 Ulrich Wesemann
Ulrich Wesemann Karl-Heinz Renner
Karl-Heinz Renner Katie Rowlands
Katie Rowlands Kai Köhler
Kai Köhler Nils Hüttermann
Nils Hüttermann Hubertus Himmerich
Hubertus Himmerich- 1Department of Psychiatry, Psychotherapy and Psychotraumatology, Bundeswehr Hospital Berlin, Berlin, Germany
- 2Faculty of Human Sciences, Institute of Psychology, Bundeswehr University Munich, Neubiberg, Germany
- 3Department of Psychological Medicine, King’s College London, Institute of Psychiatry, Psychology and Neuroscience (IoPPN), London, United Kingdom
Introduction: There is very good international research on deployment-related mental disorders in military personnel. The incidence rates show a very wide range. A new strategy is therefore proposed in order to achieve better standardization and thus better comparability of the studies. In addition to a non-deployed comparison group, we propose to compare deployed soldiers with and without critical military incidents during the deployment. This additional distinction makes it possible to differentiate between the influencing variables of actual threat and general deployment stress.
Methods: N = 358 male combat soldiers deployed to Afghanistan were included in the study. Clinical interviews were conducted several days before deployment and after deployment. Of them, n = 80 soldiers suffered a life-threatening military incident during deployment, whereas 278 soldiers did not. Odds ratios (OR) were calculated for the groups with and without critical military incidents and the new onset for PTSD, anxiety disorders and depressive disorders.
Results: When comparing both groups, we found significantly higher 1-year incidence rates in the group with critical military incidents: 6.4% vs. 1.1% (OR 6.2) for post-traumatic stress disorder (PTSD); 7.0% vs. 1.1% (OR 6.5) for depression; and 15.9% vs. 2.8% (OR 6.6) for anxiety disorders. The 1-year incidence rate of mental multimorbidity (PTSD with anxiety or depression) was 4.8% vs. 0.4% (OR 12.0).
Discussion: These results indicate that life-threatening military incidents during military deployment are important to mental health. As the different threat levels of the various missions are taken into account, additional predictors could be determined more precisely in further research.
Introduction
There is an abundance of literature on the prevalence and incidence rates of post-traumatic stress disorder (PTSD) among emergency responders (1–3) and civilians (4, 5) after major disasters. As PTSD is only one mental health outcome among others, common mental disorders such as depression or anxiety are often not recorded. A methodological problem with many studies lies in the naturalistic design. As major disasters are difficult to predict, it is not possible to carry out baseline measurements. The pure prevalence rate of mental disorders can therefore only be attributed to the events to a limited extent. In addition, the informative value is often impaired by the fact that no comparison group is included or available. For example, after the WTC terrorist attacks of 9/11, it is virtually impossible to identify emergency services personnel who were not deployed there in any way after the attack. To address this issue, meta-analyses can help reconcile such differences. However, the problem that often remains is that the clinical and methodological heterogeneity of the studies is very high. This is also significantly limiting the substance of the meta-analyses (6).
For military personnel deployed in war zones, it is somewhat easier, as the missions are more predictable and therefore allow for baseline measurements. Thus, there is a good database on mental disorders after deployments abroad (7–9), while the results of incidence rates are inconsistent in terms of timing and data collection (10, 11). Comparability is also limited by a variety of missions with different military conflict potential as well as different types of data collection, such as the use of questionnaires, clinical interviews or register studies (12, 13). As a result, the incidence rates of deployment-related mental disorders among this population vary widely, e.g., the range for PTSD is between 0.1% (14) and 27.8% (15).
Most studies include undeployed soldiers who refer to comparable units as a control group (16). Differences in the development of mental disorders can therefore be attributed to the deployment. Nevertheless, since the circumstances of deployments abroad differ from those in the home country, this comparison is somewhat problematic. Personal restrictions such as absence from home, climate changes, constant readiness, carrying out operations under different threat conditions, etc. are part of everyday life here. This means that different situations are compared over time, which is the intent of the studies, but each situation is part of the military’s self-image. Although there is no doubt that a deployment abroad increases the burden and stress level, it is only likely to contribute to the development of mental disorders in a few cases. Rather, military threats such as active combat operations, defined as violence by armed forces against people, animals or objects or violence against armed forces through attacks, mines, firefights, etc., are likely to be responsible (17–19).
Following on from these considerations, an extended approach would be to compare soldiers who are on the same deployment during the same period of time. The discrimination could then be made between a risk group of soldiers with critical military incidents, defined as events with a real risk of injury or death, and a comparison group of soldiers without such an event during deployment. The delta of new occurrences of mental disorders could thus be attributed more directly to these war-related events. This would make it easier to compare the different studies and probably lead to more consistent results. As the different threat levels of the various deployments are thus taken into account, other important predictors such as age, gender, rank, duration of deployments, equipment (20), etc. could be determined more precisely. On the other hand, different types of stressors could also be investigated in these missions. Nordstrand and colleagues found that Norwegian soldiers deployed to Afghanistan showed higher posttraumatic deprecation following the non-threat-based stressors “moral challenge or witnessing” than soldiers who experienced “personal threat” (21).
PTSD is one of the most common deployment-related mental disorder in the German Armed Forces (22). A study examining the 1-year incidence rate among German soldiers deployed to Afghanistan found that 2.1% had a new onset of PTSD (unweighted), compared to 0.2% of never-deployed soldiers (23).
To examine the extent to which critical military incidents are responsible for the incidence, we compared military personnel with and without these events. We hypothesized that soldiers exposed to a critical military incident during deployment are more likely to develop PTSD, anxiety and depressive disorders as well as “multimorbidity” defined as PTSD with a depressive or an anxiety disorder.
Methods
Eligible participants were military personnel of an entire combat troop contingent deployed in Afghanistan from November 2013 to July 2014. These troops were part of the International Security Assistance Force (ISAF) which was a multinational military mission in Afghanistan from 2001 to 2014. The baseline assessment was embedded in the deployment training in November 2013 and took place a few days before the deployment. The second survey was conducted one year after the baseline assessment and had the same framework conditions. From a total of 511, n = 496 servicewomen and men (97%) were recorded at the first measurement point. There were n = 135 (27%) drop-outs between the two assessments. The main reasons for the dropouts were changes in the military resource planning and medical conditions. We excluded n = 3 female soldiers due to lack of representativeness of such a small subgroup, thus N = 358 male combat soldiers remained.
Data collection consisted of the clinical interview Mini Diagnostic Interview for Mental Disorders (24) according to ICD-10. Therefore, troop psychologists were trained in this interview. After the training, the agreement of diagnoses between the troop psychologists was 95% (inter-rater reliability). That is acceptable. This interview covers the most common mental disorders, including PTSD, anxiety disorders and depressive disorders.
By comparing the two assessments, it is possible to calculate the new onset of mental disorders after deployment. In the present data analysis, we examined the 1-year incidence rate of mental disorders in N = 358 physically uninjured male combat soldiers. The focus was on PTSD, anxiety disorders and depressive disorders. For this purpose, all anxiety disorders, consisting of specific phobias, obsessive-compulsive disorders, agoraphobia (with and without panic attacks), panic attacks, social phobias and generalized anxiety disorders, as well as all depressive disorders, consisting of major depression, dysthymia and hypomania, were summarized.
With respect to the methodological considerations, we compared the incidence rates of 80 combat soldiers who suffered a critical military incident, and 278 who did not. All soldiers of the same rank had the same risk of encountering critical military incidents during deployment resulting in a quasi-experimental design of the study. Sociodemographic characteristics were compared between both groups using t-tests for independent samples.
Odds ratios (OR) were calculated for the groups with and without critical military incidents sand each mental health outcome for PTSD, anxiety disorders and depressive disorders. Soldiers with the specific pre-deployment diagnosis were each excluded because they were “not at risk” of developing the same diagnosis again (see Figure 1). To test for confounding variables, analysis of covariance (ANCOVA) was performed including the new onset of the specific mental disorders as dependent variable, critical incidents (yes/no) as independent variable and sociodemographic data as covariates.
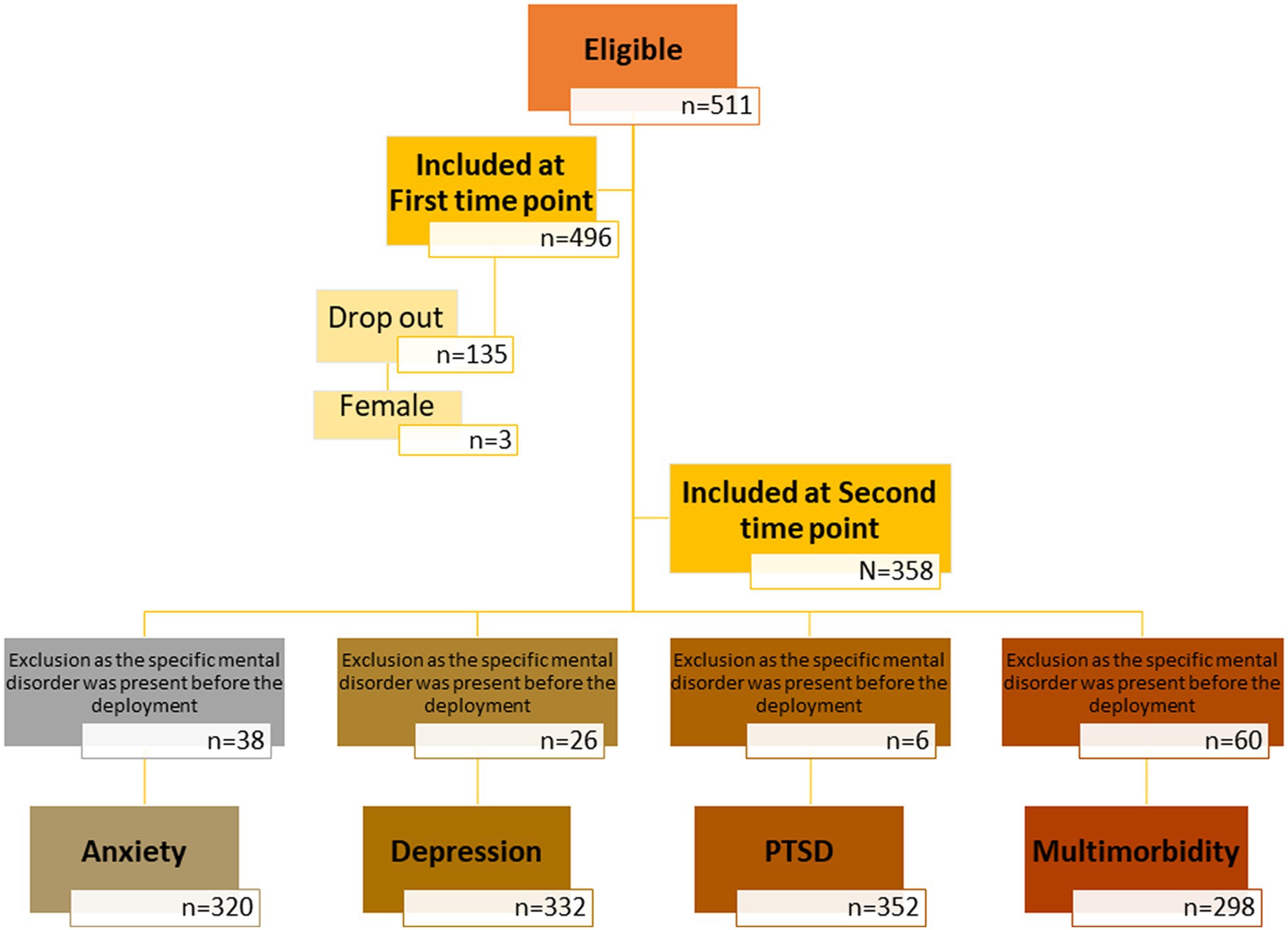
Figure 1. Flowchart illustrating the inclusion of participants in each phase.
This cohort study was commissioned by the Federal Ministry of Defence (PIII5-Az-66-55-05). The original research question of the Federal Ministry of Defense related to “Psychological Fitness” and participation was mandatory. Obtaining a written informed consent was not applicable for this project. However, the participants were informed about the meaning and purpose of the study. To comply with the ethics regulations, we therefore obtained approval from the ethics committee of the Bundeswehr University Munich (No: EK UniBw M 23-01) for this research project. In addition, the approval of the Federal Ministry of Defense was obtained for this publication. Further methodological details and legal aspects are published elsewhere (25).
Results
Age ranged from 18 to 49 years (mean 26.6 years, standard deviation 4.9; median 25 years, interquartile range 23–28 years). Participants were enlisted soldiers (n = 211, 58.9%), non-commissioned officers (n = 111, 31.0%), or officers n = 32 (8.9%). There was a small amount of missing data (n = 4; 1.1%).
Comparing both groups, with and without critical military incidents, there were no differences in sociodemographic data as shown in Table 1. The 1-year incidence rates were found for PTSD with 6.4% vs. 1.1%, depression 7.0% vs. 1.1%, and anxiety disorders 15.9% vs. 2.8% with OR ranging from 6.2 to 6.6. The 1-year incidence rate of mental multimorbidity (PTSD with anxiety or depression) was 4.8% vs. 0.4% (OR 12.0). All comparisons revealed statistically significant differences. Table 2 shows the 1-year incidence rates for the subgroups and total group.
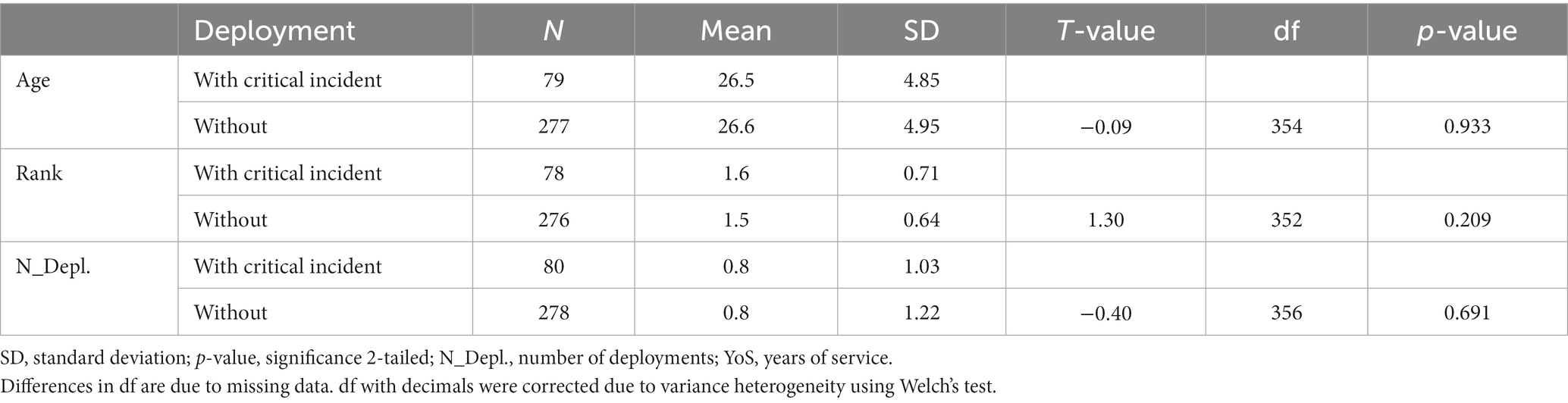
Table 1. t-test for group differences between soldiers with and without critical incidents during deployment in relation to demographic characteristics.
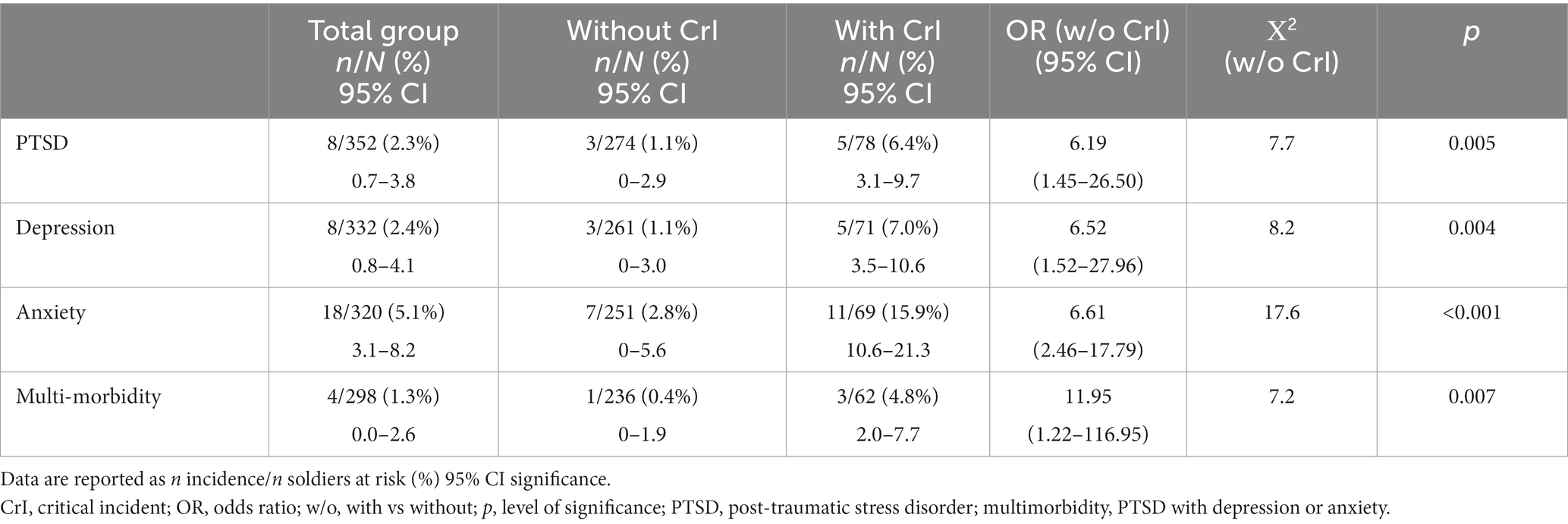
Table 2. 1-year incidence rates for male German military personnel deployed to Afghanistan with and without critical military incidents.
Although participants represent a relatively homogeneous group, ANCOVAs were conducted to test whether other factors influence the higher incidence of these mental disorders among soldiers with critical military incidents. There was no significant effect of covariates on the incidence of depressive disorders, anxiety disorders, or multimorbidity, but critical incidents remained statistically significant. As shown in Table 3, the sociodemographic data had no significant influence on the incidence of PTSD.
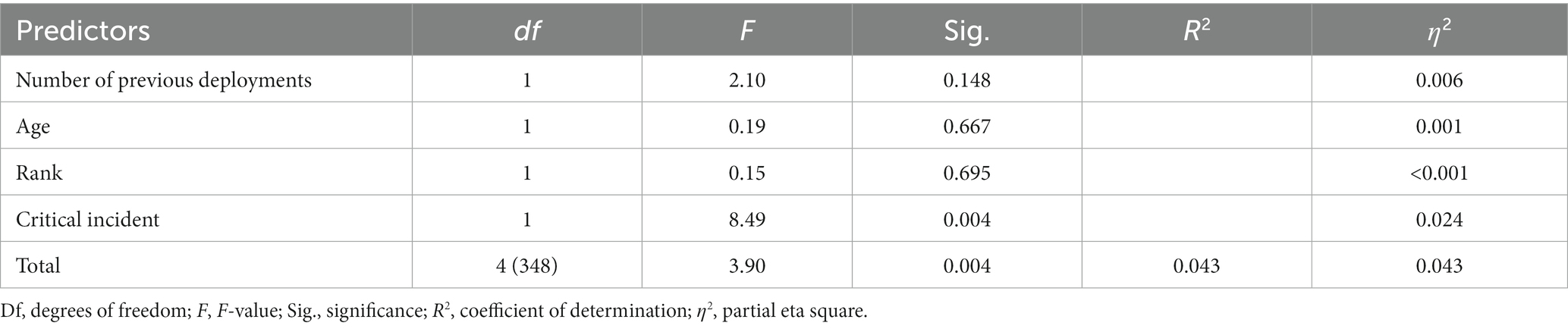
Table 3. ANCOVA to test the influence of critical incidents during deployment on the incidence of PTSD including number of previous deployments, age, and rank as covariates.
Discussion
As expected, the group that faced critical military incidents during deployment had significantly higher 1-year incidence rates for all investigated mental disorders. This was particularly pronounced in the comorbidity of PTSD with anxiety or depression. These results indicate that it is more meaningful to compare the outcomes of soldiers who experienced life-threatening military incidents to soldiers on the same deployment who did not experience such an incident, since the living conditions for both groups are comparable. The 1-year incidence for PTSD in our total group with 2.3% corresponds to the unweighted 2.1% 1-year incidence found by Wittchen and colleagues in German soldiers deployed to Afghanistan (23) and to 2.9% each for PTSD and depression found in a representative sample of U.S. Reserve and National Guard (26). The added value is the differentiation of groups with and without critical military incidents during deployment, resulting in an increased 1-year incidence of PTSD with 6.4% for the at-risk group with these incidents. The higher 1-year incidence of PTSD in our sample with no critical military incidents, compared to the never-deployed soldiers (23) of 1.1% vs. 0.2%, could be due to possible differences in exposure to critical events outside the military. In addition, the stressful environment abroad and the reintegration in the home country confer a higher vulnerability to these episodes, supporting our research strategy.
In a recently published study, Dyball and colleagues (27) examined the mental health point prevalence several years after deployment of physically injured and uninjured male military personnel. Soldiers exposed to critical military events during their deployment in Afghanistan up to 2014 were included. Compared to the uninjured group (22), our 1-year incidence rates in the total group (uninjured group with and without critical incidents) are noticeably lower in all categories. Comparing the soldiers with critical military incidents in our study to the uninjured group in the study by Dyball and colleagues (27), the rates are comparable and only remain lower for depression (7.0% vs. 16.8%) in our sample.
In addition to possible differences in the exposure to critical military incidents, the lower depression rate in our sample could be due to several factors. Firstly, results from questionnaires often overestimate mental disorders due to the specificity of the tests. Secondly, we calculated incidence rates and therefore soldiers with previous but ongoing mental disorders are not included. Finally, a large interval between deployment and testing confers a high probability of exposure to additional military and non-military life-critical incidents. We believe that the data from Dyball and colleagues (27) and ours would be more comparable if these factors were considered. This could be achieved in a collaborative project as suggested by Himmerich and colleagues (28).
While our results are not surprising, they can nonetheless be used by policy and stakeholders to address risk factors more specifically, report critical military incidents more clearly, and appreciate these incidents as occupational hazards. Since the conditions for both groups are comparable, the increased OR can most likely be attributed to the critical military incidents. This association has long been recognized for PTSD. However, our data also show such an effect for anxiety disorders and depressive disorders. In the future, this could make it even easier for those affected to have their symptoms recognized as an operational injury and thus as an occupational disease. Screening this risk group for psychological symptoms over a longer period of time seems sensible, as already suggested by Stene et al. (29) and Pirard et al. (30). Our results might also be used for psychoeducational and destigmatization programs for military personnel, as well as previously proposed virtual (31) or other pre- (32) and post-deployment training programs (33–37).
A limitation of our study results is the lack of differentiation between the various critical military incidents during the deployment and the lack of comparison between military ranks. This is due to the relatively small number of soldiers exposed to these incidents, making such sub-samples too small. In addition, the obligatory nature of data collection may have introduced biases in the responses received. It is also known that the perceived threat (38) and the witnessing of acts of violence (39) have a major influence on the psychological consequences. This was not recorded in this study, but should be taken into account in similar studies. This can make it easier to differentiate between the groups of those directly affected, those observed and those not involved. In addition, it would have been helpful to include traumatic experiences prior to deployment in the ANCOVA.
The risk of developing a mental disorder during deployment is significantly higher for members of the armed forces who experience life-threatening military incidents than for those who do not. However, the stress factors of foreign deployments alone, such as the general threat situation, appear to increase the risk. We do not have another control group of non-deployed military personnel from the same time period. However, a comparison with another study (23) shows a higher incidence of PTSD in our deployment group without life-threatening military incidents at 1.1% compared to 0.2%. This leads to the conclusion that other critical events such as sexual assaults, fear of attacks, mines, etc. also play an important role. It is therefore quite possible that both groups also exhibited more severe symptoms, but these were not sufficient for a diagnosis of PTSD, as has already been reported in other studies (40).
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: given the sensitivity of the mandatory study design, the data were not made publicly available. Data requests can be directed to the corresponding author. They are then checked on a case-by-case basis and require the approval of the Federal Ministry of Defence. Requests to access these datasets should be directed to dXdAcHR6Yncub3Jn.
Ethics statement
The studies involving humans were approved by Bundeswehr University Munich (No: EK UniBw M 23-01). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because the original research question of the Federal Ministry of Defense related to “Psychological Fitness” and participation was mandatory.
Author contributions
UW: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. K-HR: Methodology, Supervision, Validation, Writing – review & editing. KR: Formal analysis, Supervision, Validation, Writing – review & editing. KK: Formal analysis, Supervision, Validation, Writing – review & editing. NH: Formal analysis, Validation, Writing – review & editing. HH: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by the German Ministry of Defence (PIII5-Az-66-55-05). There is no influence on the content, the research question or the results.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vandentorren, S, Pirard, P, Sanna, A, Aubert, L, Motreff, Y, Dantchev, N, et al. Healthcare provision and the psychological, somatic and social impact on people involved in the terror attacks in January 2015 in Paris: cohort study. Br J Psychiatry. (2018) 212:207–14. doi: 10.1192/bjp.2017.63
2. Sahebi, A, Yousefi, K, Moayedi, S, Golitaleb, N, Esmaeili Vardanjani, A, and Golitaleb, M. Prevalence of posttraumatic stress disorder among firefighters in Iran: a systematic review and meta-analysis. Iran J Psychiatry. (2020) 15:358–65. doi: 10.18502/ijps.v15i4.4301
3. Sahebi, A, Nejati-Zarnaqi, B, Moayedi, S, Yousefi, K, Torres, M, and Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: an umbrella review of meta-analyses. Prog Neuro-Psychopharmacol Biol Psychiatry. (2021) 107:110247. doi: 10.1016/j.pnpbp.2021.110247
4. Neria, Y, Nandi, A, and Galea, S. Post-traumatic stress disorder following disasters: a systematic review. Psychol Med. (2008) 38:467–80. doi: 10.1017/S0033291707001353
5. Golitaleb, M, Mazaheri, E, Bonyadi, M, and Sahebi, A. Prevalence of post-traumatic stress disorder after flood: a systematic review and meta-analysis. Front Psych. (2022) 13:890671. doi: 10.3389/fpsyt.2022.890671
6. Ruppar, T. Meta-analysis: how to quantify and explain heterogeneity? Eur J Cardiovasc Nurs. (2020) 19:646–52. doi: 10.1177/1474515120944014
7. Maglione, MA, Chen, C, Bialas, A, Motala, A, Chang, J, Akinniranye, O, et al. Combat and operational stress control interventions and PTSD: a systematic review and meta-analysis. Mil Med. (2022) 187:e846–55. doi: 10.1093/milmed/usab310
8. Doody, CB, Egan, J, Bogue, J, and Sarma, KM. Military personnels' experience of deployment: an exploration of psychological trauma, protective influences, and resilience. Psychol Trauma. (2022) 14:545–57. doi: 10.1037/tra0001114
9. Prykhodko, II, Bielai, SV, Hrynzovskyi, AM, Zhelaho, AМ, Hodlevskyi, SO, and Kalashchenko, SI. Medical and psychological aspects of safety and adaptation of military personnel to extreme conditions. Wiad Lek. (2020) 73:679–83. doi: 10.36740/WLek202004110
10. Ariza-Montes, A, Muniz, NM, Montero-Simó, MJ, and Araque-Padilla, RA. Workplace bullying among healthcare workers. Int J Environ Res Public Health. (2013) 10:3121–39. doi: 10.3390/ijerph10083121
11. Kristensen, P, Weisæth, L, and Heir, T. Bereavement and mental health after sudden and violent losses: a review. Psychiatry. (2012) 75:76–97. doi: 10.1521/psyc.2012.75.1.76
12. Khorram-Manesh, A, Goniewicz, K, Burkle, FM, and Robinson, Y. Review of military casualties in modern conflicts-the re-emergence of casualties from armored warfare. Mil Med. (2022) 187:e313–21. doi: 10.1093/milmed/usab108
13. Khorram-Manesh, A, Burkle, FM, Phattharapornjaroen, P, Ahmadi Marzaleh, M, Sultan, MA, Mäntysaari, M, et al. The development of Swedish military healthcare system: part II-re-evaluating the military and civilian healthcare systems in crises through a dialogue and study among practitioners. Mil Med. (2021) 186:e442–50. doi: 10.1093/milmed/usaa364
14. Judkins, JL, Moore, BA, Collette, TL, Hale, WJ, Peterson, AL, and Morissette, SB. Incidence rates of posttraumatic stress disorder over a 17-year period in active duty military service members. J Trauma Stress. (2020) 33:994–1006. doi: 10.1002/jts.22558
15. Shahmiri Barzoki, H, Ebrahimi, M, Khoshdel, A, Noorbala, AA, Rahnejat, AM, Avarzamani, L, et al. Studying the prevalence of PTSD in veterans, combatants and freed soldiers of Iran-Iraq war: a systematic and meta-analysis review. Psychol Health Med. (2023) 28:812–8. doi: 10.1080/13548506.2021.1981408
16. Obuobi-Donkor, G, Oluwasina, F, Nkire, N, and Agyapong, VIO. A scoping review on the prevalence and determinants of post-traumatic stress disorder among military personnel and firefighters: implications for public policy and practice. Int J Environ Res Public Health. (2022) 19:1565. doi: 10.3390/ijerph19031565
17. Taal, EL, Vermetten, E, van Schaik, DA, and Leenstra, T. Do soldiers seek more mental health care after deployment? Analysis of mental health consultations in the Netherlands armed forces following deployment to Afghanistan. Eur J Psychotraumatol. (2014) 5:5. doi: 10.3402/ejpt.v5.23667
18. Teplova, AE, Bakker, HAHM, Perry, SIB, van Etten-Jamaludin, FS, Plat, MJ, and Bekkers, MBM. The impact of deployment and combat exposure on physical health among military personnel: a systematic review of incidence, prevalence, and risks. Mil Med. (2022) 187:e1074–85. doi: 10.1093/milmed/usab302
19. Chin, DL, and Zeber, JE. Mental health outcomes among military service members after severe injury in combat and TBI. Mil Med. (2020) 185:e711–8. doi: 10.1093/milmed/usz440
20. Sahebi, A, Hasheminejad, N, Shohani, M, Yousefi, A, Tahernejad, S, and Tahernejad, A. Personal protective equipment-associated headaches in health care workers during COVID-19: a systematic review and meta-analysis. Front Public Health. (2022) 10:942046. doi: 10.3389/fpubh.2022.942046
21. Nordstrand, AE, Bøe, HJ, Holen, A, Reichelt, JG, Gjerstad, CL, and Hjemdal, O. Danger- and non-danger-based stressors and their relations to posttraumatic deprecation or growth in Norwegian veterans deployed to Afghanistan. Eur J Psychotraumatol. (2019) 10:1601989. doi: 10.1080/20008198.2019.1601989
22. Knaust, T, Siebler, MBD, Tarnogorski, D, Skiberowski, P, Höllmer, H, Moritz, C, et al. Cross-sectional field study comparing hippocampal subfields in patients with post-traumatic stress disorder, major depressive disorder, post-traumatic stress disorder with comorbid major depressive disorder, and adjustment disorder using routine clinical data. Front Psychol. (2023) 14:1123079. doi: 10.3389/fpsyg.2023.1123079
23. Wittchen, HU, Schönfeld, S, Kirschbaum, C, Thurau, C, Trautmann, S, Steudte, S, et al. Traumatic experiences and posttraumatic stress disorder in soldiers following deployment abroad: how big is the hidden problem? Dtsch Arztebl Int. (2012) 109:559–68. doi: 10.3238/arztebl.2012.0559
24. Markgraf, J. Mini-DIPS—Handbuch [Mini diagnostic interview for mental disorder-handbook]. Berlin: Springer (1994).Revised by Jacobs, S., Krampe, H. and Wagner, T. (1999)
25. Wesemann, U, Willmund, GD, Ungerer, J, Kreim, G, Zimmermann, PL, Bühler, A, et al. Assessing psychological fitness in the military-development of an effective and economic screening instrument. Mil Med. (2018) 183:e261–9. doi: 10.1093/milmed/usy021
26. Fink, DS, Cohen, GH, Sampson, LA, Gifford, RK, Fullerton, CS, Ursano, RJ, et al. Incidence of and risk for post-traumatic stress disorder and depression in a representative sample of US reserve and National Guard. Ann Epidemiol. (2016) 26:189–97. doi: 10.1016/j.annepidem.2016.01.003
27. Dyball, D, Bennett, AN, Schofield, S, Cullinan, P, Boos, CJ, Bull, AMJ, et al. Mental health outcomes of male UK military personnel deployed to Afghanistan and the role of combat injury: analysis of baseline data from the ADVANCE cohort study. Lancet Psychiatry. (2022) 9:547–54. doi: 10.1016/S2215-0366(22)00112-2
28. Himmerich, H, Willmund, GD, Wesemann, U, Jones, N, and Fear, NT. European military mental health research: benefits of collaboration. J R Army Med Corps. (2017) 163:155–7. doi: 10.1136/jramc-2016-000676
29. Stene, LE, Vuillermoz, C, Overmeire, RV, Bilsen, J, Dückers, M, Nilsen, LG, et al. Psychosocial care responses to terrorist attacks: a country case study of Norway, France and Belgium. BMC Health Serv Res. (2022) 22:390. doi: 10.1186/s12913-022-07691-2
30. Pirard, P, Baubet, T, Motreff, Y, Rabet, G, Marillier, M, Vandentorren, S, et al. Use of mental health supports by civilians exposed to the November 2015 terrorist attacks in Paris. BMC Health Serv Res. (2020) 20:959. doi: 10.1186/s12913-020-05785-3
31. Knaust, T, Felnhofer, A, Kothgassner, OD, Höllmer, H, Gorzka, RJ, and Schulz, H. Virtual trauma interventions for the treatment of post-traumatic stress disorders: a scoping review. Front Psychol. (2020) 11:562506. doi: 10.3389/fpsyg.2020.562506
32. Niederhauser, M, Zueger, R, Sefidan, S, Annen, H, Brand, S, and Sadeghi-Bahmani, D. Does training motivation influence resilience training outcome on chronic stress? Results from an interventional study. Int J Environ Res Public Health. (2022) 19:6179. doi: 10.3390/ijerph19106179
33. Prell, R, Opatz, O, Merati, G, Gesche, B, Gunga, HC, and Maggioni, MA. Heart rate variability, risk-taking behavior and resilience in firefighters during a simulated extinguish-fire task. Front Physiol. (2020) 11:482. doi: 10.3389/fphys.2020.00482
34. Baubet, T. Les soins d'urgence en situation transculturelle [Emergency care in transcultural situations]. Rev Infirm. (2012) 178:24–5.
35. Mortelmans, LJ, Lievers, J, Dieltiens, G, and Sabbe, MB. Are Belgian military students in medical sciences better educated in disaster medicine than their civilian colleagues? J R Army Med Corps. (2016) 162:383–6. doi: 10.1136/jramc-2015-000563
36. Massazza, A, de Almeida, JF, Quinlan-Davidson, M, da Silva, RT, Devakumar, D, Peres, MFT, et al. Local understandings of PTSD and complex PTSD among health professionals working with adolescents in violent neighbourhoods of São Paulo city, Brazil. BMC Psychiatry. (2022) 22:196. doi: 10.1186/s12888-022-03821-6
37. Prykhodko, I. The model of psychological safety of a soldier's personality. Curr Issues Personal Psychol. (2021) 10:112–22. doi: 10.5114/cipp.2021.108684
38. Van Overmeire, R, Six, S, Deschepper, R, Vandekerckhove, M, and Bilsen, J. Association between feeling threatened, behaviour and symptoms of anxiety and depression: two and a half years after the terrorist attacks in Belgium. Community Ment Health J. (2022) 58:657–65. doi: 10.1007/s10597-021-00867-w
39. Van Overmeire, R, Van Keer, RL, and Bilsen, J. Impact of terrorist attacks on social relationships. Clin Psychol Psychother. (2021) 28:1472–81. doi: 10.1002/cpp.2587
Keywords: military personnel, PTSD, depression, anxiety, mental health, military deployment
Citation: Wesemann U, Renner K-H, Rowlands K, Köhler K, Hüttermann N and Himmerich H (2024) Incidence of mental disorders in soldiers deployed to Afghanistan who have or have not experienced a life-threatening military incident—a quasi-experimental cohort study. Front. Public Health. 12:1357836. doi: 10.3389/fpubh.2024.1357836
Edited by:
Hubert Annen, Military Academy, ETH Zurich, SwitzerlandReviewed by:
Glenna Tinney, Independent Consultant, Alexandria, US Minor Outlying IslandsMeenakshi Shukla, Allahabad University, India
Copyright © 2024 Wesemann, Renner, Rowlands, Köhler, Hüttermann and Himmerich. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulrich Wesemann, dXdAcHR6Yncub3Jn