 Julio Arturo Canario-Guzmán1*
Julio Arturo Canario-Guzmán1* Ricardo Elias-Melgen1Eddys Rafael Mendoza1†
Ricardo Elias-Melgen1Eddys Rafael Mendoza1† Luis Felipe Arias1†Roberto Espinal1Jeannette Báez1Sarah Iribarren2
Luis Felipe Arias1†Roberto Espinal1Jeannette Báez1Sarah Iribarren2- 1Centro Nacional de Investigaciones en Salud Materno Infantil Dr. Hugo Mendoza (CENISMI), Santo Domingo, Dominican Republic
- 2University of Washington, Seattle, WA, United States
Introduction: Video Observed-Therapy, a digital adherence technologies (DAT), could improve patients’ adherence to tuberculosis (TB) treatment. However, countries with high TB burden countries, such as the Dominican Republic, struggle to adopt DAT as a control and prevention tool to improve clinical outcomes. Objectives: To describe patients’ knowledge, attitudes and behaviors towards digital technologies for TB control and prevention in the Dominican Republic.
Methods: A mixed-method study was implemented by organizing two Focus Group Discussions (FGDs) and a survey with 137 TB patients. Qualitative data were coded using the Integrated Behavior Model (IBM) and descriptive statistics were used to analyze knowledge, attitudes, practices, and preferences. Data integration was achieved by comparing convergent and divergent results.
Results: Participants expressed a positive attitude towards using DAT to facilitate communication with health personnel to support treatment adherence. Participants noted the benefit of having an application that facilitates this process while safeguarding data privacy.
Conclusion: This study demonstrates positive attitudes among individuals with TB toward adopting digital tools in their follow-up. Current practices suggest that intent to use DAT is prevalent, emphasizing the need to fully transition from intention to adoption of DAT to improve TB treatment outcomes.
1 Introduction
The World Health Organization (WHO) and global partners recognize the critical role of digital health in advancing the global response to tuberculosis (TB) and have designed a comprehensive digital health agenda (1–4). Despite these efforts, the adoption and integration of digital adherence technologies (DAT) in the health sector, particularly in low- and middle-income countries remains challenging (5). The Dominican Republic (DR), with a high TB incidence rate, reported approximately 45 [33–57] new TB cases per 100,000 inhabitants in 2021 (6).
To reduce the burden of TB in the DR, the National TB Program (NTBP) of the Ministry of Public Health (MoPH) implements the Directly Observed Treatment Short-Course (DOTS) strategy. However, in 2020, 16% of the TB patients who started DOTS did not complete their treatment (7). Several factors contribute to incomplete treatment including difficult access to healthcare, patient knowledge, poverty, drug use, comorbid illnesses, treatment-related adverse events, poor patient-provider communication, and self-treatment (8–10).
To achieve WHO target of 90% treatment success rate (11), various initiatives have been made. These efforts include shortening treatment duration (12), improving medication adherence, integrating digital technologies and health behavior models to increase effectiveness in changing behavior and improving medication. Digital technologies (short message services -SMSs- via mobile phones) and, more specifically, digital adherence technologies (DATs) tools designed to support individuals with TB with taking their medication (medication sleeves; smart pill boxes; video-observed treatment) (13–15).
From the available alternatives to increase treatment adherence, we proposed the use of Video Observed Therapy (VOT). In the Dominican Republic, the use of messaging and video application is widespread and widely accepted. Also, VOT could address barriers with DOTS, such as travel time and related costs (16–21). TB is considered a disease of the poverty, so patients can benefit from reducing the number of visits to the clinic. VOT as intervention has evidence of improvement medication adherence (22).
At the inception of this study in 2018, VOT had not been implemented in the DR. The onset of the COVID-19 pandemic disrupted TB control efforts but accelerated global adoption of digital tools in TB programs (5, 23). In response, the DR developed a new protocol to facilitate the use of DAT for remote TB patient follow-up. Extending drug supply periods and implementing remote monitoring and support proactively can mitigate the risk of patient loss to follow-up (24–27). The overall objective of this study was to explore and describe TB patient attitudes and behavior towards digital technologies for TB control and prevention.
2 Methods
2.1 Study design
A convergent mixed-method design was used to pursue the aim of this study. Qualitative and quantitative components were combined to explore and describe TB patients’ attitudes and behavior, regarding using digital technologies in their TB care and management. Focus group discussions (FGDs) were held with nine individuals with TB, and 137 were surveyed between September and January 2021 in Santo Domingo, Dominican Republic. Ethical approval was obtained from the Research Ethics Committee at the Centro Nacional de Investigaciones en Salud Materno Infantil Dr. Hugo Mendoza (CENISMI) (#31082020). Written informed consent was obtained from all study participants. Confidentiality and data protection measures were undertaken by using encrypted laptops and files with restricted access to the study team and PI.
2.2 Qualitative component: participant focus group discussions
A FGD guide with open-ended questions was developed based on the Integrated Behavioral Model (IBM) (28) constructs, which combines constructs from the Theory of Reasoned Action (29) and Planned Behavior (30). Questions include, for example, have you ever used a telephone or a computer with the Internet to search for health information or monitor your health status? What do you like/dislike about the idea of reviewing a video recording of the patient taking medication at home and sending it to the doctor? We aimed to explore participants’ knowledge, attitudes, practices, and preferences for using digital technologies during their treatment. The questionnaire was discussed between the research team, and comments on content validation and language and cultural appropriateness of the questions. The questionnaire passed by different rounds of revision until a final version was agreed upon by the researchers. The questionnaire is in the Annex section.
The FGDs were conducted in TB Units in two health centers in the province of Santo Domingo (Boca Chica and Villa Mella). Inclusion criteria were being bacteriologically confirmed with TB, 18 years of age and older, who had initiated or recently completed treatment (within the last 3 months). Convenience sampling was used. Healthcare workers from the TB units recruited participants consecutively in person as they came in for follow-up appointments. If interested in participating, they were connected with a research team member who facilitated the informed consent process and scheduling the FGDs. Each FGDs session lasted approximately 1 h and was audio-recorded.
2.3 Quantitative component: survey
For the quantitative component, identical inclusion/exclusion criteria were applied. Participants were recruited from eight TB units across the province of Santo Domingo and the National District with the highest cases of TB in the country. Health care workers at TB units recruited participants. The survey was administered in person. The survey consisted of 58 questions in 6 sections: (a) sociodemographic, clinical, and adherence characteristics, (b) knowledge, (c) attitude, (d) practices, (e) access to health care, and (f) economic consequences. The questionnaire included questions on preferences for TB digital treatment monitoring. Data from medical records was collected to describe the clinical characteristics of the participants.
2.4 Analysis
FGD sessions were transcribed verbatim and independently coded by two research team members using practical thematic analysis that uses both deductive and inductive analysis. Categories and themes were developed a priori based on the IBM constructs to create a structured categorization matrix. Inductive codes were also developed by the two members, who meet as a team regularly to review codes and ensure consistency in reaching a consensus collaboratively. The data was analyzed using thematic analysis. The steps Saunders et al. suggested to conduct a practical thematic analysis were followed (31).
Statistical analysis was performed in the quantitative study phase using SPSS 20.0 Software. Descriptive statistics are presented in percentages, median, max and min values. The data from continuous variables (age, schooling, etc.) are presented as the median value plus the minimum and maximum values. Demographic data are presented as frequency and percentage. Quantitative and qualitative data were analyzed separately and compared to explore convergent and divergent results. The Good Reporting of a Mixed Methods Study (GRAMMS) guidelines were used to guide the reporting of this study (31).
3 Results
3.1 Quantitative findings
3.1.1 Survey participant characteristics
137 TB individuals with TB participated in the study, with 40 (n = 29.2) in the National District and 97 (n = 70.8) in Santo Domingo. Among the participants, 75 (54%) were male. Most survey participants identified as Dominican (n = 133, 97.1%), three Haitians (n = 3, 2.2%), and one Venezuelan (n = 1, 0.7%). Most reported being single (n = 78, 56.9%) and with a partner (n = 47, 34.3%). Most participants reported literacy skills, with 97.1% (n = 133) being able to read and write. Regarding education, 33% (n = 45) had a primary school level, nearly 50% (n = 69) completed secondary school, and 12% (n = 16) attended university (Table 1).
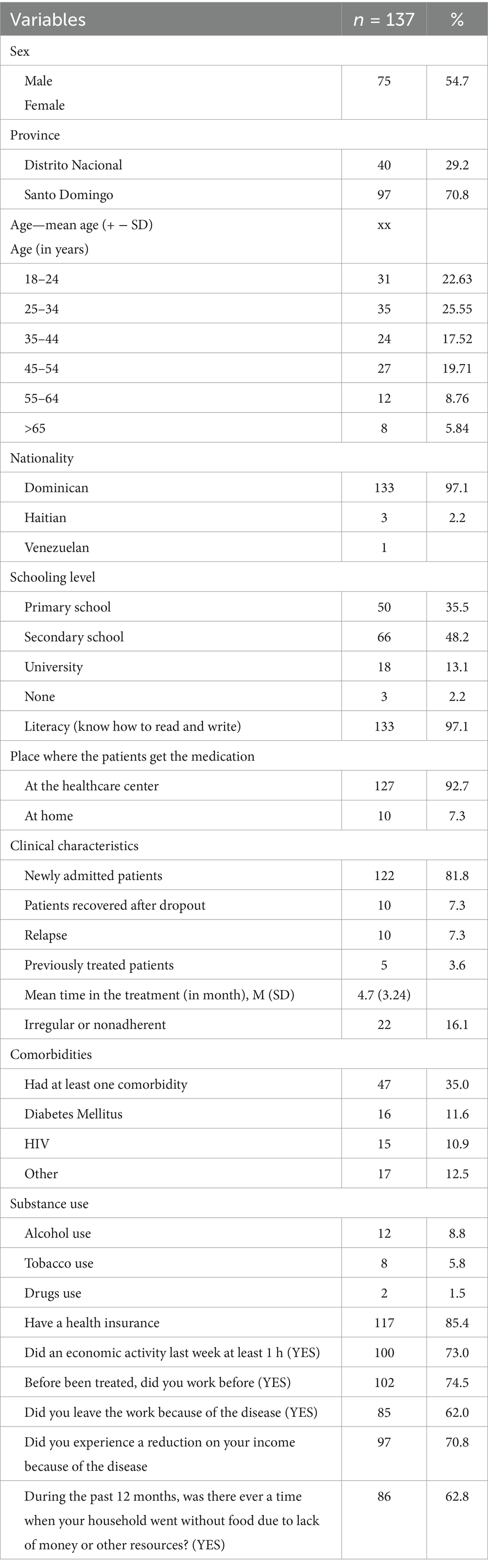
Table 1. Sociodemographic and clinical characteristics of the TB patients who were included in the study, Santo Domingo, 2019 (n = 137).
3.1.2 Clinical characteristics
Predominantly, the participants were newly admitted patients (n = 112, 81.8%), followed by those recovered after dropout (n = 10, 7.3%), relapse (n = 10, 7.3%), and previously treated patients (n = 5, 3.6%). The mean treatment duration was 4.07 months (SD: 3.27, min = 1, max = 24). A small percentage were healthcare workers (n = 6, 4.3%). Over 90% attended the health center for medication, and 95% had not completed treatment in the past 3 months. Patients who could not follow up represent 4.4% (n = 6) and 12% (n = 17) recovered. Approximately 63% (n = 86.3) were self-administering the medication and supervised by video call, 27% (n = 37) were self-administering the medication without supervision, 8% (n = 10) reported recording a video, and 2.2% (n = 3) attended the health center in person (Table 1).
3.1.3 The integrated behavioral model (IBM) categories
We summarized the results in this section. In Table 2 we integrate qualitative and quantitative data.

Table 2. Knowledge, attitudes, practices of individuals with TB related to the use of digital technologies for prevention and control, Santo Domingo, 2019 (n = 137).
3.1.3.1 Knowledge
Most participants recognized cough (73.0%, n = 100) as a disease symptom. Other symptoms were less known such as cold (46.7%, n = 64), weight loss (25.5%, n = 35), phlegm (12.4%, n = 17), shivers (13.1%, n = 18), fatigue (13.1%, n = 18). Most (97.1%, n = 133) know the disease can be cured. Of those, 81.0% (n = 111) believe it is cured with pills from the health center (self-administered), 16.8% (n = 23) mention that pills should be taken under medical supervision. Some mention resting (8.8%, n = 12) and natural or home remedies (6.6%, n = 9). Concerning factors preventing recovery, 98.5% (n = 135) believe that not taking medicine daily is the main reason. Other factors mentioned include alcohol consumption (17.5%, n = 24), poor nutrition (14.6%, n = 20), lack of rest (14.6%, n = 20), and drug use (13.1%, n = 18). Only 2.2% (n = 3) believe that lack of prayer affects healing. Table 2 shows descriptive data on knowledge questions.
3.1.3.2 Attitudes
The majority, 90.5% (n = 124), understood that a cell phone can be utilized for healthcare purposes. Receiving health-related text messages was highly rated as potentially helpful (84%). Most participants found it appropriate (n = 69, 50.4%) or very appropriate (n = 56, 40.9%) to receive reminders about their TB treatment on their phone. Regarding their level of information about TB, only 32.1% (n = 44) felt ‘very informed’, (40.9%, n = 56), while others ranged from somewhat informed (n = 16, 11.7%), ‘little informed’ (13.1%, n = 18), to ‘not at all informed’ (n = 3, 2.1%). Nearly all users understand the importance of taking medication daily to cure the disease (Table 3).
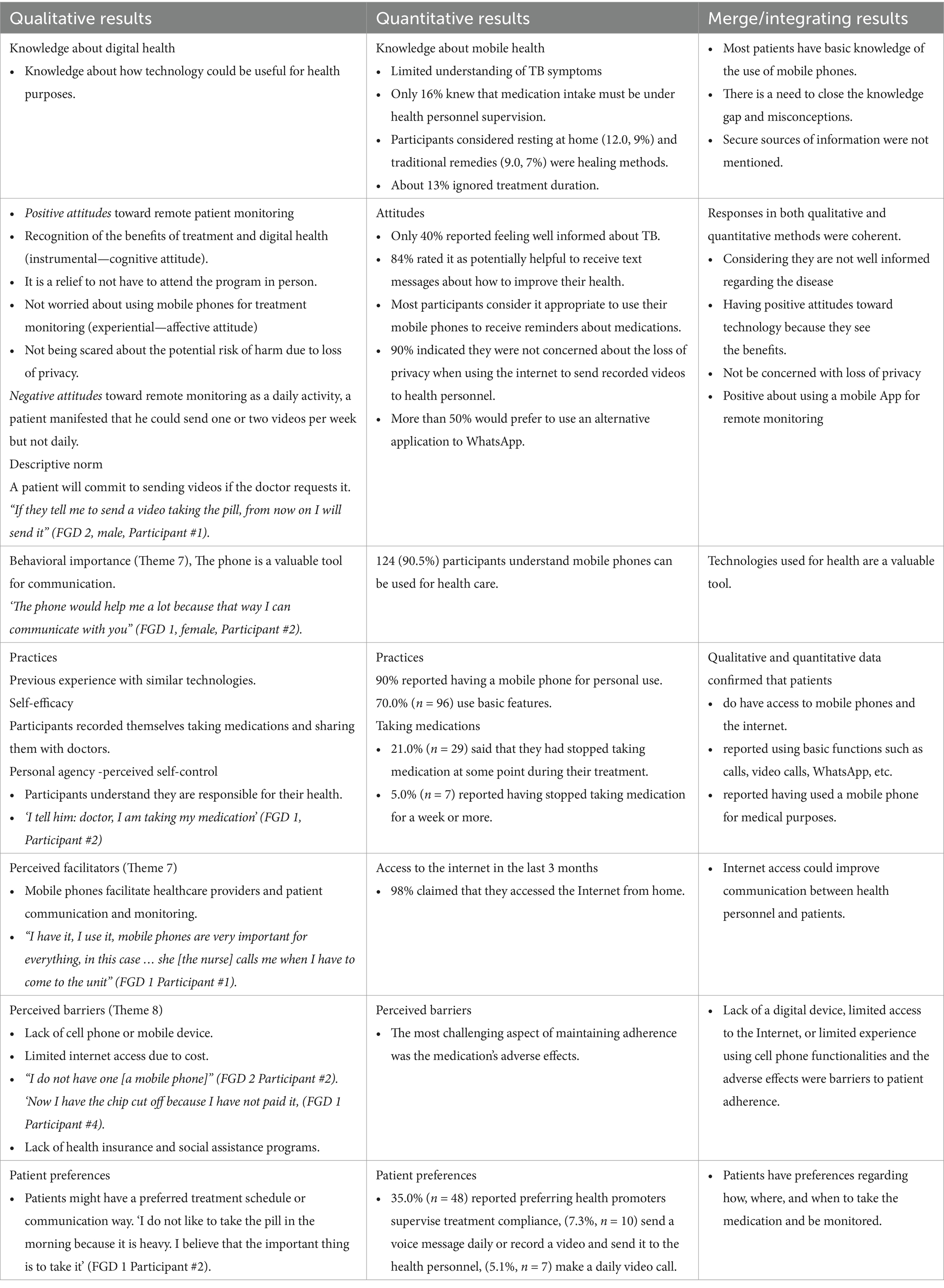
Table 3. Merge results from quantitative and qualitative analysis of IBM variables measured in individuals with TB, Santo Domingo, 2019.
3.1.3.3 Practices
A significant majority, 89.8% (n = 123) reported having a personal cell phone. Most participants, 86.9% (n = 119), used their phones several times a day, 2.2% (n = 3) said they used it only once today or in the last 24 h, while 10.2% (n = 14) responded that they do not currently use it. Basic features such as sending and receiving text messages were commonly used (n = 96, 70%). About 63% (n = 86) used their phones for personal calls, and half of them used it for chatting (WhatsApp), 23% (n = 32) for social networks (Facebook, Twitter), 10% (n = 14) for work calls, 6.6% (n = 9) for shopping, and 5% (n = 7) as an alarm clock. Having internet access from home in the last 3 months was reported by 98% (n = 123). Few reported using mobile phones as a reminder of their appointments or medication monitoring (n = 11, 8%).
3.1.4 Clinical and adherence characteristics
According to medical records, 16.1% (n = 22) of participants were irregular or nonadherent to treatment. 35% of participants had at least one comorbidity, with diabetes (11.6%, n = 16) and HIV (10.9%, n = 15) being the most frequent. Participants reported substance use: alcohol use (8.8%, n = 12), tobacco use (5.8%, n = 8), and drugs (1.5%, n = 2).
3.2 Qualitative findings
Nine patients participated in the FGDs: the first group comprised 6 users (4 men, 2 women), with ages ranging from 19 to 56 (mean 35.2), and the second group included 3 men, with ages ranging from 23 to 60 (mean 40.6). Participants had a low socioeconomic status, and the level of education was primary. Every week or every 2 weeks, they pick up the medications as scheduled by the team. The qualitative findings centered on eight core themes from IBM. Exemplars for each theme are presented in Table 2.
3.2.1 Theme 1—knowledge
This theme encompassed two categories: knowledge about digital tools and knowledge about TB as a disease. Participants described a lack of information about TB and basic knowledge about digital tools. “For me, it is important [access to technology] because at the beginning of the disease [TB] one does not know anything” (FGD 1 Participant #1).
3.2.2 Theme 2—experiential and instrumental attitudes
Participants reported not being concerned about using their cell phones for communication and treatment monitoring (experiential-affective attitude). They recognized the benefits of treatment and using digital health tools (instrumental-cognitive attitude). ‘The doctor told me like [sic] I was not taking the pill, but I take it during the week, and I said: “no, but I’ll make a video for you so you can see me taking it”’ (FGD 1 Participant #4).
3.2.3 Theme 3—Perceived norm
Participants expressed the need to demonstrate their treatment compliance by sending videos or calling health personnel. Some participants noted they would only send a video if requested explicitly by the doctor (injunctive norm—what others expect them to do -). “If they tell me to send a video taking the pill, from now on I will send it” (FGD 2, male, Participant #1).
3.2.4 Theme 4—personal agency
Comments reflected perceived self-control and self-efficacy. ‘I tell him: doctor, I am taking my medication’ (FGD 1, Participant #2). ‘I was at a party, yes, but now I am ready for my thing again [to re-start medication]’ (FGD 2 Participant #1).
3.2.5 Theme 5—practices
This theme included participants’ familiarity and proficiency in using technology and taking medication. Participants responded as if it were obvious that they knew how to use “technology” (cell phones), popular apps, and social media. ‘I use WhatsApp, Facebook, and Instagram.’ (FGD 1 Participant #4).
3.2.6 Theme 6—facilitators
Participants generally perceived mobile devices as facilitators that allow interaction with health personnel. “I have it, I use it, mobile phones are very important for everything, in this case … she [the nurse] calls me when I have to come to the unit” (FGD 1 Participant #1).
3.2.7 Theme 7—importance of the behavior
Mobile devices are considered necessary, particularly as reminders and communication channels. ‘The phone would help me a lot because that way I can communicate with you” (FGD 1, female, Participant #2).
3.2.8 Theme 8—perceived barriers
Perceived barriers were associated with the lack of a digital device, limited internet access, or limited experience using cell phone functionalities (e.g., social networks and video calls). Barriers to treatment adherence also included patient preferences regarding the time to take the medication, lack of health insurance, and participation in government assistance programs. “I do not have one [a mobile phone]” (FGD 2 Participant #2). ‘Now I have the chip cut off because I have not paid it, (FGD 1 Participant #4).
3.3 Integrating phase
Quantitative data showed a limited understanding of basic aspects of the disease, and qualitative data confirmed the importance that participants place on digital health. Positive attitudes were identified toward being remotely monitored, receiving text messages, and using their phones for health purposes. Also, they stated that they do not have privacy concerns or are scared about the potential risks of losing privacy while using digital technologies. Key findings for the IBM variables are presented in Table 3.
4 Discussion
This study aimed to describe patients’ attitudes and behaviors digital technologies for TB control and prevention. According to medical records and patient reports in the study, 16.1% of the patients showed irregular medication taking. This aligns with the National TB Program’s Annual Report 2020 findings, which reported that 11 to 25% of patients were lost to follow-up treatment, depending on their clinical and sociodemographic characteristics (23). However, the percentage of non-adherence to treatment may be even higher in this population. Unfortunately, the report did not provide a specific indicator for treatment adherence. Participants in the study showed a knowledge gap (e.g., only 16% knew the importance of DOT) and expressed a desire for more information about TB and its treatment. This situation partially explains the high rate of lost follow-up and irregular medication taking. A qualitative study of KAP towards TB in Georgia revealed good knowledge among current and former TB patients (32). Consistent with other studies, we found that patients can learn about their condition (33).
Participants expressed a positive attitude towards the benefits of using digital technology for communication with health personnel to support taking treatment and remaining adherent, dispelling fears of privacy loss. Most participants (n = 69, 50.4%) wanted to receive text messages providing health tips and reminders. Several other studies have attempted to evaluate evidence for the efficacy of various DAT interventions such as texting, Short Message Service (SMS) reminders, and mobile phone Apps, among other resources, at improving treatment adherence. Different studies have identified modest or no efficacy of SMS in improving treatment adherence (34–36), while other programs using interactive SMS (14, 15) have proven effective in enhancing medication adherence (16).
Iribarren et al. used the Information-Motivation-Behavioral Skills model to design and document the development of the intervention with a multidisciplinary team of researchers, clinicians, administrators, and patients in active TB treatment (37). In the DR, we used an Integrative Behavioral Model to develop a DAT that is informed by a health behavior model that has been found successful at improving health-related behaviors (28).
Participants reported using avoidance strategies, eluding thinking ‘negative things’ about the disease and focusing on positive aspects of treatment (such as taking medication to get well-perceived self-management). Patients’ may have an interest to demonstrate compliance with treatment as perceived norm on how they should behave as users of the healthcare services. These aspects emphasize the need for tailored text messages supporting self-regulation (16) helping them on how to avoid negative thoughts as the integrative model of behavioral prediction can be used for this purpose (38).
Environmental barriers, such as limited access to digital devices and the internet, were identified in low- and middle-income countries (17–19). Cost considerations, particularly the affordability of cell phone services, pose challenges. The average monthly mobile phone plan exceeds the purchasing power of low-income families, as most often people with TB fall into this category. When writing this report, the average low-income family makes less than $675 per month, whereas the average monthly mobile phone plan is $55.00 (39). Mobile phones are needed in order to use health apps that have been proved to be effective for scheduled follow-up visits and improves the probability of follow-up, reducing missing appointments and optimizing patient outcomes (40). So, improving access to technology to patients can be recommended for low-income TB patients in the DR.
Behavioral models have been effectively applied in TB treatment adherence studies using mobile applications (37, 41–43), and similar models have demonstrated success in understanding TB prevention and treatment (15). In a literature review of articles published between 1995 and 2015 on text messaging and mobile phone apps with adherence or compliance and youth/adolescents, only 32% of the identified studies incorporated a theoretical framework in their design (36). Our study was driven by a theoretical model that can be further reviewed, analyzed, or improved for advancing health behavior science.
4.1 Limitations
Data collection occurred during the COVID-19 pandemic in December 2020, potentially influencing participant perspectives. The low number of participants in the FGDs and the need to scrutinize psychometric properties within the IBM constructs should be considered.
The COVID-19 pandemic restrictions impacted the number of patients visiting healthcare services and the number of patients who could be invited to the clinics. Therefore, small numbers were invited to the FGD sessions for safety measures and to comply with guidelines.
4.2 Conclusions and recommendations
Findings highlight a digital divide, with some users preferring traditional healthcare visits. Interventions should consider patients’ preferences rather than impose new modalities. As most participants already use mobile phones to communicate with healthcare personnel, a VOT intervention is feasible.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité de Ética de Investigación CENISMI. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
JC-G: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. RE-M: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. EM: Data curation, Formal analysis, Investigation, Software, Writing – review & editing. LA: Investigation, Writing – review & editing, Formal analysis, Writing – original draft. RE: Writing – review & editing, Investigation, Supervision. JB: Writing – review & editing, Project administration. SI: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Research Fund of the Ministry of Higher Education and Technology FONDOCyT (Grant No. 2018-2019-3A7-214) Dominican Republic.
Acknowledgments
We are thankful to Pedro G. Suarez for his thorough review of the study protocol and manuscripts, to Yaneiris Cuevas from the National Health Service for her input during the design phase of the mobile App, and to Nicole Galán from CENISMI for her contributions reviewing the results section.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. (2015). WHO. Digital health for the end TB strategy - an agenda for action. Available online at: http://www.who.int/tb/publications/digitalhealth-TB-agenda/en/ (Accessed February 20, 2020).
2. Moscibrodzki, P, Parkinson, S, Ferry, R, Nwaneri, N, and Thies, W. (2021). Mapping the technology landscape of national TB programs: Report [internet]. Geneva, Switzerland; Available online at:https://www.theglobalfund.org/en/updates/2021/2021-10-18-mapping-the-technology-landscape-of-national-tb-programs-report/ (Accessed December 20, 2023).
3. The Stop TB Partnership. (2023). Digital health technology hub [internet]. Available online at: https://www.stoptb.org/accelerate-tb-innovations/digital-health-technology-hub (Accessed December 20, 2023).
4. World Health Organization. (2023). Report of the WHO consultation on digital technologies for tuberculosis [internet]. Available online at:https://www.who.int/publications-detail-redirect/9789240068254 (Accessed December 20, 2023).
5. Chang, LW, Njie-Carr, V, Kalenge, S, Kelly, JF, Bollinger, RC, and Alamo-Talisuna, S. Perceptions and acceptability of mHealth interventions for improving patient care at a community-based HIV/AIDS clinic in Uganda: a mixed methods study. AIDS Care. (2013) 25:874–80. doi: 10.1080/09540121.2013.774315
6. World Health Organization. (2021). Global Tuberculosis report 2021 [internet]. Available online at: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021 (Accessed October 23, 2021).
7. División de Tuberculosis, Ministerio de Salud Pública. (2017). Situación del Programa Nacional de Control de la Tuberculosis en la Republica Dominicana-2017″. Santo Domingo, República Dominicana.
8. Ruru, Y, Matasik, M, Oktavian, A, Senyorita, R, Mirino, Y, Tarigan, LH, et al. Factors associated with non-adherence during tuberculosis treatment among patients treated with DOTS strategy in Jayapura, Papua Province, Indonesia. Glob Health Action. (2018) 11:1510592. doi: 10.1080/16549716.2018.1510592
9. Zhang, J, Yang, Y, Qiao, X, Wang, L, Bai, J, Yangchen, T, et al. Factors influencing medication nonadherence to pulmonary Tuberculosis treatment in Tibet, China: a qualitative study from the patient perspective. Patient Prefer Adher. (2020) 14:1149–58. doi: 10.2147/PPA.S252448
10. Sousa, GJB, Maranhão, TA, MJS, DLT, De Souza, JT, TMM, M, and MLD, P. Prevalence and associated factors of tuberculosis treatment abandonment. Rev Esc Enferm USP. (2021) 55:e03767. doi: 10.1590/S1980-220X2020039203767
11. World Health Organization. (2023). Indicator metadata registry details [internet]. Available online at: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/332 (Accessed December 22, 2023).
12. Singh, V. Tuberculosis treatment-shortening. Drug Discov Today. (2024) 29:103955. doi: 10.1016/j.drudis.2024.103955
13. Sazali, MF, Rahim, SSSA, Mohammad, AH, Kadir, F, Payus, AO, Avoi, R, et al. Improving Tuberculosis medication adherence: the potential of integrating digital technology and health belief model. Tuberc Respir Dis. (2023) 86:82–93. doi: 10.4046/trd.2022.0148
14. Alipanah, N, Jarlsberg, L, Miller, C, Linh, NN, Falzon, D, Jaramillo, E, et al. Adherence interventions and outcomes of tuberculosis treatment: a systematic review and meta-analysis of trials and observational studies. PLoS Med. (2018) 15:e1002595. doi: 10.1371/journal.pmed.1002595
15. Hafez, G, and Van, BJFM. Digital adherence technologies in tuberculosis. Lancet Glob Health. (2023) 11:e1341–2. doi: 10.1016/S2214-109X(23)00308-X
16. Chuck, C, Robinson, E, Macaraig, M, Alexander, M, and Burzynski, J. Enhancing management of tuberculosis treatment with video directly observed therapy in new York City. Int J Tuberc Lung Dis. (2016) 20:588–93. doi: 10.5588/ijtld.15.0738
17. Holzschuh, EL, Province, S, Johnson, K, Walls, C, Shemwell, C, Martin, G, et al. Use of video directly observed therapy for treatment of latent Tuberculosis infection - Johnson County, Kansas, 2015. MMWR Morb Mortal Wkly Rep. (2017) 66:387–9. doi: 10.15585/mmwr.mm6614a3
18. Garfein, RS, Liu, L, Cuevas-Mota, J, Collins, K, Muñoz, F, Catanzaro, DG, et al. Tuberculosis treatment monitoring by video directly observed therapy in 5 health districts, California, USA. Emerg Infect Dis. (2018) 24:1806–15. doi: 10.3201/eid2410.180459
19. Garfein, RS, and Doshi, RP. Synchronous and asynchronous video observed therapy (VOT) for tuberculosis treatment adherence monitoring and support. J Clin Tuberc Mycobact Dis. (2019) 17:100098. doi: 10.1016/j.jctube.2019.100098
20. Mirsaeidi, M, Farshidpour, M, Banks-Tripp, D, Hashmi, S, Kujoth, C, and Schraufnagel, D. Video directly observed therapy for treatment of tuberculosis is patient-oriented and cost-effective. Eur Respir J. (2015) 46:871–4. doi: 10.1183/09031936.00011015
21. Nguyen, TA, Pham, MT, Nguyen, TL, Nguyen, VN, Pham, DC, Nguyen, BH, et al. Video directly observed therapy to support adherence with treatment for tuberculosis in Vietnam: a prospective cohort study. Int J Infect Dis. (2017) 65:85–9. doi: 10.1016/j.ijid.2017.09.029
22. Truong, CB, Tanni, KA, and Qian, J. Video-observed therapy versus directly observed therapy in patients with Tuberculosis. Am J Prev Med. (2022) 62:450–8. doi: 10.1016/j.amepre.2021.10.013
23. Sheet, D. Toward a comprehensive cure: digital information and communication technology is helping to meet health care challenges in India. IEEE Pulse. (2016) 7:34–7. doi: 10.1109/MPUL.2016.2607140
24. Cattamanchi, A, Crowder, R, Kityamuwesi, A, Kiwanuka, N, Lamunu, M, Namale, C, et al. Digital adherence technology for tuberculosis treatment supervision: a stepped-wedge cluster-randomized trial in Uganda. PLoS Med. (2021) 18:e1003628. doi: 10.1371/journal.pmed.1003628
25. Liu, X, Thompson, J, Dong, H, Sweeney, S, Li, X, Yuan, Y, et al. Digital adherence technologies to improve tuberculosis treatment outcomes in China: a cluster-randomised superiority trial. Lancet Glob Health. (2023) 11:e693–703. doi: 10.1016/S2214-109X(23)00068-2
26. Lee, Y, Raviglione, MC, and Flahault, A. Use of digital technology to enhance tuberculosis control: scoping review. J Med Internet Res. (2020) 22:e15727. doi: 10.2196/15727
27. Ngwatu, BK, Nsengiyumva, NP, Oxlade, O, Mappin-Kasirer, B, Nguyen, NL, Jaramillo, E, et al. The impact of digital health technologies on tuberculosis treatment: a systematic review. Eur Respir J. (2018) 51:1701596. doi: 10.1183/13993003.01596-2017
28. Ewart, CK. How integrative behavioral theory can improve health promotion and disease prevention In: Handbook of clinical health psychology: Volume 3 models and perspectives in health psychology. ed. Schneiderman N. Washington, DC, US: American Psychological Association (2004). 249–89.
29. Hale, JL, Householder, BJ, and Greene, KL. The theory of reasoned action. Persuas Handb Dev Theory Pract. (2002) 2002:259–86. doi: 10.4135/9781412976046.n14
30. Bosnjak, M, Ajzen, I, and Schmidt, P. The theory of planned behavior: selected recent advances and applications. Eur J Psychol. (2020) 16:352–6. doi: 10.5964/ejop.v16i3.3107
31. Saunders, CH, Sierpe, A, Von, PC, Kennedy, AM, Leviton, LC, Bernstein, SL, et al. Practical thematic analysis: a guide for multidisciplinary health services research teams engaging in qualitative analysis. BMJ. (2023) 381:e074256. doi: 10.1136/bmj-2022-074256
32. Zurashvili, T, Chakhaia, T, Kochlamazashvili, M, Kamkamidze, G, and Butsashvili, M. A qualitative study of knowledge, attitude and practice towards TB in Georgia. Georgian Med News. (2022) 322:43–7. Available at: https://www.who.int/publications/i/item/WHO-HTM-TB-2015.21
33. Yousif, K, Ei Maki, M, Babikir, RK, and Abuaisha, H. The effect of an educational intervention on awareness of various aspects of pulmonary tuberculosis in patients with the disease. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. (2021) 27:287–92. doi: 10.26719/emhj.20.102
34. Bediang, G, Stoll, B, Elia, N, Abena, JL, and Geissbuhler, A. SMS reminders to improve adherence and cure of tuberculosis patients in Cameroon (TB-SMS Cameroon): a randomised controlled trial. BMC Public Health. (2018) 18:583. doi: 10.1186/s12889-018-5502-x
35. Abdulrahman, SA, Rampal, L, Ibrahim, F, Radhakrishnan, AP, Kadir Shahar, H, and Othman, N. Mobile phone reminders and peer counseling improve adherence and treatment outcomes of patients on ART in Malaysia: a randomized clinical trial. PLoS One. (2017) 12:e0177698. doi: 10.1371/journal.pone.0177698
36. Badawy, SM, and Kuhns, LM. Texting and mobile phone app interventions for improving adherence to preventive behavior in adolescents: a systematic review. JMIR Mhealth Uhealth. (2017) 5:e50. doi: 10.2196/mhealth.6837
37. Iribarren, SJ, Beck, SL, Pearce, PF, Chirico, C, Etchevarria, M, and Rubinstein, F. MHealth intervention development to support patients with active Tuberculosis. J Mob Technol Med. (2014) 3:16–27. doi: 10.7309/jmtm.3.2.4
38. Yzer, M. The integrative model of behavioral prediction as a tool for designing health messages. Health Commun Message Des Theory Pract. (2012) 2012:21–40.
39. Vallejo, JS. (2023). Periódico elDinero. Salario promedio general del sector formal fue de RD$18,711 en primer trimestre 2023. Available online at: https://eldinero.com.do/233821/salario-promedio-general-del-sector-formal-fue-de-rd18711-en-primer-trimestre-2023/ (Accessed December 26, 2023).
40. Haleem, A, Javaid, M, Singh, RP, and Suman, R. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sens Int. (2021) 2:100117. doi: 10.1016/j.sintl.2021.100117
41. Munro, SA, Lewin, SA, Smith, HJ, Engel, ME, Fretheim, A, and Volmink, J. Patient adherence to Tuberculosis treatment: a systematic review of qualitative research. PLoS Med. (2007) 4:e238. doi: 10.1371/journal.pmed.0040238
42. Gebremariam, RB, Wolde, M, and Beyene, A. Determinants of adherence to anti-TB treatment and associated factors among adult TB patients in Gondar city administration, northwest, Ethiopia: based on health belief model perspective. J Health Popul Nutr. (2021) 40:49. doi: 10.1186/s41043-021-00275-6
Keywords: video observed therapy, digital adherence technologies, Tuberculosis, patient monitoring, Dominican Republic
Citation: Canario-Guzmán JA, Elias-Melgen R, Mendoza ER, Arias LF, Espinal R, Báez J and Iribarren S (2025) A mixed-method study to inform the design of a video observed therapy app to monitor individuals with TB in the Dominican Republic. Front. Public Health. 13:1529687. doi: 10.3389/fpubh.2025.1529687
Edited by:
Josef Yayan, University of Witten/Herdecke, GermanyReviewed by:
Richard S. Garfein, University of California, San Diego, United StatesNeti Juniarti, Padjadjaran University, Indonesia
Copyright © 2025 Canario-Guzmán, Elias-Melgen, Mendoza, Arias, Espinal, Báez and Iribarren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Arturo Canario-Guzmán, amNhbmFyaW9AZXRpa29zLm9yZw==
†PRESENT ADDRESS: Eddys Rafael Mendoza and Luis Felipe Arias, Fundación Etikos, Inc., Calle Enrique Henriquez, Gazcue, Distrito Nacional, Dominican Republic