 Eman Merghani Ali1,2
Eman Merghani Ali1,2 Amani Khardali1,2
Amani Khardali1,2 Nawazish Alam1,2*
Nawazish Alam1,2* Abdulkarim M. Meraya1,2
Abdulkarim M. Meraya1,2 Hilal A. Thaibah1,2Dalin A. Hassan3Mohamed Eltaib Elmobark4
Hilal A. Thaibah1,2Dalin A. Hassan3Mohamed Eltaib Elmobark4 Alanood Aladwani1,2Anugeetha Thacheril Mohanan3
Alanood Aladwani1,2Anugeetha Thacheril Mohanan3 Hanan A. Bakri5
Hanan A. Bakri5 Zamzam O. Mashraqi6Areej Mousa Salhabi2
Zamzam O. Mashraqi6Areej Mousa Salhabi2- 1Department of Clinical Practice, Faculty of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 2Pharmacy Practice Research Unit (PPRU), Department of Clinical Practice, Faculty of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 3Department of Pharmacology and Toxicology, Faculty of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 4Department of Pharmaceutics, Faculty of Pharmacy, Jazan University, Jazan, Saudi Arabia
- 5Pharmaceutical Care Department, King Fahd Central Hospital, Jazan, Saudi Arabia
- 6Pharmacy Department, Wadi Al-Dawaser Armed Forced Hospital, Wadi Al-Dawasir, Saudi Arabia
Introduction: Saudi Arabia has witnessed the first confirmed case of Mpox on July 14th, 2022. Currently, there is no approved medication for the treatment of this infection. Therefore, prevention of this infection is crucial. This study aimed to assess knowledge and attitude toward the monkeypox viral infection among pharmacy students of Jazan University in Saudi Arabia.
Methods: This is a cross-sectional, self-administered web-based study between the periods from April 2024 to June 2024. Descriptive statistics for all variables used chi-square statistics, and multivariate analysis to establish the association between participant’s demographic characteristics and knowledge of monkeypox disease.
Results: The overall level of knowledge and attitude found 32 and 44.5%, respectively among pharmacy students. The source of information was commonly social media (55.5%), and only 38% reported receiving information during medical education. The factors associated with knowledge level included gender (p = 0.02), obesity (p = 0.03), receiving information from family or friends (p = 0.03), and during medical education (p = 0.016). The factors that were associated with attitude included age (p = 0.03), chronic disease (p = 0.0001), social media (p = 0.007), and medical education (p = 0.004) as sources of information.
Conclusion: This study found the participants had a low level of knowledge and attitude toward Mpox infection. There is a need for the implementation of educational programs to know about this kind of outbreak and increase the knowledge and attitude of the students.
Introduction
Human monkeypox (Mpox) is a zoonotic disease caused by Mpox virus (1). The Mpox virus belongs to the Poxviridae family and subfamily chordopoxvirinae, genus orthopoxivirus, and Monkeypox virus species (2). It is an encapsulated double-stranded DNA virus (3, 4). Sporadic outbreaks of the virus were reported in Africa due to contact with wild animals (5). Such outbreaks and the occurrence of travel-associated cases resulted in limited secondary transmission between humans (6). Mpox was known as a rare viral zoonosis that is endemic to Western and Central Africa however, it has evolved to become a global issue (7, 8). The World Health Organization (WHO) declared Mpox a public health emergency of international concern on July 23, 2022, to address the outbreak with the required urgency (9). The first confirmed case of human Mpox in Saudi Arabia was on July 14th, 2022, and by August 2022, there were five confirmed cases (10). In the past Jazan province of Saudi Arabia experienced a Rift Valley fever outbreak in 2000 with 500 cases and many deaths hence health science students must have appropriate knowledge about such kind of outbreak through health education or training (11).
The incubation period of the virus varies from five to 21 days, while signs and symptoms can persist between 2 to 5 weeks. The symptoms start with a fever, and other symptoms include back pain, muscle aching or myalgia, chills, headache, asthenia, swelling of lymph nodes, fatigue, and rashes (12, 13). Various-sized rashes appear within 1–5 days following fever, and they appear initially on the face and then include the rest of the body, legs, arms, and feet (14). The death cases ranged from 1 to 10 percent in epidemics, and the majority of cases occurred in children and young individuals (15). Currently, there is no drug has been approved by the US Food and Drug Administration (FDA) for the treatment of Mpox; even the antiviral tecovirimat, which has been approved for the treatment of smallpox such as, has no available data on its effectiveness in the treatment of Mpox (16).
Therefore, early detection and management, as well as the prevention of such infections, are necessary, and they represent a challenge for healthcare practitioners (17). The lack of knowledge is another major challenge in tackling this outbreak. Therefore, the assessment of the knowledge and attitude of the pharmacy students is necessary as they are the future healthcare professionals who are responsible for the management of the disease hence the lack of knowledge can be of adverse significance (18). Also, pharmacy students may affect the general population’s perception of the range of different diseases and improve their awareness regarding preventive measures (19). Therefore, this study was conducted to assess the knowledge and attitude of pharmacy students regarding monkeypox infection.
Subjects and methods
Design and procedure
This study is an analytical observational cross-sectional web-based survey study conducted on the pharmacy students of Jazan University, Saudi Arabia. The study was performed between the periods from April 2024 to June 2024. The study was conducted on pharmacy students who provided informed consent and at age 18 years and older. The study was conducted using a self-administered questionnaire to assess the knowledge and attitude of the students toward the monkeypox virus. The survey included questions that investigated the demographics of the students, their knowledge, and their attitude toward the monkeypox virus. The overarching goal of the study is to know the awareness among students of healthcare field with interdisciplinary understanding of public health issues.
Study tools and data collection
Sample size was calculated by Raosoft sample size calculator. Confidence interval of 95% with a margin of 5% error. Approximately 400 undergraduate pharmacy studnets enrolled in first year to final year and a response distribution of 50%, a sample size of 188 was estimated. Data collection was carried out by a 43 item having 4 sections self-administered survey. Online surveys fulfilled the CHERRIES criteria. Multiple submission of participant’s response restricted and tracked with registered university email. Internal consistency was evaluated using Cronbach’s alpha, which yielded a value of 0.85. The questionnaire was validated by face as well as content validation. Bloom’s cut off point was determined to be used in this study with a score below 50% as low and score above 50% considered as high (20). Only completed questionnaires from participants were included in this study.
Data analysis
SPSS software was used for data processing; continuous and qualitative variables were represented using mean (±SD) and number (%), respectively. Association between levels of knowledge and attitude with other variables were done, and p ≤ 0.05 was considered significant.
Ethical consideration
The Research Ethics Committee of Jazan University approved this study. The approval number is REC 45/09/10–19, dated 24/03/2024. Participation in the study was entirely voluntary and free of coercion. Before starting the survey, all the participants provided their informed consent and confidentiality of participants were maintained.
Results
A total of 200 students were included in this study; their characteristics are displayed in Table 1. The large majority of the students aged 18–25 years, 176 (88%), were females 167 (83.5%) and singles 160 (80%). More than one-half were from rural regions 107 (53.5%) and were in the fourth year of education 102 (51%). The largest proportion, 62 (31%), reported a family monthly income of 4–10.9 KSR. There, 35 (17.5%) reported having chronic disease, and 34 (17%) reported obesity. Regarding smoking, 25 (12.5%) were smokers.
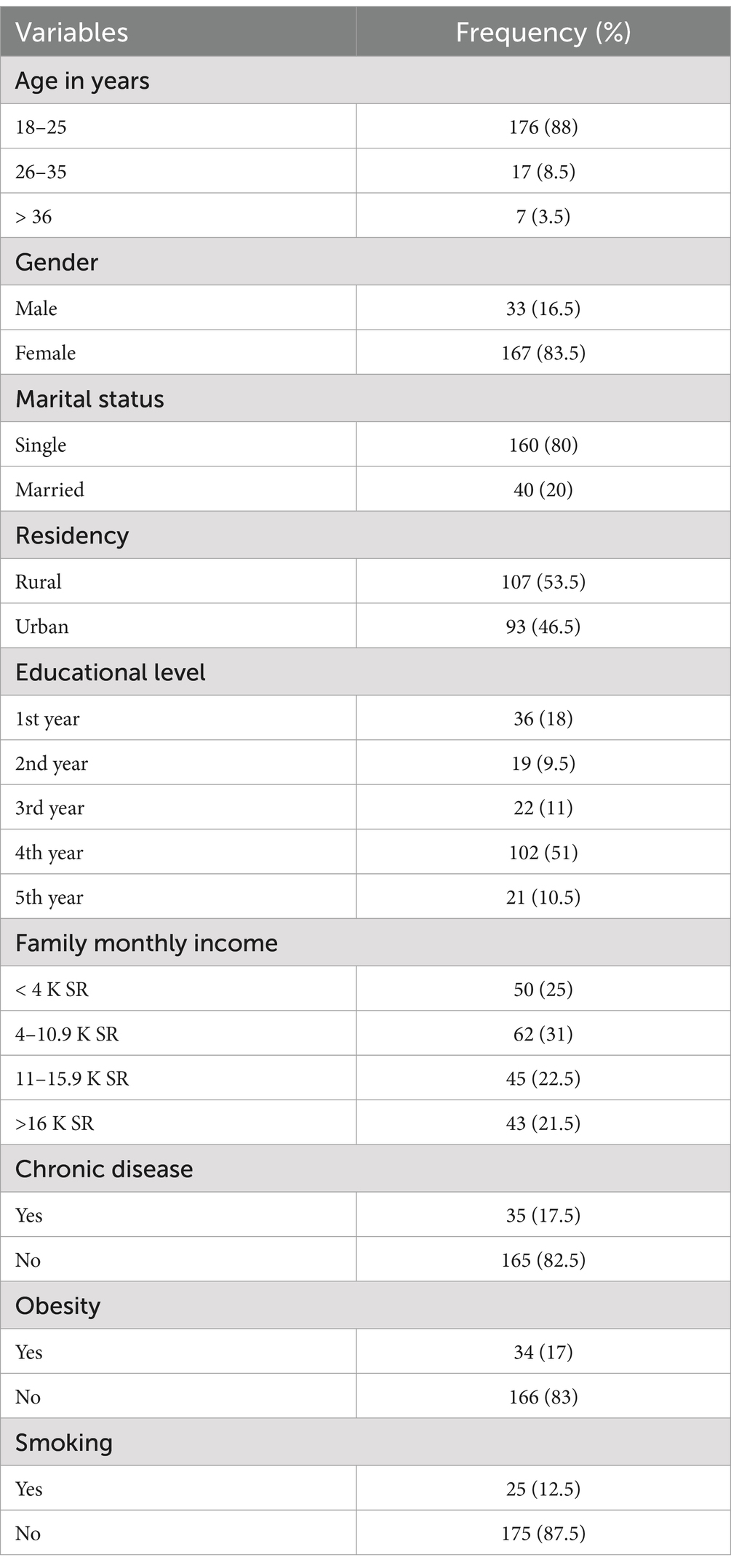
Table 1. Socio-demographic/sample characteristics (n = 200).
Five questions investigated information related to the virus (Table 2). The major source of information for the students was social media 111 (55.5%), followed by healthcare providers 64 (32%), whereas 5 (2.5%) of the students reported having no information. More than one-half, 132 (66%), reported being infected with COVID-19. The large majorities of the students reported administrating the COVID-19 vaccines 188 (94%) and completing the childhood vaccines 179 (89%). Only 76 (38%) reported receiving information about the human monkeypox virus during medical education.
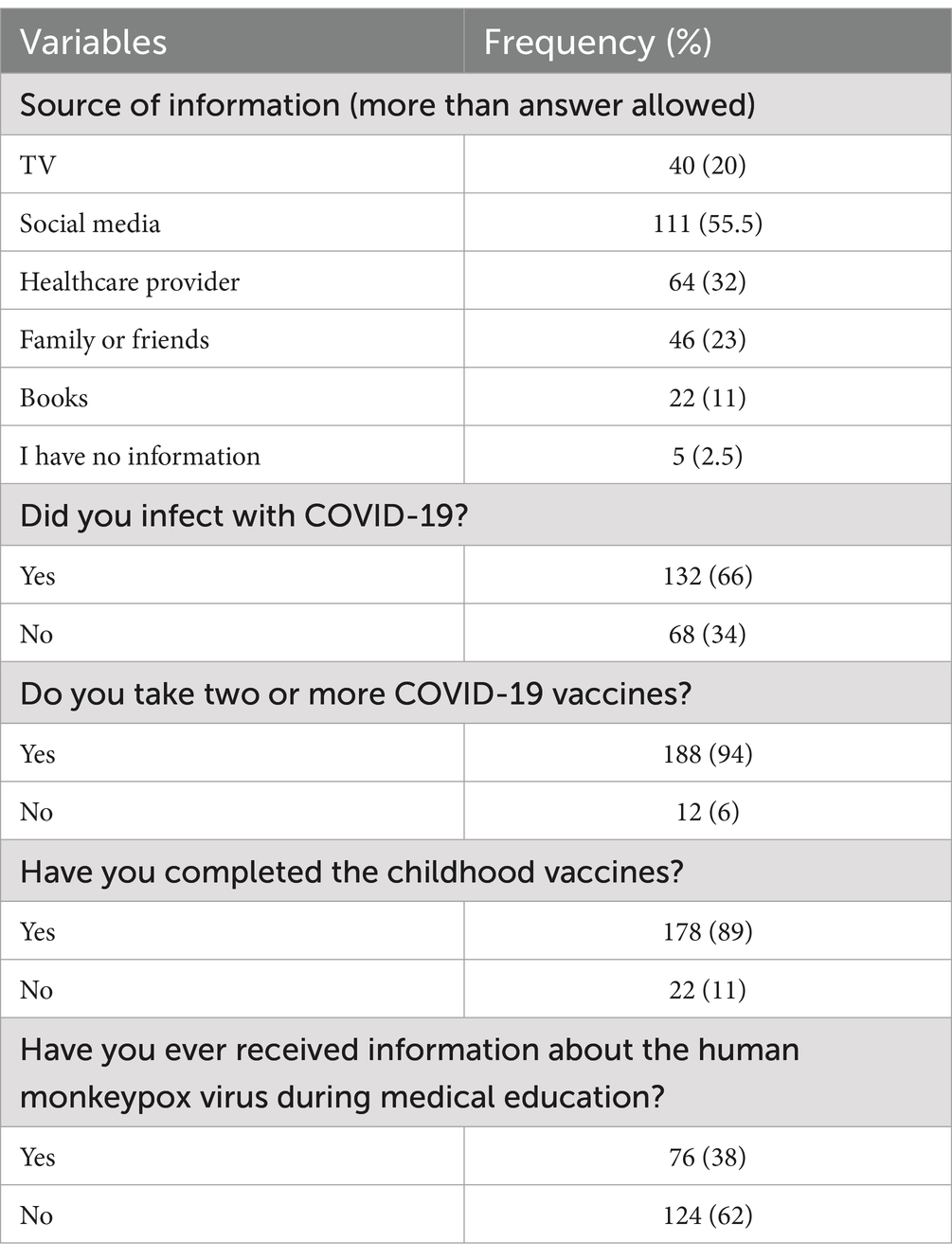
Table 2. Participants information and awareness regarding viral outbreak.
It was reported that the virus causes infectious diseases by 126 (63%) pharmacy students, whereas 28 (14%) did not know (Figure 1).
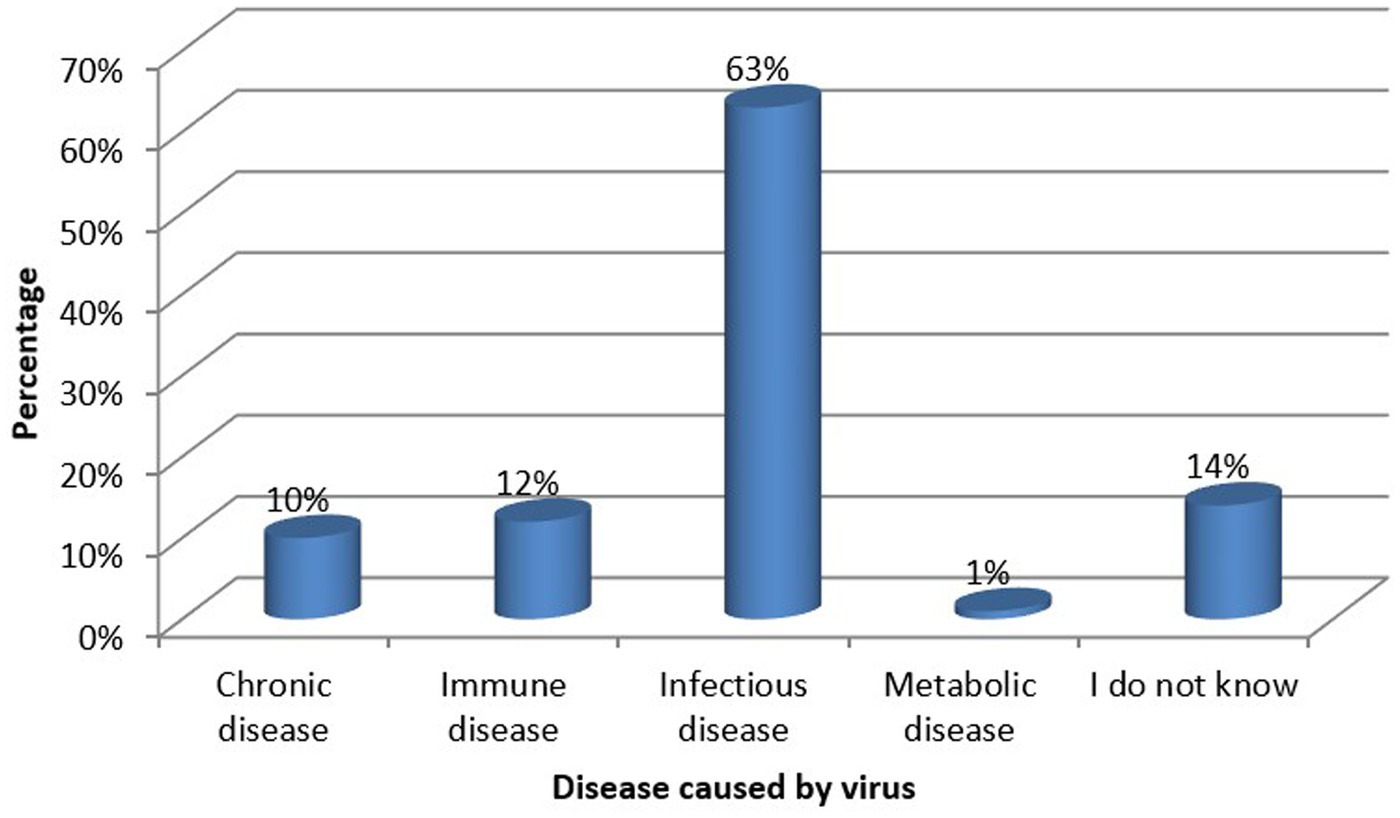
Figure 1. Disease caused by the virus according to knowledge of the students.
The students’ knowledge was investigated through 23 questions with three options as answers: either yes, no, or I do not know. The questions of knowledge and the answers of the students are shown in Table 3. The overall level of knowledge was high among 64 (32%), and it was low among more than one-half of the students 136 (68%).
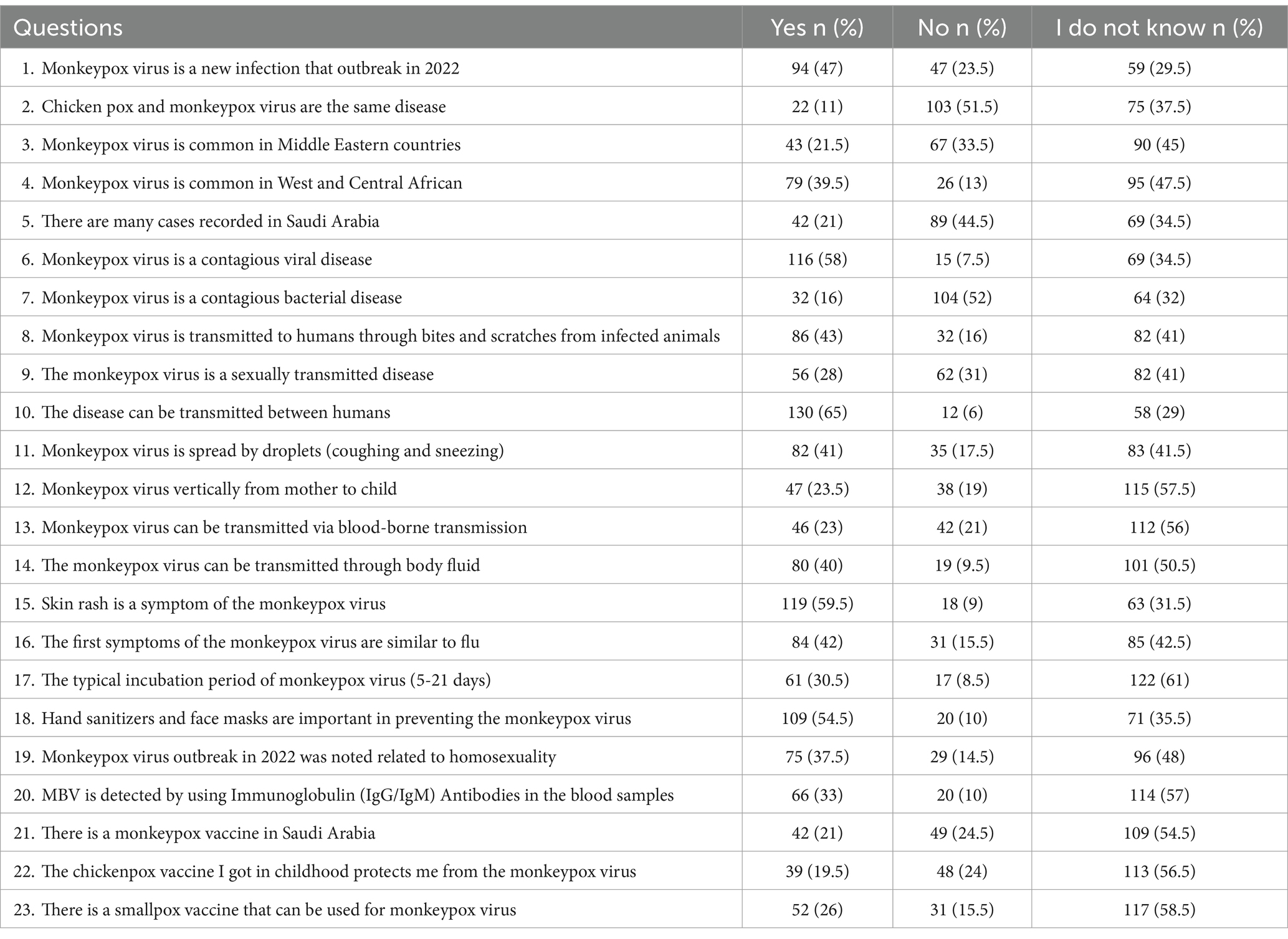
Table 3. Descriptive of participant’s knowledge regarding human Mpox.
The attitude of the students was investigated through seven questions; each question was provided with five answers: either strongly disagree, disagree, neutral, agree, or strongly agree. The questions about attitude and the students’ answers are shown in Table 4. The overall attitude of students was high among only 89 (44.5%), whereas 111 (56.5%) reported a low level of attitude.

Table 4. Descriptive of participant’s attitude regarding human Mpox.
The association between demographics and level of knowledge is shown in Table 5. There were significant association found between knowledge levels and each of gender (p = 0.02), marital status (p = 0.01), family income (p = 0.009), and obesity (p = 0.03).
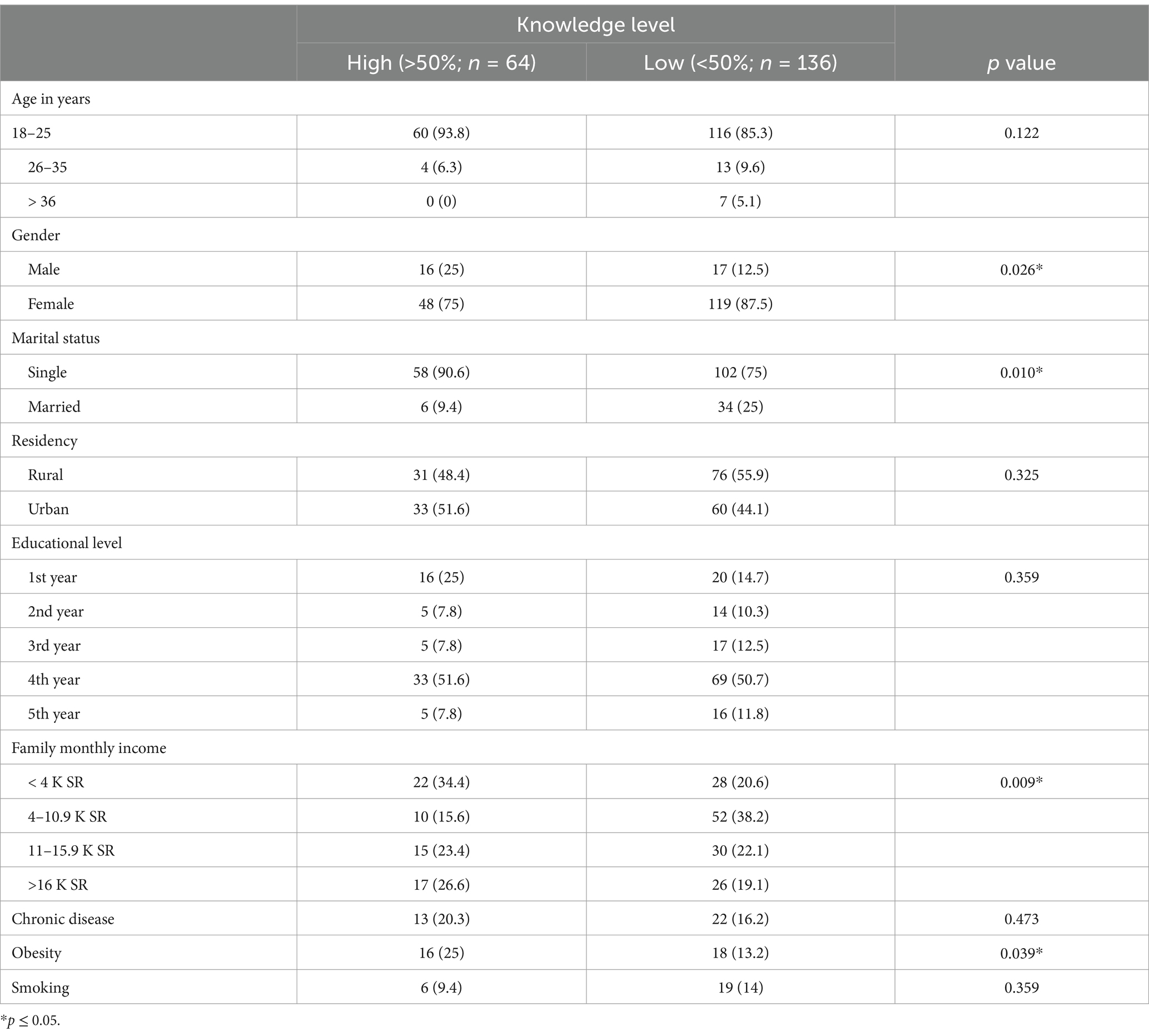
Table 5. Association between socio-demographics and knowledge level.
The association between the knowledge of the students and other factors are shown in Table 6. Significant association were found between knowledge levels and various factors, including family or friends as the source of information (p = 0.039), infection with COVID-19 (p = 0.002), receiving COVID-19 vaccine (p = 0.01), and receiving information about human monkeypox virus (p = 0.016).
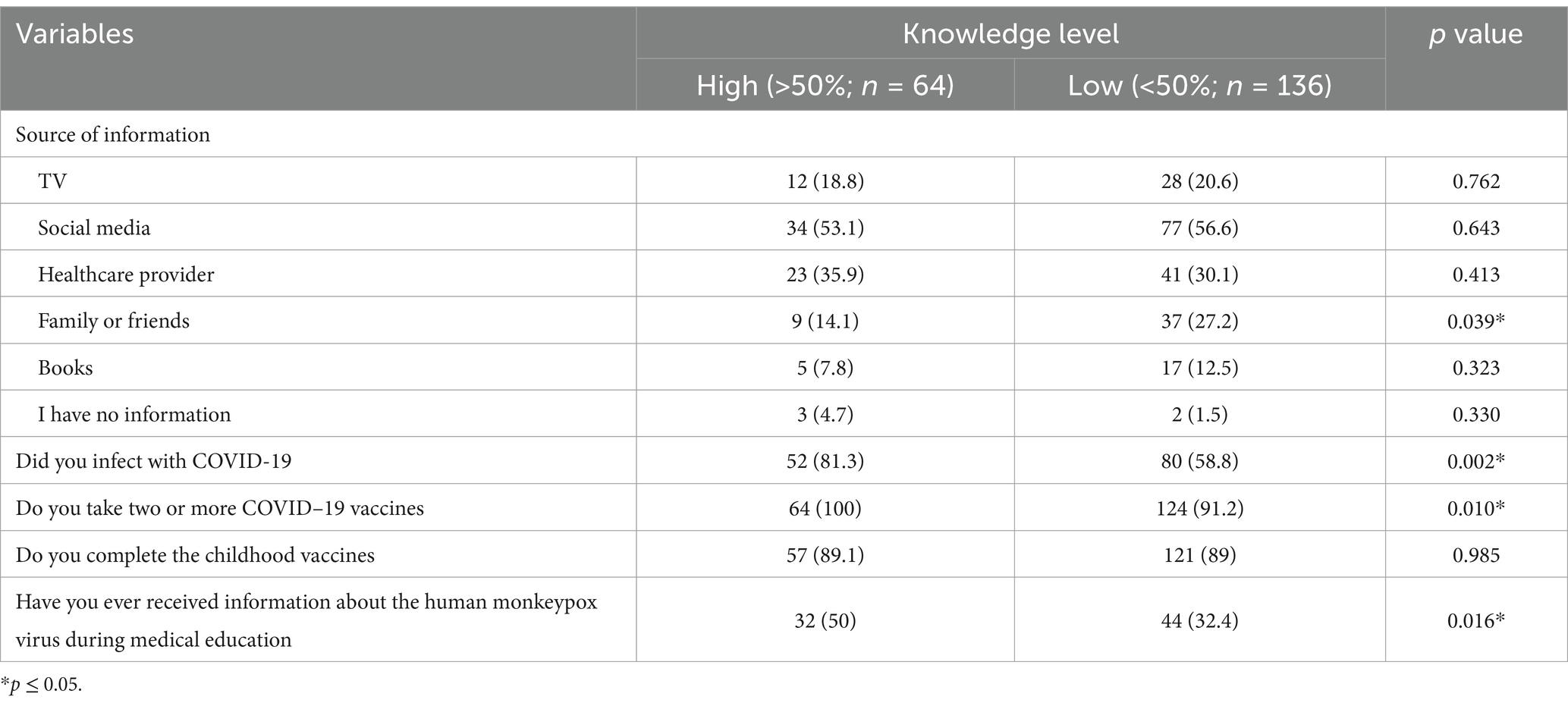
Table 6. Association between awareness and knowledge level.
The association between levels of attitude and demographics of the students are shown in Table 7. Significant associations with attitude were found regarding age (p = 0.03), family income (p = 0.0001), and having chronic disease (p = 0.0001).
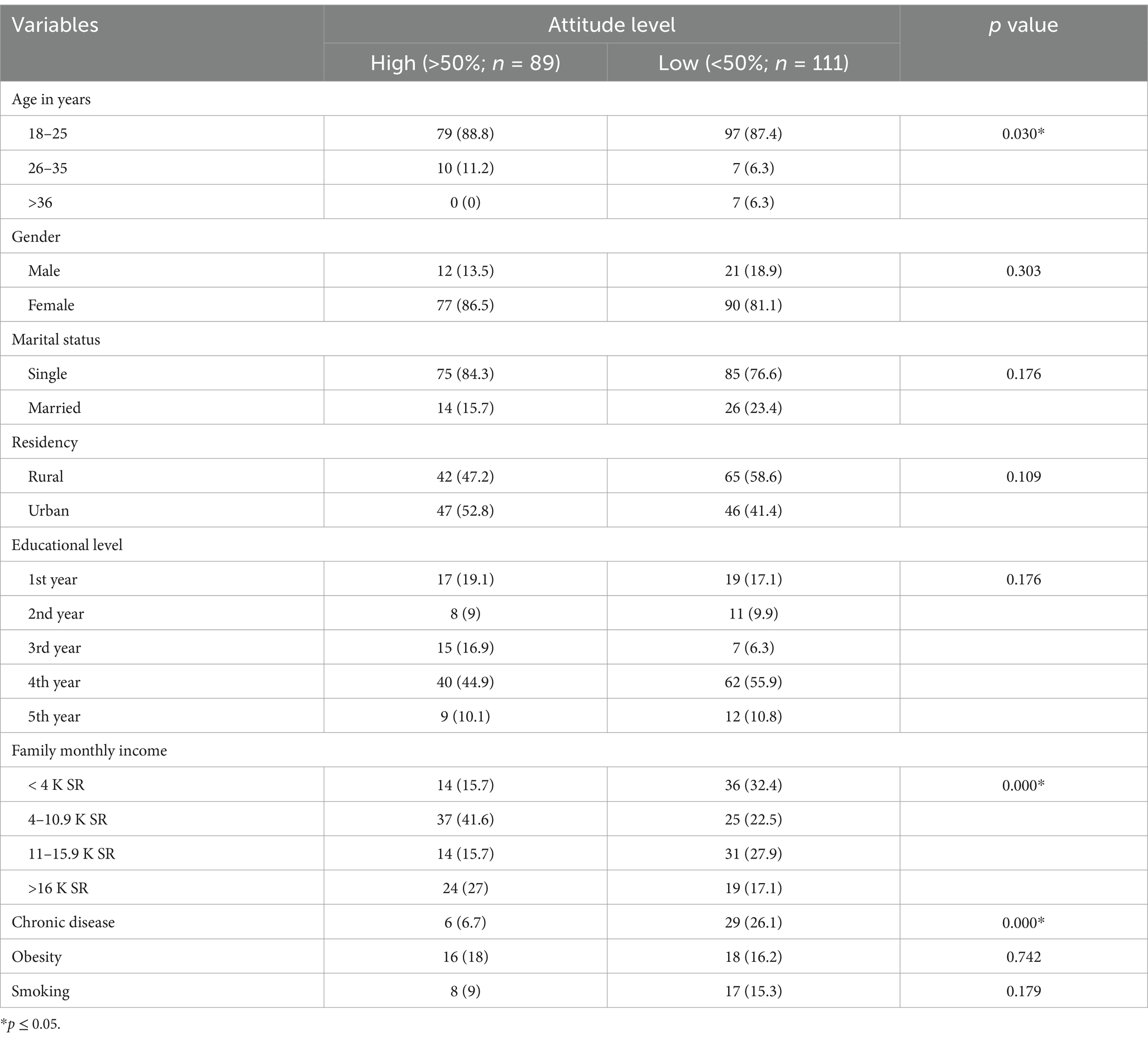
Table 7. Association between socio-demographics and attitude level.
Also, other factors displayed significant correlations with attitude levels, including social media as a source of information (p = 0.007), receiving the COVID-19 vaccine (p = 0.0001), and receiving information about human monkeypox virus (p = 0.004; Table 8).
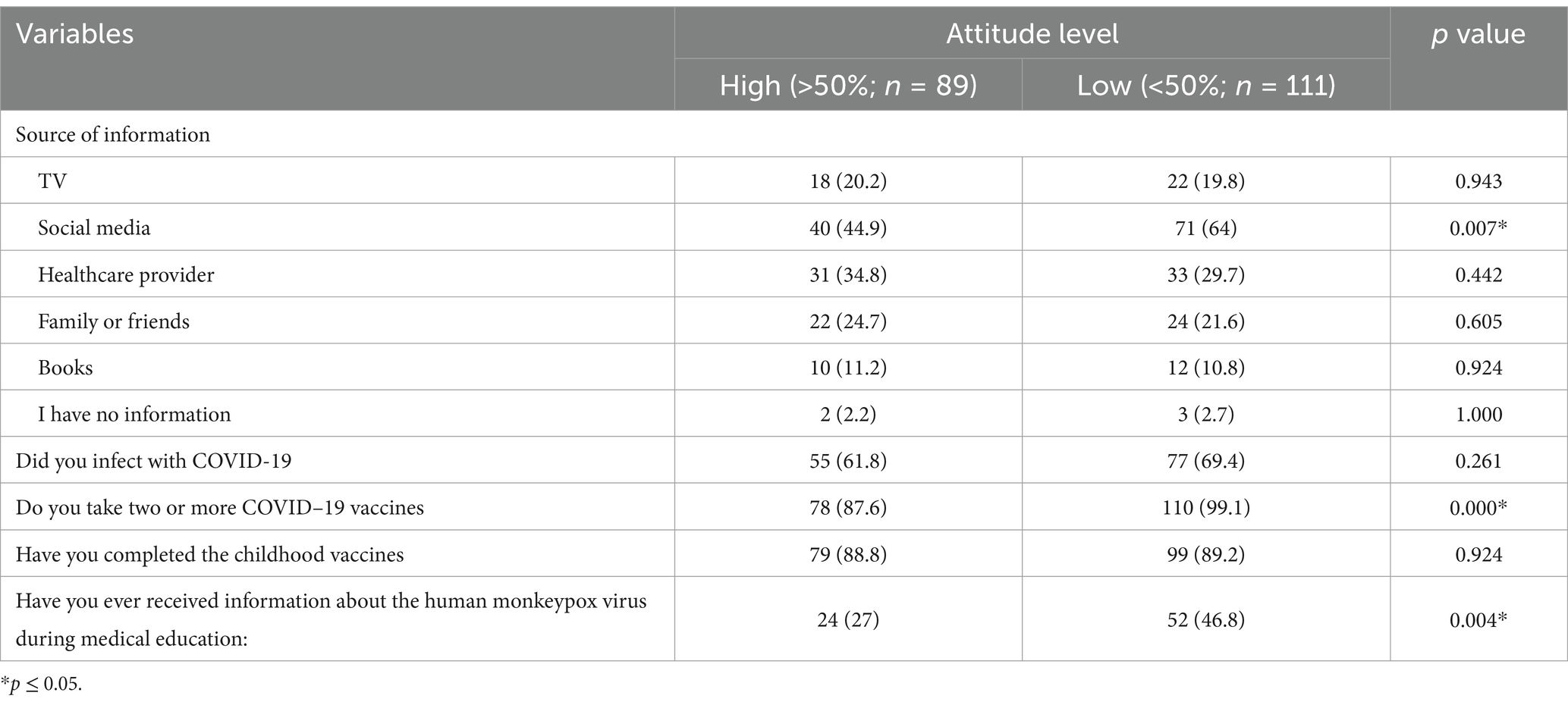
Table 8. Association between awareness and attitude level.
Discussion
This study aimed to assess the knowledge and attitude of pharmacy students regarding monkeypox infection. There is a lack of Saudi studies conducted on this subject that are focused on pharmacy students. In the current study, the overall knowledge of the students was low as higher proportions of students had a low overall level of knowledge.
A previous Saudi study conducted on healthcare practitioners and students revealed that the majority of the participants provided correct answers about the type of microorganisms that cause human Mpox infection. Also, they displayed good knowledge regarding the common symptoms but had poor knowledge regarding the less common symptoms. Additionally, 70% knew the effectiveness of antiviral drugs to treat Mpox (21). The study reported that the participants had gaps in knowledge, with a median score of knowledge of 5 out of 6 as the maximum score. In our study, more than one-half reported that the disease is a contagious viral disease, and 52% did not agree that it is a bacterial disease. Also, more than one-half of the students (59.5%) stated that skin rash is a symptom of the Mpox virus, and 42% reported that the first symptoms are similar to flu. Therefore, the findings in our study reflect gaps in the knowledge of students similar to the previous Saudi study. Additionally, the previous Saudi study found that the knowledge of the participants was independently associated with the age of the participants, where the students and health practitioners aged 30–49 years and 50–69 years reported higher scores of knowledge (22). The contrast was found in our study as there was no significant difference in the level of knowledge between different age groups of the students (p = 0.1).
Similar to our study, a previous United Arab Emirates (UAE) study conducted on medical students reported an inadequate level of knowledge regarding Mpox infection among humans. The mean score of knowledge was 73.95, which indicated a moderate level of knowledge and indicated that 49.3% of the students had good knowledge. There was a significant association between the knowledge of students and receiving information on this viral infection during their education (p<0.01) and seniority (p<0.01) (23). Therefore, it seems that the lack of knowledge among medical students is not restricted to Saudi Arabia alone but to other Arabian countries. In agreement with the previous study there was a significant association between the level of knowledge and receiving information about human Mpox during medical education (18), but in contrast to the previous study, we did not find any association between the level of knowledge and the education level.
In Pakistan, a study enrolled medical, pharmacy, and nursing students, which demonstrated that 21.6% had good knowledge, 43.2% had moderate knowledge, and 35.2% had poor knowledge. Additionally, the factors that significantly affected the level of knowledge were age (p = 0.01), education (p<0.001), and gender (p<0.001). However, in multivariate analysis, education was the only predictor of knowledge (21). The current study showed a lower level of as only 32% had a good level of knowledge, whereas more than half of the students (68%) had poor knowledge. Additionally, we did not find any association between the knowledge level and age or education level; however, in agreement with the previous study, we found that gender was associated with the level of knowledge, and females significantly tended to have lower levels of knowledge.
Another study from Pakistan conducted on University students and reported knowledge and attitude found that the overall knowledge of Mpox was average, with the presence of knowledge gaps in most aspects, whereas the overall attitude was neutral (22). Our study displayed worse findings, where the highest proportions of the students had low knowledge and low attitude. Additionally, we did not find any association between knowledge and residency of the students (p = 0.3), whereas the previous study reported a strong association between the knowledge of the students and region of respondents (24). Additionally, the age of the students was significantly associated with their attitude, and this was in agreement with our findings, where a significant association was found between knowledge and age in our study.
The variations in the levels of knowledge and attitude between our study and other studies from other countries and even the studies conducted on students from other Saudi Regions aren’t surprising. This can be explained by the fact that there are variations in the level of education and information the students receive in each country. Additionally, a previous study conducted on 11,919 medical students from 27 countries revealed that only 12.5% had training on Mpox, and only 55.3 and 51.7% had good knowledge and positive attitude toward Mpox (19). Therefore, our findings seem to be similar to the global findings regarding the low level of knowledge and attitude regarding Mpox among pharmacy students. Additionally, the positive predictors of good knowledge included obtaining information from friends, research articles, scientific websites, and social media. On the other hand, male gender had a negative association with good knowledge of Mpox (19). Despite the fact that we did not perform multivariate analysis, we found that gender had no significant association with knowledge. However, obtaining information from family and friends was associated with a low level of knowledge, which was in contrast to the previous study. Regarding attitude, being in urban regions and in the fifth year of medical education, receiving information from social media or scientific websites was associated with a positive attitude, whereas being male was negatively associated with a positive attitude. Our findings were different as residency region, educational level, and gender had no significant association with attitude. Furthermore, receiving information from social media was significantly associated with a low level of attitude.
There is a lack of studies assessing the attitude of medical/pharmacy students regarding Mpox. A previous Saudi study assessed the knowledge and attitude of healthcare workers regarding Mpox, and it was found that the majority of respondents had inadequate knowledge, but they had positive attitudes (25). In our study, both knowledge and attitude were low among the students. A study from Bangladesh conducted on nurses reported inadequate knowledge but high and positive attitude among the nurses, where the female gender was associated with better knowledge and more positive attitude (26). In our study, the female gender was associated with a low level of knowledge, and both genders had no significant variation regarding the level of attitude. There is a need for development of unified zoonotic disease surveillance system under the one health spectrum to effectively control the spread of Mpox and one health approach need to be adopted to address the crisis for special population and minimize the such outbreak in future (27, 28). The implication of this study suggest that targeted training and educational programs should be developed and implemented. Importantly, our study also highlights the need for increased education and awareness about monkeypox disease among pharmacy students in the Jazan University. By taking these steps, we can better prepare for future outbreaks and ensure the health and safety of the community.
Limitations of the study
One of the potential limitation include this study is being conducted among Jazan University pharmacy students only. Hence we cannot generalize the results to other university pharmacy student’s or other parts of country’s pharmacy students. Another limitation is the study sample could not be considered representative, due to convenience sampling and the potential for selection bias cannot be ruled out due to convenience sampling.
Conclusion
In this study, we investigated the knowledge and attitude of pharmacy students in the Jazan University, Saudi Arabia, toward monkeypox disease and its prevention. The pharmacy students in this study had a low level of knowledge and attitude toward Mpox. The lack of knowledge and negative attitude regarding Mpox seems to be a global issue among pharmacy students and even healthcare workers. Therefore, there is a great need for the establishment of educational programs incorporating pharmacy students and healthcare workers to increase their knowledge and attitude toward Mpox in order to prevent Mpox infections and appropriately manage the infection as possible. Additionally, the factors affecting the knowledge and attitude of the pharmacy students varied, and investigations of further factors are required. In contrast to the health education and health promotion comprehensive One health approach, awareness raising program need to be adopted.
Future scope
Since this study includes only Jazan University pharmacy students hence we cannot generalize the findings. Future research possibilities are to include other university pharmacy students on large sample size. Moreover, qualitative research should be administered to obtain reasonable, broad and more thorough understanding of the knowledge and attitude of human monkeypox viral infection among pharmacy students in Saudi Arabia.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by standing committee for publication and research ethics, Jazan University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EA: Writing – original draft, Conceptualization. AK: Project administration, Writing – review & editing. NA: Writing – review & editing. AbM: Supervision, Writing – review & editing. HT: Methodology, Writing – review & editing. DH: Data curation, Writing – review & editing. ME: Resources, Writing – review & editing. AA: Validation, Writing – review & editing. AnM: Formal analysis, Writing – review & editing. HB: Resources, Writing – review & editing. ZM: Resources, Visualization, Writing – review & editing. AS: Formal analysis, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Altawfiq, JA, Barry, M, and Memish, ZA. International outbreaks of Monkeypox virus infection with no established travel: a public health concern with significant knowledge gap. Travel Med Infect Dis. (2022) 49:102364. doi: 10.1016/j.tmaid.2022.102364
2. Farahat, RA, Sah, R, El-Sakka, AA, Benmelouka, AY, Kundu, M, Labieb, F, et al. Human monkeypox disease (MPX). Infez Med. (2022) 30:372–91. doi: 10.53854/liim-3003-6
3. Moore, M, and Zahra, F. Monkeypox In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing (2022). Eds. Marlyn J. Moore; Balram Rathish; Farah Zahra.
4. Kabuga, AI, and El Zowalaty, ME. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J Med Virol. (2019) 91:533–40. doi: 10.1002/jmv.25348
5. Centers for disease control and prevention (CDC). Human monkeypox - Kasai oriental, Democratic Republic of Congo, February 1996-October 1997. MMWR Morb Mortal Wkly Rep. (1997) 46:1168–71.
6. Vaughan, A, Aarons, E, Astbury, J, Balasegaram, S, Beadsworth, M, Beck, CR, et al. Two cases of monkeypox imported to the United Kingdom, September 2018. Eur Secur. (2018) 38:23. doi: 10.2807/1560-7917.ES.2018.23.38.1800509
7. Yinka-Ogunleye, A, Aruna, O, Dalhat, M, Ogoina, D, McCollum, A, Disu, Y, et al. Outbreak of human monkeypox in Nigeria in 2017–18: a clinical and epidemiological report. Lancet Infect Dis. (2019) 19:872–9. doi: 10.1016/S1473-3099(19)30294-4
8. Durski, KN, McCollum, AM, Nakazawa, Y, Petersen, BW, Reynolds, MG, Briand, S, et al. Emergence of Monkeypox - west and Central Africa, 1970-2017. MMWR Morb Mortal Wkly Rep. (2018) 67:306–10. doi: 10.15585/mmwr.mm6710a5
9. World Health Organization(WHO). WHO director-General’s statement at the press conference following IHR emergency committee regarding the multi- country outbreak of monkeypox. (2022). WHO.
10. Bunge, EM, Hoet, B, Chen, L, Lienert, F, Weidenthaler, H, Baer, LR, et al. The changing epidemiology of human monkeypox—a potential threat? A systematic review. PLoS Negl Trop Dis. (2022) 16:e0010141. doi: 10.1371/journal.pntd.0010141
12. Di Giulio, DB, and Eckburg, PB. Human monkeypox: an emerging zoonosis. Lancet Infect Dis. (2004) 4:15–25. doi: 10.1016/s1473-3099(03)00856-9
13. Alshahrani, NZ, Assiri, AM, Al-Tawfiq, JA, Rodriguez-Morales, AJ, and Sah, R. The human monkeypox in Saudi Arabia and global tourism. Ann Med Surg. (2022) 82:104686. doi: 10.1016/j.amsu.2022.104686
14. McCollum, AM, and Damon, IK. Human monkeypox. Clin Infect Dis: an official publication of the Infectious Diseases Society of America. (2014) 58:260–7. doi: 10.1093/cid/cit703
15. Petersen, E, Kantele, A, Koopmans, M, Asogun, D, Yinka-Ogunleye, A, Ihekweazu, C, et al. Human monkeypox: epidemiologic and clinical characteristics, diagnosis, and prevention. Infect Dis Clin. (2019) 33:1027–43. doi: 10.1016/j.idc.2019.03.001
16. Gallè, F, Bianco, L, Da Molin, G, Mancini, R, Sciacchitano, S, Ferracuti, S, et al. "Monkeypox: what do you know about that?" Italian adults' awareness of a new epidemic. Pathogens. (2022) 11:1285. doi: 10.3390/pathogens11111285
17. Aljahdali, SH, Albeshri, WO, Allqmani, SS, Alhindi, YZ, Elashmoony, S, Aljahdali, S, et al. Knowledge and attitude of human Monkeypox viral infection among healthcare practitioners and students in Saudi Arabia: a cross-sectional study. Cureus. (2023) 15:e45092. doi: 10.7759/cureus.45092
18. Raman, H, Jamil, A, Rasheed, A, Jairoun, AA, Lua, PL, Ibrahim, UI, et al. Knowledge of medical students towards the re-emergence of human Monkeypox virus. Cureus. (2023) 15:e46761. doi: 10.7759/cureus.46761
19. Abd ElHafeez, S, Gebreal, A, Khalil, MA, Youssef, N, Sallam, M, Elshabrawy, A, et al. Assessing disparities in medical students’ knowledge and attitude about monkeypox: a cross-sectional study of 27 countries across three continents. Front Public Health. (2023) 11:11. doi: 10.3389/fpubh.2023.1192542
20. Bloom, BS, Engelhart, MD, and Furst, EJ. Taxonomy of educational objectives: The classification of educational goals: Handbook I: Cognitive domain. New York: David McKay (1956).
21. Riad, A, Drobov, A, and Rozmarinova, J. Monkeypox knowledge and vaccine hesitancy of Czech healthcare workers: a health belief model (HBM)-based study. Vaccine. (2022) 10:202. doi: 10.3390/vaccines10122022
22. Masood, S, Alkubaisi, NA, Aslam, M, Salman, M, Baraka, MA, Mustafa, ZU, et al. Knowledge of human Monkeypox infection among final year medical, pharmacy, and nursing students: a multicenter, cross-sectional analysis from Pakistan. Health. (2023) 11:2777. doi: 10.3390/healthcare11202777
23. Kumar, N, Ahmed, F, Raza, MS, Rajpoot, PL, Rehman, W, Khatri, SA, et al. Monkeypox cross-sectional survey of knowledge, attitudes, practices, and willingness to vaccinate among university students in Pakistan. Vaccine. (2022) 11:97. doi: 10.3390/vaccines11010097
24. Qadah, T. Assessment of knowledge and attitude among healthcare workers towards monkeypox disease: a cross-sectional study from Saudi Arabia. Italian J Med. (2023) 17:1645. doi: 10.4081/itjm.2023.1645
25. Rony, MK, Sharmi, PD, Akter, D, Parvin, MR, and Alamgir, HM. Knowledge and attitude regarding human Monkeypox virus infection among nurses: a cross-sectional study. SAGE Open Nursing. (2023) 9:23779608231216619. doi: 10.1177/23779608231216619
26. Taseen, S, Nasir, F, Abbas, M, Altaf, M, Asghar, MS, and Tahir, MJ. Post-pandemic world at the mercy of monkeypox virus outbreak: time to worry or not? J Med Virol. (2022) 22:1–3. doi: 10.1002/jmv.27948
27. Najimudeen, M, Chen, HWJ, Jamaluddin, NA, Myint, MH, and Marzo, RR. Monkeypox in pregnancy: susceptibility, maternal and fetal outcomes, and one health concept. Int J MCH AIDS. (2022) 11:e594. doi: 10.21106/ijma.594
Keywords: knowledge, attitude, students, monkeypox, Jazan
Citation: Ali EM, Khardali A, Alam N, Meraya AM, Thaibah HA, Hassan DA, Elmobark ME, Aladwani A, Mohanan AT, Bakri HA, Mashraqi ZO and Salhabi AM (2025) Knowledge and attitude of human Mpox viral infection among pharmacy students in Jazan University: a web based cross-sectional study. Front. Public Health. 13:1521923. doi: 10.3389/fpubh.2025.1521923
Edited by:
Milad Zandi, Lorestan University of Medical Sciences, IranReviewed by:
Ayman A. Allam, Zagazig University, EgyptHabibollah Mirzaei, Lorestan University of Medical Sciences, Iran
Copyright © 2025 Ali, Khardali, Alam, Meraya, Thaibah, Hassan, Elmobark, Aladwani, Mohanan, Bakri, Mashraqi and Salhabi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nawazish Alam, bnJhaG1hbkBqYXphbnUuZWR1LnNh