 Patrycja Ozdoba
Patrycja Ozdoba Krzysztof Jurek
Krzysztof Jurek Beata Dobrowolska
Beata Dobrowolska- 1Department of Holistic Care and Management in Nursing, Faculty of Health Sciences, Medical University of Lublin, Lublin, Poland
- 2Institute of Sociology, Faculty of Social Sciences, John Paul II Catholic University of Lublin, Lublin, Poland
Aim: To explore the relationship of selected socio-demographic and occupational characteristics of nurses and their level of professional values, hospital ethical climate and job satisfaction.
Methods: Cross-sectional study was conducted among 388 Polish nurses from the spring of 2021 to winter of 2023, in the eastern part of Poland; and followed by Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Four research tools were used to collect data together with questionnaire for socio-demographic and occupational characteristics.
Results: Professional values such as activism correlate negatively with religious beliefs (Z = −1.789; p = 0.044), this means that nurses who are more involved in professional change activities are likely to be less associated with religious beliefs. A positive correlation was observed between the Ethical Hospital Climate Survey subscale—peer relations and nurses’ education level (H = 5.638; p = 0.048), indicating that a higher education level was associated with better relationships with colleagues at work. A negative relationship was identified between nurses’ external job satisfaction and their marital status (Z = −1.958; p = 0.040), that is, married nurses feel less satisfaction with the external aspects of their jobs than their single colleagues.
Discussion: These findings underscore that medical staff management should take into account both sociodemographic factors [e.g., age, education, place of residence, marital status, religious beliefs, as well as professional factors (working hours, qualification course, etc.)] that affect nurses’ professional values, job satisfaction and the ethical climate of the hospital. These underscore the need to adapt management strategies to the individual needs of employees, which can contribute to improving working conditions in healthcare facilities.
Data collection tool: The data collection tool consists of four sections.
Demographics: Collected background and demographic information.
Nurses’ professional values scale (NPVS-3): Assessed professional values among nurses.
Hospital ethical climate survey (HECS): Assessed hospital ethical climate among nurses.
Minnesota satisfaction questionnaire-short form (MSQ-SF): Assessed job satisfaction levels among nurses.
1 Introduction
Nurses’ professional values play a key role in shaping their attitudes, attitudes toward their work and the quality of the health care they provide (1). The professional values of nurses are the foundation of their daily work and include such aspects as empathy, responsibility, respect for patient autonomy, respect for patient dignity and the provision of professional care. It is also important to respect the principles of justice and to ensure the privacy and confidentiality of medical information. Nurses act with a high sense of responsibility and competence, constantly improving their skills, and collaborate with other members of the medical team to provide comprehensive and ethical care to patients, based on respect and understanding of their needs (2). Research is increasingly focused on identifying factors that may shape these values, taking into account both sociodemographic and work-related variables (3). Individual life experiences and long-term work in an occupation can influence occupational priorities and attitudes toward work. On the other hand, variables related to working conditions, such as workload, working hours and the type of duties performed, can also have a significant impact on the formation of nursing professional values (4). The work environment in which a nurses work can affect their sense of professional fulfillment and their willingness to pursue certain professional values (5). Understanding this relationship is important for both clinical practice and human resource management in the healthcare sector (6). In nursing practice, these values are reflected in daily decisions and actions, building an ethical climate that fosters responsible and empathetic care (6).
The ethical climate of a hospital directly affects the working environment of nurses, so ethical standards in the workplace are a foundation that affects the well-being and efficiency of nurses (7). Ethical climate, defined as a set of norms, values and practices for ethical behavior in the workplace, has a key impact on nurses’ behavior and decisions (8, 9). A positive ethical climate promotes decisions that are consistent with professional ethics, builds trust within the team, and increases job satisfaction (10). A negative ethical climate can lead to conflict, stress and professional burnout, which in turn reduces the quality of care provided (11).
Nurses’ job satisfaction is an important component of their professional well-being and has a direct impact on the quality of health care provided (12). In the face of increasing challenges in the healthcare sector, understanding the factors that influence job satisfaction becomes crucial (13). Research indicates that nurses’ job satisfaction can be analyzed in the context of a variety of variables, such as sociodemographic variables (e.g., age, gender, education) and variables related to working conditions (workload, quality of interpersonal relationships in the workplace, and opportunities for career advancement) (14, 15).
Consequently, understanding the relationship between nurses’ professional values, ethical hospital climate, job satisfaction, and sociodemographic and work environment variables is crucial to effectively managing nursing staff and creating a healthy, ethical work environment in healthcare facilities. A comprehensive approach to these relationships can help to develop strategies improving the well-being of staff and in a long-term the quality of care provided to patients.
2 Aim
To examine the relationship of selected socio-demographic and occupational characteristics of nurses and their level of professional values, hospital ethical climate and job satisfaction.
3 Materials and methods
3.1 Study design
In the period spanning from March 2021 to February 2023 within the Polish context, a descriptive, correlational, cross-sectional study was conducted. The research followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, serving as a standardized framework for reporting observational studies (16).
3.2 Study participants and settings
The study involved 388 nurses who represented different levels of education: medical secondary school, BSN, and MSN. The study group was selected using a convenience sampling method. Inclusion criteria comprised: [1] voluntary participation consent, [2] possession of a valid nursing license, [3] current employment at a hospital in eastern part of Poland, [4] a minimum of 2 years of professional experience, and [5] availability of Internet access.
3.3 Research instruments
This study utilized four research instruments for data collection.
The tool assessing nurses’ professional values, known as Nurses’ Professional Values Scale Three (NPVS-3), was designed by Weis and Schank (17) based on research on the earlier NPVS and NPVS-R scales. It consists of 28 questions, divided into three subscales: caring, activism and professionalism. These questions assess nurses’ commitment to patient care, their initiatives in improving health care conditions, and their adherence to high ethical and professional standards. Respondents rate their answers on a 5-point Likert scale, and scores can range from 28 to 140 points, where higher scores indicate stronger professional values. In the original version of the NPVS-3, the Cronbach’s alpha coefficient was 0.94 (17), and in the Polish adaptation the value reached 0.95 (18).
The tool assessing the perceptions of nursing personnel regarding various facets of the ethical climate within their workplace, known as Hospital Ethical Climate Survey (HECS). This survey tool, consisting of 26 questions rated by respondents on a 5-point Likert scale, where 1 signifies “almost never true” and 5 indicates “almost always true” (8, 9). The Polish adaptation comprises 21 items, with five items (Q1, Q2, Q4, Q8, Q9) removed due to not meeting psychometric criteria (19). HECS encompasses five subscales examining respondents’ interactions with peers, patients, managers, the hospital, and physicians. A higher total score reflects a more positive ethical climate within the surveyed organization. The original HECS version demonstrated a robust Cronbach’s alpha coefficient of 0.91 (7, 8), and for the Polish version, the coefficient stands at 0.93 (19).
The tool assessing the perceptions both intrinsic and extrinsic job satisfaction levels, known as Minnesota Satisfaction Questionnaire-Short Form (MSQ-SF). Intrinsic job satisfaction pertains to individuals’ perceptions of the inherent nature of their job duties, while extrinsic job satisfaction involves the evaluation of elements in the work situation beyond the specifics of job tasks (20). The MSQ-SF evaluates 20 job characteristics, utilizing a Likert scale ranging from 1 (I am not satisfied) to 5 (I am extremely satisfied). These characteristics encompass aspects such as achievement, independence, co-workers, recognition, and working conditions, as outlined by Weis in 1977. It’s important to note that the Cronbach’s α coefficient for the variables included in the Polish version of MSQ was reported as 0.86 (21).
The Authors Original Questionnaire (AOQ), developed specifically for this study, included questions on the sociodemographic details of the participants (sex, age, marital status, place of residence, level of education, socioeconomic conditions etc.) and questions related to their work environment, including such elements as post-graduate education, form of employment, job position, work experience, working hours, age range of patients under care, additional workplace, etc.
3.4 Data collection process
The data collection spanned from March 2021 to February 2023 in Poland. In response to the limitations posed by face-to-face interactions during the COVID-19 pandemic, the decision was made to conduct the survey remotely, utilizing an online questionnaire created through the “Google Forms” platform. In our study, we focused on nurses from eastern Poland, using several methods to ensure that the participants were exclusively from that area. Recruitment involved sending email invitations to hospitals in the eastern Poland provinces, alongside disseminating information about the study on health science and nursing blogs, discussion platforms, and social media networks associated with nurses. Prospective participants received invitations with a link to the survey questionnaire and research instruments. In the questionnaire, we included questions regarding the profession and place of work to ensure that the data was collected solely from nurses in the designated area.
A total of 586 individuals initiated the questionnaire, with 388 (66%) successfully completing and returning it. The survey invitation communicated the purpose and step-by-step process of the study, emphasized the need for informed and voluntary consent, and provided contact details for the researcher to address any queries related to the study.
3.5 Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics software, version 29. A descriptive approach was used to conduct statistical tests, which included estimating the frequency of distribution of variables, taking into account the standard deviation and mean percentage. As part of the evaluation, correlations between the NPVS-3, HECS and MSQ-SF scales, as well as sociodemographic and occupational variables, were tested using Pearson correlation, Mann–Whitney U test and Kruskal–Wallis test.
3.6 Ethical considerations
Participation in the study was entirely voluntary and anonymous. Before joining, participants were provided with detailed information about the study’s goals, processes, and characteristics, along with the freedom to withdraw from the study at any stage. It is worth noting that the Google Forms platform used to conduct the survey does not record the IP addresses of respondents, which further guarantees the anonymity of participants. All collected data is stored in an Excel file, secured with encryption, and each respondent is given a unique identification number, which ensures the confidentiality of the data. The researcher’s computer, on which this information is stored, is password protected, which is another safeguard against unauthorized access. The research commenced after obtaining approval from the Bioethics Committee at the Medical University of Lublin (reference number: KE-0254/17/2021). These measures were designed to guarantee participants full autonomy and safety in the research process.
4 Results
4.1 Study participants
A total of 388 nurses participated in the study, with an average age of about 41.60 years (SD = 11.52). The study showed that the respondents were predominantly women, accounting for as much as (n = 370, 95.4%) of the surveyed population, with a master’s degree in nursing (n = 207, 53.4%). Moreover, the majority of respondents rated their socioeconomic conditions as excellent (n = 192, 49.5%), while only (n = 16, 4.1%) considered them moderate. Detailed characteristics of the respondents are presented in Table 1.
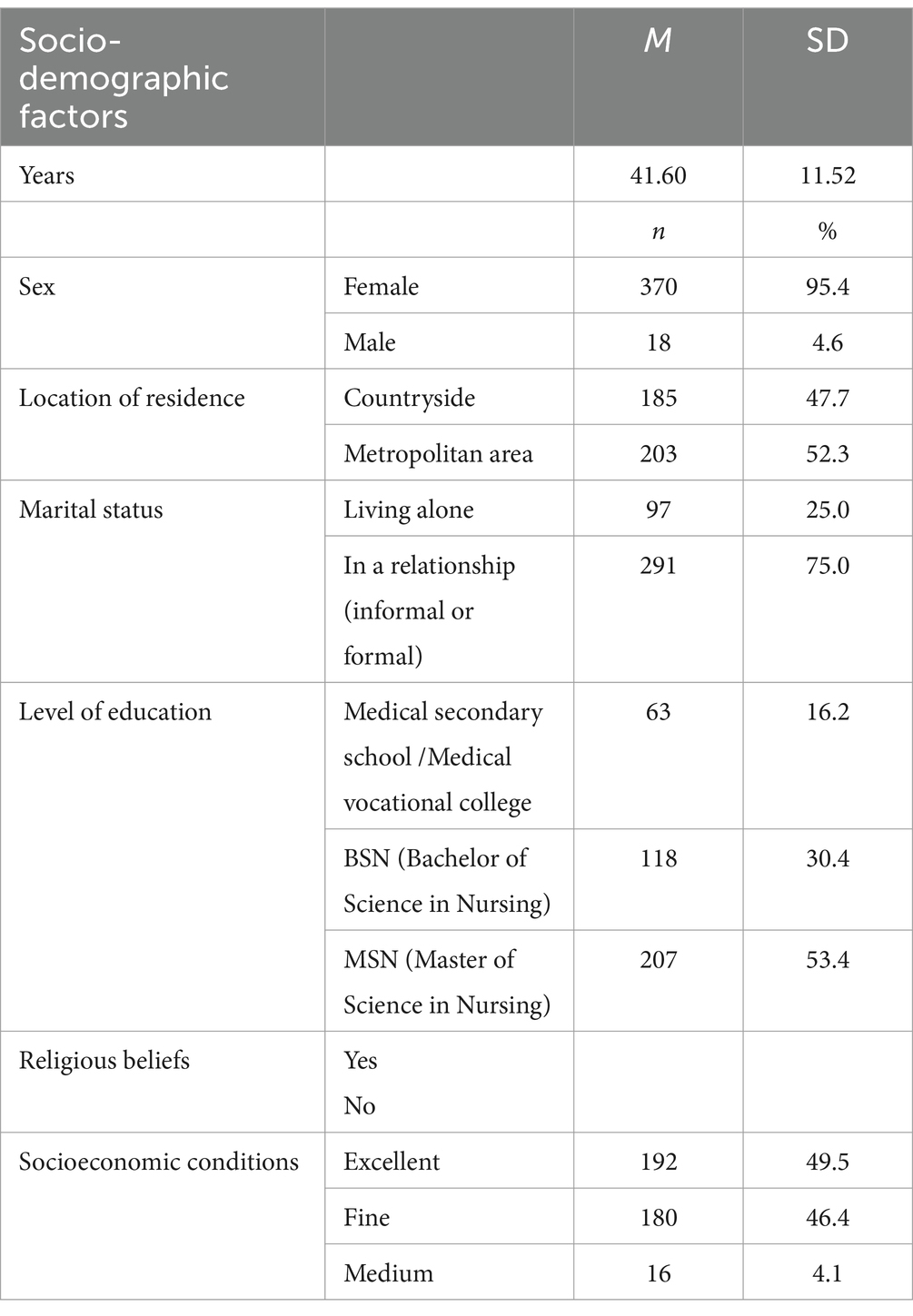
Table 1. Sociodemographic characteristics of study participants.
The most popular place for nurses to work was in Anesthesiology and Intensive Care units, accounting for (n = 126, 32.5%) of the study group, while units such as Cardiology and Dermatology were represented to a lesser extent, (n = 3, 0.8%) and (n = 6, 1.5%), respectively. The majority of nurses (67.5%) did not have a specialty or were in the process of acquiring one. Working on a 12-h system was the most common, involving (n = 273, 70.4%) of nurses, in contrast to the 8-h system, which was practiced by (n = 68, 17.5%) of respondents. Employment based on an employment contract prevailed (n = 379, 97.4%), while a small number worked on a contract of mandate (n = 7, 1.8%) or as self-employed (n = 3, 0.8%). Detailed characteristics of the respondents are presented in Table 2.
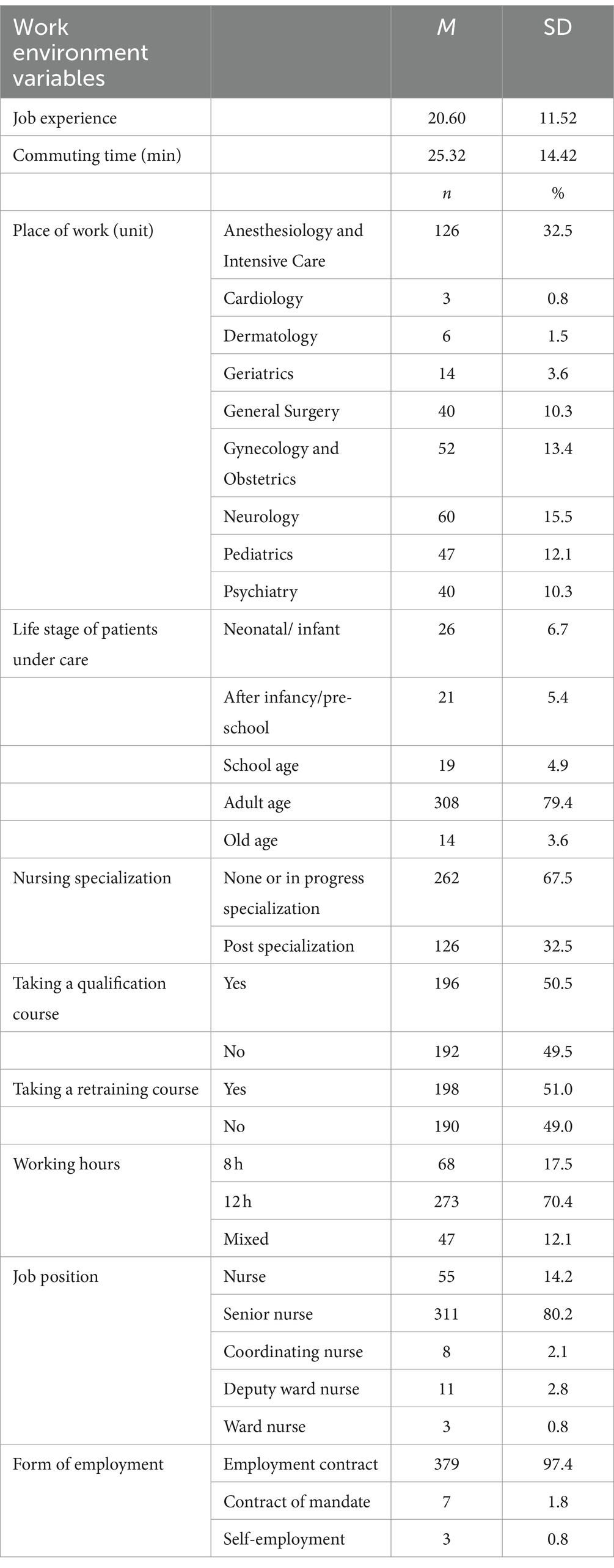
Table 2. Characteristics of the work environment.
4.2 Nurses’ professional values and sociodemographic variables and work environment
The mean scores of the NPVS-3 subscales for care, activism and professionalism are, respectively: 24.23 (SD = 4.07), 39.17 (SD = 5.14) and 21.07 (SD = 3.68). The overall score of this scale was 84.47 (SD = 7.46). A negative correlation was observed between the dimension of care and two variables such as age (r = −0.178; p = 0.024) and participation in a retraining course (Z = −1.921; p = 0.045). The activism dimension correlates negatively with religious beliefs (Z = −1.789; p = 0.044), while the overall NPVS-3 scale score shows a positive relationship with nurses’ commuting time (r = 0.101; p = 0.047) (Table 3).
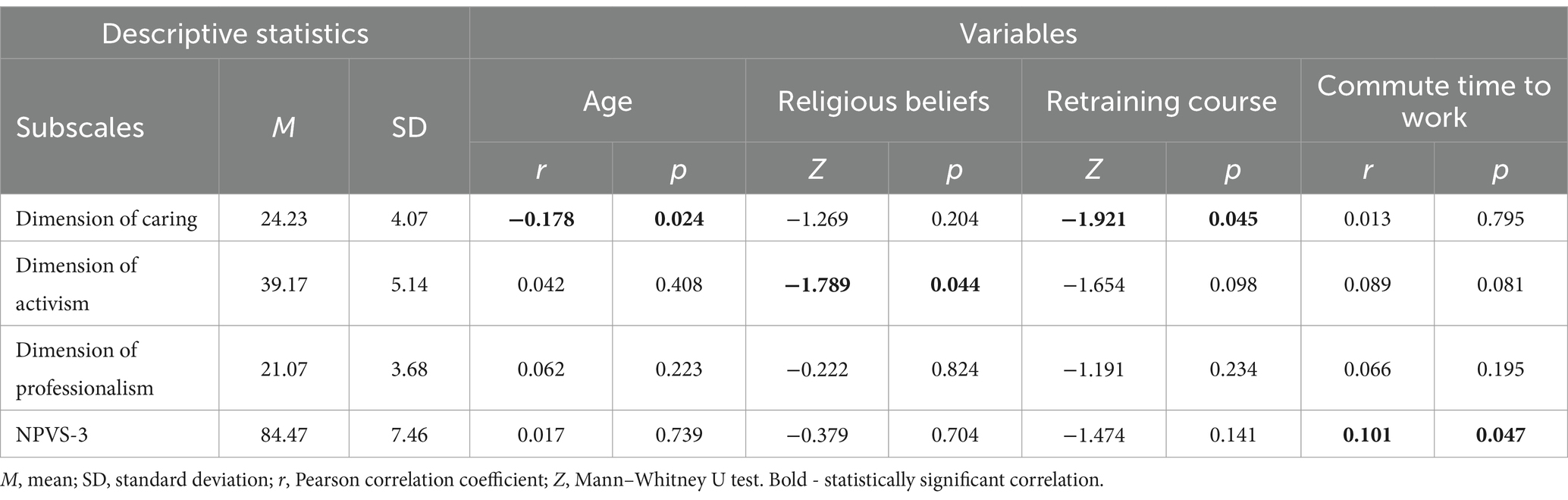
Table 3. Correlations between nurses’ professional values and selected sociodemographic and work environment variables.
4.3 Nurses’ job satisfaction and sociodemographic variables and work environment
The average scores for intrinsic satisfaction, extrinsic satisfaction and overall satisfaction (MSQ-SF) are: 24.42 (SD = 3.78), 35.95 (SD = 5.05) and 60.37 (SD = 6.29) respectively. A positive relationship was observed between the dimension of extrinsic satisfaction and age (r = 0.114; p = 0.025), job experience (r = 0.114; p = 0.025), education (H = 6.645; p = 0.036) and working hours (H = 5.993; p = 0.032). A negative relationship was additionally found between external job satisfaction among nurses and their marital status (Z = −1.958; 0.040) (Table 4).
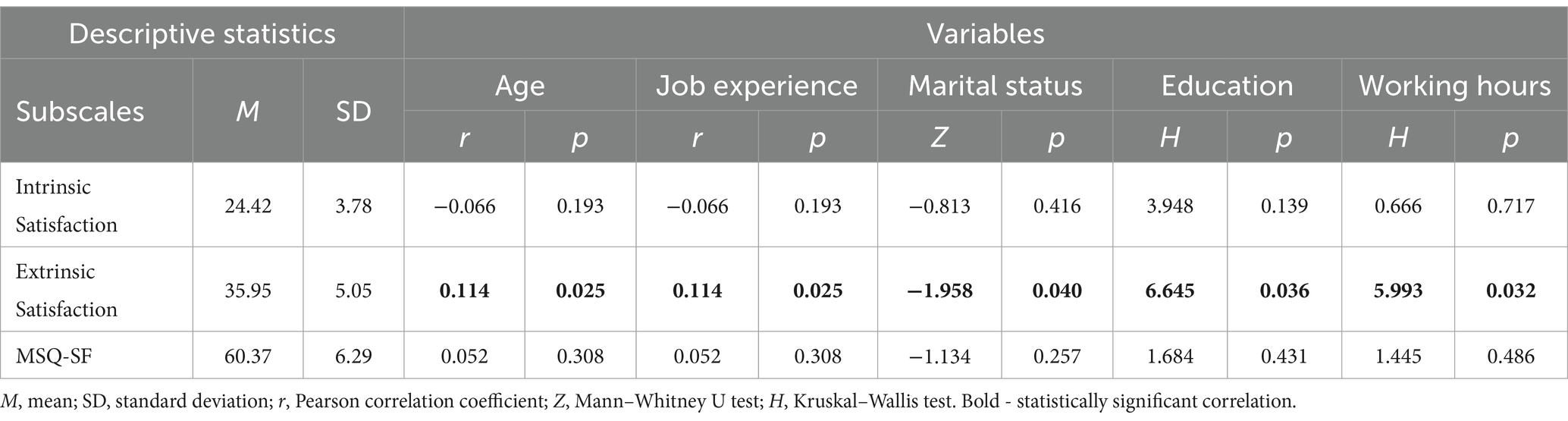
Table 4. Relationships between nurses’ job satisfaction and selected sociodemographic and work environment variables.
4.4 Ethical hospital climate among nurses and sociodemographic variables and work environment
The mean scores for the subscales on ethical hospital climate among nurses oscillate between 11.82 (SD = 2.74)—relations with peers and 17.93 (SD = 3.69)—relations with managers. A positive correlation was found between the subscale of peer relationships and nurses’ education (H = 5.638; p = 0.048). On the other hand, the relationship with physicians subscale correlates negatively with participation in the qualification course by nurses (Z = −2.706; p = 0.048) (Table 5).
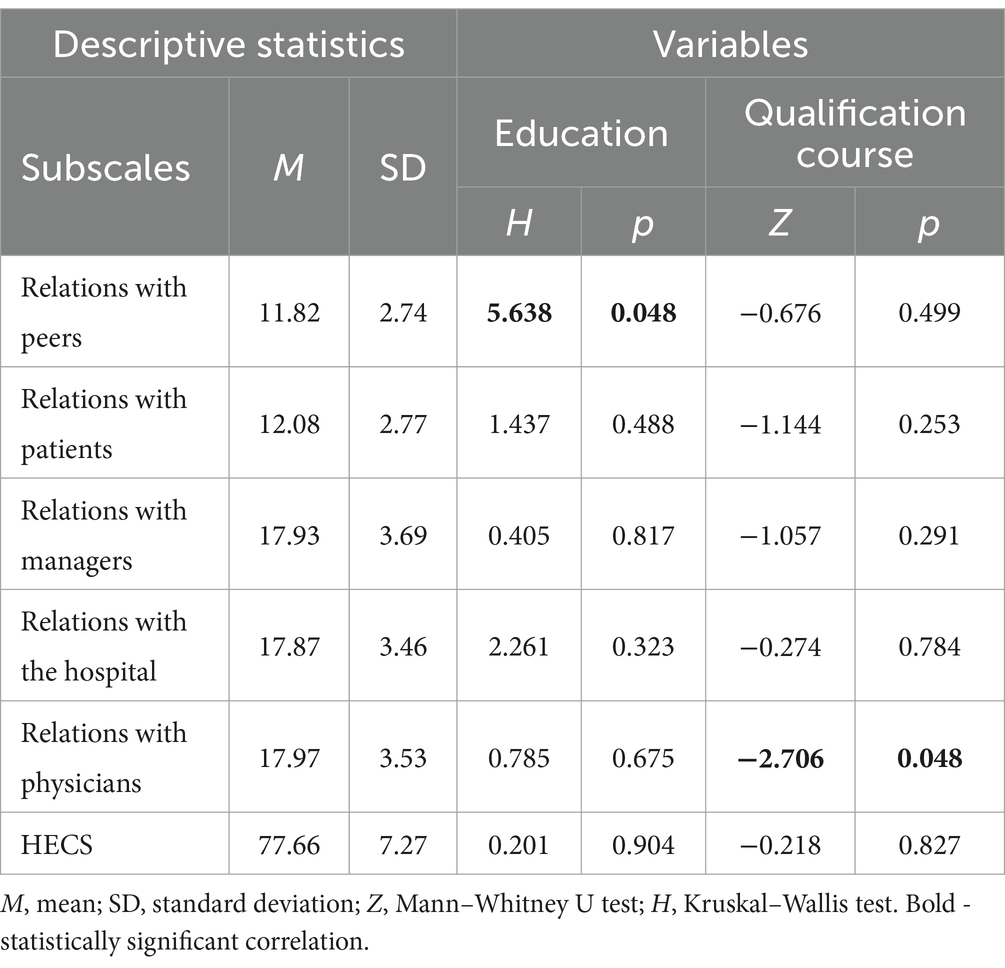
Table 5. Correlations between ethical hospital climate and selected sociodemographic and work environment variables of nurses.
5 Discussion
Professional values, the ethical climate of the hospital as well as job satisfaction are key aspects of nurses’ experience of working that influence their commitment, motivation and the quality of their work. In this study, we analyzed selected socio-demographic and work factors in terms of their relationship with nurses’ professional values, ethical hospital climate and job satisfaction.
In our study, there was a negative correlation between the dimension of care—the professional value of nurses and age (r = −0.178; p = 0.024), where the same relationship was obtained among Polish nursing students (22). The negative correlation between age and dimensions of care suggests that younger nurses may place more importance on aspects of care in their work compared to older colleagues. This may be due to generational differences, where younger generations of nurses may be more motivated or more committed to providing care to patients (23). On the other hand, older nurses may have more professional experience, which may influence their broader view of their work, which includes other aspects beyond direct care (such as management, education of new personnel, and career development), contradicting the results obtained by researchers in Egypt (24). Professional burnout, which is a common problem among nurses with longer tenure, can lead to less commitment to patient care. Physical and emotional fatigue from years of working under stressful conditions can make older nurses less likely to engage in intensive patient care (25).
The negative correlation between participation in a retraining course and dimension of care (Z = −1.921; p = 0.045) may indicate that nurses attending courses must simultaneously fulfill their normal job duties, they may feel overworked, resulting in a decrease in the quality and level of commitment to care (26). Attending refresher courses can result in additional workload, which can limit the time and resources available to devote to patient care. As a result, they may assign less importance to aspects of care in their work (27).
The professional value of activism in nursing refers to the level of nurses’ involvement in initiatives to improve working conditions, raise the quality of health care, protect patients’ rights, and bring about systemic change at various levels of health care (28). Activism can include participation in professional organizations, engaging in community activities, promoting social justice in health care, and fighting for better working conditions for nurses (17).
The negative correlation between the level of professional activism and nurses’ religious beliefs (Z = −1.789; p = 0.044) means that there is an inverse relationship between the two variables. In other words, the more involved nurses are in professional activities, the weaker their religious beliefs may be, and vice versa. The relationship between religiosity and activism among nurses may seem surprising, since intuitively it might seem that religiosity affects the care dimension more than activism. There was a higher level of activism among religious respondents than among non-believers. A likely reason for the higher level of activism among religious respondents compared to non-believers may be that many religions place a strong emphasis on action for others and community involvement. Religious nurses may be more motivated for activism because they see it as part of their spiritual and moral responsibility (29). In the context of nursing practice, religiosity may influence ethical decision-making and approaches to working with patients. Nurses with strong religious beliefs may be more likely to make decisions based on moral and ethical principles derived from their religion (30).
Our study revealed a positive relationship between the overall NPVS-3 scale score and nurses’ commuting time (r = 0.101; p = 0.047). Longer commuting time may promote a higher sense of belonging to the profession and a greater value of nursing work. Nurses who spend more time commuting may experience stronger motivation and dedication in their work, seeing it as important and necessary to overcome commuting difficulties (31).
The mean value of extrinsic satisfaction of work (M = 35.95, SD = 5.05) is higher than that of intrinsic satisfaction (M = 24.42, SD = 3.78), suggesting that nurses may value extrinsic motivators, such as working conditions and salary, more than aspects related to intrinsic motivators. This may be due to the fact that working conditions and salary have a direct impact on their daily lives and well-being, providing them with a sense of financial security and comfort (32, 33). In addition, in the face of heavy workloads and demanding conditions, external factors that improve the work situation are particularly appreciated. Job stability and job security in an occupation subject to high turnover can also play a key role (34). In some health systems and cultures, the emphasis on extrinsic motivators may be stronger and expectations for working conditions and pay higher due to high levels of stress and responsibility. All of the aforementioned factors lead nurses to value extrinsic motivators more, which is reflected in higher average values of extrinsic satisfaction (35).
Analyzing the results of the study, a positive relationship was found between extrinsic satisfaction of work and various factors of nurses such as age, work experience, education and work hours. Similar results regarding the positive relationship between satisfaction and age (as age increases, job satisfaction increases) have been obtained by researchers from India, Saudi Arabia (36, 37). As time passes and work experience increases, nurses may come to appreciate more the external aspects of their jobs, such as employment conditions, pay or career development prospects (38). Higher education also may lead to greater satisfaction with working conditions, perhaps through greater opportunities for career advancement or more favorable contracts with employers (39). Our study found a positive association between on-call length and job satisfaction among nurses, contradicting many previous studies that show a negative association between these variables. Researchers agree that 12 h shift nurses are often associated with negative consequences, such as lower quality of care, job dissatisfaction and higher levels of burnout (26, 40–42).
However, the negative relationship between external satisfaction and marital status indicates that married nurses have lower levels of satisfaction with their working conditions, which may be due to greater family responsibilities or personal life pressures (43). On the other hand, a study by Rashid et al. (44) found a significant relationship between social support from family and job satisfaction. These findings suggest that a supportive environment in family life can significantly affect nurses’ overall life satisfaction and emotional well-being. Family support acts as an important factor in increasing their job satisfaction, confirming that family relationships are crucial to improving the quality of work life in this professional group (44). A positive correlation was found between the HECS subscale on peer relationships and nurses’ education (H = 5.638; p = 0.048), it is worth noting that this result may suggest that nurses with higher levels of education value interactions and cooperation with other members of the nursing staff more. This may be linked to greater ethical awareness and communication skills, which is conducive to building healthy relationships in the workplace (45, 46).
In our study, a negative correlation was observed between the HECS subscale of relations with physicians and nurses’ participation in the qualification course. Nurses attending courses may be more assertive in expressing their opinions and making decisions, which can create conflict or tension in relationships with physicians (47). In addition, it may also be due to hierarchical changes within the healthcare team, where nurses increase their knowledge and competence, which may be perceived by some doctors as a threat to their authority (48).
Of the 586 people who began filling out the questionnaire, 388 completed the survey, corresponding to a response rate of 66%. This means that 198 participants dropped out before completing the survey. It is worth noting that the reasons for quitting may have been varied, including both factors related to the questionnaire design and the individual characteristics of the participants. For example, those with lower job satisfaction may have been less motivated to complete the survey. This shows research by Blaauw et al. (49) that nurses with low job satisfaction often struggle with job burnout, frustration and lack of commitment. These emotional burdens can result in reduced motivation to engage in additional activities, such as survey participation (49).
5.1 Limitations
This study has some limitations. Because the survey began during the SARS-CoV-2 pandemic, it had to be conducted remotely using an online platform. Such remote surveys limit the ability to directly observe behaviors or situations, making it difficult to fully assess nurses’ working conditions. The use of additional qualitative methods, such as interviews or observations, could help to better understand the context of their work and identify subtle factors affecting professional values, the ethical climate in the hospital and job satisfaction.
The study was cross-sectional in nature. It was conducted at a time point, and this makes it impossible to draw causal conclusions—this is also worth emphasizing. The survey sample was conveniently selected, which is a limitation and requires caution when interpreting the results in the context of the entire population of nurses. The study covered only one region of Poland, specifically the Eastern part of the country, which should also be noted. This geographic limitation may lead to a lack of representativeness for the country as a whole, as working conditions and cultural factors may differ in different regions.
The study did not analyze the relationship between gender and professional values, ethical climate of the hospital and job satisfaction, as the male group represented only 4.6% of the study population. Such a small representation of men prevented a reliable and statistically significant comparative analysis between the genders. To study this relationship in the future, research samples can be increased by recruiting more men, using purposive sampling, conducting multi-center studies, and developing analytical methods that take small groups into account. These measures will enable future studies to more accurately analyze differences and similarities in the variables studied between the two genders.
6 Conclusion
In a study on the relationship between socio-demographic and professional factors on professional values, job satisfaction and ethical climate among nurses, several significant correlations were observed. Older nurses and those who participated in retraining courses showed lower values related to caring for patients, while higher professional commitment was found in nurses who spent more time commuting to the hospital. In addition, the older nurses with more experience, education and longer work experience showed greater satisfaction with such external aspects of their jobs as pay, working conditions and professional development opportunities. In terms of the ethical climate of the hospital, nurses with more education had better relationships with their colleagues, but may have had difficulties in their relationships with physicians. These findings underscore the need to consider a variety of factors when developing strategies for managing nursing staff and improving the quality of health care. Additional research in this area may contribute to a better understanding of nurses’ professional experiences and identify areas for intervention.
7 Implications
Developing effective intervention strategies in the area of the relationship between nurses’ professional values, ethical hospital climate, job satisfaction, and sociodemographic and work environment variables can be a key challenge for managing medical staff and improving the quality of health care. In this context, the development of extensive training and education programs can be an effective intervention strategy. Such programs can include nursing staff and nursing management. Training courses and workshops can be conducted in the form of interactive sessions where participants have the opportunity to discuss, share experiences and practically apply the skills they have learned in the context of nursing work. These programs can focus on developing skills related to ethical decision-making, coping with professional stress and building interpersonal relationships in the workplace.
Supporting leaders and managers in their role of promoting an ethical climate and building a positive work environment can also be an important part of intervention strategies. Managers can be trained to identify and address ethical climate issues, communicate with staff, and effectively manage human resources. By strengthening managerial competencies in the areas of building positive interpersonal relationships and fostering professional values, the management of a medical facility can contribute to creating an open, trusted and productive work environment.
An important aspect of the intervention strategy is also to create open channels of communication that will enable medical employees to express their concerns, suggestions and participate in decision-making regarding the ethical climate and professional values. Open and direct communication can help build trust, increase professional engagement and improve staff-management relations. In practice, this means creating mechanisms that allow employees to participate in decisions about work organization, assess changes in the work environment, and adjust intervention strategies to meet the current needs of medical staff.
However, the implementation of these strategies requires a holistic approach and continuous monitoring of the effects to adapt the activities to changing needs and working conditions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
The studies involving humans were approved by The Bioethics Committee at the Medical University of Lublin (reference number: KE-0254/17/2021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PO: Conceptualization, Data curation, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. KJ: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. BD: Conceptualization, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Schmidt, BJ, and McArthur, EC. Professional nursing values: a concept analysis. Nurs Forum. (2018) 53:69–75. doi: 10.1111/nuf.12211
2. International Council of Nurses . The ICN code of ethics for nurses In: A Dewey and A Holecek, editors. The Nurse's healthcare ethics committee. Geneva, Switzerland: Sigma Global Nursing Excellence (2019)
3. Fernández-Feito, A, Palmeiro-Longo, MDR, Hoyuelos, SB, and García-Díaz, V. How work setting and job experience affect professional nurses' values. Nurs Ethics. (2019) 26:134–47. doi: 10.1177/0969733017700238
4. Dall'Ora, C, Ball, J, Reinius, M, and Griffiths, P. Burnout in nursing: a theoretical review. Hum Resour Health. (2020) 18:41. doi: 10.1186/s12960-020-00469-9
5. Kaya, A, and Boz, İ. The development of the professional values model in nursing. Nurs Ethics. (2019) 26:914–23. doi: 10.1177/0969733017730685
6. Tehranineshat, B, Torabizadeh, C, and Bijani, M. A study of the relationship between professional values and ethical climate and nurses' professional quality of life in Iran. Int J Nurs Sci. (2020) 7:313–9. doi: 10.1016/j.ijnss.2020.06.001
7. Essex, R, Thompson, T, Evans, TR, Fortune, V, Kalocsányiová, E, Miller, D, et al. Ethical climate in healthcare: a systematic review and meta-analysis. Nurs Ethics. (2023) 30:9697330231177419–921. doi: 10.1177/09697330231177419
9. Olson, LL . Hospital nurses' perceptions of the ethical climate of their work setting. Image J Nurs Sch. (1998) 30:345–9. doi: 10.1111/j.1547-5069.1998.tb01331.x
10. Fradelos, EC, Latsou, D, Alikari, V, Papathanasiou, IV, Roupa, A, Balang, V, et al. Greek nurses' perception of hospital ethical climate: a cross-sectional study. Adv Exp Med Biol. (2021) 1337:17–25. doi: 10.1007/978-3-030-78771-4_3
11. Lanes, TC, Dalmolin, GL, Silva, AMD, Bernardi, CMS, Schutz, TC, and Tiguman, GMB. Influence of the ethical climate on workers' health among healthcare professionals: a systematic review. Rev Gaucha Enferm. (2023) 44:e20220247. doi: 10.1590/1983-1447.2023.20220247.en
12. Tomaszewska, K, Kowalczuk, K, Majchrowicz, B, Kłos, A, and Kalita, K. Areas of professional life and job satisfaction of nurses. Front Public Health. (2024) 12:1370052. doi: 10.3389/fpubh.2024.1370052
13. Caricati, L, Sala, RL, Marletta, G, Pelosi, G, Ampollini, M, Fabbri, A, et al. Work climate, work values and professional commitment as predictors of job satisfaction in nurses. J Nurs Manag. (2014) 22:984–94. doi: 10.1111/jonm.12079
14. Yarbrough, S, Martin, P, Alfred, D, and McNeill, C. Professional values, job satisfaction, career development, and intent to stay. Nurs Ethics. (2017) 24:675–85. doi: 10.1177/0969733015623098
15. Jarosz, K, and Młynarska, A. The impact of sociodemographic factors on job satisfaction and professional burnout among nurses in urology departments. Nurs Rep. (2024) 14:883–900. doi: 10.3390/nursrep14020068
16. Skrivankova, VW, Richmond, RC, Woolf, BAR, Yarmolinsky, J, Davies, NM, Swanson, SA, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. (2021) 326:1614–21. doi: 10.1001/jama.2021.18236
17. Weis, D, and Schank, MJ. Development and psychometric evaluation of the nurses professional values Scale-3. J Nurs Meas. (2017) 25:400–10. doi: 10.1891/1061-3749.25.3.400
18. Ozdoba, P, Dziurka, M, Dziubaszewska, R, and Dobrowolska, B. Nursing based on professional values: selected psychometric properties of the polish version of the nurses professional values scale-three (NPVS-3-POL). Med Stud. (2023) 39:230–7. doi: 10.5114/ms.2023.131690
19. Dziurka, M, Ozdoba, P, Olson, L, Jedynak, A, Ozga, D, Jurek, K, et al. Hospital ethical climate survey - selected psychometric properties of the scale and results among polish nurses and midwives. BMC Nurs. (2022) 21:295. doi: 10.1186/s12912-022-01067-x
20. Weiss, DJ, Dawis, RV, England, GW, and Lofquist, LH. Minnesota satisfaction questionnaire--short form. Educ Psychol Meas. (1977) 22.
21. Ingram, T, and Głód, W. Wykorzystanie MSQ jako narzędzia badania satysfakcji z pracy w wybranej jednostce ochrony zdrowia. Szynal Joanna (red) Manag Sci. (2014) 3:31–43. doi: 10.15611/noz.2014.3.03
22. Machul, M, Dziurka, M, Gniadek, A, Gotlib, J, Gutysz-Wojnicka, A, Kotowski, M, et al. Caring ability and professional values of polish nursing students-a cross-sectional study. Int J Environ Res Public Health. (2022) 19:11308. doi: 10.3390/ijerph191811308
23. Gallegos, C, and Sortedahl, C. An exploration of professional values held by nurses at a large freestanding pediatric hospital. Pediatr Nurs. (2015) 41:187–95.
24. Ghonem, N, and Abdrabou, H. Professional values, clinical decision-making, and organizational commitment among nurses: analytic cross-sectional study. Egypt J Health Care. (2021) 12:707–21. doi: 10.21608/ejhc.2021.148841
25. Jiang, H, Huang, N, Jiang, X, Yu, J, Zhou, Y, and Pu, H. Factors related to job burnout among older nurses in Guizhou province, China. PeerJ. (2021) 9:e12333. doi: 10.7717/peerj.12333
26. Dall'Ora, C, Griffiths, P, Ball, J, Simon, M, and Aiken, LH. Association of 12 h shifts and nurses’ job satisfaction, burnout and intention to leave: findings from a cross-sectional study of 12 European countries. BMJ Open. (2015) 5:e008331. doi: 10.1136/bmjopen-2015-008331
27. Mlambo, M, Silén, C, and McGrath, C. Lifelong learning and nurses' continuing professional development, a metasynthesis of the literature. BMC Nurs. (2021) 20:62. doi: 10.1186/s12912-021-00579-2
28. Hampton, D, Heath, J, and Rayens, MK. Strengthening professional values of doctoral-level nursing students. SAGE Open Nurs. (2022) 8:23779608221126359. doi: 10.1177/23779608221126359
29. Allahyari Bouzanjani, A, Bahadori, P, and Nikoonam, P. Nurses' empathetic behaviors: the direct and indirect effect of their spiritual orientation. J Relig Health. (2021) 60:134–52. doi: 10.1007/s10943-019-00966-9
30. White, JH, Peirce, AG, and Jacobowitz, W. The relationship amongst ethical position, religiosity and self-identified culture in student nurses. Nurs Ethics. (2019) 26:2398–412. doi: 10.1177/0969733018792738
31. Møller, N, Berthelsen, C, and Hølge-Hazelton, B. Driving for the unique opportunity for work: a qualitative study of nurses' motivation to commute to work. J Manag Psychol. (2021) 37:279–93. doi: 10.1108/JMP-02-2021-0107
32. Bektas, G, Kulalar, KS, and Unver, V. The effect of nurses' occupational safety perceptions on job satisfaction: a research study conducted in Turkey. J Pak Med Assoc. (2022) 72:270–4. doi: 10.47391/JPMA.1612
33. Sewera, K, and Szpakow, A. Job satisfaction of nurses and the determinants of organizational climate: insights from hospitals in Lubelskie Voivodeship. Pielegniarstwo XXI Wieku/Nursing in the 21st Century. (2024)
34. Lu, H, Zhao, Y, and While, A. Job satisfaction among hospital nurses: a literature review. Int J Nurs Stud. (2019) 94:21–31. doi: 10.1016/j.ijnurstu.2019.01.011
35. Turner, A . How does intrinsic and extrinsic motivation drive performance culture in organizations? Cog Educ. (2017) 4:4. doi: 10.1080/2331186X.2017.1337543
36. Sharma, A, Kaushal, V, Pandey, N, Arora, P, Thiyagarajan, A, and Bhattacharya, S. Assessment of job satisfaction among nursing officers working at a tertiary care hospital in northern India. CHRISMED J Health Res. (2020) 7:35. doi: 10.4103/cjhr.cjhr_11_19
37. Al-Haroon, HI, and Al-Qahtani, MF. The demographic predictors of job satisfaction among the nurses of a major public hospital in KSA. J Taibah Univ Med Sci. (2019) 15:32–8. doi: 10.1016/j.jtumed.2019.11.003
38. Lin, CF, Lai, FC, Huang, WR, Huang, CI, and Hsieh, CJ. Satisfaction with the quality nursing work environment among psychiatric nurses working in acute care general hospitals. J Nurs Res. (2020) 28:e76. doi: 10.1097/jnr.0000000000000350
39. Shi, X, Xiong, D, Zhang, X, Han, M, Liu, L, and Wang, J. Analysis of factors influencing the job satisfaction of medical staff in tertiary public hospitals, China: a cross-sectional study. Front Psychol. (2023) 14:1048146. doi: 10.3389/fpsyg.2023.1048146
40. Stimpfel, AW, and Aiken, LH. Hospital staff nurses’ shift length associated with safety and quality of care. J Nurs Care Qual. (2013) 28:122–9. doi: 10.1097/NCQ.0b013e3182725f09
41. Ball, J, Day, T, Murrells, T, Dall’Ora, C, Rafferty, AM, Griffiths, P, et al. Cross-sectional examination of the association between shift length and hospital nurses job satisfaction and nurse reported quality measures. BMC Nurs. (2017) 16:26. doi: 10.1186/s12912-017-0221-7
42. Varghese, B, Joseph, CM, Al-Akkam, AAA, Al-Balawi, RMOAM, Swallmeh, E, and Singh, K. Nurse's experience working 12-hour shift in a tertiary level hospital in Qatar: a mixed method study. BMC Nurs. (2023) 22:213. doi: 10.1186/s12912-023-01371-0
43. Azimian, J, Piran, P, Jahanihashemi, H, and Dehghankar, L. Investigation of marital satisfaction and its relationship with job stress and general health of nurses in Qazvin, Iran. Electron Physician. (2017) 9:4231–7. doi: 10.19082/4231
44. Rashid, WEW, Nordin, MS, Omar, A, and Ismail, I. Social support, work-family enrichment and life satisfaction among married nurses in health service. Int J Soc Sci Human. (2011) 1:150–5.doi: 10.7763/IJSSH.2011.V1.26
45. Özden, D, Arslan, GG, Ertuğrul, B, and Karakaya, S. The effect of nurses' ethical leadership and ethical climate perceptions on job satisfaction. Nurs Ethics. (2019) 26:1211–25. doi: 10.1177/0969733017736924
46. Okumoto, A, Yoneyama, S, Miyata, C, and Kinoshita, A. The relationship between hospital ethical climate and continuing education in nursing ethics. PLoS One. (2022) 17:e0269034. doi: 10.1371/journal.pone.0269034
47. Crist, K, Lafferty, M, Umberfield, E, and Manojlovich, M. Which factors promote shared understanding between physicians and nurses in inpatient oncology care settings? A qualitative exploration. Cancer Nurs. (2022) 45:E338–44. doi: 10.1097/NCC.0000000000000959
48. House, S, and Havens, D. Nurses' and physicians' perceptions of nurse-physician collaboration: a systematic review. J Nurs Adm. (2017) 47:165–71. doi: 10.1097/NNA.0000000000000460
Keywords: sociodemographic, work environment, nurses, professional values, satisfaction, ethical climate
Citation: Ozdoba P, Jurek K and Dobrowolska B (2024) Professional values, ethical climate and job satisfaction of nurses and their selected sociodemographic and occupational characteristics. Front. Public Health. 12:1501102. doi: 10.3389/fpubh.2024.1501102
Edited by:
Adriano Friganovic, University of Rijeka, CroatiaReviewed by:
Dalia Almaghaslah, King Khalid University, Saudi ArabiaRobert Lovrić, Josip Juraj Strossmayer University of Osijek, Croatia
Copyright © 2024 Ozdoba, Jurek and Dobrowolska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrycja Ozdoba, cGF0cnljamEub3pkb2JhQHVtbHViLnBs