1Gdansk University of Physical Education and Sport, Gdańsk, Poland
2Department of Physical Education, Zhengzhou University, Zhengzhou, China
3Department of Sports, Recreation and Wellness, Symbiosis International (Deemed University), Hyderabad Campus, Modallaguda (V), Nandigama (M), Rangareddy, Telangana, India
Objectives: This study aimed to explore the interrelationships among leisure activities, self-reported health (SRH), anxiety, and depression in Chinese older adults using structural equation modeling (SEM).
Methods: Data from the 2018 Chinese Longitudinal Healthy Longevity Survey (CLHLS) were analyzed and 9,859 older adults were included in the analysis. The SEM was employed to examine the direct and indirect effects of leisure activities on depression through SRH and anxiety.
Results: Leisure activities significantly positively influenced SRH (β = 0.18, p < 0.001) and negatively affected depression (β = −0.16, p < 0.001) and anxiety (β = −0.09, p < 0.001). SRH decreased depression (β = −0.33, p < 0.001) and anxiety (β = −0.33, p < 0.001), while anxiety increased depression (β = 0.49, p < 0.001). SRH and anxiety mediated the relationship between leisure activities and depression.
Conclusion: The findings support the proposed model and suggest that promoting leisure activities can improve mental health in Chinese older adults.
1 Introduction
Mental health is a growing issue worldwide. According to World Health Organization (WHO), nearly 1 billion people worldwide suffer from mental disorders, equivalent to about 13% of the global population (1). Depressive and anxiety disorders are the leading contributors to this burden. Depression affects an estimated 280 million people globally, while anxiety disorders affect around 300 million people (2). Furthermore, with the outbreak of COVID-19 pandemic, a 25% increase in the prevalence of anxiety and depression worldwide has been triggered (3). Depressive disorders, peaking in older adulthood, affect approximately 63 million people or 7% of the population aged 60 years and older worldwide (4). As China has entered an aging society, the proportion of people aged 60 and over in China reached 18.70%, and the proportion of people aged 65 and over reached 13.50%, with a trend of increasing year by year (5). Improving mental health, particularly preventing anxiety and depression among older adults, has become a serious public health issue in China, especially after the COVID-19 epidemic.
Leisure activities have been identified as a positive method for improving health and well-being among older adults. These activities, which include physical, cognitive, intellectual, and social engagements, are associated with better health outcomes, successful aging and overall well-being in older adults (6–9). The participation and exploration of leisure activities among older adults have been significantly linked to depression levels and quality of life (10). Successful engagement in leisure activities during old age can help alleviate psychological stress, enhance life satisfaction, and improve overall quality of life (11). Additionally, these activities have been shown to be associated with reduced all-cause mortality among older adults (12, 13).
Although many studies have examined factors affecting depression among older adults, none have simultaneously examined the relationships among leisure activities, SRH, anxiety, and depression. In addition, there have been no studies to investigate the relationships between leisure activities and depression through mediating factors such as SRH or anxiety. Therefore, this study proposes and tests a conceptual model explaining these interrelationships using CLHLS data.
1.1 Relationships among leisure activities, SRH, anxiety, and depression
Numerous studies have highlighted the positive impact of leisure activities on the health of older adults. For instance, Yang et al. (7) demonstrated that consistent engagement in productive physical activity can enhance perceived health-related quality of life among older individuals. Similarly, Sala et al. (8) found that active participation in leisure activities helps maintain cognitive, physical, and mental health in this population. Other researchers, such as Guerrero et al. (14) have shown that leisure activities can prevent dementia and other diseases in older adults. Additionally, studies by Lin et al. (15) have identified positive associations between physical activity and SRH.
Leisure activities have also been found to prevent depression and anxiety in older adults (16, 17) and are considered a beneficial method for improving mental health. Specifically, several studies have reported that physical activity can reduce symptoms of depression and anxiety (18, 19). For example, Wanjau et al. (20) found that higher levels of physical activity are inversely related to incident depression and anxiety, suggesting that inactivity may be causally linked to these conditions. Kim et al. (21) also observed that participation in leisure physical activity and resistance exercise is associated with a lower prevalence of depressive symptoms among Korean adults. Mammen et al. (22) identified a significant inverse relationship between baseline physical activity and depression in a review of 30 primary studies. McDowell et al. (23) conducted a systematic review and meta-analysis of prospective cohort studies, finding that physical activity is associated with lower odds of self-reported anxiety symptoms, diagnosis of any anxiety disorder, and diagnosis of generalized anxiety disorder. Schuch et al. (24) found that high self-reported physical activity levels are associated with lower rates of incident anxiety compared to low physical activity levels. As a result, physical activity has been proposed as an adjunct treatment for depression and anxiety (25).
SRH is a subjective measure that encompasses biological, mental, social, and functional aspects of a person’s well-being, including individual and cultural beliefs and health behaviors (26). Research indicates that SRH effectively predicts mortality (27) and SRH is a significant predictor of current health status (28), an important indicator of depression (29), and is associated with quality of life and depression (30). For example, Badawi et al. (31) found that fair or poor self-rated health at baseline predicts a twofold increased risk for major depression at follow-up, even after adjusting for socio-demographic characteristics, lifestyle behaviors, disability, and diabetes. Depression has also been linked to poor self-rated health and increased mortality in the general population (32). More recently, Shen and Zou (33) identified an inverse nonlinear association between cardiovascular health and depression.
Studies have also shown that individuals with poorer SRH status often exhibit higher levels of anxiety symptoms. This association may stem from the negative impact of mental health problems on an individual’s overall perception of health (34). Additionally, the frequent occurrence of anxiety symptoms is closely related to a decline in health-related quality of life, and anxiety may reduce an individual’s overall satisfaction with their health by affecting their emotional state and daily functioning (35), indicating that anxiety affects not only mental health but also an individual’s subjective evaluation of their own health through psychological mechanisms (36).
In addition, studies have also shown SRH may play a mediating role between leisure activities and depression and actively engaging in leisure activities can enhance an individual’s SRH, which in turn reduces depressive symptoms (37, 38).
With regards to the relationship between anxiety and depression, comorbid depression and anxiety are highly prevalent conditions (39). Study (40) emphasized that the overlap between depression and anxiety symptoms is central to classifying affective disorders, as most patients with depression also have anxiety, and vice versa. Evidence also suggested genetic and neurobiologic similarities between depressive and anxiety disorders (41). In relation to the evolution of their comorbidity, studies demonstrated that anxiety disorders generally precede the presentation of major depressive disorder (42). A meta-analysis (43) found that anxiety and depression are bidirectional risk factors, and treating one disorder can significantly reduce the symptoms of the other. Another study (44) indicated that treatments targeting anxiety (particularly CBT and medication) can significantly improve the prognosis of patients with comorbid depression.
1.2 Research hypotheses
Drawing on the existing literature, we formulate the following hypotheses:
H1: Leisure activities will have a positive and direct impact on SRH among older adults in China.
H2: Leisure activities will have a negative effect on depression among older adults in China.
H3: Leisure activities will have a negative effect on anxiety among older adults in China.
H4: SRH will have a negative influence on depression among older adults in China.
H5: SRH will have a negative influence on anxiety among older adults in China.
H6: Anxiety will have a positive effect on depression among older adults in China.
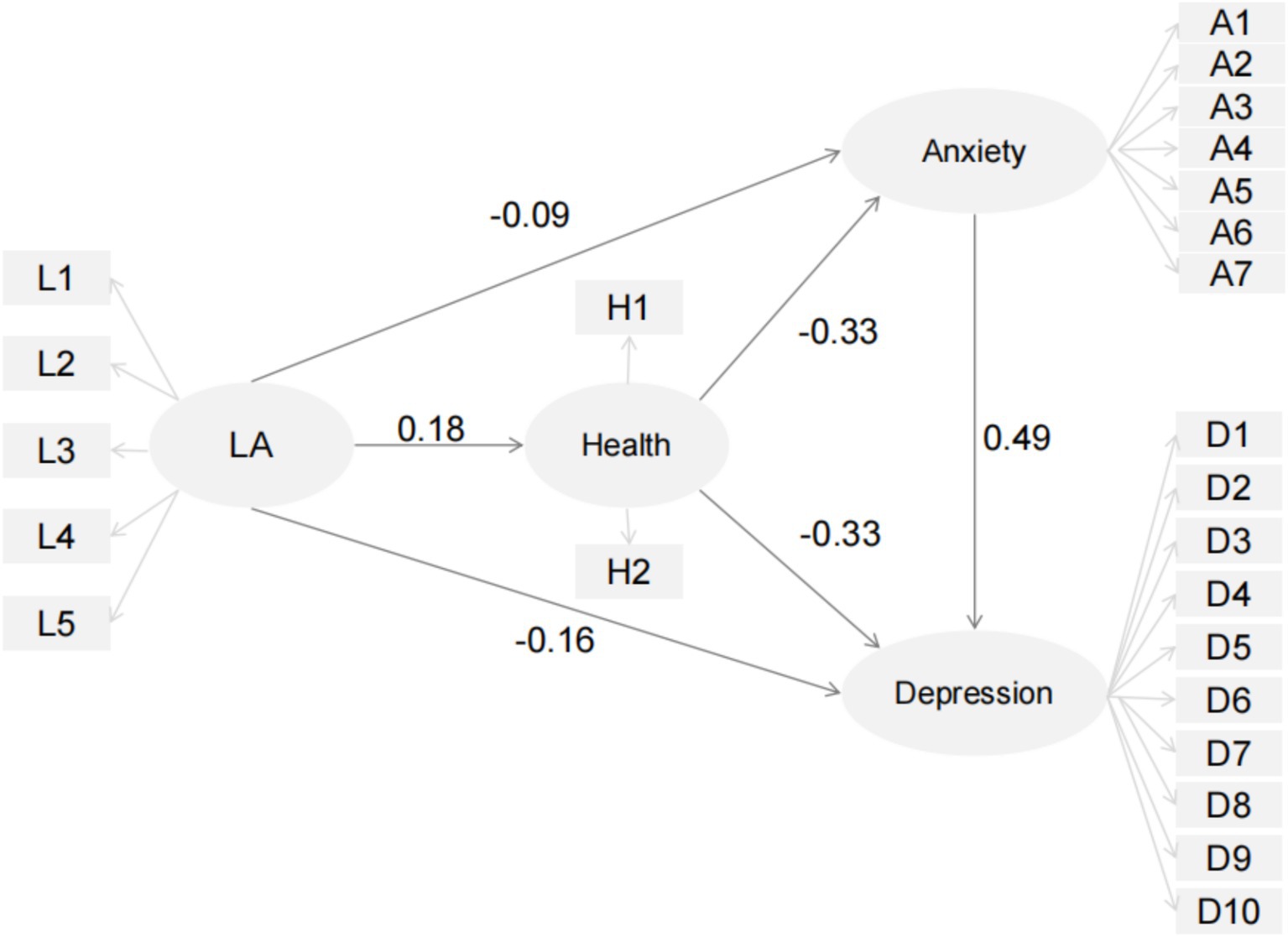
H7: SRH and anxiety will mediate the relationship between leisure activities and depression among older adults in China (Figure 1)
Figure 1
Figure 1. Proposed model of the influence of leisure activities, self-reported health, and anxiety on depression in older adults and structural test for the relationships among those variables. Of LA, leisure activities.
2 Materials and methods
2.1 Data source and samples
The present study utilized data from the 2018 wave of the CLHLS. It covers 23 out of 31 provinces in China and includes 15,874 respondents aged 50 years and older. The survey comprises more than 750 questions, covering extensive data on demographics, socioeconomic conditions, psychological traits, social participation, and health conditions. All data were collected via face-to-face interviews during in-home visits (45). The study was approved by the Ethics Committee of Peking University (IRB00001052–13074) (46). For more detailed information regarding the CLHLS, including the sampling design, response rates, attrition, and systematic assessments of data quality, readers are referred to previous publications (47, 48). Our research is a secondary analysis using data from the CLHLS. All procedures performed in studies involving human participants were in accordance with the ethical standards of the Ethics Committee of Peking University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
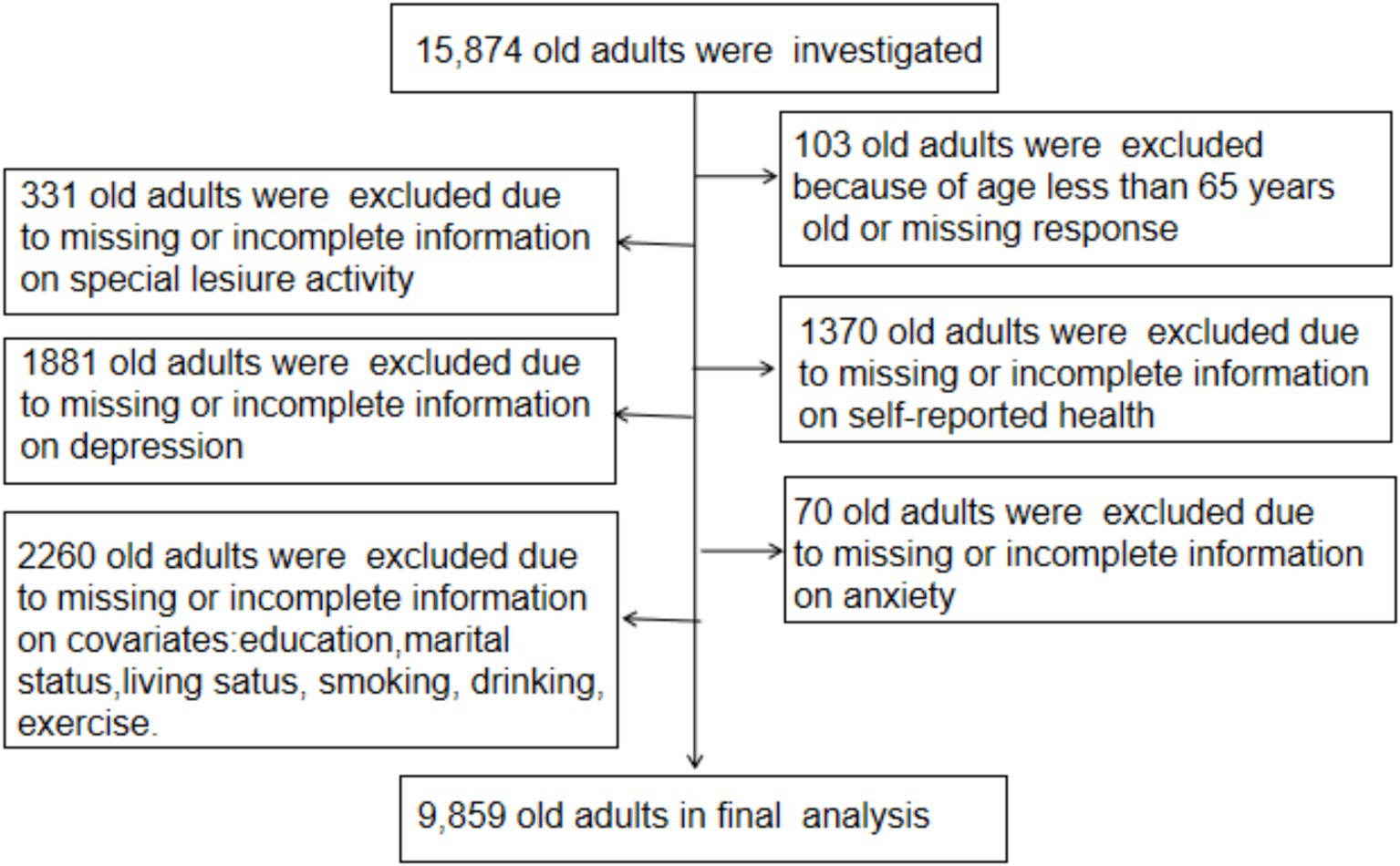
For the current analysis, participants were included if they met the following criteria: (a) aged 65 years and older; (b) complete information on variables related to leisure activities, SRH, anxiety, and depression; and (c) complete data on variables such as age, sex, residence, education level, marital status, living status (co-residence), smoking, drinking, and exercise. A total of 15,874 participants were surveyed in the 2018 wave of the CLHLS. After excluding individuals who did not meet the inclusion criteria, the final analysis included 9,859 older adults (Figure 2).
Figure 2
Figure 2. Flowchart of participants included in this study.
2.2 Assessment of leisure activities
A five-item index was used to assess participants’ engagement in leisure activities. Participants were asked, “Do you participate in the following activities?” The activities included: (a) gardening, (b) reading newspapers or books, (c) playing cards or mahjong, (d) watching TV or listening to the radio, and (e) participating in social activities. Responses for each activity were recorded on a five-point frequency scale: 1 = almost every day, 2 = not daily but at least once a week, 3 = not weekly but at least once a month, 4 = not monthly but sometimes, and 5 = never. To ensure that higher scores indicated greater participation in leisure activities, the scores were reversed such that a higher score corresponded to a higher level engagement.
2.3 Assessment of self-reported health
SRH was assessed using two questions: (a) “How do you rate your health at present?” with response options ranging from 1 (very good) to 5 (very bad); and (b) “How do you rate your health at present compared with 1 year ago?” with response options ranging from 1 (much better) to 5 (much worse). To ensure that higher scores indicated better health, the scores were reversed such that a higher score corresponded to better health status.
2.4 Assessment of anxiety
Anxiety symptoms were assessed using the 7-item Generalized Anxiety Disorder scale (GAD-7) (49), which has been validated among Chinese old adults (50, 51). Participants were asked, “In the last 2 weeks, how often have you experienced the following symptoms?” Seven items were included. Each item was rated on a 4-point scale: 0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day. The total score ranges from 0 to 21, with higher scores indicating more severe anxiety symptoms. Previous research has confirmed the reliability and validity of the GAD-7 in measuring anxiety symptoms (52). In the current study, the Cronbach’s alpha coefficient for the anxiety scale was 0.92, indicating high internal consistency.
2.5 Assessment of depression
Depression was measured using the 10-item Center for Epidemiological Studies Depression Scale (CESD-10), which has demonstrated adequate reliability (53). Participants in the 2018 CLHLS were asked to rate “how often you felt this way during the past week” for each item. Responses were recorded on a five-point scale: 1 = always, 2 = often, 3 = sometimes, 4 = seldom, and 5 = never. To ensure that higher scores indicated more severe depression, the scores were reversed such that a higher score corresponded to greater depression severity. The Cronbach’s alpha coefficient for the CESD-10 in this study was 0.81, indicating good internal consistency.
2.6 Assessment of other variables
Several factors related to demographics, socioeconomic status, and health were included in this study, as they may be potential risk factors for depression and anxiety in older adults. These factors included age, sex, residence, education level, marital status, living status (co-residence), smoking, drinking, and exercise. Residence was classified as “urban” or “rural.” Education level was assessed by asking participants the number of years they had attended school. Marital status was categorized as “married and living with spouse,” “widowed, “or “others (married but not living with spouse, divorced, or never married).” Living status (co-residence) was divided into three groups: “with household member(s), “in an institution”, and “living alone.” Participants who habitually consumed alcohol, smoked cigarettes, or engaged in physical exercise were identified as “current drinkers,” “current smokers,” or “current exercisers,” respectively.
2.7 Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD), while categorical variables are presented as frequencies and proportions (%). Data analyses were performed using SPSS software version 19 (SPSS Inc., Chicago, IL, USA) and AMOS version 23.0 (IBM, Armonk, NY, USA). Frequency analysis, reliability analysis, and correlational analysis were conducted using SPSS. Confirmatory factor analysis (CFA) and SEM were performed using AMOS. All reported p-values were based on two-sided tests.
3 Results
3.1 Characteristics of the study population
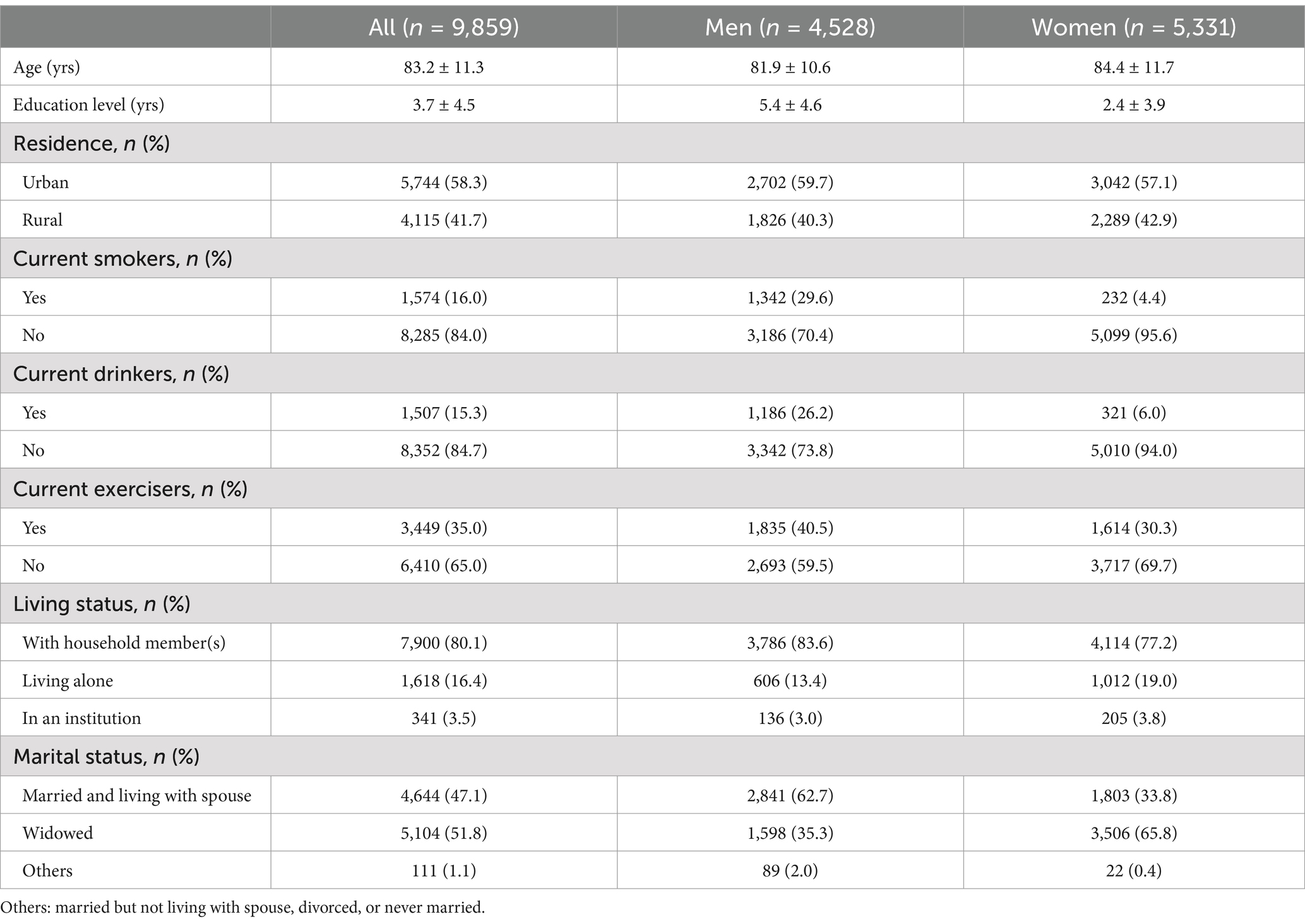
The final analytical sample included 9,859 older adults, with 45.9% males (n = 4,528) and 54.1% females (n = 5,331). The average age was 83.2 years (SD = 11.3), and the mean years of education was 3.7 years (SD = 4.5). Among the participants, 58.3% resided in urban areas, 16.0% were current smokers, 15.3% were current drinkers, and 35.0% reported engaging in regular physical exercise. In terms of living arrangements, 80.1% lived with household members, 16.4% lived alone, and 3.5% lived in institutions. Table 1 presents the detailed socio-demographic characteristics by sex.
Table 1
Table 1. The characteristics of participants stratified by sex.
3.2 Confirmatory factor analysis (CFA)
Confirmatory factor analysis was conducted to assess the measurement model, including four latent variables: leisure activities, self-reported health, anxiety, and depression. All factor loadings were statistically significant, ranging from 0.57 to 0.92, indicating acceptable construct validity. Cronbach’s alpha coefficients ranged from 0.56 (leisure activities) to 0.92 (anxiety), suggesting acceptable to excellent reliability (54, 55) (Table 2).
Table 2
Table 2. Confirmatory factor analysis: reliability, item loadings, and model fit indices.
Model fit indices indicated a good fit: RMSEA = 0.06, CFI = 0.91, NFI = 0.91, TLI = 0.90. All values exceeded the recommended thresholds (56–58), supporting the adequacy of the measurement model.
3.3 Correlations among variables
Pearson correlation analysis showed that leisure activities were positively associated with self-reported health (r = 0.20, p < 0.001), and negatively associated with depression (r = −0.13, p < 0.001) and anxiety (r = −0.05, p < 0.001). Self-reported health was negatively correlated with both depression (r = −0.26, p < 0.001) and anxiety (r = −0.19, p < 0.001), while anxiety was strongly and positively correlated with depression (r = 0.65, p < 0.001). All correlation coefficients were below 0.70, supporting discriminant validity (59) (Table 3).
Table 3
Table 3. Correlations among constructs.
3.4 SEM results for the structural model and hypotheses testing
The structural model demonstrated acceptable fit to the data: p < 0.001, RMSEA = 0.06, CFI = 0.91, TLI = 0.90.
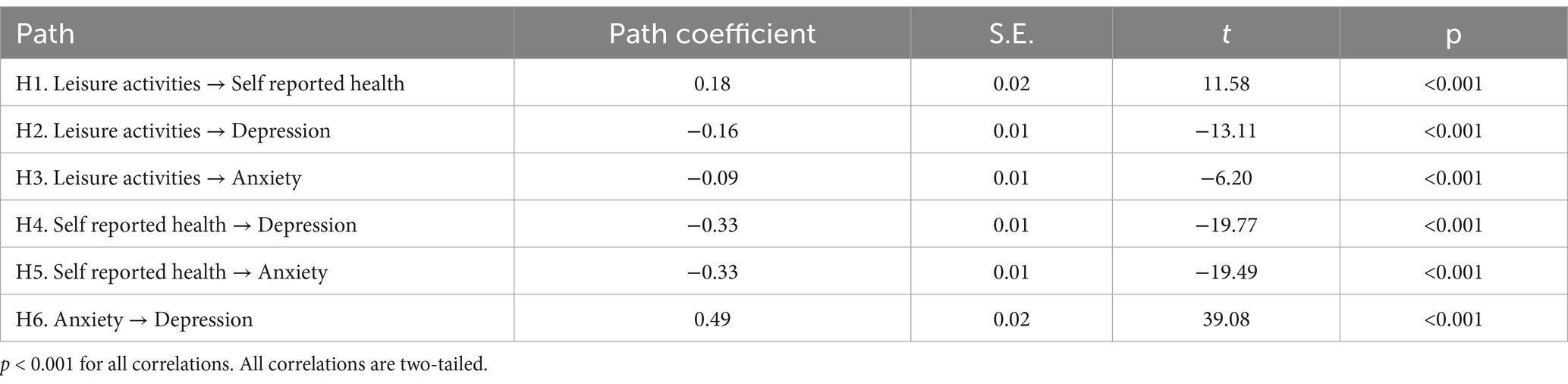
All hypothesized direct paths were significant (Table 4). Specifically:
Leisure activities positively predicted self-reported health (β = 0.18, SE = 0.02, t = 11.58, p < 0.001), supporting H1.
Leisure activities negatively predicted depression (β = −0.16, SE = 0.01, t = −13.11, p < 0.001), supporting H2.
Leisure activities negatively predicted anxiety (β = −0.09, SE = 0.01, t = −6.20, p < 0.001), supporting H3.
Self-reported health negatively predicted depression (β = −0.33, SE = 0.01, t = −19.77, p < 0.001) and anxiety (β = −0.33, SE = 0.01, t = −19.49, p < 0.001), supporting H4 and H5.
Anxiety positively predicted depression (β = 0.49, SE = 0.02, t = 39.08, p < 0.001), supporting H6.
Table 4
Table 4. Results of structural model testing.
3.5 Indirect effects and mediation analysis
Indirect effects were tested using the bias-corrected bootstrap method with 5,000 resamples. The results revealed that self-reported health and anxiety significantly mediated the relationship between leisure activities and depression, supporting H7 (Table 5).
Table 5
Table 5. Results of indirect effects of self-reported health and anxiety on depression.
The indirect effect of leisure activities on depression via self-reported health was β = −0.06.
The indirect effect via anxiety was β = −0.04.
The serial mediation effect through both self-reported health and anxiety was β = −0.03.
4 Discussion
This study supports the proposed model that elucidates the interrelationships among leisure activities, SRH, anxiety, and depression among older adults in China. Specifically, leisure activities significantly enhanced SRH while reducing depression and anxiety. SRH contributed to the reduction of depression and anxiety, and anxiety had a direct positive impact on depression. Additionally, this study demonstrated that SRH and anxiety play partial and serial mediating roles in the relationship between leisure activities and depression.
The results for Hypothesis H1 revealed a positive relationship between leisure activities and SRH among older adults in China, extending previous literature related to older adults in other countries (15). H1 suggests that participants who reported higher levels of leisure activities were likely to have better SRH. As WHO and the International Society for Physical Activity and Health have pointed out, regular activity is essential for good mental health (60). Participation in leisure activities among older adults can effectively address their mental health issues (50) and thus improve SRH. Leisure activities can also indirectly enhance SRH by improving social support and interpersonal relationships (61).
The results for Hypotheses H2 and H3 demonstrated a negative relationship between leisure activities and depression/anxiety among older adults in China, consistent with previous studies (21). This finding can be explained by the fact that increased frequency of participation in leisure activities, such as playing cards/mahjong and watching/listening to TV/radio, is particularly important for reducing risk factors like social isolation among older adults and is associated with a lower risk of cognitive impairment (62) and lesser feelings of loneliness (63). Engaging in leisure activities helps older adults find hobbies and release psychological pressure, thereby reducing anxiety and depression (50).
In the study, we further confirmed that SRH was negatively associated with depressive and anxious symptoms among older adults in China (H4 and H5), which was consistent with previous analyses conducted in Western countries indicating that SRH was negatively associated with depression/anxiety among older adults (31). A study (64) participants reporting poor or fair self-rated health had greater odds of chronic illness, major depressive syndrome, and lower socioeconomic status than those reporting good to excellent self-rated health. Similarly, another study (65) revealed that SRH was a valid measure of physiological and mental health. These findings highlight the critical role of SRH as both an indicator and predictor of mental health outcomes, particularly in older populations.
The positive relationship between anxiety and depression (H6) among older adults in China was consistent with previous studies (66), indicating that coexisting anxiety and depression are common in the Chinese population. Epidemiological research has also shown that almost half of all people with depression also have comorbid anxiety (39).
Our findings empirically support the hypothesis that the indirect effect of leisure activities on depression among Chinese older adults can be mediated by SRH and anxiety (H7). Leisure activities can improve health, and older adults with rich leisure activities are more likely to report better health, which in turn alleviates their anxiety and depression. The findings of this study enrich our understanding of the relationship between leisure activities and depression and provide a basis for policy interventions. On one hand, SRH is a predictor of anxiety and depression, as indicated by previous studies (29). When SRH worsens, it is crucial to intervene to prevent anxiety and depression. On the other hand, anxiety serves as a mediator not only between leisure activities and depression but also between SRH and depression. Anxiety has been found to be a burdensome mental health issue and is often accompanied by emotional irritation, frequent anger, sleep disorders, muscle pain, and other symptoms (67). Among older adults, anxiety can lead to cognitive impairment (68), a decline in subjective well-being (69), and lower life satisfaction (70). Policy interventions targeting depression should place greater emphasis on alleviating anxiety.
5 Strengths and limitations
This study has several notable strengths. Firstly, it utilizes a large and representative sample from China, enhancing the generalizability of the findings and providing valuable references for similar research in other countries. Secondly, the study not only explores the direct relationship between leisure activities and depression among older adults but also analyzes the mediating roles of SRH and anxiety. This multi-faceted approach enriches our understanding of the complex interactions among these variables. Additionally, the CES-D-10 and GAD-7 scales used in this study have been validated among Chinese older adults, ensuring the reliability and validity of the measurement tools.
However, there are some limitations to this study. Firstly, the assessment of depression and anxiety symptoms relied on the CES-D-10 and GAD-7 scales rather than clinical diagnostic criteria. Although these scales are validated, they may not fully capture professional clinical diagnoses. Secondly, the use of self-report questionnaires may introduce recall bias and subjective perception issues, potentially affecting the accuracy of the data. Lastly, the cross-sectional design of this study limits the ability to infer causality between the variables. Longitudinal studies are needed in the future to establish causal relationships and examine the temporal dynamics of these associations.
6 Conclusion
This study, based on data from the CLHLS, used structural equation modeling to reveal the relationships among leisure activities, SRH, anxiety, and depression in older adults in China. The findings indicate that leisure activities not only directly improve SRH and alleviate anxiety and depression but also exert indirect and serial mediation effects through SRH and anxiety. SRH emerged as a key indicator of mental health, playing an important role in preventing anxiety and depression, while anxiety significantly increased the risk of depression.
Theoretically, this study expands the research framework on mental health in older adults by confirming that the positive effects of leisure activities also apply in the Chinese context. It is the first to clearly identify the mediating roles of SRH and anxiety in these relationships. Practically, the findings provide valuable recommendations for governments, communities, and healthcare institutions: promoting leisure activities such as gardening, reading, and social engagement can effectively enhance subjective health and psychological well-being among older adults, reducing the incidence of depression and anxiety. Support and encouragement from family members and caregivers also play a critical role in facilitating participation.
Overall, this study highlights the importance of leisure activities as a strategic approach to promoting mental health in older adults. It calls for collaborative efforts across sectors to address the mental health challenges posed by China’s rapidly aging population, offering both scientific evidence and practical solutions.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the [patients/participants OR patients/participants legal guardian/next of kin] was not required to participate in this study in accordance with the national legislation and the institutional requirements.
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. World mental health report 2022. Geneva: World Health Organization (2022).
3. World Health Organization. COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide World Health Organization (2022).
4. World Health Organization. (2017). Depression and other common mental disorders: global health estimates. Geneva: World Health Organization. Available online at: https://iris.who.int/handle/10665/254610 (Accessed June 20, 2024).
6. Yen, HY, and Lin, LJ. Quality of life in older adults: benefits from the productive engagement in physical activity. J Exercise Sci Fitness. (2018) 16:49–54. doi: 10.1016/j.jesf.2018.06.001
7. Yang, X, Xu, X, Guo, L, Zhang, Y, Wang, S, and Li, Y. Effect of leisure activities on cognitive aging in older adults: a systematic review and meta-analysis. Front Psychol. (2022) 13:1080740. doi: 10.3389/fpsyg.2022.1080740
8. Sala, G, Jopp, D, Gobet, F, Ogawa, M, Ishioka, Y, Masui, Y, et al. The impact of leisure activities on older adults' cognitive function, physical function, and mental health. PLoS One. (2019) 14:e0225006. doi: 10.1371/journal.pone.0225006
9. Zhao, X, Yu, J, and Liu, N. Relationship between specific leisure activities and successful aging among older adults. J Exerc Sci Fit. (2023) 21:111–8. doi: 10.1016/j.jesf.2022.11.006
10. Jeong, EH, and Park, JH. The relationship among leisure activities, depression and quality of life in community-dwelling elderly Koreans. Gerontol Geriatric Med. (2020) 6:2333721420923449. doi: 10.1177/2333721420923449
11. Dupuis, SL, and Smale, BJA. An examination of relationship between psychological Well-being and depression and leisure activity participation among older adults. Loisir et Société/Society and Leisure. (1995) 18:67–92. doi: 10.1080/07053436.1995.10715491
12. Kobayashi, T, Tani, Y, Kino, S, Fujiwara, T, Kondo, K, and Kawachi, I. Prospective study of engagement in leisure activities and all-cause mortality among older Japanese adults. J Epidemiol. (2022) 32:245–53. doi: 10.2188/jea.JE20200427
13. Li, ZH, Zhang, XR, Lv, YB, Shen, D, Li, FR, Zhong, WF, et al. Leisure activities and all-cause mortality among the Chinese oldest-old population: a prospective community-based cohort study. J Am Med Dir Assoc. (2020) 21:713–719.e2. doi: 10.1016/j.jamda.2019.08.003
14. Guerrero Barragán, A, Lucumí, D, and Lawlor, B. Association of leisure activities with cognitive impairment and dementia in older adults in Colombia: a SABE-based study. Front Neurol. (2021) 12:629251. doi: 10.3389/fneur.2021.629251
15. Lin, SC, Tyus, N, Maloney, M, Ohri, B, and Sripipatana, A. Mental health status among women of reproductive age from underserved communities in the United States and the associations between depression and physical health. PLoS One. (2020) 15:e0231243. doi: 10.1371/journal.pone.0231243
16. Bone, JK, Bu, F, Fluharty, ME, Paul, E, Sonke, JK, and Fancourt, D. Engagement in leisure activities and depression in older adults in the United States: longitudinal evidence from the health and retirement study. Soc Sci Med. (2022) 294:114703. doi: 10.1016/j.socscimed.2022.114703
17. Fancourt, D, and Tymoszuk, U. Cultural engagement and incident depression in older adults: evidence from the English longitudinal study of ageing. Br J Psychiatry. (2019) 214:225–9. doi: 10.1192/bjp.2018.267
18. Dale, LP, Vanderloo, L, Moore, S, and Faulkner, G. Physical activity and depression, anxiety, and self-esteem in children and youth: An umbrella systematic review. Ment Health Phys Act. (2019) 16:66–79. doi: 10.1016/j.mhpa.2018.12.001
19. McDowell, CP, Dishman, RK, Vancampfort, D, Hallgren, M, Stubbs, B, Mac Donncha, C, et al. Physical activity and generalized anxiety disorder: results from the Irish longitudinal study on ageing (TILDA). Int J Epidemiol. (2018) 47:1443–53. doi: 10.1093/ije/dyy141
20. Wanjau, MN, Möller, H, Haigh, F, Milat, A, Hayek, R, Lucas, P, et al. Physical activity and depression and anxiety disorders: a systematic review of reviews and assessment of causality. AJPM Focus. (2023) 2:100074. doi: 10.1016/j.focus.2023.100074
21. Kim, EC, Jeong, A, Lee, DH, Park, DH, and Jeon, JY. Impact of leisure physical activity and resistance exercise on the prevalence of depressive symptoms in Korean adults: analysis of the Korean National Health and nutrition examination survey. J Affect Disord. (2024) 356:329–37. doi: 10.1016/j.jad.2024.04.028
22. Mammen, G, and Faulkner, G. Physical activity and the prevention of depression: a systematic review of prospective studies. Am J Prev Med. (2013) 45:649–57. doi: 10.1016/j.amepre.2013.08.001
25. Belvederi Murri, M, Ekkekakis, P, Magagnoli, M, Zampogna, D, Cattedra, S, Capobianco, L, et al. Physical exercise in major depression: reducing the mortality gap while improving clinical outcomes. Front Psych. (2019) 9:762. doi: 10.3389/fpsyt.2018.00762
26. Stanojević Jerković, O, Sauliūnė, S, Šumskas, L, Birt, CA, and Kersnik, J. Determinants of self-rated health in elderly populations in urban areas in Slovenia, Lithuania, and UK: findings of the EURO-URHIS 2 survey. Eur J Public Health. (2017) 27:74–9. doi: 10.1093/eurpub/ckv097
27. Lorem, G, Cook, S, Leon, DA, Emaus, N, and Schirmer, H. Self-reported health as a predictor of mortality: A cohort study of its relation to other health measurements and observation time. Scientific Reports. (2020) 10:4886. doi: 10.1038/s41598-020-61603-0
28. Choi, YH. Is subjective health reliable as a proxy variable for true health? A comparison of self-rated health and self-assessed change in health among middle-aged and older south Koreans. Health Soc Welfare Rev. (2016) 36:431–59. doi: 10.15709/hswr.2016.36.4.431
29. Kim, Y, and Jang, E. Low self-rated health as a risk factor for depression in South Korea: a survey of young males and females. Healthcare. (2021) 9:452. doi: 10.3390/healthcare9040452
30. Vaez, M, Kristenson, M, and Laflamme, L. Perceived quality of life and self-rated health among first-year university students. Soc Indic Res. (2004) 68:221–34. doi: 10.1023/B:SOCI.0000025594.76886.56
31. Badawi, G, Pagé, V, Smith, KJ, Gariépy, G, Malla, A, Wang, J, et al. Self-rated health: a predictor for the three-year incidence of major depression in individuals with type II diabetes. J Affect Disord. (2013) 145:100–5. doi: 10.1016/j.jad.2012.07.018
33. Shen, R, and Zou, T. The association between cardiovascular health and depression: results from the 2007-2020 NHANES. Psychiatry Res. (2024) 331:115663. doi: 10.1016/j.psychres.2023.115663
34. Vaingankar, JA, Chong, SA, Abdin, E, Kumar, FDS, Chua, BY, Sambasivam, R, et al. Understanding the relationships between mental disorders, self-reported health outcomes and positive mental health: findings from a national survey. Health Qual Life Outcomes. (2020) 18:55. doi: 10.1186/s12955-020-01308-0
35. Wilmer, MT, Anderson, K, and Reynolds, M. Correlates of quality of life in anxiety disorders: review of recent research. Curr Psychiatry Rep. (2021) 23:77. doi: 10.1007/s11920-021-01290-4
36. Kato, T. Coping with interpersonal stress and psychological distress at work: comparison of hospital nursing staff and salespeople. Psychol Res Behav Manag. (2015) 8:31–9. doi: 10.2147/PRBM.S57030
37. Lin, L, He, P, Ouyang, W, Qiu, X, Qiu, S, and Chen, J. The mediating effect of self-rated health and life satisfaction on the relationship between impaired daily living activities and depressive symptoms in older adults and latent profile analysis. China Med Herald. (2024) 21:110–5. doi: 10.20047/j.issn1673-7210.2024.23.22
38. An, S, Yuan, J, Chen, T, Yao, N, and Wang, S. The mediating effect of self-rated health on the relationship between self-care ability and depressive symptoms in older adults. J Nurs. (2022) 29:55–9. doi: 10.16460/j.issn1008-9969.2022.20.055
39. Lamers, F, van Oppen, P, Comijs, HC, Smit, JH, Spinhoven, P, Balkom, v, et al. Comorbidity patterns of anxiety and depressive disorders in a large cohort study: the Netherlands study of depression and anxiety (NESDA). J Clin Psychiatry. (2011) 72:341–8. doi: 10.4088/JCP.10m06176blu
41. Neumann, A, Nolte, IM, and Kaprio, J. Stress-related exposures amplify the effects of genetic susceptibility to depression and anxiety. Transl Psychiatry. (2021) 13:1–10. doi: 10.1038/s41398-023-02327-3
42. Beesdo, K, Pine, DS, Lieb, R, and Wittchen, HU. Incidence of social anxiety disorder and the consistent risk for secondary depression in the first three decades of life. Arch Gen Psychiatry. (2010) 68:12–20. doi: 10.1001/archpsyc.64.8.903
43. Jacobson, NC, and Newman, MG. Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol Bull. (2017) 143:1155–200. doi: 10.1037/bul0000111
45. Yi, Z. Reliability of age reporting among the Chinese oldest-old in the CLHLS datasets In: Healthy longevity in China: Demographic, socioeconomic, and psychological dimensions. Dordrecht: Springer (2008). 61–78. doi: 10.1007/978-1-4020-6752-5_4
46. Yue, Z, Liang, H, Gao, X, Qin, X, Li, H, Xiang, N, et al. The association between falls and anxiety among elderly Chinese individuals: the mediating roles of functional ability and social participation. J Affect Disord. (2022) 301:300–6. doi: 10.1016/j.jad.2022.01.070
47. Zeng, Y, Feng, Q, Hesketh, T, Christensen, K, and Vaupel, JW. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. (2017) 389:1619–29. doi: 10.1016/S0140-6736(17)30548-2
48. Chen, ZT, Wang, XM, Zhong, YS, Zhong, WF, Song, WQ, and Wu, XB. Association of changes in waist circumference, waist-to-height ratio and weight-adjusted-waist index with multimorbidity among older Chinese adults: results from the Chinese longitudinal healthy longevity survey (CLHLS). BMC Public Health. (2024) 24:318. doi: 10.1186/s12889-024-17846-x
50. Li, W, Sun, H, Xu, W, Ma, W, Yuan, X, Wu, H, et al. Leisure activity and cognitive function among Chinese old adults: the multiple mediation effect of anxiety and loneliness. J Affect Disord. (2021) 294:137–42. doi: 10.1016/j.jad.2021.07.051
51. Zhao, W, Zhang, Y, Liu, X, Yue, J, Hou, L, Xia, X, et al. Comorbid depressive and anxiety symptoms and frailty among older adults: findings from the West China health and aging trend study. J Affect Disord. (2020) 277:970–6. doi: 10.1016/j.jad.2020.08.070
52. Löwe, B, Decker, O, Müller, S, Brähler, E, Schellberg, D, Herzog, W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
53. Chen, H, and Mui, AC. Factorial validity of the Center for Epidemiologic Studies Depression Scale short form in older population in China. Int Psychogeriatr. (2014) 26:49–57. doi: 10.1017/S1041610213001701
54. Zinan, W, and Sai, GTB. Students’ perceptions of their ICT-based college English course in China: a case study. Teach English Technol. (2017) 17:53–76. Available at: https://www.researchgate.net/publication/318925995
56. Hu, LT, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
60. ISPAH International Society for Physical Activity and Health. The Bangkok declaration on physical activity for Global Health and Sustainable Development. Br J Sports Med. (2017) 51:1389–1391. doi: 10.1136/bjsports-2017-098063
61. Umberson, D, and Montez, JK. Social relationships and health: a flashpoint for health policy. J Health Soc Behav. (2010) 51:S54–66. doi: 10.1177/0022146510383501
62. Xu, M, Zhou, Y, Yan, Q, Ke, P, Yin, X, and Gong, Y. Engagement in leisure activities and cognitive function by socioeconomic groups in China: a prospective cohort study. J Affect Disord. (2023) 327:362–7. doi: 10.1016/j.jad.2023.02.026
63. Teh, JK, and Tey, NP. Effects of selected leisure activities on preventing loneliness among older Chinese. SSM Popul Health. (2019) 9:100479:100479. doi: 10.1016/j.ssmph.2019.100479
64. Ambresin, G, Chondros, P, Dowrick, C, Herrman, H, and Gunn, JM. Self-rated health and long-term prognosis of depression. Annals of Family Medicine. (2014) 12:57–65. doi: 10.1370/afm.1562
65. Hamplová, D, Klusáček, J, and Mráček, T. Assessment of self-rated health: The relative importance of physiological, mental, and socioeconomic factors. PLoS One. (2022) 17:e0267115. doi: 10.1371/journal.pone.0267115
66. Zhan, ZJ, Huang, HY, Xiao, YH, Zhao, YP, Cao, X, Cai, ZC, et al. Anxiety and depression in nasopharyngeal carcinoma patients and network analysis to identify central symptoms: a cross-sectional study from a high-incidence area. Radiother Oncol. (2024) 197:110324. doi: 10.1016/j.radonc.2024.110324
67. Xu, WQ, Lin, LH, Ding, KR, Ke, YF, Huang, JH, Hou, CL, et al. The role of depression and anxiety in the relationship between poor sleep quality and subjective cognitive decline in Chinese elderly: exploring parallel, serial, and moderated mediation. J Affect Disord. (2021) 294:464–71. doi: 10.1016/j.jad.2021.07.063
68. Divers, R, Robinson, A, Miller, L, De Vito, AN, Pugh, E, and Calamia, M. Beyond depression: examining the role of anxiety and anxiety sensitivity on subjective cognition and functioning in older adults. Aging Ment Health. (2022) 26:2300–6. doi: 10.1080/13607863.2021.1966747
69. Malone, C, and Wachholtz, A. The relationship of anxiety and depression to subjective well-being in a mainland Chinese sample. J Relig Health. (2018) 57:266–78. doi: 10.1007/s10943-017-0447-4
70. Taghiabadi, M, Kavosi, A, Mirhafez, SR, Keshvari, M, and Mehrabi, T. The association between death anxiety with spiritual experiences and life satisfaction in elderly people. Electron Physician. (2017) 9:3980–5. doi: 10.19082/3980
Keywords: leisure activities, self-reported health, anxiety, depression, Chinese older adults
Citation: Song K, Chang Y, Zhao Z and Govindasamy K (2025) Leisure activities, self-reported health, anxiety, and depression in Chinese older adults: a structural equation model analysis. Front. Public Health. 13:1459236. doi: 10.3389/fpubh.2025.1459236
Received: 04 July 2024; Accepted: 11 April 2025; Published: 09 May 2025.
Edited by:
Wing Fai Yeung, Hong Kong Polytechnic University, Hong Kong SAR, China
Reviewed by:
Raman Mishra, University College London, United Kingdom Zhihao Du, China University of Mining and Technology, China
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
 Keying Song
Keying Song Yawen Chang2*
Yawen Chang2* Zijian Zhao
Zijian Zhao Karuppasamy Govindasamy
Karuppasamy Govindasamy