 Rocío Lopez-Choquegonza
Rocío Lopez-Choquegonza Cesar Copaja-Corzo
Cesar Copaja-Corzo Javier Flores-Cohaila
Javier Flores-Cohaila- 1Facultad de Ciencias de la Salud, Universidad Privada de Tacna, Tacna, Peru
- 2Unidad de investigación para la generación y síntesis de evidencias en salud, Universidad San Ignacio de Loyola, Lima, Peru
- 3Servicio de Infectología, Hospital Nacional Edgardo Rebagliati Martins, EsSalud, Lima, Peru
- 4Hospital Nacional Victor Larco Herrera, Lima, Peru
The objective was to estimate the prevalence and identify the factors associated with Computer Vision Syndrome (CVS) among health science students at a university in Peru, we conducted a cross-sectional analytical study in Tacna, Peru, from October 12 to December 15, 2023. Participants were assessed through physical surveys. We evaluated 502 health science students; 59.2% were female, and the median age was 21 years (range 19 to 23 years). 78.1% had CVS, and 52% had moderate nomophobia. In the adjusted model, monthly family income of 2000 to 5,000 soles (PR: 0.81; 95% CI: 0.73 to 0.91) and over 5,000 soles (PR: 0.84; 95% CI: 0.74 to 0.95) was associated with a lower prevalence of CVS compared to families with income less than 2000 soles. Additionally, the prevalence of CVS was higher among students with moderate nomophobia (PR: 1.91; 95% CI: 1.24–3.16) and severe nomophobia (PR: 2.07; 95% CI: 1.31–3.48) compared to those with no symptoms or only mild symptoms of nomophobia. The prevalence of CVS is high among health science students, especially in medical students. As the severity of nomophobia increases, so does the prevalence of CVS, and higher family income is associated with lower CVS.
Introduction
Computer Vision Syndrome (CVS) is characterized by ocular symptoms such as burning, itching, foreign body sensation, tearing, excessive blinking, blurred or double vision, red and dry eyes, difficulty focusing on near tasks, light sensitivity, visual halos, and headache (1); It is estimated that the prevalence of CVS worldwide is 66% (2), with percentages ranging from 35.2 to 97.3% in adults (3), and from 12.1 to 94.8% in children (4), making it a common issue (5). While the prevalence is based only on approximate estimates, the frequency of CVS in potential risk subgroups, such as university students, remains unclear, especially with the increased use of computers, tablets, e-readers, and smartphones for educational, communicative, and recreational purposes. Additionally, the COVID-19 pandemic further escalated the use of technological devices, potentially contributing to the continued increase in the prevalence of CVS (6, 7).
CVS has been reported to impact the quality of life of those affected (8). Other research has suggested that CVS could be associated with macular integrity issues and foveal dysfunction (9). In daily life, CVS might be linked to reduced productivity, visual and musculoskeletal impairment (10), as well as disruptions in circadian rhythms, altered sleep patterns, and increased anxiety and depression (11, 12). While some potential consequences of CVS have been reported, it is not yet clear what other issues it may entail.
Some factors associated with CVS have been identified, for example in Saudi Arabia, a study evaluating 300 medical students identified that factors associated with a higher prevalence of CVS were being female and using electronic devices for more extended periods (13). Another study conducted in Saudi Arabia, involving 521 students, found that older age, female gender, refractive errors, and the use of digital devices for more than 6 h were the main factors associated with CVS among university students (14). Another study in Thailand, which assessed a population of 527 university students attending virtual classes, found that being female, having previous ocular symptoms, astigmatism, screen distance <20 cm, screen reflections, low screen brightness, inadequate sleep duration between classes, and longer screen time was associated with CVS (15). Although these studies included a considerable number of participants, they were conducted online, potentially excluding certain student populations due to accessibility and connectivity limitations. This circumstance, along with selection bias and the limited extrapolation of data to other populations, is a point to consider. Recently, the issue of CVS has been studied in Latin America. A study conducted in Colombia reported a prevalence of 41.07% (16), while another study in Peru found a prevalence of 93% (17). Although these results are concerning, both studies focused exclusively on medical students and had small sample sizes, which limits the generalizability of their findings. Additionally, among the reported studies, only one (14), used regression models to identify the strength of the association between variables; the rest only employed hypothesis testing, further limiting the clarity of their results.
It is evident that more studies are needed to provide results that are extrapolatable to other realities, as well as to evaluate other associated factors to increase knowledge in this field and to develop more precise interventions aimed at reducing this problem. Therefore, this study aims to identify the prevalence and factors associated with CVS among health science students at a university in Peru.
Methods
Design and context
An analytical cross-sectional study was conducted on health science students at the Private University of Tacna (UPT) from October 12 to December 15, 2023. The Faculty of Health Sciences (FACSA) includes the schools of medicine, dentistry, and medical technology. UPT is a non-profit private institution affiliated with the Peruvian Association of Medical Schools (ASPEFAM) and the Peruvian Association of Dental Schools (ASPEFO). Additionally, it is one of the two universities in Tacna, Peru (18).
Population
We included students from health science disciplines (Medicine, Dentistry, and Medical Technology, including Physical Therapy and Rehabilitation, Clinical Laboratory, and Pathological Anatomy) who provided informed consent. We decided to include these students because they tend to have a higher academic and financial burden to support their studies, which is reflected in multiple problems, including excessive use of electronic devices and, more frequently, the development of CVS compared to other students (17–20). Those with incomplete surveys (more than 10 missing data points) or those who decided to withdraw from the study during the survey were excluded.
A post hoc power analysis was conducted using the one-sample proportion test (power oneprop) in Stata. Considering an expected proportion of 93% (Meneses et al.) (17), an observed proportion of 78.1%, a sample size of 502 participants, and a significance level of 0.05, a statistical power of 99% was obtained.
Procedures
The data collection was carried out from November to December 2023. Entry into the classrooms was punctual at the agreed-upon time with the course instructor during class hours. Upon entry, Rocio Lopez (RL) introduced herself to the students as part of the research team, explained the research objective, provided details about voluntary participation, and explained the process of signing the informed consent if they chose to participate. She also gave the students guidelines on how to fill in each section of the data collection form.
During the survey, RL informed the students that if they had any questions while completing the form, they could raise their hand, and the researcher would approach them to address their concerns. Additionally, they were instructed to raise their hand after completing the form so RL could collect it. After this, they were told they could begin, and the average time it took for students to complete the surveys was 15 min. After all participants in the classroom had finished filling out the forms and collected all the surveys, they were thanked for their participation.
After collecting the information in physical form, the data was transferred to an Excel data collection form. Data entry was done twice by different researchers [Cesar Copaja (CC) and RL]. After completing this process, both datasets were reviewed to identify inconsistencies in the data recording. If any data differed, the physical form was consulted, and the error was corrected.
Instrument and variables
The data collection form was anonymous, and no information that could identify the participant was requested. The form consisted of three sections: First, sociodemographic characteristics (08 questions); second, use of technological devices (06 questions); and third, CVS (16 items) and nomophobia (20 questions). The complete data collection form can be found in Appendix A1.
The dependent variable was CVS. For its determination, we used the Computer Vision Syndrome Questionnaire (CVS-Q). It is a self-administered questionnaire consisting of 16 items, designed initially by Seguí et al. in 2015 in English for administrative workers (19). Our study used the validated version for Peruvian healthcare professionals (20), which reported adequate internal consistency (Cronbach’s Alpha 0.939). For interpreting the CVS-Q questionnaire, the product obtained from the intensity and frequency allows us to calculate the severity of each symptom. If the sum found from this calculation is greater than or equal to 06 points, it can be affirmed that the person has symptoms of CVS (19).
To assess nomophobia, defined as the fear of not having contact with a mobile phone (21), we used the Nomophobia Questionnaire (NMP-Q), which evaluates its severity. This is a self-report questionnaire consisting of 20 items with a 7-point Likert scale, ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). The NMP-Q was originally developed in English by Yildirim and Correia (22), In our study, we used the Spanish version validated in a population aged 13 to 19 years (23), also utilized in a similar study with university students in Peru aged 17 to 34 years, reporting overall good internal consistency (Cronbach’s Alpha 0.964) (24). For interpretation, the following criteria were considered: a total score of 20 indicates the absence of nomophobia; a score greater than 20 and less than 60 indicates a mild level of nomophobia; a total score greater than or equal to 60 and less than 100 indicates a moderate level of nomophobia; and a total score greater than or equal to 100 indicates severe nomophobia (22).
Statistics
The analyses were performed using the statistical software RStudio. To describe the population and its characteristics, we employed frequencies, percentages, measures of central tendency, and dispersion.
We utilized Poisson regression models with robust variance to address our research question. Given that this is an exploratory study, we decided to perform univariable selection to determine the variables that would enter the adjusted model (25, 26). For this, a crude analysis was performed between each variable and the outcome (CVS), and statistically significant variables (p < 0.05) were included in the multivariate model. We obtained adjusted prevalence ratios (aPR) and their respective 95% confidence intervals (CI 95%) in the multivariate analysis.
Results
A total of 534 health science students were surveyed. Out of the total, 32 surveys were excluded as they did not meet the inclusion criteria, and ultimately, the surveys of 502 students were analyzed (Figure 1).
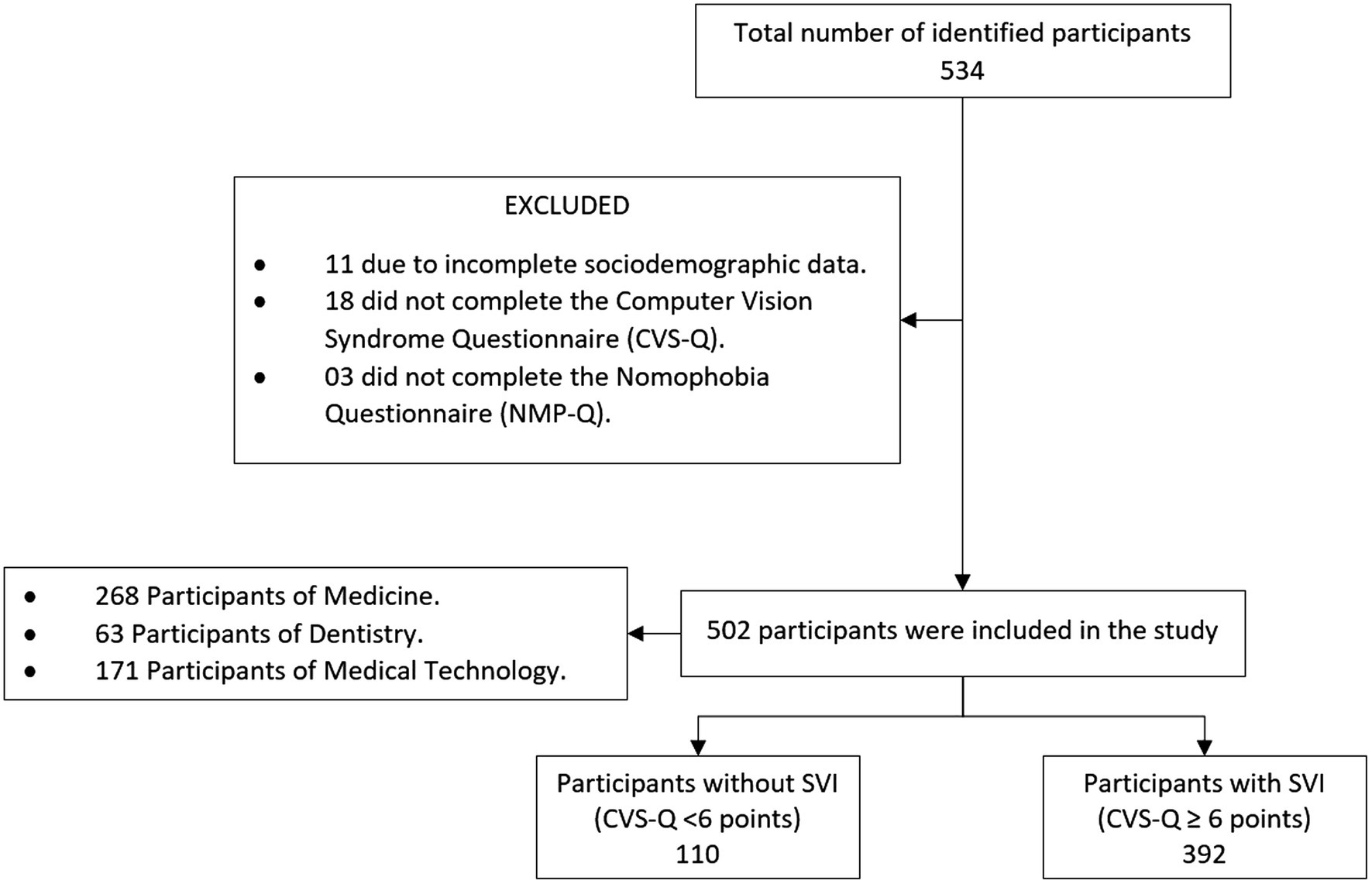
Figure 1. Selection flowchart. CVS-Q, Computer Vision Syndrome Questionnaire; CVS, Computer Vision Syndrome; NMP-Q, Nomophobia Questionnaire.
Population characteristics
The median age was 21 years (range 19 to 23 years), and 59.2% were women. Most students (53.4%) were studying medicine, and 65.7% were in the 1st to 3rd year of study.
Women had a higher prevalence of CVS (80.1%) compared to men (75.1%). Regarding the use of technological devices, 30.5% reported using their cell phones between 4 and 6 h per day. Concerning the NMP-Q scale, 52% had moderate nomophobia, and 7.4% had severe nomophobia. On the other hand, 78.1% experienced computer vision syndrome (6 points or more; Table 1).
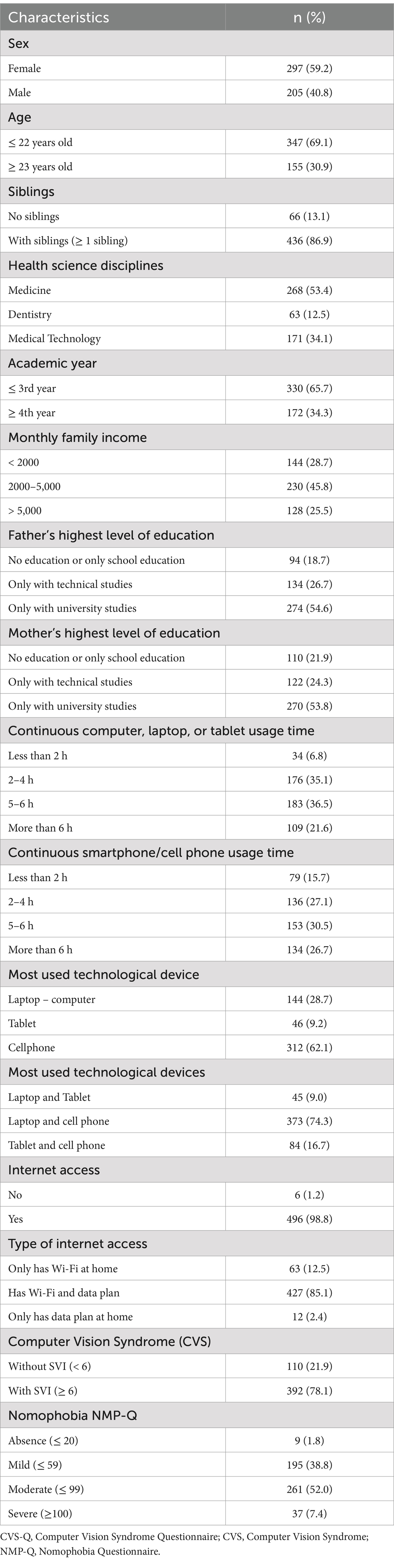
Table 1. Population Characteristics (n = 502).
CVS symptoms and nomophobia score
Participants with more frequent CVS symptoms had higher scores on the nomophobia questionnaire (NMP-Q). For example, those who experienced double vision “often or always” had an average NMP-Q score of 78.8 ± 25.1, while those who never experienced it scored 60.7 ± 23.5. Similarly, participants with frequent eye pain had a score of 76.9 ± 21.1, compared to 59.1 ± 24.6 in those who did not report this symptom (Table 2).
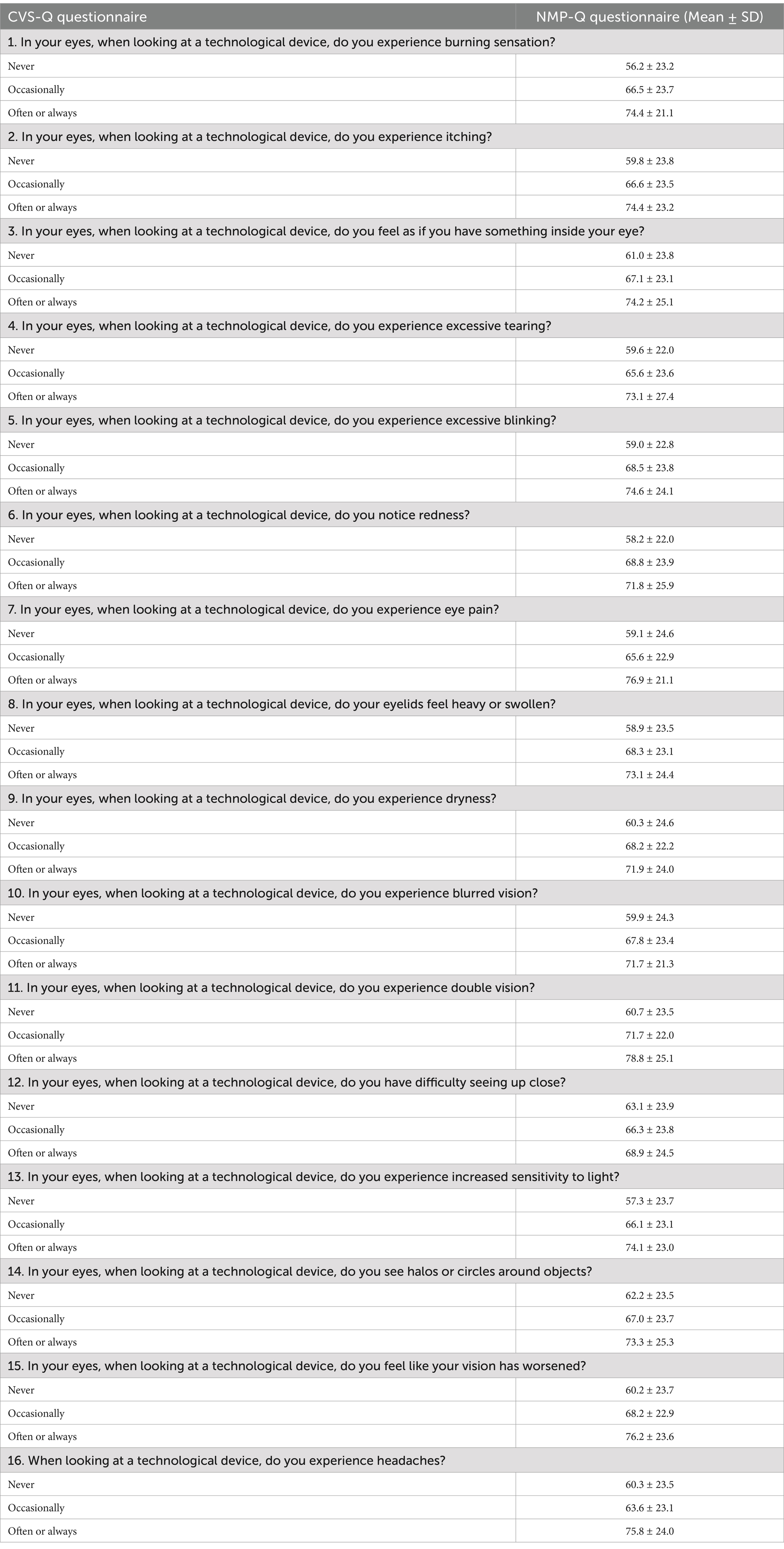
Table 2. CVS symptoms and nomophobia scores in health science students.
Factors associated with CVS
In the adjusted Poisson regression model with robust variance, we identified that a monthly family income of 2000 to 5,000 soles (aPR: 0.81; 95% CI: 0.73 to 0.91) and more than 5,000 soles (aPR: 0.84; 95% CI: 0.74 to 0.95) was associated with a lower prevalence of CVS compared to those earning less than 2000 soles per month. Additionally, the prevalence of CVS was higher in students with moderate nomophobia symptoms (PR: 1.91; 95% CI: 1.24 to 3.16), and severe nomophobia (PR: 2.07; 95% CI: 1.31 to 3.48) in comparison to those without symptoms or with mild symptoms of nomophobia (Table 3).
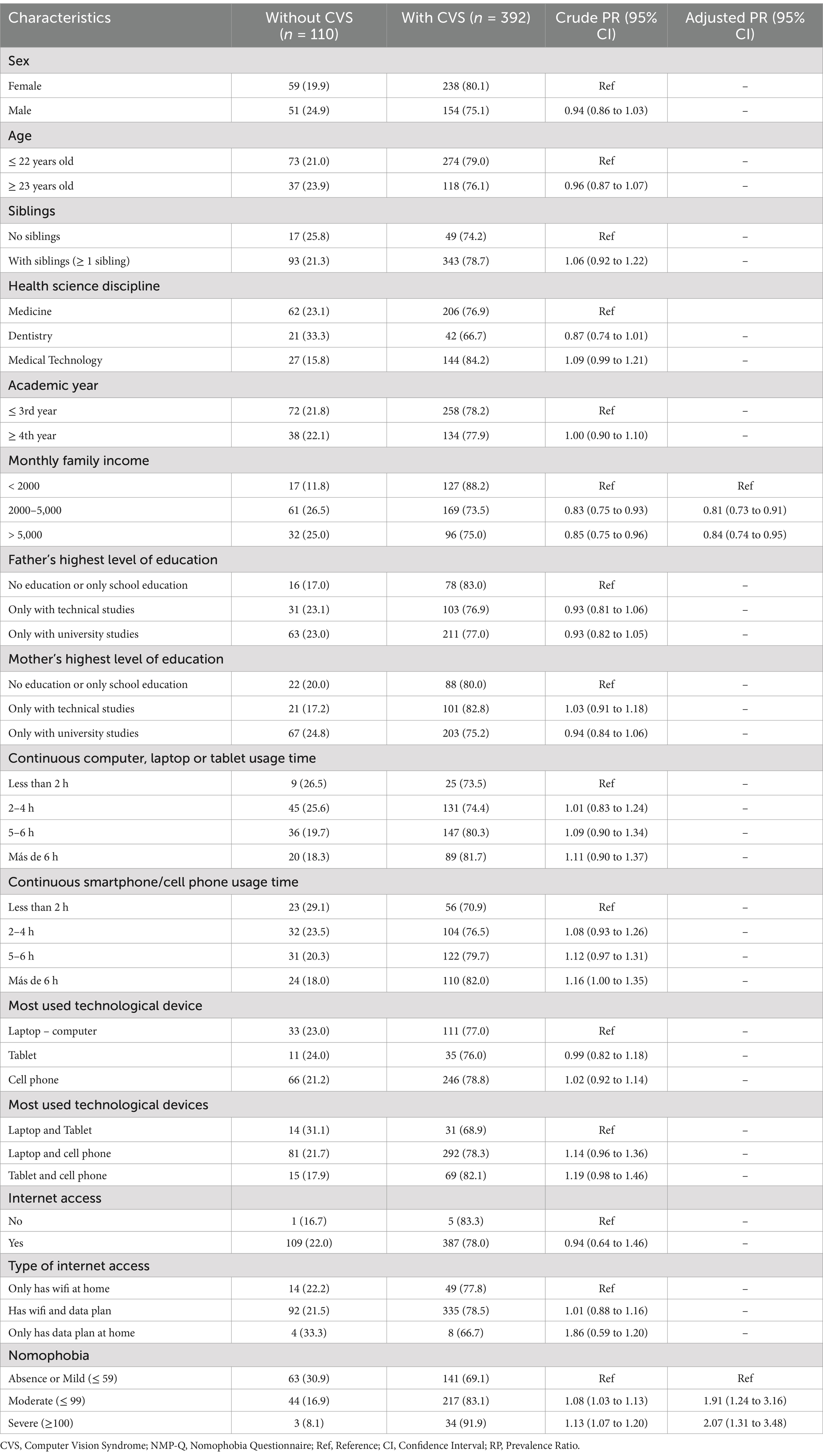
Table 3. Characteristics associated with computer vision syndrome (n = 502).
Discussion
Summary of findings
Here, we conducted a cross-sectional analytical study to investigate the prevalence of CVS, its association with nomophobia, and other related factors in 502 health sciences students from a Peruvian university. Our main findings were as follows: (1) The prevalence of CVS symptoms in this population was 78.1%; (2) There was an association between nomophobia severity and CVS, with the highest between severe nomophobia and CVS (PR: 2.07; 95% CI: 1.31 to 3.48), (3) A higher family income was associated with lower prevalence of CVS.
Comparison with prior work
We found a prevalence of 78.1% of CVS. This was like a prior systematic review that reported a global prevalence of 66% (27). In health sciences education, a study conducted in Paraguay reported a prevalence of 82.5% (28), while another study conducted in Peru reported a prevalence of 58% (29). These findings highlight the importance of CVS. One major explanation, as described by Coronel (28), is the conversion of classes from a physical to a digital space after the COVID-19 pandemic, which led to CVS. Moreover, the widespread use of mobile phones and increased screen time may be associated with the high prevalence of CVS.
We identified an inverse association between family income and CVS, and a positive association between the severity of nomophobia and CVS. A study conducted in Ethiopia reported that participants with higher monthly incomes were 54.7% less likely to develop CVS compared to those with lower average monthly incomes (30). From the perspective of social determinants, higher incomes can influence other protective factors such as access to health education resources, healthcare awareness, and preventive measures, in addition to better equipment like light filters (2). This could explain our results.
We found an association between nomophobia and CVS, which has not been previously studied in the literature. The underlying mechanism behind this association could be attributed to the increased screen time and prolonged use of digital devices associated with nomophobia behavior. Individuals becoming more dependent on smartphones may engage in extended periods of close-range focusing, leading to CVS symptoms. This is of significant importance due to the high nomophobia reported prevalence worldwide among university students, reaching almost 60% for moderate and 20% for severe nomophobia (31). Therefore, in the new and evolving digital world, where future generations may be more accustomed to smartphones and other electronic devices, it is necessary to further study this association. Nomophobia has been linked to other outcomes such as anxiety, depression, low self-esteem, and lower academic performance (32–35). However, now it seems to also be associated with CVS.
Implications
To our knowledge, this is the first study to address the association between CVS and nomophobia. Hence, this finding has several implications. For deans and faculty, the high prevalence of CVS represents a call to action for screening and early intervention strategies, integrating activities with no screens into the formal curriculum or digital wellness programs. For medical practitioners, the newly found association between nomophobia and CVS may require that when CVS is suspected, a screening of nomophobia be considered in companion to healthy digital habits and education regarding potential consequences of excessive digital device use. Researchers need to understand the association between nomophobia and CVS better, as this has not been previously explored, and consider the role of other social determinants as moderators.
Strengths and limitations
This study has limitations that should be considered. Firstly, being a cross-sectional study, we cannot determine the temporality of the associations. Additionally, since the questionnaires were self-administered, social desirability bias might be present; however, participants were informed that the survey would be anonymous, which could reduce this risk. Additionally, we were unable to perform a comprehensive ophthalmologic examination, which would have provided a more in-depth analysis of the students’ eye health. Despite its limitations, this is, to the best of our knowledge, the first study to evaluate computer vision syndrome in health sciences students in Peru. We used rigorous inclusion criteria and an adequate statistical power to ensure the validity and inference of our results.
Conclusion
In conclusion, this cross-sectional study among health sciences students in Peru found a high prevalence of CVS and a significant association between nomophobia severity and CVS, particularly between severe nomophobia and CVS. Additionally, higher family income was associated with a lower prevalence of CVS. These findings underscore the importance of addressing the growing issue of CVS and its potential link to nomophobia in the digital age. As smartphones and other electronic devices continue to rise, promoting healthy digital habits and raising awareness about the potential consequences of excessive digital device use on ocular health and overall well-being is crucial. It is crucial to develop new interventions aimed at reducing excessive smartphone use.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the project received approval from the ethics committee of FACSA at the Private University of Tacna (FACSA-CEI/119–09-2023). We obtained informed consent from the students to participate in this research. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JF-C: Data curation, Investigation, Methodology, Project administration, Validation, Writing – original draft. RL-C: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. CC-C: Conceptualization, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The Universidad San Ignacio de Loyola financed the article processing charge (Code: USIL-2024). Funding Acquisition was by authors CC-C. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1485515/full#supplementary-material
References
1. American Optometric Association. Computer vision syndrome (digital eye strain) (2022). Available at: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome
2. Lema, AK, and Anbesu, EW. Computer vision syndrome and its determinants: a systematic review and meta-analysis. SAGE Open Med. (2022) 10:20503121221142402. doi: 10.1177/20503121221142402
3. Altalhi, A, Khayyat, W, Khojah, O, Alsalmi, M, and Almarzouki, H. Computer vision syndrome among health sciences students in Saudi Arabia: prevalence and risk factors. Cureus. (2020) 12:e7060. doi: 10.7759/cureus.7060
4. Li, L, Zhang, J, Chen, M, Li, X, Chu, Q, Jiang, R, et al. Contribution of Total screen/online-course time to Asthenopia in children during COVID-19 pandemic via influencing psychological stress. Front Public Health. (2021) 9:736617. doi: 10.3389/fpubh.2021.736617
5. Randolph, SA. Computer vision syndrome. Workplace Health Saf. (2017) 65:328. doi: 10.1177/2165079917712727
6. Vargas-Peirano, M, Navarrete, P, Díaz, T, Iglesias, G, and Hoehmann, M. Atención de pacientes oftalmológicos durante la pandemia COVID-19: revisión panorámica rápida. Fortschr Med. (2020) 20:e7902. doi: 10.5867/medwave.2020.04.7902
7. Pavel, IA, Bogdanici, CM, Donica, VC, Anton, N, Savu, B, Chiriac, CP, et al. Computer vision syndrome: an ophthalmic pathology of the modern era. Medicina (Mex). (2023) 59:412. doi: 10.3390/medicina59020412
8. Ranasinghe, P, Wathurapatha, WS, Perera, YS, Lamabadusuriya, DA, Kulatunga, S, Jayawardana, N, et al. Computer vision syndrome among computer office workers in a developing country: an evaluation of prevalence and risk factors. BMC Res Notes. (2016) 9:150. doi: 10.1186/s13104-016-1962-1
9. Iqbal, M, Elzembely, H, Elmassry, A, Elgharieb, M, Assaf, A, Ibrahim, O, et al. Computer vision syndrome prevalence and ocular sequelae among medical students: a university-wide study on a marginalized visual security issue. Open Ophthalmol J. (2021) 15:156–70. doi: 10.2174/1874364102115010156
10. Vaz, F, Henriques, S, Silva, D, Roque, J, Lopes, AS, and Mota, M. Digital Asthenopia: Portuguese Group of Ergophthalmology Survey. Acta Médica Port. (2019) 32:260–5. doi: 10.20344/amp.10942
11. Merhy, G, Akel, M, Kheir, N, Hallit, S, and Obeid, S. Computer vision syndrome in Lebanese male adolescents: correlates with mental health and mediating effect of stress. Prim Care Companion CNS Disord. (2023) 25:45139. doi: 10.4088/PCC.21m03180
12. Patil, A, Null, B, Chaudhury, S, and Srivastava, S. Eyeing computer vision syndrome: awareness, knowledge, and its impact on sleep quality among medical students. Ind Psychiatry J. (2019) 28:68–74. doi: 10.4103/ipj.ipj_93_18
13. Almousa, AN, Aldofyan, MZ, Kokandi, BA, Alsubki, HE, Alqahtani, RS, Gikandi, P, et al. The impact of the COVID-19 pandemic on the prevalence of computer vision syndrome among medical students in Riyadh. Saudi Arabia Int Ophthalmol. (2023) 43:1275–83. doi: 10.1007/s10792-022-02525-w
14. AlDarrab, A, Khojah, AA, Al-Ghazwi, MH, Al-Haqbani, YJ, Al-Qahtani, NM, Al-Ajmi, MN, et al. Magnitude and determinants of computer vision syndrome among college students at a Saudi university. Middle East Afr J Ophthalmol. (2021) 28:252–6. doi: 10.4103/meajo.meajo_272_21
15. Wangsan, K, Upaphong, P, Assavanopakun, P, Sapbamrer, R, Sirikul, W, Kitro, A, et al. Self-reported computer vision syndrome among Thai university students in virtual classrooms during the COVID-19 pandemic: prevalence and associated factors. Int J Environ Res Public Health. (2022) 19:3996. doi: 10.3390/ijerph19073996
16. Ramírez-Velandia, F, Paz-Arteaga, J-C, Penagos-Aldana, LC, Paternina-Navarro, A, and Palencia-Sánchez, F. Computer vision syndrome in students of a medical School in Colombia. A Cross-Sectional Study (2022).
17. Meneses Castañeda, RM, Ramos Rodríguez, SL, Sánchez Miraval, EL, Stein Montoros, DF, Chávez Rodríguez, LG, et al. Síndrome visual informático en estudiantes de medicina en educación virtual de una universidad peruana durante el 2021. Rev Fac Med Humana. (2023) 23:25–32. Available at: http://www.scielo.org.pe/scielo.php?pid=S2308-05312023000100025&script=sci_abstract
18. UPT. Universidad Privada de Tacna (2020). Available at: https://www.upt.edu.pe/upt/web/index.php
19. Seguí, M, Cabrero-García, J, Crespo, A, Verdú, J, and Ronda, E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. J Clin Epidemiol. (2015) 68:662–73. doi: 10.1016/j.jclinepi.2015.01.015
20. Aguilar-Ramírez, MDP, and Meneses, G. Validación del instrumento “Computer Vision Syndrome Questionnaire (CVS-Q)” para la evaluación del síndrome visual informático en personal de salud de Lima. Rev Medica Hered. (2022) 33:187–95. doi: 10.20453/rmh.v33i3.4339
21. Asensio Chico, I, Díaz Maldonado, L, and Garrote, ML. Nomofobia. Enfermedades del siglo XXI. Med Fam SEMERGEN. (2018) 44:e117–8. doi: 10.1016/j.semerg.2018.05.002
22. Yildirim, C, and Correia, A-P. Exploring the dimensions of nomophobia: development and validation of a self-reported questionnaire. Comput Hum Behav. (2015) 49:130–7. doi: 10.1016/j.chb.2015.02.059
23. González-Cabrera, J, León-Mejía, A, Pérez-Sancho, C, and Calvete, E. Adaptation of the nomophobia questionnaire (NMP-Q) to Spanish in a sample of adolescents. Actas Esp Psiquiatr. (2017) 45:137–44. Available at: https://pubmed.ncbi.nlm.nih.gov/28745386/
24. Franco-Guanilo, R, and Hervias-Guerra, E. Estructura factorial, validez y confiabilidad de la escala de nomofobia en estudiantes de una universidad estatal de Lima Metropolitana. Propósitos Represent. (2022) 10:10. doi: 10.20511/pyr2022.v10n2.1572
25. Chowdhury, MZI, and Turin, TC. Variable selection strategies and its importance in clinical prediction modelling. Fam Med Community Health. (2020) 8:e000262. doi: 10.1136/fmch-2019-000262
26. Heinze, G, Wallisch, C, and Dunkler, D. Variable selection - a review and recommendations for the practicing statistician. Biom J Biom Z. (2018) 60:431–49. doi: 10.1002/bimj.201700067
27. Anbesu, EW, and Lema, AK. Prevalence of computer vision syndrome: a systematic review and meta-analysis. Sci Rep. (2023) 13:13. doi: 10.1038/s41598-023-28750-6
28. Coronel-Ocampos, J, Gómez, J, Gómez, A, Quiroga-Castañeda, PP, and Valladares-Garrido, MJ. Computer visual syndrome in medical students from a private University in Paraguay: a survey study. Front Public Health. (2022) 10:935405. doi: 10.3389/fpubh.2022.935405
29. Lindo-Cano, EF, García-Monge, VA, Castillo-Cadillo, KJ, Sánchez-Tirado, EA, Távara, IM, and Morales, J. Computer-digital vision syndrome among university students of Lima City. Open Public Health J. (2022) 15:15. doi: 10.2174/18749445-v15-e2208104
30. Lemma, MG, Beyene, KG, and Tiruneh, MA. Computer vision syndrome and associated factors among secretaries working in ministry offices in Addis Ababa, Ethiopia. Clin Optom. (2020) 12:213–22. doi: 10.2147/OPTO.S284934
31. Tuco, KG, Castro-Diaz, SD, Soriano-Moreno, DR, and Benites-Zapata, VA. Prevalence of nomophobia in university students: a systematic review and Meta-analysis. Healthc Inform Res. (2023) 29:40–53. doi: 10.4258/hir.2023.29.1.40
32. Vagka, E, Gnardellis, C, Lagiou, A, and Notara, V. Nomophobia and self-esteem: a cross sectional study in Greek university students. Int J Environ Res Public Health. (2023) 20:2929. doi: 10.3390/ijerph20042929
33. Reza, M, Tasnim, M, Afroz, M, and Ruhi, S. Exploring nomophobia among university students: identifying risk factors, correlates, and predictive insights through machine learning. J Future Sustain. (2024) 4:243–50. doi: 10.5267/j.jfs.2024.11.001
34. Gnardellis, C, Vagka, E, Lagiou, A, and Notara, V. Nomophobia and its association with depression, anxiety and stress (DASS scale), among young adults in Greece. Eur J Investig Health Psychol Educ. (2023) 13:2765–78. doi: 10.3390/ejihpe13120191
Keywords: computer vision syndrome, electronic devices, nomophobia, Peru, smartphone
Citation: Lopez-Choquegonza R, Copaja-Corzo C and Flores-Cohaila J (2025) Computer vision syndrome and its associated factors in health science students from a university in Peru. Front. Public Health. 13:1485515. doi: 10.3389/fpubh.2025.1485515
Edited by:
Anand Marya, University of Puthisastra, CambodiaReviewed by:
Pragya Sharma, Maulana Azad medical College, IndiaFrancisco Palencia-Sánchez, Pontifical Javeriana University, Colombia
Mohd Fazil Jamaludin, Universiti Teknologi MARA Cawangan Kedah, Kampus Sungai Petani, Malaysia
Copyright © 2025 Lopez-Choquegonza, Copaja-Corzo and Flores-Cohaila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cesar Copaja-Corzo, Q3NhcmNvcGFqYUBnbWFpbC5jb20=