 Majid Sartipi1,2
Majid Sartipi1,2 Asiye Aminafshar3,4*
Asiye Aminafshar3,4* Abdolrazzagh Pakzad5Mohammadreza Shafiei6
Abdolrazzagh Pakzad5Mohammadreza Shafiei6 Hojjat Farahmandnia7
Hojjat Farahmandnia7 Asghar Tavan7
Asghar Tavan7- 1Infectious Diseases and Tropical Medicine Research Center, Research Institute of Cellular and Molecular Sciences in Infectious Diseases, Zahedan University of Medical Sciences, Zahedan, Iran
- 2Department of Biostatistics and Epidemiology, School of Health, Zahedan University of Medical Sciences, Zahedan, Iran
- 3Student Research Committee, Kerman University of Medical Sciences, Kerman, Iran
- 4Health Promotion Research Center, Zahedan University of Medical Sciences, Zahedan, Iran
- 5Health, Safety, and Environmental Management (HSE), Zahedan University of Medical Sciences, Zahedan, Iran
- 6Department of Nursing, School of Nursing, Larestan University of Medical Sciences, Larestan, Iran
- 7Health in Disasters and Emergencies Research Center, Institute for Futures Studies in Health, Kerman University of Medical Sciences, Kerman, Iran
Background: An effective crisis management system like the Emergency Operations Center (EOC) influences the number of damages and human casualties during disasters and pandemics. This study examined the preparedness and management functions of the Zahedan University of Medical Sciences incident command system (ICS) in response to incidents and disasters, focusing on its implementation during the pandemic.
Materials and methods: The study employed a cross-sectional design. All members of the university’s ICS at various levels were included in the study. The data collection tool was a researcher-made questionnaire. The PCA (Principal component analysis) method was employed in SPSS 27 statistical software for data analysis.
Results: Among the extracted components, the highest mean was associated with the command and empowerment of operational teams (C2), with a mean of 3.72 (CI: 3.04–4.40). The managers working in the crisis management headquarters, at the planning and comprehensive command level, performed better than other management levels. A significant relationship was found between past crisis experience and the scores of all extracted components. Individuals who had previously been involved in crises scored higher. The p-values for components 1 to 4 were 0.002, 0.001, 0.005, and 0.019, respectively. In C1 (Comprehensive risk planning) and C2, individuals with higher education obtained better scores, 3.85 (CI: 3.15–4.55) and 3.92 (CI: 3.22–4.62) compared to individuals with lower education 3.46 (CI: 2.79–4.13) and 3.57 (CI: 2.93–4.21) (p-values 0.011 and 0.02, respectively). Also, continuous training significantly helped improve the performance of managers. Other variables such as field of study, type of employment, and job history did not show significant differences.
Conclusion: Past experiences significantly impact people’s ability to prepare and make quick decisions in times of crisis. It is essential to provide effective solutions to future managers and implement corrective measures within the crisis management system. Additionally, training and empowerment programs should be planned for all healthcare workers, and greater attention should be paid to investing in young forces.
Introduction
Natural and man-made disasters have had considerable health effects on the communities. In 2021, 432 natural disasters were recorded worldwide, a number that is increasing globally. In recent decades, pandemics have resulted in widespread disasters (1). Infectious disease pandemics are among the most significant health threats. A pandemic is a widespread infectious disease that crosses international borders and affects a large number of people in multiple regions or continents (2). In addition to mortality, viral and bacterial pandemics have adverse economic, social, and health effects on societies (3). Weaknesses in infrastructure, a lack of resources, and inadequate coordination between different institutions are among the primary factors that contribute to the complexity and prolongation of crises, including the management of pandemics (4). We require effective management to mitigate the impacts of pandemics. We must rebuild the emergency health system, establish emergency health departments, strengthen international and domestic cooperation, and strengthen public interventions in response to public health crises and pandemics (5).
In Iran, the number of disasters increased from fewer than 100 cases per year before 1980 to 300 to 400 cases between 2000 and 2019. Considering the frequency of occurrence, extent, and population density, these risks lead to both small and large disasters that sometimes require difficult recovery (6, 7). An incident with moderate severity can also affect the country’s healthcare system (8). One goal of responding to incidents and disasters in the healthcare system is to prevent and reduce casualties and physical and mental injuries. This can only be achieved with careful planning, preparation, and training of the human resources involved in the crisis (9, 10).
On the other hand, managers need access to coherent, integrated, accessible, and coordinated health services. A lack of proper planning, resource management, and intersectoral coordination will challenge the provision of healthcare services during disasters (11–13). Integrated disaster management at the global level requires a conceptual definition, such as Emergency Operations Centers (EOCs). These centers have various departments, including planning, operations, logistics, and information and communication technology (14). Strategic decisions for disaster management, coordination of multilateral responses to health incidents, collection and distribution of resources in the emergency operations center, timely information announcement to the public and the media, and interagency coordination are made here. The correct functioning of these centers enables the efficient allocation and distribution of resources, including human resources, equipment, and supplies, which must be directed to the areas with the greatest need (15).
Additionally, EOCs serve as command-and-control centers to coordinate emergency responses, facilitate risk assessment, and manage critical information. With the integration of an Incident Management System (IMS), these centers serve as strategic tools for disaster management. Standardizing processes and improving coordination help enhance incident preparedness and response (16). In addition to incidents and disasters, EOCs possess the necessary capacity to manage infectious diseases during pandemics. The World Health Organization (WHO) has also recognized the importance of EOCs in dealing with epidemics and has provided guidelines for establishing these centers at the national level. WHO recommends that Member States develop and strengthen the necessary infrastructure for managing health crises, including the establishment and strengthening of EOCs, so that they can respond effectively and in a coordinated manner to large outbreaks (17). The widespread outbreak of Ebola in West Africa between 2014 and 2016 drew the attention of policymakers to the critical role of emergency operations centers in managing health crises in countries with limited resources (18). Studies by Shuaib et al. (2017) and OO Olu et al. (2016) demonstrated that these centers can serve as effective tools in controlling the spread of diseases in these areas (16, 19). Emergency Operations Centers (EOCs) play a crucial role in managing health emergencies, particularly in developing countries with limited infrastructure. Case studies in regions such as Nigeria, Southeast Asia, and Africa have demonstrated the effectiveness of these centers in controlling infectious diseases, including Ebola, polio, COVID-19, and dengue fever (16, 20, 21). These centers enhance emergency response, mitigate the negative impacts of disasters, and expedite decision-making by coordinating efforts among various organizations and stakeholders. They provide monitoring tools and data analysis, collect, analyze, and disseminate information. Additionally, EOCs effectively manage resource constraints and improve health outcomes in resource-limited countries by facilitating resource allocation, strengthening collaboration and data sharing, and enhancing response times (16, 18, 21–23).
Early activation of the Public Health Emergency Operations Center (PH-EOC) and the use of an incident management system (IMS) during the dengue outbreak in Pakistan resulted in providing an organizational structure with clear roles and tasks for different teams, a transparent chain of Command, and an interdepartmental coordination mechanism. And the integration of accountability activities. This resulted in the early control of dengue outbreaks compared to previous outbreaks. Also, human resources training and EOC standby activation are necessary during non-pandemic periods to implement IMS in the shortest possible time. With the adoption of IMS, more effective planning, more robust coordinated response, and improved communication with health authorities and the general public will be achieved (23). The H1N1 influenza pandemic in 2009 highlighted the importance of interdepartmental coordination and information management in EOCs (24) Obstacles and factors, including IMS, communication strategies, data management, workforce capacity, and physical infrastructure, affect the effective use of these centers in managing public health emergencies (25). In their study, Tsukayama et al. (2023) examined the coordination between Public Health Emergency Operations Centers (PHEOC) in Thailand, Cambodia, Laos, and Malaysia. They found that each of these countries is committed to strengthening its national centers and enhancing cross-border communication in response to the COVID-19 pandemic. Still, gaps remain in data sharing, workforce capacity, and use of communication platforms (25).
Ryan et al. (26) investigated the importance of planning in EOCs. They stated that detailed and comprehensive planning in these centers is vital for the success of field operations and for maintaining situational awareness, especially in disaster situations. This article states that limited timing and incomplete information can create significant challenges in planning, but having a comprehensive plan can improve the accuracy and efficiency of the response. EOCs play a vital role in disaster response, and therefore, the continuity of services in disaster management is crucial for EOCs. Still, these centers may face challenges that disrupt continuity in decision-making (25, 27).
K.S-Małyjurek et al. (28) investigated the challenges in coordination between different organizations in EOCs. They demonstrated that issues such as high information load and inter-organizational inconsistency can impact the continuity of services during emergencies and disasters. This study proposes strategies to enhance coordination and improve information management, including strengthening coordination and information management within EOCs to ensure the continuity of services.
During the last global pandemic, COVID-19, EOCs played a crucial role in facilitating pandemic management. Following the World Health Organization’s announcement of the COVID-19 pandemic, Iran was also affected on February 19, 2020. By the end of October 2024, the number of confirmed COVID-19 patients in Iran was about 7,627,186, and the number of deaths was about 164,000 (29). According to the database of Zahedan University of Medical Sciences (ZUMS), since the beginning of the COVID-19 pandemic worldwide, Sistan and Baluchistan province has experienced three waves of disease outbreaks: in June 2020, October 2020, and May 2021. These statistics show that COVID-19 has had a broad impact on Iranian society, and a significant number of people have been affected by this disease (30).
Indeed, effective management in EOCs plays a crucial role in controlling crises and pandemics, as well as coordinating and enhancing the efficiency of measures. Since managers’ success in incident management depends on proper performance during disasters, it is necessary to identify the vulnerable points of the health system in disaster management to intervene effectively and improve performance as a result. Considering the importance of the incident command center’s efficiency in responding to disasters and incidents, this study aims to evaluate the effectiveness of the IMS at ZUMS and Health Services, one of the key response organizations in incidents and disasters during pandemic conditions.
Materials and methods
The current research was a cross-sectional study that investigated the efficiency of Zahedan University of Medical Sciences’ incident management system in 2019 in responding to the pandemic. The study population of all the members of the research community, i.e., managers of the university incident command and operational managers, based on the different departments of the EOC of the university and its subordinate cities, was expected to be 110 people, which included all the managers working in the university. The sampling method employed was a census, and all EOC managers, including senior, middle, and operational levels, were invited to participate in the study. However, 82 people cooperated to complete the evaluation questionnaire despite trying to maximize the number of participants. The questionnaire for managers working in Zahedan City was completed in person, while for other cities, the questionnaire was emailed, and participants were guided by phone coordination. After completing the questionnaires, we received them by post. The criteria for inclusion in the study was membership in the incident command system, and the exclusion requirement was the unwillingness to participate.
The data collection tool was a questionnaire prepared based on the national checklist for evaluating managerial functions in the preparation and response phases, as outlined in the national program for the health system’s response to disasters and emergencies, as notified by the Ministry of Health, Treatment, and Medical Education of Iran. Two indexes, the content validity index (CVI) and the content validity ratio (CVR), were employed to assess the content validity of the research tool. The validity of the questionnaire was evaluated by sending it to 10 health experts in disaster management, and their correction comments were incorporated into the final questionnaire. The CVI value obtained was 0.85, indicating strong content validity. Additionally, a CVR value of 0.70 was calculated, indicating the need to ask questions based on experts’ opinions. The reliability of the questionnaire was measured through a panel of experts and using Cronbach’s alpha coefficient (α = 0.89).
The questionnaire included a demographic information section with nine questions to collect data, and 80 questions were evaluated to measure the functions of the Emergency Operation Plan (EOP). The main questions were scored using a Likert scale of “very poor,” “poor,” “average,” “good,” and “excellent.” The total score of the main questions was categorized between 80 and 400. All the questionnaire questions are listed in Table 1.
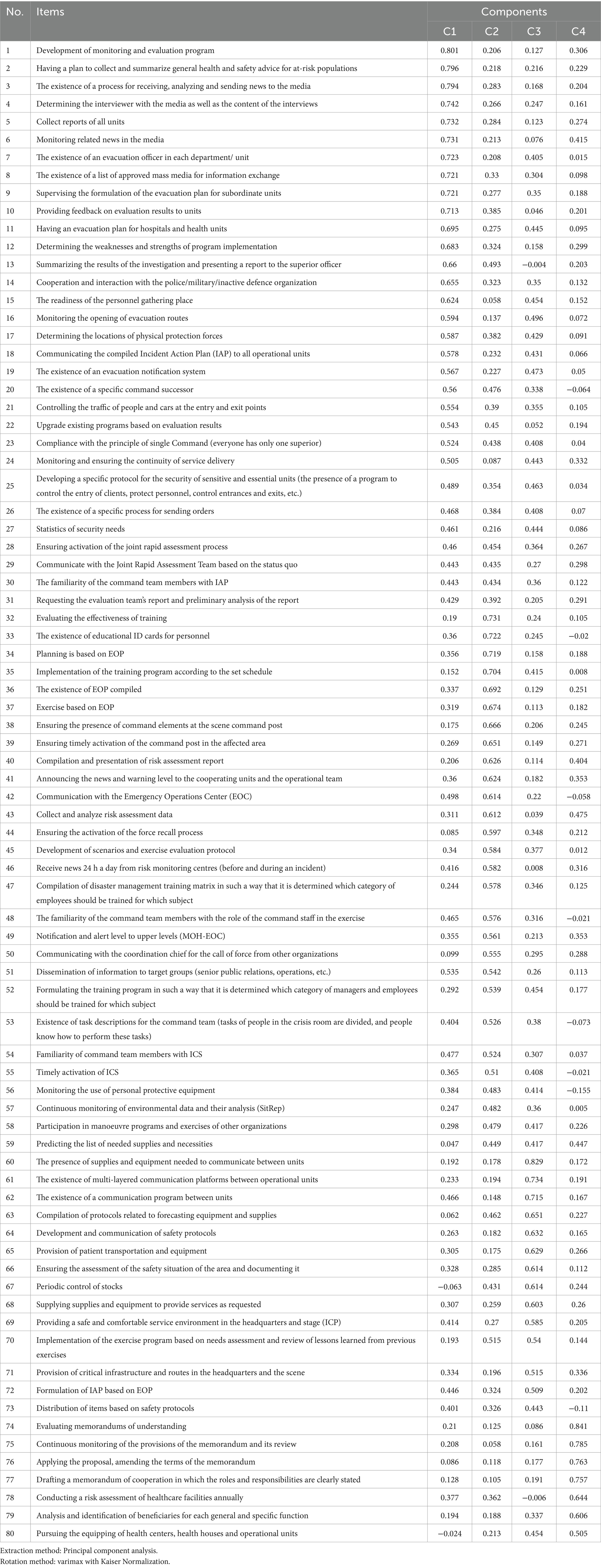
Table 1. Components and coefficients of each of the study indices (questions), extracted from PCA in participants of the incident management system of Zahedan University of Medical Sciences.
Due to the large number of questions in the questionnaire and the inability to perform applied analyses, such as regression models, directly on these questions, it was necessary to extract latent variables from the data. For this reason, analysis methods that reduce the dimensions of the data, such as factor analysis, had to be used; therefore, the Principal Component Analysis method was used to reduce the dimensions of the data. PCA is used to reduce the dimensions of many variables (questions) related to each other. PCA primarily aims to replace many correlated variables with uncorrelated principal components in regression models, thereby mitigating concerns about collinearity. The model’s first few principal components account for the most significant proportion of the total variance. The rationale for using PCA is to reduce the data’s complexity, increase the accuracy of the analysis by reducing information noise, and identify structures and patterns that may not be easily observed (31). To perform this analysis, first, KMO and Bartlett’s tests were performed for the possibility of PCA, which, according to the value of KMO = 0.907, was higher than 0.5 (32). The value of Bartlett’s statistic is 8253.894 with 2,628 degrees of freedom and a p value of less than 0.001, indicating a significant correlation between the questions. This correlation is large enough for PCA, and our data are deemed suitable for performing PCA. Then, based on the screen plot, where the point of curvature was detected in component number 4, and the total variance table was explained, the number of 4 components with a total variance of 62.888% of the total Variance of the variables (questions) explained by them, remained in the analysis (Figure 1; Table 2). Sometimes, there are defects in orthogonal models, such as non-uniformity of the explained variance distribution (so that the most considerable variance is related to the first component); there is a relationship between the variables with more than one component, so that cannot be identified the main component related variable and the coefficients of the variables are not close to 1 (high impact of the component on the variable) or zero (low impact of the component on the variable). In this case, different rotation methods will be used, the most common of which is varimax, which will solve the mentioned problems to a large extent (31). Therefore, using Varimax rotation, the coefficients of each question were determined in four components (Table 1). Then, by consulting the relevant experts, these components were named based on the questions that had the highest coefficients in each component. The questions of these components were named as follows: 31 questions in the first component (C1) with the name of Comprehensive risk planning, 28 questions in the second component (C2) under the title of Command and empowerment of operational teams, 14 questions in the third component (C3) with the name of Support and continuity of service and seven questions for the fourth component (C4) under the title of Developing and strengthening inter-sectoral cooperation. This study analyzed the components as scores and compared them to other variables, such as gender and education. Therefore, the ANOVA method was used to compare the average scores of the extracted components across different categories of measured variables. One of the assumptions of ANOVA is that the variance components in various categories of comparable variables are homogeneous. If this homogeneity of variances was not established in different classes, the Kruskal-Wallis method was used. SPSS 27 software was used for data analysis, with a significance level 0.05 in all tests.
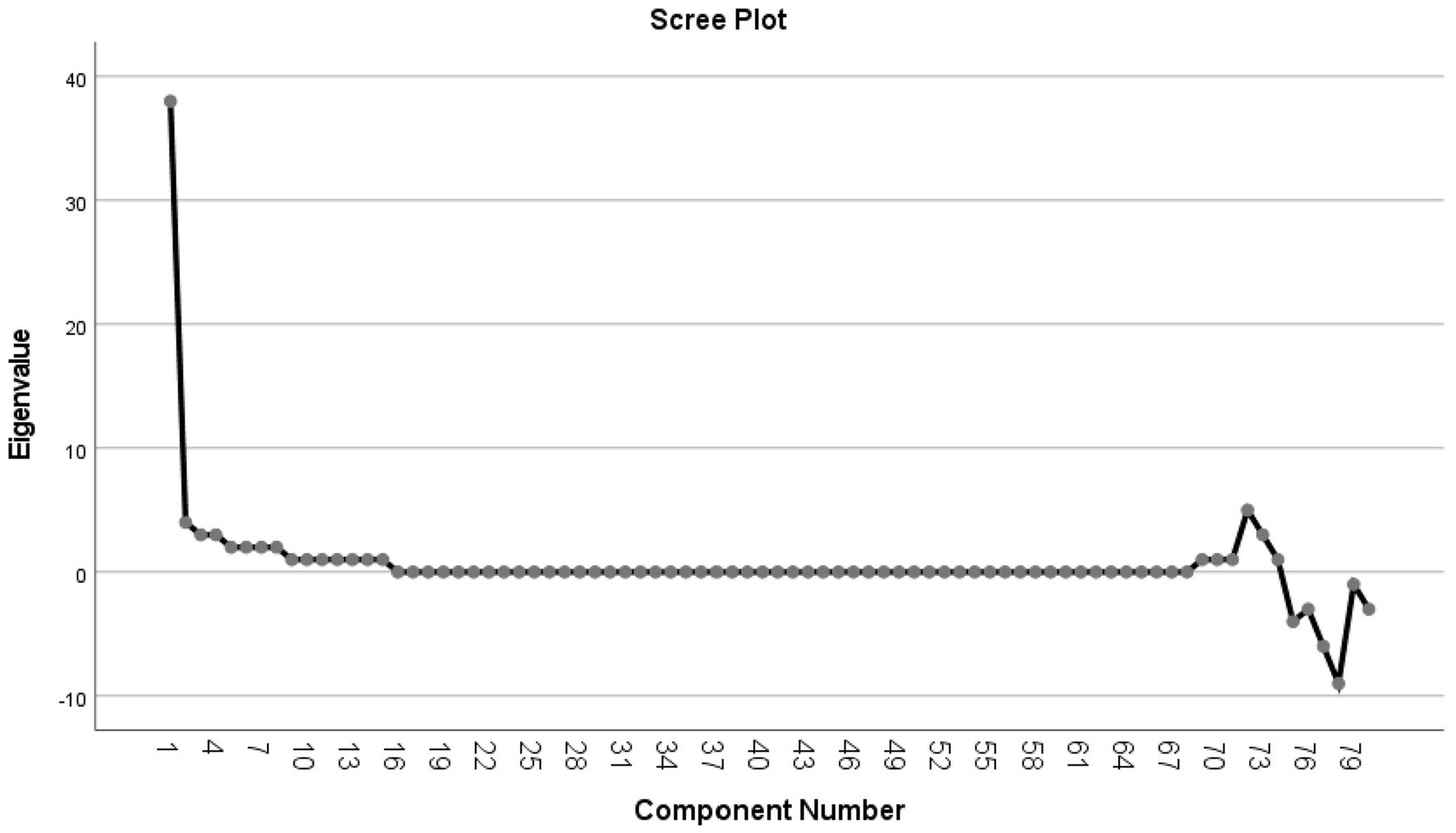
Figure 1. Scree plot of the component number and eigenvalues of questions based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
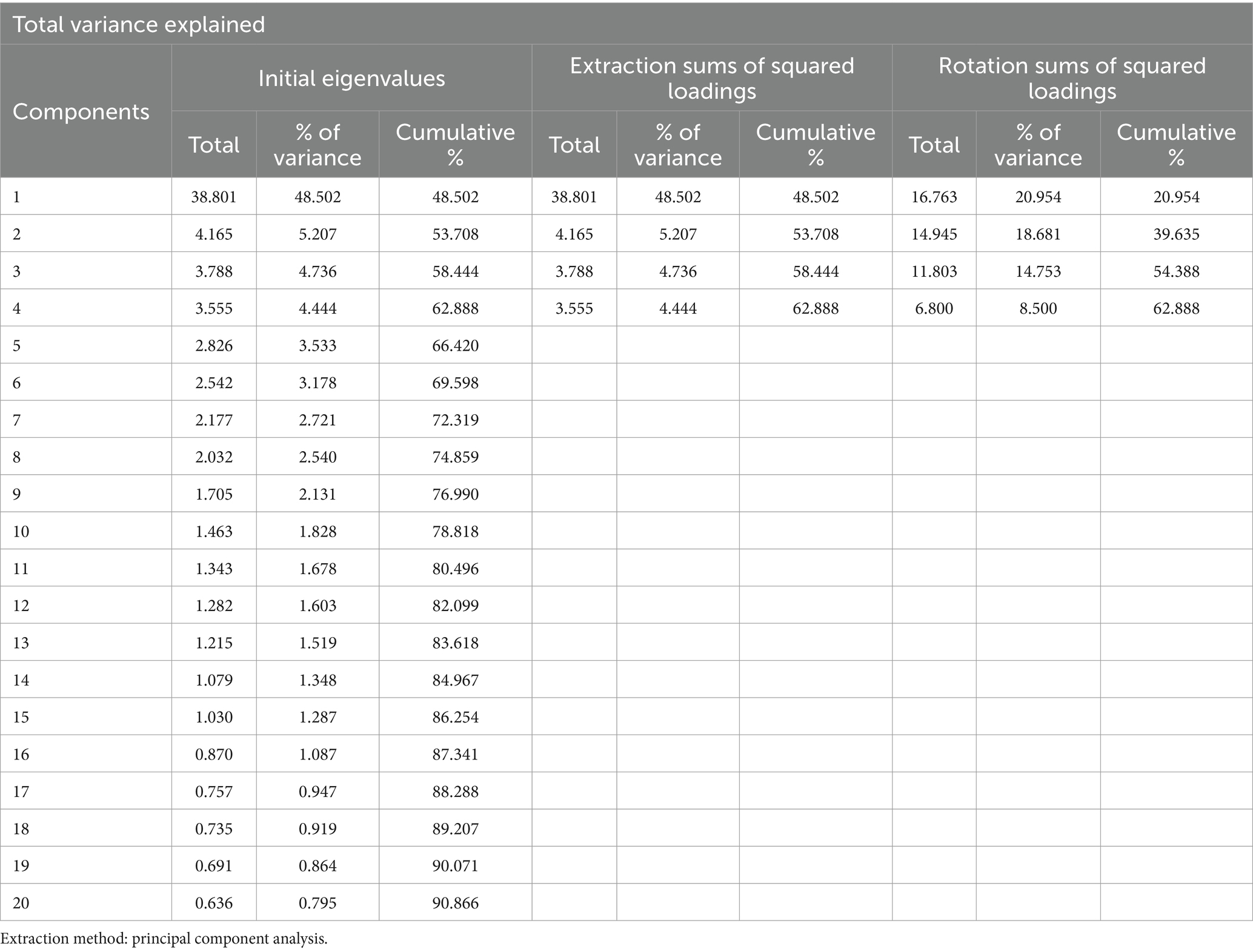
Table 2. The total variance explained extracted from PCA in participants of the incident management system of Zahedan University of Medical Sciences (Up to component 20 for brevity).
Results
Demographic
This study included 82 senior, middle, and operational managers from the university’s Incident Command System (ICS). The average age of these managers was 40.9 years, with a standard deviation of 7.96 years. Twenty women (24.4%) and 62 men (75.6%) participated. The education of the participants was as follows: 46 (56.1%) were bachelor’s degree holders, 20 (24.4%) were master’s degree holders, 8 (9.8%) were general practitioners, 2 (2.4%) PhD, 5 (6.1%) were clinical specialists, and 1 (1.2%) was a subspecialist. Additionally, in terms of field of study, 36 people (43.9%) studied health, 27 people (32.9%) studied medicine and paramedicine, and 19 people (23.2%) studied the humanities. Of the participants in the study, 47 individuals (57.3%) worked in the district health network, 30 individuals (36.6%) worked in hospitals, and five individuals (6.1%) worked in the crisis command headquarters. The working experience of managers ranged from 3 to 38 years, with a standard deviation of 8.8 years. The employment status of 43 people (52.4%) was official, 21 people (25.6%) held limited-term contracts, and 18 people (22.0%) were employed on a contract basis. Twenty-three managers (28.0%) did not have the experience of being in any crisis; 20 of them (24.4%) were present in only one crisis, and 39 (47.6%) experienced more than one crisis. Among the managers participating in the study, 80 people (97.6%) had participated in crisis management training courses. Of these, 40 people (48.8%) had participated in one course, and the remaining 40 had participated in more than one course. The managerial titles of the people participating in the study are listed in Table 3. The highest frequency was associated with health operations managers (18.3%), who were crucial in responding to crises and managing healthcare services.
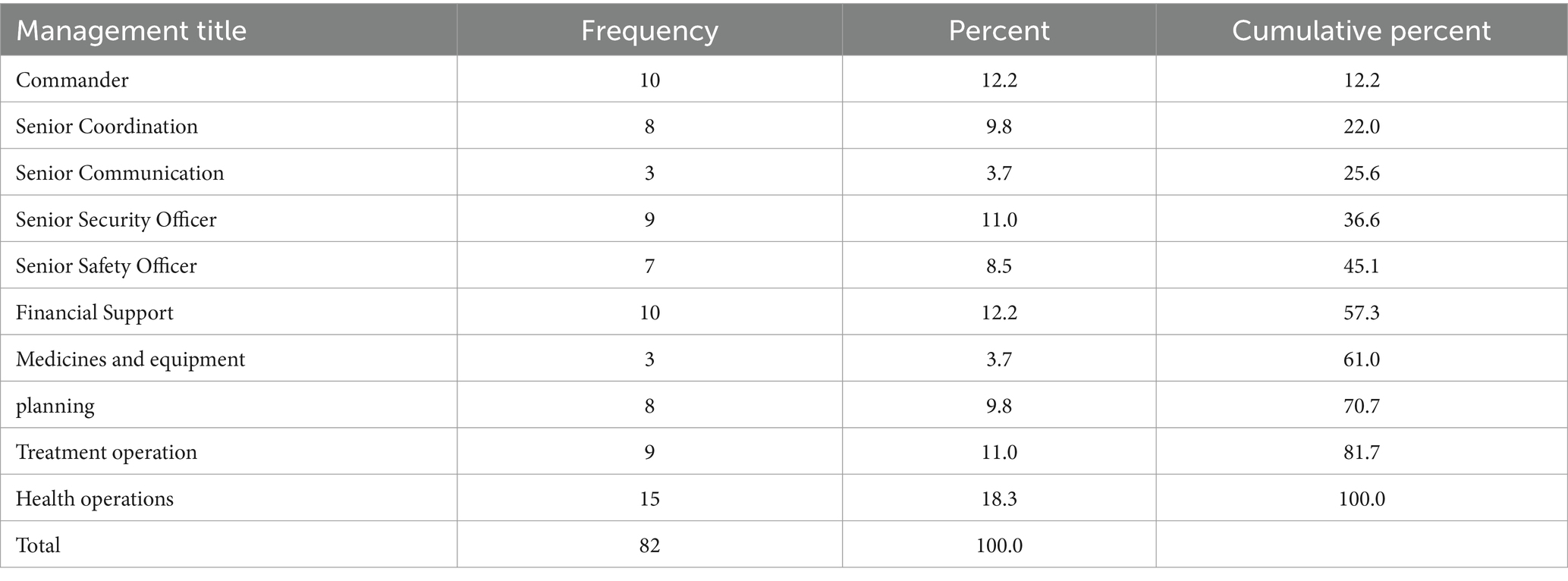
Table 3. The distribution of the organizational posts of managers in participants of the incident management system of Zahedan University of Medical Sciences.
PCA results
The average, standard deviation, minimum, and maximum scores obtained in the four components by the studied managers are listed in Table 4. The highest average score was related to the Command and empowerment of operational teams (C2), with an average of 3.72 (CI: 3.04–4.40). The component of Developing and strengthening inter-sectoral cooperation (C4) had the lowest average among the components, with a mean of 3.41 (CI: 2.61–4.21). The standard deviation of 0.80 also indicated significant differences in managers’ ability to develop and strengthen interdepartmental cooperation.
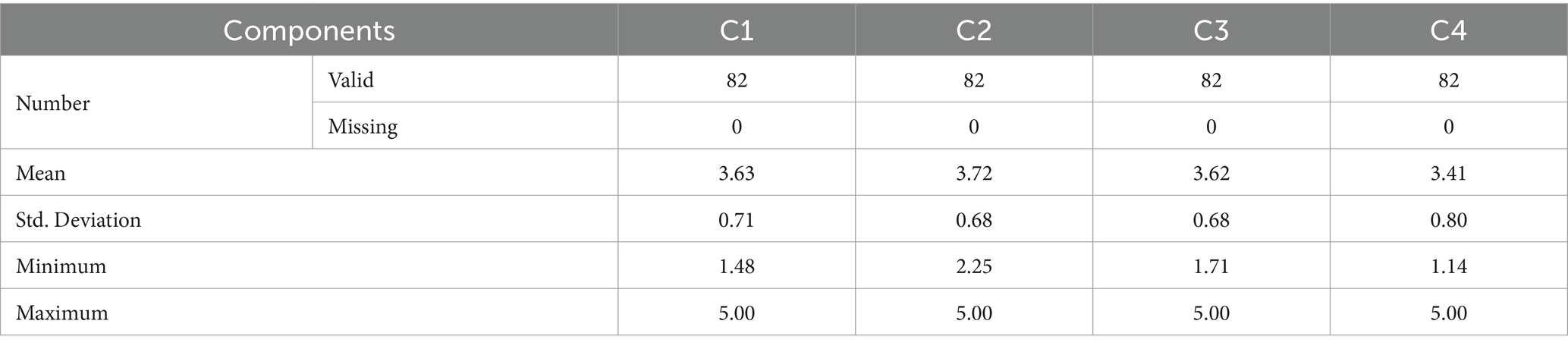
Table 4. The distribution of average, standard deviation, minimum, and maximum scores by four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
ANOVA/Kruskal-Wallis findings
In the analysis of Variance (ANOVA), the average answers of managers at the three levels of the crisis management headquarters, the health network, and hospitals to the questions in the first three components had significant differences. Still, this difference was not significant in C4. The managers of the crisis management headquarters demonstrated a better performance in Comprehensive risk planning (C1). Managers at different management levels performed differently in C2. The managers of the crisis management headquarters performed better in the Command. The average scores for the third component differed across management levels. No significant difference was observed in C4, which shows that all management levels generally performed similarly in developing interdepartmental cooperation (Table 5). Additionally, the average responses of managers, categorized by those holding a bachelor’s degree or higher, in components 1 and 2, showed significant differences.
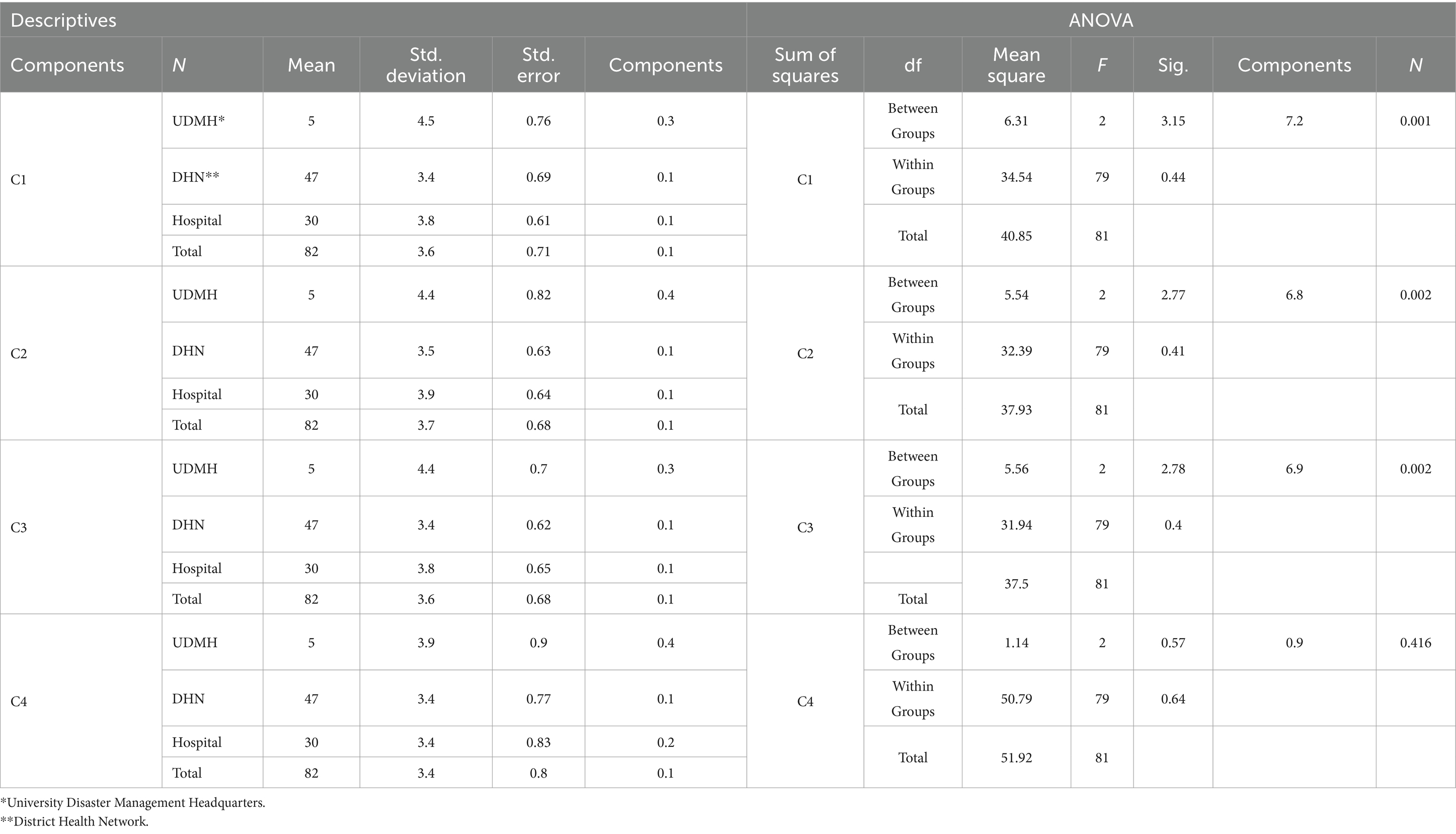
Table 5. Mean distribution and analysis of variance of the difference between the mean scores of questions related to management hierarchy by four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
In contrast, in the other two components, these differences were not significant. Managers with higher education (master’s degree and above) performed better in Comprehensive risk planning, and higher education increased their ability to command and lead operational teams (Table 6). Considering that the homogeneity of variances test was significant for the age groups and that these variances showed significant differences across different age groups, the Kruskal-Wallis test was used instead of ANOVA. In this test, it was found that there was a significant difference between the average answers of the managers to the questions in the two components, C2 (p = 0.04) and Support and continuity of service (C3) (p = 0.024).
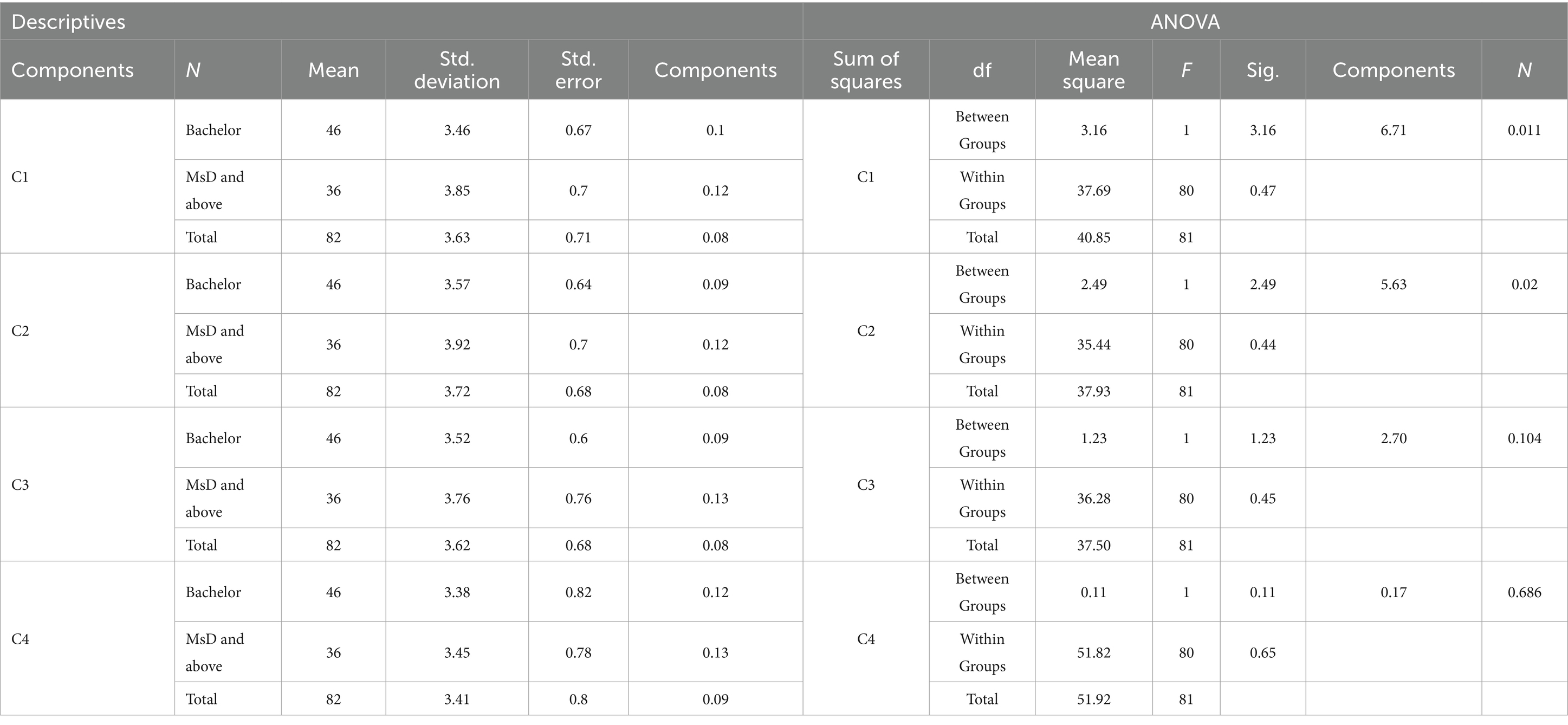
Table 6. Mean distribution and analysis of variance of the difference between the average scores of the questions related to the educational level by four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
These findings indicate that managers aged 30–40 years have given higher scores in these two areas than other groups. (Tables 7, 8) Participants with a history of attending the crisis had significantly higher average scores on the questions. In all extracted components, these differences were significant, especially in the first component (C1), which had a significance level of 0.002 (Tables 9, 10).

Table 7. The descriptive table of the Kruskal-Wallis test, the difference between the average scores of the questions related to age groups by four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.

Table 8. The Kruskal-Wallis test, the difference between the average scores of the questions related to age groups by four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
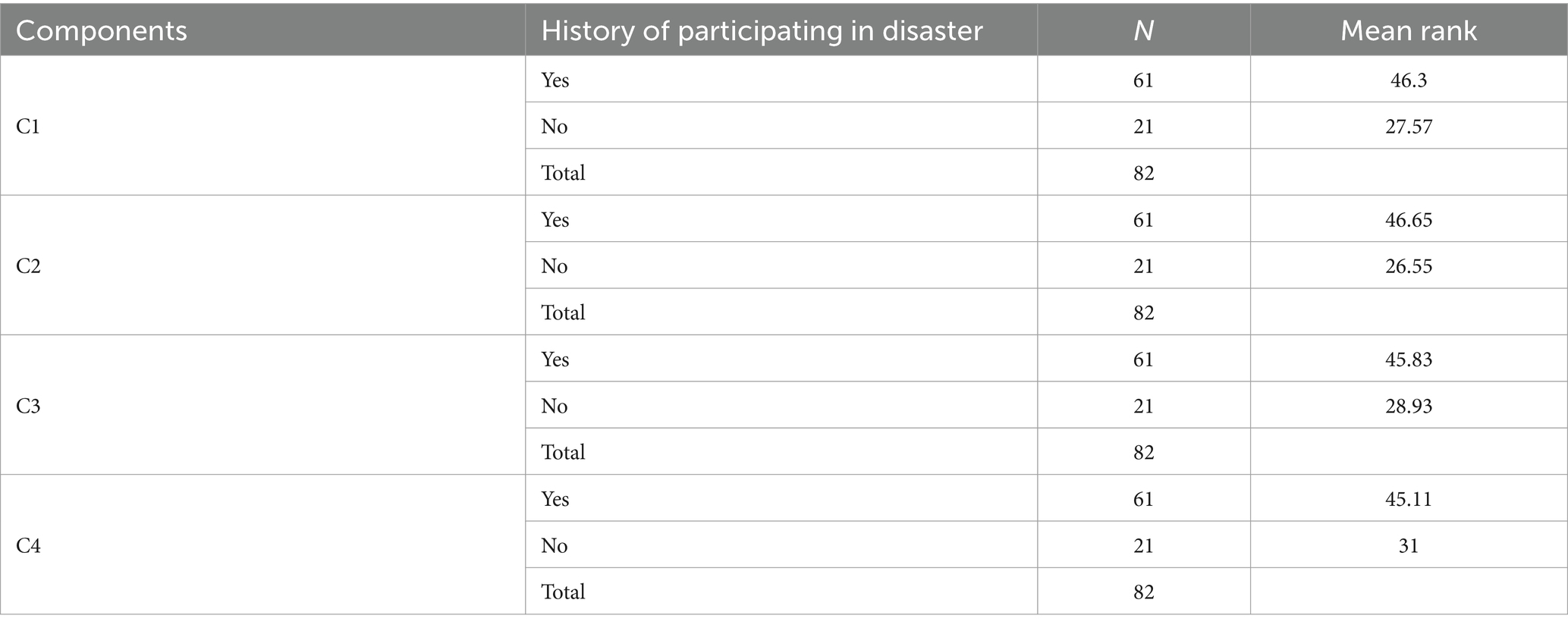
Table 9. The descriptive table of the Kruskal-Wallis test, the difference between the average scores of the questions related to the history of presence in the crisis according to the four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.

Table 10. The Kruskal-Wallis test, the difference between the average scores of the questions related to the history of presence in the crisis according to the four components based on PCA in participants of the incident management system of Zahedan University of Medical Sciences.
The average answers of the managers to the questions in the four components, according to the different classes of the other investigated variables that were included in the analysis, including the field of study (health, medical, and human sciences), the type of employment (official, contractual and limited-term contract), crisis management training courses, management position (Table 3) and job history (years of working) had no significant difference.
Discussion
Emergency Operation Centers’ (EOC) primary duties are coordination, communication, allocation and tracking of resources, collection, analysis, and dissemination of information. Also, these centers play an essential role in monitoring the current situation and providing a platform for health professionals to analyze the collected data and perform risk assessments based on it (33). On the other hand, the effective use of EOC and Incident Management System (IMS), especially in countries that face limited resources, has an essential role in political commitment, public participation, accountability, and strategic and operational changes and can be a tool to improve performance and use data for Provide accountability of health workers (16). Empowering EOC members to increase the competencies and self-confidence of the center members has an effective role in the appropriate response to emergencies and improving the efficiency of these centers in response to incidents and disasters (34). The efficiency of these centers leads to a significant difference in the number of injuries and the speed of response to the incident (35).
The present study showed a significant difference between the management level and C1, C2, and C3 scores (Table 5). The significant difference between the scores of EOC managers in university headquarters and EOC managers in health networks and hospitals is related to the scope and complexity of tasks, the amount of coordination required, and the scope of their effects. At the EOC level of the university headquarters, the scope of duties and responsibilities requires more comprehensive planning. Managers in this field should be able to anticipate possible challenges and plan for appropriate responses on a wide scale of society with a strategic approach and accurate knowledge of existing resources and capacities (36). On the other hand, the activities of EOC managers in hospitals and health networks are more focused on specific health crises and risks. Hence, their management framework is more limited and specialized (37).
The continuity of service in the university headquarters’ EOC includes educational, research, and administrative functions, which require more complex management (27). In contrast, the continuity of service in the EOC in hospitals and health networks means providing medical services to patients (38). Bandr Mzahim’s study showed that hospitals focus on solving hospital-specific challenges, including managing mass casualties and epidemics in emergencies and addressing hospital-specific needs, such as patient management, staffing, and medical equipment supply, to ensure the hospital’s delivery of care during a crisis (39). Due to being involved with different groups, including researchers, students, and technical staff, the EOC of the university headquarters needs a higher level of coordination and Command, and to empower these teams, it is required to use different specialties and communicate with related institutions at the national and international level (22). At the same time, the activities of EOC managers in hospitals and health networks are focused on teams providing medical services. The Command aims to facilitate crisis response operations and provide urgent health and medical services (38). It seems that the difference in the average score of the managers working in the EOC of the university headquarters in these three areas compared to the EOC managers of health and treatment networks and hospitals can be explained by the higher complexity and scope of their duties and the need to coordinate with a more significant number of stakeholders.
In components 1 and 2 (C1 and C2), people with higher education (master’s degree and above) scored better. The average score obtained by people with a bachelor’s degree or lower in all four fields was lower than those with a master’s degree or higher (Tables 6, 7). With the increase of specialized knowledge and analytical skills, the ability in Comprehensive risk planning and people’s leadership and command skills will increase. These people can better lead operational teams and provide effective crisis management plans. This finding was in line with the results of Xu’s study, which showed that a higher level of education can help improve the ability to plan and make decisions in critical situations (20). David A.L. Coldwell also showed that managers with a high level of education have a better position to predict and prevent crises, analyze complex situations, allocate resources effectively, and use scientific data in their decision-making processes. This educational context leads to the successful management of crises (40). Higher education enhances one’s technical and managerial skills and helps strengthen the skills needed to deal with complex crises.
Based on the study’s findings, people aged 30–40 years presented significantly higher scores in C2 and C3. Also, the average score these people gave in C1 and C4 was higher than other age groups, although these differences were insignificant. In this comparison, the age group below 30 presented lower scores (Tables 7, 8), which can be related to their less experience and less management skills. As individuals progress through chronological stages of development, their cumulative experiential knowledge and cognitive maturation facilitate enhanced decisional efficacy and predictive capabilities in complex, high-stakes environments, potentially optimizing leadership performance and strategic response mechanisms (41).
In their study, Gerry Larsson and Christina Björklund showed that older leaders make more effective decisions using better social skills and experience but still face reduced cognitive abilities in complex situations. Therefore, combining training for young leaders and using the expertise of older leaders can help improve leadership performance in organizations (42).
The present study showed a significant relationship between the experience of past crises and C1, C2, C3, and C4 scores. People who have been present in crises in the past gave higher scores in all the examined areas. This finding was consistent with the results of Shuaib et al.’s study. Previous experience in crisis management can help improve EOC performance in managing health crises and reducing the burden of disease and mortality caused by pandemics (16, 18). On the other hand, it seems that the history of being in previous crises increases the perceived self-efficacy of managers. It is necessary to put the managers in similar crises through training and practice by holding full-scale exercises while familiarizing people with the description of their duties and roles in a crisis, times of crisis, and better preparation in response operations to reduce the effect of company disasters (43, 44).
The systematic collection of information on the current situation, data analysis for risk assessment, and provision of an analytical platform for health professionals expand existing knowledge in crisis management and significantly impact the development and flexibility of health systems (45, 46). Organizational knowledge management, recording and documenting past crises’ experiences, and transferring experiences between different levels by EOCs are essential in promoting managerial knowledge and improving crisis preparedness (46). Encouraging managers to continue their studies at higher levels, holding specialized courses to strengthen analytical and management skills, special training for young managers (under 30 years old), holding full-scale maneuvers to simulate critical situations, using the experiences of experienced managers in training new employees, creating a recording and transferring system of the experiences of past crises, strengthening coordination between different levels, defining detailed job descriptions for each level, appropriate age composition in management teams (using the knowledge of older people and the energy of younger people) and improving decision-making skills in crises can help to improve performance of EOCs (47–50). Training, technology, inter-sectoral cooperation, optimal resource allocation, and the creation of local and national structures are recommended to improve crisis management and increase efficiency in disaster response. Evidence-based training and ongoing exercise programs, such as those conducted by the China Centers for Disease Control (China CDC), can improve staff productivity and coordination in crisis management. The use of digital technologies and the creation of virtual operations centers, which have shown their effectiveness during the COVID-19 pandemic, play an essential role in improving processes and human resource management. Establishing integrated crisis management structures and strengthening cross-sector collaboration, such as Pakistan’s experience with dengue fever, can increase the speed and effectiveness of responses. Improving resource allocation processes and using two-stage systems can reduce response times and improve operational accuracy. Also, establishing emergency operations centers at the local level, similar to the Nigerian experience, would help improve coordination and respond more quickly to health crises (24, 51–54).
Conclusion
Effective EOCs can reduce pressure on health infrastructure by improving access to resources, reducing response times, and strengthening intersectoral collaboration. As global health threats escalate, this study offers timely insights into optimizing the performance of EOCs to mitigate the impacts of epidemics. By implementing recommendations to improve training, invest in human resources, and intersectoral collaboration, policymakers and health leaders can enhance the effectiveness of EOCs and strengthen their capacity to manage major health crises. Emergency Operations Centers (EOCs) play a crucial role in coordinating and improving the effectiveness of health crisis responses during infectious pandemics. The efficiency of EOCs in their core functions, including resource coordination, strategic communication, data analysis, and follow-up actions, is crucial in improving preparedness and response, leading to increased resilience of health systems and the promotion of public health in emergencies. The results of this study emphasize that investing in the development and empowerment of EOCs, primarily through applying past knowledge and experiences and holding regular exercises, will strengthen organizational responses and, consequently, reduce the harm caused by health crises. It is suggested that future research should examine the long-term impacts of these centers in response to pandemics in greater detail, providing a basis for more sustainable policymaking in managing future crises. The evidence presented in this study should inform global health systems in developing Emergecy Operations Centers (EOCs) for epidemic response. Future research is recommended to investigate the long-term effectiveness of EOCs, informing evidence-based improvements in epidemic preparedness and response strategies.
Limitations
Sampling was designed as a census, but out of 110 people invited to complete the questionnaire, only 82 (74.5%) responded, which was a limitation of this study. Due to resource limitations, our study was conducted at Zahedan University of Medical Sciences, which may limit the generalizability of the results. Also, due to resource limitations, it was not possible to conduct face-to-face interviews with the samples, and the questionnaires were completed in a self-reported manner. To the extent possible, and with the necessary training over the phone, efforts were made to minimize information bias and selection bias.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MaS: Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing. AA: Conceptualization, Data curation, Investigation, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. AP: Data curation, Supervision, Writing – review & editing. MoS: Writing – original draft, Writing – review & editing. HF: Conceptualization, Supervision, Writing – review & editing. AT: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to express our sincere gratitude to all the participants in this study who shared their valuable information and helped us collect the data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
PCA, Principal Component Analysis; IAP, Incident Action Plan; EOP, Emergency Operation Plan; EOC, Emergency Operation Center; ICP, Incident Command Post; ICS, Incident Command System.
References
1. Topluoglu, S, Taylan-Ozkan, A, and Alp, E. Impact of wars and natural disasters on emerging and re-emerging infectious diseases. Front Public Health. (2023) 11:1215929. doi: 10.3389/fpubh.2023.1215929
3. Trisal, A, Pandey, B, Mandloi, D, Sarsodia, T, and Dabade, SJ. Pandemics in human history: a study of origin, enormity, mortality rate and controlling strategies. Int J Life Sci Pharma Res. (2020) 10:L141–8. doi: 10.22376/ijpbs/lpr.2020.10.4.l141-148
4. Eteng, W, Lilay, A, Tekeste, S, Mankoula, W, Collard, E, Waya, C, et al. Strengthening response coordination through public health emergency operations centers in Africa: lessons learned from 56-week webinar sessions, 2020-2021. Med Rxiv. (2022). doi: 10.1101/2022.11.22.22282627
5. Wang, J, and Wang, Z. Strengths, weaknesses, opportunities and threats (SWOT) analysis of China’s prevention and control strategy for the COVID-19 epidemic. Int J Environ Res Public Health. (2020) 17:2235. doi: 10.3390/ijerph17072235
6. Heidari, M, Sayfouri, N, Miresmaeeli, SS, and Nasiri, A. Analysis of the man-made causes of shiraz flash flood: Iran, 2019. Prehosp Disaster Med. (2020) 35:588–91. doi: 10.1017/S1049023X20000795
7. Tourani, M, Çağlayan, A, Işık, V, and Saber, R. İran’da iklim değişikliğinin, klimatolojik, meteorolojik ve hidrolojik afetlere etkisi. Türk Coğrafya Dergisi. (2022) 80:97–114. doi: 10.17211/tcd.1085714
8. Ardalan, A, Mowafi, H, and Homa, YK. Impacts of natural hazards on primary health care facilities of Iran: a 10-year retrospective survey. PLoS. (2013) 28:5. doi: 10.1371/currents.dis.ccdbd870f5d1697e4edee5eda12c5ae6
9. Djalali, A, Hosseinijenab, V, Hasani, A, Shirmardi, K, Castrén, M, Öhlén, G, et al. A fundamental, national, medical disaster management plan: an education-based model. Prehosp Disaster Med. (2012) 27:345–52. doi: 10.1017/s1049023x00007524
10. Bloom, G, Mac Gregor, H, McKenzie, A, and Sokpo, E. Strengthening health systems for resilience. IDS Evidence Rep. (2015) 111:1–28.
11. Bahadori, M, Khankeh, HR, Zaboli, R, and Malmir, I. Coordination in disaster: a narrative review. Int J Med Rev. (2015) 2:273–81.
12. Khankeh, HR. Health care services at time of natural disasters: a qualitative study. Int J Disaster Risk Sci. (2007) 2:22–35.
13. Khankeh, HR, Khorasani-Zavareh, D, Johanson, E, Mohammadi, R, Ahmadi, F, and Mohammadi, R. Disaster health-related challenges and requirements: a grounded theory study in Iran. Prehosp Disaster Med. (2011) 26:151–8. doi: 10.1017/S1049023X11006200
14. Elmahal, OM, Abdullah, A, Elzalabany, MK, Anan, HH, Samhouri, D, and Brennan, RJ. Public health emergency operation centres: status, gaps and areas for improvement in the eastern Mediterranean region. BMJ Glob Health. (2022) 7:e008573. doi: 10.1136/bmjgh-2022-008573
15. Perry, RW. Incident management systems in disaster management. Disaster Preven Manage Int J. (2003) 12:405–12. doi: 10.1108/09653560310507226
16. Shuaib, FM, Musa, PF, Muhammad, A, Musa, E, Nyanti, S, Mkanda, P, et al. Containment of Ebola and polio in low-resource settings using principles and practices of emergency operations centers in public health. J Public Health Manag Pract. (2017) 23:3–10. doi: 10.1097/PHH.0000000000000447
18. Okware, SI, Omaswa, F, Talisuna, A, Amandua, J, Amone, J, Onek, P, et al. Managing Ebola from rural to urban slum settings: experiences from Uganda. Afr Health Sci. (2015) 15:312–21. doi: 10.4314/ahs.v15i1.45
19. Olu, OO, Lamunu, M, Chimbaru, A, Adegboyega, A, Conteh, I, Nsenga, N, et al. Incident management systems are essential for effective coordination of large disease outbreaks: perspectives from the coordination of the Ebola outbreak response in Sierra Leone. Front Public Health. (2016) 4:254. doi: 10.3389/fpubh.2016.00254
20. Xu, M, and Li, S-X. Analysis of good practice of public health emergency operations centers. Asian Pac J Trop Med. (2015) 8:677–82. doi: 10.1016/j.apjtm.2015.07.006
21. Ardiansyah, M, Mirandah, E, Suyatno, A, Faqih, M, and Muazzinah, M. Disaster management and emergency response: improving coordination and preparedness. Global Int J Innov Res. (2024) 2:831–9. doi: 10.59613/global.v2i4.129
22. Eteng, W-EO, Lilay, A, Tekeste, S, Mankoula, W, Collard, E, Waya, C, et al. Strengthening COVID-19 pandemic response coordination through public health emergency operations centres (PHEOC) in Africa: review of a multi-faceted knowledge management and sharing approach, 2020–2021. PLOS. Glob Public Health. (2023) 3:e0001386. doi: 10.1371/journal.pgph.0001386
23. Malik, MW, Ikram, A, Safdar, RM, Ansari, JA, Khan, MA, Rathore, TR, et al. Use of public health emergency operations center (PH-EOC) and adaptation of incident management system (IMS) for efficient inter-sectoral coordination and collaboration for effective control of dengue fever outbreak in Pakistan-2019. Acta Trop. (2021) 219:105910. doi: 10.1016/j.actatropica.2021.105910
24. Ansell, C, Boin, A, and Keller, A. Managing transboundary crises: identifying the building blocks of an effective response system. J Conting Crisis Manage. (2010) 18:195–207. doi: 10.1111/j.1468-5973.2010.00620.x
25. Allen, T, and Spencer, R. Barriers and enablers to using an emergency operations center in public health emergency management: a scoping review. Disaster Med Public Health Prep. (2023) 17:e407. doi: 10.1017/dmp.2023.50
26. Ryan, M. Planning in the emergency operations center. Technol Forecast Soc Chang. (2013) 80:1725–31. doi: 10.1016/j.techfore.2013.01.006
27. Cavaliere, P, Cox, Z, Kendra, J, Mankins, A, Michaud, M, Nibbs, F, et al. A research agenda to explore the emergency operations center. J Emerg Manage. (2020) 18:525–34. doi: 10.5055/jem.2020.0499
28. Sienkiewicz-Małyjurek, K, and Owczarek, T. Complementarity of communication and coordination in ensuring effectiveness of emergency management networks. Sustain For. (2020) 13:221. doi: 10.3390/su13010221
29. Mathieu, E, Ritchie, H, Rodés-Guirao, L, Appel, C, Giattino, C, Hasell, J, et al. Coronavirus pandemic (COVID-19). Our World in Data. (2020). Available online at:https://ourworldindata.org/coronavirus.
30. Khalagi, K, Gharibzadeh, S, Khalili, D, Mansournia, MA, Samiee, SM, Aghamohamadi, S, et al. Prevalence of COVID-19 in Iran: results of the first survey of the Iranian COVID-19 serological surveillance programme. Clin Microbiol Infect. (2021) 27:1666–71. doi: 10.1016/j.cmi.2021.06.002
31. Kherif, F, and Latypova, A. Principal component analysis In: Machine learning : Elsevier. Academic Press (2020). 209–25. doi: 10.1016/B978-0-12-815739-8.00012-2
33. Federal Emergency Management Agency (FEMA). National Incident Management System. Washington, DC: FEMA (2017).
34. Abu Haleeqa, A, McIntyre, S, Al Afifi, S, Taqi, F, Butt, B, Simmons, R, et al., editors. Incident command virtual reality icvr immersive training system. Abu Dhabi International Petroleum Exhibition and Conference; (2018)
35. Shojaei, F, Qaraeian, P, Firoozbakht, A, Chhabra, D, and Jahangiri, K. The necessity for an integrated emergency operations center (EOC) among first responders: lesson learned from two Iranian railway accidents. Heliyon. (2023) 9:e15599. doi: 10.1016/j.heliyon.2023.e15599
36. Kumar, V, and Gupta, G. Strategic management during a pandemic. New York (NY): Routledge (2022).
37. Perry, RW. Emergency operations Centres in an era of terrorism: policy and management functions. J Conting Crisis Manag. (2003) 11:151. doi: 10.1111/j.0966-0879.2003.01104001.x
38. McLean, J, Clark, C, McKee, A, Legue, S, Cocking, J, Lamarche, A, et al. Pandemic responsiveness in an acute care setting: a community hospital’s utilization of operational resources during COVID-19. J Multidiscip Healthc. (2022) 15:1309–21. doi: 10.2147/JMDH.S361896
39. Mzahim, B, Alzahrani, A, Alzahrani, AA, Aldharman, S, Alkhamis, W, Almutairi, BS, et al. Incident management system comparison: hospital incident command system versus major incident medical management and support. Saudi J Health Sci. (2023) 12:178–87. doi: 10.4103/sjhs.sjhs_118_23
40. Coldwell, DA. Ethical leadership in crisis management: the role of university education In: A Alvinius, editor. Contemporary leadership challenges. London: Intech Open (2017). 115–30.
41. Scarpis, E, Bravo, G, Cocconi, R, and Brunelli, L. The most challenging COVID19 phases and the skills healthcare leaders need to face the pandemic. Eur J Pub Health. (2021) 31:iii345. doi: 10.1093/eurpub/ckab165.019
42. Larsson, G, and Björklund, C. Age and leadership: comparisons of age groups in different kinds of work environment. Manag Res Rev. (2020) 44:661–76. doi: 10.1108/MRR-01-2020-0040
43. Melnikov, S, Itzhaki, M, and Kagan, I. Israeli nurses’ intention to report for work in an emergency or disaster. J Nurs Scholarsh. (2014) 46:134–42. doi: 10.1111/jnu.12056
44. Aminafshar, A, Sartipi, M, and Pakzad, A. The perceived self-efficacy of senior, middle, and operations managers of the incident command system dealing with emergencies and disasters during the COVID-19 pandemic. BMC Emerg Med. (2023) 23:133. doi: 10.1186/s12873-023-00904-9
45. Emami, SG, Lorenzoni, V, and Turchetti, G. Towards resilient healthcare systems: a framework for crisis management. Int J Environ Res Public Health. (2024) 21:286. doi: 10.3390/ijerph21030286
46. World Health Organization. Strengthening the collection, analysis, and use of health workforce data and information: A handbook. Geneva: WHO (2023).
47. Dumulescu, D, and Muţiu, AI. Academic leadership in the time of COVID-19—experiences and perspectives. Front Psychol. (2021) 12:648344. doi: 10.3389/fpsyg.2021.648344
48. Tabesh, P, and Vera, DM. Top managers' improvisational decision-making in crisis: a paradox perspective. Manag Decis. (2020) 58:2235–56. doi: 10.1108/MD-08-2020-1060
49. McNamara, A. Crisis management in higher education in the time of Covid-19: the case of actor training. Educ. Sci. (2021) 11:132. doi: 10.3390/educsci11030132
50. Chernikova, O, Heitzmann, N, Stadler, M, Holzberger, D, Seidel, T, and Fischer, F. Simulation-based learning in higher education: a meta-analysis. Rev Educ Res. (2020) 90:499–541. doi: 10.3102/0034654320933544
51. Liu, MR, Ma, J, Shao, XY, Luo, HM, Liang, XF, Liu, DF, et al. Survey on provincial disease prevention and control professionals\u0027 attitudes and cognition to public health physician standardized training in China. Zhonghua Liu Xing Bing Xue Za Zhi. (2021) 42:935–40.
52. Sun, M, Xu, N, Li, C, Wu, D, Zou, J, Wang, Y, et al. The public health emergency management system in China: trends from 2002 to 2012. BMC Public Health. (2018) 18:1–9.
53. Peng, L. Crisis crowdsourcing and China’s civic participation in disaster response: Evidence from earthquake relief. China Inform. (2017) 31:327–48.
Keywords: efficiency, incident command system, pandemic, EOC, PCA
Citation: Sartipi M, Aminafshar A, Pakzad A, Shafiei M, Farahmandnia H and Tavan A (2025) Evaluating the efficiency of emergency operation centers during pandemics: a cross-sectional study with operational managers in Iran. Front. Public Health. 13:1511932. doi: 10.3389/fpubh.2025.1511932
Edited by:
Nicolai Savaskan, Public Health Service Berlin Neukölln, GermanyReviewed by:
Nathan Myers, Indiana State University, United StatesMohamed Elhakim, WHO Regional Office for the Eastern Mediterranean, Egypt
Roni Ekha Putera, Andalas University, Indonesia
Copyright © 2025 Sartipi, Aminafshar, Pakzad, Shafiei, Farahmandnia and Tavan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Asiye Aminafshar, YW1pbmFmc2hhcjY2MzFAZ21haWwuY29t