influenced by age, importance attached to wearing FFP2-masks and company support, showing that strategies need to vary depending on the particular behavior that is being targeted.
Strategies to improve adherence should be adapted depending on the aim (to raise overall adherence or adherence to individual measures) and on the group of persons that is being targeted (e.g., employees in large or small companies, in manufacturing, the wholesale or retail trade, or in the health sector). Furthermore, the government, employers and, for example, work councils and union representatives can also play an important role in increasing adherence.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The requirement of ethical approval was waived by Vorarlberg Ethics Committee (Ethikkommission Vorarlberg) for the studies involving humans because according to Austrian law, a vote from the ethics committee is not required for surveys that do not specifically include patients. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board also waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because since this is an online survey, it can be assumed that only people who want to answer the questionnaire.
Author contributions
AA: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. CK: Writing – original draft, Writing – review & editing. BK: Supervision, Writing – review & editing. US-K: Writing – review & editing. AS: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Austrian Federal Ministry for Social Affairs, Health, Care and Consumer Protection.
Acknowledgments
The authors would like to thank Daniela Schmid from the Medical University of Vienna for her help in developing a questionnaire for company employees. The authors are also grateful to L&R Social Research for programming and implementing the online survey. In addition, we would like to thank the Office of the Vorarlberg Provincial Government and the Vorarlberg Chamber of Commerce and Labor, as well as works councils, personnel managers and safety experts in large companies, union representatives, and the Vorarlberg Society of General Practice (VGAM), for distributing the questionnaire.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1347818/full#supplementary-material
References
1. Filip, R, Gheorghita Puscaselu, R, Anchidin-Norocel, L, Dimian, M, and Savage, WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. Journal of. Pers Med. (2022) 12:1295. doi: 10.3390/jpm12081295
2. Ghasempour, M, Purabdollah, M, and Sheikhnezhad, L. Lessons learned from COVID-19 for future pandemics: infection prevention in health care workers. J Caring Sci. (2023) 12:1–3. doi: 10.34172/jcs.2023.31918
3. Mazidimoradi, A, Sabet Birjandi, S, and Salehiniya, H. Effect of coronavirus disease 2019 on diagnosis and treatment of hepatocellular carcinoma: a systematic review. Explor Target Antitumor Ther. (2023) 4:1039–58. doi: 10.37349/etat.2023.00179
4. Parlindungan, F, Sumariyono, S, Hidayat, R, Wibowo, SAK, Ariane, A, Damanik, J, et al. Learning from the COVID-19 pandemic: health care disturbances and telemedicine as an alternative rheumatology practice in Indonesia. BMC Health Serv Res. (2023) 23:451. doi: 10.1186/s12913-023-09389-5
5. Schaffler-Schaden, D, Mergenthal, K, Avian, A, Huter, S, Spary-Kainz, U, Bachler, H, et al. COVI-prim longitudinal survey: experiences of primary care physicians during the early phase of the COVID-19 pandemic. Front Med. (2022) 9:761283. doi: 10.3389/fmed.2022.761283
6. Siebenhofer, A, Scott, AM, Avian, A, Terebessy, A, Mergenthal, K, Schaffler-Schaden, D, et al. COVI-prim international: similarities and discrepancies in the way general practices from seven different countries coped with the COVID-19 pandemic. Front Public Health. (2022) 10:1072515. doi: 10.3389/fpubh.2022.1072515
7. Siebenhofer, A, Huter, S, Avian, A, Mergenthal, K, Schaffler-Schaden, D, Spary-Kainz, U, et al. COVI-prim survey: challenges for Austrian and German general practitioners during initial phase of COVID-19. PLoS One. (2021) 16:e0251736–6. doi: 10.1371/journal.pone.0251736
8. Van Poel, E, van Loenen, T, Collins, C, Van Roy, K, Van den Muijsenbergh, M, and Willems, S. Barriers and enablers experienced by general practitioners in delivering safe and equitable care during COVID-19: a qualitative investigation in two countries. Healthcare. (2023) 11:3009. doi: 10.3390/healthcare11233009
9. Van Stekelenburg, B, De Cauwer, H, Barten, D, and Mortelmans, L. Attacks on health Care Workers in Historical Pandemics and COVID-19. Disaster Med Public Health Prep. (2023) 17:E309. doi: 10.1017/dmp.2022.275
10. World Health Organization. (2021). Coronavirus disease (COVID-19): overview – prevention – symptoms. Available at: https://www.who.int/health-topics/coronavirus#tab=tab_1 (Accessed Dec 1, 2023).
11. Naseer, S, Khalid, S, Parveen, S, Abbass, K, Song, H, and Achim, MV. COVID-19 outbreak: impact on global economy. Front Public Health. (2023) 10:1009393. doi: 10.3389/fpubh.2022
12. World Bank. Emerging risks to the recovery. In World Bank. World Development Report 2022: Finance for an Equitable Recovery. (2022); p 49–73.
13. Meyer, M, Wing, L, Schenkel, A, and Meschede, M. Krankheitsbedingte Fehlzeiten in der deutschen Wirtschaft im Jahr 2020 In: B Badura, A Ducki, H Schröder, and M Meyer, editors. Fehlzeiten-Report 2021: Betriebliche Prävention stärken – Lehren aus der Pandemie. Berlin, Heidelberg: Springer Berlin Heidelberg (2021). 441–538.
14. Romeo, M, Yepes-Baldó, M, and Beltrà, L. Motivation of teleworkers and non-teleworkers in times of COVID-19 in Spain: An exploratory study using non-parametric analysis and classification and regression trees. Front Psychol. (2022) 13:852758. doi: 10.3389/fpsyg.2022.852758
15. World Health Organization. Getting your workplace ready for COVID-19: How COVID-19 spreads, (2020). Available at: https://www.who.int/docs/default-source/coronaviruse/advice-for-workplace-clean-19-03-2020.pdf (Accessed Dec 1, 2023).
16. Bureau for Employers’ Activities, International Labour Organization (ILO). (2020). An employer's guide on managing your workplace during COVID-19 Vol. 2023, pp. 34). Geneva: International Labour Organization (ILO). Available at: https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---act_emp/documents/publication/wcms_740212.pdf (Accessed Dec 1, 2023).
17. Occupational Safety and Health Administration (OSHA), U.S. Department of Labor. (2023). Protecting workers: Guidance on mitigating and preventing the spread of COVID-19 in the workplace. Available at: https://www.osha.gov/coronavirus/safework (Accessed Dec 1, 2023).
18. Ingram, C, Downey, V, Roe, M, Chen, Y, Archibald, M, Kallas, K-A, et al. COVID-19 prevention and control measures in workplace settings: a rapid review and meta-analysis. Int J Environ Res Public Health. (2021) 18:7847. doi: 10.3390/ijerph18157847
19. Sasaki, N, Imamura, K, Kataoka, M, Kuroda, R, Tsuno, K, Sawada, U, et al. COVID-19 measurements at the workplace in various industries and company sizes: a 2-month follow-up cohort study of full-time employees in Japan. Environ Occup Health Pract. (2021) 3:2020-0017. doi: 10.1539/eohp.2020-0017-OA
20. Asaoka, H, Sasaki, N, Imamura, K, Kuroda, R, Tsuno, K, and Kawakami, N. Changes in COVID-19 measures in the workplace: 8-month follow-up in a cohort study of full-time employees in Japan. J Occup Health. (2021) 63:e12273. doi: 10.1002/1348-9585.12273
21. Kittel, B, Kritzinger, S, Boomgaarden, H, Prainsack, B, Eberl, JM, Kalleitner, F, et al. The Austrian Corona panel project: monitoring individual and societal dynamics amidst the COVID-19 crisis. Eur Political Sci. (2020) 20:318–44. doi: 10.1057/s41304-020-00294-7
22. Rodríguez-Blázquez, C, Romay-Barja, M, Falcón, M, Ayala, A, and Forjaz, MJ. The COSMO-Spain survey: three first rounds of the WHO behavioral insights tool. Frontiers. Public Health. (2021) 9:9. doi: 10.3389/fpubh.2021.678926
23. Steens, A, Freiesleben de Blasio, B, Veneti, L, Gimma, A, Edmunds, WJ, Van Zandvoort, K, et al. Poor self-reported adherence to COVID-19-related quarantine/isolation requests, Norway, April to July 2020. Eur Secur. (2020) 25:2001607. doi: 10.2807/1560-7917.Es.2020.25.37.2001607
24. Wright, L, Steptoe, A, and Fancourt, D. Predictors of self-reported adherence to COVID-19 guidelines. A longitudinal observational study of 51,600 UK adults. Lancet Reg Health Eur. (2021) 4:100061. doi: 10.1016/j.lanepe.2021.100061
25. Rosenstock, IM, Strecher, VJ, and Becker, MH. Social learning theory and the health belief model. Health Educ Q. (1988) 15:175–83. doi: 10.1177/109019818801500203
26. Zewdie, A, Mose, A, Sahle, T, Bedewi, J, Gashu, M, Kebede, N, et al. The health belief model’s ability to predict COVID-19 preventive behavior: a systematic review. SAGE Open Med. (2022) 10:205031212211136. doi: 10.1177/20503121221113668
27. Limbu, YB, Gautam, RK, and Pham, L. The health belief model applied to COVID-19 vaccine hesitancy: a systematic review. Vaccine. (2022) 10:973. doi: 10.3390/vaccines10060973
28. Liang, W, Duan, Y, Li, F, Rhodes, RE, Wang, X, Peiris, DLIHK, et al. Psychosocial determinants of hand hygiene, facemask wearing, and physical distancing during the COVID-19 pandemic: a systematic review and meta-analysis. Ann Behav Med. (2022) 56:1174–87. doi: 10.1093/abm/kaac049
29. Rezapouraghdam, H, and Karatepe, OM. Applying health belief model to unveil Employees' workplace COVID-19 protective behaviors: insights for the hospitality industry. Int J Ment Health Promot. (2020) 22:233–47. doi: 10.32604/IJMHP.2020.013214
30. Youssef, D, Abou-Abbas, L, Berry, A, Youssef, J, and Hassan, H. Determinants of acceptance of coronavirus disease-2019 (COVID-19) vaccine among Lebanese health care workers using health belief model. PLoS One. (2022) 17:e0264128. doi: 10.1371/journal.pone.0264128
31. Yu, Y, Lau, JTF, She, R, Chen, X, Li, L, Li, L, et al. Prevalence and associated factors of intention of COVID-19 vaccination among healthcare workers in China: application of the health belief model. Hum Vaccin Immunother. (2021) 17:2894–902. doi: 10.1080/21645515.2021.1909327
32. Alsulaiman, SA, and Rentner, TL. The use of the health belief model to assess U.S. college students’ perceptions of Covid-19 and adherence to preventive measures. J Public Health Res. (2021) 10:2273. doi: 10.4081/jphr.2021.2273
33. Shitu, K, Adugna, A, Kassie, A, and Handebo, S. Application of health belief model for the assessment of COVID-19 preventive behavior and its determinants among students: a structural equation modeling analysis. PLoS One. (2022) 17:e0263568. doi: 10.1371/journal.pone.0263568
34. Siebenhofer, A, Könczöl, C, Jeitler, K, Schmid, D, Elliott, P, and Avian, A. Predictors for adherent behavior in the COVID-19 pandemic: a cross-sectional telephone survey. Front Public Health. (2022) 10:10. doi: 10.3389/fpubh.2022.894128
35. Hsing, JC, Ma, J, Barrero-Castillero, A, Jani, SG, Pulendran, UP, Lin, BJ, et al. Influence of health beliefs on adherence to COVID-19 preventative practices: an online international study via social media. J Med Internet Res. (2021) 23:e23720. doi: 10.2196/23720
36. Lilleholt, L, Zettler, I, Betsch, C, and Böhm, R. Development and validation of the pandemic fatigue scale. Nat Commun. (2023) 14:6352. doi: 10.1038/s41467-023-42063-2
37. Ajzen, I. The theory of planned behavior. Organ Behav Hum Decis Process. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-t
38. McEachan, R, Taylor, N, Harrison, R, Lawton, R, Gardner, P, and Conner, M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann Behav Med. (2016) 50:592–612. doi: 10.1007/s12160-016-9798-4
39. Shanka, MS, and Gebremariam Kotecho, M. Combining rationality with morality – integrating theory of planned behavior with norm activation theory to explain compliance with COVID-19 prevention guidelines. Psychol Health Med. (2021) 28:305–15. doi: 10.1080/13548506.2021.1946571
40. Dillard, JP, Tian, X, Cruz, SM, Smith, RA, and Shen, LJ. Persuasive messages, social norms, and reactance: a study of masking behavior during a COVID-19 campus health campaign. Health Commun. (2023) 38:1338–48. doi: 10.1080/10410236.2021.2007579
41. Friemel, TN, and Geber, S. Social distancing during the COVID-19 pandemic in Switzerland: health protective behavior in the context of communication and perceptions of efficacy, norms, and threat. Health Commun. (2023) 38:779–89. doi: 10.1080/10410236.2021.1976360
42. Cabrera-Alvarez, P, Hornsey, MJ, and Lobera, J. Determinants of self-reported adherence to COVID-19 regulations in Spain: social norms, trust and risk perception. Health Promot Int. (2022) 37:daac138. doi: 10.1093/heapro/daac138
43. Jaffe, AE, Graupensperger, S, Blayney, JA, Duckworth, JC, and Stappenbeck, CA. The role of perceived social norms in college student vaccine hesitancy: implications for COVID-19 prevention strategies. Vaccine. (2022) 40:1888–95. doi: 10.1016/j.vaccine.2022.01.038
44. Bonner, KE, Vashist, K, Abad, NS, Kriss, JL, Meng, L, Lee, JT, et al. Behavioral and social drivers of COVID-19 vaccination in the United States, august-November 2021. Am J Prev Med. (2023) 64:865–76. doi: 10.1016/j.amepre.2023.01.014
45. Fauk, NK, Seran, AL, Raymond, C, Merry, MS, Tahir, R, Asa, GA, et al. Why do we not follow lifesaving rules? Factors affecting nonadherence to COVID-19 prevention guidelines in Indonesia: healthcare professionals' perspectives. Int J Environ Res Public Health. (2022) 19:8502. doi: 10.3390/ijerph19148502
46. Hajek, KV, and Häfner, M. Paradoxes of reactance during the COVID-19 pandemic: a social-psychological perspective. Javnost-Public. (2021) 28:290–305. doi: 10.1080/13183222.2021.1969619
47. Resnicow, K, Bacon, E, Yang, P, Hawley, S, Van Horn, ML, and An, L. Novel predictors of COVID-19 protective behaviors among US adults: cross-sectional survey. J Med Internet Res. (2021) 23:e23488. doi: 10.2196/23488
48. Qu, Y, Saffer, AJ, and Austin, L. What drives people away from COVID-19 information?: uncovering the influences of personal networks on information avoidance. Health Commun. (2023) 38:216–27. doi: 10.1080/10410236.2021.1944457
49. Link, E. A normative perspective on information avoidance behaviors: separating various types of avoidance-related norms. Commun Eur J Commun Res. (2023). doi: 10.1515/commun-2022-0085 [Epub ahead of print].
50. Li, JH. Information avoidance in the age of COVID-19: a meta-analysis. Inf Process Manag. (2023) 60:103163. doi: 10.1016/j.ipm.2022.103163
51. Wu, Y, and Mustafa, H. Exploring the impact of social media exposure patterns on people?S belief in fake news during COVID-19: a cross-gender study. Online J Commun Media Technol. (2023) 13:e202326. doi: 10.30935/ojcmt/13117
52. Zhou, HC, Cárdenas, D, and Reynolds, KJ. Norms and COVID-19 health behaviours: a longitudinal investigation of group factors. Eur J Soc Psychol. (2023) 53:720–31. doi: 10.1002/ejsp.2932
53. Borkowska, M, and Laurence, J. Coming together or coming apart? Changes in social cohesion during the Covid-19 pandemic in England. Eur Soc. (2021) 23:S618–36. doi: 10.1080/14616696.2020.1833067
54. World Health Organization (WHO). Pandemic fatigue – Reinvigorating the public to prevent COVID-19. Policy framework for supporting pandemic prevention and management (document number: WHO/EURO:2020–1160–40906-55390). Copenhagen: WHO, Regional Office for Europe (2020).
55. Berghs, M, Williams, SN, Armitage, CJ, Tampe, T, and Dienes, KA. Public perceptions of non-adherence to pandemic protection measures by self and others: a study of COVID-19 in the United Kingdom. PLoS One. (2021) 16:e0258781. doi: 10.1371/journal.pone.0258781
56. Skulmowski, A, and Standl, B. COVID-19 information fatigue? A case study of a German university website during two waves of the pandemic. Hum Behav Emerg Technol. (2021) 3:350–6. doi: 10.1002/hbe2.260
57. Hassanien, NS, Adawi, AM, Alzahrani, TA, and Adawi, EA. The mediating role of resilience and electronic health literacy in the relationship between pandemic fatigue and adherence to preventive Behaviours against COVID-19. Cureus journal of. Med Sci. (2022) 14:e29553. doi: 10.7759/cureus.29553
58. Wu, X, Lu, Y, and Jiang, B. Built environment factors moderate pandemic fatigue in social distance during the COVID-19 pandemic: a nationwide longitudinal study in the United States. Landsc Urban Plan. (2023) 233:104690. doi: 10.1016/j.landurbplan.2023.104690
59. Shi, CF, So, MC, Stelmach, S, Earn, A, Earn, DJD, and Dushoff, J. From science to politics: COVID-19 information fatigue on YouTube. BMC Public Health. (2022) 22:816. doi: 10.1186/s12889-022-13151-7
60. Harjuniemi, T. A topic among others—examining the attention dynamics of the COVID-19 pandemic through interviews with Finnish journalists. Journalism. (2023) 24:2723–40. doi: 10.1177/14648849221138431
61. Groot Kormelink, T, and Klein Gunnewiek, A. From “far away” to “shock” to “fatigue” to “Back to Normal”: how young people experienced news during the first wave of the COVID-19 pandemic. Journal Stud. (2022) 23:669–86. doi: 10.1080/1461670X.2021.1932560
62. Hwang, Y, So, J, and Jeong, S-H. Does COVID-19 message fatigue lead to misinformation acceptance? An Extension of the Risk Information Seeking and Processing Model. Health Commun. (2023) 38:2742–9. doi: 10.1080/10410236.2022.2111636
63. Domosławska-Żylińska, K, Krysińska-Pisarek, M, and Włodarczyk, D. Gender-specificity of fatigue and concerns related to the COVID-19 pandemic—a report on the polish population. Int J Environ Res Public Health. (2023) 20:5407. doi: 10.3390/ijerph20075407
64. Hassan, BAR, Mohammed, AH, Wayyes, AM, Farhan, SS, Al-Ani, OA, Blebil, A, et al. Exploring the level of lockdown fatigue and effect of personal resilience and coping behaviours on university students during the covid-19 pandemic: a cross-sectional analysis from Iraq. Curr Psychol. (2023) 42:14851–9. doi: 10.1007/s12144-022-02779-8
65. Labrague, LJ, and Ballad, CA. Lockdown fatigue among college students during the COVID-19 pandemic: predictive role of personal resilience, coping behaviors, and health. Perspect Psychiatr Care. (2021) 57:1905–12. doi: 10.1111/ppc.12765
66. Lai, DWL, Jin, JH, Yan, E, and Lee, VWP. Predictors and moderators of COVID-19 pandemic fatigue in Hong Kong. J Infect Public Health. (2023) 16:645–50. doi: 10.1016/j.jiph.2023.03.003
67. Morgul, E, Bener, A, Atak, M, Akyel, S, Aktas, S, Bhugra, D, et al. COVID-19 pandemic and psychological fatigue in Turkey. Int J Soc Psychiatry. (2021) 67:128–35. doi: 10.1177/0020764020941889
68. Taylor, S, Rachor, GS, and Asmundson, GJG. Who develops pandemic fatigue? Insights from latent class analysis. PLoS One. (2022) 17:e0276791. doi: 10.1371/journal.pone.0276791
69. Xin, L, Wang, LH, Cao, X, Tian, YN, Yang, YS, Wang, KX, et al. Prevalence and influencing factors of pandemic fatigue among Chinese public in Xi'an city during COVID-19 new normal: a cross-sectional study. Front Public Health. (2022) 10:10. doi: 10.3389/fpubh.2022.971115
70. Bredgaard, T. The Corona pandemic and working life: findings from a longitudinal Danish study. Nord J Work Life Stud. (2023) 13:3–22. doi: 10.18291/njwls.138568
71. Meyer, B, Zill, A, Dilba, D, Gerlach, R, and Schumann, S. Employee psychological well-being during the COVID-19 pandemic in Germany: a longitudinal study of demands, resources, and exhaustion. Int J Psychol. (2021) 56:532–50. doi: 10.1002/ijop.12743
72. Liu, Y, Zhang, Z, and Zhao, H. The influence of the COVID-19 event on deviant workplace behavior taking Tianjin, Beijing and Hebei as an example. Int J Environ Res Public Health. (2020) 18:59. doi: 10.3390/ijerph18010059
Keywords: COVID-19, adherence, health belief model, employees, social norms, corona fatigue, barriers to health-promoting measures, online-survey
Citation: Avian A, Könczöl C, Kubicek B, Spary-Kainz U and Siebenhofer A (2024) Predictors of adherence in Austrian employees during the COVID-19 pandemic: results of an online survey. Front. Public Health. 12:1347818. doi: 10.3389/fpubh.2024.1347818
Edited by:
Andrea Trevisan, University of Padua, ItalyReviewed by:
Sime Smolic, University of Zagreb, CroatiaUsman Talat, The University of Manchester, United Kingdom
Copyright © 2024 Avian, Könczöl, Kubicek, Spary-Kainz and Siebenhofer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexander Avian, YWxleGFuZGVyLmF2aWFuQG1lZHVuaWdyYXouYXQ=