 Pablo del Pozo-Herce1,2Enrique Baca-García1,2
Pablo del Pozo-Herce1,2Enrique Baca-García1,2 Antonio Martínez-Sabater3,4
Antonio Martínez-Sabater3,4 Elena Chover-Sierra3,5
Elena Chover-Sierra3,5 Vicente Gea-Caballero6
Vicente Gea-Caballero6 Javier Curto-Ramos7
Javier Curto-Ramos7 Michal Czapla8,9
Michal Czapla8,9 Piotr Karniej10
Piotr Karniej10 Jesús Martínez-Tofe9*Mercedes Sánchez-Barba11Regina Ruiz de Viñaspre9
Jesús Martínez-Tofe9*Mercedes Sánchez-Barba11Regina Ruiz de Viñaspre9 Raúl Juárez-Vela9,12
Raúl Juárez-Vela9,12- 1Department of Psychiatry, Fundación Jimenez Diaz University Hospital, Madrid, Spain
- 2Instituto de Investigación Sanitaria de la Fundación Jiménez Díaz, Madrid, Spain
- 3Nursing Department, Nursing Care and Education Research Group (GRIECE), Universitat de Valencia, Valencia, Spain
- 4Care Research Group (INCLIVA), Hospital Clinico Universitario de Valencia, Valencia, Spain
- 5Internal Medicine, Consorci Hospital University of Valencia, Valencia, Spain
- 6Faculty of Health Sciences, Research Group Community Health and Care, International University of Valencia, Valencia, Spain
- 7Department of Psychiatry, Clinical Psychology and Mental Health, La Paz University Hospital, Madrid, Spain
- 8Department of Emergency Medical Service, Faculty of Health Sciences, Wroclaw Medical University, Wrocław, Poland
- 9Department of Nursing, Faculty of Health Sciences, Research Group in Care, University of La Rioja, Logroño, Spain
- 10Faculty of Finance and Management, WSB University in Wroclaw, Wroclaw, Poland
- 11Department of Statistics, Faculty of Medicine, University of Salamanca, Salamanca, Spain
- 12Faculty of Medicine, Biomedical Institute of Salamanca, Prevention and Early Intervention in Mental Health, University of Salamanca, Salamanca, Spain
Background: In recent years, there has been an increasing use of sex-related substances (known as “Chemsex”) to facilitate, intensify, and prolong the sexual experience of men who have sex with men. This phenomenon poses a public health problem, increasing the risk of sexually transmitted infections (STIs) and mental disorders.
Objective: The primary aim of this study was to delve into the correlation between substance use and sexual health, specifically examining the association between different substances used and the risk of sexually transmitted infections (STIs) in the context of Chemsex in Spain.
Methods: An observational, descriptive, cross-sectional study was conducted among 563 Spanish participants between January and April 2023. Non-probabilistic purposive sampling was used by the investigators. The researchers administered a questionnaire to men who have sex with men who use substances, especially in the sexual sphere, in all the autonomous communities of Spain.
Results: 14.7% reported having practiced slamsex in the last year, and 17.94% were diagnosed with a Sexually Transmitted Infection in the previous 6 months. Of these, 21% were on PREP treatment, with the main STIs being gonorrhea (p < 0.001), chlamydia (p < 0.001), genital herpes (p = 0.020), and syphilis (p < 0.001). The 63.7% used methamphetamines as the main drug in the practice of chemsex.
Discussion: Chemsex in Spain is linked to a high prevalence of STIs, especially gonorrhea and chlamydia, even among those on PrEP treatment. The use of various drugs during chemsex, such as amyl nitrite, GHB, ecstasy, and others, correlates with higher rates of STIs, highlighting the need for interventions to reduce risk and harm. The drugs most associated with slamsex include ketamine, mephedrone, and methamphetamine, underscoring the importance of addressing the risk behaviors associated with this activity.
Conclusion: This study shows that chemsex appears to be associated with a high prevalence among men who have sex with men. Who use multiple substances in a sexual context, and are particularly exposed to sexually transmitted infections (STIs), indicating a particular need for STI prevention and care in this group.
1 Introduction
In recent years, there has been an increase in the intentional use of drugs for sex, which can last for hours or even days, among men who have sex with men (MSM) (1–6). The recreational uses of substances vary in place or environment. Some of these recreational consumptions take place in sexual environments, a term known in Europe as sexualized substance use, where we include “Chemsex” linked to the LGTBIQ+ sexual culture (7). However, we find other denominations in the world, such as “Intensive sex partying” in Australia (8), “Party and Play” (PnP) in North America, or even “sexualized drugs” used more in the general population (9). This shows that it is a global problem present at the international level.
The Chemsex phenomenon has been linked to risky sexual behaviors, as well as an increase in sexually transmitted infections (1, 10–13). According to the latest European online survey for MSM (EMIS - 2017), the section on substance use revealed the prevalence of substance use for sexual purposes in the last 12 months was 14.1% (14, 15), with Spain being one of the countries with the highest prevalence of chemsex at the European level (16, 17). The substances most commonly used in the practice of Chemsex include methamphetamine, mephedrone, and other synthetic cathinones, gamma-hydroxybutyric acid/gamma-butyrolactone (GHB/GBL) (1, 2, 9, 14, 15, 18–26) alkyl nitrites (poppers) (27) medication for erectile dysfunction (6, 28–30) and less frequently other substances such as cocaine and ketamine (13, 22, 31). If the consumption of these psychoactive substances is intravenous (19, 32) in this context, it is called slamming or slamsex (1, 6, 14, 25, 28, 29).
Several sexual practices have been described in context of chemsex, such as unprotected anal intercourse or “bareback” (33, 34) “fist-fucking” (19, 32, 33, 35) group sex (33) which have been associated with an increased risk of being diagnosed with sexually transmitted infections (STIs) such as gonorrhea, chlamydia, syphilis (6, 11, 18, 21, 23–27, 29, 32, 35–38), hepatitis C (HCV) and HIV (15, 19, 22, 30, 39). For this reason, chemsex is considered a health concern due to the increase in HIV primary infection, hepatitis C reinfections (14), and, in general, a higher probability of acquiring sexually transmitted diseases (STDs) (1, 14, 23). A higher incidence has been observed in PLHIV (People living with HIV) versus MSM who do not have HIV (15, 25). As a consequence, PLHIV are at increased risk for mental health problems (6, 25, 32, 34), specifically anxiety and depression (23, 36). In the same vein, Chemsex practices have been associated with increased risk of psychosis (6, 14) and delusional thoughts due to chronic methamphetamine use (29, 40), suicidal ideation (6, 41) anxiety, depression (14, 34), overdose (15), behavioral disturbances (6), substance addiction (26) and reduced adherence to PrEP treatment (6).
The reasons why MSM engage in chemsex can be diverse, including increasing libido (27), intensifying sexual pleasure (18), facilitating sexual euphoria and disinhibition (39), better management of negative emotions such as lack of self-confidence during sex (14,40.43), improved perceived quality of sex and relationship with internalized homophobia (14), prolonged duration of sex sessions (1) and realization of sexual fantasies.
Furthermore, the rapid changes in substance consumption, including the expansion of new psychoactive substances (NPS) reported in Europe (42), underscore the need to explore the profile of substance consumption in sexual contexts among MSM. Understanding these profiles could provide insights into the possible connection between chemsex and MSM participation in these practices, particularly in light of the association between chemsex and sexually transmitted infections (STIs), as well as the emergence of antibiotic-resistant infections.
2 Materials and methods
2.1 Study design
An observational and descriptive cross-sectional study was conducted between January and April 2023.
2.2 Population and scope of the study
The study was conducted across all autonomous communities of Spain. The investigators employed non-probabilistic purposive sampling. The sample consisted of n = 563 participants who met the following inclusion criteria: (1) being over 18 years old, (2) identifying as male, (3) experiencing attraction to men or identifying as MSM (men who have sex with men), (4) possessing proficiency in Spanish to complete the questionnaire, and (5) engaging in both sexual relations and substance use. Exclusion criteria included: (1) refusal to provide informed consent and (2) participants who incorrectly filled out or left the questionnaire incomplete.
2.3 Sociodemographic characteristics
Participants were asked to provide a series of sociodemographic characteristics as part of the survey data related to the study phenomenon. These characteristics included age, gender identity, sexual behavior, marital status, autonomous community, employment status, socioeconomic level, monthly income, level of education, and relationship status.
2.4 Study variables
To investigate substance use, participants were asked whether, within the past 12 months, they had utilized substances both in a sexual context to enhance, heighten, or extend sexual activity and in a non-sexual context.
The substances included in the questionnaire were amyl nitrites, medication for erectile dysfunction GHB/GBL, alcohol, tobacco, ecstasy, amphetamines, ketamine, methamphetamine, mephedrone, cannabis, cocaine, opioid analgesics, and heroin. The use of more than one of these substances in connection with the practice of Chemsex was considered poly-drug use. Participants were also asked about administration routes (oral or injecting). A new category called “Other substances” was introduced, allowing participants to specify any substance they used that wasn’t listed among the provided options.
The questionnaire featured a comprehensive list of substances, including tobacco, alcohol, cannabis, and cocaine. These substances were explicitly included due to their frequent association with the practice of chemsex, as supported by existing literature. Moreover, other substances commonly linked to chemsex were also included in the questionnaire, ensuring a thorough examination of substance use patterns in this context (39).
The survey was created digitally using the Microsoft Forms® platform and was subsequently migrated to the www.estudioenfermeria.com platform for digital dissemination and intellectual property control to increase methodological control and avoid duplication. The online questionnaire received 1,179 responses. Participants were recruited through disseminating the questionnaire on social networks, LGTBI-related websites, social media channels, sexual health clinics, geolocation applications, and LGTBI groups.
Participants were not offered any incentives for taking part in the study. All data were collected voluntarily, anonymously, and confidentially. The questionnaire typically required around 10 to 20 min to complete. Participants were provided with the principal investigator’s contact email address for any queries regarding the questionnaire or the study. They were explicitly informed that completing the questionnaire was voluntary and their participation was anonymous and confidential. They were also assured that they could withdraw from the study at any point if they wished to do so.
2.5 Risky sexual practices and STIs testing
Participants were queried about their marital status and if they were in a committed relationship, as well as whether they were currently using pre-exposure prophylaxis (PrEP). Moreover, participants were prompted to disclose if they had contracted any sexually transmitted infections (STIs) within the past 6 months. The STIs listed in the questionnaire encompassed Gonorrhea, Chlamydia, Genital Herpes, Syphilis, HIV, Monkeypox, and Hepatitis. A category “other STIs” was added, in which participants could specify whether they had acquired any STIs not previously collected in sexual practice in the last 6 months. A category was also collected where they had not had any STIs in the previous 6 months. The reason for choosing 6 months is because there has been an increase in STIs in the last few months (38, 43).
2.6 Statistical analysis
Descriptive analyses were conducted to examine the sociodemographic characteristics of the sample. Frequencies of Chemsex behaviors and other risky sexual practices were computed. Furthermore, differences between homosexual and heterosexual men concerning substance use during Chemsex were investigated. The chi-square statistic was used for STI diagnosis and use of pre-exposure prophylaxis.
The dataset underwent systematic cleaning, which included addressing missing values and identifying outliers. Demographic characteristics (such as age, gender, etc.) and substance use variables (e.g., alcohol, stimulants, etc.) were selected for analysis. Differences between individuals reporting Chemsex and those who did not were examined using the χ2 test for categorical data, with significance set at p < 0.05.
Additionally, participants engaging in Chemsex were stratified based on self-reported injection drug use in the previous 12 months. Differences between these subgroups were analyzed using the same statistical tests employed for Chemsex use. Logistic regression was then utilized to explore factors associated with Chemsex use, with independent variables including demographic characteristics, substance use patterns, and injection drug use status.
3 Results
3.1 Descriptive results
The final sample consisted of 563 men who have sex with men and reported substance use, residing in Spain, with ages ranging from 18 to 55 years (mean age = 36, SD = 9.20). Among the participants, 66.1% identified as gay (n = 372). Approximately half of the participants (50%, n = 264) reported completing university studies. The majority (81.3%) were employed steadily on a full-time basis. About half of the participants (49%, n = 276) reported being single. Approximately half of the sample (47.3%) reported having a socioeconomic level above 2,000 euros per month (see Table 1).
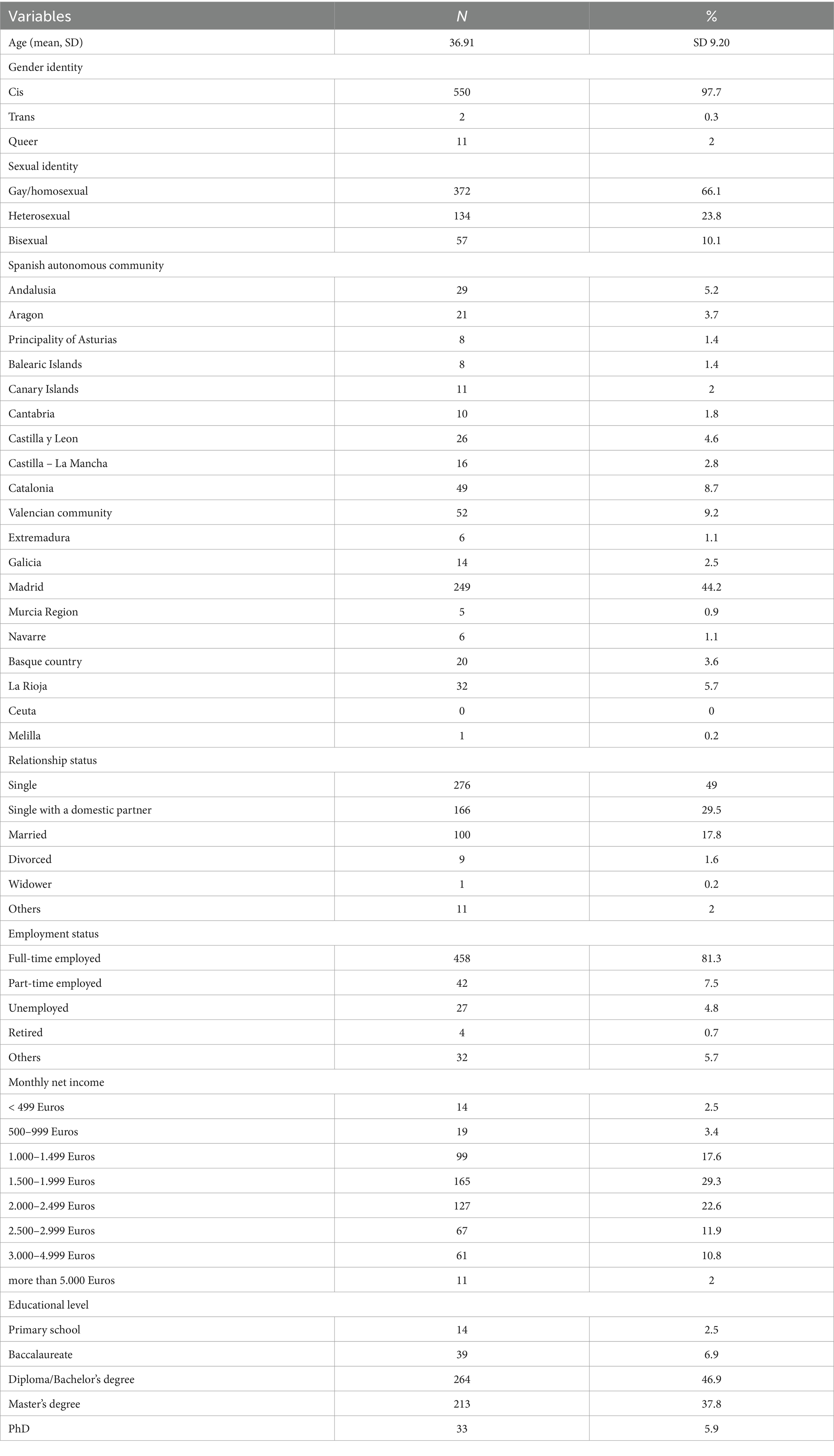
Table 1. Sociodemographic characteristics (n = 563).
3.2 Sexual risk behaviors, sexually transmitted infections, and PREP among chemsex MSM
When participants were queried about whether they had received a diagnosis of any sexually transmitted infection (STI) within the past 6 months, 101 participants (17.94%) responded affirmatively. Twenty-one percent of the sample was on PrEP treatment. Regarding participants on PrEP treatment, 35 (29.1%) were diagnosed with gonorrhea, 28 (23.3%) with chlamydia, 10 (8.33%) with genital herpes, and 21 (17.5%) with syphilis. As for participants who were not on PrEP treatment, 33 (7.44%) were diagnosed with gonorrhea, 25 (5.64%) with chlamydia, 15 (3.38%) with genital herpes, and 24 (5.41%) with syphilis. A statistically significant association was found between PrEP use and sexually transmitted infections: gonorrhea (p < 0.001); chlamydia (p < 0.001); genital herpes (p = 0.020) and syphilis (p < 0.001); no significant differences were found with HIV, Monkeypox, hepatitis, and other syphilis. The following table shows the relationship between taking PREP and having STIs (see Table 2).
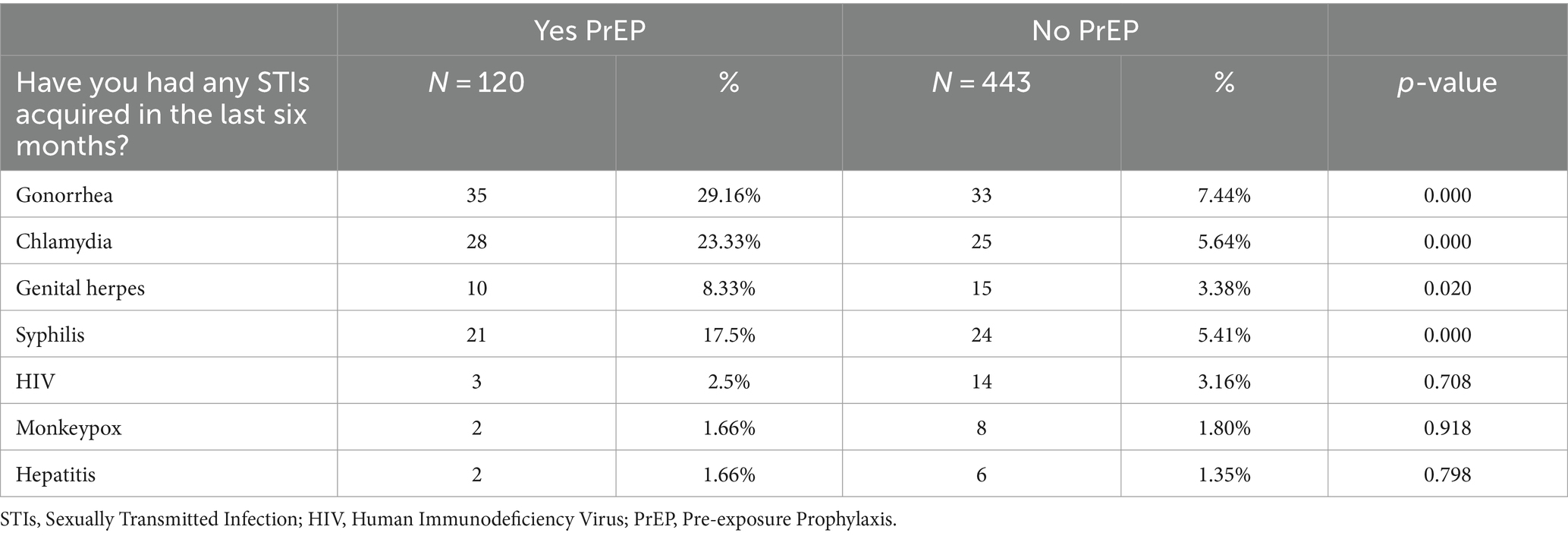
Table 2. Relationship between take of PrEP and STIs (n = 563).
3.3 Sexual risk behaviors and risky substance use among chemsex MSM
63.7% of the participants in the sample used methamphetamine as their primary chemsex drug, followed by 61.6% who used mephedrone, 61.2% amphetamines, 60.3% medication for erectile dysfunction and 60.2% GHB/GBL. Table 3 shows the distribution of the participants according to the primary drug of use. Statistically significant differences were found for substances consumed and STIs amyl nitrile (p = 0.000); medication for erectile dysfunction (p = 0.000); GHB/GBL (p = 0.000); Alcohol (p = 0. 000); Tobacco (p = 0.001); Ecstasy (p = 0.000); Amphetamines (p = 0.000); Ketamine (p = 0.000); Methamphetamine (p = 0.000); Mephedrone (p = 0.000); Cocaine (p = 0.000); opioid analgesics (p = 0.014) respectively. For example, 39.8% of GHB/GBL users had STIs vs. 18.93% of non-users, so we found statistically significant differences between users and non-users vs. GHB (p = 0.000). No statistically significant differences were found between THC and Heroin consumption with having STIs (p = 0.138; p = 0.512) respectively.
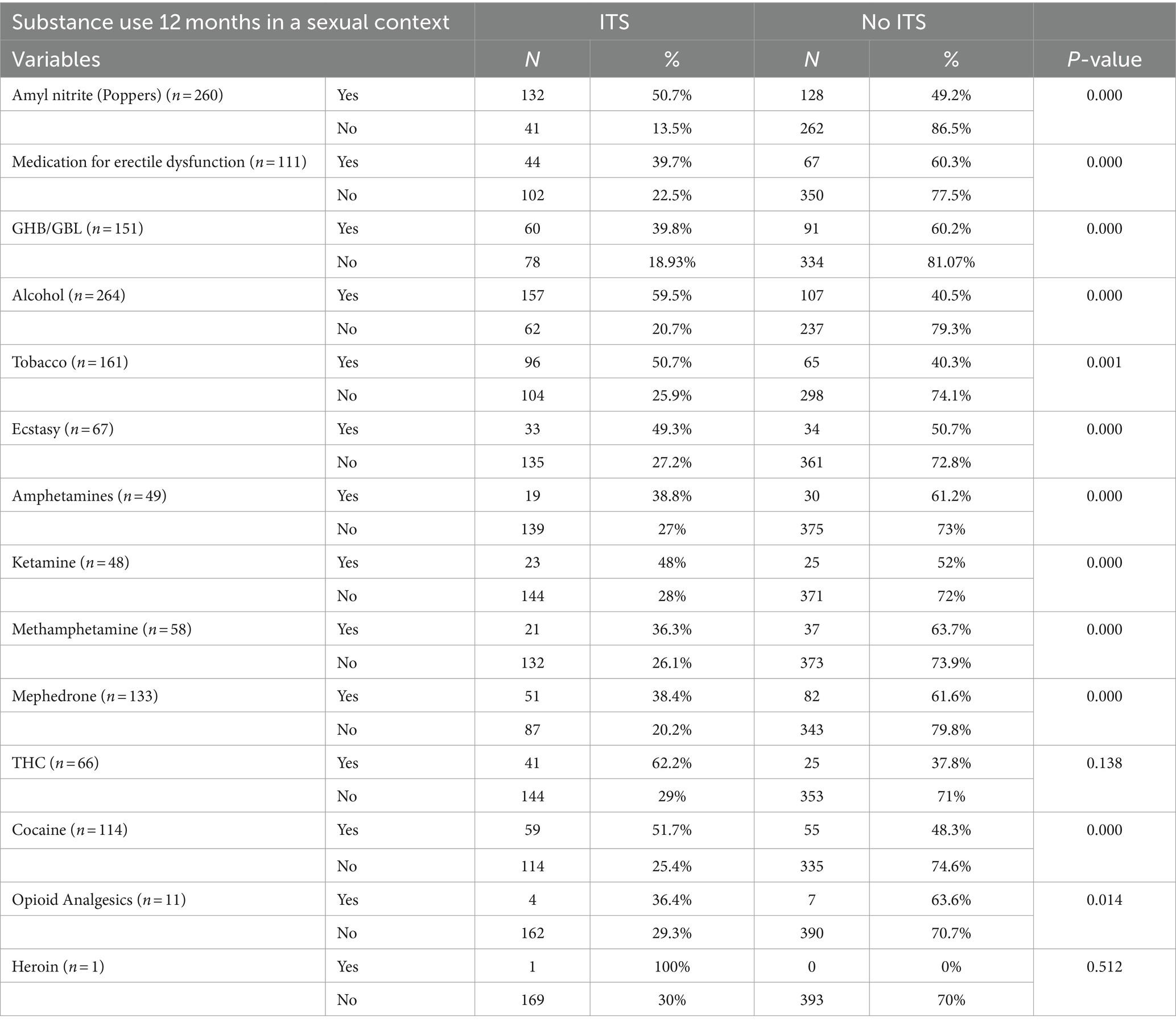
Table 3. Prevalence of substance use among sexually transmitted infections (STIs) men (n = 563).
3.4 Sexual risk behaviors and injecting substance use (slamsex) among chemsex MSM
14.7% (n = 83) of the participants practiced slamsex in the last 12 months. The most commonly used injecting substances were mephedrone (n = 53), methamphetamine (n = 21), ketamine (n = 8), and to a lesser extent heroin (n = 1). Table 4 illustrates a statistically significant association between injecting substance use (slamsex) and the diagnosis of sexually transmitted infections (STIs).
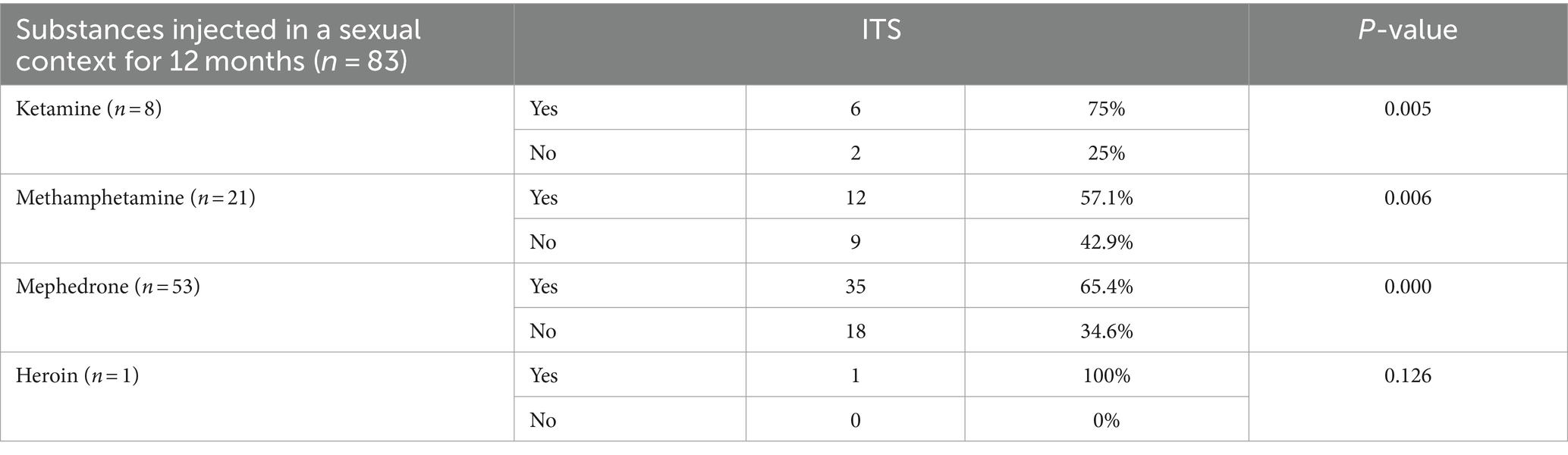
Table 4. Prevalence of injecting substance use among men with sexually transmitted infections (STIs).
4 Discussion
Our research aimed to explore the profile of men who have sex with men in a sexual context since it could explain the relationship between chemsex, sexual behavior, and the increase in the diagnosis of STIs. The profile of users who practice chemsex is that of a man between 18 and 55 years old, resident in Spain, with university studies and a permanent job. Previous research has indicated that individuals aged between 36 and 45 years old are more inclined to engage in chemsex compared to other age groups (44). These findings align with our study, where the average age of substance use and participation in chemsex was 36 years old.
Our research concludes that being a young man, living in large cities, and being exposed to environmental stressors and substance use in the last 12 months may be additional risk factors associated with a high prevalence of chemsex. These factors are in line with other studies that have scientifically established that the homosexual population is potentially up to twice as prone to experiencing psychotic symptoms compared to the heterosexual population (45, 46). Chemsex has been identified as a coping mechanism for the stressors that men who have sex with men (MSM) encounter regularly (45, 47).
The research presents an alarming picture of the prevalence of sexually transmitted infections (STIs) among men who have sex with men (MSM) involved in chemsex and slamsex. According to the study data, 17.94% (n = 101) of the participants reported being diagnosed with any STI in the last 6 months, data that is consistent with other studies (15, 30). An important finding of our research and worth noting is that 21% of the sample was on treatment with pre-exposure prophylaxis (PrEP), observing a strong association between being on treatment with PrEP and the diagnosis of gonorrhea, chlamydia, genital herpes, and syphilis, which also confirms the results of similar studies (35, 48).
This is striking, as one might expect those on PrEP to be less exposed to STIs due to their greater awareness of sexual health and regular intake of preventive medication. However, the results show that, among participants on PrEP, there were higher rates of diagnosed STIs: 29.16% for gonorrhea, 23.33% for chlamydia, 8.33% for genital herpes, and 17.5% for syphilis. In comparison, those who were not on PrEP also had a significant prevalence of STIs, but to a lesser extent: 7.44% for gonorrhea, 5.64% for chlamydia, 3.38% for genital herpes, and 5.41% for syphilis. Thus, there is an increasing trend among MSM in treatment with PrEP who practice chemsex with higher rates of STI diagnoses (18, 29, 32, 35–37, 48–50). For all of the above, harm reduction strategies and community-based chemsex approaches that combine support services with health promotion and education activities should be pursued (51–53). Given the entry of PrEP into the service portfolio of the National Health System (SNS), the Secretariat of the National AIDS Plan (SPNS) launched the SIPrEP in 2020, an information and monitoring system for the implementation. Running and implementation in the different Autonomous Communities (CCAA) of the PrEP programs, with the aim of collecting information on the number of participants, their characteristics, their clinical evolution and the effectiveness of PrEP. Thus, up to and including 2023, the estimated number of users who were taking PrEP is 18,075 people (54).
On the other hand, substance use appears to be associated with an increased risk of STIs in general. MSM who engage in chemsex have been reported to be at increased risk of transmitting STIs and at increased risk of engaging in risky sexual behaviors, and acquiring HIV (55). People who use amyl nitrite, GHB/GBL, alcohol, ecstasy, amphetamines, ketamine, methamphetamine, mephedrone, and cocaine have a higher proportion of STIs compared to those who do not use these substances. When considering substance use in the context of chemsex and slamsex, the results show a significant association between the use of certain substances and the prevalence of STIs. For example, 39.8% of GHB/GBL users had STIs compared to 18.93% of non-users, suggesting that the use of these substances is associated with an increased risk of STIs. Data that are also consistent with other studies in which drugs used in the chemsex context were related to STIs and sexual risk behaviors (30, 56–61). Moreover, the findings of a previous study demonstrated a 2.83-fold increase in the likelihood of acquiring a sexually transmitted infection (STI) among chemsex users (30). This result aligns with the outcomes of the current study.
These data reinforce the need for continued sexual health education and safer practices, even among those on PrEP. The high prevalence of STIs among participants on PrEP suggests that access to preventive medication is not sufficient to eliminate STI risk and that other factors, such as sexual risk behavior, may be at play.
In regards to slamsex, it is notable that a significant percentage of participants in our study reported consuming injected substances (14.7%) in the past year compared to those who did not inject drugs. Among individuals who engaged in slamsex, a higher frequency of STI diagnoses was observed, consistent with findings from other studies. For instance, research has shown that 15.7% of individuals who practiced slamsex in the previous year reported a higher frequency of STI diagnoses and engaged in high-risk sexual behaviors (29). Other studies focused on drug use and STI risk have shown an increased risk of STI acquisition by people who use drugs (39), which may be related to the search for new sensations and experiences as well as disinhibition. Risk behaviors associated with chemsex, such as having multiple sexual partners, having unprotected sex, engaging in fisting and slamsex, as well as sharing injection equipment, may be risk factors for acquiring STIs in the past 6 months in the context of chemsex (29, 36, 45).
Along the same lines, the most commonly consumed injecting drugs during slamsex associated with STI diagnosis in our study were ketamine (75%), followed by mephedrone (65.4%), and methamphetamine (57.1%). The potent stimulant effect of mephedrone has been associated with a heightened risk of engaging in high-risk sexual behaviors, which in turn increases the risk of HIV infection and other sexually transmitted infections (STIs) (62). Additionally, mephedrone use has been linked to severe psychiatric symptoms, intoxications, and dependence on injecting drugs (29). This includes a range of adverse effects such as binge drinking, anxiety, binge eating, withdrawal symptoms, and psychotic symptomatology resulting from injecting mephedrone use (6, 29, 63).
The significant prevalence of substance use within the context of chemsex, coupled with its correlation with risky sexual behaviors, underscores the importance of targeting men who have sex with men (MSM) as a critical population for prevention strategies. These findings support the need for comprehensive interventions that address both substance use and sexual health to reduce STI risk in vulnerable populations, especially in populations where chemsex is prevalent, as appears to be the case in Spain and who are on PrEP treatment. Addressing chemsex can yield broader positive impacts on individuals’ mental, sexual, social, financial, and overall health. A retrospective case review conducted in a London service found that half of MSM who reported engaging in chemsex perceived subsequent adverse physical and mental health consequences, highlighting the need for comprehensive support and intervention strategies (32, 64).
Furthermore, there exists an association between engaging in chemsex and the heightened risk of experiencing emotional instability, including symptoms of anxiety and depression. These findings align with numerous previous studies conducted among MSM, which have consistently reported a link between drug use for sexual purposes and an increased likelihood of experiencing depressive outcomes (39). Indeed, some studies have identified anxiety as a predictor in the relationship between psychosis and chemsex (29). Conversely, other research has found no significant differences in anxiety levels, although it did reveal that chemsex users exhibited higher scores on the GAD-7 scale (34). This may suggest that the use of substances to extend time in a sexual context may provoke depressive symptoms with ideas of guilt and ruin of the people who practice it, or also, it may be depressive symptoms such as social isolation and loneliness that lead to substance use in a sexual context to disinhibit themselves and be a way to socialize with other people. Our findings also suggest that risk factors such as substance use, poly consumption, engaging in slamsex, and injecting methamphetamine use are associated with an elevated likelihood of experiencing a psychotic break. This association with the risk of psychosis aligns with the results of previously published studies (29, 45).
Associations have been noted between chemsex and an increased risk of suicide. Additionally, there is evidence of an association between chemsex, impulsivity, and distorted body perception. A recent meta-analysis conducted in Sweden (65) reported a suicide attempt rate of 10% in gay men compared to 2.2% in heterosexual men. This suggests that MSM and individuals involved in chemsex may have a higher lifetime risk of suicide attempts compared to the general population (34).
5 Strengths and limitations of the study
One of the strengths of our study is that the survey was anonymous, so participants may be especially willing to disclose their chemsex experiences. Other strengths of our study are validated measurement methods, multivariate analysis, and explicit questions about chemsex.
Our findings have certain limitations. Using a cross-sectional study design means that the relationships between variables cannot be interpreted as cause-and-effect. Additionally, the use of non-probability purposive sampling to obtain the sample restricts the generalizability of our results to the broader MSM population. However, the sizable sample size suggests that the results hold validity. Since this is a self-administered survey, the results reflect the respondents’ viewpoints, which may not fully represent the clinical experience. Furthermore, variations in participants’ roles may have influenced their knowledge, experiences, and perceptions of the chemsex phenomenon.
6 Conclusion
The study highlights the high prevalence of “chemsex” among men who have sex with men (MSM), increasing the risk of STIs. It underlines the urgent need for preventive strategies and care programs tailored to this population. Chemsex poses unique public health challenges, requiring a comprehensive approach that addresses substance use and sexual health. Individuals involved exhibit high-risk behaviors, along with symptoms of psychopathology and substance dependence. Therefore, identification, education and prevention programs are crucial to mitigate negative consequences. Improving awareness of PrEP as HIV prevention can be effective, as can screening programs for health problems related to drug use, and interventions to increase awareness of risks and provide access to health resources.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Committee of the University of La Rioja with verification code (CSV) (D2R1m2Iu3vLVPdIzGZVVnK0h6N558tCyN). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PP-H: Writing – review & editing, Writing – original draft, Methodology, Conceptualization. EB-G: Writing – review & editing, Writing – original draft, Supervision, Conceptualization. AM-S: Writing – original draft, Methodology, Investigation, Data curation, Conceptualization. EC-S: Writing – original draft, Supervision, Software, Methodology, Formal analysis, Conceptualization. VG-C: Writing – original draft, Visualization, Validation, Resources, Project administration, Funding acquisition, Formal analysis. JC-R: Writing – original draft, Methodology, Formal analysis. MC: Writing – original draft, Methodology, Investigation, Conceptualization. PK: Writing – original draft. JM-T: Writing – original draft, Resources, Project administration, Methodology, Investigation. MS-B: Writing – original draft, Project administration, Formal analysis. RV: Writing – original draft, Visualization, Validation, Software, Resources, Project administration, Investigation, Funding acquisition, Formal analysis. RJ-V: Writing – review & editing, Writing – original draft, Supervision, Methodology, Investigation, Funding acquisition, Formal analysis, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank all the participants who have contributed to part of the contributed to part of it.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fernández-Dávila, P. Sesión de sexo, morbo y vicio: una aproximación holística para entender la aparición del fenómeno ChemSex entre hombres gais, bisexuales y otros hombres que tienen sexo con hombres en España. Rev Multidiscip Sida. (2016) 4:41–65.
2. McCall, H, Adams, N, Mason, D, and Willis, J. What is chemsex and why does it matter? BMJ. (2015) 351:5790. doi: 10.1136/bmj.h5790
3. Dolengevich-Segal, H, Rodríguez-salgado, B, Bellesteros-López, J, and Molina-Prado, R. Chemsex. Un fenómeno emergente. Adicciones. (2017) 29:207–9. doi: 10.20882/adicciones.894
4. Ocón, RS, and Del Amo, J. Abordaje del fenómeno del Chemsex. Una propuesta desde el Plan Nacional sobre el SIDA. Rev Esp Salud Pública. (2020) 94:4.
5. Ramos, JC, Dolengevich-Segal, H, Ocón, RS, and Egozcue, MJ. Documento técnico: abordaje de la salud mental del usuario con prácticas de chemsex. Madrid: MSD. (2020). Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/chemSex/docs/Abordaje_salud_mental_chemsex.pdf.
6. del Pozo-Herce, P, Martínez-Sabater, A, Chover-Sierra, E, Gea-Caballero, V, Satústegui-Dordá, PJ, Saus-Ortega, C, et al. Application of the Delphi method for content validity analysis of a questionnaire to determine the risk factors of the Chemsex. Healthcare. (2023) 11:2905. doi: 10.3390/healthcare11212905
7. Soriano, R. Guía de Prevención de Adicciones en Canarias. Chemsex. Consejería de Sanidad del Gobierno de Canarias. Servicio Canario de Salud (2022). Available at: https://www3.gobiernodecanarias.org/sanidad/scs/content/134b92f6-91ed-11ed-845a-9b76754ff4dd/ChemSex_Guia_web.pdf.
8. Bourne, A, Reid, D, Hickson, F, Torres-Rueda, S, and Weatherburn, P. The Chemsex study: Drug use in sexual settings among gay and bisexual men in Lambeth, Southwark and Lewisham. London School of Hygiene and Tropical Medicine, London. (2014). Available at: https://researchonline.lshtm.ac.uk/id/eprint/2197245/.
9. Ballesteros-López, J, Molina-Prado, R, Rodríguez-Salgado, B, Martin-Herrero, J, and Dolengevich-Segal, H. Mephedrone and chemsex. A descriptive analisis of a sample of patients in Madrid. Rev Española de Drogodepend. (2014) 41:47–61.
10. Ward, C, McQuillan, O, and Evans, R. O14 Chemsex, consent and the rise in sexual assault. Sex Transm Infect. (2017) 93:A5.2–A5. doi: 10.1136/sextrans-2017-053232.14
11. Pufall E.L.Kall, M, Shahmanesh, M, Nardone, A, Gilson, R, Delpech, V, et al. Sexualized drug use ('chemsex') and high-risk sexual behaviours in HIV-positive men who have sex with men. HIV Med. (2018) 19:261–70. doi: 10.1111/hiv.12574
12. Queiroz, A, Sousa, AF, De-Brignol, S, Araujo, TM, and Reis, RK. Vulnerability to HIV among older men who have sex with men users of dating apps in Brazil. Braz J Infect Dis. (2019) 23:298–306. doi: 10.1016/j.bjid.2019.07.005
13. Malandain, L, Mosser, S, Mouchabac, S, Blanc, JV, Alexandre, C, and Thibaut, F. Chemical sex (chemsex) in a population of French university students. Dialogues Clin Neurosci. (2022) 23:39–43. doi: 10.1080/19585969.2022.2042163
14. Gavín, P, Arbelo, N, Monràs, M, Nuño, L, Bruguera, P, De la Mora, L, et al. Uso de metanfetamina en el contexto chemsex y sus consecuencias en la salud mental: un estudio descriptivo. Rev Esp Salud Pública. (2021) 95:31.
15. Salusso, D, Nuñez, S, Cabrini, M, Rolón, MJ, and Cahn, P. Chemsex y uso de sustancias durante las relaciones sexuales: resultados de una encuesta realizada en Argentina. Actual SIDA infectol. (2020) 28:40–50. doi: 10.52226/revista.v28i103.56
16. Ministerio de Sanidad. Ley 40/2015 Boletín Oficial del Estado. Ministerio de Sanidad (2020). Sección III. (Cited 2024 January 12), pp. 52211–52217. Available at: https://www.boe.es/boe/dias/2020/07/16/pdfs/BOE-A-2020-7990.pdf.
17. EMIS. Resultados en España. Madrid: Ministerio de Sanidad, Política Social e Igualdad. Encuesta online europea para hombres que tienen relaciones sexuales con hombres. (2020). Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/INFORMES/Encuesta_Europea_On-line_para_hombres_que_tienen_sexo_con_otros_hombres._Acces.pdf.
18. Amundsen, E, Haugstvedt, A, Skogen, V, and Berg, RC. Health characteristics associated with chemsex among men who have sex with men: results from a cross-sectional clinic survey in Norway. PLoS One. (2022) 17:e0275618. doi: 10.1371/journal.pone.0275618
19. Evers, YJ, Van-Liere, GA, Hoebe, CJ, and Dukers-Muijrers, NH. Chemsex among men who have sex with men living outside major cities and associations with sexually transmitted infections: a cross-sectional study in the Netherlands. PLoS One. (2019) 14:e0216732. doi: 10.1371/journal.pone.0216732
20. Stuart, D, and Weyman, J. ChemSex and care-planning: one year in practice. HIV Nurs. (2015) 15:24–8.
21. Ruiz-Robledillo, N, Ferrer-Cascales, R, Portilla-Tamarit, I, Alcocer-Bruno, C, Clement-Carbonell, V, and Portilla, J. Chemsex practices and health-related quality of life in Spanish men with HIV who Have sex with men. J Clin Med. (2021) 10:1662. doi: 10.3390/jcm10081662
22. Maxwell, S, Shahmanesh, M, and Gafos, M. Chemsex behaviours among men who have sex with men: a systematic review of the literature. Int J Drug Policy. (2019) 63:74–89. doi: 10.1016/j.drugpo.2018.11.014
23. Pakianathan, M, Whittaker, W, Lee, MJ, Avery, J, Green, S, Nathan, B, et al. Chemsex and new HIV diagnosis in gay, bisexual and other men who have sex with men attending sexual health clinics. HIV Med. (2018) 19:485–90. doi: 10.1111/hiv.12629
24. Frankis, J, Flowers, P, McDaid, L, and Bourne, A. Low levels of chemsex among men who have sex with men, but high levels of risk among men who engage in chemsex: analysis of a cross-sectional online survey across four countries. Sex Health. (2018) 15:144–50. doi: 10.1071/SH17159
25. Whitlock, G, Protopapas, K, Bernardino, JI, Imaz, A, Curran, A, Stingone, C, et al. Chems4EU: chemsex use and its impacts across four European countries in HIV-positive men who have sex with men attending HIV services. HIV Med. (2021) 22:944–57. doi: 10.1111/hiv.13160
26. Evers, YJ, Dukers-Muijrers, NH, Kampman, CJ, Van-Liere, GA, Hautvast, JL, Koedijk, FD, et al. Prevalence of drug use during sex among swingers and perceived benefits and risks - a cross-sectional internet survey in the Netherlands. Sex Transm Infect. (2020) 96:40–6. doi: 10.1136/sextrans-2019-054113
27. Coll, J, and Fumaz, C. Recreational drugs and sex in men who have sex with men: chemsex, risks, health problems related, emotional factors and intervention strategies. Rev Enf Emerg. (2016) 15:77–84.
28. Íncera-Fernández, D, Román, FJ, Moreno-Guillén, S, and Gámez-Guadix, M. Understanding sexualized drug use: substances, reasons, consequences, and self-perceptions among men who Have sex with other men in Spain. Int J Environ Res Public Health. (2023) 20:2751. doi: 10.3390/ijerph20032751
29. Dolengevich-Segal, H, Gonzalez-Baeza, A, Valencia, J, Valencia-Ortega, E, Cabello, A, Tellez-Molina, MJ, et al. Drug-related and psychopathological symptoms in HIV-positive men who have sex with men who inject drugs during sex (slamsex): data from the U-SEX GESIDA 9416 study. PLoS One. (2019) 14:12. doi: 10.1371/journal.pone.0220272
30. Kohli, M, Hickson, F, Free, C, Reid, D, and Weatherburn, P. Cross-sectional analysis of chemsex drug use and gonorrhoea diagnosis among men who have sex with men in the UK. Sex Health. (2019) 16:464–72. doi: 10.1071/SH18159
31. Lawn, W, Aldridge, A, Xia, R, and Winstock, AR. Substance-linked sex in heterosexual, homosexual, and bisexual men and women: an online, cross-sectional «global drug survey» report. J Sex Med Mai. (2019) 16:721–32. doi: 10.1016/j.jsxm.2019.02.018
32. Hegazi, A, Lee, MJ, Whittaker, W, Green, S, Simms, R, Cutts, R, et al. Chemsex and the city: sexualised substance use in gay bisexual and other men who have sex with men attending sexual health clinics. Int J STD AIDS. (2017) 28:362–6. doi: 10.1177/0956462416651229
33. Ryan, P, Dolengevich-Segal, H, Ramos-Ruperto, L, Cabello, A, Sanchez-Conde, M, Vergas, J, et al. Patterns of sexualized drug use among gay, bisexual, and other men who Have sex with men living with HIV: insights from a comprehensive study—the U-SEX-2 GESIDA 9416 study. J Clin Med. (2023) 12:12. doi: 10.3390/jcm12237293
34. Bohn, A, Sander, D, Köhler, T, Hees, N, Oswald, F, Scherbaum, N, et al. Chemsex and mental health of men who Have SexWith men in Germany. Front Psych. (2020) 11:11. doi: 10.3389/fpsyt.2020.542301
35. Tomkins, A, George, R, and Kliner, M. Sexualised drug taking among men who have sex with men: a systematic review. Perspects Public Health. (2019) 139:23–33. doi: 10.1177/1757913918778872
36. Hibbert, MP, Brett, CE, Porcellato, LA, and Hope, VD. Psychosocial and sexual characteristics associated with sexualised drug use and chemsex among men who have sex with men (MSM) in the UK. Sex Transm Infect. (2019) 95:342–50. doi: 10.1136/sextrans-2018-053933
37. Gonzalez-Baeza, A, Dolengevich-Segal, H, Perez-Valero, I, Cabello, A, Tellez, MJ, Sanz, J, et al. Sexualized drug use (chemsex) is associated with high-risk sexual behaviors and sexually transmitted infections in HIV-positive men who Have sex with men: data from the U-SEX GESIDA 9416 study. AIDS Patient Care STDs. (2018) 32:112–8. doi: 10.1089/apc.2017.0263
38. Drückler, S, Van Rooijen, MS, and De Vries, HJ. Chemsex among men who Have sex with men: a sexualized drug use survey among clients of the sexually transmitted infection outpatient clinic and users of a gay dating app in Amsterdam, the Netherlands. Sex Transm Dis. (2018) 45:325–31. doi: 10.1097/OLQ.0000000000000753
39. Íncera-Fernández, D, Román, FJ, and Gámez-Guadix, M. Risky Sexual Practices, sexually transmitted infections, motivations, and mental health among heterosexual women and men who practice sexualized drug use in Spain. Int J Environ Res Public Health. (2022) 19:19. doi: 10.3390/ijerph19116387
40. Lea, T, Mao, L, Hopwood, M, Prestage, G, Zablotska, I, de Wit, J, et al. Methamphetamine use among gay and bisexual men in Australia: trends in recent and regular use from the gay Community periodic surveys. Int J Drug Policy. (2016) 29:66–72. doi: 10.1016/j.drugpo.2016.01.003
41. Dolengevich-Segal, H, Rodríguez-Salgado, B, Gómez-Arnau, J, and Sánchez-Mateos, D. Severe psychosis, drug dependence, and hepatitis C related to slamming Mephedrone. Case Rep Psychiatry. (2016) 2016:1–5. doi: 10.1155/2016/8379562
42. EMCDDA. European drug report 2018: trends and developments. European monitoring centre for drugs and drug addiction. (2018). Available at: https://www.emcdda.europa.eu/publications/edr/trends-developments/2018_en (Accessed June 20, 2018).
43. Grupo de Trabajo de Chemsex del Plan Nacional Sobre el Sida. Informe sobre chemsex en España. Dirección General de Salud Pública Calidad e Innovación (2019). Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/docs/informeCHEMSEX.pdf.
44. Kennedy, R, Murira, J, Foster, K, Heinsbroek, E, Keane, F, Pal, N, et al. Sexualized drug use and specialist service experience among MSM attending urban and rural sexual health clinics in England and Scotland. Int J STD AIDS. (2021) 32:1338–46. doi: 10.1177/09564624211041456
45. Moreno-Gámez, L, Hernández-Huerta, D, and Lahera, G. Chemsex and psychosis: a systematic review. Behav Sci. (2022) 12:15. doi: 10.3390/bs12120516
46. Gevonden, MJ, Selten, JP, Myin-Germeys, I, De Graaf, R, Have, MT, Van Dorsselaer, S, et al. Sexual minority status and psychotic symptoms: findings from the Netherlands mental health survey and incidence studies (NEMESIS). Psychol Med. (2014) 44:421–33. doi: 10.1017/S0033291713000718
47. Lafortune, D, Blais, M, Miller, G, Dion, L, Lalonde, F, and Dargis, L. Psychological and interpersonal factors associated with sexualized drug use among men who Have sex with men: a mixed-methods systematic review. Arch Sex Behav. (2021) 50:427–60. doi: 10.1007/s10508-020-01741-8
48. Guerra, FM, Salway, TJ, Beckett, R, Friedman, L, and Buchan, SA. Review of sexualized drug use associated with sexually transmitted and blood-borne infections in gay, bisexual and other men who have sex with men. Drug Alcohol Depend. (2020) 216:108237. doi: 10.1016/j.drugalcdep.2020.108237
49. Chen, X, Li, XL, Zheng, J, Zhao, JS, He, JM, Zhang, GQ, et al. Club drugs and HIV/STD infection: an exploratory analysis among men who Have sex with men in Changsha, China. PLoS One. (2015) 10:10. doi: 10.1371/journal.pone.0126320
50. Achterbergh, RC, De Vries, HJ, Boyd, A, Davidovich, U, Druckler, S, Hoornenborg, E, et al. Identification and characterization of latent classes based on drug use among men who have sex with men at risk of sexually transmitted infections in Amsterdam, the Netherlands. Addiction. (2020) 115:121–33. doi: 10.1111/add.14774
51. Stardust, Z, Kolstee, J, Joksic, S, Gray, J, and Hannan, S. A community-led, harm-reduction approach to chemsex: case study from Australia's largest gay city. Sex Health. (2018) 15:179–81. doi: 10.1071/SH17145
52. Burgess, K, Parkhill, G, Wiggins, J, Ruth, S, and Stoovè, M. Re-wired: treatment and peer support for men who have sex with men who use methamphetamine. Sex Health. (2018) 15:157–9. doi: 10.1071/SH17148
53. Schecke, H, Lea, T, Bohn, A, Kohler, T, Sander, D, Scherbaum, N, et al. Crystal methamphetamine use in sexual settings among German men who Have sex with men. Front Psych. (2019) 10:10. doi: 10.3389/fpsyt.2019.00886
54. División de Control de VIH, ITS, Hepatitis virales y Tuberculosis. Sistema de información de programas de Profilaxis Pre-exposición al VIH en España (SIPrEP). Informe de resultados noviembre 2019-mayo 2023. Ministerio de Sanidad, Julio (2023). Available at: https://www.sanidad.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/PrEP/Informe_SIPrEP_nov_19_mayo_23.pdf
55. Darke, S, Kaye, S, McKetin, R, and Duflou, J. Major physical and psychological harms of methamphetamine use. Drug Alcohol Rev. (2008) 27:253–62. doi: 10.1080/09595230801923702
56. Bonell, CP, Hickson, FC, Weatherburn, P, and Reid, DS. Methamphetamine use among gay men across the UK. Int J Drug Policy. (2010) 21:244–6. doi: 10.1016/j.drugpo.2009.07.002
57. Vu, NT, Maher, L, and Zablotska, I. Amphetamine-type stimulants and HIV infection among men who have sex with men: implications on HIV research and prevention from a systematic review and metaanalysis. J Int AIDS Soc. (2015) 18:18. doi: 10.7448/IAS.18.1.19273
58. Prestage, G, Grierson, J, Bradley, J, Hurley, M, and Hudson, J. The role of drugs during group sex among gay men in Australia. Sex Health. (2009) 6:310–7. doi: 10.1071/SH09014
59. Melendez-Torres, GJ, Hickson, F, Reid, D, Weatherburn, P, and Bonell, C. Nested event-level case-control study of drug use and sexual outcomes in multipartner encounters reported by men who have sex with men. AIDS Behav. (2016) 20:646–54. doi: 10.1007/s10461-015-1127-6
60. Boone, MR, Cook, SH, and Wilson, P. Substance use and sexual risk behavior in HIV-positive men who have sex with men: an episode level analysis. AIDS Behav. (2013) 17:1883–7. doi: 10.1007/s10461-012-0167-4
61. Bourne, A, Reid, D, Hickson, F, Torres-Rueda, S, and Weatherburn, P. Illicit drug use in sexual settings ('chemsex') and HIV/STI transmission risk behaviour among gay men in South London: findings from a qualitative study. Sex Transm Infect. (2015) 91:564–8. doi: 10.1136/sextrans-2015-052052
62. Abdulrahim, D, and Bowden-Jones, O. Guidance on the Management of Acute and Chronic Harms of Club drugs and novel psychoactive substances. Novel psychoactive treatment UK network (NEPTUNE). Public Health (2015).
63. Van Hout, MC, Crowley, D, O'Dea, S, and Clarke, S. Chasing the rainbow: pleasure, sex-based sociality and consumerism in navigating and exiting the Irish Chemsex scene. Cult Health Sex. (2019) 21:1074–86. doi: 10.1080/13691058.2018.1529336
64. Wiggins, H, Ogaz, D, Mebrahtu, H, Sullivan, A, Bowden-Jones, O, Field, N, et al. Demand for and availability of specialist chemsex services in the UK: a cross-sectional survey of sexual health clinics. Int J Drug Policy. (2018) 55:155–8. doi: 10.1016/j.drugpo.2017.12.016
Keywords: substance use, HIV infections, sexual behavior, STIs, pre-exposure prophylaxis, sexually transmitted infection
Citation: del Pozo-Herce P, Baca-García E, Martínez-Sabater A, Chover-Sierra E, Gea-Caballero V, Curto-Ramos J, Czapla M, Karniej P, Martínez-Tofe J, Sánchez-Barba M, de Viñaspre RR and Juárez-Vela R (2024) Descriptive study on substance uses and risk of sexually transmitted infections in the practice of Chemsex in Spain. Front. Public Health. 12:1391390. doi: 10.3389/fpubh.2024.1391390
Edited by:
Samer El Hayek, Erada Center for Treatment and Rehab, United Arab EmiratesReviewed by:
Alberto Tovar Reinoso, Autonomous University of Madrid, SpainLukasz Pietrzykowski, Nicolaus Copernicus University in Toruń, Poland
Marek Konop, Medical University of Warsaw, Poland
Copyright © 2024 del Pozo-Herce, Baca-García, Martínez-Sabater, Chover-Sierra, Gea-Caballero, Curto-Ramos, Czapla, Karniej, Martínez-Tofe, Sánchez-Barba, de Viñaspre and Juárez-Vela. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jesús Martínez-Tofe, amVzdXMubWFydGluZXp0QHVuaXJpb2phLmVz