 Ângela Maria Natal de Souza1
Ângela Maria Natal de Souza1 Dalila Pinto de Souza Fernandes2
Dalila Pinto de Souza Fernandes2 Isabella Silva Castro3
Isabella Silva Castro3 Fernanda Gaspar Gróla1
Fernanda Gaspar Gróla1 Andréia Queiroz Ribeiro1*
Andréia Queiroz Ribeiro1*- 1Department of Nutrition and Health, Federal University of Viçosa, Viçosa, Minas Gerais, Brazil
- 2University Restaurant, Federal University of Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil
- 3School of Nursing, Federal University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil
Introduction: Sleep problems and frailty are associated with adverse health outcomes in older adults, including mortality, and constitute a major public health challenge.
Objective: This study investigated the association between sleep quality and duration and frailty in older adults, with emphasis on methods of evaluation.
Methods: This systematic review was guided by the Preferred Reporting Items for Systematic Reviews and MetaAnalyses (PRISMA). The Embase, Medline (Pubmed) and Cochrane libraries were searched, with no time restrictions for publications.
Results and discussion: Of the 17 studies included in this review, all published between 2009 and 2024, 13 were cross-sectional and only four were longitudinal. The Pittsburgh Sleep Quality Index and the Fried phenotype were widely used as methods to assess, respectively, sleep and frailty. Studies evaluating insomnia and frailty by the Fried phenotype all found an independent association. Poor sleep quality was independently associated with pre-frailty and frailty. Sleep onset insomnia, but not sleep maintenance insomnia, was associated with frailty. Short (5 h) and long (9 h) sleep duration were also associated with frailty. Poor sleep quality was associated with pre-frailty and frailty in older adults. The results show a wide diversity of methods for assessing both exposure (sleep quality) and outcome (frailty) and point to a need for further – especially longitudinal – research on the relationship between sleep and frailty.
1 Introduction
Sleep is crucial to health, since during this process a number of reactions take place to maintain body homeostasis (1). Sleep-related problems are highly prevalent worldwide. Insomnia is defined as a sleep disorder characterized by dissatisfaction with qualitative or quantitative sleep (2), especially, is between 12 and 20% prevalent in older adults (2) and a challenge for public health, given the risks it poses for healthy aging. Sleep problems and disorders are associated with higher risks of mortality, cardiovascular diseases, depression and other conditions (3–5).
Meanwhile, another challenge to healthy aging is frailty, a multidimensional condition that leads to a decline in the ability to resist internal and external stressors, thus increasing both harmful effects on various organs and individual vulnerability (6) and associated with higher risk of hospitalization, falls and mortality (7, 8).
There has been growing interest in investigating the association between sleep quality and duration and frailty in older adults, because both conditions are precursors of disability and morbimortality (9). However, studies of this relationship have returned inconsistent results. Some studies find an association between only short (< 5 h) sleep duration and frailty (10, 11), while others find an association with only long (> 9 h) sleep duration (12) and others observe frailty to be associated with both short and long sleep duration (11).
In addition, methods of measuring both sleep and frailty vary considerably, and this may be one of the reasons for inconsistent results. Sleep can be evaluated by using subjective and objective measures (13), and studies that combine both can provide more comprehensive information about sleep quality and duration. Objective measurement is particularly important in studies of populations of older adults, because of the cognitive decline, including difficulties with memory, common in this age group (14). Similarly, various tools are used to assess frailty, chiefly the frailty phenotype (7), frailty index (15) and frailty scale (16).
Accordingly, this systematic review investigated the association between sleep quality and duration and frailty in non-institutionalized older adults, with emphasis on the methods employed in the studies to evaluate these events.
2 Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (17) and registered in the International Prospective Register of Systematic Reviews (PROSPERO) under No. CD42023441262.
The research question, “Is there an association between sleep quality and frailty in older adults?,” applied the following PICOS strategy:
P (population): community-dwelling older adults over 60 years of age.
I (exposure): sleep quality as diagnosed by the criteria used in the original studies.
C (control): does not apply.
O (outcome): frailty as diagnosed by the criteria used in the original studies.
S (study design): observational studies.
2.1 Search strategy
Studies were retrieved by searching the Pubmed, Embase and Cochrane Library electronic databases, using a combination of MESH search terms (“sleep quality” OR “sleep hygiene”) AND (frailty OR “frail older adults” OR “frailty syndrome” OR frailties) and EMTREE terms (“sleep quality” OR “sleep quality scale” OR “sleep disorders”) AND (Frailty OR “Frailty phenotype” OR “Frailty Syndrome” OR fragility). The reference lists of the relevant original and review articles were also screened manually for related studies. The searches were performed independently by two authors (AMNS; DPSF), the last in August 2024.
2.2 Criteria for inclusion and exclusion
2.2.1 Inclusion criteria
Original observational (longitudinal and cross-sectional) studies of older adults (60 years of age or older), published in English, Spanish and Portuguese, were included, irrespective of publication date.
2.2.2 Exclusion criteria
Animal studies, studies whose abstract and full-length article could not be accessed, studies of elders living in nursing homes for older adults and studies formatted as posters, letters of comment, conference proceedings, summaries and reviews were not included. Lastly, studies of populations with specific conditions were also not included (Figure 1).

Figure 1. Flowchart of study inclusion and exclusion criteria.
2.3 Selection of studies
Two authors searched each database independently, using the specified search strategies. First, articles were selected by title and then, by reading the abstract. Duplicate articles were removed and a final selection was made by reading in full against the inclusion criteria. In the event of disagreements, a third researcher (AQR) was called on.
2.4 Data extraction
Once articles had been read and approved for inclusion in the systematic review, the following data were extracted: author, year and country of publication, study population, study type, sleep assessment methods, frailty assessment methods and main results. Data were also extracted by two authors independently and then compared.
2.5 Quality assessment
Studies included in this review were assessed for methodological quality using the Checklist proposed by the Joanna Briggs Institute (18), which is specific to each study type (cohort, case–control, cross-sectional and so on). After evaluation, the studies were classified as low (< 50%), moderate (50–70%) or high (≥ 70%) quality (19) (Supplementary Tables S1, S2).
3 Results
The 17 studies included (Figure 1) evaluated a total of 58,447 older adults, whose average age ranged from 64 to 84 years. Most studies were cross-sectional and only four were prospective cohorts (20–23). In 10 studies, the population was mostly female. Most of the studies were conducted in China (12, 23–26), followed by Mexico (10, 11, 27) and the United States (20, 28, 29) (Table 1). No studies were retrieved by the reverse search.
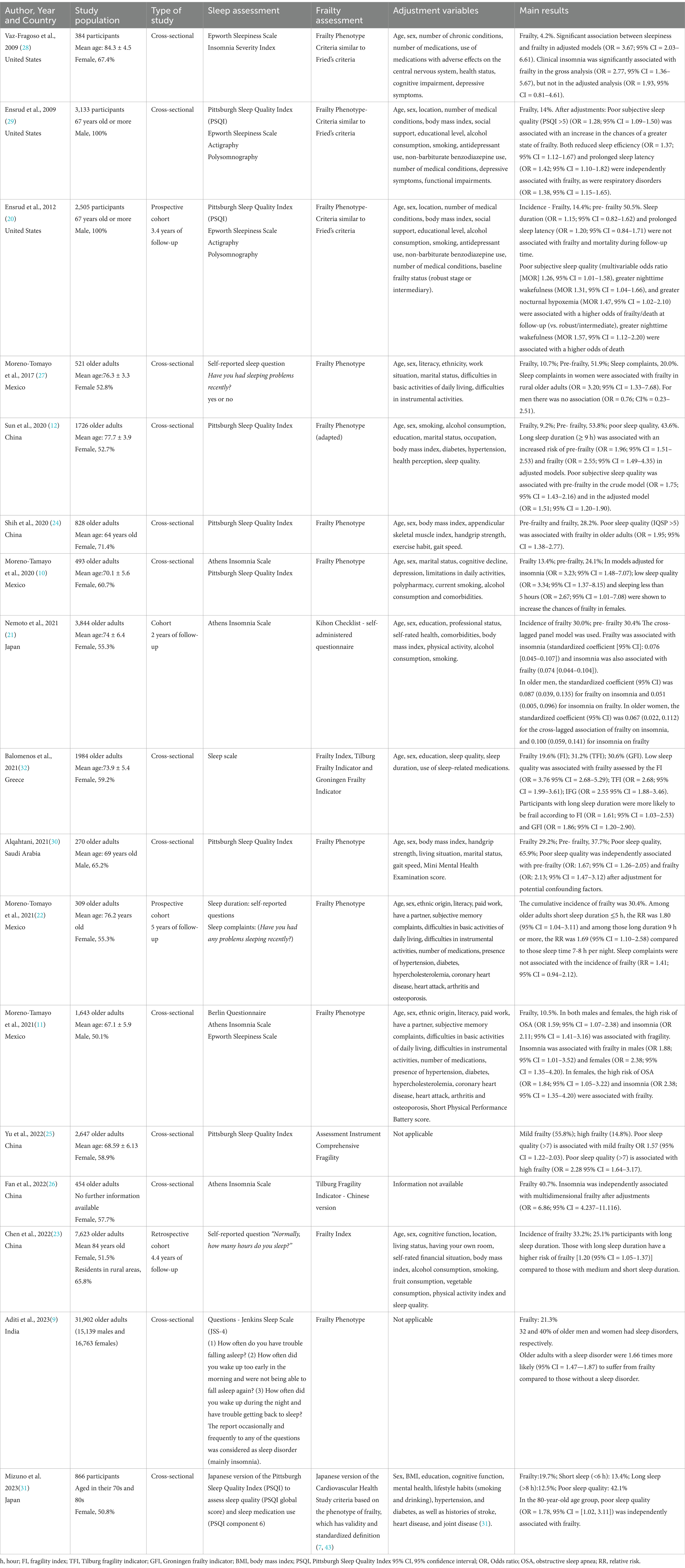
Table 1. Main characteristics of the studies included in this review.
Sleep was evaluated by different assessment measures, most of them subjective – Pittsburgh sleep quality index (n = 9), Epworth sleepiness scale (n = 4), STOP-Bang questionnaires (1), insomnia severity index (n = 1), Athens insomnia scale (n = 4), sleep scale (n = 1), Jenkins sleep scale (JSS-4) (n = 1), Berlin questionnaire (n = 1) and questions (n = 3), such as “Have you had problems with sleep recently?” “Have you had any trouble sleeping recently?” and “Normally, how many hours do you sleep?” Four studies used objective measurements: actigraphy (n = 2) and polysomnography (n = 2). Three studies used a single self-reported question to assess sleep (11, 23, 27) and only two made combined use of objective and subjective measures: the Pittsburgh sleep quality index (PSQI), Epworth sleepiness scale, actigraphy and polysomnography (20, 29) (Table 1).
Prevalence of insomnia ranged from 0.8 to 46.5% (21, 26); of poor sleep quality (IQSP >5), from 40.7 to 65.9% (30); of short sleep duration (5 h), from 11 to 25.5% (20, 23); and of long sleep duration (9 h), from 4.7 to 38.5% (10, 11). Another study, using a different cutoff point for sleep duration, revealed 13.4% prevalence of short sleep (< 6 h) and 12.5% of long sleep (> 8 h) (31). A single study estimated a prevalence of 8.9% for severe sleep apnoea, 16.6% for poor sleep efficiency and 9.2% for prolonged latency (20) at baseline (Table 1). Also, 32% of older men and 40% of women had sleep disorders (9).
Frailty was identified using mainly the Fried frailty phenotype (n = 12), frailty index (n = 2), Tilburg frailty indicator (n = 2), frail scale (1), Groningen frailty indicator (n = 1), Kihon checklist and comprehensive frailty assessment tool (n = 1). Note, however, that more than half the studies (66.7%) used the Fried frailty phenotype (9–12, 20, 22, 24, 27–31) (Table 1).
Studies using the Fried frailty phenotype found prevalence of pre-frailty ranging from 24.1% (10) to 53.8% (11), and frailty prevalence of 9.2% (11) to 41.2% (28). A single study, which evaluated frailty by other methods, pointed to prevalence of frailty of 19.6% (frailty index), 31.2% (Tilburg frailty indicator), 30.6% (Groninger frailty indicator) (30) (Table 1). The only two studies assessing incidence of pre-frailty found 35.8% (21) and 50.5% (20). Incidence of frailty was found to be 14.4% (20), 30.0% (21), 30.4% (22) and 33.2% (23).
After adjustments, one cross-sectional study carried out with 1,643 older adults Mexicans revealed that the high risk of OSA associated with frailty (OR = 1.59; 95% CI = 1.07–2.38) in the global sample and among women (OR = 1.84; 95% CI = 1.05–3.22), on the contrary, among men there was no association (OR = 1.65; 95% CI = 0.65–2.19) (11).
Excessive sleepiness was evaluated in five studies evaluated excessive sleepiness and only one cross-sectional study observed its association with frailty (OR = 3.67, 95% CI = 2.03–6.61) (28).
One cross-sectional study revealed that reduced sleep efficiency (OR = 1.37; 95% CI = 1.12–1.67) and sleep latency (OR = 1.42; 95% CI = 1.10–1.82) were associated with frailty (29). On the other hand, a longitudinal analysis of that same population found no association between sleep latency and frailty (OR = 1.20; 95% CI 0.84–1.71), while nighttime wakefulness of 90 min or longer was the only parameter of objective sleep–wake patterns associated whit frailty/dead or dead (OR = 1.31; 95% CI = 1.04–1.66 and 1.57 95% CI = 1.12–2.20 respectively) (20). Poor sleep quality (HEI > 5) was associated with pre-frailty (12, 30) and frailty (9, 24, 29–32), but only in cross-sectional studies. Sleep complaints in older adult women living in rural areas were associated with frailty in a cross-sectional analysis (OR = 3.20; 95% CI = 1.33–7.68) (27), but not in a longitudinal analysis (RR = 1.41; 95% CI = 0.94–2.12) (11).
In the 80-year-old age group, poor sleep quality was independently associated with frailty (OR = 1.78; 95% CI = [1.02, 3.11]) (31). Older adults with a sleep disorder were 0.66 times more likely (OR = 1.66; 95% CI = [1.47—1.87]) to be frail than those with no sleep disorder (p < 0.001) (9).
Insomnia was associated with frailty in both cross-sectional analyses (10, 26) and longitudinal analyses (21, 22). Short (< 5 h) sleep duration was associated with frailty in a cross-sectional analysis (OR = 2.67; 95% CI = 1.01–7.08) (10), but not in a longitudinal study (OR: 1.15; 95% CI = 0.82–1.62) (20). Long (9 h) sleep duration was associated with frailty, but only in cross-sectional analyses (12, 23, 32).
Methodological quality evaluation of 14 cross-sectional studies classified only one as being of low quality (Supplementary Table S1), while none of the four cohort studies was found to be of low quality (Supplementary Table S2).
4 Discussion
The 17 studies included in this systematic review found that insomnia, short and long sleep duration, poor efficiency, prolonged latency, obstructive sleep apnoea and poor sleep quality are associated with pre-frailty and frailty in community-dwelling older adults in several different countries.
A variety of methods for assessing exposure and outcome were identified. On the one hand, this reflects the complexity of evaluating both sleep and frailty and, on the other, it indicates the need to standardize methods for evaluating these events. Use of a single self-reported question to assess sleep may fail to consider other sleep problems.
In that light, use of a combination of objective and subjective measures of sleep can yield more robust results. Nonetheless, this review found that studies using objective measures of sleep are scarce and, in longitudinal analysis, no association was observed between the sleep parameters evaluated and frailty. This reinforces the need for further longitudinal studies using objective sleep assessment measures.
Methods used assess frailty differed in the dimensions evaluated, reflecting the multidimensionality of this condition. The frailty phenotype, for example, evaluates five criteria in the physical dimension (fatigue, involuntary weight loss, muscle weakness, gait speed and physical activity) and individuals can be classified on these criteria as robust, pre-frail and frail (7). Other approaches address non-physical (e.g., cognitive and clinical) dimensions. However, these approaches are not always easy to apply in clinical practice and epidemiological research, as they can be time-consuming and entail broader evaluation.
Of the 17 studies evaluated, 16 found independent associations between sleep problems and frailty. As regards mechanisms for this association, one hypothesis is that alterations in sleep may cause hormonal changes, such as decreases in growth hormone, insulin-like growth factor and testosterone production, with impacts including increased muscle protein breakdown, which favors the emergence of geriatric syndromes (sarcopoenia and frailty) (33). This occurs with sleep disorders that shorten the deep sleep phase (34), which also results in increased cortisol levels, culminating in impaired physical function (33).
Given that inflammation is known to be one of the pathophysiological bases of frailty (7), the association between sleep quality and frailty stages could also be explained on the basis that sleep disorders, such as insomnia and long sleep duration, favor changes in inflammation levels involving increased C-reactive protein, interleukin-6 and tumor necrosis factor (TNF-α) (32, 35, 36). In addition, long-duration sleep may result from sleep disorders such as insomnia, obstructive sleep apnoea and restless leg syndrome (37). Also, short-duration sleep can also result in lowered testosterone levels and increased oxidative stress (33), thus contributing to the development of frailty.
Among the studies that showed significant associations between sleep disorders and frailty (n = 17), almost all (n = 13) performed adjustments for confounding variables and were adjusted for sex and age.
As age progresses, hormonal changes, such as a gradual reduction of free testosterone, occur in both sexes, culminating in greater susceptibility to frailty in men and sarcopenia in women (35, 38, 39). Sarcopenia, in turn, is part of the pathophysiological basis of frailty. Also, unlike men, women with over 5 years of menopause or early menopause, and thus falling estrogen levels, are at higher risk of musculoskeletal disorders, such as sarcopenia, which can progress to frailty (40). Common changes in aging include reduced resting energy expenditure in skeletal muscle. This decline occurs faster in females, suggesting that women are more prone to developing frailty (38, 41, 42). Since the evidence above indicates important differences between the sexes, studies that stratify by sex are important in order to understand better how the association between sleep and frailty behaves in men and women.
It is known that sleep problems may occur in older adults due to the presence of comorbidities, thus increasing their susceptibility to frailty (20). This underlines the need to consider these conditions in the process of adjustment for confounding variables in statistical analysis. Ten of the studies included in this review performed adjustments for comorbidities.
However, no pattern was observed among the studies in the selection of confounding variables for adjustment, which partly undermines the degree to which their findings approximate to reality.
Furthermore, a study included in this review evaluated the bidirectional relationship between frailty and insomnia and concluded that the association between frailty and insomnia was significant, especially in men (21), which highlights the need for future studies on the causal relationship between frailty and sleep quality and duration.
Our results also point to the need for more comprehensive assessment of sleep in older adults, including screening, diagnosis and intervention measures to improve sleep quality, mainly because several aspects of sleep quality are associated with physical frailty in this age group. Most health care services for frail older adults do not currently screen for and treat sleep disorders. Given the importance of frailty in current geriatric medicine, it is important to perform a comprehensive geriatric evaluation in older patients with sleep disorders.
4.1 Strengths and limitations
The strengths of this review include the fact that it included 17 studies on the subject in different countries, most of which were of moderate to high methodological quality. The relationship between sleep issues and frailty has only recently been investigated and, considering the impact that poor sleep quality and frailty can have on the health of older adults, as well as the accelerating growth of older adult populations and the reversibility pre-frailty and frailty, it is important to investigate the association between sleep quality and frailty.
On the other hand, most of the studies were cross-sectional, posing a need for more cohort-type studies, which would afford a better understanding of the causal relationship between sleep quality and frailty conditions. Moreover, the studies reviewed may be prone to recall bias, specifically in self-reported sleep variables. Furthermore, a meta-analysis was not possible to be carried out due to the heterogeneity of the studies included in this review, for example, different ways of assessing sleep quality and frailty. Another limitation is the fact that this systematic review included only articles published in English, Spanish and Portuguese, which may limit the representation of some regions of the world, especially those areas whose studies are published in other languages.
5 Conclusion
We observed that poor sleep quality (insomnia, sleep deprivation, obstructive sleep apnea, excessive daytime sleepiness) and short/long sleep duration was associated with pre-frailty and frailty in older adults. This combination may result in other adverse health outcomes compromising the quality of life of this population.
The results of this review also suggest a need for further research on the relationship between sleep and frailty, including longitudinal studies and surveys stratified by sex.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ÂS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. DF: Data curation, Investigation, Visualization, Writing – original draft, Writing – review & editing, Methodology. IC: Visualization, Writing – original draft, Writing – review & editing. FG: Visualization, Writing – original draft, Writing – review & editing. AR: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1539849/full#supplementary-material
References
1. Deboer, TOM. Sleep homeostasis and the circadian clock: do the circadian pacemaker and the sleep homeostat influence each other's functioning? Neurobiol Sleep Circadian Rhythms. (2018) 5:68–77. doi: 10.1016/j.nbscr.2018.02.003
2. Patel, D, Steinberg, J, and Patel, P. Insomnia in the elderly: a review. J Clin Sleep Med. (2018) 14:1017–24. doi: 10.5664/jcsm.7172
3. He, M, Deng, X, Zhu, Y, Huan, L, and Niu, W. The relationship between sleep duration and all-cause mortality in older adults: an updated meta-analysis and dose-response. BMC Public Health. (2020) 20:1179. doi: 10.1186/s12889-020-09275-3
4. Choi, Y, and Choi, JW. Association of sleep disturbance with risk of cardiovascular disease and all-cause mortality in patients with new-onset type 2 diabetes: data from the Korean NHIS-HEALS. Cardiovasc Diabetol. (2020) 19:61. doi: 10.1186/s12933-020-01032-5
5. Xin-lin, L, Jiayin, W, Xinying, Z, Zhuo, M, and Wentao, Z. Relationship between night-sleep duration and risk for depression among middle-aged and older people: a dose–response. Front Physiol. (2023) 14:1085091. doi: 10.3389/fphys.2023.1085091
6. Marcucci, M, Damanti, S, Germini, F, Apostolo, J, Bobrowicz-Campos, E, Gwyther, H, et al. Interventions to prevent, delay or reverse frailty in older people: a journey towards clinical guidelines. BMC Med. (2019) 17:193. doi: 10.1186/s12916-019-1434-2
7. Fried, LP, Tangen, CM, Walston, J, Newman, AB, Hirsch, C, Gottdiener, J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:146–56. doi: 10.1093/gerona/56.3.m146
8. Ekram, ARMS, Woods, RL, Britt, C, Espinoza, S, Ernst, ME, and Ryan, J. The association between frailty and all-cause mortality in community-dwelling older individuals: an umbrella review. J Frailty Aging. (2021) 10:320–6. doi: 10.14283/jfa.2021.20
9. Aditi, SSK, Jaiswal, AK, and Verma, M. Is there a ubiquitous association between sleep disorder and frailty? Findings from LASI (2017-18). BMC Geriatr. (2023) 23:429. doi: 10.1186/s12877-023-04148-x
10. Moreno-Tamayo, K, Manrique-Espinoza, B, Ortiz-Barrios, LB, Cárdenas-Bahena, Á, Ramírez-García, E, and Sánchez-García, S. Insomnia, low sleep quality, and sleeping little are associated with frailty in Mexican women. Maturitas. (2020) 136:7–12. doi: 10.1016/j.maturitas.2020.03.005
11. Moreno-Tamayo, K, Manrique-Espinoza, B, Guerrero-Zúñiga, S, Ramírez-García, E, and Sánchez-García, S. Sex differences in the association between risk of obstructive sleep apnea, insomnia, and frailty in older adults. Nat Sci Sleep. (2021) 13:1461–72. doi: 10.2147/NSS.S320192
12. Sun, XH, Ma, T, Yao, S, Chen, ZK, Xu, WD, Jiang, XY, et al. Associations of sleep quality and sleep duration with frailty and pre-frailty in an older adults population Rugao longevity and ageing study. BMC Geriatr. (2020) 20:9. doi: 10.1186/s12877-019-1407-5
13. Neves, GSML, Macedo, P, and Gomes, MM. Sleep Disorders: update (1/2). Bras Neurol. (2017) 53:19–30.
14. Blazer, DG, Yaffe, K, and Karlawish, J. Cognitive aging: a report from the Institute of Medicine. JAMA. (2015) 313:2121–2. doi: 10.1001/jama.2015.4380
15. Rockwood, K, and Mitnitski, A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci. (2007) 62:722–7. doi: 10.1093/gerona/62.7.722
16. Morley, JE, Malmstrom, TK, and Miller, DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. (2012) 16:601–8. doi: 10.1007/s12603-012-0084-2
17. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DGPRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
18. Moola, S, Munn, Z, Tufanaru, C, Aromataris, E, Sears, K, Sfetcu, R, et al. Systematic reviews of etiology and risk In: E Aromataris and Z Munn, editors. JBI manual for evidence synthesis. Adelaide: The Joanna Briggs Institute (2020)
19. Yapa, HE, Purtell, L, Chambers, S, and Bonner, A. The relationship between chronic kidney disease, symptoms and health-related quality of life: a systematic review. J Ren Care. (2020) 46:74–8. doi: 10.1111/jorc.12303
20. Ensrud, KE, Blackwell, TL, Ancoli-Israel, S, Redline, S, Cawthon, PM, Paudel, ML, et al. Sleep disturbances and risk of frailty and mortality in older men. Sleep Med. (2012) 13:1217–25. doi: 10.1016/j.sleep.2012.04.010
21. Nemoto, Y, Sato, S, Kitabatake, Y, Nakamura, M, Takeda, N, Maruo, K, et al. Bidirecional relationship between insomnia and frailty in older adults: a 2-year longitudinal study. Arch Gerontol Geriatr. (2021). doi: 10.1016/j.archger.2021.104519
22. Moreno-Tamayo, K, Manrique-Espinoza, B, Morales-Carmona, E, and Salinas-Rodríguez, A. Sleep duration and incident frailty: the rural frailty study. BMC Geriatr. (2021) 21:368. doi: 10.1186/s12877-021-02272-0
23. Chen, S, Wang, Y, Wang, Z, Zhang, X, Deng, C, Ma, B, et al. Sleep duration and frailty risk among older adults: evidence from a retrospective, population-based cohort study. J Nutr Health Aging. (2022) 26:383–90. doi: 10.1007/s12603-022-1766-z
24. Shih, AC, Chen, LH, Tsai, CC, and Chen, JY. Correlation between sleep quality and frailty status among middle-aged and older Taiwanese people: a community-based, cross-sectional study. Int J Environ Res Public Health. (2020) 17:9457. doi: 10.3390/ijerph17249457
25. Yu, X, Shi, Z, Wang, D, Niu, Y, Xu, C, Ma, Y, et al. Prevalence and associated factors of frailty among community dwelling older adults in Northwest China: a cross-sectional study. BMJ Open. (2022) 12:e060089. doi: 10.1136/bmjopen-2021-060089
26. Fan, J, Liu, Y, Wang, Q, Zhao, H, Kong, L, and Li, J. Association of insomnia and multidimensional frailty in community-dwelling older adults: a cross-sectional survey. J Clin Nurs. (2022) 31:167–73. doi: 10.1111/jocn.15893
27. Moreno-Tamayo, K, Manrique-Espinoza, B, Rosas-Carrasco, O, Pérez-Moreno, A, and Salinas-Rodríguez, A. Sleep complaints are associated with frailty in Mexican older adults in a rural setting. Geriatr Gerontol Int. (2017) 17:2573–8. doi: 10.1111/ggi.13111
28. Vaz-Fragoso, CA, Gahbauer, EA, Van Ness, PH, and Gill, TM. Sleep-wake disturbances and frailty in community-living older persons. J Am Geriatr Soc. (2009) 57:2094–100. doi: 10.1111/j.1532-5415.2009.02522.x
29. Ensrud, KE, Blackwell, TL, Redline, S, Ancoli-Israel, S, Paudel, ML, Cawthon, PM, et al. Osteoporotic fractures in men study group. Sleep disturbances and frailty status in older community-dwelling men. J Am Geriatr Soc. (2009) 57:2085–93. doi: 10.1111/j.1532-5415.2009.02490.x
30. Alqahtani, BA. Association between physical frailty and sleep quality among Saudi older adults: a community-based, cross-sectional study. Int J Environ Res Public Health. (2021) 18:12741. doi: 10.3390/ijerph182312741
31. Mizuno, T, Godai, K, Kabayama, M, Akasaka, H, Kido, M, Isaka, M, et al. Age group differences in the association between sleep status and frailty among community-dwelling older adults: the SONIC study. Gerontol Geriatr Med. (2023) 9:23337214231205432. doi: 10.1177/23337214231205432
32. Balomenos, V, Ntanasi, E, Anastasiou, CA, Socrates, C, Velonakis, G, Karavasilis, E, et al. Association between sleep disturbances and frailty: evidence from a population-based study. J Am Med Dir Assoc. (2021) 22:551–8. doi: 10.1016/j.jamda.2020.08.012
33. Piovezan, RD, Abucham, J, Dos Santos, RV, Mello, MT, Tufik, S, and Poyares, D. The impact of sleep on age-related sarcopenia: possible connections and clinical implications. Ageing Res Rev. (2015) 23:210–20. doi: 10.1016/j.arr.2015.07.003
34. Van Cauter, E, Spiegel, K, Tasali, E, and Leproult, R. Metabolic consequences of sleep and sleep loss. Sleep Med. (2008) 9:S23–8. doi: 10.1016/S1389-9457(08)70013-3
35. Irwin, MR, Olmstead, R, and Carroll, JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. (2016) 80:40–52. doi: 10.1016/j.biopsych.2015.05.014
36. Lee, WJ, Peng, LN, Liang, CK, Chiou, ST, and Chen, LK. Long sleep duration, independent of frailty and chronic inflammation, was associated with higher mortality: a national population-based study. Geriatr Gerontol Int. (2017) 17:1481–7. doi: 10.1111/ggi.12899
37. Chen, HC, Hsu, NW, and Chou, P. The association between sleep duration and hand grip strength in community-dwelling older adults: the Yilan study, Taiwan. Sleep. (2017) 40:21. doi: 10.1093/sleep/zsx021
38. Swiecicka, A, Eendebak, RJAH, Lunt, M, O'Neill, TW, Bartfai, G, Casanueva, FF, et al. European male ageing study group reproductive hormone levels predict changes in frailty status in community-dwelling older men: European male ageing study prospective data. J Clin Endocrinol Metab. (2018) 103:701–9. doi: 10.1210/jc.2017-01172
39. Yuki, A, Ando, F, Otsuka, R, and Shimokata, H. Low free testosterone is associated with loss of appendicular muscle mass in Japanese community-dwelling women. Geriatr Gerontol Int. (2015) 15:326–33. doi: 10.1111/ggi.12278
40. Khadilkar, SS. Musculoskeletal Disorders and Menopause. J Obstet Gynaecol India. (2019) 69:99–103. doi: 10.1007/s13224-019-01213-7
41. Geisler, C, Braun, W, Pourhassan, M, Schweitzer, L, Glüer, CC, Bosy-Westphal, A, et al. Gender-specific associations in age-related changes in resting energy expenditure (REE) and MRI measured body composition in healthy Caucasians. J Gerontol A Biol Sci Med Sci. (2016) 71:941–6. doi: 10.1093/gerona/glv211
42. Park, C, and Ko, FC. The science of frailty: sex differences. Clin Geriatr Med. (2021) 37:625–38. doi: 10.1016/j.cger.2021.05.008
Keywords: older adults, frailty, sleep quality, sleep complaints, aging, systematic review
Citation: Souza ÂMNd, Fernandes DPdS, Castro IS, Gróla FG and Ribeiro AQ (2025) Sleep quality and duration and frailty in older adults: a systematic review. Front. Public Health. 13:1539849. doi: 10.3389/fpubh.2025.1539849
Edited by:
Di Wu, Guangzhou Center for Disease Control and Prevention, ChinaReviewed by:
Selene Guerrero Zúñiga, National Institute of Respiratory Diseases-Mexico (INER), MexicoSandra Öberg, Jönköping University, Sweden
Copyright © 2025 Souza, Fernandes, Castro, Gróla and Ribeiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andréia Queiroz Ribeiro, YW5kcmVpYS5yaWJlaXJvQHVmdi5icg==