 Jhanvi Dholakia
Jhanvi Dholakia Anantha Narayanan2
Anantha Narayanan2- 1Department of General Surgery, Waikato Hospital, Hamilton, New Zealand
- 2Department of Vascular Surgery, Waikato Hospital, Hamilton, New Zealand
Burnout is a growing phenomenon among medical professionals due to aging patient populations and an increasing burden of chronic disease, in a resource constrained environment. We aim to quantify the prevalence of burnout in surgical specialists and registrars at a tertiary center in New Zealand and identify contributory factors, using a New Zealand based tool, the McEwan Burnout Questionnaire. Of the 110 people surveyed, 55% respondents had concern or high risk of burnout. Contributory factors were frustration with management, lack of resources and long working hours, with predominance toward fatigue and service provision over career progression among the registrar group. Bullying and harassment were reported more in the sub-specialty groups. More time in private practice appeared to be associated with less concern for burnout. These high rates of burnout require targeted interventions toward contributory factors to protect our workers and to maintain a sustainable workforce.
Introduction
Occupational burnout results from overwhelming unmanaged workplace stress that leads to mental exhaustion, dissociation from one’s work, negative feelings and reduced efficacy (1). In recent years, increasing rates of burnout have been reported in the doctor population as worldwide workforce shortages have exacerbated working conditions, compounded by stressors such as budget cuts, bureaucratic processes and lack of autonomy (2–4). Doctors with burnout describe being unable to empathize with their patients, a sense of depersonalization and a fall in self-worth (5). Surgeons are particularly prone to burnout, highlighted in Medscape survey of twelve thousand American doctors with 45% of the general surgeons experiencing burnout, with similar findings among orthopedic and plastic surgical specialties (6, 7). Attributable factors include poor work-life balance, long working hours, erratic on call schedules, inability to cope with patient suffering, and hospital management issues (8–11). An individual surgeon suffering from burnout is at risk of increased rates of psychiatric comorbidities, alcohol and substance use, and suicide and is also associated with poorer patient outcomes (12–14). There is a greater association of burnout with patient errors, which is associated with higher rates of depression in physicians (3). Patients treated by depersonalized physicians are reported to have longer recovery periods once they leave hospital (15). Burnout leads to higher attrition rates for surgeons, further worsening workforce shortages and leading to increased financial costs to healthcare (16). This study by Han et al. has estimated the annual cost of burnout to be $4.6 billion in the United States alone (16). Understanding the incidence and predictors of burnout among surgeons is therefore paramount to creating meaningful change in clinician wellbeing.
There are no studies that report burnout across all surgical specialists in New Zealand. The aim of this study is to identify the prevalence of burnout in cross-specialty senior medical officers/surgeons (SMO), training registrars (TR) and non-training registrars (NTR), and establish factors that may be associated with burnout, using a survey tool developed in New Zealand for the resident population.
Materials and methods
This survey based observational cross-sectional study was conducted at a major tertiary hospital in New Zealand in October 2023. The Consensus-Based Checklist for Reporting of Survey Studies (CROSS) was utilized in the design (17). All surgical SMO, TR and NTR (n = 239) at our hospital were invited to participate in our study. Respondents were non-incentivized, and responses were anonymized. Respondents were recruited through email contact and surveys disseminated by SurveyMonkey™, with follow up emails sent at 4 and 8 weeks. Incomplete surveys were excluded from the study.
Demographic data collected included age, gender, current specialty, level of training, level of experience and private and public work division for specialists. The McEwan Burnout Questionnaire (MBQ) (Supplementary material), developed for the New Zealand population, assesses the three parts of the burnout syndrome using 20 questions each answered with a Likert scale (18). Cumulative scores were calculated, which allowed individuals to be stratified according to their risk of burnout into broad categories of “doing well” (0–25), or “not doing well” (>25), with further sub-categories of “concern for burnout” (26–39), “high risk of burnout” (40–59) and “burnt out” (60–80) (18). Additionally, respondents identified factors that contributed to their workplace stress.
TR and NTR were grouped as resident medical officers (RMO). Specialties were grouped to three categories: general surgery, orthopedic surgery and subspecialty surgery (which included cardiothoracic, otolaryngology, maxillofacial, neurosurgery, ophthalmology, plastic and burns surgery, urology and vascular surgery).
Statistics
Summary statistics were calculated for all outcomes of interest. Parametric data between groups was compared using unpaired student’s t-test. Ranked non-parametric data were compared using Mann–Whitney U testing. Categorical data were compared using the Pearson Chi squared and Fisher’s Exact test. A multivariate regression analysis was performed to establish associations between variables. Analysis was carried out using SPSS (v29.0). A p-value < 0.05 was considered statistically significant.
Ethics statement
This project was deemed out of scope of the Health and Disability Ethics Committee (HDEC REF: 2024 OOS 21393). All respondents gave informed consent and completed the questionnaire voluntarily.
Results
Of the 239 people invited to participate, 110 people completed the survey in its entirety (46% response rate). Of these respondents, 24 (22%) were female and 67 (61%) were SMOs. Demographic data is shown in Table 1. Three respondents did not disclose their specialty, and one respondent did not disclose their gender.
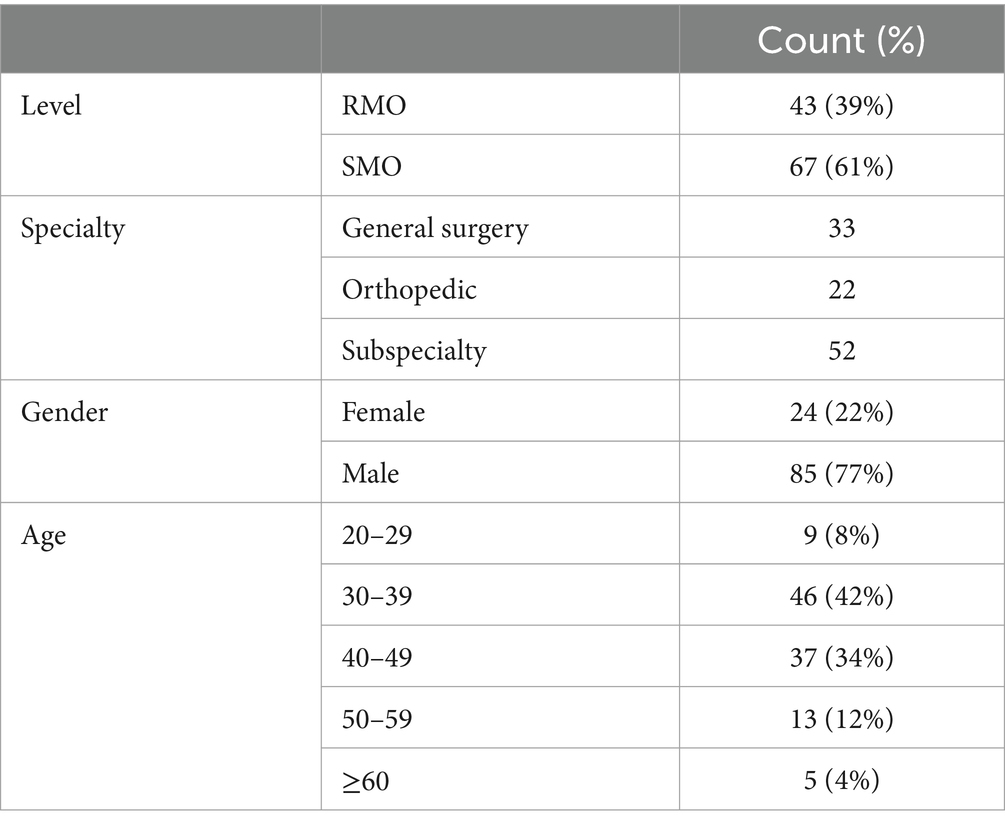
Table 1. Demographic data.
Cumulative scores were calculated from the survey results. The mean burnout score in our cohort was 28 (SD 13.7, range 1–71). As shown in Table 2, in this population 49 people (45%) were doing well, and 61 (55%) were “not doing well.” Of these, 37 (34%) had concern for burnout, 23 (21%) were at high risk of burnout and 1 (1%) person was burnt out. In the RMO group, 65% respondents presented as “not doing well,” compared to 51% in the SMO group (p = 0.25). The highest risk age group was 20–29 years with 67% respondents presenting as “not doing well.” There was a non-significant tendency toward lower mean burnout scores as clinician age increased. In the individuals over the age of 60 years, all 13 respondents were “doing well.”
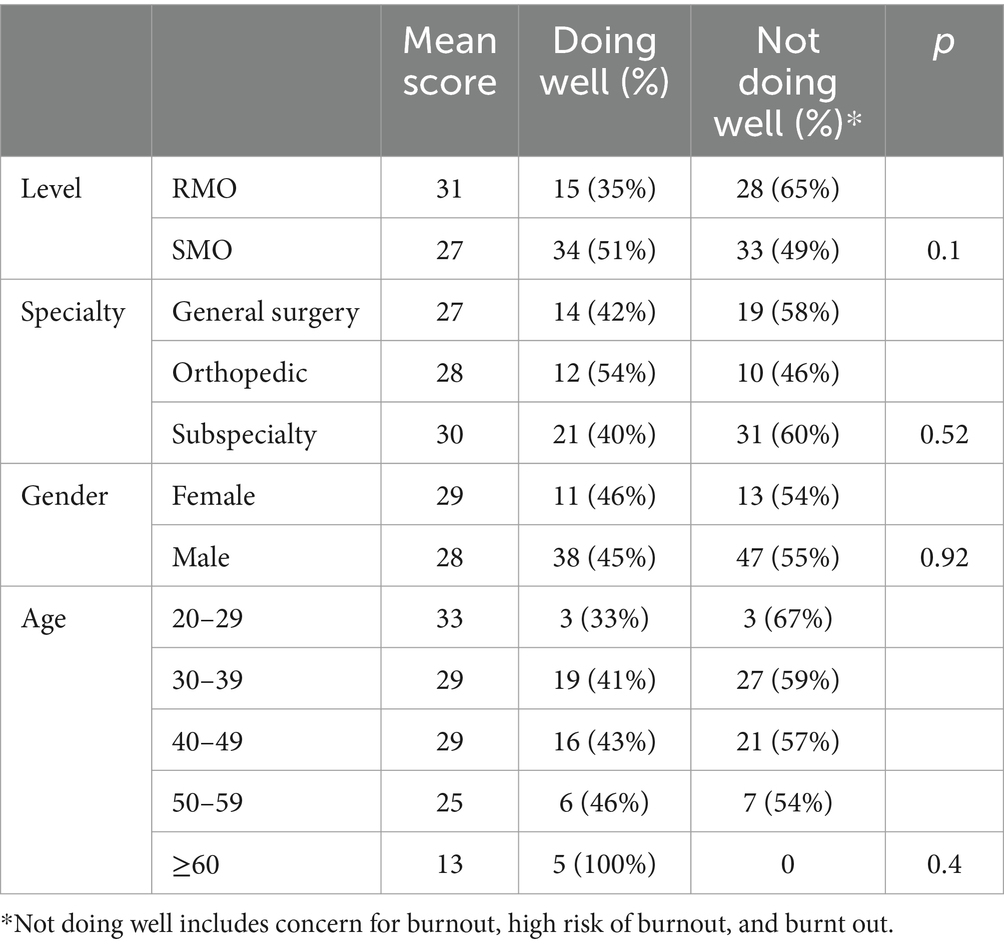
Table 2. Burnout by demographic.
In the SMO group, 20 respondents (30%) spent more than one third of their clinical time in private practice. Of this subgroup, only 5% scored as “not doing well” compared to 26% in the group that spent less than one-third of their clinical time in private practice (p = 0.05), suggesting that clinical time spent in private practice may be associated with lower burnout rates. Subgroup analysis showed that in the RMO group, 8 (30%) male respondents were “not doing well,” compared to 10 (59%) female respondents (p = 0.06). This tendency toward gender difference was not seen in the specialist SMO population. Of the different specialties, cardiothoracic and, plastic and burns surgery presented with the greatest proportion of people “not doing well,” 88 and 62%, respectively. Specialties where the majority of respondents were doing well included neurosurgery (57%), vascular (57%), and orthopedics (55%).
Bullying and harassment contributed to burnout in 21% of respondents in RMO group and 20% of the SMO group. Overall, there were no gender differences in reporting bullying and harassment, however within the RMO subgroup there was a higher reported prevalence among male respondents (25% vs. 4%, p = 0.02). Bullying and harassment as a reported contributor to burnout was also noted to be more prevalent in the subspecialty group with 31% compared to General surgery (9%), and Orthopedic surgery (14%) (p = 0.037).
Sub analysis by gender showed more females identified acquisition of training positions as a factor contributing to burnout (42%) compared to males (12%) (p < 0.001) and there was a non-significant tendency toward females reporting clinical uncertainty to be a contributor of burnout (42%) compared to males (27%) (p = 0.08).
Common factors contributing to workplace stress in all groups included frustration with management (66%), lack of resource (64%), long working hours (56%), interference with home life (50%) and fatigue (49%). Factors that did not contribute significantly to burnout included boredom (2%), private practice (7%), and medico-legal concerns (9%). The RMO group compared to the SMO group were more likely to report fatigue (70% vs. 36%, p < 0.001) and service provision being valued over career progression (70% vs. 31%, p < 0.001) as contributory factors. However, lack of resource was a more common response in the SMO population (76% vs. 47%, p = 0.002). The fear of bad outcomes was a contributor of burnout in both SMO (28%) and RMO (44%) groups (p = 0.08).
Discussion
This study demonstrates that burnout has a prevalence of 25% in our surgical population, with a further 33% of doctors showing concern for burnout. This is similar to international literature that shows a burnout rate of 40–80% in surgeons and training surgeons (19–21). Time in private practice appeared to be associated with less concern for burnout in the SMO group. Junior staff were more at risk of burnout and were more likely to report fatigue and service provision as contributory factors. The male RMO and subspecialty groups reported a higher tendency to experience bullying and harassment, while female RMO describe acquisition of training positions and clinical uncertainty to be contributors of burnout.
Our results are in line with published literature highlighting the prevalence of burnout among RMOs. This has been attributed to multiple factors in this group, which include long working hours without breaks, shift work, on-calls, and greater than 80-h work weeks (22–24). These working conditions are known to cause significant physiological strain such as periods of increased heart rate (25) and increased levels of cortisol (26, 27) in junior doctors compared to senior staff associated with on call periods. Multiple programs such as resilience training, mindfulness training, ergonomics workshops and neurofeedback workshops have shown to improve wellbeing and decrease risk of burnout in surgeons and surgical residents (28–30).
Time split between private and public work showed that surgeons who spent more than a third of their time in private practice were at less risk of burnout. This may be related to multiple factors such as increased autonomy, less resource constraints, and less bureaucratic measures in the private sector (31). Private practice also provides greater earning potential which in turn could be associated to improved job satisfaction, a feeling of adequate compensation and therefore, decreases the risk of burnout (32–34).
This study demonstrated a tendency toward female RMOs reporting a higher rate of burnout compared to their male counterparts, which is reflective of prior studies (24, 35). Multiple studies have reported the underlying cause for this gender-based disparity is likely the higher rate of microaggressions by way of discrimination, abuse and harassment that women experience in a surgical workplace (24, 36, 37). A separate study found that women were more likely to receive negative comments about pregnancy from their colleagues, experience more harsh evaluations from their supervisors, and frequently be mistaken for non-medical staff (38). Interestingly, however, in our cohort, males were more likely to report bullying as a cause of burnout than females.
Areas of intervention to decrease burnout can be directed at the individual doctor level, at the hospital level and at a national level. For the doctor, protective factors focus on developing emotional coping strategies to deal with adverse events through resilience training, mindfulness and professional support groups (21, 39). The “Operating with Respect” and “Training in Professional Skills” courses, developed by the Royal Australasian College of Surgeons look to educate individuals on addressing and responding to bullying and harassment and improve conflict resolution skills (40). At the institutional level, mentoring, access to general practitioners, childcare access and support, peer support programs and small discussion groups, and adequate financial compensation are factors which may decrease stressors and thus decrease the rate of burnout (41–43). At the national level recognizing surgeon mental health as collateral damage in an overworked system is important, to then be able to implement safer working hours, increase resources through better staffing, provide more support, and thus decrease attrition thus benefitting the health service (44).
There are limitations to this study. Despite a satisfactory response rate of 46%, respondent bias may skew the results toward those who are interested in or feel strongly toward reporting burnout. The female respondent rate if 22% is slightly lower than the proportion of females in the total surgical workforce (28%) as described by the 2023 Workforce Survey report from the Medical Council of New Zealand, which may influence the gender-based findings in our study. This study was conducted in one major tertiary center with subspecialty departments, the views expressed here may be limited in their generalizability to different tertiary institutions or smaller regional hospitals within or outside of New Zealand.
Conclusion
In this cohort of 110 surgical specialists and registrars, 55% respondents had concern or high risk of burnout using the McEwan Burnout Questionnaire. Contributory factors were frustration with management, lack of resource and long working hours, with predominance toward fatigue and service provision over career progression among the RMO group. Bullying and harassment were reported more in the sub-specialty groups. More time in private practice appeared to be associated with less concern. These high rates of burnout require targeted interventions toward contributory factors to protect our workers to maintain a sustainable workforce.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The requirement of ethical approval was waived by Health and Disability Ethics Committee (HDEC REF: 2024 OOS 21393) for the studies involving humans because Health and Disability Ethics Committee (HDEC REF: 2024 OOS 21393). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. AN: Formal analysis, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing. NS: Conceptualization, Data curation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1541892/full#supplementary-material
References
1. World Health Organisation. Burnout an “occupational phenomenon”: International classification of diseases [internet]. Geneva: World Health Organisation (2019) Available at: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases.
2. Greep, NC, Woolhandler, S, and Himmelstein, D. Physician burnout: fix the doctor or fix the system? Am J Med. (2022) 135:416–7. doi: 10.1016/j.amjmed.2021.10.011
3. Lacy, BE, and Chan, JL. Physician burnout: the hidden health care crisis. Clin Gastroenterol Hepatol. (2018) 16:311–7. doi: 10.1016/j.cgh.2017.06.043
4. New Zealand Medical Council. The New Zealand medical workforce in 2021 [internet]. Wellington: New Zealand Medical Council (2021) Available at: https://www.nzdoctor.co.nz/sites/default/files/2022-06/Medical_Council_Workforce-Survey-Report-2021.pdf.
5. Maslach, C, Jackson, S, and Leiter, M. The Maslach burnout inventory manual In: W Zalaquett, editor. Evaluating stress: A book of resources. The Scarecrow Press (1997). 191–218.
6. Travers, V. Burnout in orthopedic surgeons. Orthop Traumatol Surg Res. (2020) 106:S7–S12. doi: 10.1016/j.otsr.2019.04.029
7. Khansa, I, and Janis, JE. A growing epidemic: plastic surgeons and burnout-a literature review. Plast Reconstr Surg. (2019) 144:298e–305e. doi: 10.1097/PRS.0000000000005875
8. Shanafelt, TD, Balch, CM, Bechamps, GJ, Russell, T, Dyrbye, L, Satele, D, et al. Burnout and career satisfaction among American surgeons. Ann Surg. (2009) 250:463–71. doi: 10.1097/SLA.0b013e3181ac4dfd
9. Dyrbye, LN, Shanafelt, TD, Balch, CM, Satele, D, Sloan, J, and Freischlag, J. Relationship between work-home conflicts and burnout among American surgeons: a comparison by sex. Arch Surg. (2011) 146:211–7. doi: 10.1001/archsurg.2010.310
10. Barrack, RL, Miller, LS, Sotile, WM, Sotile, MO, and Rubash, HE. Effect of duty hour standards on burnout among orthopaedic surgery residents. Clin Orthop Relat Res. (2006) 449:134–7. doi: 10.1097/01.blo.0000224030.78108.58
11. Gifford, E, Galante, J, Kaji, AH, Nguyen, V, Nelson, MT, Sidwell, RA, et al. Factors associated with general surgery residents’ desire to leave residency programs: a multi-institutional study. JAMA Surg. (2014) 149:948–53. doi: 10.1001/jamasurg.2014.935
12. Yaghmour, NA, Brigham, TP, Richter, T, Miller, RS, Philibert, I, Baldwin, DWC, et al. Causes of death of residents in ACGME-accredited programs 2000 through 2014: implications for the learning environment. Acad Med. (2017) 92:976–83. doi: 10.1097/ACM.0000000000001736
13. Hewitt, DB, Chung, JW, Ellis, RJ, Cheung, EO, Moskowitz, JT, Hu, YY, et al. National Evaluation of surgical resident grit and the association with wellness outcomes. JAMA Surg. (2021) 156:856–63. doi: 10.1001/jamasurg.2021.2378
14. Dewa, CS, Loong, D, Bonato, S, and Trojanowski, L. The relationship between physician burnout and quality of healthcare in terms of safety and acceptability: a systematic review. BMJ Open. (2017) 7:e015141. doi: 10.1136/bmjopen-2016-015141
15. Halbesleben, JRB, and Rathert, C. Linking physician burnout and patient outcomes. Health Care Manag Rev. (2008) 33:29–39. doi: 10.1097/01.HMR.0000304493.87898.72
16. Han, S, Shanafelt, TD, Sinsky, CA, Awad, KM, Dyrbye, LN, Fiscus, LC, et al. Estimating the attributable cost of physician burnout in the United States. Ann Intern Med. (2019) 170:784–90. doi: 10.7326/M18-1422
17. Sharma, A, Minh Duc, NT, Luu Lam Thang, T, Nam, NH, Ng, SJ, Abbas, KS, et al. A consensus-based checklist for reporting of survey studies (CROSS). J Gen Intern Med. (2021) 36:3179–87. doi: 10.1007/s11606-021-06737-1
18. McEwan, J. Burnout questionnaire [internet]. New Zealand: Resilience building ; (2003). Available at: https://drstress.co.nz/wp-content/uploads/2020/02/resilience-building-handout.pdf.
19. Dimou, FM, Eckelbarger, D, and Riall, TS. Surgeon burnout: a systematic review. J Am Coll Surg. (2016) 222:1230–9. doi: 10.1016/j.jamcollsurg.2016.03.022
20. Elmore, LC, Jeffe, DB, Jin, L, Awad, MM, and Turnbull, IR. National Survey of burnout among US general surgery residents. J Am Coll Surg. (2016) 223:440–51. doi: 10.1016/j.jamcollsurg.2016.05.014
21. Brandt, ML. Sustaining a career in surgery. Am J Surg. (2017) 214:707–14. doi: 10.1016/j.amjsurg.2017.06.022
22. Jackson, T, Provencio, A, Bentley-Kumar, K, Pearcy, C, Cook, T, McLean, K, et al. PTSD and surgical residents: everybody hurts … sometimes. Am J Surg. (2017) 214:1118–24. doi: 10.1016/j.amjsurg.2017.08.037
23. Kinslow, K, Sutherland, M, McKenney, M, and Elkbuli, A. Reported burnout among U.S. general surgery residents: a survey of the association of program directors in surgery members. Ann Med Surg. (2020) 60:14–9. doi: 10.1016/j.amsu.2020.10.012
24. Hu, Y-Y, Ellis, RJ, Hewitt, DB, Yang, AD, Cheung, EO, Moskowitz, JT, et al. Discrimination, abuse, harassment, and burnout in surgical residency training. N Engl J Med. (2019) 381:1741–52. doi: 10.1056/NEJMsa1903759
25. Tendulkar, AP, Victorino, GP, Chong, TJ, Bullard, KM, Liu, TH, and Harken, AH. Quantification of surgical resident stress “on call”. J Am Coll Surg. (2005) 201:560–4. doi: 10.1016/j.jamcollsurg.2005.05.004
26. Schlosser, K, Maschuw, K, Kupietz, E, Weyers, P, Schneider, R, Rothmund, M, et al. Call-associated acute fatigue in surgical residents--subjective perception or objective fact? A cross-sectional observational study to examine the influence of fatigue on surgical performance. World J Surg. (2012) 36:2276–87. doi: 10.1007/s00268-012-1699-5
27. Choshen-Hillel, S, Ishqer, A, Mahameed, F, Reiter, J, Gozal, D, Gileles-Hillel, A, et al. Acute and chronic sleep deprivation in residents: cognition and stress biomarkers. Med Educ. (2021) 55:174–84. doi: 10.1111/medu.14296
28. Song, Y, Swendiman, RA, Shannon, AB, Torres-Landa, S, Khan, FN, Williams, NN, et al. Can we coach resilience? An evaluation of professional resilience coaching as a well-being initiative for surgical interns. J Surg Educ. (2020) 77:1481–9. doi: 10.1016/j.jsurg.2020.04.014
29. Saway, BF, Seidel, LW, Dane, FC, and Wattsman, T. Mindfulness in the OR: a pilot study investigating the efficacy of an abbreviated mindfulness intervention on improving performance in the operating room. J Surg Educ. (2021) 78:1611–7. doi: 10.1016/j.jsurg.2021.03.013
30. Cerier, E, Hu, A, Goldring, A, Rho, M, and Kulkarni, SA. Ergonomics workshop improves musculoskeletal symptoms in general surgery residents. J Surg Res. (2022) 280:567–74. doi: 10.1016/j.jss.2022.06.014
31. Leigh, JP, Tancredi, DJ, and Kravitz, RL. Physician career satisfaction within specialties. BMC Health Serv Res. (2009) 9:166. doi: 10.1186/1472-6963-9-166
32. Kao, AC, Jager, AJ, Koenig, BA, Moller, AC, Tutty, MA, Williams, GC, et al. Physician perception of pay fairness and its association with work satisfaction, intent to leave practice, and personal health. J Gen Intern Med. (2018) 33:812–7. doi: 10.1007/s11606-017-4303-8
33. Prakash, S, and Satiani, B. Analysis of compensation disparities between junior academic and private practice vascular surgeons. Ann Vasc Surg. (2017) 39:236–41. doi: 10.1016/j.avsg.2016.05.127
34. Baimas-George, M, Fleischer, B, Korndorffer, JR, Slakey, D, and DuCoin, C. The economics of private practice versus academia in surgery. J Surg Educ. (2018) 75:1276–80. doi: 10.1016/j.jsurg.2018.03.006
35. Dahlke, AR, Johnson, JK, Greenberg, CC, Love, R, Kreutzer, L, Hewitt, DB, et al. Gender differences in utilization of duty-hour regulations, aspects of burnout, and psychological well-being among general surgery residents in the United States. Ann Surg. (2018) 268:204–11. doi: 10.1097/SLA.0000000000002700
36. Zhang, LM, Ellis, RJ, Ma, M, Cheung, EO, Hoyt, DB, Bilimoria, KY, et al. Prevalence, types, and sources of bullying reported by US general surgery residents in 2019. JAMA. (2020) 323:2093–5. doi: 10.1001/jama.2020.2901
37. Lund, S, D’Angelo, JD, Jogerst, K, Warner, SG, Busch, R, and D’Angelo, ALD. Revealing hidden experiences: gendered microaggressions and surgical faculty burnout. Surgery. (2022) 172:885–9. doi: 10.1016/j.surg.2022.04.032
38. Schlick, CJR, Ellis, RJ, Etkin, CD, Greenberg, CC, Greenberg, JA, Turner, PL, et al. Experiences of gender discrimination and sexual harassment among residents in general surgery programs across the US. JAMA Surg. (2021) 156:942–52. doi: 10.1001/jamasurg.2021.3195
39. Gleason, F, Baker, SJ, Wood, T, Wood, L, Hollis, RH, Chu, DI, et al. Emotional intelligence and burnout in surgical residents: a 5-year study. J Surg Educ. (2020) 77:e63–70. doi: 10.1016/j.jsurg.2020.07.044
40. Royal Australasian College of Surgeons. Building respect, improving patient safety: From awareness to action. Melbourne: (2015) Available at: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/Judy-Finn/EAG-Report_Recs-and-Actions_150822.pdf?rev=2cc5598bc2464f978bbbf53d5825f970&hash=CBC9B35F39A644274345F14C0511560D.
41. Shen, MR, Zhuo, L, Madison, K, Bredbeck, BC, Kemp, MT, Santos-Parker, JR, et al. How we do it: an innovative general surgery mentoring program. J Surg Educ. (2022) 79:1088–92. doi: 10.1016/j.jsurg.2022.04.004
42. Castillo-Angeles, M, Smink, DS, and Rangel, EL. Perspectives of general surgery program directors on paternity leave during surgical training. JAMA Surg. (2022) 157:105–11. doi: 10.1001/jamasurg.2021.6223
43. Livingston-Rosanoff, D, Shubeck, SP, Kanters, AE, Dossett, LA, Minter, RM, and Wilke, LG. Got Milk? Design and implementation of a lactation support program for surgeons. Ann Surg. (2019) 270:31–2. doi: 10.1097/SLA.0000000000003269
Keywords: surgery, burnout, workforce, stress, McEwan Burnout Questionnaire, wellbeing, resilience
Citation: Dholakia J, Narayanan A and Smith N (2025) Prevalence and contributory factors to burnout in the New Zealand surgical specialist and registrar population. Front. Public Health. 13:1541892. doi: 10.3389/fpubh.2025.1541892
Edited by:
Angela Stufano, University of Bari Aldo Moro, ItalyReviewed by:
Brandt Wiskur, University of Oklahoma Health Sciences Center, United StatesAline Yacoubian, American University of Beirut Medical Center, Lebanon
Copyright © 2025 Dholakia, Narayanan and Smith. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jhanvi Dholakia, amhhbnZpLmRob2xha2lhQGhvdG1haWwuY29t