 Bushra Ali
Bushra Ali Tim Evans
Tim Evans Rhonda Cohen
Rhonda Cohen Anne Elliott
Anne Elliott- 1Department Science and Technology, London Sports Institute, Middlesex University London, London, United Kingdom
- 2Business and Political Economy, Middlesex University London, London, United Kingdom
The United Arab Emirates is experiencing a rising burden of non-communicable diseases, particularly metabolic syndrome (MetS), driven by rapid urbanization and lifestyle changes. In Dubai's diverse population, where expatriates constitute 85% of residents, understanding perspectives on physical activity (PA) is essential for effective prevention strategies. This qualitative study explored stakeholder experiences and views on PA as a preventive measure for MetS. Semi-structured interviews were conducted with 20 stakeholders, including policy officials, gym owners, trainers, gym members, and inactive individuals, recruited through purposive and snowball sampling. Data were analyzed using thematic analysis and Hofstede's cultural framework to examine cultural influences on PA behaviors. Results indicated broad recognition of PA's importance in managing MetS but identified significant cultural and environmental barriers to participation. Key themes included cultural perceptions shaping engagement with PA and infrastructure challenges. These findings highlight the need for culturally tailored interventions and multisectoral collaboration to promote active lifestyles in Dubai's multi-ethnic context. This research offers valuable insights to guide public health initiatives aiming to reduce the burden of MetS through culturally sensitive approaches suited to this unique urban environment.
Background
Physical inactivity is formally defined as the failure to engage in a level of PA that is sufficient to meet the established public health guidelines. These guidelines specify a range of 150–300 min of moderate to vigorous PA, or 75–150 min of vigorous PA, or an equivalent combination of moderate-to-vigorous PA ((1)). It serves as a significant risk factor for developing multiple health conditions, including obesity, cardiovascular disease, diabetes, and musculoskeletal disorders. This phenomenon adversely affects metabolic function by reducing basal metabolic rate, promoting muscle atrophy, and impairing insulin sensitivity. These metabolic disruptions trigger adaptive responses whereby the body compensates for reduced PA through systematic metabolic adjustments. The resulting adaptation is characterized by elevated insulin and leptin secretion, diminished energy expenditure, and compromised insulin-mediated glucose regulation, establishing a pathophysiological cascade that may progress to MetS (2).
MetS is diagnosed when an individual has at least three of the following five criteria (3):
° Elevated waist circumference (For the Middle East*: men ≥ 94 cm, women ≥ 80 cm).
° Elevated triglycerides: ≥150 mg/dL (1.7 mmol/L), or specific treatment for this lipid abnormality.
° Reduced high-density lipoprotein (HDL) cholesterol: < 40 mg/dL (1.03 mmol/L) in men, < 50 mg/dL (1.29 mmol/L) in women, or specific treatment for this lipid abnormality.
° Elevated blood pressure: systolic ≥130 and/or diastolic ≥85 mm Hg, or treatment of previously diagnosed hypertension.
° Elevated fasting glucose: ≥100 mg/dL (5.6 mmol/L), or previously diagnosed type 2 diabetes.
*The International Diabetes Federation (IDF) provides waist circumference recommendations for MetS, which are uniform for women globally due to the limited availability of robust data. However, these recommendations differ slightly for men of European descent (Europids) compared to those of Asian descent. The classification of levels for Asian populations is derived from the recommendations provided by the WHO. Limited data is currently accessible for other regions; nevertheless, until new data becomes available, recommendations for Europid males are being applied to men from the Middle East, Eastern Mediterranean region, and Sub-Saharan Africa (4). This regional adaptation of diagnostic criteria is particularly relevant given that a systematic review by Mahmoud and Sulaiman (5) highlights that the high prevalence of MetS in the UAE has become a significant concern, primarily because of its association with premature mortality from NCDs. The potential mechanism that contributes to the development of these diseases is the high occurrence of physical inactivity (6).
In the pre-oil era, the inhabitants of the UAE typically led active and diversified lifestyles adapted to the region's geographical and climatic conditions. These lifestyles were characterized by activities such as trade, fishing, pearling, nomadic herding, agriculture, and traditional crafts (7). Many of these tasks were often performed manually or with the help of basic tools, which would require more physical effort compared to modern, mechanized methods. Nonetheless, over the last several decades there has been a significant improvement in living conditions and a rise in the usage of primarily mechanized technology, which has spread to all segments of Dubai's population. From this point on, a noticeable increase was discerned toward sedentary lifestyles and diminished levels of PA within the populace (8). While Dubai's development has brought about significant improvements in overall health and wellbeing, evidenced by increased life expectancy and reduced infant and maternal mortality rates, it has also given rise to new health challenges. The rapid urbanization and lifestyle changes associated with economic growth have led to an increase in obesity and NCDs, resulting in a rise in years lived with disability (YLDs) (9). The government of Dubai has shown a firm dedication to public health, led by Crown Prince HH Sheik Hamdan Bin Mohammad bin Rashid Al Maktoum, who is driving an ambitious effort to establish Dubai as a worldwide frontrunner in fitness and wellbeing (10). This forward-thinking strategy demonstrates the emirate's commitment to improving the wellbeing of its citizens and establishing new standards for promoting urban health.
This study is motivated by the evolving health landscape in the UAE, particularly regarding MetS, and recognizes the opportunity for customized PA initiatives that resonate with Dubai's multicultural population. Dubai's selection as the research focus aligns with its renowned openness to innovation and ongoing dedication to promoting active lifestyles. As a forward-thinking urban center, Dubai is uniquely positioned to potentially inspire and inform public health strategies, not only within the UAE but possibly across the broader Arab region, showcasing the potential of culturally attuned health promotion in diverse urban environments.
Aims and objectives
Aims
To explore stakeholders' perceptions of PA for the prevention and management of MetS, with a focus on identifying barriers, cultural influences, motivators, and opportunities for enhancing PA engagement.
Objectives
• To examine the perceptions and experiences of stakeholders (from policy developers to end-users) regarding PA for MetS prevention and management.
• To identify key barriers, cultural influences, and motivators affecting PA engagement among stakeholders.
• To explore opportunities and strategies suggested by stakeholders for improving PA engagement and MetS prevention in the future.
• To assess stakeholders' priorities and aspirations for enhancing PA participation in the context of MetS.
Methods
Theoretical framework
Interpretivism underpins this study, focusing on how individuals construct meaning through social interactions (11). This paradigm is particularly relevant for exploring perspectives on PA, as these are shaped by shared assumptions and collective experiences that reveal the motivations and processes behind organizational and individual actions (12). The ontological stance is constructivist, positing that reality is not fixed but is continually created through social relationships; as Walker et al. (13) note, truth is found in social spaces and interactions. Consequently, the research question is grounded in the socially constructed views of individuals, and understanding these multiple perspectives is key to generating knowledge from a constructivist viewpoint. This interpretivist-constructivist approach is particularly suited to multicultural contexts such as Dubai, where diverse social realities must be explored to understand the PA landscape.
This study employs Stakeholder Theory as its conceptual foundation, defining stakeholders as individuals or groups affected by, interested in, or able to influence PA interventions (14, 15). Stakeholder Analysis serves as the primary qualitative methodology, systematically identifying, categorizing, and prioritizing stakeholders based on their interests, influence, and potential impact (16). This approach uniquely examines data both within and across stakeholder groups, revealing group-specific and overarching themes that capture the complexity of stakeholder perspectives in PA initiatives. Stakeholder engagement throughout the research process is essential for integrating evidence into interventions, enhancing their relevance, sustainability, transparency, and community ownership (17).
Data are collected through semi-structured interviews, a method well-suited to interpretivist research as it acknowledges the collaborative and co-constructive nature of knowledge production between researchers and participants (11). This approach allows for in-depth exploration of stakeholder experiences, needs, and motivations, providing actionable insights for the design and delivery of effective, contextually relevant PA interventions.
Sample
Stakeholders were organized into six defined “levels” based on their functional roles within the PA ecosystem. These levels were then mapped onto the Power–Interest Matrix according to their relative influence (power) and engagement (interest) in the project. The classification was as follows:
• Level 1: Senior Policy Officials—High Power, Low Interest
• Level 2: Gym Owners—High Power, High Interest
• Level 3: Gym Managers—Moderate Power, High Interest
• Level 4: Personal Trainers—Low Power, High Interest
• Level 5: Active Individuals/Gym Members—Low Power, Moderate Interest
• Level 6: Inactive Individuals—Low Power, Low Interest
Active individuals (Level 5) were defined as those self-reporting at least 150 min of moderate physical activity per week, aligning with WHO guidelines. Inactive individuals (Level 6) reported less or no regular activity. Classification occurred during initial screening interviews.
These levels were then mapped onto the Power–Interest Matrix according to their relative influence (power) and engagement (interest) in the project, as illustrated in Figure 1.

Figure 1. Mapping stakeholders in Dubai: power interest index.
This approach enabled strategic stakeholder mapping by aligning levels with engagement priorities. Stakeholder placement was informed by their role in decision-making, resource control, programme implementation, or behavioral impact. The classification supported tailored engagement strategies and effective allocation of communication efforts.
To ensure comprehensive representation across these stakeholder levels—ranging from senior policymakers to inactive individuals—a purposive sampling strategy was employed, supplemented by snowball and convenience sampling techniques. Initial participants were drawn from the fitness industry contacts known to the researcher, followed by targeted recruitment. The study adopted a broad definition of PA, encompassing exercise in gyms, fitness centers, sports clubs, homes, and outdoor environments, with recognition of Dubai's climate favoring indoor, climate-controlled settings.
According to Patton (18), determining sample size in qualitative research is guided by the study's aims, the depth of understanding sought, and practical considerations such as available resources and the richness of the data collected. In line with Sandelowski (19) and Vasileiou et al. (20), the sample was kept small to allow for in-depth, case-focused analysis. Malterud et al.'s (21) concept of “information power” informed the decision to recruit 2 to 4 participants per stakeholder group, as the focused research aim, and specificity of participants were expected to yield sufficiently rich data. The final sample included 20 participants (10 males and 10 females), aged 32 to 58, all Dubai residents. Gatekeeper approval was obtained for interviews with senior policy officials.
To reflect Dubai's multiethnic demographic, participants were selected from diverse nationalities, including Serbia, Iraq, the UK, the Philippines, Portugal, Azerbaijan, India, Pakistan, Canada, Syria, and Sri Lanka. A detailed summary of participant characteristics is provided in Appendix B.
Participants were selected based on their affiliation with chosen stakeholder groups and were Dubai residents. When approached, a total of 31 individuals responded and inquired about further details. They received participant information sheets (PIS) and consent forms via email, 20 of them agreed to go ahead with the interview, 2 individuals provided delayed responses, while the remaining recipients did not respond.
Ethics
The researcher obtained informed consent from interviewees and recorded verbal consent from those who could not provide a written form. The London Sport Institute Middlesex University Ethics Sub-committee, and the Middlesex University Dubai, Research Committee approved the research. Stakeholder analysis involves ethical and practical issues like confidentiality. To ensure anonymity, identities were substituted with pseudonyms throughout the analysis. A significant challenge during semi-structured interviews was ensuring the neutrality of questions, especially when addressing spontaneous or unscripted follow-ups. To maintain research quality, researchers must craft questions carefully and be aware of potential sources of bias (22). The interview preparation aligned with Gubrium et al. (23) guidelines, emphasizing building trust, formulating insightful inquiries, and creating a supportive atmosphere.
The author's extensive 20-year residency and professional experience in the UAE, combined with cultural origins in the Arab world, provided insider perspective essential for understanding local PA practices and institutional dynamics. This positioning facilitated participant access and trust-building while enabling culturally informed data interpretation. To address potential insider bias, systematic reflexivity measures were implemented, including research journaling, peer debriefing sessions, and participant validation of findings, thereby strengthening the study's credibility and analytical rigor (24).
Data collection
Semi-structured interviews (25) were conducted both face-to-face and online at participants' residences or workplaces, with each session lasting between 30 and 60 min. Most interviews took place online, offering greater scheduling flexibility and accommodating participants' availability. The interviews explored various aspects of PA interventions, including factors that facilitate or hinder engagement, common health concerns, and strategies for addressing cultural influences on health behaviors and lifestyle choices. The semi-structured format allowed the interviewer to tailor questions to each participant's background and context, ensuring relevance and depth in every conversation. This flexibility enabled the interviewer to prioritize prompts according to participants' lived experiences and roles, thereby enriching the quality of the data collected. At the same time, the approach maintained a consistent framework across interviews, allowing for systematic exploration of emerging themes.
Interview guide development
The interview guide was constructed by first reviewing the study's theoretical framework and relevant literature on PA promotion and MetS. Questions were designed to elicit detailed responses about experiences, opinions, and strategies, in line with the study's qualitative approach. The draft interview guide was piloted with two volunteers unaffiliated with the final study group. Feedback was gathered regarding clarity, comprehensiveness, and relevance. Based on this input, as well as comments from supervisors and a qualitative research expert, the guide was revised to enhance its clarity and ensure comprehensive coverage of all intended themes. The final version was approved for face validity before interviews commenced.
The full set of interview prompts and questions used in this study is provided in Appendix A for reference.
Data analysis
The qualitative data were analyzed using a multi-layered stakeholder analysis framework, which comprised horizontal analysis (within-group thematic analysis), vertical analysis (cross-group comparative analysis), and cultural content analysis using Hofstede's Cultural Dimensions (26). This framework enabled a systematic and nuanced exploration of stakeholder perspectives and cultural influences on PA participation in Dubai (see Figure 2).
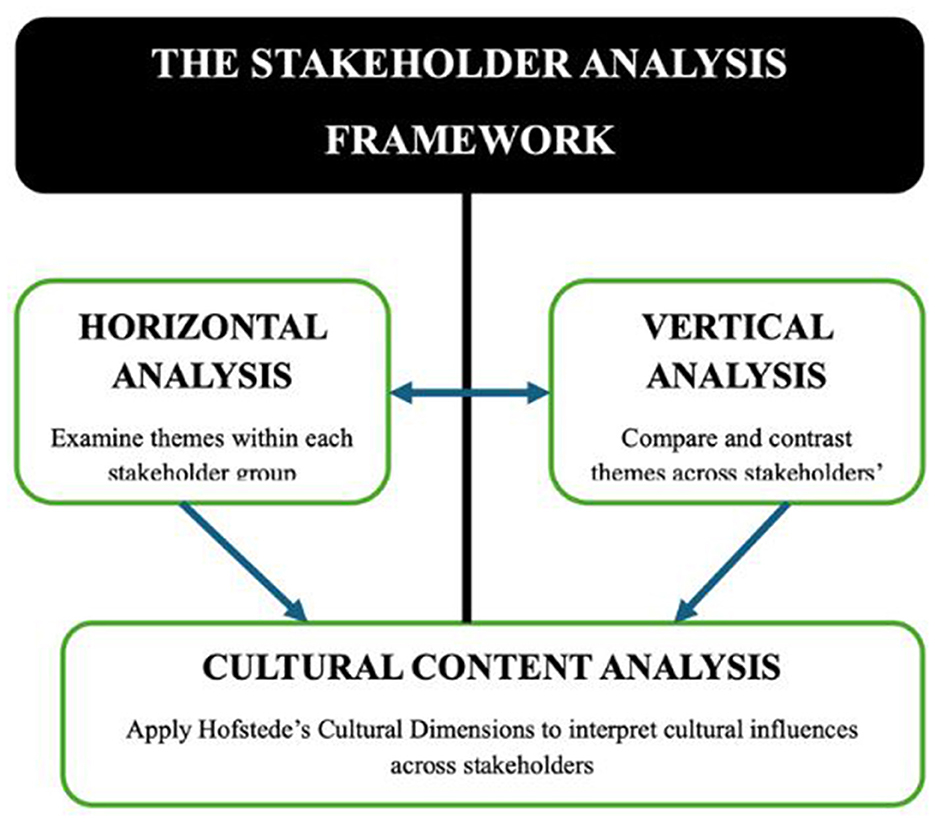
Figure 2. ) The stakeholder analysis framework. A schematic overview of the three-layered analytic approach: horizontal analysis (within-group), vertical analysis (cross-group), and cultural content analysis using Hofstede's dimensions.
Data preparation and coding
Audio recordings were transcribed verbatim and anonymized. Initial coding involved manual identification of relevant passages and documentation of potential themes and categories. Subsequently, NVivo 12 (QSR International, Burlington, MA, USA) was used to facilitate electronic coding, organization, and retrieval of data. Both open (inductive) and hierarchical (deductive) coding approaches were applied, allowing for the emergence of new themes while also categorizing data according to stakeholder levels. All interviews, regardless of the specific prompts used, were thematically analyzed against the full set of research questions to maintain analytic consistency and comparability across participants.
Horizontal analysis (within-group thematic analysis)
A preliminary horizontal analysis was conducted to identify recurring themes, patterns, and shared characteristics among stakeholders within the same group. This process enabled the recognition of experiences and attitudes unique to each stakeholder category.
Vertical analysis (cross-group comparative analysis)
Following horizontal analysis, a vertical analysis was performed to examine variations in themes and perspectives across different levels of the stakeholder hierarchy. This involved comparing codes and themes across groups, from senior policy officials to inactive individuals, to reveal how organizational roles and positions influenced attitudes and behaviors related to PA. Hierarchical coding in NVivo supported this process, and themes were continuously refined through team discussions.
Cultural content analysis
To assess cultural influences within Dubai's multi-ethnic population, a targeted content analysis was conducted using Hofstede's Cultural Dimensions Framework (26). Themes and codes related to cultural values, norms, and behaviors were mapped to established dimensions such as individualism vs. collectivism and power distance. This facilitated cross-cultural comparisons and provided deeper insight into how cultural context shapes stakeholder perspectives on PA. The use of Hofstede's framework aligns with its application in workplace wellness and global health initiatives, supporting the development of culturally tailored interventions.
Integration of analytical methodologies
The integration of manual and electronic coding, horizontal and vertical analyses, and cultural content analysis enabled a thorough examination of stakeholder perspectives and the identification of cultural determinants influencing PA participation. NVivo's visualization and matrix query tools were used to explore relationships between codes and support robust theme development.
Rigor and reflexivity
All coding and theme development were conducted in an iterative and reflexive manner, with regular team meetings to refine categories and resolve discrepancies. This ensured analytic rigor and credibility of findings.
Findings
Stakeholder interviews revealed four key themes on the role of PA in addressing MetS in Dubai: (1) Gaps in Interventions and Awareness, (2) Barriers to PA, (3) Cultural Influences, and (4) Motivators and Opportunities. Although the interview guide included prompts about COVID-19′s impact, these responses did not contribute novel themes relevant to the study aims; thus, they are not reported in the results. Table 1 presents the themes, sub-themes, and representative quotations that illustrate stakeholder perspectives and support the thematic analysis.
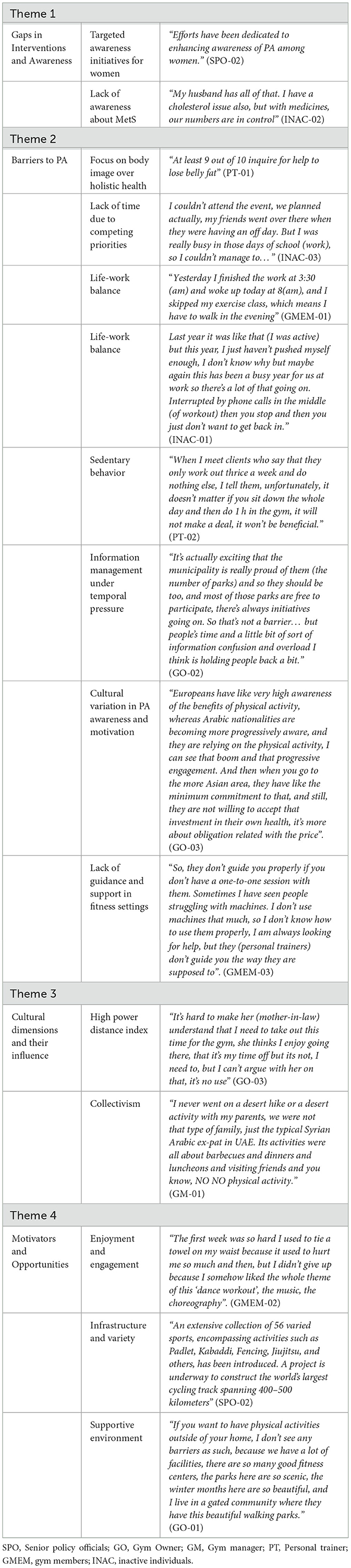
Table 1. Themes, subthemes, and representative quotations from stakeholder interviews on the role of physical activity in addressing metabolic syndrome in Dubai.
Results
Gaps in interventions and awareness
Participants widely recognized the presence of PA initiatives and facilities across Dubai, reflecting government and community efforts to promote active lifestyles. However, many expressed concerns about the inclusivity and accessibility of these programs, suggesting that certain population groups—such as lower-income individuals or culturally diverse communities—may be underserved. Several participants noted that while facilities exist, their geographic distribution and operating hours do not always align with users' needs, limiting practical access.
A recurrent theme was the lack of sustained engagement; participants observed that initial enthusiasm often waned due to insufficient follow-up or program adaptation over time. The absence of culturally tailored programming was also highlighted, with some reporting that interventions failed to reflect the social norms or preferences of their communities, thereby reducing relevance and appeal.
A critical finding was the pervasive low awareness of MetS and its link to PA. Many participants demonstrated limited understanding of how regular PA can prevent or manage metabolic conditions, frequently associating treatment primarily with medication. This knowledge gap appeared to reduce the urgency for adopting preventive behaviors like exercise, resulting in inconsistent or minimal participation. Furthermore, even those motivated to engage with PA resources encountered barriers such as unclear messaging or inadequate support, which hindered effective utilization of existing interventions.
Barriers to PA
Multiple barriers to PA were reported, each reflecting different dimensions of participants' lived experiences. Financial constraints were a prominent obstacle, with several individuals highlighting the prohibitive cost of gym memberships or specialized programs. This economic barrier was particularly acute for lower socioeconomic groups, restricting their options for structured exercise.
Within fitness facilities, participants described a lack of adequate guidance and personalized support. Many recounted experiences where personal trainers prioritized sales targets over providing foundational instruction or encouragement, leaving members feeling unsupported. Some trainers themselves acknowledged institutional pressures to focus on client acquisition, which limited their ability to assist non-paying members effectively.
Time scarcity emerged as a significant barrier, with participants balancing demanding work schedules, family responsibilities, and social commitments. The challenge of fitting regular exercise into busy days was a common refrain, often resulting in sporadic or insufficient activity. Additionally, extended periods of sedentary behavior during work hours were noted as a concern, with participants recognizing that occasional exercise did not fully offset prolonged inactivity.
Cultural dimensions influencing PA
Cultural context played a central role in shaping PA behaviors. In environments characterized by high Power Distance Index (PDI), participants reported limited capacity to advocate for their own needs regarding exercise time or facilities, particularly in workplace and family settings. Deference to authority figures often constrained grassroots initiatives but simultaneously elevated the influence of formal prescriptions, such as medical advice, which could legitimize PA within hierarchical social structures.
Collectivist values were evident in participants' prioritization of family and community obligations over personal exercise routines. Many described feeling compelled to attend traditional events or fulfill social roles that took precedence over PA, complicating efforts to maintain consistent activity. These cultural expectations often reduced individual autonomy in health-related decision-making.
Awareness and motivation levels varied significantly across cultural groups. While some demonstrated clear understanding and intrinsic motivation for PA, others participated primarily due to external pressures or social expectations. This heterogeneity underscored the complexity of cultural factors influencing behavior.
Motivators and opportunities
Despite barriers, many participants exhibited resilience and adaptability in sustaining PA. Enjoyment was frequently cited as a powerful motivator, with dance-based workouts and group activities fostering both physical engagement and social connection. Participants expressed pride in recent community infrastructure developments, such as new sports facilities and cycling tracks, which enhanced accessibility and created opportunities for shared experiences.
The social dimension of PA was important; activities that promoted community belonging and were perceived as enjoyable helped overcome initial discomfort or logistical challenges. Participants also valued accessible guidance and supportive environments, which contributed to sustained participation.
Stakeholder perspectives
The study's stakeholder-driven design captured diverse perspectives from multiple organizational levels and cultural backgrounds. This inclusivity provided a nuanced, multi-ethnic understanding of factors influencing PA engagement, enhancing the relevance of findings to Dubai's heterogeneous population.
Overall, these findings align closely with the research aims by providing a detailed and comprehensive understanding of the systemic, cultural, and individual factors influencing PA engagement for MetS prevention in Dubai. This alignment confirms that the study effectively captured the key dimensions it intended to investigate.
Discussion
This study provides valuable insights into the complex landscape of PA engagement as a strategy for preventing MetS in Dubai. The findings highlight critical gaps in awareness and intervention design, systemic and cultural barriers, as well as motivators and opportunities that shape PA participation.
The pervasive lack of awareness about MetS and its relationship to PA is a significant concern. Participants' limited understanding aligns with prior research emphasizing the need for effective translation of scientific knowledge into accessible public health messaging (27). This gap undermines motivation for preventive behaviors and suggests that existing health promotion efforts may not be sufficiently targeted or comprehensible to diverse populations.
Financial and structural barriers identified reflect well-established socioeconomic determinants of PA participation (28, 39)). The reported inadequacy of guidance and personalized support within fitness environments parallels findings from Bauman et al. (29), underscoring how service delivery models focused on sales rather than member support can discourage sustained engagement.
Time scarcity and concerns about prolonged sedentary work patterns further complicate PA adherence, consistent with literature documenting these as common obstacles (30, 31). These findings support calls for interventions that not only promote structured exercise but also encourage frequent movement throughout the day, such as active breaks or ergonomic workplace adjustments.
Cultural factors emerged as pivotal determinants. High Power Distance Index (PDI) contexts limit individual agency but enhance the authority of healthcare providers, whose recommendations carry substantial weight and can legitimize PA within hierarchical and collectivist family structures (26, 32). The collectivist emphasis on communal obligations consistently took precedence over individual health pursuits, mirroring findings across diverse populations (29, 33, 34).
These cultural dynamics underscore the importance of tailored, culturally sensitive interventions. Integrating PA into communal events or offering family-oriented exercise options may better align with local values. Framing PA as beneficial to the collective and endorsed by authoritative medical advice can enhance acceptance and adherence (35, 36).
The strong role of enjoyment and community infrastructure as motivators aligns with self-determination theory, which identifies intrinsic motivation as critical to sustained PA (37). Participants' positive response to engaging formats and social connectedness suggests that interventions prioritizing these aspects may be particularly effective (38).
Finally, the stakeholder-driven and culturally inclusive design of this study strengthens the applicability of findings across Dubai's multi-ethnic population and offers valuable lessons for other rapidly urbanizing, multicultural settings facing similar challenges.
In conclusion, the results and their interpretation align with the research aims by elucidating the multifaceted interactions among policy, culture, and individual behavior that shape PA participation. This alignment highlights the study's contribution to advancing culturally informed and contextually relevant strategies for MetS prevention.
Broader implications
The findings of this study emphasize the critical need for public health interventions that are not only comprehensive and sustainable but also deeply attuned to the cultural, structural, and socioeconomic realities of multi-ethnic urban environments such as Dubai. Generic or one-size-fits-all health promotion messages are unlikely to achieve the desired impact without addressing the specific barriers and motivational drivers identified here.
Integrated, cross-sectoral collaboration emerges as a key strategy. Healthcare providers, who hold respected positions especially in high PDI societies, should play a central role in promoting PA. Their involvement as trusted sources of culturally sensitive health education and advocates for active lifestyles can legitimize PA behaviors, enabling individuals to negotiate time and space for exercise within hierarchical family and social structures.
Partnerships that bridge healthcare systems, fitness professionals, and community organizations are essential to create continuity of care and foster sustained engagement. Fitness environments must evolve to provide culturally competent support and personalized guidance rather than prioritizing sales targets. This approach can help overcome barriers related to inadequate assistance and enhance long-term participation.
Tailored educational initiatives co-developed with community leaders and healthcare professionals can effectively bridge knowledge gaps and accommodate diverse cultural values. Strategies that integrate PA into communal events or family-oriented activities will resonate better with collectivist populations and improve relevance and uptake.
These insights have broader relevance beyond Dubai. Other rapidly urbanizing cities with diverse populations facing metabolic health challenges can draw upon these findings to develop culturally grounded, medically integrated strategies to combat sedentary lifestyles and improve metabolic health outcomes. In summary, the results, themes, and their interpretation align with the research aims by providing nuanced insights into how policy, culture, and behavior interact to shape PA participation, thereby informing culturally appropriate strategies to address MetS.
Limitations
This study has several limitations that should be considered. First, the voluntary nature of participation may have introduced self-selection bias, potentially limiting the representativeness of the sample and the generalizability of the findings. It is possible that individuals with a greater interest or experience in PA were more likely to participate. Second, time constraints and limited access to senior stakeholders may have impacted the depth and breadth of data saturation, restricting the exploration of certain perspectives or themes. Third, regional skepticism toward research and concerns about confidentiality could have influenced participants' openness, potentially resulting in socially desirable responses, particularly when discussing cultural or institutional barriers. Fourth, while the semi-structured interview format provided valuable flexibility, it also introduced variability in data collection that may affect the comparability of responses across interviews. Finally, although the interview guide included prompts regarding the impact of COVID-19, participant responses did not yield distinct or relevant themes aligned with the study's aims. Consequently, these data were excluded from the main findings, which may limit the comprehensiveness of pandemic-related influences in our results. Future research should seek to address these limitations through larger, more representative quantitative studies and the use of mixed methods approaches to validate and expand upon these findings.
Conclusion
This research offers a comprehensive exploration of the multifaceted interplay between policy, culture, and individual behavior influencing PA engagement as a strategy to address MetS in Dubai. By capturing diverse stakeholder perspectives, from policymakers to less active individuals, the study reveals both encouraging progress and persistent barriers.
Despite strong policy commitments and infrastructural developments, financial constraints, limited public awareness, and entrenched sedentary cultural norms continue to challenge widespread PA participation. The nuanced examination of cultural factors, particularly high PDI and collectivist values provides actionable insights for tailoring interventions that resonate locally.
These findings establish a foundation for developing culturally sensitive, evidence-based strategies aligned with Dubai's vision of becoming a global leader in fitness and reducing the metabolic disease burden. Moreover, the lessons learned here offer valuable guidance for public health efforts in other rapidly urbanizing, multicultural settings.
Sustained investment in culturally responsive interventions, ongoing research, and cross-sectoral collaboration will be essential to advance PA promotion and improve metabolic health outcomes both locally and globally.
Data availability statement
The datasets generated and analyzed during the current study contain interview transcripts in which all participant identifiers have been replaced with pseudonyms to preserve confidentiality. Due to the sensitive nature of the qualitative data, and in accordance with participant consent and ethical guidelines, the full transcripts are not publicly available. Data may be made available from the corresponding author on reasonable request, subject to ethical approval and in line with data protection laws.
Ethics statement
The studies involving humans were approved by MORE Ethics Committee Middlesex University London. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BA: Conceptualization, Methodology, Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. AE: Methodology, Formal analysis, Writing – review & editing. TE: Methodology, Formal analysis, Writing – review & editing. RC: Methodology, Formal analysis, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The author gratefully acknowledges all participants for generously sharing their time and valuable perspectives, which were essential to the completion of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1477025/full#supplementary-material
References
1. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
2. Yaribeygi H, Atkin SL, Simental-Mendía LE, Sahebkar A. Molecular mechanisms by which aerobic exercise induces insulin sensitivity. J Cell Physiol. (2019) 234:12385–92. doi: 10.1002/jcp.28066
3. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American heart association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
4. Yamout R, Ammar W, Tabbara J, Fares S, Assi M, Sibai AM. Waist circumference cutoff points for predicting metabolic abnormalities in Lebanese adults. Arch Med Sci Civil Dis. (2019) 4:64–71. doi: 10.5114/amscd.2019.86814
5. Mahmoud I, Sulaiman N. Prevalence of metabolic syndrome and associated risk factors in the United Arab Emirates: a cross-sectional population-based study. Front Public Health. (2022) 9:811006. doi: 10.3389/fpubh.2021.811006
6. Gariballa SEE, Al-Bluwi G, Yasin J. Physical activity level and dietary intake associated with fat-free muscle mass changes during intentional weight loss in overweight and obese subjects. Nutrients. (2024) 16:4044. doi: 10.3390/nu16234044
7. Ansari G, Qutub I. Characteristics of urban growth in the gulf states a Socio-cultural Analysis. In: Town-Talk: The Dynamics of Urban Anthropology (1983). doi: 10.1163/9789004672598_007
8. Alnakhi WK, Mamdouh H, Hussain HY, Ibrahim GM, Ahmad AS, Ali R, et al. The socio-demographic characteristics associated with non-communicable diseases among the adult population of Dubai: results from Dubai Household Survey 2019. Healthcare. (2021) 9:1139. doi: 10.3390/healthcare9091139
9. Zhang Z, Zhao M, Zhang Y, Feng Y. How does urbanization affect public health? New evidence from 175 countries worldwide. Front Public Health. (2023) 10:1096964. doi: 10.3389/fpubh.2022.1096964
10. Government of Dubai. Dubai Fitness Challenge: Transforming Dubai into the world's most active city. (2021). Available online at: https://www.dubaifitnesschallenge.com/about (Accessed June 20, 2025).
11. Packer MJ, Goicoechea J. Sociocultural and constructivist theories of learning: ontology, not just epistemology. Educ Psychol. (2000) 35:227–41. doi: 10.1207/S15326985EP3504_02
12. Parker LD, Roffey BH. Methodological themes: back to the drawing board: revisiting grounded theory and the everyday accountant's and manager's reality. Account Audit Account J. (1997) 10:212–47. doi: 10.1108/09513579710166730
13. Walker DH, Bourne LM, Shelley A. Influence, stakeholder mapping and visualization. Constr Manag Econ. (2008) 26:645–58. doi: 10.1080/01446190701882390
14. Freeman RE, Harrison JS, Zyglidopoulos S. Stakeholder Theory: Concepts and Strategies. Cambridge: Cambridge University Press (2018). doi: 10.1017/9781108539500
15. Brugha R, Varvasovszky Z. Stakeholder analysis: a review. Health Policy Plan. (2000) 15:239–46. doi: 10.1093/heapol/15.3.239
16. Reed MS, Graves A, Dandy N, Posthumus H, Hubacek K, Morris J, et al. Who's in and why? A typology of stakeholder analysis methods for natural resource management. J Environ Manage. (2009) 90:1933–49. doi: 10.1016/j.jenvman.2009.01.001
17. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. (2021) 374:n2061. doi: 10.1136/bmj.n2061
18. Patton MQ. Qualitative Research and Evaluation Methods. Thousand Oaks, CA: Sage Publications (2002).
19. Sandelowski M. Sample size in qualitative research. Res Nurs Health. (1995) 18:179–83. doi: 10.1002/nur.4770180211
20. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. (2018) 18:1–18. doi: 10.1186/s12874-018-0594-7
21. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. (2016) 26:1753–60. doi: 10.1177/1049732315617444
23. Gubrium JF, Holstein JA, Marvasti AB, McKinney KD. The SAGE Handbook of Interview Research: The Complexity of the Craft. Thousand Oaks, CA: Sage Publications (2012). doi: 10.4135/9781452218403
24. Unluer S. Being an insider researcher while conducting case study research. Qual Rep. (2012) 17:1–14. doi: 10.46743/2160-3715/2012.1752
25. Easterby-Smith M, Thorpe R, Jackson PR. Management Research. Thousand Oaks, CA: Sage Publications (2012).
26. Hofstede G. Dimensionalizing cultures: the Hofstede model. Online Readings Psychol Cult. (2011) 2:2307-0919.1014. doi: 10.9707/2307-0919.1014
27. Marcus BH, Williams DM, Dubbert PM, Sallis JF, King AC, Yancey AK, et al. Physical activity intervention studies: what we know and what we need to know: a scientific statement from the American heart association council on nutrition, physical activity, and metabolism (subcommittee on physical activity); council on cardiovascular disease in the young; and the interdisciplinary working group on quality of care and outcomes research. Circulation. (2006) 114:2739–52. doi: 10.1161/CIRCULATIONAHA.106.179683
28. Kamphuis CBM, Van Lenthe FJ, Giskes K, Huisman M, Brug J, Mackenbach JP. Socioeconomic status, environmental and individual factors, sports participation. Med Sci Sports Exerc. (2008) 40:71. doi: 10.1249/mss.0b013e318158e467
29. Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. (2012) 380:258–71. doi: 10.1016/S0140-6736(12)60735-1
30. Baillot A, Chenail S, Barros Polita N, Simoneau M, Libourel M, Nazon E, et al. Physical activity motives, barriers, and preferences in people with obesity: a systematic review. PLoS ONE. (2021) 16:e0253114. doi: 10.1371/journal.pone.0253114
31. Messing K, Dautel J-P. Is sitting really the new smoking? health of north american workers exposed to prolonged static standing. New Solutions. (2025) 35:10482911251324524. doi: 10.1177/10482911251324524
32. Kyynärsalmi A, Hammarén M, Kanste O. Understanding power distance in healthcare: a scoping review. Nurs Inq. (2025) 32:e70022. doi: 10.1111/nin.70022
33. Oyibo K, Orji R, Vassileva J. Developing culturally relevant design guidelines for encouraging physical activity: a social cognitive theory perspective. J Healthc Inform Res. (2018) 2:319–52. doi: 10.1007/s41666-018-0026-9
34. Peng B, Ng JY, Ha AS. Barriers and facilitators to physical activity for young adult women: a systematic review and thematic synthesis of qualitative literature. Int J Behav Nutr Phys Act. (2023) 20:23. doi: 10.1186/s12966-023-01411-7
35. Latif M, Blee K, Demichele M, Simi P, Alexander S. Why white supremacist women become disillusioned, and why they leave. Sociol Q. (2020) 61:367–88. doi: 10.1080/00380253.2019.1625733
36. Sebastian AT, Rajkumar E, Tejaswini P, Lakshmi R, Romate J. Applying social cognitive theory to predict physical activity and dietary behavior among patients with type-2 diabetes. Health Psychol Res. (2021) 9:24510. doi: 10.52965/001c.24510
37. Deci EL, Ryan RM. Intrinsic Motivation and Self-determination in Human Behavior. Springer Science and Business Media: New York (2013).
38. Gidney G, Bocarro JN, Bunds K, Koenigstorfer J. The relationship between the environment and physical activity-related motivational trajectories. Psychol Sport Exerc. (2024) 75:102719. doi: 10.1016/j.psychsport.2024.102719
Keywords: physical activity, metabolic syndrome, Hofstede cultural framework, stakeholder theory, non-communicable diseases
Citation: Ali B, Evans T, Cohen R and Elliott A (2025) Perspectives of physical activity in combating metabolic syndrome: insights from a multi-ethnic urban population. Front. Public Health 13:1477025. doi: 10.3389/fpubh.2025.1477025
Received: 30 January 2025; Accepted: 22 July 2025;
Published: 22 August 2025.
Edited by:
Laisa Liane Paineiras-Domingos, Federal University of Bahia (UFBA), BrazilReviewed by:
Eva Krczal, University for Continuing Education Krems, AustriaDewi Selvina Rosdiana, University of Indonesia, Indonesia
Copyright © 2025 Ali, Evans, Cohen and Elliott. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bushra Ali, c2EzMjIyQGxpdmUubWR4LmFjLnVr