 Samuel Obeng Nkrumah1*
Samuel Obeng Nkrumah1* Medard Kofi Adu1
Medard Kofi Adu1 Belinda Agyapong2
Belinda Agyapong2 Raquel da Luz Dias1
Raquel da Luz Dias1 Vincent Israel Opoku Agyapong1,2
Vincent Israel Opoku Agyapong1,2- 1Department of Psychiatry, Dalhousie University, Halifax, NS, Canada
- 2Department of Psychiatry, University of Alberta, Edmonton, AB, Canada
Background: The mental well-being of physicians is increasingly recognized as vital, both for their personal health and the quality of care they provide to patients. Physicians face a variety of mental health challenges, including depression, anxiety, and burnout, which have become prevalent issues globally. These mental health concerns are like those found in the general population but are particularly significant in the demanding healthcare setting.
Objective: This review aims to explore the prevalence and correlates of depression, anxiety, and burnout among physicians and residents in training.
Methods: A comprehensive literature review was conducted, searching databases such as Medline, PubMed, Scopus, CINAHL, and PsycINFO. The review focused on studies published from 2021 to 2024 that addressed the prevalence of these mental health conditions in physicians and residents. The findings, in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, were summarized in detailed tables.
Results: Following titles and abstracts screening, 196 publications were selected for full-text review, with 92 articles ultimately included in the analysis. The results revealed significant variability in the prevalence of burnout, depression, and anxiety. Burnout rates among physicians ranged from 4.7 to 90.1% and from 18.3 to 94% among residents. Depression prevalence ranged from 4.8 to 66.5% in physicians and from 7.7 to 93% in residents. Anxiety rates were between 8 and 78.9% in physicians and 10 to 63.9% in residents. Notably, women reported higher rates of all three conditions compared to men. Key factors influencing these mental health conditions included demographics (age, gender, education, financial status, family situation, occupation), psychological conditions, social factors (stigma, family life), work organization (workload, work conditions), and COVID-19-related issues (caring for COVID-19 patients, fear of infection, working in high-risk areas, concerns about personal protective equipment (PPE), and testing positive).
Conclusion: This review indicates a high prevalence of burnout, depression, and anxiety among physicians and residents, with female participants consistently showing higher rates than males. These findings can guide policymakers and healthcare administrators in designing targeted programs and interventions to help reduce these mental health issues in these groups.
1 Introduction
In the demanding and high-stress environment of the healthcare profession, the mental well-being of physicians is increasingly recognized as a critical component of both individual health and patient care quality. Ensuring a robust and capable cadre of physicians is fundamental to the effectiveness of any nation’s healthcare infrastructure (1). The suboptimal mental health and wellness of healthcare personnel have organizational repercussions for patient safety, satisfaction, and overall experience (1). Physicians can experience a wide array of mental health conditions alongside various challenges impacting their overall wellness, including burnout. Like the broader populace, prevalent mental health issues among physicians include depression, anxiety, and burnout (2). Depression, anxiety, and burnout represent significant challenges faced by physicians worldwide (3–9), impacting not only their personal lives but also their professional performance and the broader healthcare system. As frontline providers, physicians bear the crucial duty of delivering top-tier medical care to patients amidst the intricacies of healthcare systems, rapidly evolving medical knowledge, and the emotional rigors of patient engagements. Intense work settings, substantial workloads, extended shifts, resource constraints, organizational changes, and a culture characterized by blame and apprehension have all been identified as contributing elements (10–12), increasing the susceptibility of physicians to mental health issues. Physicians and residents often avoid seeking mental health support due to stigma and concerns over their professional reputations. Many fear that acknowledging psychological issues such as burnout, anxiety, or depression might be seen as a weakness (2) and negatively impact their careers. A 2018 study by Aaronson et al. identified key barriers to mental health care access during residency, highlighting a lack of time, confidentiality concerns, and potential career consequences as major deterrents (13). Additionally, notable medical professionals have publicly discussed their own mental health struggles, further illustrating the damaging effects of stigma within the medical field (2).
Depression ranks as the primary contributor to global ill health and disability. It is characterized by persistent feelings of sadness, fatigue, hopelessness, loss of appetite, and loss of interest or pleasure in activities (14), and it is a prevalent mental health condition among physicians. Approximately 280 million people in the world have depression, and more than 700, 000 people die due to suicide every year (14). Studies consistently report higher rates of depression among physicians compared to the general population (15–17). Numerous people grappling with mental health difficulties encounter insufficient support structures and are discouraged by the social stigma attached to such issues, impeding their capacity to access the essential treatment needed to pursue fulfilling and productive lives, a circumstance in which physicians are not exempt. Mata et al. conducted a significant systematic review and meta-analysis that brought together findings from 54 distinct cross-sectional and longitudinal studies encompassing more than 17,500 resident physicians across 18 nations. Regardless of the country or specialty under investigation, similar rates of depression symptoms among physicians were observed. The combined assessment of depression caseness, indicating the proportion of physicians exhibiting clinically significant depressive symptoms, was calculated at 28.8% (with a 95% confidence interval of 25.3–32.5%) (18).
Anxiety is another common mental health challenge faced by physicians. In 2019, approximately 301 million individuals globally experienced anxiety disorders, which stood as the most prevalent among all mental health conditions, characterized by feelings of apprehension, worry, and tension (19). The pressure to make critical decisions, maintain clinical competence, and provide optimal care in high-stakes situations can contribute to heightened anxiety levels among physicians. Moreover, the rapid pace of medical advancements, coupled with the need to keep abreast of new diagnostic and treatment modalities, can exacerbate feelings of uncertainty and insecurity, further impacting physician well-being. Numerous studies have demonstrated a higher prevalence of anxiety among physicians (6, 20, 21). A cross-sectional study conducted by Gong et al., among 2,641 physicians working in public hospitals in China found that approximately 25.67% of doctors displayed signs of anxiety, while 28.13% exhibited symptoms of depression, and 19.01% experienced both anxiety and depression. These mental health challenges among the surveyed physicians were linked to self-reported declines in physical well-being, instances of workplace violence, extended work hours surpassing 60 per week, frequent night shifts occurring twice or more weekly, and a lack of consistent physical activity (22).
Freudenberger, a psychologist, introduced the notion of burnout in a paper titled “Staff Burnout,” (23) and its recognition gained traction with the introduction of the Maslach Burnout Inventory (MBI) assessment tool by Maslach and Jackson in 1981 (24). Burnout arises as an adverse workplace condition due to prolonged exposure to stress associated with one’s job (25). It is often described as a syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment (26). It is particularly prevalent among individuals who are employed in roles that involve frequent direct interaction with others (27) and is prevalent among physicians across various specialties and practice settings (28–33). The chronic stressors inherent in medical practice, such as heavy workloads, time pressures, and the emotional toll of patient care, can lead to feelings of burnout over time. Physician burnout has garnered more focus over the years (34, 35). Physicians experiencing burnout tend to make more medical errors (36, 37), are more inclined to leave their positions (38), express lower job satisfaction (39), and have implications on healthcare costs (37). Also, burnout among physicians has been associated with poorer patient perceptions of care (40), making it a significant concern for healthcare organizations and policymakers. In a cross-sectional study conducted by O’Dea et al., among 683 general practitioners (constituting 27.3% of practicing Irish general practitioners), 52.7% reported significant emotional exhaustion, 31.6% scored high on depersonalization, and 16.3% exhibited low levels of personal accomplishment. Overall, 6.6% experienced all three symptoms, meeting the criteria for burnout (41).
Despite growing recognition of the importance of addressing mental health issues among physicians, there remains a need for a comprehensive understanding of the prevalence and correlates of depression, anxiety, and burnout within this population. The primary objective of this scoping review is to map the existing literature on the prevalence and correlates of depression, anxiety, and burnout among physicians. It aims to provide insights into the scope and magnitude of mental health challenges faced by physicians and medical trainees (residents and fellows) across different specialties, practice settings, and geographic regions. Specifically, this scoping review will address the following: The prevalence of depression, anxiety, and burnout among physicians across different specialties and practice settings; Influence of associated factors, e.g., demographic characteristics (e.g., age, gender), professional factors (e.g., years of experience, work hours), social and psychological factors on the prevalence of depression, anxiety, and burnout among physicians. The review seeks to offer critical insights for healthcare policymakers, administrators, educators, and researchers. The findings can serve as a foundation for developing targeted interventions and support systems aimed at improving the mental health and well-being of physicians and residents. In turn, this not only enhances patient care but also boosts the overall efficiency and effectiveness of the healthcare system.
2 Methods
2.1 Search strategy
A literature search was conducted to look for articles that explored the prevalence and correlates of depression, anxiety, and burnout among physicians, residents, and fellows. The databases Medline, PubMed, Scopus, CINAHL, and PsycINFO were searched in the second week of April 2024, focusing on studies published from January 1, 2021, to May 1, 2024. Only articles written in English were considered. The search aimed to find studies examining the prevalence of each condition separately (e.g., just depression) and those addressing two or all three conditions together (e.g., depression, anxiety, and burnout). The search terms included: “prevalence of depression,” “prevalence of anxiety,” “prevalence of burnout,” “depression,” “burnout,” “anxiety,” “prevalence,” “physicians,” “doctors,” “medical practitioners,” and “resident physicians.” Appendix 1 provides some examples of the search strategy. Two reviewers (S.O.N and M.A) independently searched the databases and reviewed the articles. The screening process had two stages: an initial screening of titles and abstracts to assess relevance, followed by a full-text screening. Articles meeting the initial inclusion criteria advanced to the full-text screening phase. Disagreements were resolved by consulting a third reviewer (B.A). The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (42).
2.2 Inclusion and exclusion criteria
Articles were included based on the following criteria: (1) studies published between 2021 and 2024 in English, (2) a clearly defined sample of physicians, residents, and fellows, (3) clear reporting of prevalence for depression, burnout, or anxiety, and (4) a clearly stated study design, such as cross-sectional, cohort, mixed-method, transverse, or longitudinal. Studies that did not sample physicians, were reviews, protocols, or experimental studies were excluded. The study measures of interest were depression, anxiety, or burnout. Thus, studies were excluded if they did not report prevalence or did not focus on physicians or residents. Excluded populations were: (1) Medical students (2) individuals from other health-related fields (e.g., dentistry, pharmacy, nursing, allied health sciences), and (3) other healthcare professionals.
2.3 Data extraction process
Information was extracted and summarized in a table, which included the author’s name, publication year, country of study, study population, sample size, response rate, tools used to assess mental health conditions (depression, anxiety, or burnout), prevalence of these conditions, and any associated factors (Table 1).

Table 1. Prevalence and correlates of burnout among physicians and postgraduate medical trainees in studies conducted from 2021 to 2024.
3 Results
A total of 3,367 records were retrieved from the search (Figure 1). After removing 799 duplicates, 2,568 publications remained. Title and abstract screening further reduced this number to 196 publications for full-text review. Of these, 3 could not be retrieved, leaving 193 publications for review. Ultimately, 101 articles were excluded, resulting in 92 articles selected for data extraction.
Figure 1. PRISMA flow diagram illustrating the selection process for relevant studies on the prevalence and correlates of burnout, depression, and anxiety among physicians and postgraduate medical trainees.
3.1 Study characteristics
The articles reviewed included study designs such as cross-sectional, longitudinal, transverse, cohort and mixed methods. Of the 92 articles included in the review, 44 (47.8%) were published in 2021, 27 (29.3%) were published in 2022, 16 (17.4%) were published in 2023 and 5 (5.4%) were published in 2024. Among the studies, four were cohort studies (43–46), two used mixed methods (47, 48), one was transverse (49), one was longitudinal (50), and the remaining 84 were cross-sectional. The sample sizes ranged from 120 to 11,570 for residents in training and from 51 to 55,000 for physicians/doctors. Out of the 92 studies, 50 focused solely on burnout, 10 addressed only depression, and 5 examined anxiety alone. Additionally, 12 studies investigated both anxiety and depression, 3 focused on burnout and depression, and 12 covered burnout, anxiety, and depression (as shown in Figure 2). Burnout was the most frequently assessed condition 70.65% (n = 65), followed by depression 40.2% (n = 37) and anxiety 29.3% (n = 29). Response rates varied widely from 9.9 to 96.89%, with 22 studies not reporting response rates at all. Most of the studies were conducted in Asia, accounting for 42% (n = 39), followed by North America at 20% (n = 18), Europe at 18% (n = 17), South America at 11% (n = 10), and Africa at 9% (n = 8) as illustrated in Figure 3. The target population in most studies was physicians 67.4% (n = 62), followed by residents 27.2% (n = 25), with 5.4% (n = 5) targeting both physicians and residents.
Figure 2. Number of articles reporting burnout, anxiety, depression or combinations of these conditions.
Figure 3. Summary of studies by continents.
3.2 Prevalence of burnout
Sixty-five (70.7%) of the included studies addressed burnout (Table 1). Out of these, 76.9% (50 out of 65) focused solely on burnout (45–48, 50–95), 4.6% (3 studies) assessed both burnout and depression (44, 96, 97), and 18.5% (12 studies) examined burnout together with depression, and anxiety (98–109). Of the 65 studies on burnout, 26.2% (n = 17) sampled residents, 7.7% (n = 5) sampled both residents and physicians, while the remainder 66.2% (n = 43) focused on physicians. Most surveys (n = 45) used the MBI or a variation of it, and researchers presented the outcomes in different ways (Table 1). Although the majority of studies used the MBI tool, the criteria for classifying ‘overall burnout’ varied. Some studies defined burnout as having at least one of the following: high levels of emotional exhaustion, high depersonalization, or low personal accomplishment (79, 82, 84). Others required high levels in all three constructs simultaneously (71). Other tools included the Copenhagen Burnout Inventory (CBI) (51, 58, 61, 66, 72, 76, 89, 94, 96, 109), Oldenburg Burnout Inventory (OLBI) (87, 106), and the Mini-Z Burnout Assessment (62, 104). Single-study tools included the Burnout Assessment Tool (44), Burnout Measure-Short Version (48), Professional Fulfillment Index (59), Well-Being Index (55), and Professional Quality of Life Scale (46). One study used a single-item, non-proprietary validated burnout measure developed by Schmoldt and colleagues (80). Nearly all studies reported the overall prevalence of burnout, which ranged from 4.7% (44) to 94% (63). For residents, the prevalence ranged from 18.3% (71) to 94% (63), while for physicians, it ranged from 4.7% (44) to 90.1% (61). Burnout prevalence was generally higher among females compared to males, except for two studies which reported the opposite (82, 102). Most of the included studies (n = 63/65) identified factors associated with burnout among physicians and residents, while the remaining two papers reported only the prevalence of burnout (84, 107).
3.3 Prevalence of depression
A total of 37 studies reported the prevalence of depression among physicians or residents in training (Table 2). Of these, 27% (10 studies) focused solely on depression, 32.4% (12 studies) examined both depression and anxiety, 8.1% (3 studies) looked at depression and burnout, and another 32.4% (12 studies) assessed depression in combination with both burnout and anxiety. Among these studies, 32.4% (12 studies) sampled residents, 5.4% (2 studies) sampled both residents and physicians, and 62.2% (23 studies) focused exclusively on physicians. The study samples varied, as did the tools used to measure depression. The most frequently used tool was the Patient Health Questionnaire, employed in 54.1% (20 studies) of the studies (43, 96, 98, 100, 102, 104–107, 110–120). Other tools included the Depression Anxiety Stress Scale (DASS), used in 16.2% (6 studies) (101, 103, 109, 121–123), the Hospital Anxiety Depression Scale (HADS), used in 13.5% (5 studies) (99, 108, 124–126), and the Center for Epidemiological Studies Depression scale (CESD), used in 5.4% (2 studies) (3, 127). Single-study tools included the Self-Rating Depression Scale (SDS) (128), Symptom Checklist-Core Depression (SCL-CD) (44), General Health Questionnaire (GHQ) (129), and Primary Care Evaluation of Mental Disorders (PRIME-MD) (97). The overall prevalence of depression varied widely, ranging from 4.8% (44) to 66.5% (109) among physicians, and from 7.7% (111) to 93% (119) among residents in training (Table 2). Depression prevalence was generally higher among females compared to males. Most of the studies (n = 33) explored factors associated with depression, while the remaining four studies focused solely on prevalence.
Table 2. Prevalence and correlates of depression among Physicians and postgraduate medical trainees in studies conducted from 2021 to 2024.
3.4 Prevalence of anxiety
A total of 29 studies investigated the prevalence of anxiety among physicians and/or residents in training (Table 3). Among these, 17.2% (5 studies) focused exclusively on anxiety, 41.4% (12 studies) examined both anxiety and depression and another 41.4% (12 studies) assessed anxiety along with burnout and depression. Of these studies, 69% (20 studies) sampled physicians, while 31% (9 studies) focused on residents in training. The most commonly used survey tool is the Generalized Anxiety Disorder scale or its variations, utilized in 48.3% (14 studies) (49, 98, 100, 104, 106, 107, 110, 114–116, 118, 130–132), with outcomes detailed in (Table 3). Other tools included the Depression Anxiety Stress Scale (DASS), used in 20.7% (6 studies) (101, 103, 109, 121–123), and the Hospital Anxiety Depression Scale (HADS), used in 17.4% (5 studies) (99, 108, 124–126). Additionally, single-study tools included the Beck Anxiety Inventory (BAI) (133), the Self-Rating Anxiety Scale (SAS) (128), the Patient Health Questionnaire (PHQ) (102), and the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (105). The overall prevalence of anxiety ranged from 8% (131) to 78.9% (115) among physicians and from 10% (49) to 63.9% (122) among residents in training. Additionally, the prevalence of anxiety reported in the included studies showed higher levels among females. Most of the studies (n = 25) investigated factors associated with anxiety, while the remaining four studies did not provide any information on associated factors with anxiety.
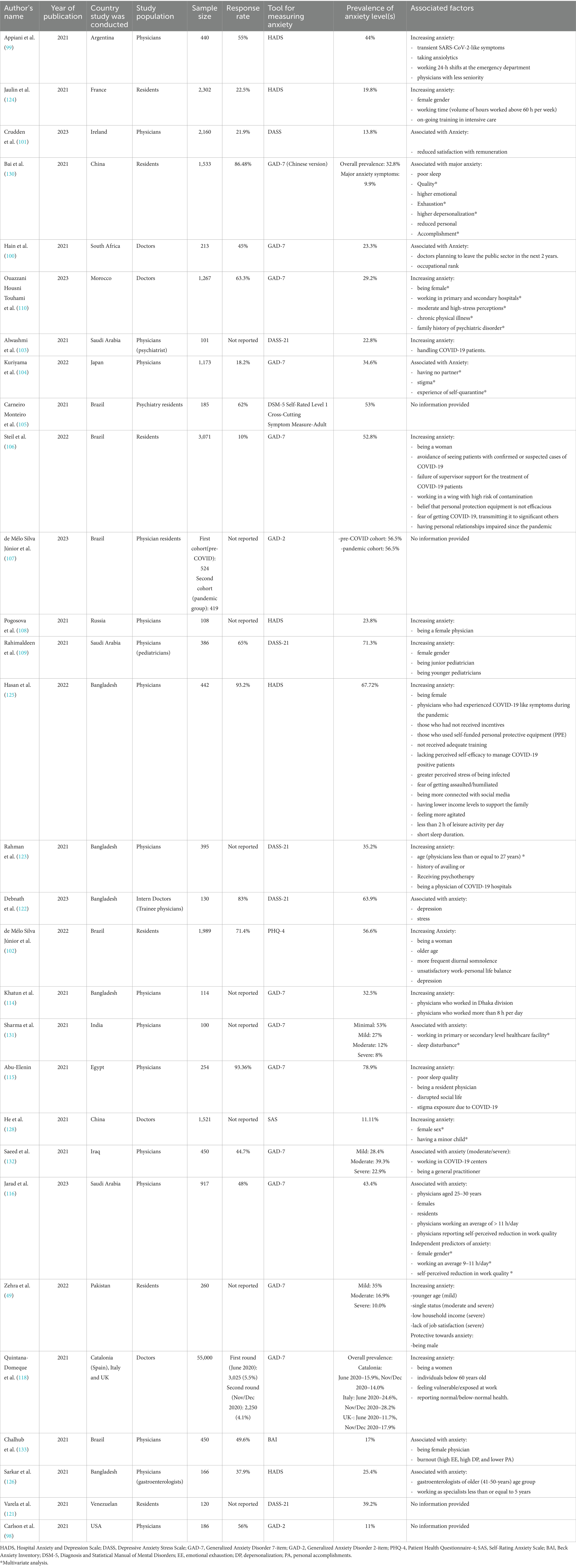
Table 3. Prevalence and correlates of anxiety among Physicians and postgraduate medical trainees in studies conducted from 2021 to 2024.
3.5 Factors associated with burnout, depression and anxiety
Factors associated with burnout, depression and anxiety were grouped into the following categories: sociodemographic, psychological, social, and organizational. Most of these factors were increasing burnout, depression and anxiety, but protective factors were also identified.
3.5.1 Factors associated with burnout
3.5.1.1 Sociodemographic factors
Age: In eight studies, younger age was associated with higher levels of burnout (51, 54, 57, 61, 78, 79, 102, 109). One study specifically found that younger residents were more likely to experience reduced personal accomplishment (PA) (77). The impact of older age on burnout was less consistent: three studies reported that older individuals experienced lower levels of burnout (46, 64, 96), while another study found higher burnout rates among older age groups (50).
Gender: Sixteen studies found that females experienced higher levels of burnout (45, 46, 48, 51, 54, 58, 61, 69, 70, 76, 79, 89, 100, 103, 108, 109). Conversely, two studies reported that males had higher burnout levels (82, 102).
Marital Status/Having Children: The findings on marital status and burnout were inconsistent. In some studies, being married was associated with increased burnout (82, 104), while in others, it was linked to decreased burnout (61). Being single or not married was associated with higher burnout levels (46). Additionally, four studies found that having children increased burnout (50, 60, 61, 82), whereas one study reported that having more children served as a protective factor against burnout (65).
Financial Situation: Factors such as inadequate compensation (94), financial problems (72), financial pressure (45), lower income (87), and educational debt exceeding $250,000 (69) were all associated with increased burnout. Conversely, financial well-being was linked to decreased burnout (61), and higher income satisfaction was identified as a protective factor against burnout (65).
Professional Experience: Three studies found increased burnout among junior physicians (44, 99, 109). Being a resident was often associated with increased burnout (51, 85, 87, 103), though one study reported decreased burnout (68). Less professional experience generally correlated with higher burnout (60, 61, 75, 81, 89).
3.5.1.2 Psychological factors
Higher burnout was associated with pre-existing psychological factors including depression (54, 56, 58, 68, 101, 102), anxiety (54, 56, 58), and stress (66, 78).
3.5.1.3 Social factors associated with burnout
Burnout was associated with several social factors, including psychological abuse (102), unfair treatment at work (55), poor work-life balance and lack of vacation or leisure (57), limited social activities (67), stigmatization for treating COVID-19 patients, and workplace violence (72). In four studies, physicians and residents reported that family life was associated with increased burnout. High burnout was linked to factors such as the quality of family relationships (105), living with a family member with comorbidities (61), limited family time for residents (93), and strained personal relationships since the COVID-19 pandemic (106).
3.5.1.4 Organizational factors
Eight studies found that working long hours (over 40 h per week) were associated with higher burnout (67, 68, 77, 78, 82, 89, 93, 97). Additionally, more frequent night shifts (48, 88), extended on-call hours (54, 88), and 24-h shifts (99) were all linked to increased burnout.
3.5.1.5 Burnout related to COVID-19 pandemic
The COVID-19 pandemic led to higher burnout due to factors including transient symptoms (99), caring for COVID-19 patients (53), fear of infection, working in high-risk contamination areas, concerns about PPE effectiveness (106), and testing positive for COVID-19 (48).
3.5.1.6 Protective factors against burnout
The authors also highlighted protective factors against burnout, including resilience and strong institutional support (56), having more children and greater income satisfaction (65), and faculty support (93). Additionally, researchers identified several other factors that help reduce burnout: professional efficacy (101), access to mental health services and insurance for personal illness or emergencies (97), staff grade or trainee status combined with higher perceived support (68), being of Black or Asian descent and being in smaller programs (69), being an International Medical Graduate (IMG) and part of a racial minority (74), and regular exercise (three times a week for 20 min) (46).
3.5.2 Factors associated with depression
3.5.2.1 Sociodemographic factors
Age: Younger age was linked to higher levels of depression in 7 studies (3, 43, 109, 114, 116, 120, 123). The relationship between older age and depression was inconsistent. One study found that older age was associated with lower depression rates in a multivariable analysis (128), while another study found the opposite, with older age linked to higher depression (126).
Gender: Thirteen studies identified being female as a factor associated with increased depression (3, 43, 44, 102, 106, 109, 114, 116, 118, 120, 124, 125, 128), while two studies reported higher depression rates in males (108, 123).
Marital Status/Having Children: In four studies, being single or unmarried was associated with higher depression (3, 43, 114, 120). Only one study found that being married was linked to increased depression (121). Additionally, a multivariate analysis indicated that having children was associated with higher depression levels (128).
Educational Level and Financial Situation: A multivariate analysis found that a higher educational level was linked to increased depression (3). Low income (125), low salary (3), and financial concerns (97) were associated with higher depression.
3.5.2.2 Professional experience
Two studies reported increased depression among junior physicians (44, 99). Three studies found that being a resident in training was linked to increased depression (113, 115, 116), and less professional experience was associated with higher depression (120).
3.5.2.3 Psychological factors
Higher depression levels were associated with pre-existing psychological factors, including anxiety (102, 122), burnout (102), stress (110, 111, 122), and poor sleep (3, 43, 115, 117, 125).
3.5.2.4 Social factors
Several social factors were linked to increased depression, including psychological abuse (102), stigmatization from exposure to COVID-19 and disrupted social life (115), and fewer than 2 h of daily leisure activities (125). In one study, having a hobby or leisure time was associated with lower depression (113).
3.5.2.5 Organizational factors
Four studies found that long working hours were associated with higher depression (43, 97, 113, 124). Additionally, working 24-h shifts in the emergency department (99) and a higher clinical workload (101) were all linked to increased depression.
3.5.2.6 Depression related to the COVID-19 pandemic
The COVID-19 pandemic led to increased depression levels due to several factors, including transient symptoms (99, 125), direct contact with COVID-19 patients (120), avoiding patients with confirmed or suspected COVID-19 cases, working in high-risk contamination areas, fear of contracting the virus and transmitting it to loved ones (106); and a lack of confidence in effectively managing COVID-19 patients (125).
3.5.3 Factors associated with anxiety
3.5.3.1 Sociodemographic factors
Age: Four studies (49, 109, 116, 123) found that younger age was linked to higher levels of anxiety. Conversely, two studies (102, 126) found that older age was associated with increased anxiety.
Gender: Eleven studies (102, 106, 108–110, 116, 118, 124, 125, 128, 133) identified being female as a factor associated with increased anxiety, while one study (49) reported that being male was a protective factor against anxiety.
Marital Status/Having Children: Two studies (49, 104) linked being single or unmarried with higher anxiety. Additionally, a multivariate analysis suggested that having children was associated with higher anxiety levels (128).
Financial Situation: Factors such as lower income levels (125), dissatisfaction with remuneration (101), and low household income (49) were all linked to higher anxiety.
3.5.3.2 Occupational and professional experience
Two studies (99, 109) reported increased anxiety among junior physicians while being a resident was associated with higher anxiety in two studies (115, 116). Increased anxiety was also linked to a lack of job satisfaction (49) and working as a specialist for 5 years or less (126).
3.5.3.3 Psychological factors
Anxiety was associated with stress (122, 125), depression (102, 122), burnout (133), and poor sleep (115, 125, 130, 131). A multivariate analysis linked moderate to high stress perceptions and a family history of psychological disorders to increased anxiety (110).
3.5.3.4 Social factors
Several social factors, such as stigmatization from COVID-19 exposure (104, 115), disrupted social life (115), less than 2 h of daily leisure activities (125), and unsatisfactory work-life balance (102), were associated with increased anxiety.
3.5.3.5 Organizational factors
Increased anxiety was found in physicians working more than 8 h per day (114) or an average of 11 h per day (116), and working 24-h shifts in the emergency department (99). Increased anxiety was reported in residents working over 60 h per week (124).
3.5.3.6 Anxiety related to the COVID-19 pandemic
The COVID-19 pandemic increased anxiety levels due to various factors, including transient symptoms (99, 125); handling of COVID-19 patients (103); avoiding contact with confirmed or suspected COVID-19 cases, working in high-risk areas, fear of contracting and transmitting the virus (106); lack of confidence in managing COVID-19 patients (125); and working in COVID-19 hospitals or centers (123, 132).
4 Discussion
The prevalence and correlates of burnout, depression, and anxiety among physicians and postgraduate medical trainees are critical areas of research that have gained significant attention in recent years. This scoping review highlights the alarming rates of mental health issues in this demographic, with burnout, depression, and anxiety being prevalent and deeply intertwined. In this review, the studies varied considerably in their methodology and findings. The most used tools by researchers were the MBI for burnout, the Patient Health Questionnaire-9 (PHQ-9) for depression, and the Generalized Anxiety Disorder-7 (GAD-7) for anxiety. These tools are recognized as the standard instruments to measure these mental health conditions. For burnout, different versions of the MBI were applied. Additionally, even in studies that utilized the same MBI version, results were reported inconsistently. For example, some studies presented burnout rates as an overall figure (55, 100, 103, 106), while others broke down the results into burnout subdimensions (71, 95, 108). Similarly, in studies measuring depression and anxiety, alongside the commonly used PHQ-9 and GAD-7, other instruments such as the Depression, Anxiety, and Stress Scales (DASS) and the Hospital Anxiety and Depression Scale (HADS) were also employed. Several sociodemographic, psychological, social, and organizational factors contribute to these mental health challenges, particularly during the ongoing COVID-19 pandemic. The review indicated a stronger focus on assessing burnout, depression, and anxiety among physicians compared to residents in training. This discrepancy was further evident in studies that included both groups, with physicians being more frequently sampled (60, 85). One potential reason for this could be the differing accessibility between physicians and residents. Physicians often remain in one facility, while residents frequently rotate through different healthcare centers, making it more challenging to reach them for surveys and assessments. The findings of this review underline the urgency of addressing these issues and providing effective interventions and support for healthcare professionals.
4.1 Prevalence of burnout, depression, and anxiety
The prevalence of burnout, depression, and anxiety among physicians and postgraduate medical trainees in the included studies ranged widely. For burnout, the review uncovered considerable variability in prevalence estimates among physicians and residents, with significant differences in how burnout was defined and measured across studies. Burnout prevalence ranged widely from 4.7 to 90.1% among physicians and from 18.3 to 94% among residents in training, with higher rates generally found in residents compared to practicing physicians. These findings seem to agree with what has been reported in a previous systematic review (0 to 80.5%) (28). Although global estimates suggest that burnout affects around 50% of both physicians (134) and residents (135), the review found that over 20 studies on physicians and 7 studies on residents reported burnout prevalence levels exceeding 50%. Burnout was most commonly measured using the MBI, although different tools and criteria for burnout classification led to variability in findings. The high prevalence of burnout among residents, in particular, aligns with previous studies that have highlighted the intensity of training, long working hours, and high emotional demands as key contributors (34). The prevalence of depression among physicians and residents also varied significantly, ranging from 4.8 to 66.5% among physicians and 7.7 to 93% among residents. The findings are consistent with prior research indicating that medical trainees and physicians are at heightened risk of depression compared to the general population (15, 17). Anxiety, similarly, had a wide prevalence range, from 8 to 78.9% among physicians, and from 10 to 63.9% among residents. This reflects the intense work pressure, substantial workloads, extended shifts, resource constraints, and organizational changes, all contributing (10–12), to increase mental health issues in physicians and medical trainees. Most of the studies reviewed reported prevalence exceeding 35% in both conditions, which is higher than the 20.5% for depression and 25.8% for anxiety found in a global systematic review and meta-analysis (136). Similarly, Mata et al. reported a 28.8% prevalence of depression among resident physicians (18), a figure lower than what was found in the majority of studies assessing depression in residents included in this review. This lower prevalence of depression reported in Mata et al.’s review compared to most studies included in our analysis may be attributed to several factors: the inclusion of more recent studies that reflect heightened mental health challenges during the COVID-19 pandemic; broader geographic coverage, especially from low- and middle-income countries with diverse healthcare contexts; and methodological variations such as differences in assessment tools, diagnostic thresholds, and sampling strategies.
4.2 Sociodemographic factors
Sociodemographic factors, such as age, gender, marital status, and financial situation, were consistently associated with higher levels of burnout, depression, and anxiety. Younger age, particularly among residents and junior physicians, was frequently linked to higher levels of these mental health issues. This is in line with research indicating that early-career professionals are more vulnerable to the psychological stressors of medical training (137). Conversely, the impact of age on burnout and depression in older physicians was inconsistent, suggesting that other factors might influence the relationship between age and mental health outcomes in healthcare professionals. Junior physicians and residents experience higher burnout, anxiety and depression rates (44, 51, 85), likely due to their lack of experience and the overwhelming demands of their roles compared to senior physicians who have acquired experience in the job. Frequent night shifts (48) and extended on-call hours (54, 88), which are more common among junior physicians and residents, further contributing to higher burnout in these groups.
Gender differences were another notable finding. Female physicians and residents generally reported higher levels of burnout, depression, and anxiety compared to their male counterparts (76, 79, 108, 109, 116, 118, 125). This disparity may be explained by gender role theory which suggests that women are more likely to express emotional and physical exhaustion, leading to higher scores on emotional exhaustion scales (138). Also, the added pressure of balancing professional responsibilities and family duties can lead to emotional exhaustion and increased burnout and psychological issues. Additionally, some researchers propose that men may generally exhibit higher resilience (139), which refers to the ability to adapt effectively in the face of stress and adversity (140). Research also suggests that resilience has an inverse relationship with burnout (141), meaning individuals with higher resilience may be better protected against burnout. However, a small number of studies reported higher burnout or depression rates in males, possibly due to cultural or institutional factors that present unique challenges for men.
The relationship between marital status, having children, and mental health outcomes was less consistent. While some studies found that being married or having children increased burnout, depression, and anxiety (60, 82, 104, 121, 128), others identified these factors as protective. The diversity of findings may be due to the complex interaction between personal, professional, and societal expectations, which may differ across cultural and institutional settings.
Financial stress was a significant factor in the mental health challenges faced by physicians and residents. Studies have shown that inadequate compensation, educational debt, and financial insecurity and pressures contribute to burnout, depression, and anxiety (45, 69, 94, 125). A study in South Africa found that lower income was associated with higher burnout levels among physicians during the COVID-19 pandemic (87). These findings highlight the importance of addressing financial well-being as part of broader efforts to improve mental health outcomes in the medical profession.
4.3 Psychological and social factors
Psychological factors such as depression, anxiety, and stress were strongly associated with burnout, depression, and anxiety. Physicians and residents with pre-existing psychological conditions are at greater risk of experiencing burnout, anxiety and depression (56, 66, 102). This is not surprising given the interrelated nature of these mental health conditions, which often co-occur among healthcare professionals. A study conducted in Morocco linked high anxiety levels to increased stress perception and a family history of psychological disorders (110). The impact of psychological distress is compounded by the high demands of medical practice, where the emotional toll of patient care and the expectation of constant performance can exacerbate existing mental health struggles.
Social factors, including poor work-life balance, limited social activities, and family life stress, were also significant contributors to burnout, depression, and anxiety. The disruption of social life and family dynamics due to long working hours, night shifts, and emotional exhaustion may lead to healthcare professionals’ mental health issues. Shift work often disrupts work-life balance and contributes to sleep deprivation, further increasing burnout risk (142). In Brazil, residents with an unsatisfactory work-life balance experience higher anxiety levels (102). Conversely, a study in Malaysia found that having hobbies or leisure activities was linked to lower depression levels among residents (113). The COVID-19 pandemic further intensified these social stressors, with many physicians and residents reporting additional challenges such as stigmatization for treating COVID-19 patients (73), family concerns, and fear of infecting loved ones (143).
4.4 Organizational factors
Work-related factors, including long working hours, high workload, night shifts, and extended on-call hours, were identified as significant predictors of burnout, depression, and anxiety (67, 68, 77, 99). These findings are consistent with a large body of literature that highlights the detrimental effects of work-related stressors on healthcare workers’ mental health (141). The strain of working over 40 h a week, frequent night shifts, and 24-h shifts exacerbates feelings of exhaustion, stress, and emotional depletion, leading to higher levels of burnout anxiety and depression.
The COVID-19 pandemic has been a key organizational factor in exacerbating these mental health issues. Healthcare workers, particularly those in high-risk areas such as emergency departments and intensive care units (99), reported increased levels of burnout, depression, and anxiety due to the overwhelming demands of treating COVID-19 patients, fear of infection, and inadequate protective measures. The pandemic’s impact on mental health highlights the urgent need for better institutional support, improved personal protective equipment (PPE), and mental health resources for frontline healthcare workers.
4.5 Protective factors
Several protective factors were identified in the studies reviewed, including resilience, and strong institutional support (56), access to mental health services (97), and faculty support (93). These findings suggest that fostering a supportive work environment, promoting mental health resources, and encouraging work-life balance can help mitigate the negative impact of stressors on physicians and residents. Additionally, personal factors such as exercising three times a week for 20 min (46), professional efficacy (101), and having a supportive family life were all identified as protective factors against burnout. These findings emphasize the importance of a multifaceted approach to addressing mental health in the medical profession.
4.6 Implications for policy and practice
The findings of this scoping review underscore the widespread and significant mental health challenges faced by physicians and postgraduate medical trainees, including burnout, depression, and anxiety. These issues are not only detrimental to the well-being of healthcare providers but also have serious implications for patient care, workforce sustainability, and healthcare system efficiency. Therefore, urgent attention and targeted interventions are required at multiple levels to mitigate the impact of these mental health conditions. Firstly, healthcare organizations must prioritize mental health and well-being in their workplace policies. This includes promoting a culture of psychological safety, providing access to mental health services, and ensuring that physicians and trainees have opportunities to engage in stress-reducing activities. Implementing institutional support systems, such as counseling services, peer support programs, and resilience training, could significantly help reduce burnout and foster a healthier work environment. Reducing work-related demands and enhancing access to resources may help residents lower their stress levels and improve their overall well-being (144).
Furthermore, providing financial support and improving compensation for healthcare professionals, especially in regions with significant income disparities, may help alleviate stressors contributing to these mental health issues. Secondly, addressing work-life balance is critical in both policy and practice. Policies that regulate working hours, reduce excessive shifts, and prevent burnout-inducing workloads should be implemented. For instance, limiting mandatory on-call hours and advocating for reasonable shift schedules, stress management, training in mindfulness could mitigate the stress and burnout identified in this review (145, 146). Additionally, providing sufficient time off and family leave would help professionals manage personal responsibilities alongside demanding work schedules. Finally, the incorporation of mental health education into medical training is essential. Training future healthcare providers to recognize the early signs of burnout, depression, and anxiety, and equipping them with coping strategies, could significantly reduce the prevalence of these conditions in the long term. Integrating mental health discussions into residency and ongoing professional development programs may help destigmatize these issues and empower healthcare providers to seek help when needed.
5 Strength and limitations
One of the key strengths of this study is its comprehensive and up-to-date examination of the prevalence of major mental health conditions, such as burnout, depression, and anxiety, which are often studied individually but not collectively. The findings offer valuable data that can assist in monitoring changes in these conditions over time. However, the study has some limitations. Firstly, while a significant number of papers were included, the search did not cover all available databases, leaving a possibility that some relevant studies were missed or excluded due to publication bias. Secondly, the research was limited to studies published between 2021 and April 2024 and written only in English, which further restricts its scope. Thirdly, different methods were used to measure the prevalence of burnout, depression, and anxiety, making it difficult to produce a unified estimate for each condition. Future studies should focus on reporting rates specific to each assessment tool rather than merging results from different scales. Fourthly, many of the studies did not mention the validity and reliability of the tools they used. Among the most used tools were the MBI for burnout, the PHQ-9 for depression, and the GAD-7 for anxiety. These tools are widely used globally, with strong evidence supporting their reliability and consistency. For instance, the GAD-7 demonstrates good test–retest reliability and strong internal consistency (147, 148). The MBI, a concise questionnaire used to evaluate burnout symptoms and their intensity, has shown strong reliability. Specifically, it has Cronbach’s alpha values of 0.90 for emotional exhaustion, 0.76 for depersonalization, and 0.76 for personal accomplishment (149). Similarly, the PHQ-9, widely used for depression screening, exhibits solid psychometric properties with good sensitivity and high internal consistency (150, 151), making it a reliable tool for assessing depression symptoms. Thus, the choice and selection of tools in the retrieved studies seem to be appropriate. Lastly, another limitation of our study is the lack of a formal assessment of bias and methodological quality among the included studies. Future updates to this review will address this gap by incorporating a meta-analysis and employing standardized tools to systematically evaluate the risk of bias and study quality. Despite these limitations, this study provides a crucial resource for future research on the prevalence of burnout, depression, and anxiety, emphasizing the need for consistent methodologies and longitudinal studies.
6 Conclusion
The high prevalence of burnout, depression, and anxiety among physicians and postgraduate medical trainees is a concerning issue that requires immediate attention. This review highlights the complex interplay of sociodemographic, psychological, social, and organizational factors contributing to mental health challenges in this group. The psychological well-being of these professionals is critical, as it directly impacts patient care and overall healthcare outcomes. Additionally, our review highlights a consistently high prevalence of burnout, anxiety, and depression across multiple high-quality studies, underscoring the need for urgent action at both policy and institutional levels. To mitigate these issues, healthcare organizations must prioritize the mental health and well-being of their staff by implementing policies that promote work-life balance, financial security, mental health resources, and institutional support. Additionally, addressing the unique challenges faced by female physicians, junior physicians, and residents is essential to creating a healthier and more sustainable medical workforce. Ultimately, improving mental health outcomes in healthcare professionals will lead to better care for patients and a more resilient healthcare system. It is essential to prioritize and implement interventions that support the psychological well-being of physicians and residents, with the goal of preventing or reducing burnout, depression, and anxiety. One promising approach is the use of evidence-based mobile text messaging technology, which offers a convenient, cost-effective, and accessible way to provide psychological support to those in need (152, 153). This review offers valuable insights to inform policymakers and healthcare administrators in designing effective strategies to mitigate burnout, depression, and anxiety among medical professionals.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
SO: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MA: Writing – review & editing. BA: Writing – review & editing. RD: Writing – review & editing. VA: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by QE II foundation, Heart & Stroke Foundation and Department of Psychiatry, Faculty of Medicine.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1537108/full#supplementary-material
References
1. Wallace, JE, Lemaire, JB, and Ghali, WA. Physician wellness: a missing quality indicator. Lancet. (2009) 374:1714–21. doi: 10.1016/S0140-6736(09)61424-0
2. Association of American Medical Colleges. (2023). Out of the shadows: physicians share their mental health struggles. Available online at: https://www.aamc.org/news/out-shadows-physicians-share-their-mental-health-struggles#:~:text=They%20suffer%20depression%2C%20anxiety%2C%20burnout,rate%20among%20nonphysicians%20was%208%25 (Accessed May 28, 2024).
3. Chen, Y, Shen, X, Feng, J, Lei, Z, Zhang, W, Song, X, et al. Prevalence and predictors of depression among emergency physicians: a national cross-sectional study. BMC Psychiatry. (2022) 22:69. doi: 10.1186/s12888-022-03687-8
4. Adam, AR, and Golu, FT. Prevalence of depression among physicians: a comprehensive meta-analysis. Rom Med J. (2021) 68:327. doi: 10.37897/RMJ.2021.3.1
5. Wurm, W, Vogel, K, Holl, A, Ebner, C, Bayer, D, Mörkl, S, et al. Depression-burnout overlap in physicians. PLoS One. (2016) 11:e0149913. doi: 10.1371/journal.pone.0149913
6. Białek, K. The prevalence and associated factors of anxiety and depression symptoms among critical care physicians. Med Stud. (2021) 37:131–9. doi: 10.5114/ms.2021.107457
7. Shanafelt, TD, Sinsky, C, Dyrbye, LN, Trockel, M, and West, CP. Burnout among physicians compared with individuals with a professional or doctoral degree in a field outside of medicine. Mayo Clin Proc. (2019) 94:549–551. doi: 10.1016/j.mayocp.2018.11.035
8. Stanetić, KD, Savić, SM, and Račić, M. The prevalence of stress and burnout syndrome in hospital doctors and family physicians. Med Pregl. (2016) 69:356–65. doi: 10.2298/mpns1612356s
9. Yilmaz, A. Burnout, job satisfaction, and anxiety-depression among family physicians: a cross-sectional study. J Family Med Prim Care. (2018) 7:952–6. doi: 10.4103/jfmpc.jfmpc_59_18
10. Lemaire, JB, and Wallace, JE. Burnout among doctors. British Medical Journal Publishing Group. BMJ. (2017). 358:j3360 doi: 10.1136/bmj.j3360
11. Wilkinson, E. UK NHS staff: stressed, exhausted, burnt out. Lancet. (2015) 385:841–2. doi: 10.1016/S0140-6736(15)60470-6
12. Harvey, SB, Modini, M, Joyce, S, Milligan-Saville, JS, Tan, L, Mykletun, A, et al. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup Environ Med. (2017) 74:301–10. doi: 10.1136/oemed-2016-104015
13. Aaronson, AL, Backes, K, Agarwal, G, Goldstein, JL, and Anzia, J. Mental health during residency training: assessing the barriers to seeking care. Acad Psychiatry. (2018) 42:469–72. doi: 10.1007/s40596-017-0881-3
14. World Health Organization (2023). Depressive disorder (depression). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression (Accessed June 3, 2024).
15. Joules, N, Williams, DM, and Thompson, AW. Depression in resident physicians: a systematic review. Open J Depression. (2014) 3:89–100. doi: 10.4236/ojd.2014.33013
16. Sen, S, Kranzler, HR, Krystal, JH, Speller, H, Chan, G, Gelernter, J, et al. A prospective cohort study investigating factors associated with depression during medical internship. Arch Gen Psychiatry. (2010) 67:557–65. doi: 10.1001/archgenpsychiatry.2010.41
17. Dyrbye, LN, Thomas, MR, and Shanafelt, TD. Systematic review of depression, anxiety, and other indicators of psychological distress among US and Canadian medical students. Acad Med. (2006) 81:354–73. doi: 10.1097/00001888-200604000-00009
18. Mata, DA, Ramos, MA, Bansal, N, Khan, R, Guille, C, Di Angelantonio, E, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. (2015) 314:2373–83. doi: 10.1001/jama.2015.15845
19. World Health Organization (2023). Anxiety disorders. Available online at: https://www.who.int/news-room/fact-sheets/detail/anxiety-disorders (Accessed June 4, 2024).
20. Elhadi, M, Khaled, A, Malek, AB, El-Azhari, AE-A, Gwea, AZ, Zaid, A, et al. Prevalence of anxiety and depressive symptoms among emergency physicians in Libya after civil war: a cross-sectional study. BMJ Open. (2020) 10:e039382. doi: 10.1136/bmjopen-2020-039382
21. Fond, G, Boulangeat, C, Messiaen, M, Duba, A, Boucekine, M, Auquier, P, et al. Anxiety and depression in young physicians: prevalence and associated factors. The MESSIAEN national study. L'Encéphale. (2022) 48:26–30. doi: 10.1016/j.encep.2021.02.005
22. Gong, Y, Han, T, Chen, W, Dib, HH, Yang, G, Zhuang, R, et al. Prevalence of anxiety and depressive symptoms and related risk factors among physicians in China: a cross-sectional study. PLoS One. (2014) 9:e103242. doi: 10.1371/journal.pone.0103242
23. Freudenberger, HJ. Staff burn-out. J Soc Issues. (1974) 30:159–65. doi: 10.1111/j.1540-4560.1974.tb00706.x
24. Maslach, C, and Jackson, SE. The measurement of experienced burnout. J Organ Behav. (1981) 2:99–113. doi: 10.1002/job.4030020205
25. World Health Organization. (2019). Burn-out an “occupational phenomenon”: international classification of diseases. Available online at: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases. (Accessed June 4, 2024).
26. Weber, J-C. Practical judgment and burn-out syndrome among physicians. Rev Med Interne. (2015) 36:548–50. doi: 10.1016/j.revmed.2015.04.008
27. Martins, LF, Laport, TJ, Menezes, V, Medeiros, PB, and Ronzani, TM. Burnout syndrome in primary health care professionals. Ciênc Saúde Coletiva. (2014) 19:4739. doi: 10.1590/1413-812320141912.03202013
28. Rotenstein, LS, Torre, M, Ramos, MA, Rosales, RC, Guille, C, Sen, S, et al. Prevalence of burnout among physicians: a systematic review. JAMA. (2018) 320:1131–50. doi: 10.1001/jama.2018.12777
29. Sanfilippo, F, Palumbo, GJ, Noto, A, Pennisi, S, Mineri, M, Vasile, F, et al. Prevalence of burnout among intensive care physicians: a systematic review. Revista Brasileira de terapia intensiva. (2020) 32:458–67. doi: 10.5935/0103-507X.20200076
30. Hiver, C, Villa, A, Bellagamba, G, and Lehucher-Michel, M-P. Burnout prevalence among European physicians: a systematic review and meta-analysis. Int Arch Occup Environ Health. (2022) 95:259–73. doi: 10.1007/s00420-021-01782-z
31. Kumar, S. Burnout and doctors: prevalence, prevention and intervention. MDPI (2016). MDPI, based in Basel, Switzerland. doi: 10.3390/healthcare4030037
32. Naji, L, Singh, B, Shah, A, Naji, F, Dennis, B, Kavanagh, O, et al. Global prevalence of burnout among postgraduate medical trainees: a systematic review and meta-regression. CMAJ Open. (2021) 9:E189–200. doi: 10.9778/cmajo.20200068
33. Boutou, A, Pitsiou, G, Sourla, E, and Kioumis, I. Burnout syndrome among emergency medicine physicians: an update on its prevalence and risk factors. Eur Rev Med Pharmacol Sci. (2019) 23:9058–65. doi: 10.26355/eurrev_201910_19308
34. Dyrbye, LN, Shanafelt, TD, Sinsky, CA, Cipriano, PF, Bhatt, J, Ommaya, A, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. NAM Perspect. (2017). doi: 10.31478/201707b
35. Thomas, LR, Ripp, JA, and West, CP. Charter on physician well-being. JAMA. (2018) 319:1541–2. doi: 10.1001/jama.2018.1331
36. Tawfik, DS, Scheid, A, Profit, J, Shanafelt, T, Trockel, M, Adair, KC, et al. Evidence relating health care provider burnout and quality of care: a systematic review and meta-analysis. Ann Intern Med. (2019) 171:555–67. doi: 10.7326/M19-1152
37. Salyers, MP, Bonfils, KA, Luther, L, Firmin, RL, White, DA, Adams, EL, et al. The relationship between professional burnout and quality and safety in healthcare: a meta-analysis. J Gen Intern Med. (2017) 32:475–82. doi: 10.1007/s11606-016-3886-9
38. Han, S, Shanafelt, TD, Sinsky, CA, Awad, KM, Dyrbye, LN, Fiscus, LC, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. (2019) 170:784–90. doi: 10.7326/M18-1422
39. Shanafelt, TD, Balch, CM, Bechamps, GJ, Russell, T, Dyrbye, L, Satele, D, et al. Burnout and career satisfaction among American surgeons. Ann Surg. (2009) 250:463–71. doi: 10.1097/SLA.0b013e3181ac4dfd
40. Chung, S, Dillon, EC, Meehan, AE, Nordgren, R, and Frosch, DL. The relationship between primary care physician burnout and patient-reported care experiences: a cross-sectional study. J Gen Intern Med. (2020) 35:2357–64. doi: 10.1007/s11606-020-05770-w
41. O’Dea, B, O’Connor, P, Lydon, S, and Murphy, AW. Prevalence of burnout among Irish general practitioners: a cross-sectional study. Ir J Med Sci (1971 -). (2017) 186:447–53. doi: 10.1007/s11845-016-1407-9
42. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372. doi: 10.1136/bmj.n71
43. Chen, L, Zhao, Z, Wang, Z, Zhou, Y, Zhou, X, Pan, H, et al. Prevalence and risk factors for depression among training physicians in China and the United States. Sci Rep. (2022) 12:8170. doi: 10.1038/s41598-022-12066-y
44. Hagqvist, E, Ekberg, K, Lidwall, U, Nyberg, A, Landstad, BJ, Wilczek, A, et al. The Swedish HealthPhys study: study description and prevalence of clinical burnout and major depression among physicians. Chronic Stress. (2022) 6:24705470221083866. doi: 10.1177/24705470221083866
45. Chan, EP, Stringer, LS, Forster, A, Meeks, WD, Fang, R, Franc-Guimond, J, et al. Burnout in Canadian urology: cohort analysis from the 2018 Canadian Urological Association census. Can Urol Assoc J. (2021) 15:S5. doi: 10.5489/cuaj.7232
46. Doolittle, BR. Association of burnout with emotional coping strategies, friendship, and institutional support among internal medicine physicians. J Clin Psychol Med Settings. (2021) 28:361–7. doi: 10.1007/s10880-020-09724-6
47. Blazin, LJ, Terao, MA, Spraker-Perlman, H, Baker, JN, McLaughlin Crabtree, V, Mandrell, BN, et al. Never enough time: mixed methods study identifies drivers of temporal demand that contribute to burnout among physicians who care for pediatric hematology-oncology patients. JCO Oncol Pract. (2021) 17:e958–71. doi: 10.1200/OP.20.00754
48. Alrawashdeh, HM, Al-Tammemi, AB, Alzawahreh, MK, Al-Tamimi, A, Elkholy, M, Al Sarireh, F, et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public Health. (2021) 21:1–18. doi: 10.1186/s12889-021-10897-4
49. Zehra, S, Qureshi, FM, Faiz, S, and Khalid, K. Magnitude and pattern of anxiety levels with gender wise predilection of coping strategies amid resident doctors of emergency department. Pakistan J Med Sci. (2022) 38:5105. doi: 10.12669/pjms.38.4.5105
50. Seda-Gombau, G, Montero-Alía, JJ, Moreno-Gabriel, E, and Torán-Monserrat, P. Impact of the COVID-19 pandemic on burnout in primary care physicians in Catalonia. Int J Environ Res Public Health. (2021) 18:9031. doi: 10.3390/ijerph18179031
51. Fiabane, E, Margheritti, S, Aiello, EN, Magnone, S, Miglioretti, M, Gabanelli, P, et al. Prevalence and determinants of Italian physicians’ burnout in the “post-COVID-19” era. Int Arch Occup Environ Health. (2023) 96:377–87. doi: 10.1007/s00420-022-01929-6
52. Matsuo, T, Takahashi, O, Kitaoka, K, Arioka, H, and Kobayashi, D. Resident burnout and work environment. Intern Med. (2021) 60:1369–76. doi: 10.2169/internalmedicine.5872-20
53. Ofei-Dodoo, S, Loo-Gross, C, and Kellerman, R. Burnout, depression, anxiety, and stress among family physicians in Kansas responding to the COVID-19 pandemic. J Am Board Family Med. (2021) 34:522–30. doi: 10.3122/jabfm.2021.03.200523
54. Al-Humadi, S, Bronson, B, Muhlrad, S, Paulus, M, Hong, H, and Cáceda, R. Depression, suicidal thoughts, and burnout among physicians during the COVID-19 pandemic: a survey-based cross-sectional study. Acad Psychiatry. (2021) 45:557–65. doi: 10.1007/s40596-021-01490-3
55. Rubin, B, Goldfarb, R, Satele, D, and Graham, L. Burnout and distress among physicians in a cardiovascular Centre of a quaternary hospital network: a cross-sectional survey. CMAJ Open. (2021) 9:E10–8. doi: 10.9778/cmajo.20200057
56. Che, L, Ma, S, Zhang, YL, and Huang, Y. Burnout among Chinese anesthesiologists after the COVID-19 pandemic peak: a national survey. Anesth Analg. (2023) 137:392–8. doi: 10.1213/ANE.0000000000006298
57. Jiménez-Labaig, P, Pacheco-Barcia, V, Cebrià, A, Gálvez, F, Obispo, B, Páez, D, et al. Identifying and preventing burnout in young oncologists, an overwhelming challenge in the COVID-19 era: a study of the Spanish Society of Medical Oncology (SEOM). ESMO Open. (2021) 6:100215. doi: 10.1016/j.esmoop.2021.100215
58. Baptista, S, Teixeira, A, Castro, L, Cunha, M, Serrão, C, Rodrigues, A, et al. Physician burnout in primary care during the COVID-19 pandemic: a cross-sectional study in Portugal. J Prim Care Community Health. (2021) 12:21501327211008437. doi: 10.1177/21501327211008437
59. Tipwong, A, Hall, NC, Snell, L, Chamnan, P, Moreno, M, and Harley, JM. Clinical teaching self-efficacy positively predicts professional fulfillment and negatively predicts burnout amongst Thai physicians: a cross-sectional survey. BMC Med Educ. (2024) 24:361. doi: 10.1186/s12909-024-05325-1
60. Hamdan, M, Haddad, BI, Alshrouf, MA, Al-Ani, A, Alisi, MS, Hammad, Y, et al. Burnout, grit and resilience among Jordanian orthopedic surgeons: a cross-sectional study. BMC Med Educ. (2023) 23:593. doi: 10.1186/s12909-023-04572-y
61. Youssef, D, Youssef, J, Abou-Abbas, L, Kawtharani, M, and Hassan, H. Prevalence and correlates of burnout among physicians in a developing country facing multi-layered crises: a cross-sectional study. Sci Rep. (2022) 12:12615. doi: 10.1038/s41598-022-16095-5
62. Nonaka, S, Makiishi, T, Nishimura, Y, Nagasaki, K, Shikino, K, Izumiya, M, et al. Prevalence of burnout among internal medicine and primary care physicians before and during the COVID-19 pandemic in Japan. Intern Med. (2022) 61:647–51. doi: 10.2169/internalmedicine.8118-21
63. Turalde, CWR, Espiritu, AI, Macinas, IDN, and Jamora, RDG. Burnout among neurology residents during the COVID-19 pandemic: a national cross-sectional study. Neurol Sci. (2022) 43:1–9. doi: 10.1007/s10072-021-05675-4
64. Singh, S, Farrelly, A, Chan, C, Nicholls, B, Nazeri-Rad, N, Bellicoso, D, et al. Prevalence and workplace drivers of burnout in cancer care physicians in Ontario, Canada. JCO Oncol Pract. (2022) 18:e60–71. doi: 10.1200/OP.21.00170
65. Wang, J, Hu, B, Peng, Z, Song, H, Cai, S, Rao, X, et al. Prevalence of burnout among intensivists in mainland China: a nationwide cross-sectional survey. Crit Care. (2021) 25:1–10. doi: 10.1186/s13054-020-03439-8
66. Nimer, A, Naser, S, Sultan, N, Alasad, RS, Rabadi, A, Abu-Jubba, M, et al. Burnout syndrome during residency training in Jordan: prevalence, risk factors, and implications. Int J Environ Res Public Health. (2021) 18:1557. doi: 10.3390/ijerph18041557
67. Celik, SU, Aslan, A, Coskun, E, Coban, BN, Haner, Z, Kart, S, et al. Prevalence and associated factors for burnout among attending general surgeons: a national cross-sectional survey. BMC Health Serv Res. (2021) 21:1–11. doi: 10.1186/s12913-020-06024-5
68. Boland, JW, Kabir, M, Spilg, EG, Webber, C, Bush, SH, Murtagh, F, et al. Over a third of palliative medicine physicians meet burnout criteria. Age. (2023) 21:31–40. doi: 10.1177/02692163231153067
69. Doe, S, Coutinho, A, Weidner, A, Cheng, Y, Sanders, K, Bazemore, AW, et al. Prevalence and predictors of burnout among resident family physicians. Fam Med. (2024) 56:148. doi: 10.22454/FamMed.2024.875388
70. Keith, J. The burnout in Canadian pathology initiative: pathologist burnout prevalence, drivers, and existing mitigation strategies. Arch Pathol Lab Med. (2023) 147:568–76. doi: 10.5858/arpa.2021-0200-OA
71. Alenezi, NK, Alyami, AH, Alrehaili, BO, Arruhaily, AA, Alenazi, NK, and Al-Dubai, SAR. Prevalence and associated factors of burnout among saudi resident doctors: a multicenter cross-sectional study. Alpha Psychiatr. (2022) 23:173. doi: 10.5152/alphapsychiatry.2022.21361
72. Kurzthaler, I, Kemmler, G, Holzner, B, and Hofer, A. Physician's burnout and the COVID-19 pandemic—a nationwide cross-sectional study in Austria. Front Psychol. (2021) 12:784131. doi: 10.3389/fpsyt.2021.784131
73. Marques-Pinto, A, Moreira, S, Costa-Lopes, R, Zózimo, N, and Vala, J. Predictors of burnout among physicians: evidence from a national study in Portugal. Front Psychol. (2021) 12:699974. doi: 10.3389/fpsyg.2021.699974
74. Yuan, JH, Huang, Y, Rosgen, BK, Donnelly, S, Lan, X, and Katz, SJ. Burnout and fatigue amongst internal medicine residents: a cross-sectional study on the impact of alternative scheduling models on resident wellness. PLoS One. (2023) 18:e0291457. doi: 10.1371/journal.pone.0291457
75. Mcloughlin, C, Abdalla, A, O’Callaghan, AK, Casey, S, and Barrett, E. The impact of COVID-19 on burnout, psychological well-being, and work satisfaction in psychiatry trainees in Ireland. Acad Psychiatry. (2022) 46:701–9. doi: 10.1007/s40596-022-01633-0
76. Werdecker, L, and Esch, T. Burnout, satisfaction and happiness among German general practitioners (GPs): a cross-sectional survey on health resources and stressors. PLoS One. (2021) 16:e0253447. doi: 10.1371/journal.pone.0253447
77. Shalaby, R, Oluwasina, F, Eboreime, E, El Gindi, H, Agyapong, B, Hrabok, M, et al. Burnout among residents: prevalence and predictors of depersonalization, emotional exhaustion and professional unfulfillment among resident doctors in Canada. Int J Environ Res Public Health. (2023) 20:3677. doi: 10.3390/ijerph20043677
78. Salihu, MO, Makanjuola, AB, Abiodun, OA, and Kuranga, AT. Predictors of burnout among resident doctors in a Nigerian teaching hospital. The South African Journal of Psychiatry: SAJP: the journal of the Society of Psychiatrists of South Africa. (2023) 29. doi: 10.4102/sajpsychiatry.v29i0.2017
79. Rashid, F, Uddin RAM, E, Mehedi HH,, Dhar, S, Bhuiyan, NH, Sattar, MA, et al. Burnout syndrome among frontline doctors of secondary and tertiary care hospitals of Bangladesh during COVID-19 pandemic. PLoS One. (2022) 17:e0277875. doi: 10.1371/journal.pone.0277875
80. Gajjar, J, Pullen, N, Li, Y, Weir, S, and Wright, JG. Impact of the COVID-19 pandemic upon self-reported physician burnout in Ontario, Canada: evidence from a repeated cross-sectional survey. BMJ Open. (2022) 12:e060138. doi: 10.1136/bmjopen-2021-060138
81. Ghazwani, EY. Prevalence and determinants of burnout among palliative care clinicians in Saudi Arabia. Front Public Health. (2022) 9:834407. doi: 10.3389/fpubh.2021.834407
82. Shahi, S, Paudel, DR, and Bhandari, TR. Burnout among resident doctors: An observational study. Ann Med Surg. (2022) 76:103437. doi: 10.1016/j.amsu.2022.103437
83. Pawłowicz-Szlarska, E, Skrzypczyk, P, Stańczyk, M, Pańczyk-Tomaszewska, M, and Nowicki, M. Burnout syndrome among pediatric nephrologists—report on its prevalence, severity, and predisposing factors. Medicina. (2022) 58:446. doi: 10.3390/medicina58030446
84. Fumis, RRL, Costa, ELV, Dal’Col, SVC, Azevedo, LCP, and Junior, LP. Burnout syndrome in intensive care physicians in time of the COVID-19: a cross-sectional study. BMJ Open. (2022) 12:e057272. doi: 10.1136/bmjopen-2021-057272
85. Ghoraishian, M, Mehrjardi, HZ, Askari, J, Abrisham, S-MJ, and Sobhan, MR. The frequency of burnout among Iranian orthopedic surgeons and residents. Arch Bone Jt Surg. (2022) 10:78. doi: 10.22038/abjs.2021.52914.2625
86. Passos, LS, Alves, VS, Rodrigues, LARL, and Saraiva, LV. Burnout syndrome in resident physicians of a Federal University. Rev Assoc Med Bras. (2022) 68:24–30. doi: 10.1590/1806-9282.20210241
87. Khan, S, Ntatamala, I, Baatjies, R, and Adams, S. Prevalence and determinants of burnout among south African doctors during the COVID-19 pandemic. S Afr J Psychiatry. (2024) 30:2225. doi: 10.4102/sajpsychiatry.v30i0.2225
88. Sobczuk, P, Gawlik-Urban, A, Sigorski, D, Kiszka, J, Osmola, M, Machulska-Ciuraj, K, et al. Prevalence and factors associated with professional burnout in polish oncologists—results of a nationwide survey. ESMO Open. (2024) 9:102230. doi: 10.1016/j.esmoop.2023.102230
89. Pius, RE, Ajuluchukwu, JN, and Roberts, AA. Prevalence and correlates of burn-out among Nigerian medical doctors during the COVID-19 pandemic: a cross-sectional study. BMJ Open. (2023) 13:e076673. doi: 10.1136/bmjopen-2023-076673
90. Oluwadiya, KS, Olasinde, AA, Adeoti, AO, Adeoye, O, Oluwadiya, IO, and Kadiri, IA. The high cost of healing and teaching: a cross-sectional survey of burnout among academic physicians in Nigeria. BMC Health Serv Res. (2023) 23:1357. doi: 10.1186/s12913-023-10366-1
91. Medina-Ortiz, O, Oses Gil, A, AlcendraGonzález, J, Diego Vivas, J, Sánchez, MP, Sánchez, LP, et al. Burnout syndrome in emergency physicians in Venezuela early in the COVID-19 pandemic. Curr Psychiatry Res Rev. (2022) 18:229–35. doi: 10.2174/2666082218666220513145349
92. Nguyen, AT, Kim, S, Keyes, M, Petereit, DG, Mourtada, F, Rossi, PJ, et al. Evaluation of burnout in physician members of the American brachytherapy society. Brachytherapy. (2022) 21:362–8. doi: 10.1016/j.brachy.2022.01.004
93. Bean, AC, Schroeder, AN, McKernan, GP, Mesoros, M, Silver, JK, Verduzco-Gutierrez, M, et al. Factors associated with burnout in physical medicine and rehabilitation residents in the United States. Am J Phys Med Rehabil. (2022) 101:674–84. doi: 10.1097/PHM.0000000000001886
94. McGarry, E, and O’Connor, L. Assessing burnout rates and contributing factors in emergency medical services clinicians. J Work Behav Health. (2024) 39:288–301. doi: 10.1080/15555240.2023.2292119
95. Kondrich, JE, Han, R, Clark, S, and Platt, SL. Burnout in pediatric emergency medicine physicians: a predictive model. Pediatr Emerg Care. (2022) 38:e1003:–e8. doi: 10.1097/PEC.0000000000002425
96. Kwan, KY, Chan, LW, Cheng, P, Leung, GK, and Lau, C. Burnout and well-being in young doctors in Hong Kong: a territory-wide cross-sectional survey. Hong Kong Med J. (2021) 27:330. doi: 10.12809/hkmj219610
97. Sharp, M, Burkart, KM, Adelman, MH, Ashton, RW, Biddison, LD, Bosslet, GT, et al. A national survey of burnout and depression among fellows training in pulmonary and critical care medicine: a special report by the association of pulmonary and critical care medicine program directors. Chest. (2021) 159:733–42. doi: 10.1016/j.chest.2020.08.2117
98. Carlson, ML, Larson, DP, O’Brien, EK, Lohse, CM, Kircher, ML, Gurgel, RK, et al. Prevalence of and associations with distress and professional burnout among otolaryngologists: part II, attending physicians. Otolaryngol Head Neck Surg. (2021) 164:1030–9. doi: 10.1177/0194599820959279
99. Appiani, FJ, Rodriguez Cairoli, F, Sarotto, L, Yaryour, C, Basile, ME, and Duarte, JM. Prevalence of stress, burnout syndrome, anxiety and depression among physicians of a teaching hospital during the COVID-19 pandemic. Arch Argent Pediatr. (2021) 119:317–24. doi: 10.5546/aap.2021.eng.317
100. Hain, S, Tomita, A, Milligan, P, and Chiliza, B. Retain rural doctors: burnout, depression and anxiety in medical doctors working in rural KwaZulu-Natal Province, South Africa. S Afr Med J. (2021) 111:1197–204. doi: 10.7196/SAMJ.2021.v111i12.15841
101. Crudden, G, Margiotta, F, and Doherty, AM. Physician burnout and symptom of anxiety and depression: burnout in consultant doctors in Ireland study (BICDIS). PLoS One. (2023) 18:e0276027. doi: 10.1371/journal.pone.0276027
102. de Mélo Silva Júnior, ML, Valença, MM, and Rocha-Filho, PAS. Individual and residency program factors related to depression, anxiety and burnout in physician residents–a Brazilian survey. BMC Psychiatry. (2022) 22:272. doi: 10.1186/s12888-022-03916-0
103. Alwashmi, AH, and Alkhamees, AA. Burnout and the psychological impact among physiatrists in Saudi Arabia during COVID-19. Int J Environ Res Public Health. (2021) 18:9621. doi: 10.3390/ijerph18189621
104. Kuriyama, A, Shikino, K, Moriya, M, Sadohara, M, Nonaka, S, Nagasaki, K, et al. Burnout, depression, anxiety, and insomnia of internists and primary care physicians during the COVID-19 pandemic in Japan: a cross-sectional survey. Asian J Psychiatr. (2022) 68:102956. doi: 10.1016/j.ajp.2021.102956
105. Carneiro Monteiro, GM, Marcon, G, Gabbard, GO, Baeza, FLC, and Hauck, S. Psychiatric symptoms, burnout and associated factors in psychiatry residents. Trends Psychiatry Psychother. (2021) 43:207–16. doi: 10.47626/2237-6089-2020-0040
106. Steil, A, Pereira Tokeshi, AB, Bernardo, LS, da Silva Neto, GP, Davi, RF, Bárbara, AFS, et al. Medical residents’ mental distress in the COVID-19 pandemic: an urgent need for mental health care. PLoS One. (2022) 17:e0266228. doi: 10.1371/journal.pone.0266228
107. de Mélo Silva Júnior, ML, Sapia, AV, Cavalcanti Neto, JM, Barbosa, NMG, Neiva, VBC, and Sauaia Filho, EN. The first wave of COVID-19 and mental distress of physician residents in Brazil: a comparison between two cohorts. Hum Resour Health. (2023) 21:10. doi: 10.1186/s12960-022-00790-5
108. Pogosova, N, Isakova, S, Sokolova, OY, Ausheva, A, Zhetisheva, R, and Arutyunov, A. Occupational burnout, psychological status and quality of life in primary care physicians working in outpatient settings. Kardiologiia. (2021) 61:69–78. doi: 10.18087/cardio.2021.6.n1538
109. Rahimaldeen, RM, Aboalshamat, KT, Almehmadi, BM, Aljubairy, BM, Aljohani, AM, Nur, KI, et al. Burnout, psychological disorders and perceived quality of care among pediatricians in the western region of Saudi Arabia. Fam Med Prim Care Rev. (2021) 23:209. doi: 10.5114/fmpcr.2021.105928
110. Ouazzani Housni Touhami, Y, Maiouak, M, Ouraghene, A, Hammani, Z, Abdi, CMF, Benhammou, I, et al. The prevalence and associated factors of depression, anxiety, and PTSD among Moroccan medical doctors in the COVID-19 pandemic: a national study. Psychol Health Med. (2023) 28:211–24. doi: 10.1080/13548506.2022.2067574
111. Pitanupong, J, Anantapong, K, and Aunjitsakul, W. Depression among psychiatrists and psychiatry trainees and its associated factors regarding work, social support, and loneliness. BMC Psychiatry. (2024) 24:97. doi: 10.1186/s12888-024-05569-7
112. Ng, APP, Chin, WY, Wan, EYF, Chen, J, and Lau, CS. Prevalence of depression and suicide ideation in Hong Kong doctors: a cross-sectional study. Sci Rep. (2021) 11:19366. doi: 10.1038/s41598-021-98668-4
113. Nair, N, Ng, CG, and Sulaiman, AH. Depressive symptoms in residents of a tertiary training hospital in Malaysia: the prevalence and associated factors. Asian J Psychiatr. (2021) 56:102548. doi: 10.1016/j.ajp.2021.102548
114. Khatun, MF, Parvin, MF, Rashid, MM-u, Alam, MS, Kamrunnahar, M, Talukder, A, et al. Mental health of physicians during COVID-19 outbreak in Bangladesh: a web-based cross-sectional survey. Front Public Health. (2021) 9:592058. doi: 10.3389/fpubh.2021.592058
115. Abu-Elenin, MM. Immediate psychological outcomes associated with COVID-19 pandemic in frontline physicians: a cross-sectional study in Egypt. BMC Psychiatry. (2021) 21:215. doi: 10.1186/s12888-021-03225-y
116. Jarad, JA, Aldohilan, FM, Ghulam, RZ, Fallatah, RZ, Alzahrani, AK, El Kheir, DYM, et al. Long-term psychological effects of the COVID-19 pandemic: anxiety and depression among physicians in a tertiary referral hospital. Saudi J Med Med Sci. (2023) 11:36–43. doi: 10.4103/sjmms.sjmms_507_22
117. Bai, S, Chang, Q, Yao, D, Zhang, Y, Wu, B, and Shan, L. The prevalence and risk factors for major depression and suicidal ideation in medical residents based on a large multi-center cross-sectional study using the propensity score-matched method. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:2279–91. doi: 10.1007/s00127-022-02351-6
118. Quintana-Domeque, C, Lee, I, Zhang, A, Proto, E, Battisti, M, and Ho, A. Anxiety and depression among medical doctors in Catalonia, Italy, and the UK during the COVID-19 pandemic. PLoS One. (2021) 16:e0259213. doi: 10.1371/journal.pone.0259213
119. Hameed, TK, Al Dubayee, MS, Masuadi, EM, Al-Anzi, FG, and Al Asmary, NA. Prevalence of depressive symptoms and excessive daytime sleepiness in a cohort of Saudi doctors under training: a cross sectional study. J Taibah Univ Med Sci. (2021) 16:695–9. doi: 10.1016/j.jtumed.2021.05.003
120. Elghazally, NM, and Abdeldaim, D. Depression among medical staff during the coronavirus disease-19 pandemic in Egypt: a comparative web-based cross-sectional study. Open Access Maced J Med Sci. (2021) 9:1578–85. doi: 10.3889/oamjms.2021.7791
121. Varela, R, Sánchez, ME, Méndez-Colmenares, A, Ahumada, A, Añez, R, and Salazar, J. Prevalence of depression, anxiety and stress in medical residents from a Venezuelan hospital. Gac Med Caracas. (2021) 129:32–8. doi: 10.47307/GMC.2021.129.1.5
122. Debnath, PR, Islam, MS, Karmakar, PK, Sarker, R, Zhai, ZW, and Potenza, MN. Mental health concerns, insomnia, and loneliness among intern doctors amidst the COVID-19 pandemic: evidence from a large tertiary care hospital in Bangladesh. Int J Ment Heal Addict. (2023) 21:1799–819. doi: 10.1007/s11469-021-00690-0
123. Rahman, A, Deeba, F, Akhter, S, Bashar, F, Nomani, D, Koot, J, et al. Mental health condition of physicians working frontline with COVID-19 patients in Bangladesh. BMC Psychiatry. (2021) 21:615. doi: 10.1186/s12888-021-03629-w
124. Jaulin, F, Nguyen, DP, Marty, F, Druette, L, Plaud, B, Duret, C, et al. Perceived stress, anxiety and depressive symptoms among anaesthesia and intensive care residents: a French national survey. Anaesth Crit Care Pain Med. (2021) 40:100830. doi: 10.1016/j.accpm.2021.100830
125. Hasan, MT, Hossain, S, Safa, F, Anjum, A, Khan, AH, Koly, KN, et al. Anxiety and depressive symptoms among physicians during the COVID-19 pandemic in Bangladesh: a cross-sectional study. Global Mental Health. (2022) 9:285–97. doi: 10.1017/gmh.2022.30
126. Sarkar, M, Saha, M, Rana, M, and Saha, S. Anxiety and depression among gastroenterologists: an online survey in Bangladesh. Gastroenterol Rev. (2021) 16:358–63. doi: 10.5114/pg.2021.111585
127. Fu, C, Wang, G, Shi, X, and Cao, F. Social support and depressive symptoms among physicians in tertiary hospitals in China: a cross-sectional study. BMC Psychiatry. (2021) 21:217. doi: 10.1186/s12888-021-03219-w
128. He, L, Wang, J, Zhang, L, Wang, F, Dong, W, and Zhao, W. Risk factors for anxiety and depressive symptoms in doctors during the coronavirus disease 2019 pandemic. Front Psychol. (2021) 12:687440. doi: 10.3389/fpsyt.2021.687440
129. Ji, J, Han, Y, Li, R, Jin, H, Yin, C, Niu, L, et al. The role of effort-reward imbalance and depressive symptoms in the relationship between long working hours and presenteeism among Chinese village doctors: a moderated mediation model. BMC Psychiatry. (2023) 23:497. doi: 10.1186/s12888-023-04986-4
130. Bai, S, Chang, Q, Yao, D, Zhang, Y, Wu, B, and Zhao, Y. Anxiety in residents in China: prevalence and risk factors in a multicenter study. Acad Med. (2021) 96:718–27. doi: 10.1097/ACM.0000000000003913
131. Sharma, V, Kumar, N, Gupta, B, and Mahajan, A. Impact of COVID-19 pandemic on orthopaedic surgeons in terms of anxiety, sleep outcomes and change in management practices: a cross-sectional study from India. J Orthop Surg. (2021) 29:23094990211001621. doi: 10.1177/23094990211001621
132. Saeed, BA, Shabila, NP, and Aziz, AJ. Stress and anxiety among physicians during the COVID-19 outbreak in the Iraqi Kurdistan region: An online survey. PLoS One. (2021) 16:e0253903. doi: 10.1371/journal.pone.0253903
133. Chalhub, RÁ, Menezes, MS, Aguiar, CVN, Santos-Lins, LS, Martins Netto, E, Brites, C, et al. Anxiety, health-related quality of life, and symptoms of burnout in frontline physicians during the COVID-19 pandemic. Braz J Infect Dis. (2021) 25:101618. doi: 10.1016/j.bjid.2021.101618
134. West, CP, Dyrbye, LN, Erwin, PJ, and Shanafelt, TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272–81. doi: 10.1016/S0140-6736(16)31279-X
135. Low, ZX, Yeo, KA, Sharma, VK, Leung, GK, McIntyre, RS, Guerrero, A, et al. Prevalence of burnout in medical and surgical residents: a meta-analysis. Int J Environ Res Public Health. (2019) 16:1479. doi: 10.3390/ijerph16091479
136. Johns, G, Samuel, V, Freemantle, L, Lewis, J, and Waddington, L. The global prevalence of depression and anxiety among doctors during the covid-19 pandemic: systematic review and meta-analysis. J Affect Disord. (2022) 298:431–41. doi: 10.1016/j.jad.2021.11.026
137. Dyrbye, LN, West, CP, Satele, D, Boone, S, Tan, L, Sloan, J, et al. Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad Med. (2014) 89:443–51. doi: 10.1097/ACM.0000000000000134
138. Eagly, AH. Sex differences in social behavior: A social-role interpretation. New York: Psychology Press (2013). doi: 10.4324/9780203781906
139. Jordan, RK, Shah, SS, Desai, H, Tripi, J, Mitchell, A, and Worth, RG. Variation of stress levels, burnout, and resilience throughout the academic year in first-year medical students. PLoS One. (2020) 15:e0240667. doi: 10.1371/journal.pone.0240667
140. Tugade, MM, and Fredrickson, BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J Pers Soc Psychol. (2004) 86:320–33. doi: 10.1037/0022-3514.86.2.320
141. Tawfik, DS, Profit, J, Morgenthaler, TI, Satele, DV, Sinsky, CA, Dyrbye, LN, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clin Proc. (2018). 93, 1571–1580. doi: 10.1016/j.mayocp.2018.05.014
142. Amanullah, S, and Ramesh Shankar, R. The impact of COVID-19 on physician burnout globally: a review. Healthcare. (2020). 8, 421. doi: 10.3390/healthcare8040421
143. Taylor, S, Landry, CA, Rachor, GS, Paluszek, MM, and Asmundson, GJ. Fear and avoidance of healthcare workers: an important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord. (2020) 75:102289. doi: 10.1016/j.janxdis.2020.102289
144. Huang, L, Caspari, JH, Sun, X, Thai, J, Li, Y, Chen, F-z, et al. Risk and protective factors for burnout among physicians from standardized residency training programs in Shanghai: a cross-sectional study. BMC Health Serv Res. (2020) 20:1–12. doi: 10.1186/s12913-020-05816-z
145. Williams, D, Tricomi, G, Gupta, J, and Janise, A. Efficacy of burnout interventions in the medical education pipeline. Acad Psychiatry. (2015) 39:47–54. doi: 10.1007/s40596-014-0197-5
146. Lawlor, SK, Low, CM, Carlson, ML, Rajasekaran, K, and Choby, G. Burnout and well-being in otolaryngology trainees: a systematic review. World J Otorhinol Head Neck Surg. (2022) 8:118–25. doi: 10.1002/wjo2.21
147. Kroenke, K, Spitzer, RL, Williams, JB, Monahan, PO, and Löwe, B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
148. Owusu, E, Shalaby, R, Eboreime, E, Nkire, N, Agyapong, B, Obuobi-Donkor, G, et al. Prevalence and predictors of generalized anxiety disorder symptoms in residents of Fort McMurray five years after the devastating wildfires. Trauma Care. (2022) 2:282–97. doi: 10.3390/traumacare2020024
149. Complete dissertation by statistics solutions. (n.d.). Maslach burnout inventory (MBI). [Available from: https://www.statisticssolutions.com/free-resources/directory-of-survey-instruments/maslach-burnout-inventory-mbi/#:~:text=Reliability%20and%20Validity&text=Cronbach%20alpha%20ratings%20of%200.90,used%20for%20test%2Dretest%20reliability (Accessed July 18, 2024).
150. Shin, C, Ko, Y-H, An, H, Yoon, H-K, and Han, C. Normative data and psychometric properties of the patient health Questionnaire-9 in a nationally representative Korean population. BMC Psychiatry. (2020) 20:1–10. doi: 10.1186/s12888-020-02613-0
151. Levis, B, Benedetti, A, and Thombs, BD. Accuracy of patient health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. (2019):l1476. doi: 10.1136/bmj.l1476
152. Agyapong, VIO, Hrabok, M, Vuong, W, Gusnowski, A, Shalaby, R, Mrklas, K, et al. Closing the psychological treatment gap during the COVID-19 pandemic with a supportive text messaging program: protocol for implementation and evaluation. JMIR Res Protocols. (2020) 9:e19292. doi: 10.2196/19292
153. Agyapong, VIO, Hrabok, M, Vuong, W, Shalaby, R, Noble, JM, Gusnowski, A, et al. Changes in stress, anxiety, and depression levels of subscribers to a daily supportive text message program (Text4Hope) during the COVID-19 pandemic: cross-sectional survey study. JMIR Mental Health. (2020) 7:e22423. doi: 10.2196/22423
Keywords: physicians, residents, prevalence, burnout, depression, anxiety
Citation: Obeng Nkrumah S, Adu MK, Agyapong B, da Luz Dias R and Agyapong VIO (2025) Prevalence and correlates of depression, anxiety, and burnout among physicians and postgraduate medical trainees: a scoping review of recent literature. Front. Public Health. 13:1537108. doi: 10.3389/fpubh.2025.1537108
Edited by:
Wulf Rössler, Charité University Medicine Berlin, GermanyReviewed by:
Víctor Hugo Fernández-Bedoya, Cesar Vallejo University, PeruAline Yacoubian, American University of Beirut Medical Center, Lebanon
Copyright © 2025 Obeng Nkrumah, Adu, Agyapong, da Luz Dias and Agyapong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samuel Obeng Nkrumah, c200MTYzOTVAZGFsLmNh