 Karen Belkić1,2,3,4*
Karen Belkić1,2,3,4*- 1Department of Oncology/Pathology, Karolinska Institute, Stockholm, Sweden
- 2Department of Medical Radiation Physics and Nuclear Medicine, Karolinska University Hospital, Stockholm, Sweden
- 3School of Community and Global Health, Claremont Graduate University, Claremont, CA, United States
- 4Institute for Health Promotion and Disease Prevention Research, University of Southern California School of Medicine, Los Angeles, CA, United States
Background: Physician burnout has become a public-health crisis. The need is dire for robust organizational solutions, focusing on reduction of specific stressors. The physician-specific Occupational Stressor Index (OSI) based on cognitive ergonomics can help. Individual-participant data (IPD) from different studies addressing physician burnout are lacking.
Aims: To perform IPD analysis regarding job stressors and their relation to physician burnout and to utilize the IPD results to inform a systematic review of the stressors that show an association with physician burnout, focusing on intervention studies.
Methods: PRISMA guidelines are followed for the IPD analysis and systematic review of intervention studies on the implicated stressors, taking the COVID-19 pandemic into consideration. The IPD analysis is performed on studies using the physician-specific OSI vis-à-vis burnout assessed by the Copenhagen Burnout Inventory (CBI). Odds ratios (OR) ± 95% confidence-intervals (CI) are reported, adjusting for age, gender and caring for patients with suspected COVID-19 infection.
Results: Three studies fulfilled the inclusion criteria, providing complete IPD data for 95 physicians. Thirty-two (33.7%) physicians had total OSI scores >88, for which intervention is urgently needed. Unit-change in the total stressor burden assessed via OSI yielded OR = 1.11 (95%CI: 1.03–1.18) (p = 0.003) for personal burnout, OR = 1.17 (95%CI: 1.08–1.26) (p = 0.0001) for work-related burnout and OR = 1.07 (95%CI: 1.01–1.15) (p = 0.03) for patient-related burnout. Caring for patients with suspected COVID-19 infection showed significant multivariable results (p = 0.04) only for personal burnout. Twenty distinct work stressors revealed multivariable associations with CBI. Systematic examination via PUBMED, CINAHL and OVID Medline yielded 33 publications mitigating those stressors among physicians. Adequate staffing was pivotal. Clerical staff off-loaded administrative burden. Information-technology staff helped diminish interruptions, enhancing workflow. Cross-coverage reduced time constraints, ensured separate periods for non-clinical tasks, and ≥1 work-free day/week. Several interventions impacted physician burnout, as did recognition of physicians' efforts/achievements. Other OSI-identified stressors were insufficiently examined in intervention studies: e.g. vacation; appropriately-timed, cross-covered restbreaks; and counter-measures for emotionally-disturbing aspects of MD's work, particularly during the pandemic.
Conclusions: Further participatory-action research is needed in well-controlled intervention trials to alleviate physician burnout.
1 Introduction
High rates of burnout have been reported among physicians for many years (1–3). In the most recent period, physician burnout has aroused even more attention, with the added burden of the COVID-19 pandemic (4–7). According to major health care organizations, physician burnout represents a public health crisis. Implicit in this clarion call is a call for action, especially given that burnout is reversible and preventable (8).
Having been rigorously selected to be mentally healthy and after finishing long, arduous preparation prior to starting actual professional life, a “super-healthy worker effect” is anticipated in physicians. Namely, compared to other populations, physicians would be expected to have far lower prevalence of untoward psychological outcomes (9). The fact that the situation is just the contrary, i.e., that burnout and even more serious mental health disorders, including risk of suicide, are actually more widespread among physicians (2, 10), strongly implicates exposure to deleterious work conditions. Consequently, identification of the contributory job stressors and, whenever possible, their alleviation, become the priority.
Of late, cognitive ergonomics and how it could inform interventions have received renewed attention directed toward physicians (11–13). Yet, there exists a comprehensive work stressor model based upon cognitive ergonomics and brain research (14), which has been effectively applied among several occupational groups, including physicians. That theory-based model, the Occupational Stressor Index (OSI), has been fully-operationalized specifically for physicians (15). The latter was achieved through “participatory action research” (16), reflecting hands-on experience and was presented to colleagues as “for physicians, by physicians” (15).
The overall stressor load of a given work environment is reflected in the total OSI score. When that exceeds the clinical cutpoint of 88, intervention is urgently required (17, 18). The OSI model includes major dimensions of the generic work stressor models, e.g., “high demands” (14, 19), operationalizing these concretely regarding time and allocation of mental resources, as germane to the specific occupation. Informed by cognitive ergonomics, the OSI model also considers other dimensions. In particular, the possibility of encountering harm contributes heavily to the stressor burden (14), with the nervous system selectively attending to threatening stimuli (20, 21). The term “threat avoidant vigilance” denotes having to follow such stimuli, responding quickly, with errors or delays having serious, potentially fatal consequences (14, 20, 22, 23). Without consideration of threat avoidant vigilance, the stressor burden of physicians, as well as that of nurses, airline pilots, professional drivers, police and firefighters, among others, is markedly underestimated (15, 18, 23). Importantly, the OSI includes stressor aspects such as threat avoidant vigilance, missing from the sociological models (14).
The OSI affords an in-depth qualitative and quantitative description of the stressor burden (15, 18, 23), similar to theory-guided, on-site evaluation of the mental structure of job tasks (24, 25). Since the OSI is questionnaire-based, it does not require on-the-job analysis, but its diagnostic accuracy can be thereby further enhanced. This is especially helpful for design and implementation of interventions.
The OSI questionnaires are constructed to be relevant and succinct, with the queries presented in an order which is logical for the participants from a given occupation. The responses are then coded according to the OSI model, such that all the specific OSI's are numerically and theoretically compatible. The OSI for physicians questionnaire and the OSI score sheet are available at Supplemental Digital Content, http://links.lww.com/SMJ/A230 and http://links.lww.com/SMJ/A231. Further details can be found in Belkić and Savić (18).
Burnout has been assessed with a number of validated instruments (26–29), as well as by some explicit, single-item queries (30–33). The Maslach Burnout Inventory (MBI) is based upon the original definition of burnout as a syndrome of “emotional exhaustion, depersonalization, and reduced personal accomplishment” (26). The Copenhagen Burnout Inventory (CBI) has been widely used in the international setting, being directly available without charge. According to its Authors, the CBI appropriately focuses on the key attribute of fatigue and exhaustion applied to specific domains of one's life. The CBI avoids queries concerning depersonalization that may elicit negative reactions in many cultures (29). There are three components in the CBI: (A) personal burnout, as physical and emotional exhaustion not explicitly connected to work; (B) work-related burnout, assessing how much the former is actually associated with one's job and (C) querying about the linkage between physical and emotional exhaustion while working with patients or other “clients” (29). The CBI is especially appropriate for physicians, and has been used in many health care settings internationally, prior to as well as during the height of the COVID-19 pandemic (3, 4, 6, 9, 29, 34–40).
There have been a number of published reviews addressing physician burnout, suggesting that individual-focused and organizational measures could help mitigate or prevent its occurrence (13, 41–46). However, the evidence is considered overall of low quality. In particular, organizational interventions that “focus on reduction of specific stressors” are sparse (45) (p. 2). The physician-specific OSI, with its basis in cognitive ergonomics, and objective, comprehensive, quantifiable assessment of work-conditions, could contribute to this goal. It also warrants note that, to the best of our knowledge after extensive searching, the published reviews on physician burnout have relied upon aggregate data from various publications. In other words, the original data on each participating physician have not been jointly analyzed across studies. Assessing individual-level data from all studies that address a specific clinical-research question is “considered a gold-standard approach to evidence synthesis” (47) (p. 1657). This is one of the aims of the present study, namely to perform individual participant data (IPD) analysis regarding job stressors and their relation to physician burnout. The physician-specific OSI will be the method of analysis for work conditions, with the CBI as the assessment measure of outcomes. The second aim is to utilize the results of the IPD to inform a systematic review of each of the stressors that show an association with physician burnout. The main focus of the latter will be to identify and assess published intervention studies targeting at the mitigation or elimination of the implicated work stressor among physicians. The impact of the COVID-19 pandemic will be taken into consideration throughout.
2 Methods
2.1 Eligibility criteria for the IPD
For inclusion in the IPD, study participants should have been full-time employed physicians, with the physician-specific OSI used to evaluate their work conditions and burnout assessed via the CBI, as the outcome, and basic demographic data (age and gender) available. There was no restriction on study design nor year(s) when conducted.
2.2 Identification of studies
The electronic search engines in this and all the other searches for this article were: PUBMED, CINAHL, and Ovid Medline, conducted through June 2024. Studies identified from other sources such as reference lists were also considered. As summarized in Figure 1 for the IPD studies, two search branches were implemented, with details in Supplementary material 1. The first search combined (physicians or doctors) with (Copenhagen Burnout Inventory or CBI). The second search combined (Occupational Stressor Index) with (health professionals). After merging the two branches, five studies were found applying the physician-specific OSI with burnout as an outcome. Two of these described a clinical interventional for a psychiatrist on sick-leave for burnout (18, 48). However, the Oldenburg Burnout Inventory had been used therein, such that these did not fully meet the requirements for the IPD. They were included in part II of the present paper, focusing on interventions. Three studies from two centers fulfilled all the inclusion criteria, yielding IPD data for 95–97 physicians (9, 34, 39). These fully anonymized data were made available for the present analysis. As per Goyal et al. (9), Belkić and Rustagi (34), and Nedić and Belkić (39), all the research, as well as the treatment of the current anonymized data are in full accordance with the World Medical Association's Declaration of Helsinki.
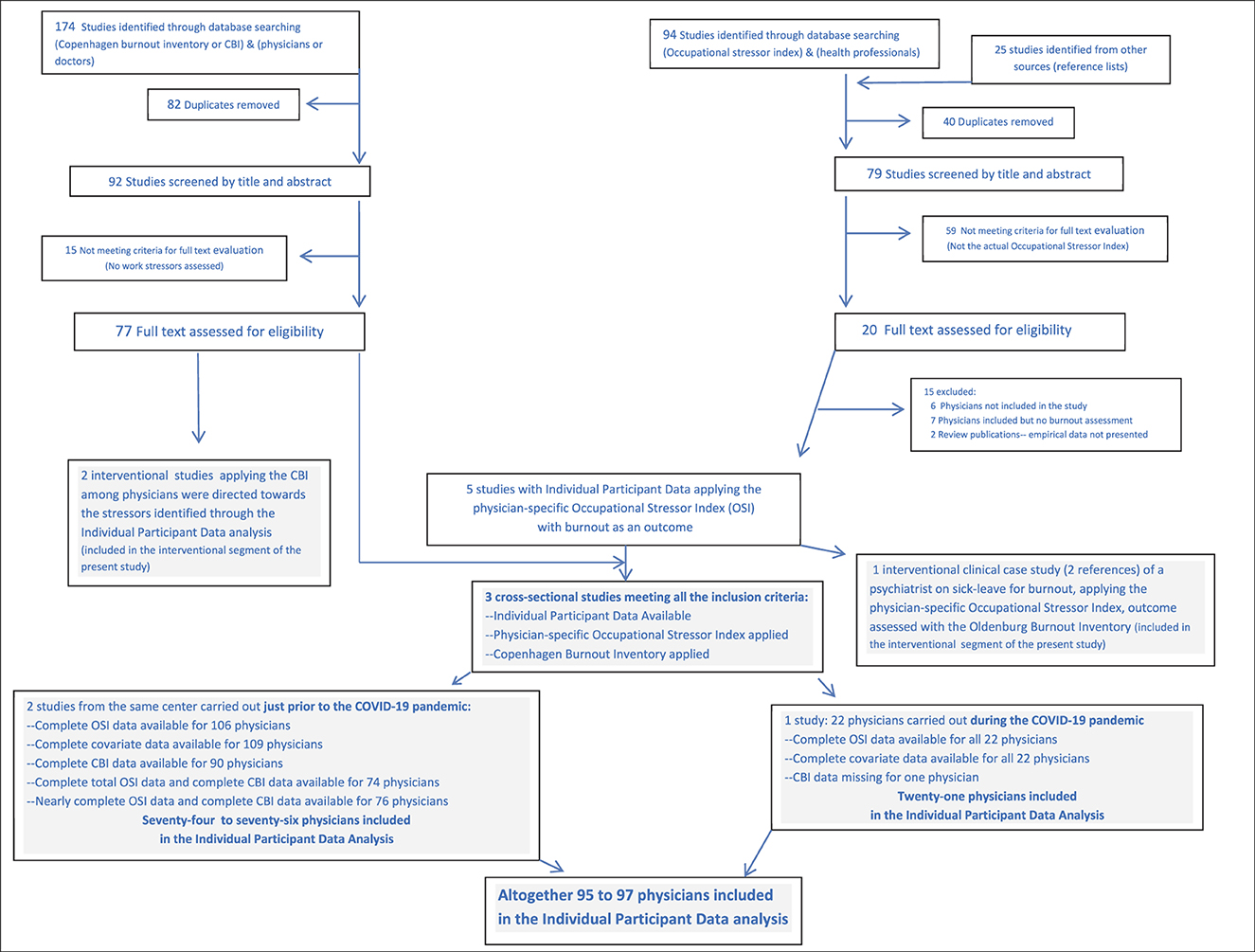
Figure 1. Flow chart for selection of studies addressing physician burnout, included in the individual participant data analysis as per PRISMA guidelines.
2.3 Analysis of the individual participant data
The available data for the IPD were all cross-sectional, i.e., baseline only. Two of the studies had been carried out in English in which all the participants were entirely fluent, on the level of a first-language (9, 34). All materials for the third study (39) were in Serbian, the primary language of all the participating physicians. Translation-back-translation was used to verify the equivalence of the Serbian language versions of all the instruments with respect to the originals in English.
Studies (9, 34) from the All India Institute of Medical Sciences in Jodhpur were carried out among physicians in 2018–2019, i.e., just prior to the outbreak of the COVID-19 pandemic. The participation rate was 43%. Data for Nedić and Belkić (39) were collected from November 2021 through April 2022 among primary care physicians and nurses working at the COVID-19 Outpatient Respiratory Center in Novi Sad, Serbia, with 100% participation. The present IPD analysis from Nedić and Belkić (39) includes only the physicians.
The data from the 3 studies were placed into a single data set. Therein, each study was labeled, on the basis of which a variable was introduced as to whether the data were collected during or prior to the onset of the COVID-19 pandemic. The OSI data were complete for 106 physicians from Jodhpur and for all 22 participating physicians from Novi Sad. Complete CBI data were available for 90 physicians from Jodhpur and for 21 of the 22 physicians from Novi Sad. Covariates were age, gender and work-years as a physician, complete for 109 Jodhpur physicians and all 22 of those from Novi Sad. Altogether there were complete data for 95 physicians (74 from Jodhpur and 21 from Novi Sad) and nearly complete data for 97 physicians (76 from Jodhpur and 21 from Novi Sad).
Firstly, extensive univariate analysis was performed. Age and working years as a physician were strongly correlated (Pearson r = 0.85, p = 0.000). To avoid multicollinearity, age was selected as the covariate for inclusion in all the multivariable analysis. Gender and work during vs. prior to the COVID-19 pandemic were the other two covariables included in all the multivariable analyses.
The outcome measures [personal (A), work-related (B) and patient-related burnout (C)] were dichotomized at their respective median cutpoints for multiple logistic regression, which was used to compute odds ratios (OR) and 95% confidence intervals (CI). Multiple logistic regression (M Log R) was applied to assess the effect of unit change in the total OSI on burnout (A), (B), and (C). In addition, M Log R was carried out with total OSI scores dichotomized at the clinically-determined cutpoint of 88, above which urgent intervention has been deemed to be needed (17, 18). Next, the relation between work stressors as evaluated using the OSI questionnaire and each of the burnout components was assessed via M Log R. Results with p < 0.05 for the OSI stressor are displayed, as are trends, generally with 0.05 ≤ p ≤ 0.08.
The internal consistency, examined by the Standardized Cronbach alpha was 0.84 for the total OSI, 0.90 for burnout (A), 0.87 for burnout (B), and 0.92 for burnout (C). We tested for the potential random effect of work during vs. prior to the COVID-19 pandemic via Variance Components Analysis, with respect to all three CBI outcome variables. The p values were identical or very close to those obtained in M Log R analysis.
Only complete data were used in the analyses, with no imputation whatsoever. According to the outlined search strategies, all potentially eligible studies were included for the IPD analysis. We consider this single-stage IPD analysis to be complete for the investigated questions. Statistica software (14.0.0.15, 2021 TIBCO version) was used throughout for the IPD analysis.
2.4 Systematic literature review
A systematic literature review was undertaken for each of the OSI stressors for which there was a multivariable association with one or more of the burnout indices. A very brief presentation of observational investigations is given in the main text, highlighting a few of the most salient findings, with the search strategies and further details in Supplementary material 2. A major focus in the Results Section will be on intervention studies impacting the job stressor and carried out among physicians, with particular attention to burnout when assessed as an outcome.
3 Results
3.1 Univariate findings and multiple logistic regression for total OSI among the physicians with IPD
Table 1 provides a summary of the major univariate findings for the physicians included in the IPD analysis. These encompass key demographic data, the total OSI scores, the totals for the OSI levels and OSI aspects, and CBI personal, work-related and patient-related burnout scores. There were quite similar percentages of practice areas: General practice/community medicine, Surgery/anesthesia/emergency medicine and Internal medicine/pediatrics/psychiatry/dermatology/combined specialties. Thirty-two (33.7%) of the 95 physicians included in the IPD analysis for whom these data were available had a total OSI score above the cutoff point of 88, for which intervention is urgently needed.
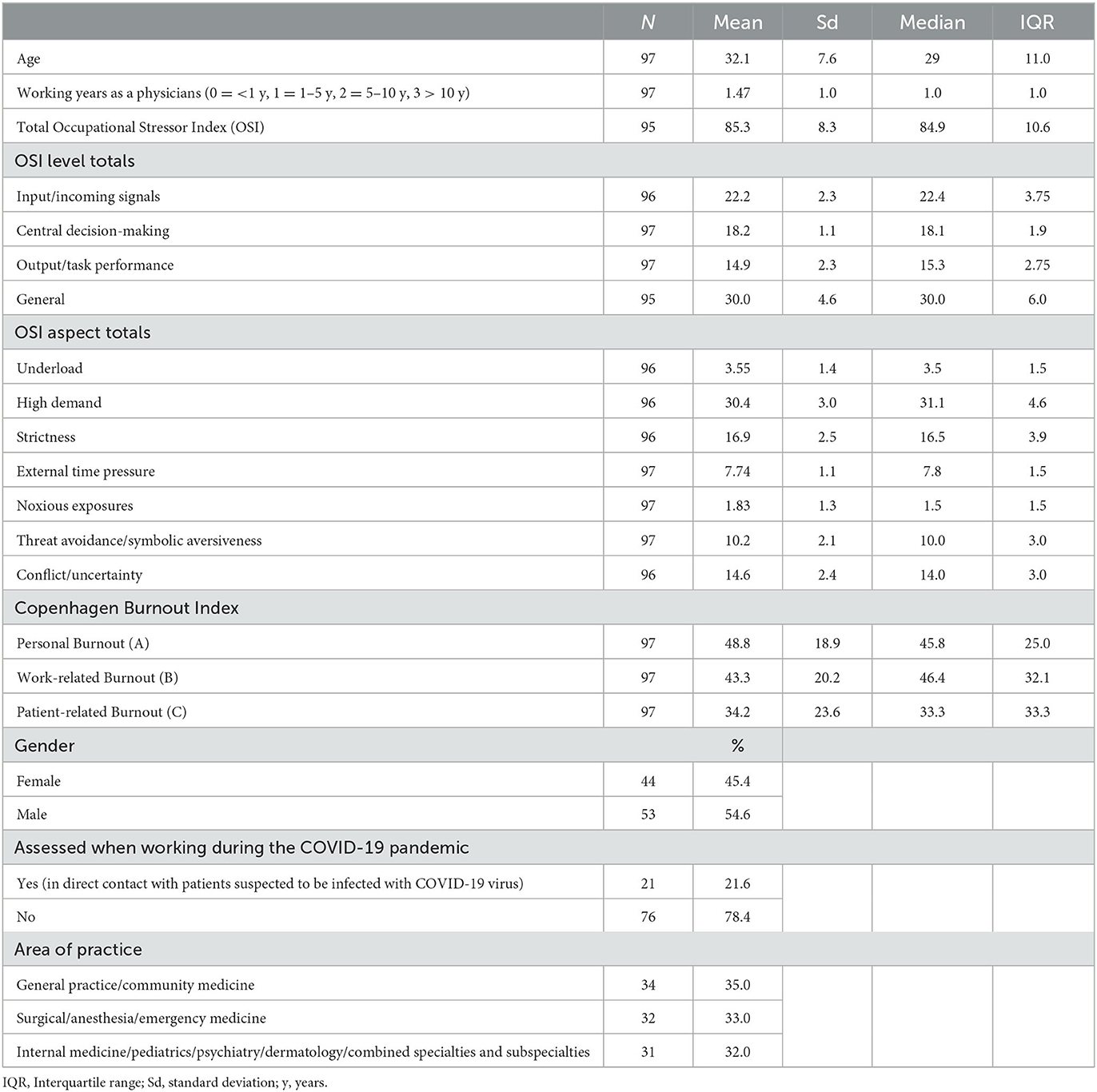
Table 1. Major univariate findings for the physicians included in the individual participant data analysis.
Altogether about 22% of the physicians included in the IPD analysis were working in direct contact with patients suspected of being infected with COVID-19 virus, when they completed the surveys. The full univariate data from the physician-specific OSI questionnaire for all the physicians included in the IPD analysis are given in Supplementary material 3.
For those included in the IPD analysis, the total OSI scores were higher ( = 87.0 ± 7.8) among the 74 physicians working prior to the COVID-19 pandemic compared to ( = 79.2 ± 7.3) among the 21 physicians working during the pandemic (2-sample t-test, p = 0.000). Full univariate details on each of the stressors assessed via the OSI questionnaire for the physicians working during the pre-pandemic studies and for those who worked during the pandemic, are presented in the Supplements from Belkić and Rustagi (34) and Nedić and Belkić (39), respectively.
The M Log R findings are presented in Table 2 for the total OSI scores in relation to CBI personal, work-related and patient-related burnout scores, with the three covariates: age, gender and whether or not assessment was when working during the COVID-19 pandemic. For personal burnout above the median integer cutpoint of 46, both working during the COVID-19 pandemic and unit change in OSI yielded significant ORs, with an order of magnitude greater p-value for unit change in total OSI scores. The OR for work-related burnout above the median integer cutpoint of 46 was more strongly associated with a unit change in total OSI. Albeit not as strong as for age and gender, a unit change in total OSI scores was significantly associated with patient-related burnout surpassing the integer median cutpoint of 33. The ORs were nearly 4 and over 8 for total OSI scores above 88 being related, respectively, to personal and work-related burnout in the adjusted M Log R analysis of Table 2.
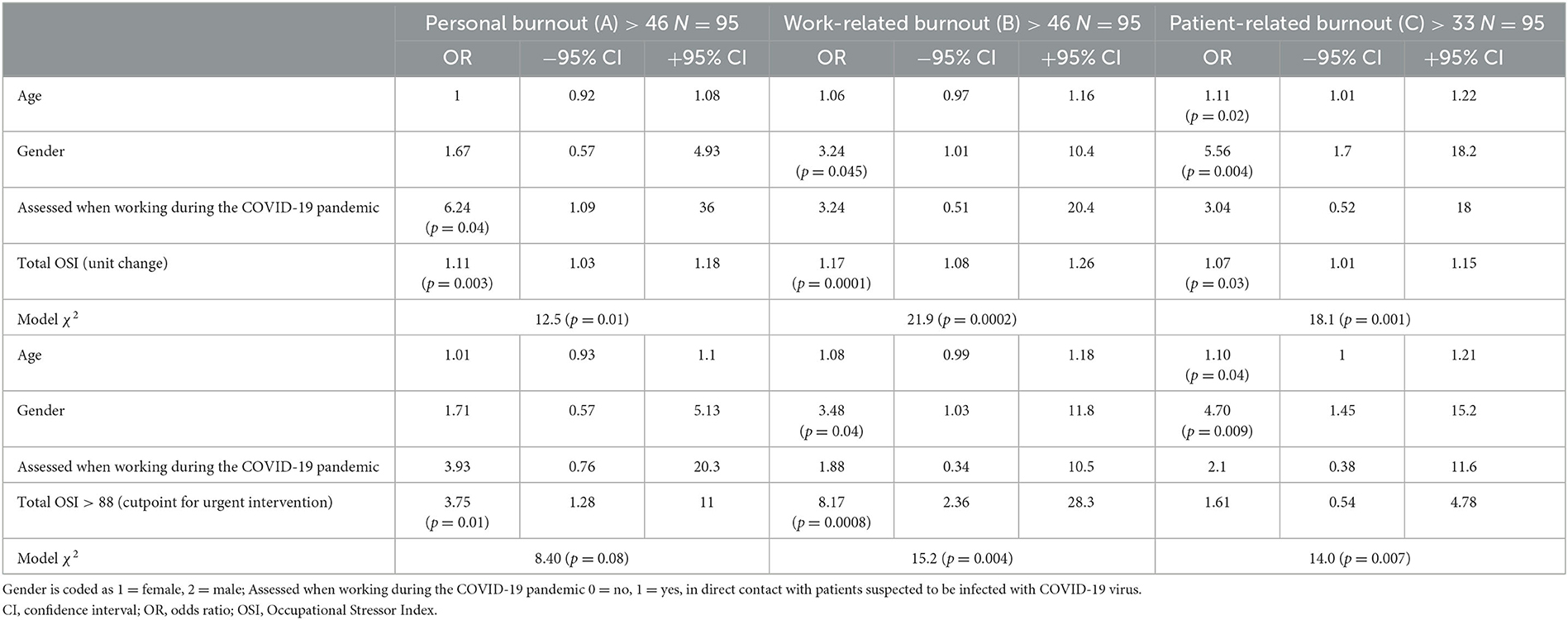
Table 2. The total Occupational Stressor Index in relation to the Copenhagen Burnout Indices among the physicians with individual participant data: multivariable logistic regression analysis.
3.2 Queries from the OSI questionnaire yielding multivariable associations with burnout
In Table 3, the queries from the OSI questionnaire yielding multivariable associations with each of the three categories of burnout are displayed. From the OR, 95% CI and p-values, the stressors most highly associated with each of the three categories of burnout are identified. These can be used to rank the stressors most highly associated with each of the three categories of burnout.

Table 3. Questions from the physician-specific Occupational Stressor Index showing significant or near significant adjusted odds-ratios with personal, work-related and/or patient-related burnout for the physicians included in the individual participant data analysis.
Table 3 begins with sub-section C focusing on Work Hours and Scheduling.
3.3 Work hours and scheduling (OSI Sub-section C)
3.3.1 Usual number of work days
The median number of usual workdays per week was 6 for the 97 physicians included in the IPD analysis (Supplementary material 3). Thirty-two (33%) had no weekly free days, i.e., they worked 7 days/week. This variable was associated with an adjusted OR of ~3.5 (95% CI 1.3–9.0) for work-related burnout above the median (>46) (Table 3).
Although there were many cross-sectional studies regarding work hours and physician burnout, most of which did show an association (Supplementary material 2), few of them addressed the number of workdays, per se. Among those that did, an investigation carried out in 2009 from Japan of 494 physicians of various specialties, indicated that having only 2–4 days off/month (compared to >8 days off/month) yielded an OR = 3.61 (95% CI 1.09–12.5) for burnout assessed via the MBI, adjusting for gender, marital status, clinical experience, place of work, location and specialty (49). In late 2020, among 226 general practitioners (GPs) from the U.K. who worked >3 days per week, a single-item measure of burnout was marginally higher than for 180 GPs who worked 3 or fewer days/week (32).
As summarized in Table 4, five interventional investigations included a reduction in the number of workdays/week (30, 50–53). A cluster-randomized trial introducing an interrupted schedule with weekend cross-coverage for medical intensivist physicians yielded an adjusted mean decrease in burnout (p = 0.003) compared to working continuously for a half-month. Work-home life imbalance and job distress were also significantly lowered with the interrupted schedule. Notwithstanding diminished continuity of care by the intensivists, patient outcomes were not worsened (50). Among the Duty Hour Restrictions for Post-Graduate Medical Education in the U.S., were those implemented in 2011. In three institutions in which this included 1 day off every 7 days, as well as shorter night call shifts, first-year residents in internal medicine showed trends toward diminution in mean incident burnout, emotion exhaustion and depersonalization compared to controls examined in 2008–2009 (53). However, the Authors conclude: “this multi-institutional study found that the implementation of 2011 duty hours standards was not associated with significantly lower rates of burnout among first-year IM (internal medicine) residents, and that unacceptably high rates of burnout persist” (p. 498). Among emergency medicine (EM) and IM residents working in a Minneapolis, Minnesota urban safety net hospital, a number of interventions were implemented in a 5-year cohort study (30). One of these was providing an extra day off for senior residents on ward duty. Significant improvements in empathy perception as a component of burnout, as well as sleep, peer support and nurture of personal relationships were reported during the follow-up period. A single item explicitly assessing burnout per se, oscillated between 25% and 35% during the follow-up period. No burnout assessment was reported in retrospective study of surgical residents (51) which indicated that providing a free day from clinical work after night call and other work hour limitations did not diminish their operative case volume. As a simulation study aimed at reducing physician burnout, Geva et al. (52) indicated that shared service could provide days off.

Table 4. Intervention studies on work stressors associated with physician burnout.
3.3.2 Work hours per week
Altogether 37 of the 97 physicians included in the IPD worked over 80 h/week, which was also the mean (Supplementary material 3). With each hour of increased weekly work time, there was a greater likelihood of work-related burnout above the median (p = 0.04) (Table 3).
In 2003, Work Hour Restrictions (WHR) were mandated to be 80 h maximum for Post-Graduate Medical Education in the U.S. Several publications assessed burnout among residents in relation to number of work hours/week (54–59). As indicated in Table 4, some of these studies assessed different groups of residents prior to and after the WHR were implemented. Diminution in burnout rates and its components using the MBI was seen in nearly all the studies. Two investigations among practicing physicians outside post-graduate training (60, 61) also suggested that work hour limitations helped diminish burnout.
3.3.3 Contacted during free time
The majority of the 97 physicians included in the IPD analysis were contacted occasionally or frequently by phone and/or email outside duty time about clinical care of patients or other job-related issues. This was associated with an almost two-fold increased likelihood of work-related burnout >46 and nearly as high a chance for patient-related burnout scores above the median, as per the adjusted analysis (Table 3).
The searched literature on this topic among physicians mainly yielded publications regarding electronic health records (EHR) and other documentation issues. These will be considered in Section 3.10 regarding workload and activities. One study (62) carried out among 106 palliative care providers captured the essence of this stressor. Namely, “work intrusiveness” when with family or friends or attending to domestic obligations. This was correlated (p = 0.005) with work-related burnout. Physicians, however, were not included in that study.
Among the interventions implemented for IM and EM residents in the 5-year cohort study (30) was removal of after-hours consult pager calls, with transfer of some responsibilities to faculty during that time. As noted, significantly improved empathy perception as a component of burnout, as well as improved sleep, peer support and nurture of personal relationships were reported during the follow-up period (Table 4).
3.3.4 Insufficient work-free, paid vacation
There was substantial variation in the scores regarding work-free paid vacation among the 97 physicians, with a median score of 1 (3–4 weeks/year). Insufficient work-free vacation was related to personal burnout and more strongly to work-related burnout in the adjusted multi-variable IPD analysis (Table 3).
Many cross-sectional publications prior to and during the COVID-19 pandemic concordantly reported a direct or indirect association between insufficient vacation time free from clinical and other work obligations and physician burnout (Supplementary material 2). Among the most recent studies (63), of 3,024 U.S. physicians, taking more than 3 weeks of vacation and having full EHR coverage had an adjusted OR = 0.66 (95% CI: 0.45–0.98) and 0.74 (95% CI: 0.63–0.88), respectively, for MBI. Progressively elevated adjusted OR's for MBI were found with greater vacation time spent on patient-related work, up to OR = 1.9 (95% CI: 1.36–2.73) if >90 min/day. Among 498 women physicians, 66.3% reported an increase in at least one work-related activity while on vacation during the COVID-19 pandemic. The most frequently endorsed strategy for reducing work engagement during vacation was formal discussions at the workplace/department (64). Vacation time was considered the highest reform priority in a study of 525 Canadian family physicians (65). Notwithstanding the importance of work-free vacation for physicians, no intervention studies were found addressing this issue.
3.3.5 Insufficient rest breaks
Approximately two-thirds of the 97 physicians included in the IPD analysis lacked genuine rest breaks free from work obligations. The vast majority had only short rest breaks during work hours. The more infrequent the rest breaks, the greater the likelihood of work-related burnout (OR = 3.26, 95%CI 1.1–9.6). The longer time without even a short rest break, the greater the likelihood not only for burnout (B), but also for personal burnout (OR = 2.77, 95% CI 0.98–7.89) (Table 3).
There are some cross-sectional studies in which rest-breaks were considered in relation to burnout (Supplementary material 2). Among emergency department health professionals in a French university hospital, including 28 physicians, lacking adequate time for eating or completely skipping meals was a significant risk factor for burnout (66). In the above-described study of GPs in the U.K., taking ≥2 breaks in sitting per hour was associated with a lower score on the single-item measure of burnout (p = 0.007) (32). During the COVID-19 pandemic, even when rest breaks were formally available, the chance to actually rest and recover during such times was often compromised. The latter was associated with work-related burnout (p < 0.01) in a study of National Health Service staff in the U.K. (67).
Published intervention studies directly impacting rest breaks and burnout among physicians are sparse. As indicated in Table 4, indirect evidence can be gleaned from Hutter et al. (58) that the greater likelihood of eating lunch after implementation of WHR could have contributed to improved burnout profile and indices of motivation among surgical residents. One of the immediately implemented measures that may have contributed to overall clinical improvement in the case study of an exhausted psychiatrist was at least 10 min of undisturbed break time between outpatients (18, 48). A randomized, controlled trial providing an undisturbed 5-h sleep period to internal medicine interns was associated with longer sleep which, in turn, was associated with lowered emotional exhaustion and depersonalization (p < 0.01). However, there were no significant differences in MBI burnout indices at the end of the 4-week intervention and control periods (68). An extra hour of rest breaks per week was not associated with changes in CBI at 10-week follow-up among interns during their emergency department rotation (38).
3.3.6 Total OSI high demand
Most of the queries in Section 3.3 of the OSI questionnaire contribute to the General Level of the High Demand aspect of the OSI. For the present IPD analysis, with age, gender and working during the COVID-19 pandemic included as covariates, total High Demand scores yielded an OR (± 95% CI) = 1.20 (1.01 – 1.42) (p = 0.03) for Personal Burnout >46, and 1.25 (1.05 – 1.48) (p = 0.01) for Work-related Burnout >46.
3.4 Salary, possibilities for advancement and recognition (OSI Sub-section D)
3.4.1 Lacks recognition of good work
The median for recognition of good work was 0.5, corresponding to “Yes, to some extent” for the 97 physicians for whom there are IPD. When such recognition is lacking, the likelihood of work-related burnout is nearly three-fold among these physicians (Table 3).
The importance of recognizing physicians' work has been widely acknowledged. A cross-sectional study of 2,145 general practitioners carried out during mid-2022 in Chongqing, China, revealed significant multivariable associations between receiving sufficient recognition from patients (as well as from the medical team) and lower scores on each of the three components of the MBI. These findings suggested that lack of recognition contributed to burnout among the physicians evaluated in the study (69).
Three publications were identified in which interventions were aimed at enhancing professional recognition among physicians. As noted in Table 4, in the first of these, a pilot study (70) carried out among 36 primary care professionals in Thessaloniki, Greece, the professional recognition intervention was associated with increased positive emotions and lower arousal emotions at follow-up. Burnout, per se, was not assessed. The Authors state that to their knowledge, “this is the first intervention targeting professional recognition implemented in health-care settings” (p. 950). A peer-recognition program completed by 72 EM residents in the U.S. yielded improved feelings of recognized accomplishments and perception of a comfortable, supportive work environment at 6-month follow-up. However, no significant changes in burnout as assessed by the Stanford Professional Fulfillment Index were noted in association with the intervention (8). For the third study (30), the “package of interventions” included a newsletter “celebrating resident achievements” (p. 690). As noted, empathy perception was significantly improved, as were sleep, peer support and nurture of personal relationships.
3.4.2 Total OSI underload
Lack of recognition of good work, as well as the other items in Sub-section D of the OSI questionnaire for MDs are used to generate the total Underload score in the OSI. These queries are all part of the General level of the Underload aspect, and are quite akin to the low reward component of the Effort Reward Imbalance model (14, 71). With age, gender and working during the COVID-19 pandemic as covariates, for the present IPD analysis, total Underload scores showed an OR (± 95% CI) = 1.61 (1.11 – 2.34) (p = 0.01) for Work-related Burnout >46, and 1.54 (1.02 – 2.32) (p = 0.04) for Patient-related Burnout >33.
3.5 Work conditions (OSI Sub-section E)
3.5.1 Office conditions
As noted in Supplementary material 3, there were many untoward office conditions including cramped office space, several people sharing an office, the majority not even having their own desk, with ten of the 97 physicians working in windowless offices. The greater the percent of work time spent in the office, the greater the likelihood of personal and work-related burnout in the multivariable analysis (Table 3).
Some cross-sectional investigations included assessment of office conditions in relation physician burnout. Among 1,498 anesthesiologists and intensivists in France carried out in 2018, having less “personal space” showed a strong relation (p = 0.000) with personal and work-related CBI scores >50 (35). The impact of untoward office conditions became even more salient during the COVID-19 pandemic. An investigation carried out in 2020 revealed a significant association between accessing daylight during work and reduced burnout in 406 physicians and nurses (72). The importance of the physical environment, in particular, separate space to “step away from work demands” was also highlighted in a mixed methods study of physicians and other emergency health care workers published in 2023 (73).
No larger-scale intervention studies among physicians regarding office conditions and burnout were identified. However, among the immediate interventions reported in the case study of the exhausted psychiatrist who had shared a windowless office with a colleague, was to provide her a separate office with a window. Thereby, she could also see her patients without having to search for another room, plus ensuring that she had the chance to take the above-described rest breaks (18, 48). In Larsen et al. (74), focus groups of radiologists, referring clinicians and trainees gave their qualitative and quantitative feedback during the process of redesigning radiology reading rooms with “purposeful space” and separate areas for various work activities. Burnout was a noted consideration, but its explicit assessment was not reported. In the above-cited multi-faceted intervention study (30), attention was given to lighting in rooms used by residents, with the mentioned improvements in empathy perception, sleep, peer support and nurture of personal relationships (Table 4).
3.5.2 Radiation exposure
Approximately 30% of the 97 physicians reported being exposed to radiation during work, 19 (66%) of whom did not wear a radiation badge. Exposure to radiation was associated in multivariable analysis with work-related burnout and more strongly with personal burnout (Table 3).
Relatively few publications were found in which radiation exposure and burnout are addressed with regard to physicians, as listed in Supplementary material 2. Among these, in the most recent study (75) carried out among 215 residents in internal medicine, concerns about burnout and about radiation exposure were significantly greater among the female physicians. However, no assessment was reported in that or the other studies regarding the relation between radiation exposure and burnout.
The exposure queries in part E of the OSI questionnaire concerning work conditions refer not only to the purely physical aspects, but also to attendant hazards/broader aversiveness. Radiation exposure is scored within the OSI as part of hazardous task performance, within the threat avoidant vigilance/symbolic aversiveness aspect of the OSI.
3.5.3 Listening to emotionally-disturbing accounts
The aversiveness of listening to emotionally-disturbing accounts is included on the input level of threat avoidant vigilance. The median response to this query among the 97 physicians was 1, corresponding to occasionally listening to such accounts. Twenty-three of these physicians answered that they frequently did so. Albeit with rather wide 95% CI, the adjusted OR was 1.89 for personal burnout associated with this stressor (Table 3).
Concordant findings were reported in other cross-sectional studies. Among 285 psychiatrists and 326 non-psychiatrist Paris hospital physicians, “emotional demands” (a dichotomous variable) were associated with personal and work-related burnout and with an expanded definition of burnout (C) referring to all interpersonal interactions (76). The OR's were between 3 and 4. Exposure to “high emotional demands” among 278 Sri Lankan post-graduate physicians also showed adjusted ORs between 3 and 4 for burnout (A), (B) and (C) (3). Oncologists, whose subspecialty area entails heavy exposure to that which is emotionally disturbing, are reported to be particularly vulnerable to burnout (77).
In the physician-specific OSI questionnaire, the query is intentionally left open as to what the respondent considers emotionally disturbing. This is scored according to the reported frequency of exposure, broadly reflecting intensity. The key is to recognize when the emotional toll has become excessive, and to intervene with protective measures (18). In Table 4, four different studies are reviewed in relation to this stressor. Therein, various interventional strategies are presented and their impact on burnout and other measures of physician wellbeing are described. Among these was a 2-day course for hematology-oncology residents focused on serious illness communication, which was not associated with a noteworthy decline in burnout (A), (B), or (C) compared to baseline nor compared to controls. Self-efficacy was, however, improved in relation to communicating existential issues and uncertainties with patients. The Authors conclude: “The high level of burnout among physicians in hemato-oncology calls for institutional interventions in addition to training” (37) (p. 547). Although burnout per se was not evaluated, a Zoom-based debriefing program implemented among 35 emergency department residents and attending physicians was considered “an acceptable and useful approach to support emotional wellbeing during the coronavirus pandemic” (78) (p. 88). Informed by successful strategies among infantry soldiers, recommendations have been put forward for anesthesiologists faced with pediatric deaths (79).
3.6 Mishaps at work (OSI Sub-section F)
The aversiveness which physicians may encounter becomes more explicit in Section 3.6 of the OSI questionnaire. The topic of suicide is broached therein, firstly among patients and then among colleagues and other coworkers. This combined exposure to suicide contributes to threat avoidant vigilance on the general level. Altogether, 35 (36%) of the 97 physicians had some work-related exposure to suicide, associated with an increased likelihood of personal and work-related burnout (Table 3).
3.6.1 Attempted or actual patient suicide
Nineteen of the 97 (20%) of physicians either heard about or had patients who attempted or committed suicide. Eight physicians had actually cared for one or more such patients.
We found relatively few articles addressing the toll on physicians of caring for such patients. A cross-sectional investigation among 368 hospital healthcare providers in Malaysia (80) examined attitudes toward patients who are suicidal. Only the personal accomplishment component of the MBI showed an association with understanding and willingness to aid patients who had attempted suicide. A study of 90 psychiatrists attending a conference in the U.S. indicated that after the suicide of a patient, the majority sought support from a colleague and/or from a family member or friend (81).
The earlier-cited case study illustrates the potential impact of patient suicide even for an experienced psychiatrist (18, 48), who subsequently became so exhausted that she needed major help to be able to return to work. Among the implemented measures was a temporary relief from work in the emergency department to diminish her exposure to the most acutely-ill psychiatric patients (Table 4). A protocol was evaluated among psychiatry residents, ten of whom had experienced patient suicide during their residency (82). The program included a primary response of the supervisor to meet and discuss the physician's initial emotional response, medico-legal issues and coverage of work duties, if needed. A more involved secondary response from the training director offered referral psychotherapy and other further support, group reflections and meeting with other colleagues who had similar experience. Nine of the ten residents followed the protocol. The most helpful was to talk with attending physicians who had faced such adverse events. Findings on the MBI did not differ between the 39 residents who did not have patient suicide vs. the ten who did.
3.6.2 Attempted or actual suicide of person(s) with whom one works
Nearly 25% of the 97 physician stated that there had been one or more suicide attempts or completed suicide among colleagues or staff at work. In the majority of cases, the person was known, and there were altogether sixteen actual suicides reported.
Notwithstanding the large body of literature on suicide among physicians (83), until recently there has been a surprising lack of attention to its impact on colleagues. As poignantly described nearly two decades ago: “The suicides that had already occurred were never discussed openly, no one undertook a publicly acknowledged serious analysis of the causes, and no other clear safeguards were put into place. The deaths were simply accepted as a fact of medical life” (84) (p. 2474). Moreover, it has been stated: “no silence is as profound as that which greets the news of a suicide in the medical community” (85) (p. 247).
In 2021, the American Medical Association published a comprehensive toolkit for responding to a physician's suicide (86), which includes support to close colleagues, insofar as the physician's family granted permission to share that information. The importance of help to coworkers after suicide is well-recognized, especially by nurses (87, 88). However, no intervention studies were found addressing physicians after an attempted or completed suicide of a colleague or staff at work. Two U.S. programs have been described that appear to improve physician-to-physician suicide risk assessment and support (89, 90).
3.6.3 Official complaint against the physician
About 20% of the 97 physicians had ever testified in court in an official capacity and/or had received an official complaint about their work. The latter was associated with an elevated risk of work-related burnout in the IPD analysis (Table 3).
Many cross-sectional studies have indicated that untoward patient outcomes, especially if followed by medico-legal processes are linked to physician burnout (Supplementary material 2). These “adverse events” impact profoundly upon the physician, who has been termed the “second victim” and who is also in need of and reportedly helped by peer support (91–93). An intervention study included 17 EM physicians with active lawsuits who participated in Group Peer Support Sessions akin to those developed during the COVID-19 pandemic (33). The single item MBI assessment was essentially unchanged after compared to before the intervention, as were other indices of distress. The Authors underscore: “Despite increasing burnout in the specialty of emergency medicine…during the study time frame, burnout did not worsen in participants… [such that] formal peer support offered by EM groups can be an effective option to normalize the experience of being sued, promote wellness, and benefit physicians who endure the often long and stressful process of a medical malpractice lawsuit” (p. 205) (Table 4).
3.6.4 Total OSI threat avoidant vigilance/symbolic aversiveness
Two of the questions in OSI Sub-section E on work conditions (exposure to visually-disturbing scenes and listening to emotionally-disturbing accounts) contribute to threat avoidant vigilance on the input level. The third threat avoidant vigilance input level element is the degree to which sustained alertness is required to avoid serious consequences. This element has a narrowed range (minimum of 1 for physicians without actual patient contact, such as is often the case for pathologists). The maximum score of 2 is given for clinicians with substantial emergency and/or inpatient work.
For all physicians, there is obviously potential injury or fatality that can be the consequence of a wrong decision. This is reflected on the central decision-making level of the OSI by a single threat avoidant vigilance stressor, which has a fixed score at the maximum (which is 2).
Hazardous task performance (output level) takes into account exposure to radiation, threat of violence and infection risk, also queried in OSI Sub-section E on work conditions. As seen in Supplementary material 3, altogether 84 of the 97 physicians included in the IPD stated that they faced risk of infection.
Sub-section F comes thereafter to inquire about more sensitive issues, termed “mishaps”, all of which contribute to threat avoidant vigilance, mainly on the general level. Among these are having witnessed or experienced accidents or injuries, litigation/testifying in court, including official complaints, suicide of patients and of colleagues or other persons at work, and lack of a system in place for non-medical emergencies. With the covariates (age, gender and working in direct contact with patients suspected to be infected with COVID-19 virus), total threat avoidant vigilance scores showed an OR (± 95% CI) = 1.25 (1.01–1.54) (p = 0.04) for Personal Burnout >46, and 1.31 (1.05–1.63) (p = 0.01) for Work-related Burnout >46 for 96 of the physicians in the IPD analysis.
3.7 Time pressure at work (OSI Sub-section G)
3.7.1 Time constraints preclude completion of work tasks
Nearly half of the 97 physicians stated that sometimes or often it was not possible to complete their work tasks even with maximal effort. Time constraints precluding completion of work tasks were associated with a markedly higher likelihood of personal burnout, and a weaker relation to patient-related burnout in the IPD analysis (Table 3).
Workload/time pressure conflict has been associated directly or indirectly with physician burnout in some publications (Supplementary material 2). An observational study among hospital emergency professionals, including 34 physicians, underscored the heavy time pressure associated with that work environment (94). The need for multi-level solutions to address increased clinician overload/time pressure and burnout was highlighted in a study of 721 U.K. physicians, poignantly entitled: “It's like juggling fire daily” (95).
Although burnout per se was not reported, an intervention implemented among IM residents and faculty aimed to minimize conflicting responsibilities via a “clinic buddy” system (96). Time pressure was thereby reduced, and although continuity was also slightly diminished, there was no impact on patient outcomes. Of the many interventions implemented in the 5-year cohort study among IM and EM residents (30), more time was allowed for patient visits during clinic. Significantly improved empathy perception, sleep, peer support and nurture of personal relationships were reported during the follow-up period, as noted (Table 4).
3.8 Problems and restrictions (OSI Sub-section H)
3.8.1 Problems/deficiencies hinder patient care—understaffing specifically hinders patient care
Over half of the 97 physicians indicated that problems/deficiencies occasionally or often hinder patient care. A greater frequency of such hindrances was associated with over three-fold likelihood of work-related burnout above 46 in the adjusted analysis. The most often cited hindrance was understaffing, reported by 44 of the 97 physicians. Albeit with a lower 95% CI of 0.86, when understaffing was indicated as a hindrance, the adjusted OR was nearly two for work-related burnout above the median of 46 (Table 3).
Among 1,925 European EM practitioners, 84% of whom were physicians, a survey carried out in early 2022 indicated an OR = 2.7 (95% CI 2.2–3.4) for abbreviated Maslach burnout associated with sometimes understaffing, and OR = 10.0 (95% CI 7.4–13.7) for often understaffing (97). Understaffing has been concordantly cited as a major stressor by physicians in various settings, who underscored the need for hiring more personnel (95, 98). In their open-ended responses, forty-eight (50%) of the 97 physicians included in the present IPD analysis suggested increased employment of staff as a needed work-place intervention (34, 39). It has been suggested that a “Chief Wellness Officer” could help alleviate these problems, e.g., by ensuring additional clinical staff teams during high demand seasons (99).
As summarized in Table 4, two studies implemented some type of increased clinician staffing. In (100), carried out in the primary care setting, a dyad of a physician and a certified medical assistant (CMA) was replaced in the intervention by a team of two health care providers and three CMAs who together were responsible for a panel of patients. At 6-month follow-up, emotional exhaustion and depersonalization were lowered among the physicians in the intervention group compared to baseline, and self-efficacy augmented, whereas a worsening trend was observed over this time period among the control group of physicians. In Quirk et al. (30), “jeopardy resident coverage” provided short-notice replacement for residents who needed time-off for vital personal life events. Together with the other interventions, improved outcomes were seen among the residents in that program. Interventions in which clerical staff are included to cover EHR-related tasks are reviewed in Section 3.10 on workload and activities.
3.8.2 Interruptions from people hinder task performance
Thirty-one percent of the 97 physicians answered that interruptions from other people, including phone calls, occasionally prevented them from proceeding with their work. Another 17 physicians (18%) stated that such interruptions were frequent. The adjusted ORs for personal and work-related burnout above the median were, respectively, over 5 and nearly 8 in relation to these interruptions, which are the strongest multi-variable associations of all the examined work stressors (Table 3).
“Interruptions are [overall] considered one of the most common work stressors” (101) (p. 185), impinging on flow which is a key component of healthy work conditions (13, 14, 18, 31). Quite a few publications have emphasized the need to reduce interruptions for physicians (Supplementary material 2). Among 58 U.S. hospital physicians (102), frequent pages or interruptions for non-urgent matters showed the strongest bivariate relation of all the assessed job stressors to high MBI (p = 0.003).
Interventions to diminish physician interruptions in the outpatient setting suggested in the earlier-cited review article (13), included silencing phones when seeing patients, as well as during charting, and designating separate time to address non-urgent issues. A suggested intervention made by most of the 21 participating EM physicians (73) was to have “a separate space for themselves to reduce interruptions” (p. 270). Along these lines, as noted in Table 4, improved layout for radiology reading rooms appeared to help diminish interruptions, according to some of the physician statements as per (74). In particular, a deep reading space was designed for tasks that “require sustained periods of uninterrupted focus” (p. 111).
Implementing scheduling software for emergency surgery also reportedly reduced interruptions (103). “Geographical cohorting”, whereby physicians are limited to a single geographic location, was successfully carried out in the critical care setting (104), with several improved patient outcomes, as well as diminishing interruptions for the physicians. Residents together with the information technology (IT) staff developed an EHR-integrated text paging system which markedly diminished the number of interruptions, compared to traditional paging which required 100% telephone response. Although burnout was not explicitly assessed, “stress and frustration” were both reportedly reduced in 88% of the 25 participating residents (105). Only one publication was found assessing the impact of an intervention to reduce interruptions in actual relation to physician burnout (31). Among the 17 participating residents working in the emergency department, although the frequency of non-urgent calls decreased (p = 0.03), there was no change in reported degree of burnout from non-urgent calls (assessed via a single explicit query) (p = 0.84).
3.9 Interpersonal interactions and social climate (OSI Sub-section I)
3.9.1 Lacking redress of grievances
Slightly fewer than half of the 97 physicians included in the IPD analysis stated that an efficient and confidential grievance procedure was available to them. Among the remaining physicians, either such a procedure, albeit available, was reportedly ineffective and/or without confidentiality guaranteed (42 physicians) or there was no possibility to redress grievances at work (seven physicians). In the adjusted logistic regression analysis, lack of an adequate procedure for redressing grievances was associated with over a two-fold likelihood of personal and work related burnout (Table 3).
Only one observational publication (106) was identified in which grievance redress was presented in relation to the MDs themselves. In three focus-groups, altogether 28 women physicians explored issues of gender inequity across career stages. Among the themes raised was the need for institutional transparency regarding grievances. Burnout per se, in specific relation to the lack of grievance procedures, did not appear to have been examined in that study.
None of the other queries in Section 3.9 of the OSI questionnaire concerning interpersonal issues showed any statistical relation to the burnout indices in the present IPD analysis. This may be due to the relatively favorable findings for the other queries in that Section, as seen in Supplementary material 3.
3.10 Workload and activities (OSI Sub-section J)
3.10.1 Handling patients who cannot give a history
Only 25 of the 97 physicians stated that they rarely or never handled patients who could not give a history, while 22 stated that they frequently did so. This stressor was associated with over a two-fold increase in adjusted logistic regression analysis with all three types of burnout (Table 3). The burden of this stressor does not seem to have been included in other studies of physician burnout (Supplementary material 2).
3.10.2 No separate time for non-clinical duties
Altogether 89 of the 97 physicians had other duties besides clinical work. Teaching in small groups and research were the most frequent of these, with administrative and other pedagogical tasks somewhat less common. Forty-six of these physicians had both pedagogical and research duties. Only 21 (24%) of the 89 physicians had separate time allocated for non-clinical assignments. Most were obliged to intersperse them with their clinical work. Adjusted multivariate logistic regression revealed over a three-fold elevated risk for personal and work-related burnout (>46) associated with lacking separate time allocated to non-clinical duties for those 89 physicians (Table 3).
A few studies have focused on the conflict between clinical and non-clinical duties, mainly among physicians in the academic setting for whom the need to separately allocate time for the multiple roles was emphasized (41). A publication from the Baskent University Ankara Hospital, Turkey, included 258 physicians for whom insufficient time for scientific research was associated with higher emotional exhaustion (p < 0.001) as assessed by the MBI (107). Concordantly, among 490 early-career “physician-scientists” in Japan, work-related burnout scores were lower among those with larger amounts of grant funding (p = 0.013), implying that more separate time could be allocated to scientific work (36).
An intervention study (108) of a cohort design was identified in which a faculty schedule change was instituted among eight acute care surgeons at a trauma and tertiary care center (Table 4). Protected academic time was one of the changes. In addition, continuous call was reduced from 24 to 12 h with no other clinical obligations during the on-call week. This ensured that the surgeon was free to leave as soon as the on-call was completed. Compared to baseline, at 1-year follow-up among the eight participating surgeons, overall MBI burnout was reduced by 12.5%, emotional exhaustion decreased by 28%, depersonalization was lowered by 38% and personal accomplishment increased by 12.5%. Clinical, administrative and academic parameters indicated that there was no diminution in the surgeons' productivity. Protected time for research was also one of the many interventions introduced among IM and EM residents, with improved empathy perception, sleep, peer support and nurture of personal relationships noted during the follow-up period (30).
3.10.3 Performing tasks that seem pointless
Just over 20% of the 97 physicians answered that they were obliged to perform tasks they consider pointless. In the OSI model, this is a general level stressor within the conflict/uncertainty aspect, corresponding to lack of coherence. In adjusted analysis, the likelihood of personal burnout above the median was over three-fold higher, and of work-related burnout nearly five-fold higher among those 20 physicians (Table 3).
A closely-related concept is that of “illegitimate tasks” (109), that are not necessarily pointless, but are unreasonable and/or unfairly assigned. Such tasks may be within the domain of other personnel. For the present IPD, altogether 28 of the 97 physicians stated that they performed tasks outside the realm of a physician, i.e., duties of other personnel. Although there was an association between these two OSI queries (Pearson χ2 = 5.5, p = 0.02), only ten physicians answered that they performed seemingly pointless tasks as well as tasks of other personnel. There was no relation whatsoever between performing tasks of other personnel and any of the 3 burnout indices. These findings can be explained as follows: physicians may be called upon to perform tasks such as phlebotomy or recording electrocardiograms that are clinically essential, but should be performed by other personnel. For physicians, tasks that seem pointless are often of administrative/clerical (34). In the above-cited review (41), academic physicians reported that administrative responsibilities were the least meaningful. Moreover, spending <20% of work hours in the physician's perceived most meaningful activity reportedly showed the strongest association with burnout.
Many observational studies have addressed the burden on physicians of performing administrative tasks, especially regarding EHR, electronic health records (Supplementary material 2). Via the Berne Illegitimate Task scale (109), a strong relation (p < 0.001) was found between performing “illegitimate tasks” and personal, work-related and patient-related burnout among nearly 500 general practitioners in Germany (40).
An intervention to relieve administrative burden by providing clerical staff to cover some EHR tasks was carried out among seven academic internists in Birmingham, Alabama (110) (Table 4). At the 4-month follow-up, two physicians compared to four at baseline, reported feeling burned-out at least weekly from work, and none felt that they had become callous toward people (reflective of MBI depersonalization) compared to two of the seven who had felt so prior to the intervention. The Authors conclude that this intervention “allows physicians to spend more time focusing on patient care, resulting in improved patient interactions, increased productivity and improved physician satisfaction” (p. 363).
A year-long crossover study examined the impact of medical scribes among 18 primary-care physicians working at Kaiser Permanente in Northern California. The intervention was associated with diminished after-hours EHR documentation and greater chance of spending at least 75% of time interacting directly with the patient, rather than on computer. Although not explicitly assessed in their article, the Authors foresaw that reducing the EHR burden faced by primary care physicians could potentially diminish burnout (111). In the earlier described large-scale cross-sectional study (61) of urologists, explicitly carried out during the COVID-19 pandemic, hiring a scribe was, by self-report, considered the most effective strategy to reduce burnout. The Authors underscored the need for organizational support to “increase participation and effectiveness of burnout interventions” (p. 101).
3.10.4 Total OSI conflict/uncertainty
The majority of the questions in sub-sections “Time pressure at work” (G) through “Workload and activities” (J) of the OSI questionnaire contribute to the Conflict/uncertainty aspect. The input level contains two elements that are scored maximally. Namely, signal/noise and signal/signal conflict are essential features for all physicians.
There is some variability regarding the degree to which there are conflicts/uncertainty at the central decision-making level. Handling patients who cannot give a history or who are severely disturbed, language barriers and delays/difficulties in obtaining medical records or lab are all potential sources of missing information needed for decision-making. The need to adjust plans due to unforeseen circumstances is scored higher with emergency and/or intensive care unit (ICU) responsibilities. However, one element of conflict/uncertainty on the central decision making level is scored maximally for all physicians, i.e., contradictory information.
Conflicting demands in time and space, to which time constraints contribute, problems/deficiencies that hinder patient care and interruptions are all elements of conflict/uncertainty on the output/task performance level. On the general level, conflict arises with the interpersonal issues addressed in Section 3.9 of the OSI questionnaire and some items in Section 3.10. As noted, lacking separate time for non-clinical duties and performing tasks that seem pointless were both associated in multivariable analysis with increased likelihood of personal and work-related burnout.
Of all the OSI aspects, the total conflict/uncertainty scores showed the most powerful associations with the three types of burnout, in the analyses that included covariates: age, gender and working in direct contact with patients suspected to be infected with COVID-19 virus. The OR (± 95% CI) was 1.45 (1.16–1.81) (p = 0.001) for personal burnout >46, 1.76 (1.32–2.34) (p = 0.0001) for work-related burnout >46 and 1.25 (1.003–1.55) (p = 0.04) for patient-related burnout >33 among the 96 physicians in the IPD analysis.
4 Discussion
The total stressor burden as assessed by the OSI showed a powerful multivariable association with all three burnout indices among the physicians included in the present IPD analysis. Working in direct contact with patients suspected to be infected with COVID-19 virus was yet an additional burden, whose impact appeared to be strongest for personal burnout. When the total OSI surpassed 88, the clinical cutpoint for urgent intervention, the likelihood of work-related burnout being above the median of 46, was over eight-fold. These findings for the total OSI justified the identification of potentially contributory job stressors, as performed herein for the IPD. Altogether there were 20 distinct work stressors showing multivariable association with one or more of the burnout indices.
The next step was to search for published interventions in which the implicated stressors were diminished among physicians. Altogether 33 publications were found. Burnout was explicitly assessed as an outcome in 21 (63.6%) investigations, with a favorable impact at least to the level of p < 0.10 for one or more indices observed in 13 (62%) of these studies. Two other intervention studies, each with fewer than ten physicians, showed a favorable, albeit statistically non-significant, impact on burnout (108, 110).
Six of the 33 intervention studies (37, 38, 50, 68, 100, 111) were of a randomized controlled design. In contrast, in 4 reports different physicians were examined prior to and after the intervention (53, 54, 56, 57). Two case studies (18, 48, 79) were included, as well. All but 5 of the 33 studies were explicitly conducted in the U.S.
For several of the implicated stressors, no published intervention studies to reduce the burden were found. These stressors were: insufficient work-free paid vacation, radiation exposure, suicide attempt or completed suicide of person(s) at work, lack of grievance procedure, and handling patients who cannot give a history. On the other hand, 8 of the 33 (24.2%) intervention studies addressed weekly work hours, mainly in relation to the 2003 mandated WHR in the U.S. for Post-Graduate Medical Education. All but one (55) of those reports showed an impact on burnout or other indices of physician wellbeing.
Of all the 33 identified intervention studies, the cluster-randomized investigation of 45 intensive care physicians at various levels of training (50) is deemed the most rigorous. Not only was the impact of diminishing the number of consecutive work days assessed in relation burnout and other indices of physician wellbeing, patient outcomes were also considered. Compared to standard continuous ICU responsibility for ~15 days, interrupted weekend cross-coverage yielded significantly diminished physician burnout without adversely affecting patient care.
Some other of the identified interventions (30, 96, 100) also implemented cross-coverage, effectively lowering time constraints (96). Emotional exhaustion was significantly reduced among the primary care physicians in the centers with cross-coverage, compared to those working in the status quo centers (100). In (30), cross-coverage provided short-notice replacement for urgent personal needs of the residents, as well as transferring after-hours paging to faculty. Cross-coverage among physicians was certainly also necessary to guarantee separate time for non-clinical activities. In the small intervention study of acute care surgeons carried out during the COVID-19 pandemic, favorable changes were observed in all three MBI indices a year after they were guaranteed protected academic time, as well as having assured coverage at the conclusion of their scheduled on-call duty (108).
Besides cross-coverage among physicians, staffing issues are also relevant for other team members in the health care system. In particular, administrative tasks often extend work hours. This impinges on the physician's scheduled free time, including vacations (63), as well as compromising attention to patients, and thereby undermining the meaningfulness of the physician's work (41). Assigning at least some administrative activity to clerical personnel, was beneficial for reducing burnout (61, 110), as well as diminishing after-hours worktime and allowing the physician to spend more time with patients (111). Collaboration between physicians and IT staff also appeared to be an effective strategy against interruptions (105). That stressor showed the most powerful multivariable associations with personal and work-related burnout for the physicians included in the IPD analysis. Partnership with IT staff could help develop other strategies to reduce the physician stressor load. Besides reducing administrative burden, measures could be instituted e.g., to safeguard against medication dosage errors through computer programming (18).
Rigorously-designed studies focused on a single stressor to which physicians are exposed are obviously vital for guiding evidence-based intervention strategies. However, such interventions may be insufficient to genuinely impact physician burnout, particularly if the overall stressor load is very heavy, e.g., with the total OSI score above the cutpoint of 88. Comprehensive organizational interventions were carried out among residents in (30). These would have lowered the scores for underload (recognition of good work), high demand (more days off plus after-workhour coverage) and conflict/uncertainty (diminished time constraints, improved staffing with cross-coverage, protected time for research). The total OSI would have been diminished by several points. In addition, there were interventions on the individual level: resiliency training, mental health support plus primary wellness care (30). Although the single-item explicit burnout measure did not change notably during the 5-years with implementation of these organizational and personal interventions, there was a significant increase in empathy perception, sleep, peer support and nurturing of personal relationships (30). Several other studies also reported interventions on the personal level (8, 18, 33, 38, 48, 60, 61, 78, 79, 82). Reduction in work hours together with counseling were associated with a nearly 30% diminution in full-time sick leave at 1-year follow-up for practicing physicians in Norway, as well as significantly lowered emotional exhaustion and depersonalization (60).
For physicians with full-blown burnout syndrome, or even more serious mental health disorders, return to work can be facilitated by care from a clinician with multifaceted expertise in psychiatry/psychology as well as occupational medicine (23). This was illustrated by the case study (18, 48) included herein. Multiple interventions were implemented on the organizational and individual level, coordinated by the occupational psychiatrist. With the immediate steps, some of which were temporary, the total OSI was lowered by 17 points [from 106 (in the “acute danger level”) to 89 (just above the cutpoint for urgent intervention needed)]. The physician, a psychiatrist herself, was thereby able to return to work, albeit, at first, in a limited capacity. With temporary release from emergency duty, threat avoidant vigilance was slightly diminished, as she was somewhat protected from visually disturbing scenes such as suicide and trauma, as well as from listening to the most intensely emotionally-disturbing accounts. The case study of the grieving anesthesiology resident faced with the death of the pediatric patient (79) concordantly underscores the vital importance of interventions that address the threat avoidant vigilance burden.
The heightened acute infection hazard associated with the COVID-19 pandemic intensified the threat avoidant vigilance burden for physicians. This, in turn, impacted other stressors. For example, the extra time needed to properly use personal protective equipment often compromised restbreaks, such that even when a hot cooked meal was provided free of charge, “adequate time to eat and digest such a meal was often lacking” (39) (p. 524). Cross-coverage by a “float” physician who is well informed about the clinical status of the patients for whom he/she is covering could have been implemented to ensure adequate rest breaks for colleagues (34). Unfortunately, none of the larger-scale intervention studies addressing this topic (38, 58, 68) were conducted during the COVID-19 pandemic. Moreover, studies (38, 58, 68) do not appear to have been designed to assess the impact of providing properly-covered restbreaks during active work hours for physicians. Such investigations are urgently needed, given the potential benefits of this intervention (112).
Quirk et al. (30) provide an example of the potential feasibility of implementing a “package” of organizational interventions among a fairly sizable group of resident physicians. Included therein are some initial approaches to providing cross coverage. The latter is an essential step for many of the needed interventions, including ensuring adequate rest breaks. A “float” physician is an excellent solution, which, during on-site evaluation, this author has observed to be very practical. An initial outlay may be needed to cover this extra staffing, which can be a barrier. In addition, close cooperation among the physicians is vital, and this entails effort and training. In the longer run, this strategy would be cost-effective in protecting the health and work capacity of the physicians. The role of “float” physician can be very rewarding, bolstering knowledge and skills. The potential social cohesion engendered thereby is an added benefit.
The emotional toll of physicians' work during the COVID-19 pandemic further contributed to the threat avoidant vigilance burden. Although burnout, per se, was not assessed in Monette et al. (78), the weekly debriefings for clinicians providing emergency services during that time, were seen to facilitate a “safe environment”. Further helpful countermeasures regarding personal accomplishments were seen in the peer-to-peer recognition program for EM residents carried out during 2021–2022 (8).
Recognition of the special service to the community was implemented through discounts at local shops for the health care providers working at the COVID-19 Outpatient Respiratory Center in Nedić and Belkić (39). As noted, nearly all the median scores on Section 3.9 Interpersonal interactions and social climate were favorable with narrow interquartile ranges for the physicians included in the IPD analysis. Thus, intervention studies regarding these topics were not assessed in the present review. On the other hand, the median night shift work scores were maximal, such that limited variance did not permit detection of the impact of this stressor on physician burnout.
Further, regarding the IPD, all the data were cross-sectional and were mainly self-reported. This precludes inferences about the temporal nature of the identified associations and common method bias cannot be excluded. Based on these findings from cross-sectional data, the relationships between exposure to specific stressors and burnout among the physicians included in the IPD analysis cannot be unequivocally viewed as causal. Longitudinal follow-up studies are needed to help to establish causality. Interventional designs, larger scale as well as clinical case studies, can provide convergent validation, insofar as diminished exposure to one or more specific stressors is associated with amelioration of burnout.
There was a limited number of fairly small studies fulfilling all the inclusion criteria for the IPD. Consequently, power limitations must be considered. These also reduce the generalizability of the IPD findings. The relatively small percentage of senior level, attending physicians further diminishes generalizability.
The IPD data were collected from physicians working at an Academic Medical Institute in South Asia (India) and an ambulatory medical center in SouthEast Europe (Serbia). While potentially enhancing the generalizability of the IPD findings, these geographic and institutional factors require attention.
The identified intervention studies were from the U.S. and Western Europe. Since physician burnout is a global concern, a much broader international perspective is needed. Particular attention is warranted regarding the cultural setting, with greater appreciation of the needs of physicians working in developing countries.
Notwithstanding the limitations of the present work, the individual participant data analysis by the MD-specific Occupational Stressor Index provides substantial clues as to how physician burnout could be better prevented. Several of the identified contributory stressors had been previously underappreciated. The systematic review of intervention studies on the OSI-identified stressors further helps fill the gap, by focusing on the called-for attention to reduction of specific stressors. Together, these two facets of the present paper help pave the way toward more effective strategies to combat physician burnout, contributing to the following conclusions.
5 Conclusions
The strength and consistency of the reported evidence support the implementation of cross-coverage, so that physicians are guaranteed, at the very least, one day per week or alternating weekends entirely free from work obligations. Concordantly, an upper limit to weekly work hours including constraints on intrusions into free-time outside work hours is recommended. Work-free, paid vacation of adequate duration as well as appropriately timed and cross-covered rest breaks need to be examined as interventions to protect against physician burnout. The stressors related to work hours and scheduling contribute to high demands among physicians and are associated with increased personal and work-related burnout.
Recognition of the physician's efforts and achievements is a vital and easily implementable intervention. This would counteract underload, thereby diminishing work-related and patient-related burnout.
Radiation exposure and prolonged time spent in inadequate office/workspace adversely impact physician burnout. With the heightened infection risk during the COVID-19 pandemic, untoward physical conditions increased the hazards of physicians' work. An overly heavy exposure to that which is emotionally-disturbing further contributes to the burden. Suicide, whether of a patient, colleague or other coworker, is particularly devastating, as are medical errors that eventuate in lawsuits or other official complaints, for which the physician is often the “second victim”. Supportive counter-measures are indispensable. All these exposures add to the threat avoidant vigilance load, increasing the risk of personal and work-related burnout.
Although conflicts and uncertainty are part and parcel of physicians' work, modifiable stressors exacerbate this burden. Adequate staffing would be pivotal for mitigating many of these. Clerical staff can help offload administrative burden, allowing physicians to focus attention more directly on patients. Information technology staff can aid in devising ways to diminish interruptions, thereby enhancing work flow. Cross coverage among physicians can lower time constraints and ensure separate periods for vital non-clinical tasks. The total conflict/uncertainty score, assessed via the physician-specific OSI impacts heavily on all three types of burnout, as assessed by the CBI.
The total OSI score is a powerful gauge of personal, work-related and patient-related burnout risk among physicians, even when accounting for work directly with patients suspected of acute infection with COVID-19 virus. In clinical practice, lowering the total OSI score has facilitated return to healthier work for physicians suffering from burnout. The MD-specific OSI, developed “for physicians, by physicians” and based upon cognitive ergonomics is useful for guiding participatory action research. Well-controlled trials, with appropriately tailored interventions (77) would thereby help alleviate the scourge of burnout among this profession.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
KB: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the research grants from Radiumhemmet at the Karolinska University Hospital and the County Council of Stockholm (FoUU) to which the author is grateful. Open Access has been provided by the Karolinska Institute, Stockholm, Sweden.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declares that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1514706/full#supplementary-material
Abbreviations
CBI, Copenhagen burnout inventory; CI, Confidence interval; CMA, Certified medical assistant; EHR, Electronic health records; EM, Emergency medicine; GPs, General practitioners; ICU, Intensive care unit; IM, Internal medicine; IPD, Individual participant data; IT, Information technology; MBI, Maslach burnout inventory; M Log R, Multiple logistic regression; OR, Odds ratio; OSI, Occupational Stressor Index; WHR, Work hour restrictions.
References
1. Embriaco N, Papazian L, Kentish-Barnes N, Pochard F, Azoulay E. Burnout syndrome among critical care health care workers. Curr Opin Crit Care. (2007) 13:482–8. doi: 10.1097/MCC.0b013e3282efd28a
2. Shanafelt TD, Boone S, Tan L, Dyrbye LN, Sotile W, Satele D., et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. (2012) 172:1377–85. doi: 10.1001/archinternmed.2012.3199
3. Fernando BMS, Samaranayake DL. Burnout among postgraduate doctors in Colombo: prevalence, associated factors and association with self-reported patient care. BMC Med Educ. (2019) 19:373. doi: 10.1186/s12909-019-1810-9
4. Ferry AV, Wereski R, Strachan FE, Mills NL. Predictors of UK healthcare worker burnout during the COVID-19 pandemic. QJM. (2021) 114:374–80. doi: 10.1093/qjmed/hcab065
5. Latsou D, Bolosi F-M, Androutsou L, Geitona M. Professional quality of life and occupational stress in healthcare professionals during the COVID-19 pandemic in Greece. Health Serv Insights. (2022) 15:1–9. doi: 10.1177/11786329221096042
6. Mijić Marić A, Palameta M, Zalihić A, Bender M, Mabić M, Berberović M, et al. Prevalence of burnout among health care workers in the Federation of Bosnia and Herzegovina during the coronavirus disease-2019 pandemic: a cross-sectional study. Croat Med J. (2022) 63:482–9. doi: 10.3325/cmj.2022.63.482
7. Wahlster S, Sharma M, Lewis A, Patel PV, Hartog CS, Jannotta G, et al. The Coronavirus disease 2019 pandemic's effect on critical care resources and health-care providers. A global survey. Chest. (2021) 159:619–33. doi: 10.1016/j.chest.2020.09.070
8. Chang J, Saggar V, Cortijo-Brown A, Friedman BW, Jones M, Li-Sauerwine S, et al. Improving physician well-being and reducing burnout using a peer-to-peer recognition program. AEM Educ Train. (2023) 7:e10861. doi: 10.1002/aet2.10861
9. Goyal P, Rustagi N, Belkić K. Physicians' total burden of occupational stressors: over three-fold increased odds of burnout. South Med J. (2021) 114:409–15. doi: 10.14423/SMJ.0000000000001277
10. Awan S, Diwan MN, Aamir A, Allahuddin Z, Irfan M, Carano A, et al. Suicide in healthcare workers: determinants, challenges, and the impact of COVID-19. Front Psychiatry. (2022) 12:792925. doi: 10.3389/fpsyt.2021.792925
11. Sinsky CA, Privitera MR. Creating a “Manageable Cockpit” for clinicians: a shared responsibility. JAMA Intern Med. (2018) 178:741–2. doi: 10.1001/jamainternmed.2018.0575
12. Szulewski A, Howes D, van Merriënboer JJ, Sweller J. From theory to practice: the application of cognitive load theory to the practice of medicine. Acad Med. (2021) 96:24–30. doi: 10.1097/ACM.0000000000003524
13. Li-Wang J, Townsley A, Katta R. Cognitive ergonomics: a review of interventions for outpatient practice. Cureus. (2023) 15:e44258. doi: 10.7759/cureus.44258
14. Levi L, Bartley M, Marmot M, Karasek R, Theorell T, Siegrist J, et al. Stressors at the workplace: theoretical models. Occup Med. (2000) 15:69–105.
15. Belkić K. The Occupational Stress Index: An Approach Derived from Cognitive Ergonomics and Brain Research for Clinical Practice. Cambridge: Cambridge International Science Publishing (2003).
16. Israel B, Goldenhar L, Baker E, Heaney CA, Schurman SJ. Occupational stress, safety and health: conceptual framework and principles for effective prevention interventions. J Occup Health Psychol. (1996) 1:261–86. doi: 10.1037/1076-8998.1.3.261
17. Nedić O. Occupational Stressors and Physician Health with a Focus upon Cardiovascular Disease (dissertation). University of Novi Sad, Novi Sad (2006).
18. Belkić K, Savić Č. Job Stressors and Mental Health: A Proactive Clinical Perspective. Toh Tuck (Singapore): World Scientific (2013).
19. Karasek R. Job demands, job decision latitude and mental strain: implications for job redesign. Adm Sci Q. (1979) 24:285–308. doi: 10.2307/2392498
20. Belkić K, Savić Č, Djordjević M, Uglješić M, Micković Lj. Event-related potentials in professional city drivers: heightened sensitivity to cognitively relevant visual signals. Physiol Behav. (1992) 52:423–7. doi: 10.1016/0031-9384(92)90327-X
21. Friedman MJ, Charney DS, Deutch A. Neurobiological and Clinical Consequences of Stress: From Normal Adaptation to Post-Traumatic Stress Disorder. Philadelphia: Lippincott-Raven (1995).
22. Fuller R. A conceptualization of driving behaviour as threat avoidance. Ergonomics. (1984) 27:1139–55. doi: 10.1080/00140138408963596
23. Savić Č, Belkić K. Why are job stressors relevant for psychiatry? Br J Psychiatry. (2014) 205:425–7. doi: 10.1192/bjp.bp.114.154054
24. Greiner BA, Krause N. Expert-observer assessment of job characteristics. Occup Med. (2000) 15:175–83.
25. Volpert W. The model of hierarchical-sequential organization of action. In:Hacker W, Volpert W, von Cranach M, , editors. Cognitive and Motivational Aspects of Action. Amsterdam: Elsevier (1982). p. 35–51.
26. Maslach C, Jackson S. Maslach Burnout Inventory Manual (2nd Edn.). Palo Alto: Consulting Psychologists Press (1986).
27. Melamed S, Kushnir T, Shirom A. Burnout and risk factors for cardiovascular diseases. Behav Med. (1992) 18:53–60. doi: 10.1080/08964289.1992.9935172
28. Demerouti E, Bakker AB, Vardakou I, Kantas A. The convergent validity of two burnout instruments: a multitrait-multimethod analysis. Eur J Psychol Assess. (2003) 19:12–23. doi: 10.1027//1015-5759.19.1.12
29. Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress. (2005) 19:192–207. doi: 10.1080/02678370500297720
30. Quirk R, Rodin H, Linzer M. Targeting causes of burnout in residency: an innovative approach used at Hennepin healthcare. Acad Med. (2021) 96:690–4. doi: 10.1097/ACM.0000000000003940
31. Luu T, Spiegelman L, Nykin D, Abido K, Roh J, Rudkin S, et al. Implementation of an electronic health record-based messaging system in the emergency department: effects on physician workflow and resident burnout. J Patient Saf. (2022) 18:e542–6. doi: 10.1097/PTS.0000000000000869
32. Biddle GJ, Thomas N, Edwardson CL, Clemes SA, Daley AJ. Burnout, psychological wellbeing, and musculoskeletal complaints in UK GPs: an observational study. BJGP Open. (2023) 7:BJGPO.2023.0007. doi: 10.3399/BJGPO.2023.0007
33. Doehring MC, Strachan CC, Haut L, Heniff M, Crevier K, Crittendon M, et al. Establishing a novel group-based litigation peer support program to promote wellness for physicians involved in medical malpractice lawsuits. Clin Pract Cases Emerg Med. (2023) 7:205–9. doi: 10.5811/CPCEM.1377
34. Belkić K, Rustagi N. Job stressors in relation to burnout and compromised sleep among academic physicians in India. Work. (2024) 78:505–25. doi: 10.3233/WOR-230383
35. Berger B, Cungi PJ, Arzalier S, Lieutaud T, Velly L, Simeone P, et al. Incidence of burnout syndrome among anesthesiologists and intensivists in France: the REPAR Study. Int J Environ Res Public Health. (2023) 20:1771. doi: 10.3390/ijerph20031771
36. Perumalswami CR, Takenoshita S, Tanabe A, Kanda R, Hiraike H, Okinaga H, et al. Workplace resources, mentorship, and burnout in early career physician-scientists: a cross sectional study in Japan. BMC Med Educ. (2020) 20:178. doi: 10.1186/s12909-020-02072-x
37. Funding E, Viftrup DT, Knudsen MB, Haunstrup LM, Tolver A, Clemmensen SN. Impact of training in serious illness communication and work life balance on physicians' self-efficacy, clinical practice and perception of roles. Adv Med Educ Pract. (2023) 14:547–55. doi: 10.2147/AMEP.S406570
38. Ireland MJ, Clough B, Gill K, Langan F, O'Connor A, Spencer L, et al. A randomized controlled trial of mindfulness to reduce stress and burnout among intern medical practitioners. Med Teach. (2017) 39:409–14. doi: 10.1080/0142159X.2017.1294749
39. Nedić O, Belkić K. Job stressors and burnout among nurses and primary-care physicians working at a dedicated outpatient respiratory center for patients with suspected or confirmed COVID-19. Am J Ind Med. (2023) 66:510–28. doi: 10.1002/ajim.23475
40. Werdecker L, Esch T. Burnout, satisfaction and happiness among German general practitioners (GPs): a cross-sectional survey on health resources and stressors. PLoS ONE. (2021) 16:e0253447. doi: 10.1371/journal.pone.0253447
41. Banerjee G, Mitchell JD, Brzezinski M, DePorre A, Ballard HA. Burnout in academic physicians. Perm J. (2023) 27:142–9. doi: 10.7812/TPP/23.032
42. Cohen C, Pignata S, Bezak E, Tie M, Childs J. Workplace interventions to improve well-being and reduce burnout for nurses, physicians and allied healthcare professionals: a systematic review. BMJ Open. (2023) 13:e071203. doi: 10.1136/bmjopen-2022-071203
43. De Simone S, Vargas M, Servillo G. Organizational strategies to reduce physician burnout: a systematic review and meta-analysis. Aging Clin Exp Res. (2021) 33:883–94. doi: 10.1007/s40520-019-01368-3
44. Panagioti M, Panagopoulou E, Bower P, Lewith G, Kontopantelis E, Chew-Graham C, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. (2017) 177:195–205. doi: 10.1001/jamainternmed.2016.7674
45. Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev. (2015) 2015:CD002892. doi: 10.1002/14651858.CD002892.pub5
46. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272–81.doi: 10.1016/S0140-6736(16)31279-X
47. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, et al. Preferred reporting items for systematic review and meta-analyses of individual participant data: the PRISMA-IPD statement. JAMA. (2015) 313:1657–65. doi: 10.1001/jama.2015.3656
48. Belkić K, Nedić O. Physician health challenges and return to work—insights from participatory action research for physicians by physicians. Med Pregl. (2019) 72:367–73. doi: 10.2298/MPNS1912367B
49. Saijo Y, Chiba S, Yoshioka E, Kawanishi Y, Nakagi Y, Itoh T, et al. Effects of work burden, job strain and support on depressive symptoms and burnout among Japanese physicians. Int J Occup Med Environ Health. (2014) 27:980–92. doi: 10.2478/s13382-014-0324-2
50. Ali NA, Hammersley J, Hoffmann SP, O'Brien JM Jr, Phillips GS, Rashkin M, et al. Continuity of care in intensive care units: a cluster-randomized trial of intensivist staffing. Am J Respir Crit Care Med. (2011) 184:803–8. doi: 10.1164/rccm.201103-0555OC
51. Ferguson CM, Kellogg KC, Hutter M, Warshaw AL. Effect of work-hour reforms on operative case volume of surgical residents. Curr Surg. (2005) 62:535–8. doi: 10.1016/j.cursur.2005.04.001
52. Geva A, Landrigan CP, van der Velden MG, Randolph AG. Simulation of a novel schedule for Intensivist staffing to improve continuity of patient care and reduce physician burnout. Crit Care Med. (2017) 45:1138–44. doi: 10.1097/CCM.0000000000002319
53. Ripp JA, Bellini L, Fallar R, Bazari H, Katz JT, Korenstein D. The impact of duty hours restrictions on job burnout in internal medicine residents: a 3-institution comparison study. Acad Med. (2015) 90:494–9. doi: 10.1097/ACM.0000000000000641
54. Barrack RL, Miller LS, Sotile WM, Sotile MO, Rubash HE. Effect of duty hour standards on burnout among orthopaedic surgery residents. Clin Orthop Relat Res. (2006) 449:134–7. doi: 10.1097/01.blo.0000224030.78108.58
55. Gelfand DV, Podnos YD. Carmichael JC, Saltzman DJ, Wilson SE, Williams RA. Effect of the 80-hour workweek on resident burnout. Arch Surg. (2004) 139:933–40. doi: 10.1001/archsurg.139.9.933
56. Goitein L, Shanafelt TD, Wipf JE, Slatore CG, Back AL. The effects of work-hour limitations on resident well-being, patient care, and education in an internal medicine residency program. Arch Intern Med. (2005) 165:2601–6. doi: 10.1001/archinte.165.22.2601
57. Gopal R, Glasheen JJ, Miyoshi TJ, Prochazka AV. Burnout and internal medicine resident work-hour restrictions. Arch Intern Med. (2005) 165:2595–600. doi: 10.1001/archinte.165.22.2595
58. Hutter MM, Kellogg KC, Ferguson CM, Abbott WM, Warshaw AL. The impact of the 80-hour resident workweek on surgical residents and attending surgeons. Ann Surg. (2006) 243:864–71. doi: 10.1097/01.sla.0000220042.48310.66
59. Martini S, Arfken CL, Balon R. Comparison of burnout among medical residents before and after the implementation of work hours limits. Acad Psychiatry. (2006) 30:352–55. doi: 10.1176/appi.ap.30.4.352
60. Isaksson Rø KE, Gude T, Tyssen R, Aasland OG. Counseling for burnout in Norwegian doctors: one year cohort study. BMJ. (2008) 337:1146–9. doi: 10.1136/bmj.a2004
61. Shoureshi P, Guerre M, Seideman CA, Callejas DG, Amling CL, Bassale S, et al. Addressing burnout in urology: a qualitative assessment of interventions. Urol Pract. (2022) 9:101–7. doi: 10.1097/UPJ.0000000000000282
62. Fattori A, Pedruzzi M, Cantarella C, Bonzini M. The burden in palliative care assistance: a comparison of psychosocial risks and burnout between inpatient hospice and home care services workers. Palliat Support Care. (2023) 21:49–56. doi: 10.1017/S1478951521001887
63. Sinsky CA, Trockel MT, Dyrbye LN, Wang H, Carlasare LE, West CP, et al. Vacation days taken, work during vacation, and burnout among US physicians. JAMA Netw Open. (2024) 7:e2351635. doi: 10.1001/jamanetworkopen.2023.51635
64. Marshall AL, Elafros M, Duma N. Work patterns of women physicians during vacation: a cross-sectional study. J Womens Health (Larchmt). (2022) 31:573–9. doi: 10.1089/jwh.2021.0100
65. Hedden L, Banihosseini S, Strydom N, McCracken R. Family physician perspectives on primary care reform priorities: a cross-sectional survey. CMAJ Open. (2021) 9:E466–73. doi: 10.9778/cmajo.20200102
66. Durand A-C, Bompard C, Sportiello J, Michelet P, Gentile S. Stress and burnout among professionals working in the emergency department in a French university hospital: prevalence and associated factors. Work. (2019) 63:57–67. doi: 10.3233/WOR-192908
67. Gemine R, Davies GR, Tarrant S, Davies RM, James M, Lewis K. Factors associated with work-related burnout in NHS staff during COVID-19: a cross-sectional mixed methods study. BMJ Open. (2021) 11:e042591. doi: 10.1136/bmjopen-2020-042591
68. Shea JA, Bellini LM, Dinges DF, Curtis ML, Tao Y, Zhu J, et al. Impact of protected sleep period for internal medicine interns on overnight call on depression, burnout, and empathy. J Grad Med Educ. (2014) 6:256–63. doi: 10.4300/JGME-D-13-00241.1
69. Xu Y, Deng J, Tan W, Yang W, Deng H. Mental health of general practitioners in Chongqing, China during COVID-19: a cross-sectional study. BMJ Open. (2023) 13:e068333. doi: 10.1136/bmjopen-2022-068333
70. Angelopoulou P, Panagopoulou E. Is wellbeing at work related to professional recognition: a pilot intervention. Psychol Health Med. (2020) 25:950–7. doi: 10.1080/13548506.2019.1707239
71. Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. (1996) 1:27–41. doi: 10.1037/1076-8998.1.1.27
72. Ziabari SMZ, Andalib E, Faghani M, Roodsari NN, Arzhangi N, Khesht-Masjedi MF, et al. Evidence-based design in the hospital environment: a staff's burnout study in the COVID-19 era. HERD. (2023) 16:236–49. doi: 10.1177/19375867221148168
73. Bosch SJ, Valipoor S, Alakshendra A, De Portu G, Mohammadigorji S, Rittenbacher D, et al. Coping and caregiving: leveraging environmental design to moderate stress among healthcare workers in the emergency department setting. HERD. (2023) 16:261–77. doi: 10.1177/19375867231151243
74. Larsen EP, Hailu T, Sheldon L, Ginader A, Bodo N, Dewane D, Degnan AJ, Finley J, Sze RW. Optimizing radiology reading room design: the Eudaimonia Radiology Machine. J Am Coll Radiol. (2021) 18:108-20. doi: 10.1016/j.jacr.2020.09.041
75. Advani R, Arjonilla M, Guerson A, Taub E, Monzur F. Gender-specific attitudes of internal medicine residents toward gastroenterology. Dig Dis Sci. (2022) 67:5044–52. doi: 10.1007/s10620-022-07541-5
76. Hardy P, Costemale-Lacoste JF, Trichard C, Butlen-Ducuing F, Devouge I, Cerboneschi V, et al. Comparison of burnout, anxiety and depressive syndromes in hospital psychiatrists and other physicians: results from the ESTEM study. Psychiatry Res. (2020) 284:112662. doi: 10.1016/j.psychres.2019.112662
77. Hagani N, Yagil D, Cohen M. Burnout among among oncologists and oncology nurses: a systematic review and meta-analysis. Health Psychol. (2022) 41:53–64. doi: 10.1037/hea0001155
78. Monette DL, Macias-Konstantopoulos WL, Brown DFM, Raja AS, Takayesu JK, A. video-based debriefing program to support emergency medicine clinician well-being during the COVID-19 pandemic. West J Emerg Med. (2020) 21:88–92. doi: 10.5811/westjem.2020.8.48579
79. Soto RG. Rosen GP. Pediatric death: guidelines for the grieving anesthesiologist. J Clin Anesth. (2003) 15:275–7. doi: 10.1016/S0952-8180(03)00027-8
80. Siau CS, Chan CMH, Wee LH, Wahab S, Visvalingam U, Chen WS, et al. Depression and anxiety predict healthcare workers' understanding of and willingness to help suicide attempt patients. Omega (Westport). (2023) 87:469–84. doi: 10.1177/00302228211021746
81. Erlich MD, Rolin SA, Dixon LB, Adler DA, Oslin DW, Levine B, et al. Why we need to enhance suicide postvention: evaluating a survey of psychiatrists' behaviors after the suicide of a patient. J Nerv Ment Dis. (2017) 205:507–11. doi: 10.1097/NMD.0000000000000682
82. Agrawal A, Gitlin M, Melancon SNT, Booth BI, Ghandhi J, DeBonis K. Responding to a tragedy: evaluation of a postvention protocol among adult psychiatry residents. Acad Psychiatry. (2021) 45:262–71. doi: 10.1007/s40596-021-01418-x
83. Duarte D, El-Hagrassy MM, Couto TCE, Gurgel W, Fregni F, Correa H. Male and female physician suicidality: a systematic review and meta-analysis. JAMA Psychiatry. (2020) 77:587–97. doi: 10.1001/jamapsychiatry.2020.0011
84. Schernhammer E. Taking their own lives—the high rate of physician suicide. N Engl J Med. (2005) 352:2473–6. doi: 10.1056/NEJMp058014
85. Legato MJ. Physician suicide: unnecessary losses. Gender Med. (2009) 6:247. doi: 10.1016/j.genm.2009.04.002
86. Dyrbye L, Jin J, Yu Moutier C, Bucks C. After a Physician Suicide. Respond Compassionately and Effectively as an Organization. Chicago: American Medical Association (2021). Available online at: https://www.ama-assn.org/practice-management/ama-steps-forward/after-physiciansuicide-responding-organization-toolkit (accessed September 4, 2024).
87. Lynn CW. When a coworker completes suicide. AAOHN J. (2008) 56:459–69. doi: 10.1177/216507990805601104
88. Bartone PT, Bartone JV, Violanti JM, Gileno Z. Peer support services for bereaved survivors: a systematic review. Omega (Westport). (2019) 80:137–66. doi: 10.1177/0030222817728204
89. Ey S, Moffit M, Kinzie JM, Brunett PH. Feasibility of a comprehensive wellness and suicide prevention program: a decade of caring for physicians in training and practice. J Grad Med Educ. (2016) 8:747–53. doi: 10.4300/JGME-D-16-00034.1
90. Zabar S, Hanley K, Horlick M, Cocks P, Altshuler L, Watsula-Morley A, et al. “I cannot take this any more!”: preparing interns to identify and help a struggling colleague. J Gen Intern Med. (2019) 34:773–7. doi: 10.1007/s11606-019-04886-y
91. Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. (2000) 320:726–7. doi: 10.1136/bmj.320.7237.726
92. Rappaport DI, Selbst SM. Medical errors and malpractice lawsuits: impact on providers—Part 2 of 6. Pediatr Emerg Care. (2019) 35:440–2. doi: 10.1097/PEC.0000000000001856
93. Gupta K, Rivadeneira NA, Lisker S, Chahal K, Gross N, Sarkar U. Multispecialty physician online survey reveals that burnout related to adverse event involvement may be mitigated by peer support. J Patient Saf. (2022) 18:531–8. doi: 10.1097/PTS.0000000000001008
94. Lancman S, Mângia EF, Muramoto MT. Impact of conflict and violence on workers in a hospital emergency room. Work. (2013) 45:519–27. doi: 10.3233/WOR-131638
95. Dominic C, Gopal DP, Sidhu A. ‘It's like juggling fire daily': well-being, workload and burnout in the British NHS—A survey of 721 physicians. Work. (2021) 70:395–403. doi: 10.3233/WOR-205337
96. Jantea R, Buranosky R, Simak D, Hoffman E, Zimmer SM, Elnicki DM. The 50/50 block schedule: impact on residents' and preceptors' perceptions, patient outcomes, and continuity of care. Teach Learn Med. (2018) 30:223–32. doi: 10.1080/10401334.2017.1371606
97. Petrino R, Riesgo LG, Yilmaz B. Burnout in emergency medicine professionals after 2 years of the COVID-19 pandemic: a threat to the healthcare system? Eur J Emerg Med. (2022) 29:279–84. doi: 10.1097/MEJ.0000000000000952
98. Dillon EC, Tai-Seale M, Meehan A, Martin V, Nordgren R, Lee T, et al. Frontline perspectives on physician burnout and strategies to improve well-being: interviews with physicians and health system leaders. J Gen Intern Med. (2020) 35:261–7. doi: 10.1007/s11606-019-05381-0
99. Walia S, Nordenholz KE, Krywko D, Norvell JG, Hewitt KV, Parmele KT, et al. The Chief Wellness Officer: a long overdue catalyst for systemic change in Emergency Medicine. Int J Health Plann Manage. (2024) 39:141–51. doi: 10.1002/hpm.3714
100. Gregory ST, Menser T, Gregory BT. An organizational intervention to reduce physician burnout. J Healthc Manag. (2018) 63:338–52. doi: 10.1097/JHM-D-16-00037
101. Rick VB, Brandl C, Mertens A, Nitsch V. Work interruptions of office workers: the influence of the complexity of primary work tasks on the perception of interruptions. Work. (2024) 77:185–96. doi: 10.3233/WOR-220684
102. Mazur LM, Adapa K, Meltzer-Brody S, Karwowski W. Towards better understanding of workplace factors contributing to hospitalist burden and burnout prior to COVID-19 pandemic. Appl Ergon. (2023) 106:103884. doi: 10.1016/j.apergo.2022.103884
103. Lee J, Aoude A, Alhalabi B, Watt A, Lessard L. Can an emergency surgery scheduling software improve residents' time management and quality of life? McGill J Med. (2022) 20:10–15. doi: 10.26443/mjm.v20i2.893
104. Kapoor R, Gupta N, Roberts SD, Naum C, Perkins AJ, Khan BA. Impact of geographical cohorting in the ICU: an academic tertiary care center experience. Crit Care Explor. (2020) 2:e0212. doi: 10.1097/CCE.0000000000000212
105. Lapointe R, Bhesania S, Tanner T, Peruri A, Mehta P. An innovative approach to improve communication and reduce physician stress and burnout in a university affiliated residency program. J Med Syst. (2018) 42:117. doi: 10.1007/s10916-018-0956-z
106. Chesak SS, Salinas M, Abraham H, Harris CE, Carey EC, Khalsa T, et al. Experiences of gender inequity among women physicians across career stages: findings from Participant Focus Groups. Womens Health Rep (New Rochelle). (2022) 3:359–68. doi: 10.1089/whr.2021.0051
107. Ozkula G, Durukan E. Burnout syndrome among physicians: the role of socio-demographic characteristics. Dusunen Adam J Psychiat Neurol Sci. (2017) 30:136–44. doi: 10.5350/DAJPN2017300207
108. Jones CE, Fox ED, Holsten SB, White CQ, Sayyid RK, O'Keeffe T, et al. Burnout reduction in acute care surgeons: impact of faculty schedule change at a level 1 trauma and tertiary care center. J Trauma Acute Care Surg. (2022) 93:439–45. doi: 10.1097/TA.0000000000003736
109. Semmer NK, Jacobshagen N, Meier LL, Elfering A, Beehr TA, Kälin W, et al. Illegitimate tasks as a source of work stress. Work Stress. (2015) 29:32–56. doi: 10.1080/02678373.2014.1003996
110. Contratto E, Romp K, Estrada C, Agne A, Willett L. Physician order entry clerical support improves physician satisfaction and productivity. South Med J. (2017) 110:363–8. doi: 10.14423/SMJ.0000000000000645
111. Mishra P, Kiang JC, Grant RW. Association of medical scribes in primary care with physician workflow and patient experience. JAMA Intern Med. (2018) 178:1467–72. doi: 10.1001/jamainternmed.2018.3956
Keywords: work conditions, physicians, occupational health, burnout, participatory action research
Citation: Belkić K (2025) Toward better prevention of physician burnout: insights from individual participant data using the MD-specific Occupational Stressor Index and organizational interventions. Front. Public Health 13:1514706. doi: 10.3389/fpubh.2025.1514706
Received: 21 October 2024; Accepted: 26 February 2025;
Published: 19 March 2025.
Edited by:
Adriano Friganovic, University of Rijeka, CroatiaReviewed by:
Massimo Tusconi, University of Cagliari, ItalyMiri Cohen, University of Haifa, Israel
Paul Wojda, University of St. Thomas, United States
Copyright © 2025 Belkić. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karen Belkić, a2FyZW4uYmVsa2ljQGtpLnNl