 Ariane Mamguem Kamga1*
Ariane Mamguem Kamga1* Samiratou Ouédraogo2
Samiratou Ouédraogo2 Firmin Nongodo Kaboré3
Firmin Nongodo Kaboré3 Isidore Tiandiogo Traoré3Esperance Ouédraogo4Armel Poda5,6Arnaud Eric Diendéré7Dramane Kania3
Isidore Tiandiogo Traoré3Esperance Ouédraogo4Armel Poda5,6Arnaud Eric Diendéré7Dramane Kania3 Hermann Badolo2
Hermann Badolo2 Guillaume Sanou2Amariane Koné3Therese Samdapawindé Kagoné3Blahima Konaté4Rachel Médah3Nathalie de Rekeneire8
Guillaume Sanou2Amariane Koné3Therese Samdapawindé Kagoné3Blahima Konaté4Rachel Médah3Nathalie de Rekeneire8 Boukary Ouédraogo7Oumar Billa1Gilles Paradis9Halidou Tinto10Tienhan Sandrine Dabakuyo-yonli1
Boukary Ouédraogo7Oumar Billa1Gilles Paradis9Halidou Tinto10Tienhan Sandrine Dabakuyo-yonli1- 1Centre Georges François Leclerc, Dijon, France
- 2National Population Health Observatory, National Institute of Public Health, Ouagadougou, Burkina Faso
- 3MURAZ Center, Bobo-Dioulasso, Burkina Faso
- 4Centre National de la Recherche Scientifique et Technologique, Ouagadougou, Burkina Faso
- 5Department of Infectious Diseases, Sourô Sanou University Hospital, Bobo Dioulasso, Burkina Faso
- 6Higher Institute of Health Sciences, Nazi Boni University, Bobo Dioulasso, Burkina Faso
- 7Bogodogo University Hospital, Ouagadougou, Burkina Faso
- 8Expertise France, Paris, France
- 9McGill University, Montreal, QA, Canada
- 10Nanoro Clinical Research Unit, Health Sciences Research Institute, National Centre for Scientific and Technological Research, Bobo Dioulasso, Burkina Faso
Objectives: To assess treatment and identify predictive factors of worsening in COVID-19 patients.
Methods: This study was ambispective (both prospective and retrospective) and part of a multidisciplinary, multicenter project designed to generate epidemiological, sociological and anthropological data about the COVID-19 epidemic in Burkina Faso. Medical records of patients admitted for COVID-19 at the hospitals of Ouagadougou and Bobo-Dioulasso from March 2020 to April 2021 were reviewed. To identify predictive factors of severe complications, we used Poisson regression models.
Results: In total, 1,511 patients were included, of whom 70% were aged ≤50 years, 59% were men and 97% were living in an urban area. Of the 86% of patients treated, 92.9% of them received the combo Azithromycin-hydroxychloroquine. A total of 78 (5.2%) patients experienced complications during hospitalization, and 49 (3.3%) patients died. Multivariate analysis identified patient's age, residence and comorbidity as factors associated with poor outcomes.
Conclusions: Although most people had symptoms, most of them recovered without sequelae, and few patients had severe forms of disease. Age was a strong predictor of worse outcomes in this population.
Introduction
Coronavirus diseases 19 (COVID-19) remains a global pandemic that continues to strain healthcare systems. Although most often benign, it is estimated that around 14% of infected individuals will develop a severe form of infection (1).
Northern countries were the most severely affected by COVID-19 at the beginning of the pandemic, and given that their strong health systems struggled with the disease, the worst was predicted for Africa and other developing countries (2–4). As time passed by, the scenario did not evolve as predicted in Africa, raising several questions about population-acquired immunity, asymptomatic cases, the number of reported cases, whether or not PCR testing was routine (5–7), what treatment to administrate and what factors might predict worsening of the disease.
Burkina Faso is one of the countries affected by the COVID-19 in Africa (8), with the first cases diagnosed in March 2020. As of April 10, 2025, there have been 22,106 reported cases in the country (9), with Ouagadougou and Bobo-Dioulasso being the two most affected major cities (10). The response plan put in place by the government recommended that in addition to barrier measures to limit the spread of the virus, suspected cases of patients with COVID-19 should be identified and treated in health facilities requisitioned by the government in the acute phase the pandemic.
There is a growing body of literature examining the prognostic factors of COVID-19. Many factors have been identified, such as advanced age, sex, comorbidities, oxygen saturation, clinical signs and biological factors (11–14). However, patient and disease factors vary from region to region (15, 16).
Since the notification of the first cases in the country, several studies have been conducted in Burkina Faso to identify the best therapy to manage cases, or socio-anthropological and prognostic studies (10, 17–19). These studies were either conducted in the capital, Ouagadougou only (10, 17, 18), with data collection limited to a few health facilities and using mortality as the outcome criterion (18), or they focused on only one of the severe forms of COVID-19 (18). Moreover, there are few data on how COVID-19 patients were treated in Burkina-Faso.
Thus, the objective of this study was to assess how patients with COVID-19 infection managed in the hospitals of Ouagadougou and Bobo-Dioulasso, Burkina Faso were treated and identify factors associated with worsening and death.
Methods
Study design
This study was part of a large, multidisciplinary, multicenter project (20) designed to generate epidemiological, sociological and anthropological data about the COVID-19 epidemic in Burkina Faso. The present study is an ambispective study (i.e., both prospective and retrospective), and includes all cases admitted to the official COVID-19 management centers in Ouagadougou and Bobo Dioulasso, the two main cities of Burkina Faso, from March 2020 to April 2021.
Inclusion and exclusion criteria
To be eligible, patients had to be hospitalized or have been hospitalized and managed for COVID-19 in the four referral hospitals in Ouagadougou and Bobo-Dioulasso: Souro-Sanou, Tengandogo, Bogodogo and Yagaldo Ouedraogo during the period of March 2020 to April 2021.
Statement of ethical approval
This study is a part of a multicenter project that has been approved by the Ministry of Health (N° 2020-00952/MS/CAB/INSP/CM) and the National Ethics Committee for health research of Burkina Faso (N° 2020-8-140). This study was performed in accordance with the ethical standards of the national research committee, the principles of Good Clinical Practice and the 1964 Helsinki declaration and its later amendments. All study participant of this study has provided signed consent.
Procedure
The prospective part of the study took place from September 13, 2020 to April 30, 2021. Medical records of patients admitted for COVID-19 in the hospitals of Ouagadougou and Bobo-Dioulasso were review. Data were collected using a questionnaire (see supplementary material). Patients were follow-up till death or discharge from the hospital.
Outcome
The main outcome of this study was the proportion of severe complications. Severe complications were defined as the occurrence any one of the following: severe pneumonitis, acute respiratory distress syndrome (ARDS), sepsis, septic shock, coma or death in patients infected with SARS-CoV-2. The proportion of deaths was also assessed.
Independent variables
The following variables were collected for all patients: age, sex, place of residence (urban vs. rural), clinical signs on admission and during hospitalization, comorbidities at admission, lifestyle habits (alcohol, smoking status) and context of contamination as self-reported by patients. Age was categorized into <50 years vs. 50 years or more.
Comorbidities were divided into two categories (No comorbidities vs. at least one comorbidity). Comorbidities included diabetes, high blood pressure (HBP), HIV and other chronic conditions (cardiovascular, neurological, respiratory, renal, rheumatological, hepatic disease). Oxygen saturation in room air at admission (SaO2) was dichotomized as SaO2 < 94% and SaO2 ≥ 94%.
A threshold of 15 was used to dichotomize the Glasgow score. Subjects were considered symptomatic if they had at least one of the symptoms listed in the case report form. Clinical signs on admission were grouped into the following symptom classes: general (fatigue, fever, chills, anorexia, multiorgan failure), respiratory (cough, dyspnea, wheezing, chest pain), neurological (disturbed consciousness, convulsions, headache, ageusia, anosmia), digestive (abdominal pain, diarrhea, nausea/vomiting), musculoskeletal (joint pain, myalgia), Ear Nose and Throat (sore throat, epistaxis, rhinitis) and other symptoms (rash, conjunctivitis, etc.).
Statistical analyses
Categorical variables are presented as number and percentage, and continuous variables as mean ± standard deviation (SD), or median and range, as appropriate.
To identify predictive factors of severe complications, we constructed two Poisson regression models (21). The first was built to identify correlates of admission with severe complications. The second was to identify factors associated with the occurrence of severe complications (including death). For this latter model, we excluded patients who were admitted directly with severe complications.
We first performed univariable analysis. Eligible variables for the multivariable model were all those with p-value < 0.10 by univariable analysis. We then performed backward stepwise selection to obtain the final models. Finally, prognostic factors of time to death were determined using a Cox regression model. Results are reported as relative risk (RR) for Poisson regression models or hazard ratio (HR) for the Cox model with their 95% confidence intervals and p-values.
Test results were considered significant for p-values < 0.05 for descriptive analyses. Considering the multiple analyses we conducted, Bonferroni's correction was applied setting the p-value for the Poisson models to 0.017. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Sociodemographic characteristics
In total, 1,511 people were hospitalized and managed for COVID-19 in the 4 referral teaching hospitals in Ouagadougou and Bobo-Dioulasso. Among them, nearly 60% were living in Ouagadougou. The majority were men (59%), aged 50 years old or less (70%) and living in an urban area (98%; Table 1).
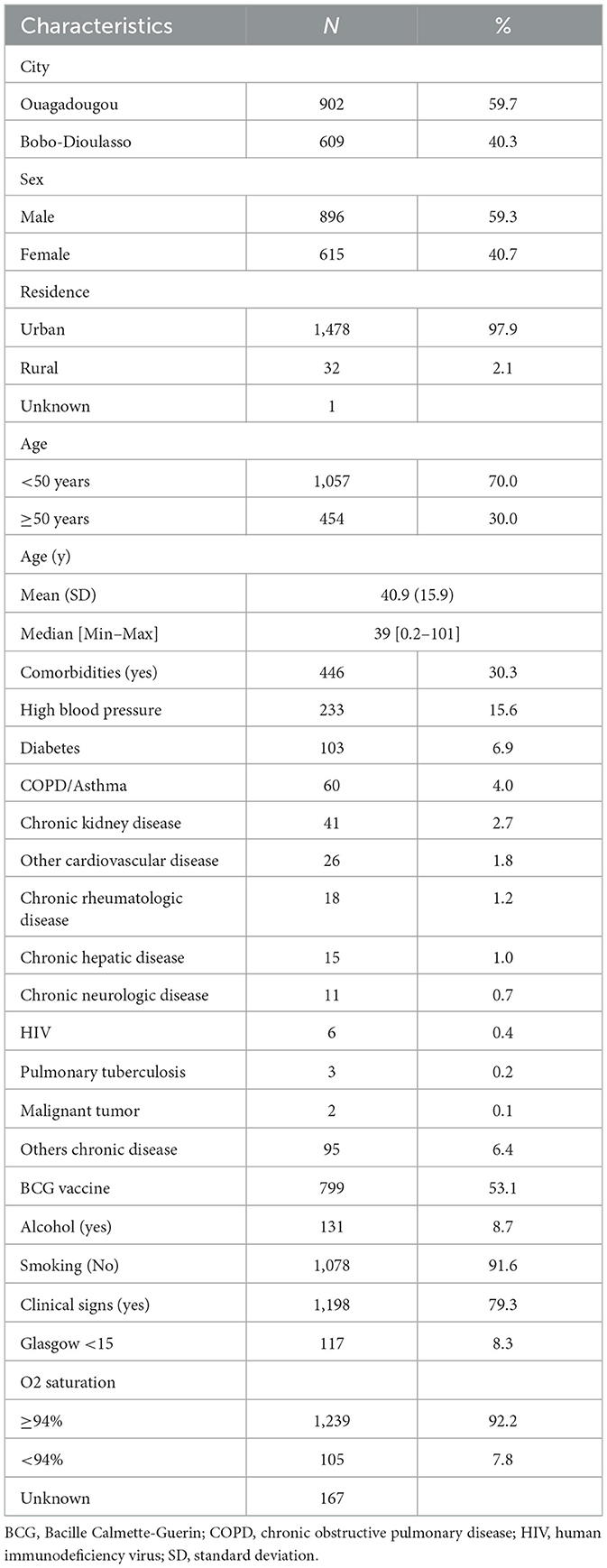
Table 1. Description of baseline characteristics of patients.
Clinical features
The population was relatively in good health overall (87% in good general condition), with few comorbidities (30% had comorbidities) and a generally healthy lifestyle, with few smokers and consumers of alcohol. The most frequent comorbidities were diabetes (7%), HBP (16%) and chronic obstructive pulmonary disease (COPD)/asthma (4%; Table 1).
Nearly 4 out of 5 patients had symptoms on admission. The main symptoms were cough (38.6%), fatigue (38%), fever (35%), headache (32%), body aches (29%) and rhinitis (29%). Only 16% of patients had dyspnea (Figure 1). People aged 50 years and older had more symptoms compared to those aged < 50 years. Symptoms such as dyspnea, cough, fever and fatigue were more likely to persist at discharge in older patients (Figure 2).
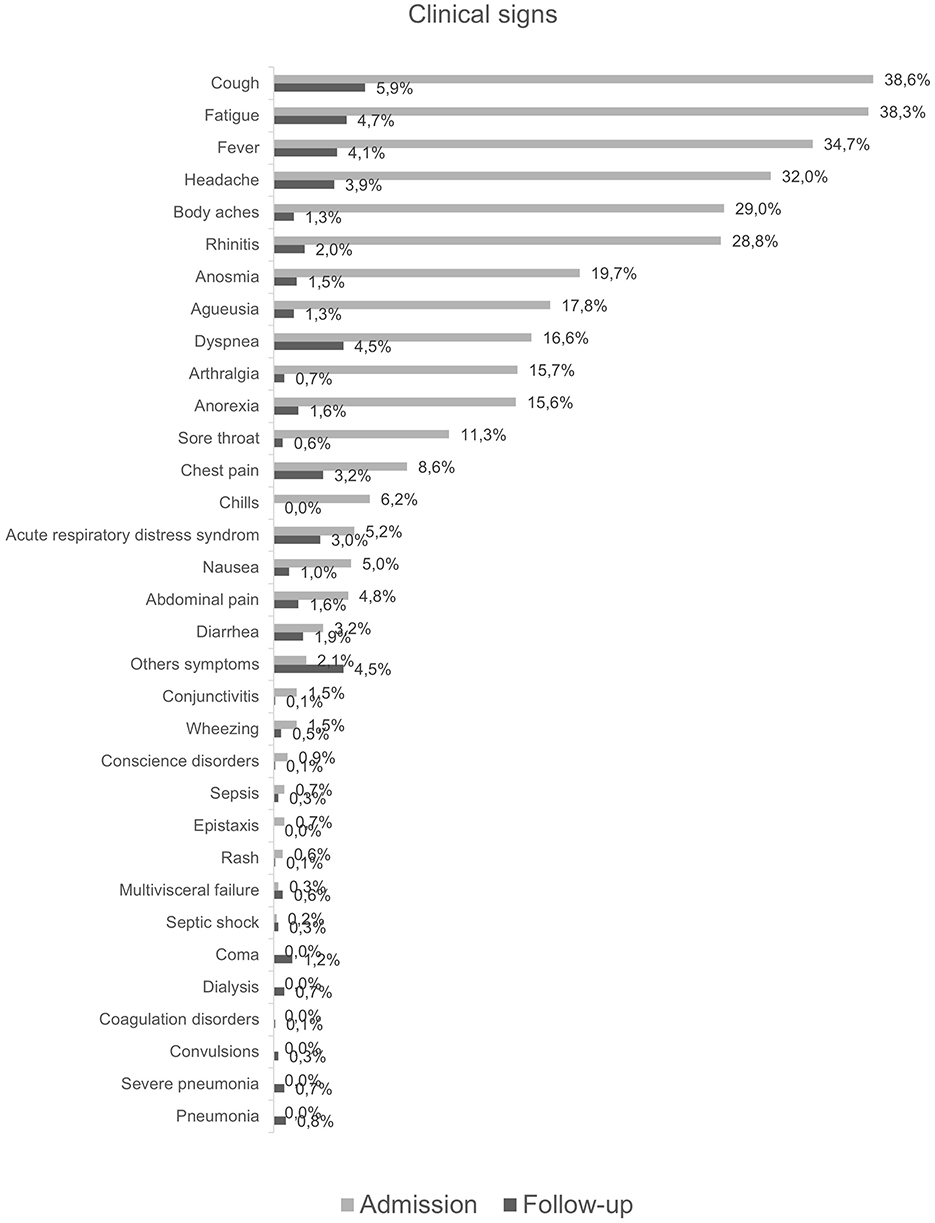
Figure 1. Description of symptoms at admission and during hospitalization.
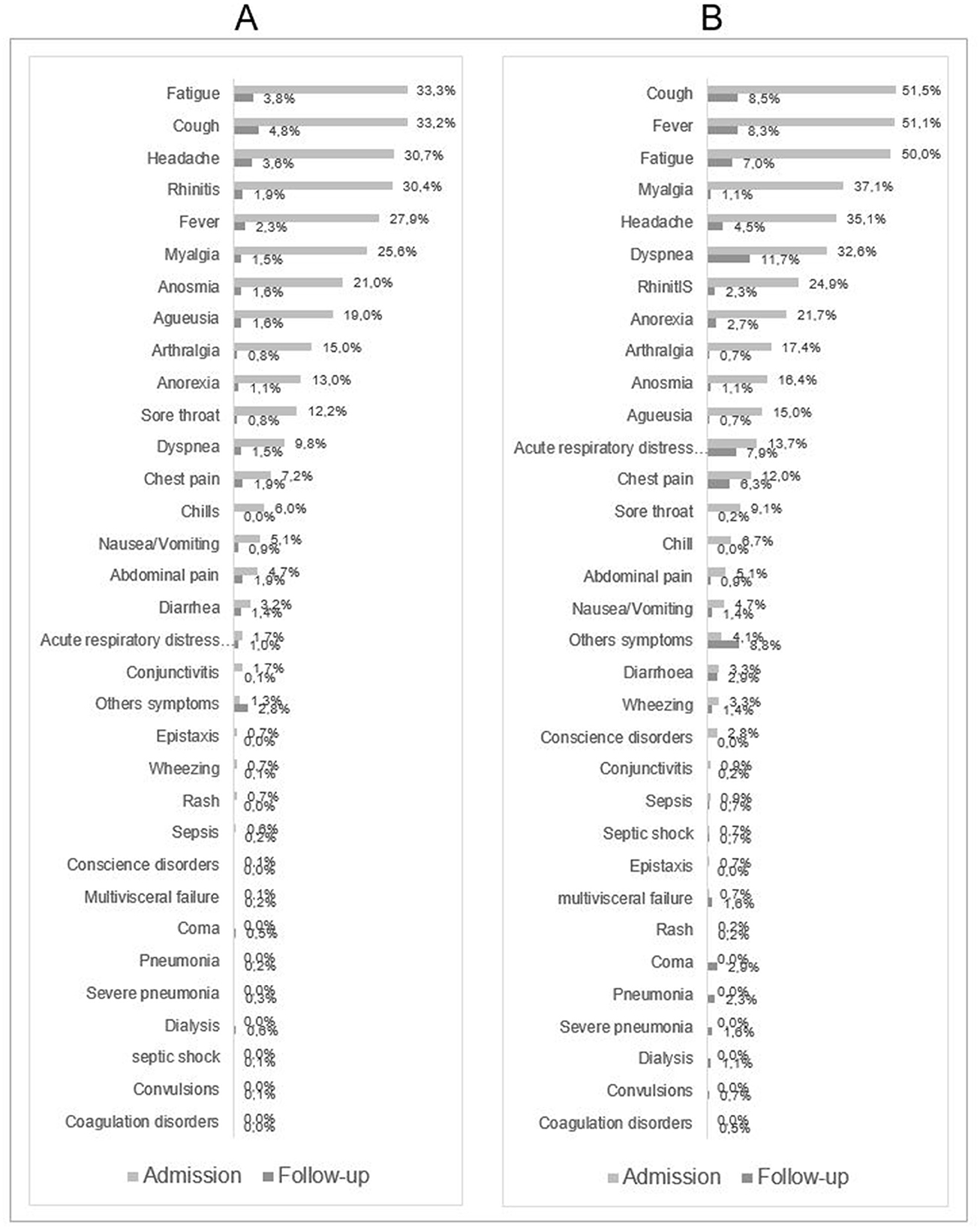
Figure 2. Description of symptoms at admission and during hospitalization for patients aged < 50 years (A) and patients aged 50 years or more (B).
Among younger patients, the most persistent symptom at discharge was cough (?5%) (Figure 2). Four percent of patients had auto medication before attending medical facilities.
Treatment and outcomes
Eighty-six percent of patients received treatment. Among them, 92.9 % had been treated by the combo Azithromycin and hydroxychloroquine, 11.4% had received antibiotherapy other than azithromycin and 12% had symptomatic treatments (paracetamol, etc.). One hundred and thirty-four (9.4%) patients had oxygen therapy and 77 (5.4%) patients had tracheal intubation.
In our study population, 82 (5.7%) patients arrived at the hospital with severe forms, 78 (5.2%) patients had complications during hospitalization, 49 (3.3%) patients died. There was a difference in terms of complications and death according to age (p = 0.001) but no difference was found when comparing men to women (p = 0.001). Overall, 90% of patients recovered without sequelae (Table 2).
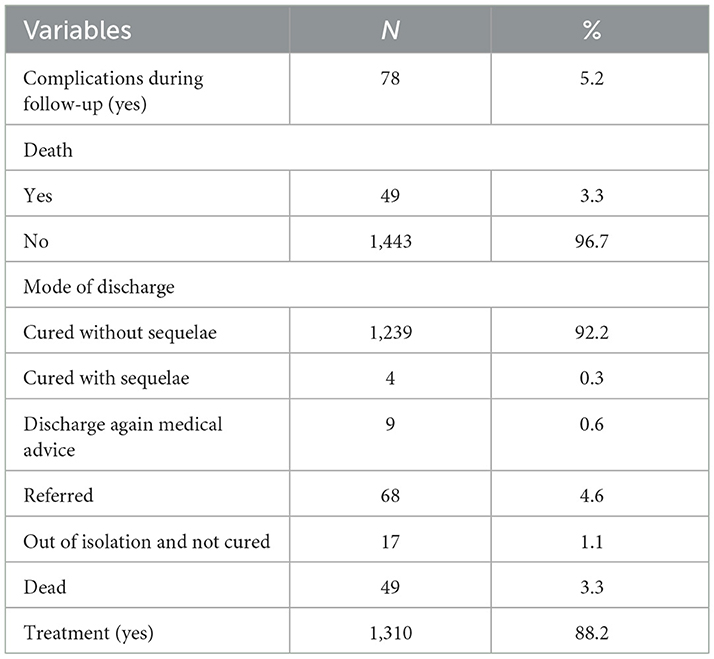
Table 2. Description of outcomes and treatments.
Correlate and predictive factors
Age and residence were both predictors of admission with complications (age ≥ 50yrs; RR [95% CI]: 4.71 [2.56 – 8.66]; rural residence, RR [95% CI]: 2.67 [1.37 – 5.21]) and were also predictive factors associated with the occurrence of complications during hospitalization (age ≥ 50yrs RR [95% CI]: 3.33 [1.24 – 8.98]; rural residence RR [95% CI]: 9.02 [2.34 – 34.79]) (Table 3).
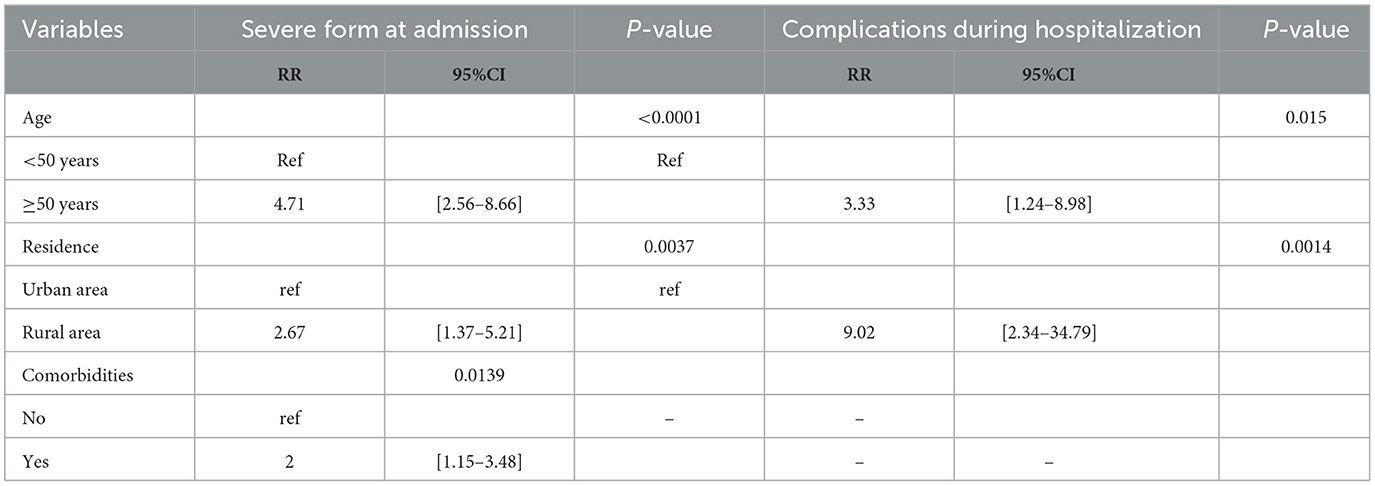
Table 3. Predictive factors of severe form of disease at admission and complications during hospitalization.
Furthermore, comorbidities (RR [95% CI]: 2 [1.15 – 3.48]) were associated with an increased risk of admission with complications (Table 3). Only age (HR [95% CI]:11.81 [3.42 – 40.75]) and the presence of respiratory symptoms at admission (HR [95% CI]: 21.7 [2.75 – 172.08]) were prognostic factors of mortality (Table 3).
Discussion
The aim of this study was to assess the treatment and identify the factors associated with complications (worsening and death) among patients admitted with COVID-19 infection to hospitals in the two major cities of Burkina Faso, namely Ouagadougou and Bobo-Dioulasso.
We found that among people with COVID-19 infection in Burkina-Faso, few (6%) were admitted to hospitals with severe forms, and only 5% had a complication during hospitalization. This result shows that patients managed for COVID-19 in the major cities of Burkina Faso mainly had a mild form of disease. One explanation may be that in our study, the population was young, with a median age of 39 years, and had a relatively healthy lifestyle, with few smokers or alcohol consumers.
The young age of our population may be a protective factor against the development of severe forms of SARS-CoV-2 infection. However, based on the current state of knowledge, people with comorbidities like diabetes or high blood pressure may develop severe forms of COVID-19. In our study, only 16% and 7% had high blood pressure and diabetes respectively.
These results are in line with the findings of other studies in Burkina Faso (10, 17, 18) and Africa (18, 22), reporting mild or moderate forms as the most commonly encountered forms in COVID-19 patients. Nevertheless, data about lifestyle habits were self-reported, and we cannot exclude the possibility that they may be underreported.
The combo azithromycin-hydroxychloroquine (AZ-HCQ) was the main treatment received by COVID-19 patients. At the first breakthrough of COVID-19, researchers around the globe have tested several drugs and AZ-HCQ was one of them. Later through the spread of the COVID-19 disease, its efficacy had become of topic for debate among peers and in the scientific community.
In Burkina Faso, an observational and prospective study (CHLORAZ) (23) set up in order to assess the safety of AZ-HCQ, had found AZ-HCQ to be well tolerated by COVID-19 patients. Later on, others studies (19, 24) had focused on efficacy of AZ-HCQ and had shown no harmful outcomes in COVID-19 patients who took AZ-HCQ.
Although 79% of patients in this study presented symptoms at admission for COVID-19, most (90%) recovered fully without sequelae at discharge. This again suggests that people in Burkina Faso admitted for COVID-19 predominantly had a benign form of disease. This is also support by the low level of intensive care use seen among the patients, with only 8% of participants in this study requiring oxygen therapy. Nevertheless, some symptoms still persist at the time of discharge, particularly in people older than 50 years old.
Concerning factors associated with complications, age was associated with both severe form of disease at admission, and worsening of the disease. People aged 50 years and older had a three- and four-fold increase risk of having a severe form or worsening of the disease respectively, compared to those aged under 50.
Since the pandemic began, age has been clearly identified as a strong factor for severe forms or developing complications in patients with COVID-19 (11, 12). In most studies, people aged 60 years or older are at increased risk of complications due to COVID-19 (6, 12, 16, 25). Our study shows that even before 60 years old, there is already a risk of developing complications due to COVID-19. Age was also significantly associated with the risk of death.
The area of residence was found to be associated with both a severe form, and worsening of the disease, whereby living in a rural area was significantly associated with the likelihood of having a severe form of disease at admission. Health facilities are often far from rural areas, making it difficult for people living in rural areas to have prompt access to healthcare facilities.
Aside from the distance to the healthcare facilities, a fear of out-of-pocket expenses, such as direct costs of treatment and indirect costs for transportation and accommodation, could be one reason why patients in rural areas do not attend health facilities. In addition, most people living in rural areas in Burkina Faso are farmers who live off their crops.
For these people, losing a day's work means a corresponding loss of income, so they only go to hospital as a last resort. This late presentation could at least partially explain the higher proportion of severe forms in those from rural areas. In our study, 16% of patients living in a rural area presented either acute respiratory distress syndrome or sepsis at admission, and people living in rural areas also had a higher risk of poor outcomes.
Comorbidities were significantly associated with patients having severe forms at admission. Diabetes and HBP were identified as being associated with worse outcomes in COVID-19 patients (19, 24). In our study, 30% of patients presented one or more comorbidities, and the most common were HBP (15.6%), diabetes (6.9%), and COPD/asthma (4%). Comorbidity was associated with the occurrence of complications during follow-up in patients with a benign form at admission in univariate analysis, but not in multivariate analysis.
We also looked at the effect of comorbidities individually, mainly high blood pressure, diabetes and COPD/asthma. Both HBP and diabetes were independently associated with worsening in COVID-19 patients by univariate analyses, but this association was not significant in multivariate analysis. These findings on HBP is in line with those of Ouedraogo et al. (20) who found that HBP was an independent factor for ARDS in univariate but not in multivariate analysis.
As for diabetes, our results are contrary to those found by Ouedraogo et al. (20) and Diendéré et al. (10), who respectively reported that diabetes was associated with ARDS and hypoxia in COVID-19 patients. This difference may be due to the time when the study was conducted. Indeed, Ouedraogo et al. (20) and Diendéré et al. (10) conducted their studies during the first wave, at a time when scientific knowledge about the disease was scarce.
Our study included both waves and after the first wave, diabetes was already established as risk factor for worsening of the disease. Thus, during the second wave, people with diabetes were known to be at risk of complications, and may have had more COVID-19 prevention protocols to reduce their risk of acquiring the infection. This is reflected by the proportion of COVID-19 patients with diabetes in these studies, namely 12.4% and 8.4% respectively for Diendéré et al. (10) and Ouedraogo et al. (20) and only 6.9% in our study.
Men were more frequently affected by COVID-19 in this study, with 59% of males in our population. However, gender was not significantly associated with complications or death, contrary to reports from other studies in Africa and around the world, where an association between sex and poor outcomes in COVID-19 patients has been identified (13, 26).
The strengths of this study include the data collection at four hospitals, which ensured a high number of patients and also reduced possible selection bias. Contrary to other studies conducted in Burkina Faso, our study included the city of Bobo-Dioulasso, which is one of the main cities, apart from Ouagadougou, most impacted by COVID-19. This study also has strengths, such as the use of the robust Poisson method (21) to identify predictive factors of worsening given, the low rate of complications in our study population.
However, this study also has some limitations. Although, we tested correlations between variables before including them in the models, we didn't calculate the variance inflation factor (VIF), which could have helped detect multicollinearity in the models and clarified the wide confidence intervals observed. Additionally, the exclusion of patients with complications at admission before performing the second regression model may introduce bias.
But, to mitigate this potential bias, we compared patients with complications at admission to those included in the model to assess whether there were significant differences between the two groups. The populations differed in terms of dyspnea, myalgia, abdominal pain and fatigue but only dyspnea (data not shown) was included in the model as part of the respiratory symptoms.
Furthermore, biological and radiological data were not included in the analysis of predictive factors. The reason be that these data were only available for a limited number of individuals at the hospitals where our data were collected. Burkina Faso is a low-income country where a large proportion of the population are working in the informal sector. Exams such laboratory tests or radiographs come with additional costs for patients, and given the socio-economic conditions, few individuals are able to afford them.
In conclusion, despite these limitations, the study offers valuable insights into the predictors of poor outcomes among COVID-19 patients in Burkina. While most patients had symptoms, the majority of patients in this young study population recovered without sequelae, and the overall proportion of complications was low. Patients were mainly treated with AZ-HCQ. The factors associated with poor outcomes are consistent with those found in the literature, including age, place of residence and comorbidities.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statement
The studies involving humans were approved by National Ethics Committee for health research Ouagadougou Burkina Faso. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
AM: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Writing – original draft. SO: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing. FK: Data curation, Methodology, Project administration, Writing – review & editing. IT: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Writing – review & editing. EO: Data curation, Investigation, Writing – review & editing. AP: Data curation, Investigation, Writing – review & editing. AD: Data curation, Investigation, Writing – review & editing. DK: Data curation, Investigation, Writing – review & editing. HB: Methodology, Writing – review & editing. GS: Data curation, Investigation, Writing – review & editing. AK: Writing – review & editing. TSK: Writing – review & editing. BK: Writing – review & editing. RM: Writing – review & editing. NR: Writing – review & editing. BO: Data curation, Writing – review & editing. OB: Methodology, Writing – review & editing. GP: Methodology, Supervision, Writing – review & editing. HT: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – review & editing. TD-y: Conceptualization, Data curation, Funding acquisition, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project was supported by the ANRS (France REcherche Nord & Sud Sida-hiv-Hépatites) [ANRS-COV13/EMuLCOVID-19]. The funding bodies was not involved in the study design, collection, analysis, and interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We thank ANRS (France REcherche Nord&Sud Sida-hiv-Hépatites) for funding this project and also all the members of the scientific council of this project for their scientific contributions namely: Léon Savadogo, Philippe Van De Perre, Dominique Costagliola, Fernand Bationo, Alice Montoyo, Apolline Sondo and Christine Kafando. We also thanks Fiona Ecarnot, PhD (EA3920, University of Franche-Comté, Besancon, France) for English language editing.
Conflict of interest
AP was employed by the Sourô Sanou University Hospital, Bobo Dioulasso, Burkina Faso at the Department of Infectious Diseases.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Verity R, Okell LC, Dorigatti I, Winskill P, Whittaker C, Imai N, et al. Estimates of the severity of coronavirus disease 2019: a model-based analysis. Lancet Infect Dis. (2020) 20:669–77. doi: 10.1016/S1473-3099(20)30243-7
2. El-Sadr WM, Justman J. Africa in the path of COVID-19. N Engl J Med. (2020). 383:e11 doi: 10.1056/NEJMp2008193
3. Cabore JW, Karamagi HC, Kipruto H, Asamani JA, Droti B, Seydi ABW, et al. The potential effects of widespread community transmission of SARS-CoV-2 infection in the World Health Organization African Region: a predictive model. BMJ Glob Health. (2020) 5:e002647. doi: 10.1136/bmjgh-2020-002647
4. Sze S, Pan D, Nevill CR, Gray LJ, Martin CA, Nazareth J, et al. Ethnicity and clinical outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. (2020) 29:100630. doi: 10.1016/j.eclinm.2020.100630
5. Sagna T, Ouedraogo P, Traore L, Obiri-Yeboah D, Yonli A, Tapsoba A, et al. Enigma of the high prevalence of anti-SARS-CoV-2 antibodies in HIV-positive people with no symptoms of COVID-19 in Burkina Faso. J Public Health Afr. (2022) 13.1778. doi: 10.4081/jphia.2022.1778
6. Kirenga BJ, Byakika-Kibwika P. Excess COVID-19 mortality among critically ill patients in Africa. Lancet. (2021) 397:1860–1. doi: 10.1016/S0140-6736(21)00576-6
7. Olumade TJ, Uzairue LI. Clinical characteristics of 4499 COVID-19 patients in Africa: a meta-analysis. J Med Virol. (2021) 93:3055–61. doi: 10.1002/jmv.26848
8. Coronavirus (COVID-19). WHO | Regional Office for Africa. Available online at: https://www.afro.who.int/health-topics/coronavirus-covid-19 (Accessed February 15, 2023).
9. World Health Organization. Available online at: https://www.who.int/countries/bfa/ (Accessed April 10, 2025).
10. Diendéré EA, Sondo KA, Ouédraogo AR, Dahourou DL, Cissé K, Sawadogo A, et al. Predictors of severe hypoxemia among COVID-19 patients in Burkina Faso (West Africa): findings from hospital based cross-sectional study. Int J Infect Dis. (2021) 108:289–95. doi: 10.1016/j.ijid.2021.04.007
11. Sensusiati AD, Amin M, Nasronudin N, Rosyid AN, Ramadhan NA, Lathifah R, et al. Age, neutrophil lymphocyte ratio, and radiographic assessment of the quantity of lung edema (RALE) score to predict in-hospital mortality in COVID-19 patients: a retrospective study. F1000Res. (2021) 9:1286. doi: 10.12688/f1000research.26723.2
12. Biswas M, Rahaman S, Biswas TK, Haque Z, Ibrahim B. Association of sex, age, and comorbidities with mortality in COVID-19 patients: a systematic review and meta-analysis. Intervirology. (2021) 64:36–47. doi: 10.1159/000512592
13. Kragholm K, Andersen MP, Gerds TA, Butt JH, Østergaard L, Polcwiartek C, et al. Association between male sex and outcomes of coronavirus disease 2019 (COVID-19)-a Danish Nationwide, Register-based Study. Clin Infect Dis. (2021) 73:e4025-e4030. doi: 10.1093/cid/ciaa924
14. Thoreau B, Galland J, Delrue M, Neuwirth M, Stepanian A, Chauvin A, et al. D-dimer level and neutrophils count as predictive and prognostic factors of pulmonary embolism in severe non-ICU COVID-19 patients. Viruses. (2021) 13:758. doi: 10.3390/v13050758
15. Jang JG, Hur J, Choi EY, Hong KS, Lee W, Ahn JH. Prognostic factors for severe coronavirus disease 2019 in Daegu, Korea. J Korean Med Sci. (2020) 35:e209. doi: 10.3346/jkms.2020.35.e209
16. Nguimkeu P, Tadadjeu S. Why is the number of COVID-19 cases lower than expected in Sub-Saharan Africa? A cross-sectional analysis of the role of demographic and geographic factors. World Dev. (2021) 138:105251. doi: 10.1016/j.worlddev.2020.105251
17. Jaspard M, Sow MS, Juchet S, Dienderé E, Serra B, Kojan R, et al. Clinical presentation, outcomes and factors associated with mortality: a prospective study from three COVID-19 referral care centres in West Africa. Int J Infect Dis. (2021) 108:45–52. doi: 10.1016/j.ijid.2021.05.024
18. Ouédraogo AR, Bougma G, Baguiya A, Sawadogo A, Kaboré PR, Minougou CJ, et al. Facteurs associés à la survenue de la détresse respiratoire aiguë et au décès chez des patients atteints de COVID-19 au Burkina Faso. Rev Mal Respir. (2021) 38:240–8. doi: 10.1016/j.rmr.2021.02.001
19. Rouamba T, Ouédraogo E, Barry H, Yaméogo NV, Sondo A, Boly R, et al. Assessment of recovery time, worsening, and death among inpatients and outpatients with COVID-19, treated with hydroxychloroquine or chloroquine plus azithromycin combination in Burkina Faso. Int J Infect Dis. (2022) 118:224–9. doi: 10.1016/j.ijid.2022.02.034
20. Traoré IT, Ouedraogo S, Kania D, Kaboré FN, Konaté B, Médah R, et al. COVID-19 epidemiological, sociological and anthropological investigation: study protocol for a multidisciplinary mixed methods research in Burkina Faso. BMC Infect Dis. (2021) 21:896. doi: 10.1186/s12879-021-06543-4
21. Chen W, Qian L, Shi J, Franklin M. Comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med Res Methodol. (2018) 18:63. doi: 10.1186/s12874-018-0519-5
22. Fouda Mbarga N, Epee E, Mbarga M, Ouamba P, Nanda H, Nkengni A, et al. Clinical profile and factors associated with COVID-19 in Yaounde, Cameroon: a prospective cohort study. PLoS ONE. (2021) 16:e0251504. doi: 10.1371/journal.pone.0251504
23. Rouamba T, Barry H, Ouédraogo E, Tahita MC, Yaméogo NV, Poda A, et al. Safety of chloroquine or hydroxychloroquine plus azithromycin for the treatment of COVID-19 patients in Burkina Faso: an Observational Prospective Cohort Study. Ther Clin Risk Manag. (2021) 17:1187–98. doi: 10.2147/TCRM.S330813
24. Baguiya A, Poda A, Cissé K, Sondo AK, Ouedraogo B et al. Effect of hydroxychloroquine or chloroquine and azithromycin on COVID-19 patients' recovery and mortality: evidence from a hospital based retrospective cohort study conducted in Burkina Faso. J Infect Dis Epidemiol. (2021) 7:192. doi: 10.23937/2474-3658/1510192
25. Sila T, Suriyaamorn W, Toh C, Rajborirug S, Surasombatpattana S, Thongsuksai P et al. Factors associated with the worsening of COVID-19 symptoms among cohorts in community- or home-isolation care in southern Thailand. Front. Public Health, (2024) 12:1350304. doi: 10.3389/fpubh.2024.1350304
Keywords: age, comorbidity, COVID-19, complications, treatment
Citation: Mamguem Kamga A, Ouédraogo S, Kaboré FN, Traoré IT, Ouédraogo E, Poda A, Diendéré AE, Kania D, Badolo H, Sanou G, Koné A, Kagoné TS, Konaté B, Médah R, Rekeneire Nd, Ouédraogo B, Billa O, Paradis G, Tinto H and Dabakuyo-yonli TS (2025) Characteristics, management and factors associated with poor outcomes in COVID-19 patients in Burkina Faso: insights from a 2021 large-scale ambispective study. Front. Public Health 13:1542024. doi: 10.3389/fpubh.2025.1542024
Received: 09 December 2024; Accepted: 13 June 2025;
Published: 10 July 2025.
Edited by:
Hem Chandra Jha, Indian Institute of Technology Indore, IndiaReviewed by:
Sulaimon Adigun Muse, Lagos State University of Education LASUED, NigeriaEustachio Cuscianna, University of Bari Aldo Moro, Italy
Jacques L. Tamuzi, Stellenbosch University, South Africa
Copyright © 2025 Mamguem Kamga, Ouédraogo, Kaboré, Traoré, Ouédraogo, Poda, Diendéré, Kania, Badolo, Sanou, Koné, Kagoné, Konaté, Médah, Rekeneire, Ouédraogo, Billa, Paradis, Tinto and Dabakuyo-yonli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ariane Mamguem Kamga, YXJpYW5lLm1hbWd1ZW1rYW1nYUB5YWhvby5jb20=