 Catarina Simões
Catarina Simões Inês Fronteira
Inês Fronteira Ana Rita Pedro
Ana Rita Pedro- 1NOVA National School of Public Health, Public Health Research Centre, Universidade NOVA de Lisboa, Lisbon, Portugal
- 2NOVA National School of Public Health, Public Health Research Centre, Comprehensive Health Research Center, CHRC, REAL, CCAL, NOVA University Lisbon, Lisbon, Portugal
- 3Global Health and Tropical Medicine, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa, Lisbon, Portugal
Introduction: Burnout among physicians is a worldwide concern issue, impacting individual well-being and healthcare efficiency and jeopardizing the achievement of Universal Health Coverage. Using the Portuguese National Health Service scenario, we aimed at identifying the factors that contribute to burnout of physicians and interventions that can be helpful in its prevention.
Methods: We used a Delphi panel technique with three rounds of participation with 16 specialists, including physicians, psychologists, academics and hospital administrators.
Results: Organizational variables such system strain, staff overload, and unfavourable working circumstances were pointed as the main contributing factors of burnout. Consensus was reached that courses of action, such as resource allocation, legislative changes, and promotion of a healthier workplace environment can help prevent physician burnout. Non-organizational tactics such as workplace amenities and health literacy initiatives were also considered relevant. Identified knowledge gaps comprised long-term effects of burnout, leadership influence, and environmental repercussions.
Discussion: The study concludes that addressing organizational factors and implementing targeted interventions are crucial for improving physician well-being and aiding healthcare efficiency in Portugal but also in similar contexts.
Introduction
Burnout is a pressing worldwide issue that became even more evident with the COVID-19 pandemic (1, 2). A systematic review looking at the effects of the COVID-19 pandemic on the health of healthcare workers revealed a prevalence of 46% of burnout, and demonstrated an increasing trend manifesting in a series of physical, emotional, cognitive, and behavioral symptoms (3).
Physicians seem to be particularly affected (4). In 2021, a study conducted in the United States of America (USA) revealed that 62.8% of physicians experienced burnout (versus 38.2% in 2020) (1). The demanding nature of the medical work has raised concerns about the mental health and well-being of physicians (5–7). A study in Lebanon revealed that around 70% of physicians had work-related burnout (8). Other studies revealed that levels of burnout varied across subspecialities with emergency doctors and general practitioners being among the most affected (2, 9, 10). Portugal, a 10 million inhabitants southern Europe country, with a National Health Service (NHS) health system is no exception to this scenario. A study among 9,176 physicians revealed that 66% had high levels of emotional exhaustion, 33% depersonalization and 39% decreased personal accomplishment (11).
Burnout is defined in the ICD-11 as a syndrome resulting from chronic workplace stress that has not been successfully managed. It is characterized by emotional exhaustion (feelings of energy depletion), depersonalization (increased mental distance from one’s job, or feelings of negativism or cynicism related to one’s job), and a reduced sense of personal accomplishment (12).
Recent systematic reviews and meta-analyses have significantly advanced our understanding of the complex factors underpinning burnout. They have emphasized the interconnected relationships among burnout, depression, and anxiety, highlighting the multifactorial etiology of the syndrome, while showing that unfavourable work environments are closely linked to the development of burnout symptoms (13, 14). In support of these conclusions, empirical study conducted in Brazil during the COVID-19 pandemic identified key organizational pressures and shown a significant prevalence of burnout among medical staff in public hospital networks (15). Together, these studies show that a combination of environmental, organizational, and individual variables can lead to burnout.
Burnout syndrome not only lowers the quality of life of the individual, and leads to poor mental health but also has broader implications for the healthcare system, potentially jeopardizing patient care and overall system efficiency (10, 16–19). For instance, in 2019, the attributable cost of physician burnout in the United States was 4.6 billion USD (20). Burnout has been linked to a decrease in patient safety, which has resulted in assistance errors, poor outcomes, patient dissatisfaction, and an increase in patient and family complaints (18). Additionally, burnout can lead to a deterioration of teamwork climate, safety, and job satisfaction, all of which have an adverse effect on patient safety (18, 21, 22). Furthermore, burnout has been linked to a higher risk of infections related to healthcare and a decline in the standard of patient care (18, 23). Therefore, tackling burnout among health workers, particularly physicians, is paramount to improve patient safety and the overall system efficiency.
The need to tackle burnout in physicians and improving their physical and mental health and well-being has been recognized (24, 25). Although there is a developing body of knowledge about contributing factors to the syndrome and the best health management strategies to address it, this knowledge is not yet precisely adapted to the particular difficulties faced by doctors at sub-regional and local level. This study aims to address this gap using a Delphi study. By identifying and consensualising these points, we seek to provide practical insights, suggested by specialists that can contribute to physician well-being and enhance the overall sustainability of the healthcare system.
Materials and methods
Consensus methods aim to reach broad agreement on a controversial issue by having experts propose solutions to a defined problem based on their experience, within a structured framework (26). The Delphi method is a qualitative approach used to systematically gather key insights from a group of experts by collecting, clarifying, and sharing their experiences through a series of questionnaires. This technique relies on four core features: participant anonymity, structured interaction, controlled feedback, and statistical aggregation of group responses (27, 28).
A Delphi panel was conducted between April and May 2024, with the aim to identify factors contributing to burnout and the most effective strategies to prevent and mitigate this syndrome in Portuguese NHS physicians. Portugal is a South European country that has one of the largest ratio of physician per 1,000 inhabitants and one of the lowest of nurses per 1,000 inhabitants (ratio of nurses to doctors of 1.3) which indicates a health system largely dependent of the first (29). Nevertheless, the country faces a shortage of physicians.
The methodological criteria were all established (Figure 1) before the technique was implemented, ensuring the rigorous design necessary for obtaining reliable and reproducible results.
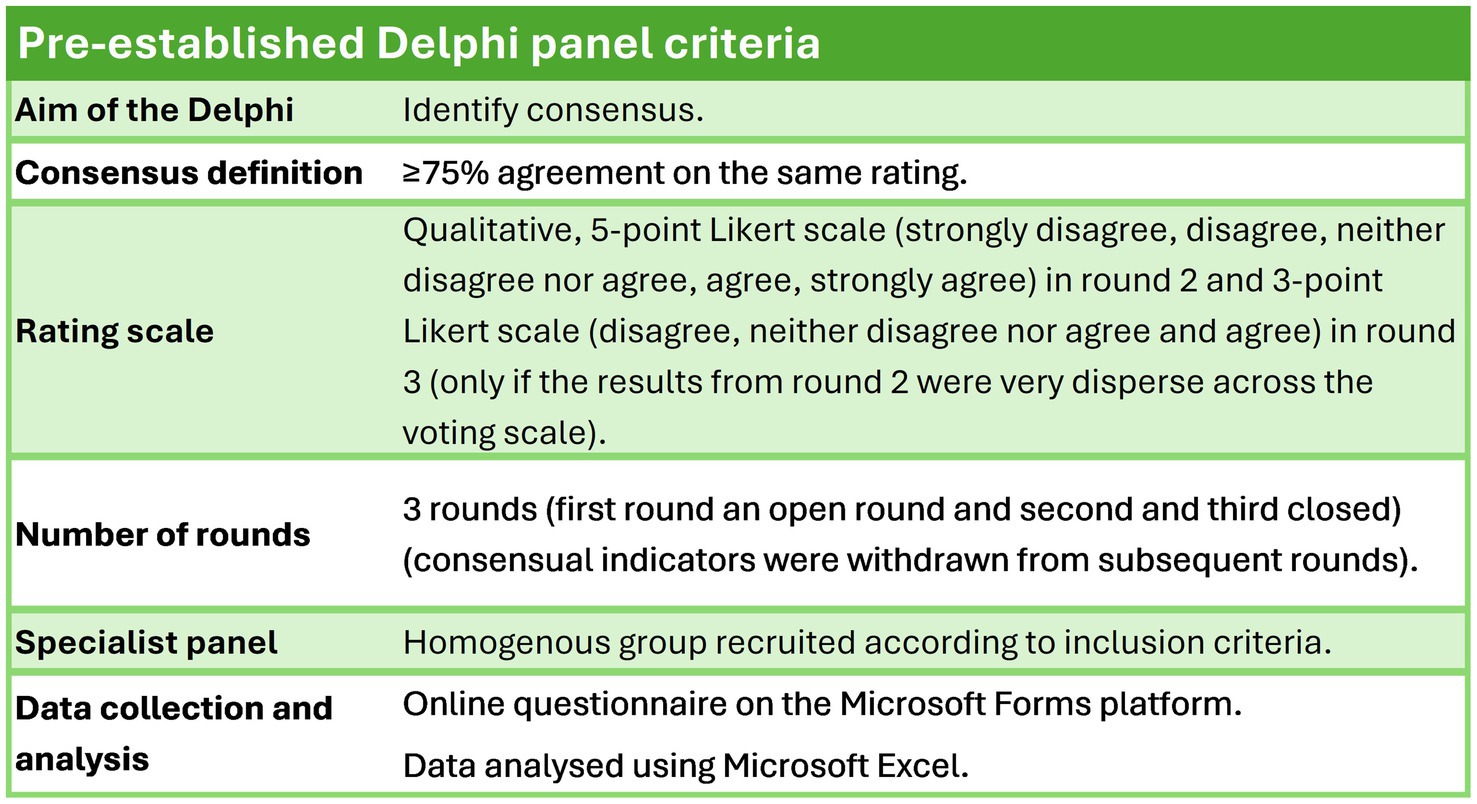
Figure 1. Pre-established methodological criteria for the Delphi panel.
There were three rounds of questionnaires, based on other healthcare Delphi models and according to the available time. The specialists were invited to participate if they met at least one of the following criteria: have a published article about burnout syndrome in the last 5 years, have at least 10 years of experience as academic in the mental health field or be an hospital administrator.
Invites were sent to 50 Portuguese experts, and 18 of them accepted an invitation via e-mail to respond. Sixteen experts (8 woman and 8 men) completed the 3 rounds of the Delphi panel, their professional backgrounds varied from physicians (6) (3 general practice; 1 public health; 1 occupational health; and 1 psychiatry), psychologists (6), academics (1 occupational health professor) to hospital administrators (3).
As the Delphi technique highly depends on the participation of external experts, one of the study’s greatest concerns was the insufficient number of recruited experts or their dropout during successive rounds. To mitigate this situation, some strategies were implemented: use of an online platform, available anytime and anywhere; adoption of a fully anonymous and confidential methodology; have a maximum of 3 rounds; in round 3, the previous results were presented alongside the indicators for reclassification, encouraging an immediate response; each expert was provided with an individual password to access the questionnaires, enabling the identification of missing responses and allowing for timely reminders.
The decision to invite 50 experts was based on the understanding that response rates in Delphi studies tend to be low, as participation requires a sustained commitment across multiple rounds (30, 31). Prior literature indicates that Delphi panels commonly range from 8 to 20 participants (32). While larger panels can enhance stability by reducing the influence of individual experts, excessively large groups may introduce logistical challenges (33). Given these considerations, we aimed to secure a final panel within this recommended range. Anticipating that not all invited experts would accept, we extended invitations accordingly. The final sample of 16 experts falls within the range suggested in the literature, ensuring a diverse set of perspectives while maintaining methodological rigor within the Portuguese healthcare context.
All the questions were of an obligatory nature so the respondents could not go forward with survey without answering the previous questions first. While answering the forms, the experts could change their answers, however after submission it was impossible to do so.
The first round of the Delphi consisted of three open-ended questions, tackling the contributing factors (“From your point of view, what do you think are the main factors—at an individual, organizational and/or system level—that contribute to burnout among physicians in the Portuguese NHS?), promising tactics/interventions to prevent and mitigate burnout (“What specific health management interventions, inside or outside Portugal, do you consider to be promising in preventing and mitigating burnout among physicians in the Portuguese NHS?), and knowledge gaps (“From your professional point of view, what specific areas or aspects related to physicians’ well-being, burnout or interventions in the area of mental health promotion are still little explored or not well understood?”).
The answers given by the experts that responded to the questionnaire were rounded up, and the bullet points present in them were put as possible answers in the second round of the panel, with the goal of the experts rating them using a 5-point Likert scale (strongly disagree, disagree, neither disagree nor agree, agree, strongly agree).
A consensus was deemed achieved when agreement reached or surpassed 75% for one of the voting options on each indicator. The consensus rate was calculated by dividing the number of respondents who agree on a particular indicator by the total number of respondents who provided answers for that indicator. The result was then multiplied by 100 to convert it into a percentage.
Considering the diverging distribution of responses in the second round – meaning that even with a lower consensus threshold than the one applied (≥75%) agreement would not be possible – it was decided to group the extremes. Specifically, the “strongly disagree” and “disagree” votes were combined, as were the “agree” and “strongly agree” votes. This approach aimed to facilitate the identification of areas of consensus while acknowledging that it may result in some loss of nuance. When consensus was achieved, the indicator was withdrawn from the next rounds.
The statements that did not reach consensus in the second round were sent for a third and final round. For each of the questions, the experts could consult a graph detailing the distribution of votes (percentagewise) on each answer that did not reach the predefined level of agreement in a single voting option. In this final round, the experts were asked to rate the topics based on a 3-point Likert scale (disagree, neither disagree nor agree and agree).
Results
Participation and dropout rates
The response rate was 89% since the only existing drop out, between the first and second round, was circa 11%. The final round was answered by 16 specialists.
Factors that contribute to physician burnout
The main factors that contribute to burnout can be differentiated in individual (if related to the physician) and organizational or system level (if not intrinsic to physician). Out of the 42 factors identified in the answers to the first round, only 3 were strictly related with the physician, namely the difficulty in work life balance, family and financial problems and a predisposition to mental health disorders (genetic or somatic) or undiagnosed mental illness. Of these factors only the difficulty in reconciling professional and personal life reached consensus, with a 75% consensus rate.
Of the 39 organizational or system level factors, only 15 achieved consensus (75% or more level of agreement), making the consensus rate for this type of factors 38%. Among these were high demand, work overload, lack of organizational support and poor management, poor working conditions and remuneration, lack of professional recognition, absence of supporting and reporting mechanisms, non-existence of initiatives to promote professional well-being and the turnover of healthcare professionals. All but one (turnover of healthcare professionals) of the statements reached consensus in the second round.
The factors not intrinsically linked to the physician far outweighed those that were (93% of the statements in the first round). The same pattern was observed in the 16 statements that reached consensus (94% were organizational or system level).
Details on the distribution of the level of agreement/disagreement are presented in Figure 2.
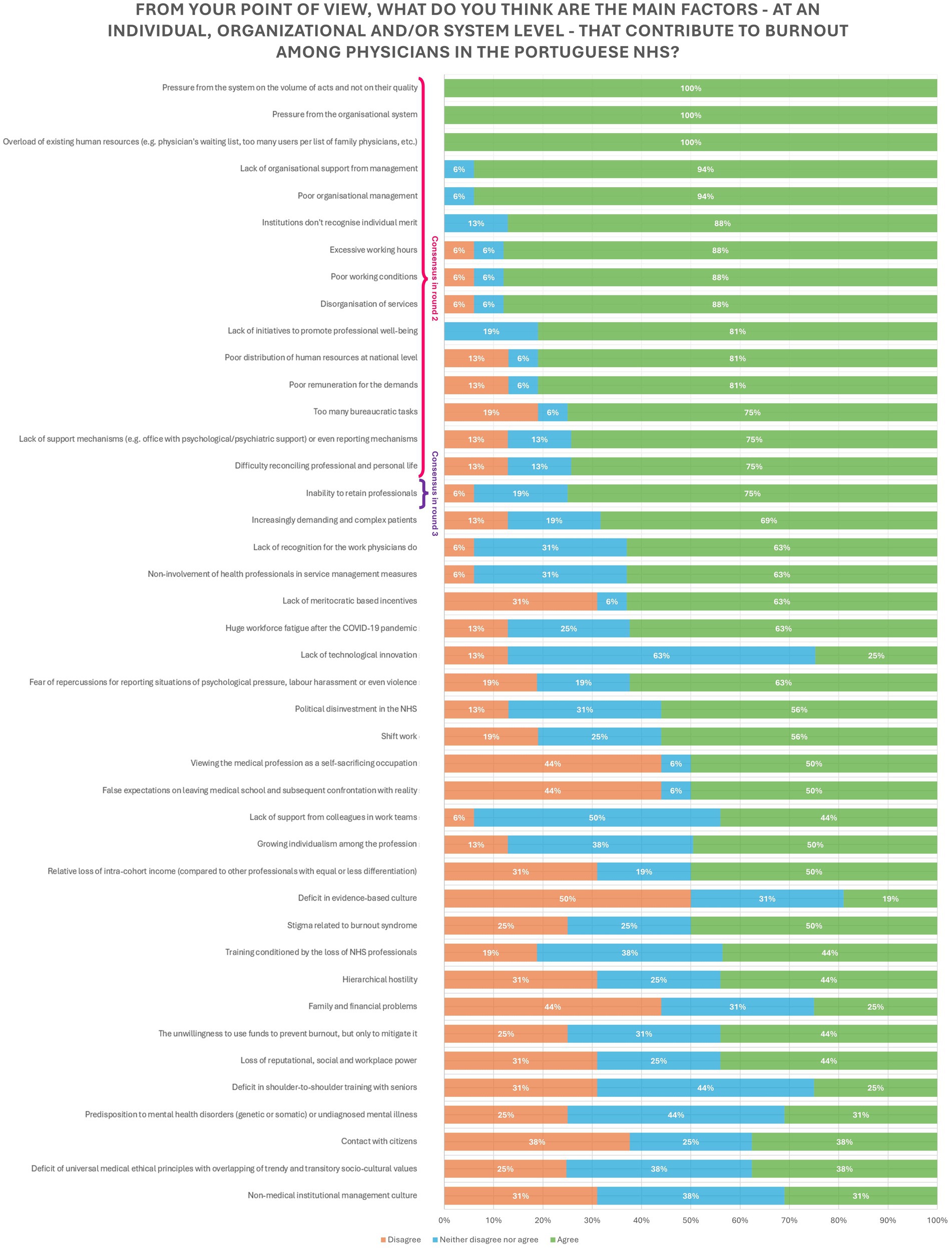
Figure 2. Factors that contribute to burnout among physicians in the Portuguese NHS.
Interventions to prevent and mitigate burnout in physicians
The interventions to prevent and mitigate burnout can be differentiated according to their focus on management or not. Out of the 36 statements collected from the answers given in the first round, 25 were meant for institutional management, while 11 of them were not.
Of the 25 organizational based interventions, only 14 reached consensuses (consensus rate = 56%). They focused mainly on changing the current policy, increasing the resources allocated to NHS, implementing of report and support mechanisms, improving working conditions (i.e., infrastructure, salaries and distribution of work) and promoting a better work culture by implementing healthier work values and fostering inter-personal relationships between coworkers.
Of the other 11 interventions that did not focus on management, only 7 gained consensuses (consensus rate = 64%). They focused mainly on the creation of supporting services, like gyms and nurseries within the work facilities, implementing a literacy project focused on the theme of burnout aimed at physicians and the managers, as well as increasing the population’s health literacy skills. Promotion and implementation of occupational health measures and of monitoring culture for burnout but also other mental health outcomes (e.g., stress) as well as the implementation of mindfulness and coaching programs were interventions that also achieved consensus.
All the statements that reached consensus did so in the second round.
The interventions targeting the management of the institutions more than doubled those not management related, making up to 69% of the total statements given. The same pattern was observed in the statements that reached consensus (21 in total), where 67% of the statements represented interventions for the organizations. Details on the distribution of the level of agreement/disagreement are presented in Figure 3.
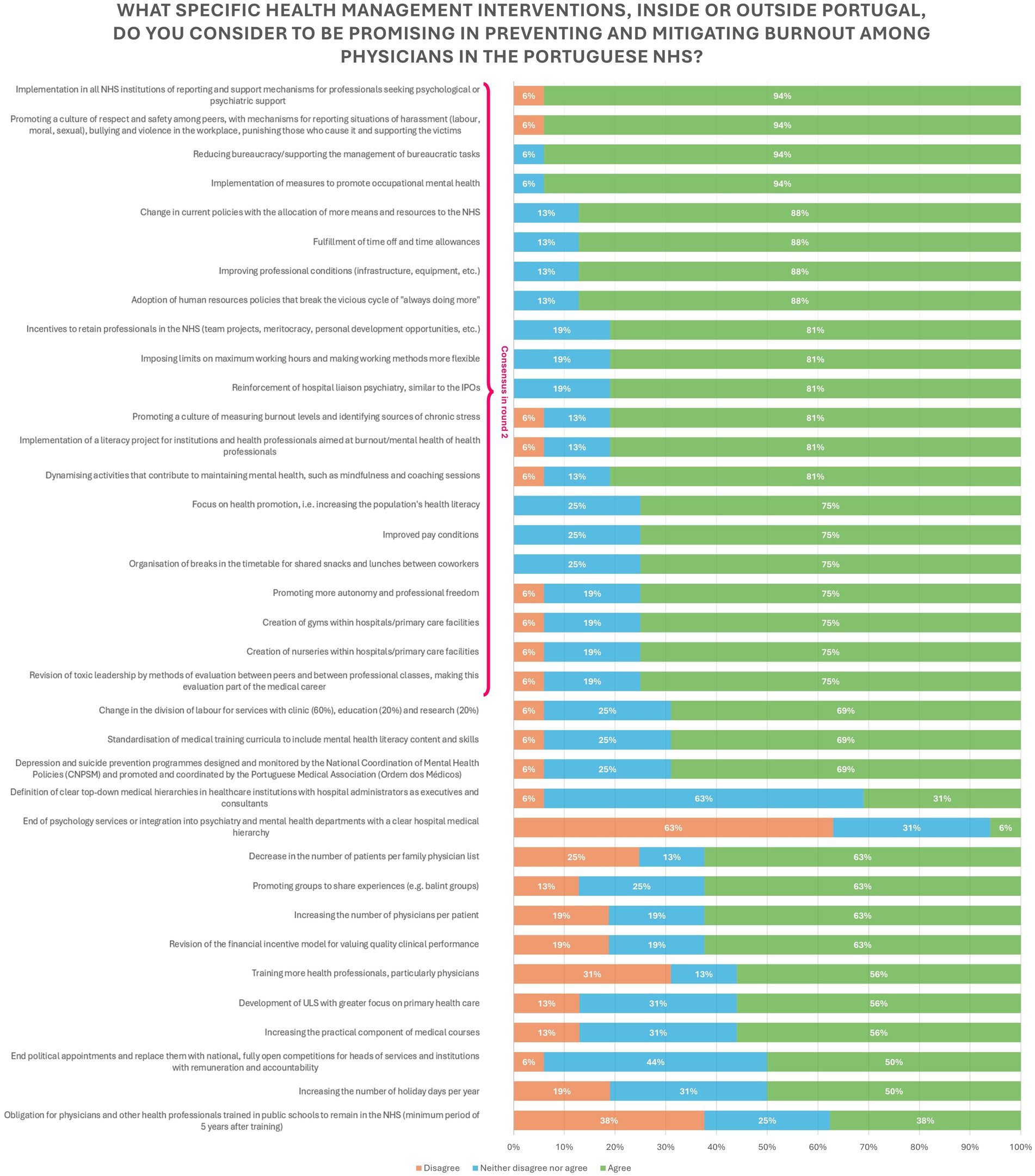
Figure 3. Health management interventions to prevent and mitigate burnout among physicians in the Portuguese NHS.
Knowledge gaps
The knowledge gaps can be classified in physician knowledge gaps and context/environment gaps. Out of the 17 statements collected from the answers given in the first round, 7 of them were strictly related to the physician, while the other 10 were not. All of these 10 reached consensuses, with the higher scores belonging to how work environments can affect clinical outcomes, the influence of leadership on burnout, the long-term effects on healthcare provided by burned out professionals and the diagnosis and monitoring of occupational stress.
Of the 7 knowledge gaps that focused on the individual, 6 gained consensuses (consensus rate = 86%). They focused mainly on connecting burnout with other factors, such as hours spent in the emergency department, for example, or the relationship between burnout and previous experiences of emotional burden. However, the higher percentage of consensus was achieved on the lack of studies addressing mental health issues throughout the various stages of the medical career, on the specificity of the individual responses to adversity and episodes of mental illness and the consequences for the physicians, their families and their patients.
All the statements that reached consensus did so in the second round except for three (individual responses to adversity and episodes of mental illness, relationship between peer and supervision support and burnout, and the relationship between burnout and experiences with previous emotional burden).
The knowledge gaps related with the environment/context outweighed those linked to the physicians, making up 59% of the statements given in the first round. The same pattern was observed in the statements that reached consensus (16 in total), where 63% of the statements were not directly linked with the physicians.
Details on the distribution of the level of agreement/disagreement are presented in Figure 4.
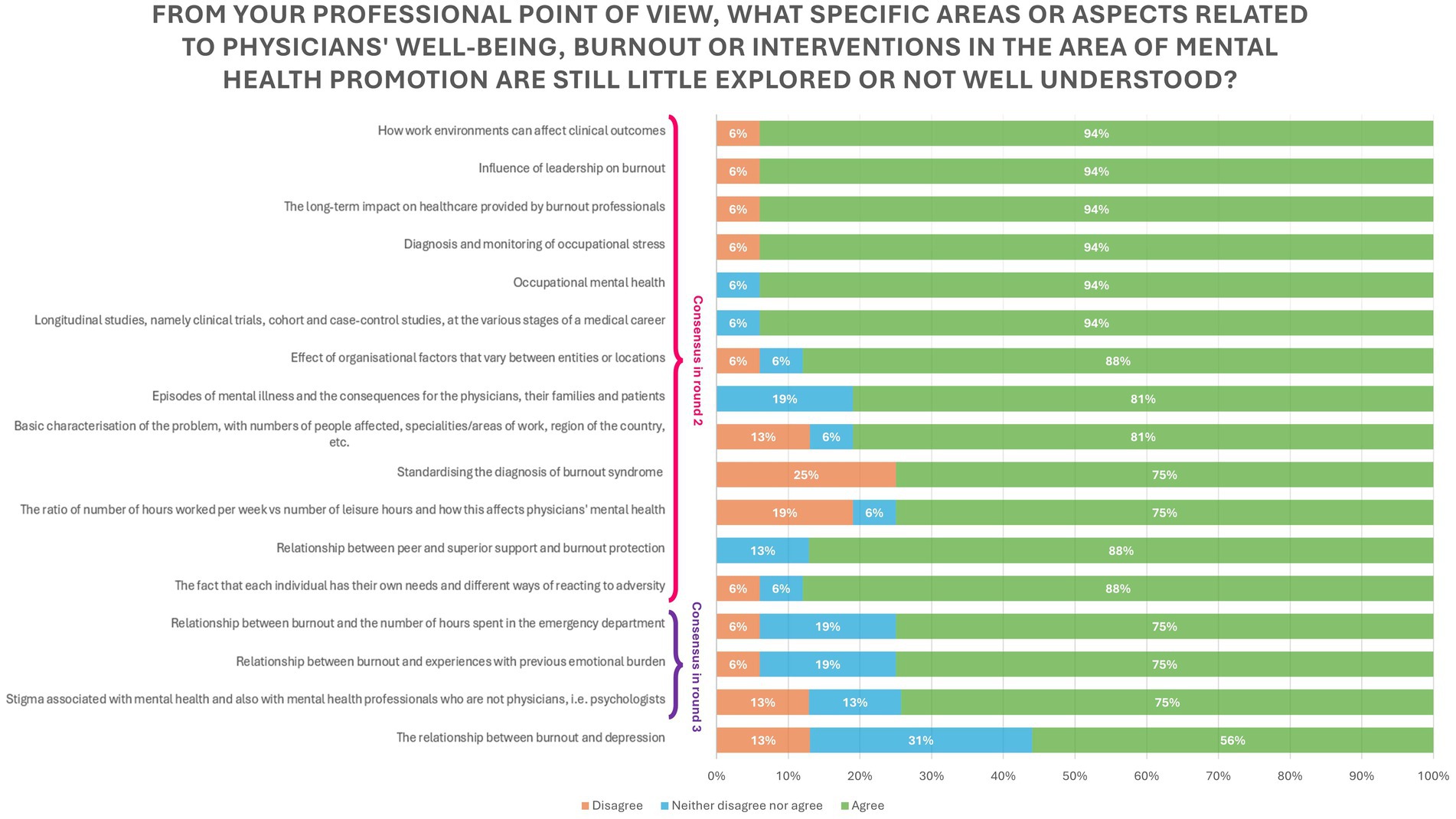
Figure 4. Knowledge gaps in physician’s well-being, burnout or in interventions in the area of mental health.
Discussion
The pervasive issue of physician burnout has garnered increasing attention in recent years, with a growing body of evidence highlighting the critical role that organizational factors play in exacerbating this problem (34). This study, using a Delphi approach, aimed to identify key factors contributing to physician burnout and interventions to prevent the syndrome and mitigate its impact within the Portuguese NHS. The results of this study emphasize the increasingly clear role of organizational factors in contributing to physician burnout. The consensus reached on factors such as system pressure, work overload, poor working conditions, and lack of organizational support indicates that these systemic issues are more significant contributors to burnout than individual factors, emphasizing the impact of workplace environment on burnout.
Individual factors, such as work-life balance, reached consensus in this panel but were significantly outnumbered by organizational factors. This suggests that while individual interventions are important, they are insufficient on their own and must be part of a broader strategy to addresses system related issues. This hypothesis falls in line with emerging evidence that suggests personal resilience tools must be supported by robust organizational strategies to maximize their effectiveness and help prevent burnout (35, 36).
Most interventions that achieved consensus were also organization focused. These included policy changes, increased resource allocation, better working conditions, and fostering a healthier work environment which indicates a strong recognition among experts that improving the organizational environment is essential for mitigating burnout. The effectiveness of such interventions has been supported by prior research, which suggests that systemic changes can lead to significant improvements in employee well-being and job satisfaction (37, 38).
Interventions such as implementing workplace supporting facilities like gyms and nurseries, promoting burnout literacy, and enhancing occupational health also achieved consensus. While not directly related to management, they address important aspects of work-life balance and personal health, further supporting the need for a holistic approach to burnout prevention, as previous literature has also called for (39, 40).
Despite the increasing understanding of physician burnout, there remains a significant gap in knowledge, highlighting the need for further research to fully grasp its complexities and develop effective interventions (41). With the goal of being a starting point for much needed future research in the area, one of the questions of the Delphi panel focused on the knowledge gaps related to physicians’ well-being, burnout or interventions if the area of mental health promotion. The experts identified several knowledge gaps, particularly in understanding the long-term effects of burnout, the influence of leadership on burnout, and the relationship between work environments and clinical outcomes. These answers emphasized the need for comprehensive studies that explore these aspects in greater depth and that can present evidence-based interventions to prevent burnout and support burned out physicians. Future studies should evaluate the effectiveness of targeted interventions and preventive strategies, providing research-supported solutions to improve healthcare system sustainability.
Although the recommendations derived from this study seek to address physician burnout broadly, there are differences in their viability within the existing Portuguese NHS. Certain suggestions, including expanding access to mental health care and encouraging work-life balance, are in line with NHS policies and programs already in place. Others, including more funding for physician well-being initiatives or structural modifications to task allocation, can call for more resources and changes to existing policies. To evaluate how well these suggestions can be implemented in the present healthcare system, more study and policy debates are required.
While the Delphi panel questions focused on understanding burnout at a Portuguese NHS level, some findings may be relevant to other countries with similar public health systems. The Portuguese NHS shares key characteristics to other public health systems around the world, sharing both strengths and challenges (42). Like many national health systems, the Portuguese NHS seeks to ensure that all citizens, regardless of income, have access to basic medical services (42, 43). However, it has the same problems as publicly funded healthcare around the world, such as high demand, a lack of resources, and a staffing deficit. Long waiting times, ineffective administration, and employee burnout are common problems that are similar across public healthcare in other countries (44, 45). Nevertheless, while the results provide valuable insights for other publicly funded healthcare systems facing similar structural challenges, generalizations should be made cautiously, considering that country-specific factors may influence the applicability of these findings.
This study has some limitations. The reliance on the opinion of experts through a Delphi panel may introduce bias, as the findings are based on the subjective views of those who participated in the study (46). Nevertheless, we tried to mitigate this bias by having a variety of experts ranging from academics to physicians currently practising. The decision to group the extremes of the 5-point Likert scale (i.e., joining the “strongly disagree” and the “disagree” voting options, as well as the “agree” and “strongly agree”) after the distribution of votes in the 2nd round was deemed the most viable solution for achieving conclusive results while maintaining their reliability. Also noteworthy, is the fact that the third and final round did not add many consensuses into fruition which can be perceived as a confirmation that the experts felt strongly about the subject and the votes they gave in the second round remained consistent, even after being asked to consider them again, after changing from a 5-point Likert scale to a 3-point one.
Conclusion
This study identified significant organizational factors contributing to physician burnout and interventions to prevent and mitigate the syndrome. In this study, the main contributing factors of burnout include inadequate organizational support, system pressure, personnel overload, unfavourable working circumstances, and inadequate compensation. Interventions targeting these factors, such as policy changes, increased resource allocation, and promotion of a healthier work culture, achieved strong consensus among experts. Non-organizational tactics such as the implementation of workplace amenities and health literacy programs were also considered crucial.
By highlighting the importance of organizational factors over individual ones, this research contributes to our understanding of physician burnout and some of the solutions to tackle it. The findings suggest that systemic changes within healthcare institutions are more crucial than interventions targeting individual resilience. By identifying specific organizational interventions, this study contributes to a more nuanced approach to preventing and mitigating burnout. These results may influence management strategies and policies in healthcare systems dealing with comparable problems.
Burnout in the healthcare industry is a complex problem that primarily calls for systemic approaches while also emphasizing the value of individual-based interventions. Subsequent research may examine the interaction between individual and organizational elements, scrutinizing the ways in which personal characteristics and coping strategies intersect with systemic influences. This all-encompassing method might result in more thorough burnout prevention techniques.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/ participants OR patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
CS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Visualization, Writing – original draft, Writing – review & editing. IF: Validation, Writing – review & editing. AP: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Fundação para a Ciência e Tecnologia (FCT, Portugal) through national funds to the Associated Laboratory in Translation and Innovation Towards Global Health REAL (LA/P/0117/2020).
Acknowledgments
We sincerely thank the experts for their voluntary participation in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Shanafelt, TD, West, CP, Dyrbye, LN, Trockel, M, Tutty, M, Wang, H, et al. Changes in burnout and satisfaction with work-life integration in physicians during the first 2 years of the COVID-19 pandemic. Mayo Clin Proc. (2022) 97:2248–58. doi: 10.1016/j.mayocp.2022.09.002
2. Ortega, MV, Hidrue, MK, Lehrhoff, SR, Ellis, DB, Sisodia, RC, Curry, WT, et al. Patterns in physician burnout in a stable-linked cohort. JAMA Netw Open. (2023) 6:e2336745. doi: 10.1001/jamanetworkopen.2023.36745
3. Fronteira, I, Mathews, V, Matsumoto, K, Amde, W, Pereira, A, et al. Impacts for health and care workers of Covid-19 and other public health emergencies of international concern: living systematic review, meta-analysis and policy recommendations. Hum Resour Health. (2024) 22:10. doi: 10.1186/s12960-024-00892-2
4. Tanios, M, Haberman, D, Bouchard, J, Motherwell, M, and Patel, J. Analyses of burn-out among medical professionals and suggested solutions—a narrative review. J Hosp Manag Health Policy. (2022) 6:7. doi: 10.21037/jhmhp-20-153
5. Sovold, LE, Naslund, JA, Kousoulis, AA, Saxena, S, Qoronfleh, MW, Grobler, C, et al. Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Front Public Health. (2021) 9:679397. doi: 10.3389/fpubh.2021.679397
6. Li, YT, Chen, SJ, Lin, KJ, Ku, GC, Kao, WY, and Chen, IS. Relationships among healthcare providers’ job demands, leisure involvement, emotional exhaustion, and leave intention under the COVID-19 pandemic. Healthcare (Basel). (2022) 11:56. doi: 10.3390/healthcare11010056
7. Ferreira, S, Sousa, MM, Moreira, PS, Sousa, N, Picó-Pérez, M, and Morgado, P. A wake-up call for burnout in Portuguese physicians during the COVID-19 outbreak: national survey study. JMIR Public Health Surveill. (2021) 7:e24312. doi: 10.2196/24312
8. Youssef, D, Youssef, J, Abou-Abbas, L, Kawtharani, M, and Hassan, H. Prevalence and correlates of burnout among physicians in a developing country facing multi-layered crises: a cross-sectional study. Sci Rep. (2022) 12:12615. doi: 10.1038/s41598-022-16095-5
9. Batanda, I. Prevalence of burnout among healthcare professionals: a survey at fort portal regional referral hospital. Npj Ment Health Res. (2024) 3:1–10. doi: 10.1038/s44184-024-00061-2
10. Rotenstein, LS, Torre, M, Ramos, MA, Rosales, RC, Guille, C, Sen, S, et al. Prevalence of burnout among physicians: a systematic review. JAMA. (2018) 320:1131–50. doi: 10.1001/jama.2018.12777
11. Marques-Pinto, A, Moreira, S, Costa-Lopes, R, Zózimo, N, and Vala, J. Predictors of burnout among physicians: evidence from a national study in Portugal. Front Psychol. (2021) 12:699974. doi: 10.3389/fpsyg.2021.699974
12. World Health Organization. Burn-out an “occupational phenomenon”: international classification of diseases (2019). Available online at: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (Accessed October 17, 2024)
13. Aronsson, G, Theorell, T, Grape, T, Hammarstrom, A, Hogstedt, C, Marteinsdottir, I, et al. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health. (2017) 17:264. doi: 10.1186/s12889-017-4153-7
14. Koutsimani, P, Montgomery, A, and Georganta, K. The relationship between burnout, depression, and anxiety: a systematic review and meta-analysis. Front Psychol. (2019) 10:284. doi: 10.3389/fpsyg.2019.00284
15. Martins, P, Luzia, RWS, Filho, JAP, Welsh, KS, Fuzikawa, C, Nicolato, R, et al. Prevalence and factors associated with burnout among health professionals of a public hospital network during the COVID-19 pandemic. PLoS One. (2024) 19:e0298187. doi: 10.1371/journal.pone.0298187
16. Patel, RS, Bachu, R, Adikey, A, Malik, M, and Shah, M. Factors related to physician burnout and its consequences: a review. Behav Sci. (2018) 8:98. doi: 10.3390/bs8110098
17. Dewa, CS, Loong, D, Bonato, S, and Trojanowski, L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. (2017) 7:e015141. doi: 10.1136/bmjopen-2016-015141
18. Garcia, CL, Abreu, LC, Ramos, JL, Castro, CF, Smiderle, FR, Santos, JA, et al. Influence of burnout on patient safety: systematic review and meta-analysis. Med Kaunas Lith. (2019) 55:553. doi: 10.3390/medicina55090553
19. Maslach, C, and Leiter, MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. (2016) 15:103–11. doi: 10.1002/wps.20311
20. Han, S, Shanafelt, TD, Sinsky, CA, Awad, KM, Dyrbye, LN, Fiscus, LC, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. (2019) 170:784–90. doi: 10.7326/M18-1422
21. Shin, P, Desai, V, Conte, AH, and Qiu, C. Time out: the impact of physician burnout on patient care quality and safety in perioperative medicine. Perm J. (2023) 27:160–8. doi: 10.7812/TPP/23.015
22. Alrawashdeh, HM, Al-Tammemi, AB, Alzawahreh, MK, Al-Tamimi, A, Elkholy, M, Al Sarireh, F, et al. Occupational burnout and job satisfaction among physicians in times of COVID-19 crisis: a convergent parallel mixed-method study. BMC Public Health. (2021) 21:811. doi: 10.1186/s12889-021-10897-4
23. Patrick, A, and Pryor, R. COVID-19, burnout, and healthcare-associated infections: a focus on wellness as a top safety priority. Antimicrob Steward Healthc Epidemiol. (2023) 3:e155. doi: 10.1017/ash.2023.191
24. European Junior Doctors Association. Policy on burnout and psychosocial wellbeing (2023). Available online at: https://www.juniordoctors.eu/sites/default/files/2023-06/EJD-2023-015_P_Policy%20on%20burnout%20and%20psychosocial%20wellbeing.pdf (Accessed October 17, 2024)
25. Agency for Healthcare Research and Quality. Physician burnout; (2023). Available online at: https://www.ahrq.gov/prevention/clinician/ahrq-works/burnout/index.html (Accessed October 17, 2024)
26. Fink, A, Kosecoff, J, Chassin, M, and Brook, RH. Consensus methods: characteristics and guidelines for use. Am J Public Health. (1984) 74:979–83. doi: 10.2105/ajph.74.9.979
27. Diamond, IR, Grant, RC, Feldman, BM, Pencharz, PB, Ling, SC, Moore, AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. (2014) 67:401–9. doi: 10.1016/j.jclinepi.2013.12.002
28. Skulmoski, GJ, Hartman, FT, and Krahn, J. The Delphi method for graduate research. J Inf Technol Educ Res. (2007) 6:1–21. doi: 10.28945/199
29. OECD. Doctors (overall number) In: Health at a glance 2023: OECD indicators. Paris: OECD (2023). 232.
30. Humphrey-Murto, S, Varpio, L, Gonsalves, C, and Wood, TJ. Using consensus group methods such as Delphi and nominal group in medical education research. Med Teach. (2017) 39:14–9. doi: 10.1080/0142159X.2017.1245856
31. Trevelyan, EG, and Robinson, PN. Delphi methodology in health research: how to do it? Eur J Integr Med. (2015) 7:423–8. doi: 10.1016/j.eujim.2015.07.002
32. Shang, Z. Use of Delphi in health sciences research: a narrative review. Medicine (Baltimore). (2023) 102:e32829. doi: 10.1097/MD.0000000000032829
33. Hsu, C-C, and Sandford, BA. The Delphi technique: making sense of consensus. Pract Assess Res Eval. (2007) 12:10. doi: 10.7275/pdz9-th90
34. Tawfik, DS, Profit, J, Webber, S, and Shanafelt, TD. Organizational factors affecting physician well-being. Curr Treat Options Pediatr. (2019) 5:11–25. doi: 10.1007/s40746-019-00147-6
35. Oliver, D. David Oliver: when “resilience” becomes a dirty word. BMJ. (2017) 358:j3604. doi: 10.1136/bmj.j3604
36. Balme, E. Doctors need to be supported, not trained in resilience. BMJ. (2015) 351:h4709. doi: 10.1136/bmj.h4709
37. Fox, KE, Johnson, ST, Berkman, LF, Sianoja, M, Soh, Y, Kubzansky, LD, et al. Organisational- and group-level workplace interventions and their effect on multiple domains of worker well-being: a systematic review. Work Stress. (2021) 36:30–59. doi: 10.1080/02678373.2021.1969476
38. West, CP, Dyrbye, LN, Erwin, PJ, and Shanafelt, TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet Lond Engl. (2016) 388:2272–81. doi: 10.1016/S0140-6736(16)31279-X
39. Gaeta, TJ. Need for a holistic approach to reducing burnout and promoting well-being. J Am Coll Emerg Physicians Open. (2020) 1:1050–1. doi: 10.1002/emp2.12111
40. National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine. Committee on systems approaches to improve patient care by supporting clinician well-being. Taking action against clinician burnout: A systems approach to professional well-being [Internet]. Washington, DC: National Academies Press (US) (2019). 334 p.
41. West, CP, Dyrbye, LN, and Shanafelt, TD. Physician burnout: contributors, consequences and solutions. J Intern Med. (2018) 283:516–29. doi: 10.1111/joim.12752
42. European Observatory on Health Systems and Policies. Countries covered by the HSPM platform (2024). Available online at: https://eurohealthobservatory.who.int/monitors/health-systems-monitor/countries-hspm (Accessed November 5, 2024)
43. de A, SJ, Augusto, GF, Fronteira, I, and Hernández-Quevedo, C. Portugal: health system review. Health Syst Transit. (2017) 19:1–184.
44. Looi, MK. The European healthcare workforce crisis: how bad is it? BMJ. (2024) 384:q8. doi: 10.1136/bmj.q8
45. Azzopardi-Muscat, N, Zapata, T, and Kluge, H. Moving from health workforce crisis to health workforce success: the time to act is now. Lancet Reg Health Eur. (2023) 35:100765. doi: 10.1016/j.lanepe.2023.100765
Keywords: burnout, interventions, mental health, NHS, Delphi
Citation: Simões C, Fronteira I and Pedro AR (2025) Factors that contribute to physician burnout, interventions to prevent and mitigate burnout and knowledge gaps—a Delphi study. Front. Public Health. 13:1540214. doi: 10.3389/fpubh.2025.1540214
Edited by:
Angela Stufano, University of Bari Aldo Moro, ItalyReviewed by:
Sinan Yılmaz, Atatürk University, TürkiyeAline Yacoubian, American University of Beirut Medical Center, Lebanon
Ricardo Veiga, Federal University of Minas Gerais, Brazil
Copyright © 2025 Simões, Fronteira and Pedro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catarina Simões, Y3JyLnNpbW9lc0BlbnNwLnVubC5wdA==