 Yangfeng Xu1
Yangfeng Xu1 YunYing Jin
YunYing Jin- 1Department of Emergency, Dongyang People's Hospital, Dongyang, China
- 2Intensive Care Unit, Dongyang People's Hospital, Dongyang, China
Background and objective: Heatstroke (HS) is a life-threatening condition resulting from thermal injury within the body, and it is associated with a significantly high mortality rate. This study aimed to assess the knowledge, attitudes and practices (KAP) among the general community population toward heatstroke.
Methods: The web-based cross-sectional study was conducted between September 2023 and October 2023 at the Emergency Department of Dongyang People's Hospital. A self-designed questionnaire was developed to collect demographic information of the general community population and to assess their knowledge, attitudes and practices toward heatstroke.
Results: A total of 1,356 valid questionnaires were collected. Among the participants, 875 (64.53%) were female, and 496 (36.58%) had regular exercise. The mean knowledge, attitudes and practices scores were 12.73 ± 1.42 (possible range: 0–14), 33.74 ± 2.91 (possible range: 8–40) and 34.65 ± 5.30 (possible range: 8–40), respectively. The structural equation model demonstrated that education had direct effects on knowledge (β = 0.017, p < 0.001), attitudes (β = 0.123, p < 0.001), and practices (β = −0.094, p < 0.001). Moreover, knowledge had direct effects on attitudes (β = 1.920, p < 0.001), and attitudes had direct effects on practices (β = 0.642, p < 0.001).
Conclusion: The findings revealed that the general community population have sufficient knowledge, active attitudes and proactive practices toward the heatstroke. However, there is still room for improvement and it is necessary to develop and implement educational initiatives and interventions designed to further enhance their KAP toward heatstroke.
Introduction
Heatstroke (HS) arises when the human body's temperature regulation system fails due to excessive environmental heat exposure. This failure leads to a dangerous elevation in core body temperature (Tcore), surpassing 40.6°C, which in turn can cause central nervous system dysfunction, manifesting as delirium, convulsions, and coma. As a severe condition resulting from internal thermal injury, heatstroke presents a significant life-threatening risk and is associated with a notably high mortality rate (1, 2).
Exposure to a hot environment is identified as a direct precursor to heatstroke (3). Due to the progressive impact of global warming, the incidence of fatalities from heat waves is increasing. For instance, in August 2003, an extended and intense heat wave in Europe was associated with 14,800 heat-related deaths in France alone (4). Another study highlights the relationship between HS and heat waves, noting that the relative risk of HS during heat wave days, as opposed to non-heat wave days, significantly declined from 71.0 in 1999 to 3.5 in 2010 (5). In China, the epidemiology of heatstroke exhibits distinctive patterns due to the country's vast geographical diversity and climatic variations. High daily maximum temperatures are closely linked to the incidence of heatstroke, with a 30.5% excess risk for each 1°C increment over the heatwave threshold (6). Urban areas, such as Shaoxing, experience a predominance of mild heatstroke cases, although severe cases and fatalities are not uncommon (7). Heat-related illnesses in China are concentrated in urban regions, particularly around the Yangtze River, with heightened vulnerability observed in the older adult and males aged 45–64 (8). This heightened susceptibility can be attributed to the aging process of human tissues and organs, which leads to a diminished capacity for heat dissipation (9). Consequently, this reduction in thermoregulatory efficiency accelerates the increase in core body temperature during episodes of heat exposure.
Timely and effective intervention holds paramount significance in enhancing the survival rate and prognosis of heatstroke patients (4). Timely and appropriate intervention can mitigate mortality and enhance the prognosis of heatstroke patients. Initiating treatment for heatstroke at the earliest possible stage, particularly in prehospital settings such as the home, is crucial (10). Before the arrival of professional medical assistance, on-site responders are instrumental in providing immediate care to individuals suffering from heatstroke. Their roles include critical actions such as extricating patients from the hot environment and implementing cooling strategies, for instance, the use of ice blankets. Currently, there is a lack of research examining the knowledge base of the general population regarding heatstroke and the corresponding practical measures that should be taken in response.
Knowledge, Attitudes, and Practices (KAP) framework, which serves as a crucial tool in public health for assessing and enhancing the awareness, attitudes, and practices of a population regarding specific health issues, offering invaluable insights essential for designing targeted and effective health interventions (11, 12). Therefore, this study aimed to explore the KAP among the general community population toward heatstroke. This exploration sought to gauge the existing level of awareness and prevalent attitudes and practices, thereby providing valuable insights for the development of tailored educational and preventive strategies.
Methods
Study design and participants
This cross-sectional survey was conducted between September 2023 and October 2023 at the Emergency Department of Dongyang People's Hospital. The study was ethically approved by the Ethics Committee of Dongyang People's Hospital (Approval no. 2023-YX-289) and informed consent was obtained from the study participants.
The inclusion criteria for this study were as follows: (1) participants aged 18 years or above, (2) having access to the internet to complete the web-based questionnaire, and (3) volunteering for participation in the study and demonstrate an understanding of the questionnaire. Data collection was conducted anonymously. To avoid duplicate responses, an IP restriction was applied, meaning that the survey could be filled out only once from any given IP address.
Questionnaire
The questionnaire was crafted following the guidelines outlined in the Expert consensus on the diagnosis and treatment of Heatstroke in China (13) and pertinent literature on heatstroke (14–16). The initial draft underwent refinement through feedback from two senior experts, all holding the title of associate professor, with expertise in emergency medicine. Following these revisions, a preliminary trial was conducted on a limited scale (n = 38), yielding a Cronbach's alpha coefficient value of 0.738, indicative of good internal consistency.
The final questionnaire, written in Chinese, encompassed four dimensions: demographic information, knowledge, attitudes and practices. The demographic section comprised 14 items, while the knowledge, attitudes, and practices dimensions included 16, 8, and 8 items, respectively. Notably, questions K2 and K14 were intentionally designed as trap questions, presenting precisely opposite meanings, both of them were excluded from scoring and subsequent statistical analyses. Participants who selected “right” or “wrong” for both questions were considered to have a logical conflict and were subsequently excluded from the survey. Consequently, the knowledge items were assigned 1 point for a correct answer and 0 points for incorrect responses, resulting in a possible score range of 0–14. The attitude items were scored on a five-point Likert scale ranging from very positive (5 points) to very negative (1 point), with a possible score range of 8 to 40. Similarly, the practice items were scored on a five-point Likert scale, ranging from very consistent (5 points) to very inconsistent (1 point), with a possible score range of 8 to 40. Sufficient knowledge, active attitudes, and proactive practices were defined as achieving scores surpassing 75% of the maximum possible score in each respective section (17).
The data were gathered through an online questionnaire administered via Sojump (http://www.sojump.com). This questionnaire was disseminated through WeChat platform.
Statistical analysis
STATA 17.0 (Stata Corporation, College Station, TX, USA) was used for statistical analysis. The continuous variables were expressed as mean ± standard deviation (SD), and the categorical variables was expressed as n (%). The continuous variables conformed to a normal distribution were tested by the t-test or ANOVA. In multivariate analysis, 75% of the total score was used as the cut-off value. Pearson correlation was used to analyze the correlation between knowledge, attitudes, and practices. The structural equation model (SEM) for evaluating knowledge, attitudes, and practices regarding heatstroke among the general community population was established using AMOS 24.0 (IBM, NY, United States). The model fitting was evaluated with CMIN/DF (Chi-square fit statistics/degree of freedom), RMSEA (root mean square error of approximation), IFI (incremental fix index), TLI (Tucker-Lewis index) and CFI (comparative fix index). Two-sided p < 0.05 were considered statistically significant.
Results
In this study, 1,356 questionnaires were collected. Among the participants, 875 (64.53%) of them were female and the average age was 39.73 ± 9.81 years old. A total of 849 (62.61%) presented BMI within the range of 18.5 to 23.9 kg/m2. A majority, comprising 699 individuals (51.55%), were indoor workers. Notably, 1,026 participants (75.66%) reported no habits of smoking or drinking. Regular physical activity was reported by 496 participants (36.58%), and 1,186 (87.46%) were not aware of any recent heatstroke incidents around them recently. The mean knowledge, attitude and practice scores were 12.73 ± 1.42 (possible range: 0–14), 33.74 ± 2.91 (possible range: 8–40) and 34.65 ± 5.30 (possible range: 8–40), respectively (Table 1).
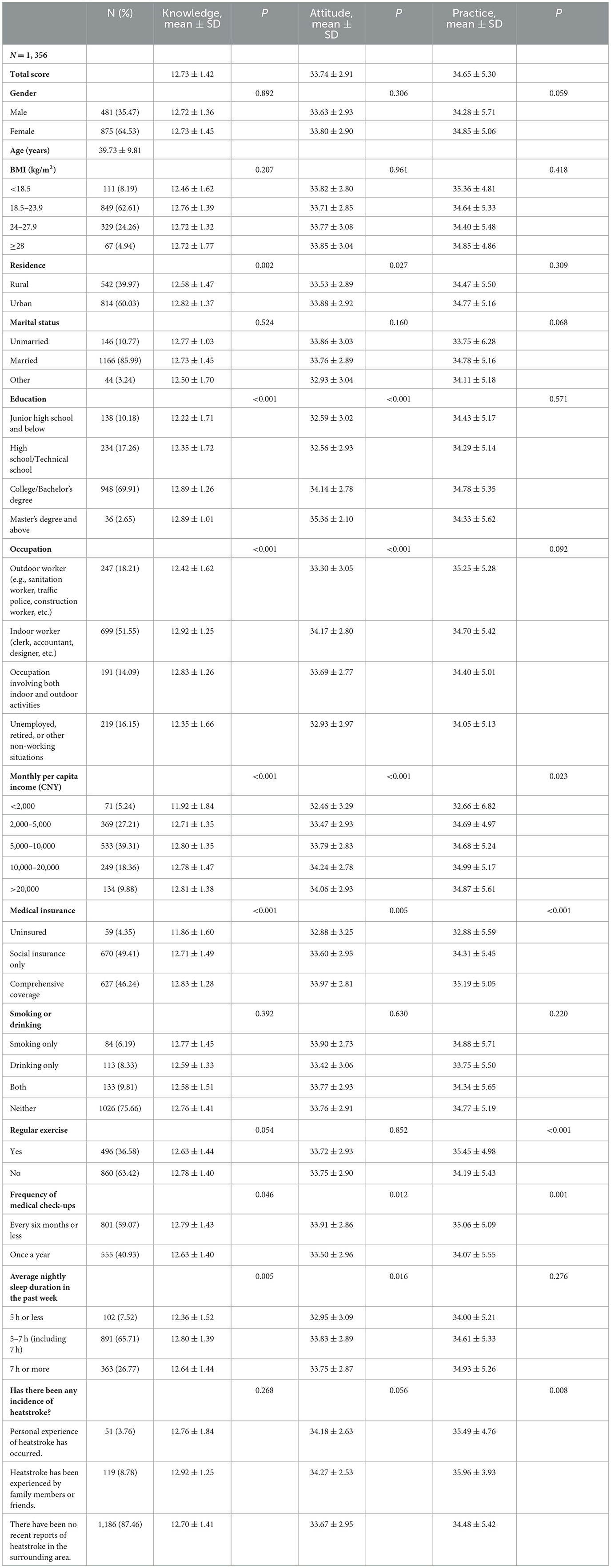
Table 1. Knowledge, attitudes, and practices scores and demographic characteristics.
The three knowledge items with the highest correctness rates were as follows: “On-site treatment for heatstroke patients should involve laying them flat, tilting their head to one side, unfastening buttons and belts, and removing outer clothing to facilitate breathing and heat dissipation.” (K12) with 98.16%, “Environments with high temperatures and high humidity are prone to induce heatstroke.” (K3) with 97.42%, and “Outdoor laborers (such as farmers, construction workers) or individuals engaging in high-intensity sports (such as athletes or trainees in military exercises) are more susceptible to heatstroke.” (K6) with 97.27%. The three items with the lowest correctness rates were “Once heatstroke occurs, even in extremely hot environments, the patient should not be moved.” (K11) with 71.02%, “If heatstroke-induced coma occurs during physical training, and the person quickly regains consciousness, hospital treatment may not be necessary.” (K15) with 75.22%, and “Inadequate rest time may induce heatstroke.” (K8) with 85.99% (Table 2).
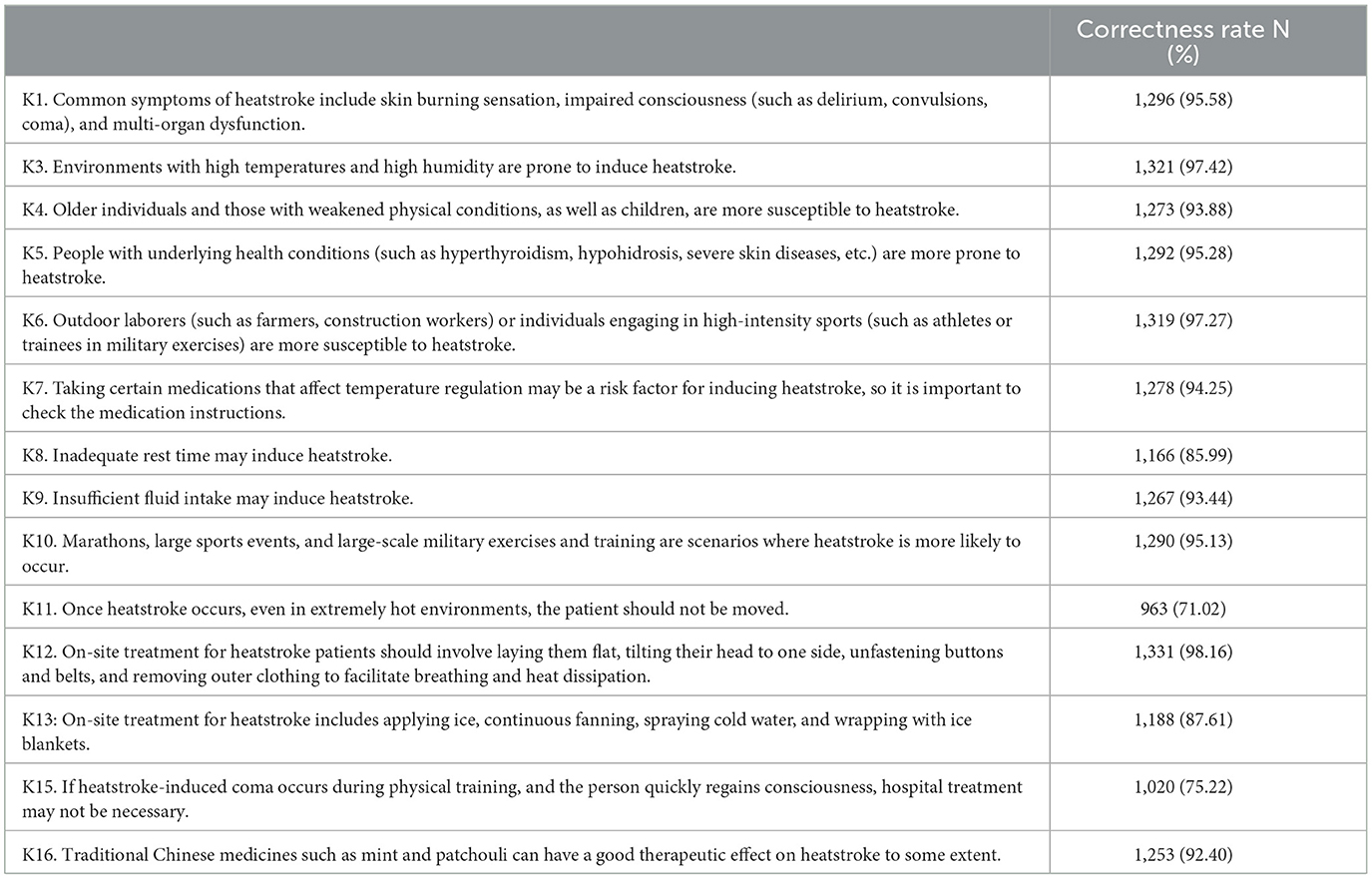
Table 2. Knowledge.
The responses to the attitude items indicated that most of the participants have a very positive or positive attitude toward all the items, specifically: 64.97 % strongly agree that knowledge about heatstroke is important for prevention and treatment (A1). Moreover, 65.56% strongly approved that employers should provide more measures to protect employees from heatstroke (A4). In addition, 51.62% were very worried about themselves or their relative experiencing heatstroke in the high temperatures (A5), and 59.14% were very willing to assist in the treatment of patients (A8) (Table 3).
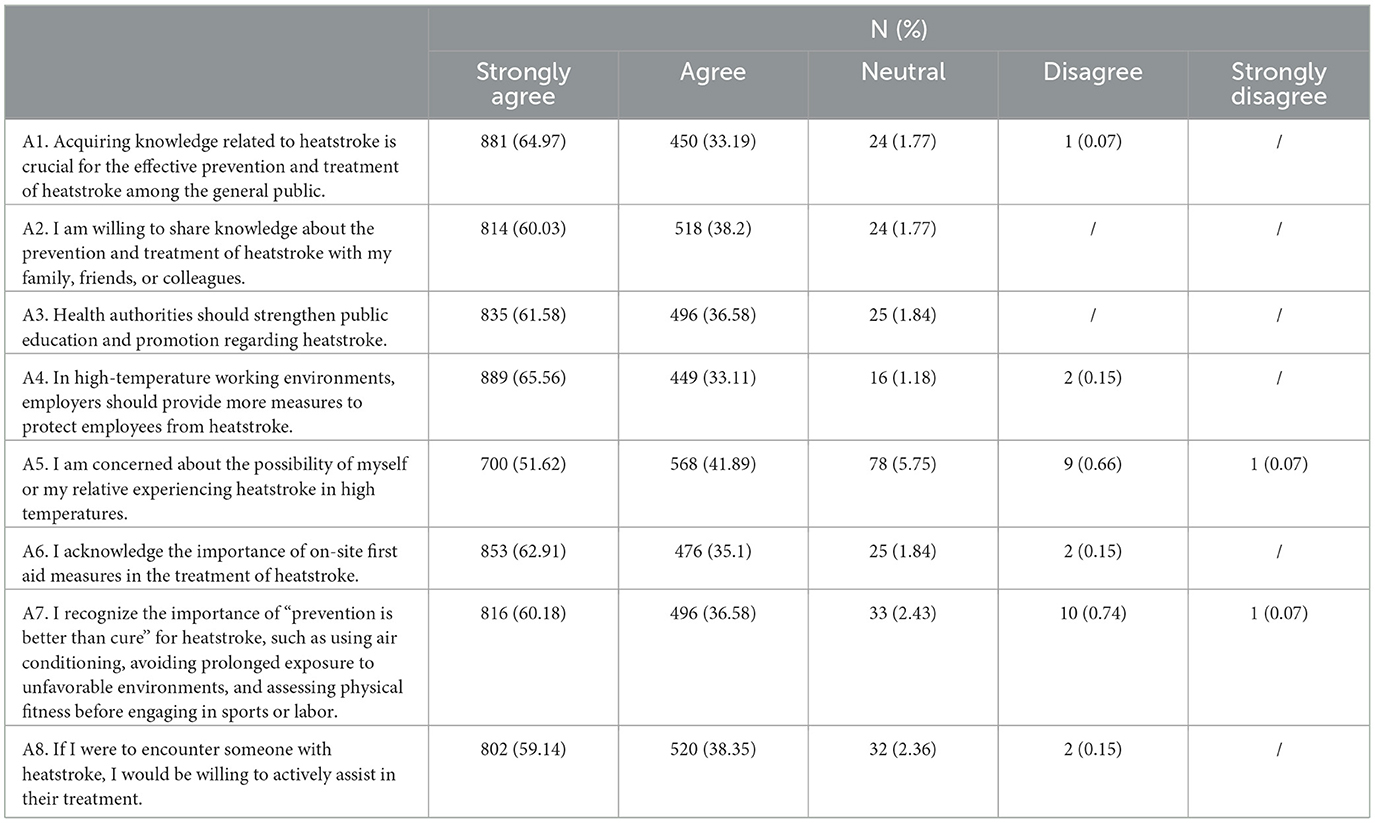
Table 3. Attitudes.
Moreover, 49.19% of them were very willing to participate in training related to heatstroke first aid (P2). In hot weather, 59% were well hydrated (P5), 56.49% were concerned about the possible effects of medication on thermoregulation (P6), 58.78% were alerted to symptoms such as burning skin and dizziness (P7), and 58.33% prompted those around them to take precautions (P8) (Table 4).

Table 4. Practices.
Pearson's analysis was performed to assess the relationship between knowledge, attitude, and practice. It demonstrated that knowledge and attitudes were positively correlated (r = 0.177, P < 0.001), and knowledge and practices were also positively correlated (r = 0.079, P = 0.004). Additionally, there was a positive correlation between attitudes and practices (r = 0.454, P < 0.001) (Supplementary Table S1).
Multivariate analysis showed that occupation of outdoor worker (OR = 0.476, 95% CI: 0.259–0.876, P = 0.017) was independently associated with sufficient knowledge (Supplementary Table S2). Meanwhile, knowledge (OR = 1.208, 95% CI: 1.108–1.318, P < 0.001), age (OR = 0.982, 95% CI: 0.968–0.996, P = 0.013), master's degree and above (OR = 3.929, 95% CI: 1.108–13.935, P = 0.034), and monthly per capita income (CNY) of 10,000–20,000 CNY (OR = 2.075, 95% CI: 1.108–3.884, P = 0.023) were independently associated with active attitudes (Supplementary Table S3). Furthermore, attitudes (OR = 1.287, 95% CI: 1.225–1.351, P < 0.001), monthly per capita income (CNY) of 2,000–5,000 CNY (OR = 2.180, 95% CI: 1.187–4.006, P = 0.012), having regular exercise (OR = 1.829, 95% CI: 1.335–2.505, P < 0.001), having medical check-ups every 6 months or less (OR = 1.370, 95% CI: 1.026–1.830, P = 0.033), and heatstroke having been experienced by family members or friends (OR = 2.267, 95% CI: 1.203–4.273, P = 0.011) were independently associated with proactive practice (Supplementary Table S4).
The fitting index of the structural equation model (CMIN/DF = 5.180; RMSEA = 0.056; IFI = 0.908; TLI = 0.900; CFI = 0.908) outperformed the respective threshold value, signifying that the data satisfactorily fit the structural model (Supplementary Table S5). The results showed that education had direct effects on knowledge (β = 0.017, p < 0.001), attitudes (β = 0.123, p < 0.001), and practices (β = −0.094, p < 0.001). Moreover, knowledge had direct effects on attitudes (β = 1.920, p < 0.001), and attitudes had direct effects on practices (β = 0.642, p < 0.001) (Supplementary Table S6 and Figure 1).
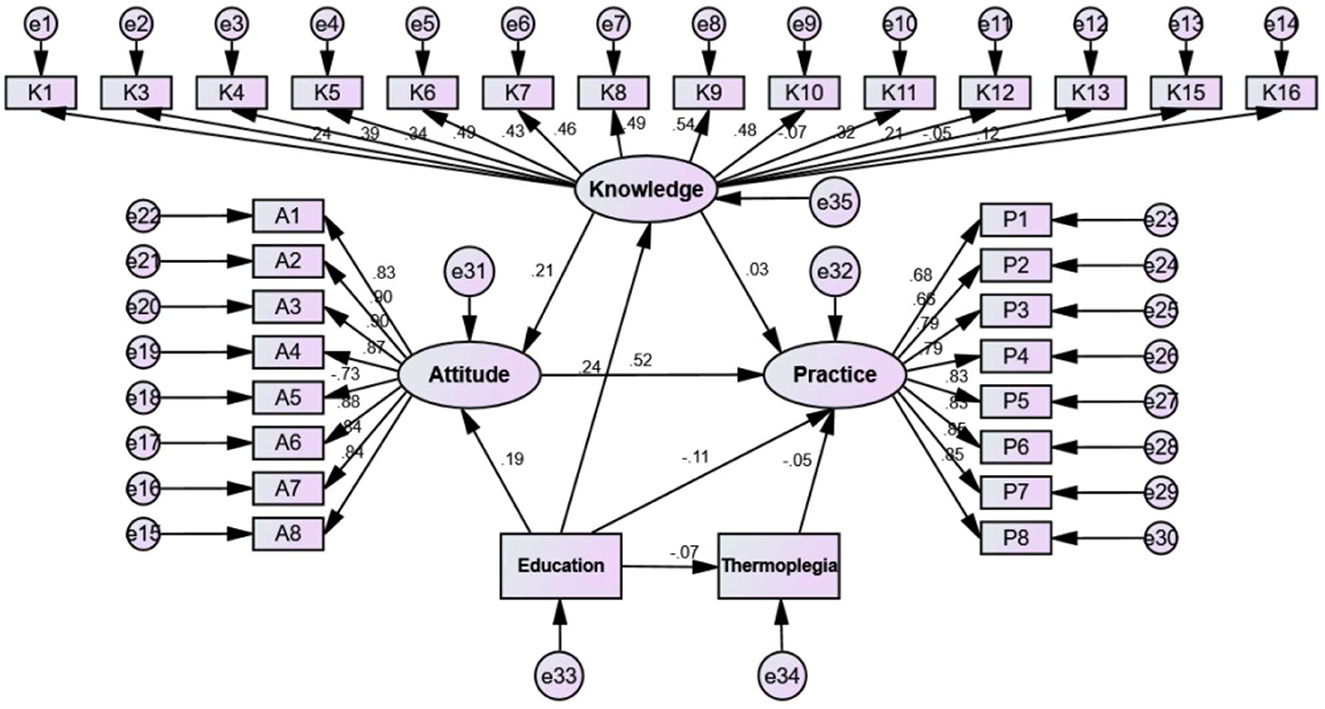
Figure 1. Structural equation modeling.
Discussion
This study revealed that the general community population have sufficient knowledge, active attitudes and proactive practices toward the heatstroke.
Participants demonstrated commendable awareness regarding common symptoms and risk factors for heatstroke, such as high temperatures and humidity. However, notable knowledge gaps exist concerning the appropriate response to heatstroke-induced coma during physical training and the potential therapeutic effects of traditional Chinese medicines. Previous studies have highlighted the importance of public knowledge in preventing heat-related illnesses (18, 19), yet disparities in specific knowledge areas underscore the need for targeted educational campaigns.
Most of the participants exhibited positive inclinations toward acquiring knowledge and sharing it with others. However, concerns arise regarding the perceived necessity of public education on heatstroke and employer responsibilities in high-temperature work environments. These findings align with research emphasizing the role of positive attitudes in promoting health-related behaviors (20, 21), yet the identified gaps suggest the potential for reinforcing educational initiatives, especially in workplace settings. Recognizing the positive attitudes toward employer responsibilities in high-temperature work environments, workplace interventions are crucial.
In terms of practices, participants reported consistent engagement in acquiring knowledge through various channels and assessing their health before physical exertion. However, disparities exist, with fewer individuals engaging in on-site first aid training and preparing home items for heatstroke prevention. These findings echo the importance of knowledge translation into practical behaviors (22, 23) while highlighting areas for intervention, particularly in enhancing first aid preparedness. Collaboration with local healthcare providers and community organizations can facilitate the implementation of such programs (24). While many participants reported consistent practices in acquiring knowledge and assessing health before physical exertion, there is room for improvement in home-based preventive measures. Public health campaigns should encourage individuals to prepare home items, such as thermometers, blood pressure monitors, and ice packs, to handle potential heatstroke occurrences. Practical guidance on assembling a heatstroke preparedness kit can be disseminated through various channels, including social media and community workshops (25).
Notably, urban residents demonstrated higher mean scores in both knowledge and attitude compared to their rural counterparts in this study, underscoring the potential influence of urbanization on awareness and attitudes toward heatstroke. This aligns with existing literature suggesting that urban areas often have better access to health information and resources, potentially contributing to heightened knowledge and more positive attitudes (26, 27). This finding resonates with numerous studies emphasizing the positive correlation between education and health-related knowledge (28, 29). The pronounced impact of occupation, particularly the lower knowledge scores among outdoor workers, aligns with previous research indicating occupational disparities in health knowledge (30, 31). Additionally, the positive correlation between monthly per capita income and knowledge and attitude scores emphasizes the role of socio-economic factors in shaping KAP outcomes, reflecting findings from studies on health literacy and socio-economic status (32, 33). This study highlights the significant influence of urbanization, occupation, and socio-economic status on the KAP toward heatstroke, revealing key disparities and potential areas for targeted educational and resource allocation efforts.
Moreover, the results of SEM demonstrated that education exerted direct positive effects on knowledge, attitudes, and practices, aligning with the notion that educational interventions can be instrumental in fostering a holistic approach to heatstroke prevention (34), suggesting that educational interventions could be pivotal in enhancing heatstroke prevention measures. However, the negative association between education and practices might indicate that while education improves knowledge and attitudes, it does not always translate into practical application. This paradox warrants further investigation, possibly indicating a gap between theoretical understanding and real-world implementation that needs to be addressed through more practical, hands-on educational strategies.
The limitations of the study include its cross-sectional nature, which precludes causal inferences, and the potential for self-selection bias. Additionally, the web-based distribution of the questionnaire may have excluded individuals with limited internet access or technological proficiency. Future research should aim to include these populations to provide a more comprehensive understanding of the community's KAP toward heatstroke.
Nevertheless, this study still holds significant clinical relevance as it offers valuable insights into the current state of knowledge, attitudes, and practices toward heatstroke, which can guide the development of targeted educational and preventive strategies in healthcare settings.
Conclusion
The findings revealed that the general community population have sufficient knowledge, active attitudes and proactive practices toward the heatstroke. However, there is still room for improvement and it is necessary to develop and implement educational initiatives and interventions designed to further enhance their KAP toward heatstroke. Employers should implement comprehensive measures to protect outdoor workers, providing adequate rest time, hydration facilities, and heat-resistant clothing. Educational programs within workplaces can further enhance employees' awareness of heatstroke risks and preventive measures.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Dongyang People's Hospital (Approval No. 2023-YX-289). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YX: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. JC: Conceptualization, Data curation, Formal analysis, Writing – review & editing. JD: Conceptualization, Data curation, Formal analysis, Writing – review & editing. YJ: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1373025/full#supplementary-material
References
1. Dong X, Li JJ, Ma N, Liu AZ, Liu JW. Anti-inflammatory and anti-oxidative effects of isorhamnetin for protection against lung injury in a rat model of heatstroke in a dry-heat environment. Med Sci Monit. (2022) 28:e935426. doi: 10.12659/MSM.935426
2. Deng Q, Zhao J, Liu W, Li Y. Heatstroke at home: prediction by thermoregulation modeling. Build Environ. (2018) 137:147–56. doi: 10.1016/j.buildenv.2018.04.017
3. Lin Y, Zhang Y. Renoprotective effect of oral rehydration solution III in exertional heatstroke rats. Ren Fail. (2019) 41:190–6. doi: 10.1080/0886022X.2019.1590211
4. Argaud L, Ferry T, Le QH, Marfisi A, Ciorba D, Achache P, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. (2007) 167:2177–83. doi: 10.1001/archinte.167.20.ioi70147
5. Wang Y, Bobb JF, Papi B, Wang Y, Kosheleva A, Di Q, et al. Heat stroke admissions during heat waves in 1,916 US counties for the period from 1999 to 2010 and their effect modifiers. Environ Health. (2016) 15:83. doi: 10.1186/s12940-016-0167-3
6. Li Y, Li C, Luo S, He J, Cheng Y, Jin Y. Impacts of extremely high temperature and heatwave on heatstroke in Chongqing, China. Environ Sci Pollut Res Int. (2017) 24:8534–40. doi: 10.1007/s11356-017-8457-z
7. Jiang GQ Li M, Xing C, Wang SS, Tao JH. Epidemiological features of heatstroke in Shaoxing, China in 2008-2014. Chin J Ind Hyg Occup Dis. (2016) 34:131–3. doi: 10.3760/cma.j.issn.1001-9391.2016.02.014
8. Gu S, Huang C, Bai L, Chu C, Liu Q. Heat-related illness in China, summer of 2013. Int J Biometeorol. (2016) 60:131–7. doi: 10.1007/s00484-015-1011-0
9. Ou Y, Wang F, Zhao J, Deng Q. Risk of heatstroke in healthy elderly during heatwaves: a thermoregulatory modeling study. Build Environ. (2023) 237:110324. doi: 10.1016/j.buildenv.2023.110324
10. Zhao J, Wang H, Li Y, Xiao F, Deng Q. Heatstroke recovery at home as predicted by human thermoregulation modeling. Build Environ. (2020) 173:106752. doi: 10.1016/j.buildenv.2020.106752
11. Aerts C, Revilla M, Duval L, Paaijmans K, Chandrabose J, Cox H, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. (2020) 14:e0008149. doi: 10.1371/journal.pntd.0008149
12. Mumena WA. Maternal knowledge, attitude and practices toward free sugar and the associations with free sugar intake in children. Nutrients. (2021) 13:403. doi: 10.3390/nu13124403
13. Liu SY, Song JC, Mao HD, Zhao JB, Song Q. Expert consensus on the diagnosis and treatment of heat stroke in China. Military Med Res. (2020) 7:1. doi: 10.1186/s40779-019-0229-2
14. Bouchama A, Abuyassin B, Lehe C, Laitano O, Jay O, O'Connor FG, et al. Classic and exertional heatstroke. Nat Rev Dis Primers. (2022) 8:8. doi: 10.1038/s41572-021-00334-6
15. Rublee C, Dresser C, Giudice C, Lemery J, Sorensen C. Evidence-based heatstroke management in the emergency department. West J Emerg Med. (2021) 22:186–95. doi: 10.5811/westjem.2020.11.49007
16. Singletary EM, Zideman DA, Bendall JC, Berry DC, Borra V, Carlson JN, et al. International consensus on first aid science with treatment recommendations. Circulation. (2020) 142:S284–334. doi: 10.1161/CIR.0000000000000897
17. Malaeb D, Sallam M, Younes S, Mourad N, Sarray El Dine A, Obeid S, et al. Knowledge, attitude, and practice in a sample of the lebanese population regarding cholera. Int J Environ Res Pub Health. (2022) 19:243. doi: 10.3390/ijerph192316243
18. Luque JS, Becker A, Bossak BH, Grzywacz JG, Tovar-Aguilar JA, Guo Y. Knowledge and practices to avoid heat-related illness among hispanic farmworkers along the Florida-Georgia line. J Agromedicine. (2020) 25:190–200. doi: 10.1080/1059924X.2019.1670312
19. Yezli S, Mushi A, Yassin Y, Maashi F, Khan A. Knowledge, attitude and practice of pilgrims regarding heat-related illnesses during the 2017 Hajj Mass gathering. Int J Environ Res Pub Health. (2019) 16:215. doi: 10.3390/ijerph16173215
20. Kubzansky LD, Huffman JC, Boehm JK, Hernandez R, Kim ES, Koga HK, et al. Positive psychological well-being and cardiovascular disease: JACC health promotion series. J Am Coll Cardiol. (2018) 72:1382–96. doi: 10.1016/j.jacc.2018.07.042
21. Rice EL, Klein WMP. Interactions among perceived norms and attitudes about health-related behaviors in U.S. adolescents. Health Psychol Off J Div Am Psychol Assoc. (2019) 38:268–75. doi: 10.1037/hea0000722
22. Castner J. Knowledge translation of science advances into emergency nursing practice with the reach, effectiveness, adoption, implementation, and maintenance framework. J Emerg Nurs. (2020) 46:141–6. doi: 10.1016/j.jen.2020.01.006
23. Lambert K, Mahoney K, Parfrey PS. Changing health-related behaviors 4: realizing impact of health research through knowledge translation. Methods Mol Biol. (2021) 2249:597–612. doi: 10.1007/978-1-0716-1138-8_32
24. Alkassas W, Rajab AM, Alrashood ST, Khan MA, Dibas M, Zaman M. Heat-related illnesses in a mass gathering event and the necessity for newer diagnostic criteria: a field study. Environ Sci Pollut Res Int. (2021) 28:16682–9. doi: 10.1007/s11356-020-12154-4
25. Sulzer M, Christen A, Matzarakis A. A low-cost sensor network for real-time thermal stress monitoring and communication in occupational contexts. Sensors. (2022) 22:828. doi: 10.3390/s22051828
26. Whitehead J, Pearson AL, Lawrenson R, Atatoa-Carr P. Spatial equity and realised access to healthcare - a geospatial analysis of general practitioner enrolments in Waikato, New Zealand. Rural Remote Health. (2019) 19:5349. doi: 10.22605/RRH5349
27. Xu R, Mu T, Liu Y, Ye Y, Xu C. Trends in the disparities and equity of the distribution of traditional Chinese medicine health resources in China from 2010 to 2020. PLoS ONE. (2022) 17:e0275712. doi: 10.1371/journal.pone.0275712
28. Stasch L, Ohlendorf J, Baumann U, Ernst G, Lange K, Konietzny C, et al. Parental disease specific knowledge and its impact on health-related quality of life. Children. (2022) 9:98. doi: 10.3390/children9010098
29. Yang Y, Wang S, Chen L, Luo M, Xue L, Cui D, et al. Socioeconomic status, social capital, health risk behaviors, and health-related quality of life among Chinese older adults. Health Qual Life Outcomes. (2020) 18:291. doi: 10.1186/s12955-020-01540-8
30. Khayatzadeh-Mahani M, Hassani Mehraban A, Kamali M, Parvizy S, Haghani H, Amini M. Development and validation of occupation based practice measure (OBPM). Can J Occup Ther Rev Can d'ergotherapie. (2022) 89:283–93. doi: 10.1177/00084174221102722
31. Krzepota J, Sadowska D, Biernat E. Relationships between physical activity and quality of life in pregnant women in the second and third trimester. Int J Environ Res Pub Health. (2018) 15:745. doi: 10.3390/ijerph15122745
32. Li C, Guo Y. The effect of socio-economic status on health information literacy among urban older adults: evidence from western China. Int J Environ Res Public Health. (2021) 18:501. doi: 10.3390/ijerph18073501
33. Zanobini P, Lorini C, Lastrucci V, Minardi V, Possenti V, Masocco M, et al. Health literacy, socio-economic determinants, and healthy behaviours: results from a large representative sample of Tuscany Region, Italy. Int J Environ Res Pub Health. (2021) 18:2432. doi: 10.3390/ijerph182312432
Keywords: knowledge, attitudes, practices, heatstroke, cross-sectional study
Citation: Xu Y, Chen J, Du J and Jin Y (2024) Knowledge, attitudes, and practices among the general community population toward heatstroke. Front. Public Health 12:1373025. doi: 10.3389/fpubh.2024.1373025
Received: 19 January 2024; Accepted: 13 May 2024;
Published: 24 May 2024.
Edited by:
Morteza Arab-Zozani, Birjand University of Medical Sciences, IranReviewed by:
Qihong Deng, Zhengzhou University, ChinaRamji Bogati, Nepal Open University, Nepal
Hamidreza Aghababaeian, Dezful University of Medical Sciences (DUMS), Iran
Copyright © 2024 Xu, Chen, Du and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: YunYing Jin, MTU4Njc5NzA0NzZAMTYzLmNvbQ==