 Luís Antônio Gilberti Panucci1,2
Luís Antônio Gilberti Panucci1,2 Luiza Sant’Anna Pinheiro1
Luiza Sant’Anna Pinheiro1 João Pedro Teixeira Roque1
João Pedro Teixeira Roque1 Edilson Ferreira Flores3Rogério Giuffrida2,4
Edilson Ferreira Flores3Rogério Giuffrida2,4 Luiz Euribel Prestes-Carneiro2,3*
Luiz Euribel Prestes-Carneiro2,3*- 1Hospital Estadual de Presidente Prudente, Presidente Prudente, Brazil
- 2Faculty of Medicine, University of Western São Paulo, Presidente Prudente, Brazil
- 3Department of Statistics, Faculty of Science and Technology, São Paulo State University, Presidente Prudente, Brazil
- 4Postgraduate Program in Health Sciences, University of Western São Paulo, Presidente Prudente, Brazil
Introduction: Vaccination coverage among pregnant women in Brazil remains poorly documented, particularly in low-resource settings. This study aimed to (1) assess the completeness of vaccine records on prenatal cards and (2) evaluate pregnant women’s knowledge of vaccines recommended by the Brazilian National Immunization Program (NIP).
Methods: : A cross-sectional study was conducted at the Hospital Estadual de Presidente Prudente (HEPP), a public secondary hospital in São Paulo, Brazil, between August 2022 and April 2023. The study population comprised 1,130 women admitted for delivery, of whom 541 (47.9%) had prenatal cards available for review. Postpartum, data from the prenatal cards were extracted, and participants completed a structured questionnaire to assess their vaccine knowledge. Sociodemographic data were obtained from electronic medical records. Univariate analyses were performed using Pearson’s Chi-Squared or Fisher’s Exact Test. Only 11.2% of the reviewed prenatal cards documented complete vaccination with all four NIP-recommended vaccines, while 31% contained no vaccine records at all. The tetanus, diphtheria, and acellular pertussis (Tdap) vaccine had the highest documented coverage (61%). The mean age of participants was 27.1 ± 0.3 years. Although most participants (91.1%) believed they had been vaccinated during pregnancy, only 61.5% could specify which vaccines they had received. No significant association was found between sociodemographic factors and the completeness of vaccine documentation. The low level of vaccination documentation and the critical knowledge gaps identified in this study highlight deficiencies in the quality of prenatal care within Brazil’s Unified Health System (SUS) in the Western region of São Paulo state. Addressing these issues requires concerted efforts to improve healthcare provider training, strengthen public health education, and standardize documentation practices.
1 Introduction
Vaccination during pregnancy is essential for protecting both mothers and newborns from infectious diseases (1, 2). Newborns depend on maternal antibodies, transferred transplacentally and through breastfeeding, to acquire critical immunity during early infancy (3). In Brazil, the National Immunization Program (NIP) oversees population-wide vaccination efforts, prioritizing pregnant women and children (4, 5). The NIP recommends four key vaccines during pregnancy: tetanus, diphtheria, and acellular pertussis (Tdap), hepatitis B, influenza, and COVID-19 (6).
Since 1988, the prenatal card has served as a mandatory health record in Brazil’s public and private healthcare systems, documenting obstetric care, test results, and vaccinations (6, 7). This tool is critical for recording essential health information, including vaccination status, which guides healthcare providers during childbirth (8). Despite its importance, studies using prenatal card data have revealed systemic issues, such as incomplete documentation and inconsistent record-keeping within the Unified Health System (SUS) (4, 9). Although the Brazilian Ministry of Health updated the prenatal card in 2022 to improve usability (7), challenges persist in adequately training healthcare teams to maintain accurate records (4, 9). The COVID-19 pandemic further exacerbated these issues, as disruptions in healthcare services during 2020–2021 led to declines in vaccination coverage and increased risks of preventable diseases (10).
Globally, education is a key determinant of health outcomes, influencing indicators such as infant mortality, vaccination rates, and life expectancy (11). Even in high-income countries, lower levels of educational attainment are associated with reduced health literacy and limited healthcare access (12). Nevertheless, the impact of maternal education on vaccination adherence remains underexplored, particularly in low-resource settings (13, 14).
In Brazil, despite NIP efforts to achieve 90% coverage among pregnant women, national Tdap coverage reached only 87.9% by 2024 (15, 16). Clinical observations by the authors at the Hospital Estadual de Presidente Prudente (HEPP) revealed a notable decline in the registration of vaccinations on prenatal cards during the COVID-19 pandemic. This led to the hypothesis that, in the western region of São Paulo state, primary care professionals may be insufficiently trained to record vaccination data accurately, resulting in pregnant women receiving inadequate information about the importance of immunization. Therefore, this study aimed to (1) assess the completeness of vaccine records on prenatal cards and (2) evaluate pregnant women’s knowledge of vaccines recommended by the NIP.
2 Methodology
2.1 Study area and design
This cross-sectional study was conducted in the western region of São Paulo, one of the state’s 18 Regional Health Care Networks (RHCN) (17). This region comprises 45 municipalities with a total population of approximately 753,000 (18). The study was set at the Hospital Estadual de Presidente Prudente (HEPP), a tertiary public hospital that serves as a regional referral center for high-risk pregnancies within Brazil’s Unified Health System (SUS).
2.2 Data collection from pre-natal cards and structured questionnaire
The study was conducted between August 1, 2022, and April 30, 2023. Women admitted for delivery at HEPP were considered for inclusion. Upon admission, sociodemographic data—including municipality of residence, educational level, marital status, and occupation—were obtained from the hospital’s electronic records.
During the immediate postpartum period, an obstetrician invited eligible women to participate. For those who provided informed consent, two data collection procedures were performed. First, the pages of the participant’s prenatal card containing identification and vaccination records were photographed, and the data were transcribed into a digital spreadsheet. Second, the same obstetrician administered a structured questionnaire adapted from validated instruments (19–21). The questionnaire included items assessing participants’ awareness of maternal vaccines, the perceived adequacy of the information they had received, and their understanding of maternal antibody transfer.
2.3 Association of epidemiological variables and dTpa, HBV, influenza and COVID-19
The primary association examined was between the registration of the tetanus, diphtheria, and acellular pertussis (Tdap) vaccine on prenatal cards and maternal education level. The Tdap vaccine is a key indicator used by the Brazilian Ministry of Health to monitor vaccination in vulnerable groups, including pregnant women (16). Maternal education was categorized into two groups based on data from electronic medical records: higher education (completed high school or a complete/incomplete university degree), depicted in white in Figure 1; and lower education (incomplete high school or only elementary education), depicted in blue in Figure 1.
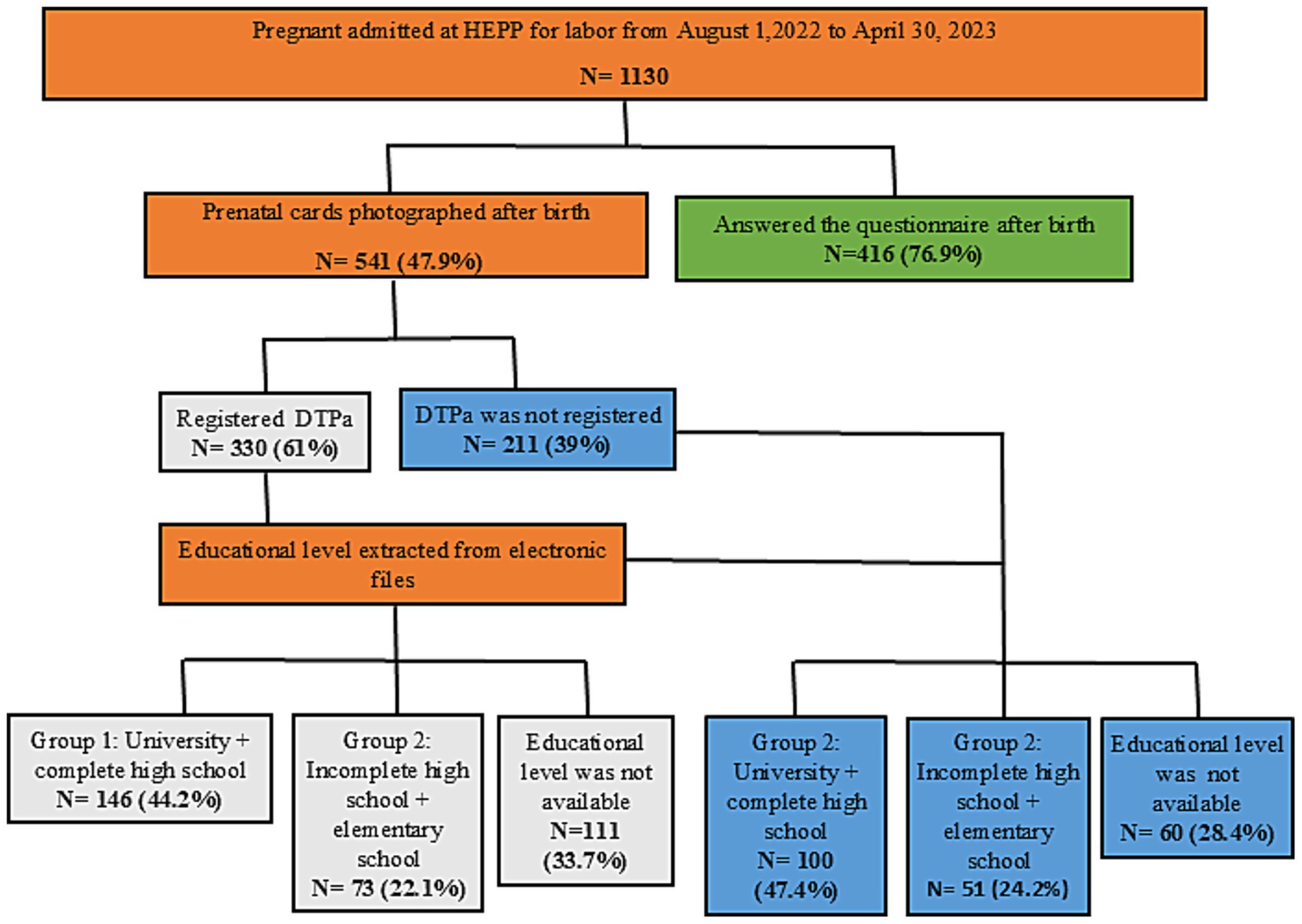
Figure 1. Flow chart illustrating the study design for pregnant women admitted for labor at HEPP. Colors indicate the different maternal education groups: Group 1 (white) represents higher education, defined as having a university degree (complete or incomplete) or having completed high school; Group 2 (blue) represents lower education, defined as having incomplete high school or only elementary education. dTpa, acellular diphtheria-tetanus-pertussis.
The secondary associations examined were between the registration of the other NIP-recommended vaccines (hepatitis B, influenza, and COVID-19) and other epidemiological variables (age, race, marital status, and occupation). Data for all variables were extracted from electronic records. Records with incomplete or inconsistent data were excluded from the corresponding analyses.
2.4 Statistical analysis
All statistical analyses were performed using R software (R Core Team, 2024). Continuous variables, such as age, were reported as mean ± SEM, while categorical variables were presented as frequencies and percentages (%). Statistical significance for all tests was defined as a p-value < 0.05.
The association between maternal education and Tdap registration was assessed using the chi-square test with Yates’ correction, and odds ratios (OR) with 95% confidence intervals (CI) were calculated. For the secondary analyses, associations between other vaccine registrations and epidemiological variables were assessed using Pearson’s Chi-Squared Test or Fisher’s Exact Test. Corresponding odds ratios and 95% confidence intervals were also calculated for these factors.
3 Results
3.1 Profile of vaccination coverage documented on prenatal cards
During the study period, 1,130 women were admitted for delivery at HEPP. Among these, prenatal cards were available for review for 541 women (47.9%), who constituted the study sample (Figure 1).
Of the reviewed cards, complete vaccination (documentation of all four NIP-recommended vaccines) was recorded on only 61 cards (11.2%). A partial record of three vaccines was found on 203 cards (37.5%), two vaccines on 86 cards (15.8%), and a single vaccine on 23 cards (4.2%). Notably, 168 prenatal cards (31.0%) contained no vaccination records whatsoever (Figure 2).
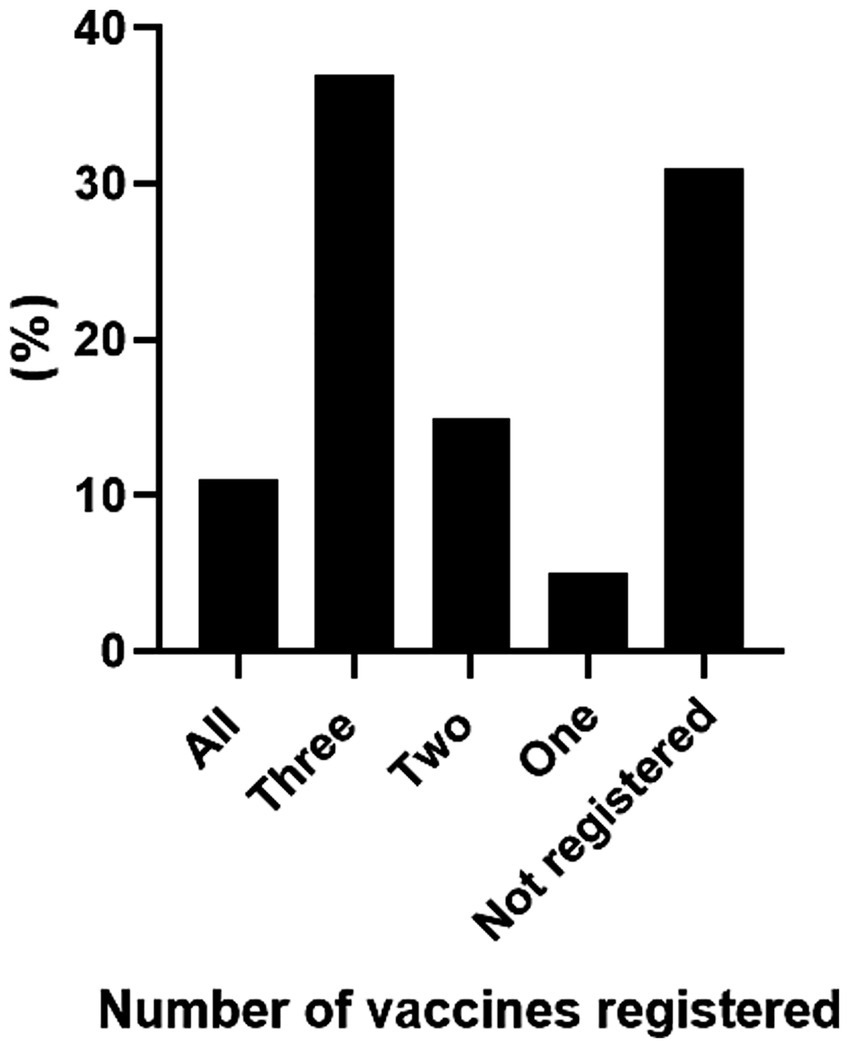
Figure 2. Percentage of vaccines registered in the prenatal cards. Prenatal cards of pregnant women admitted for labor at HEPP. The columns represent the number of vaccines registered, with the final column indicating cases where no vaccination was recorded, from August 2022 to April 2023.
The tetanus, diphtheria, and acellular pertussis (Tdap) vaccine had the highest documented coverage, appearing on 330 cards (61.0%), whereas the COVID-19 vaccine had the lowest, with only 84 records (15.5%) (Figure 3). The most common two-vaccine combination was Tdap and hepatitis B (n = 285). Among women with three vaccines recorded, the most frequent combination was Tdap, hepatitis B, and influenza (n = 248).
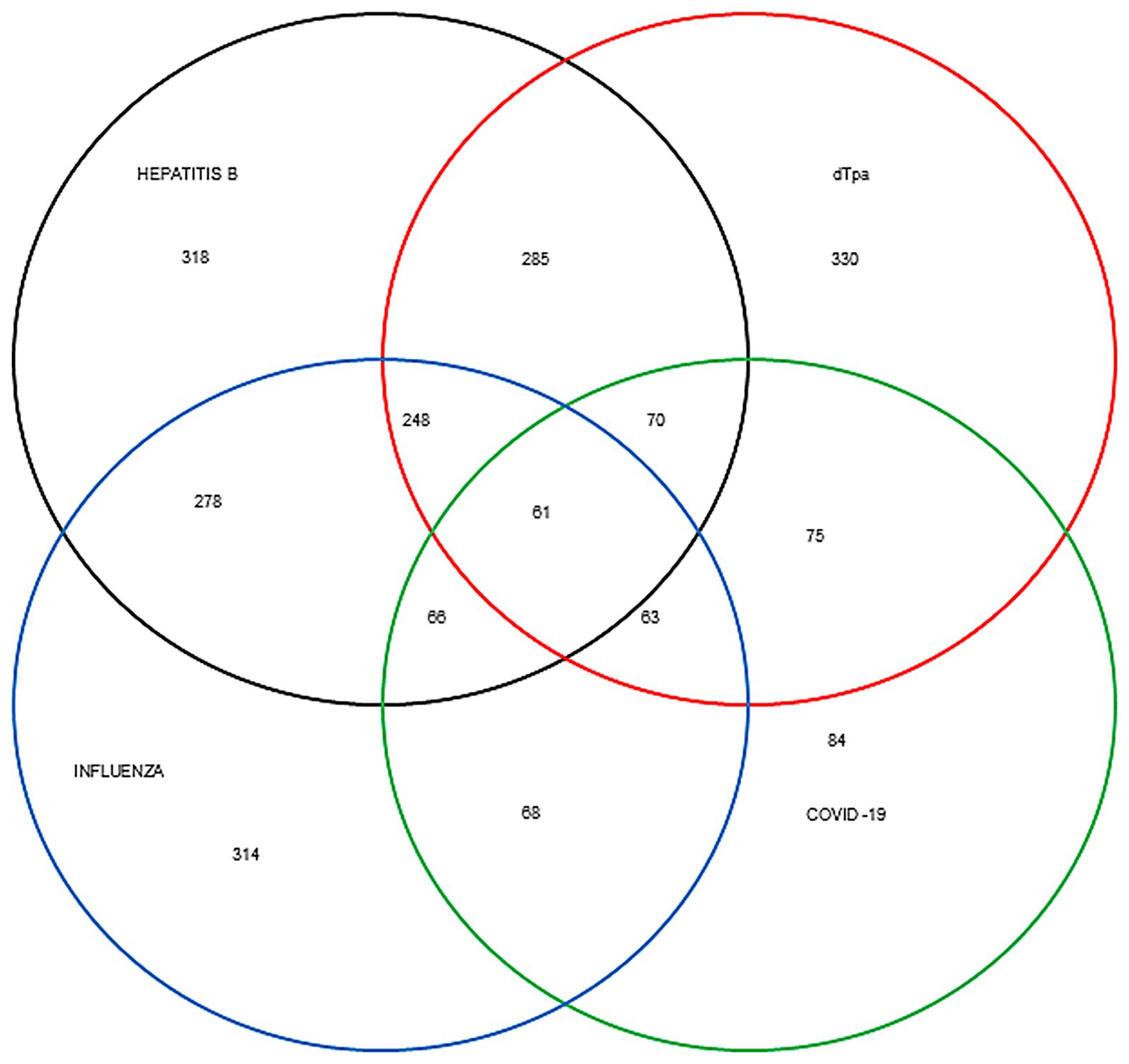
Figure 3. Venn diagram providing a schematic representation of registered vaccines. The proportion of pregnant women who received 2, 3, or 4 vaccines, as registered on prenatal cards from August 2022 to April 2023. dTpa, acellular diphtheria-tetanus-pertussis.
The mean age of the participants for whom data was available was 27.1 ± 0.3 years (95% CI, 26.4–27.7, range, 14–50 years, n = 431). The largest proportion of participants (20.8%) belonged to the 26–30-year age group, while adolescents (14–17 years) constituted 4.9% of the sample (Figure 4).
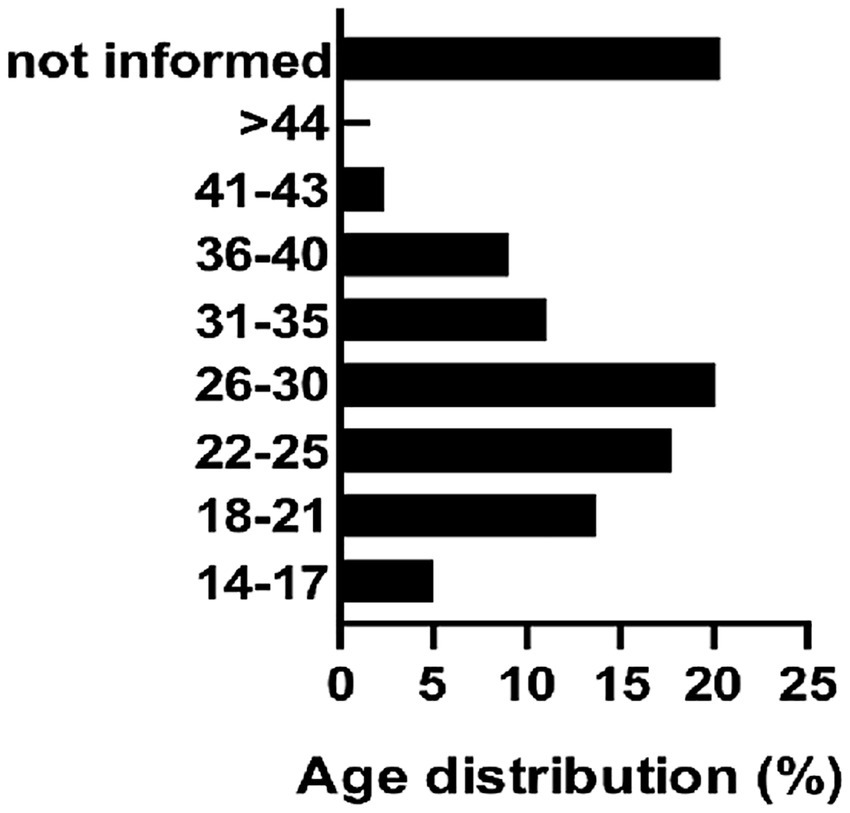
Figure 4. Percent of age distribution of pregnant women. Age was registered in the Prenatal Cards of Women Admitted for Labor at HEPP (August 2022–April 2023). Columns represent different age groups.
3.2 Knowledge regarding NIP-recommended vaccines during pregnancy
Of the 541 women in the initial sample, 416 (76.9%) completed the structured questionnaire (Figure 1). The survey’s structure and the knowledge domains it assessed are illustrated in Figure 5.
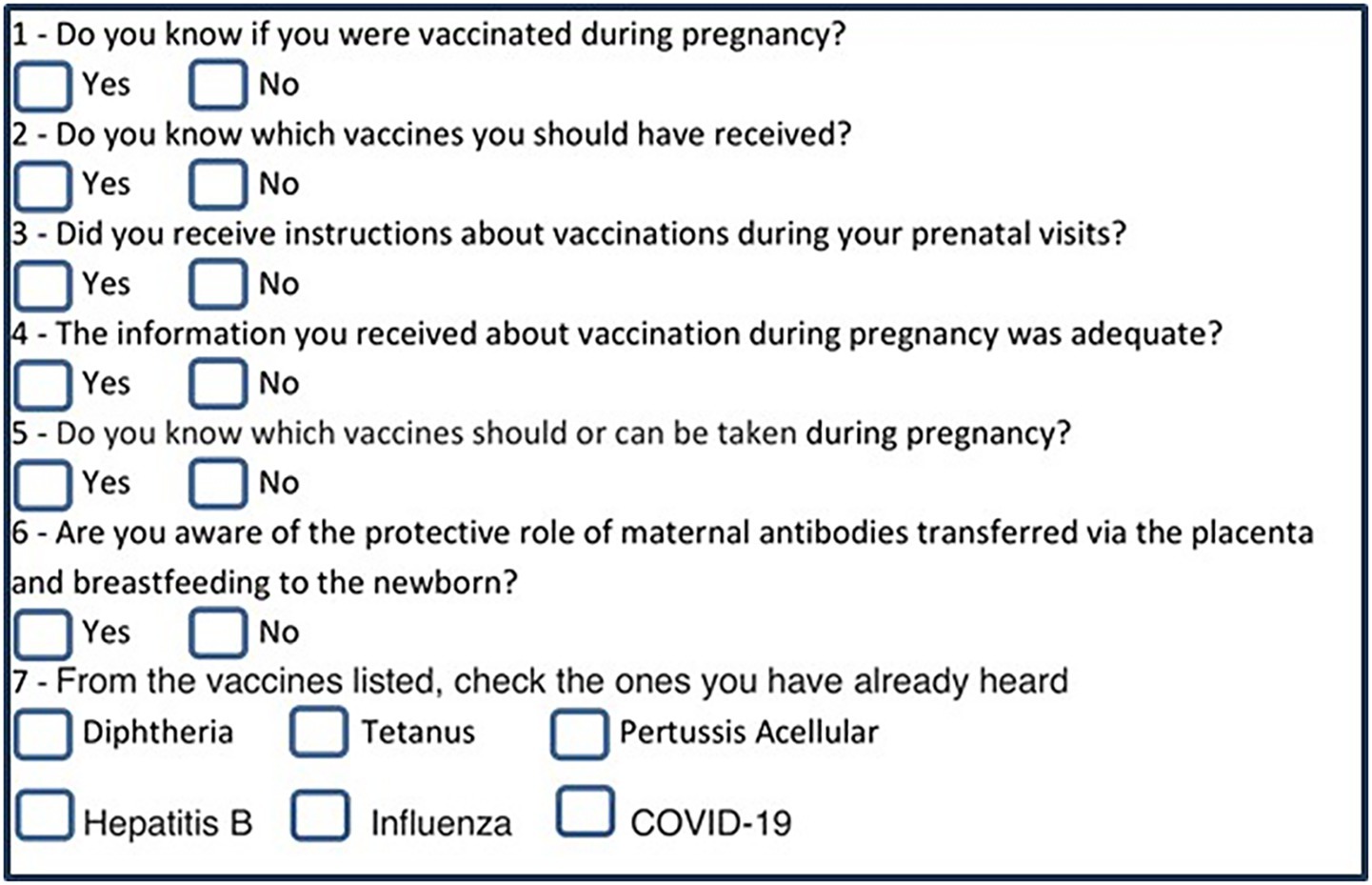
Figure 5. Survey questions assessing the knowledge of vaccination. The structured questionnaire was applied among patients admitted for labor at HEPP (August 2022–April 2023).
The findings on vaccination knowledge are presented in Table 1. While a high proportion of participants (91.1%) knew they had been vaccinated during their pregnancy, only 61.5% could specify which vaccines they had received. Most women (80.8%) reported receiving some instruction about vaccination from healthcare providers; however, only 42.5% considered this information adequate. Furthermore, a substantial number of participants (74.0%) were unaware of the specific vaccines they were eligible to receive during pregnancy. Regarding the protective role of maternal antibodies, 62.0% of respondents indicated awareness.
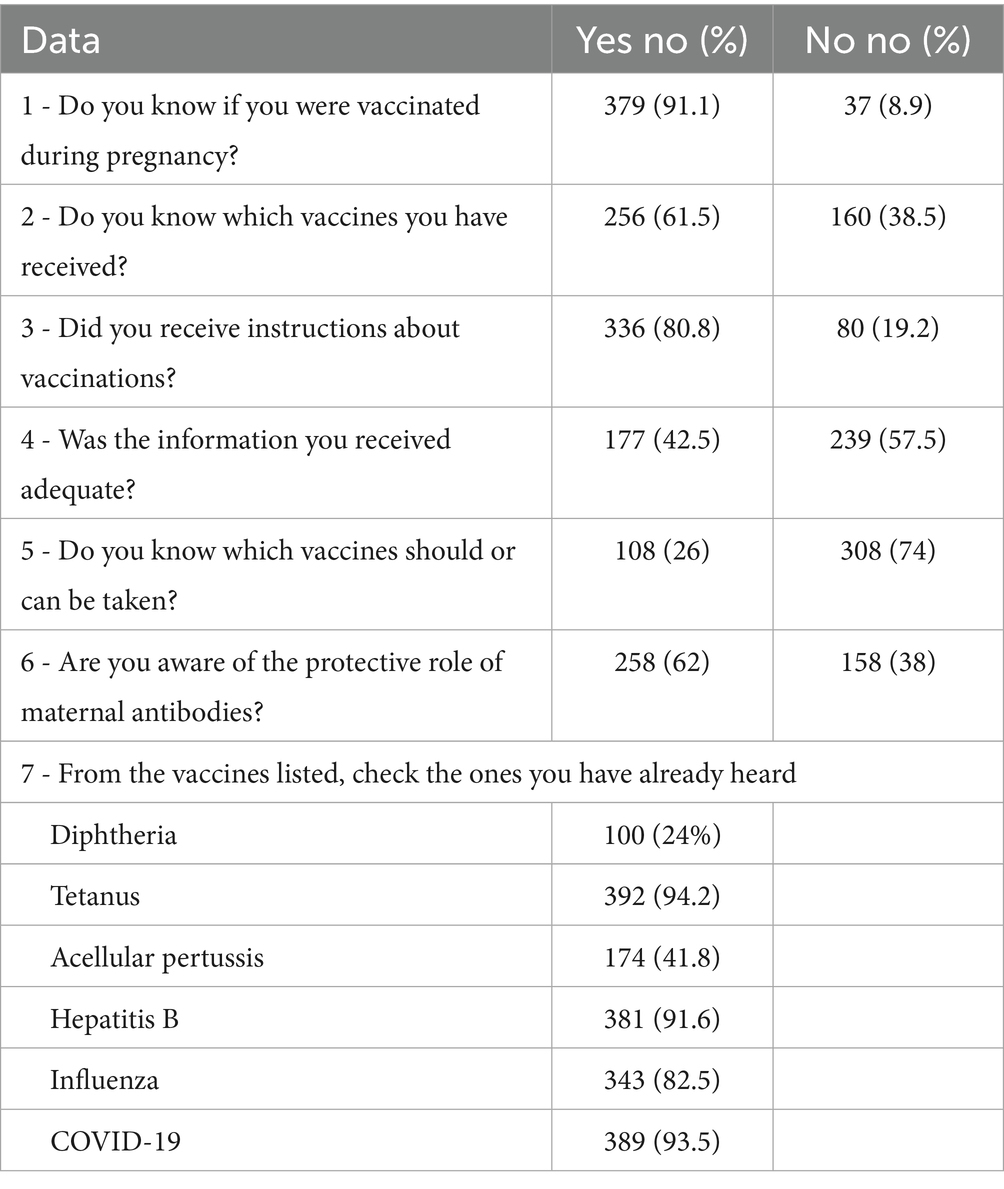
Table 1. Data regarding vaccination knowledge of 416 pregnant women admitted for labor at HEPP (August 2022–April 2023).
In terms of name recognition for specific vaccine-preventable diseases, participants were most familiar with tetanus (94.2%), followed by COVID-19 (93.5%) and hepatitis B (91.6%). Diphtheria was the least recognized disease (Table 1).
3.3 Association of epidemiological variables and dTpa, HBV, influenza and COVID-19 vaccination
The primary analysis focused on the association between maternal education and Tdap vaccine registration among the 541 participants with available prenatal cards. Overall, Tdap vaccination was recorded on 61.0% of the cards and was absent from 39.0% (Figure 1). Among participants with a Tdap record, 44.2% had a higher educational level and 22.1% had a lower educational level; data on education was missing for the remaining 33.7%. Among those without a Tdap record, 47.4% had a higher educational level and 24.2% had a lower educational level, with data missing for 28.4%.
The proportion of Tdap registration was comparable between educational levels: 59.3% of the higher education group had a vaccine record, versus 58.9% of the lower education group. A chi-square test confirmed that there was no statistically significant association between maternal education and Tdap registration (χ2 = 0.008, p = 0.93). Furthermore, logistic regression analysis confirmed the absence of a significant link (OR = 1.03; 95% CI: 0.64–1.67).
Finally, a univariate analysis found no significant association between the registration of any of the four NIP-recommended vaccines (Tdap, hepatitis B, influenza, and COVID-19) and other epidemiological variables, including maternal age, race, marital status, and occupation (Table 2).
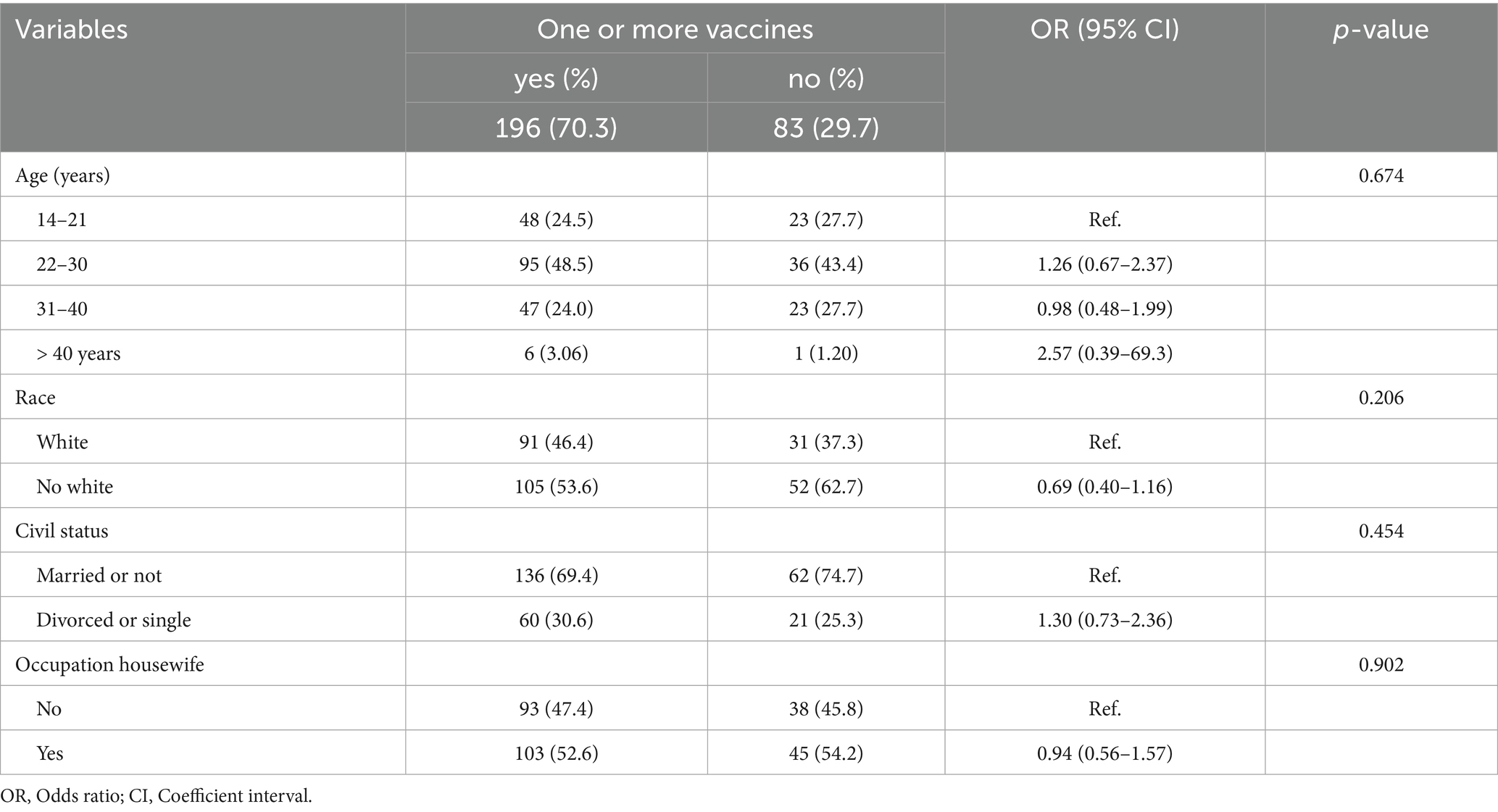
Table 2. Association of one or more vaccines registered in prenatal cards with epidemiological characteristics of pregnant women admitted for labor (N = 279) in HEPP, univariate analysis.
4 Discussion
This study reveals critical gaps in both vaccination documentation and knowledge among pregnant women in the western region of São Paulo. A key finding was that only 11.2% of prenatal cards documented all four NIP-recommended vaccines, while an alarming 31% contained no vaccination records at all. Furthermore, while most participants knew they had been vaccinated, just over 60% could specify which vaccines they had received, and less than half considered the information provided by healthcare professionals to be adequate. Together, these findings underscore systemic challenges in the quality of prenatal care and the accuracy of health records within the SUS.
The low rate of complete vaccine registration (11.2%) observed in this study is a significant concern. This issue was first noted clinically by the authors at HEPP during the COVID-19 pandemic and appears to have persisted. Several factors may explain these poor documentation rates. On the provider and system side, potential factors include a lack of awareness among healthcare professionals regarding current vaccine recommendations and failures at primary care centers to verify and transcribe all necessary information onto the prenatal card (22). The specific context of the western region of São Paulo, which comprises many small municipalities, may also play a role, as healthcare professionals in these areas may not be sufficiently prepared to provide comprehensive counseling on maternal immunization (17).
On the patient side, additional factors may contribute, including concerns about vaccine safety for the mother or newborn, apprehension about side effects, doubts regarding efficacy, and the proliferation of misinformation (22). Fears of contracting COVID-19 at healthcare facilities, especially during 2020–2021, likely also contributed to decreased engagement with routine health services, including vaccination (10).
In Brazil, the health-seeking behaviors of pregnant women are aimed at safeguarding their own health and that of their babies. These behaviors, which include attending prenatal care, seeking help for complications, and preparing for delivery, are shaped by determinants such as education, socioeconomic status, cultural beliefs, and knowledge of pregnancy’s danger signs. However, pregnant women face significant challenges, including poor access to care, prevalent misinformation, and social inequalities, even though prenatal care is a public health priority (5, 8, 9).
Trust in the public healthcare system (SUS) varies greatly across the country’s diverse regions. This trust is often influenced by socioeconomic inequality, educational levels, a lack of effective guidance from providers, and potential discrimination. For instance, in regions like the Northeast and the Amazon, which are often characterized by high poverty rates, low educational attainment, and significant geographical barriers to healthcare, trust in the system can be particularly low. Moreover, even in the peripheries of large cities in more developed states, pregnant women’s confidence in the public health system is often compromised (4, 5, 8, 16).
The low completeness of vaccine registration observed in our study is consistent with findings from other regions in Brazil. For example, a study in Botucatu (São Paulo) reported that 68.4% of pregnant women received recommended vaccines a rate significantly higher than the complete coverage found in our study, yet still below NIP targets (22). Similarly, research in Greater Vitória (Espírito Santo) reported 59.3% Tdap vaccine coverage, highlighting documentation inconsistencies across public health services (23). Furthermore, a national study documented a sharp decrease in Tdap coverage for pregnant women to 45.4% in 2020 from 63.2% in 2019, far from the national target of 95% (4, 16). While Latin American influenza vaccination rates average around 59% (24), even high-income countries like the U. S. and Italy report persistent gaps in maternal vaccine uptake despite robust healthcare infrastructures (14, 25). Collectively, these trends point to systemic barriers including misinformation, insufficient provider training, and logistical challenges That impede vaccination efforts worldwide (22–25).
Our analysis of vaccine combinations, illustrated in a Venn diagram, revealed specific patterns in partial vaccination. The most common two-vaccine combination was Tdap and hepatitis B (HBV), while the most frequent three-vaccine combination was Tdap, HBV, and influenza. These results align with our questionnaire findings, in which Tdap, hepatitis B, and influenza were, in that order, the most commonly recognized vaccines. In contrast, a study in Italy reported that the most frequently recalled combination during pregnancy was Tdap and COVID-19 (26). This contrast highlights the low COVID-19 vaccination coverage observed in our study and across Brazil. Although COVID-19 vaccination during pregnancy is safe and effective in reducing complications for both the mother and newborn, its uptake remains below targets worldwide (27). For instance, a large cohort study in Rio de Janeiro reported that only 53.0% of pregnant women had received at least one dose of a COVID-19 vaccine (28).
The mean age of the participants was 27.1 years, with a range of 14 to 50 years. The largest age group was 26–30 years (20.8%); however, a substantial proportion (18.6%) of participants were adolescents and young adults (aged 14–21 years) (Figure 5). This high prevalence of young mothers reflects a demographic reality frequently observed in the maternity wards at HEPP and raises important public health considerations regarding maternal and child well-being.
Several factors may contribute to the high rate of adolescent and young adult pregnancy in this population. One significant factor is the intergenerational cycle of early childbearing, wherein daughters of teenage mothers have a higher risk of becoming teenage mothers themselves. This cycle is often linked to poverty, lower educational attainment, and limited access to healthcare and other opportunities (14, 24, 29). The study population, drawn entirely from the SUS, is largely characterized by these socioeconomic vulnerabilities.
Although adolescent pregnancy rates have been decreasing, they remain high in Brazil compared to global averages (29). National studies confirm this trend; for example, data from the 2013 National Health Survey showed that a large proportion of first pregnancies in Brazil occur during adolescence, particularly in regions with poorer socioeconomic conditions (9). Similarly, a large study of SUS users found that women aged 12–19 years accounted for 21.4% of pregnant and postpartum patients analyzed (8). This context is particularly relevant to the western region of São Paulo, which is one of the state’s most socioeconomically challenged areas, with several municipalities exhibiting low Human Development Index scores (30). While our study did not assess socioeconomic status directly, this underlying vulnerability is a recognized characteristic of pregnant women served by the SUS (31).
Knowledge gaps regarding vaccination persist among pregnant women worldwide (19, 20, 24, 25). In our study, participants most frequently recognized tetanus and COVID-19 by name; in contrast, the importance of protection against diseases like acellular pertussis and diphtheria was less understood. Only 57.5% of respondents felt sufficiently informed by healthcare professionals about maternal immunization, and a mere 38% were aware of the protective role of transplacental antibody transfer.
Defining the precise reasons for these knowledge gaps among pregnant women in western São Paulo is challenging. We suggest that while healthcare providers are seen as a reliable source of information, their recommendations alone may be insufficient. Systemic issues, such as high turnover among healthcare professionals within the SUS, can lead to disruptions in the continuity of prenatal care. Other factors, including low socioeconomic status, lower maternal education, and delayed initiation of prenatal care, also likely contribute to the observed knowledge gaps in our region.
Global evidence underscores the critical role of healthcare providers in enhancing vaccine uptake during pregnancy (19, 20, 24, 25). For example, a study in France reported that adherence to vaccination among pregnant women was positively associated with awareness of maternal vaccines, confidence in vaccine effectiveness, and receiving recommendations from healthcare professionals (20). Similarly, a U.S.-based study demonstrated that clear recommendations from providers, coupled with educational materials, significantly improved acceptance rates for both influenza and Tdap vaccines (19). In several Latin American countries, including Brazil, pregnant women exhibited limited knowledge regarding the role of maternal antibodies and the specific vaccines recommended during pregnancy (32). Collectively, these findings underline the importance of training healthcare professionals to deliver accurate, timely, and personalized vaccination counseling.
The Tdap vaccine, which protects against tetanus, diphtheria, and pertussis (whooping cough), is mandatory for all pregnant women in Brazil (6, 22). Given that most women admitted for delivery at HEPP experience high social vulnerability, we investigated whether higher maternal education was associated with a greater likelihood of having Tdap vaccination recorded on their prenatal cards. Our study found no significant association, challenging the common assumption that higher education invariably leads to better health-seeking behaviors.
A possible explanation for this result is the relative socioeconomic homogeneity of the study population. This homogeneity was reflected not only in the lack of association between education and Tdap registration but also in the absence of significant associations between other epidemiological variables (age, race, marital status, occupation) and the registration of other recommended vaccines. Our findings are in line with other Brazilian studies. Research in a São Paulo state city found no association between completing the postpartum vaccination schedule (Tdap and hepatitis B) and maternal education, age, race, or marital status (22). Similarly, a study in Belo Horizonte (Minas Gerais) found no link between tetanus vaccine uptake and maternal education (33).
In contrast, other studies have found an association. In Italy, higher educational levels were significantly associated with vaccination during pregnancy (14), and interventions in Latin America that included a provider education component positively impacted maternal vaccine uptake (34). These conflicting findings likely reflect the descriptive nature of many of these studies, which are subject to various confounding variables and biases that can differ by location and population.
Through Brazil’s Unified Health System (SUS), the country has achieved high prenatal care coverage, exceeding 97%, with most women receiving care in primary health units. In the western region of São Paulo (DRS-XI), SUS-affiliated prenatal healthcare is available in all municipalities, ensuring access to monitoring, testing, vaccination, and linkage to a maternity hospital for delivery (8, 15, 16, 23). However, high accessibility does not always translate to high vaccine uptake. In Brazil and elsewhere, individual perceptions of vaccine safety strongly influence pregnant women’s decisions, with fears about side effects or negative beliefs often leading to hesitancy (25, 26, 34).
This study has several strengths that underscore the reliability and value of its findings. First, it benefits from a large and representative sample, analyzing 47.9% of the 1,130 women admitted for delivery at HEPP during the study period, a major referral center for 45 municipalities. Second, the study has a comprehensive design, assessing three different aspects: the documentation of vaccines on prenatal cards, the association between epidemiological variables and vaccine registration, and the participants’ own knowledge of vaccination. Third, the data collection was rigorous and standardized, conducted by a single researcher to ensure consistency. Finally, the study has direct practical applications, providing valuable insights for developing regions facing similar challenges with vaccine uptake and documentation. The findings contribute significantly to the scientific literature and have the potential to be replicated at state or national levels.
This study has several limitations that should be noted. (i) The study was conducted exclusively in a public hospital (SUS). This may limit the generalizability of our findings, as pregnant women served by private healthcare providers who may exhibit higher vaccination coverage and more consistent documentation were not included. (ii) Our analysis was restricted to the standardized prenatal card issued by the Brazilian Ministry of Health (MS) to ensure data consistency. It is known that these standard cards are not always used in primary care centers; vaccination data are sometimes recorded on different documents or formats, which could have led to an underestimation of the true documentation rate. (iii) A significant portion of women did not have their prenatal cards available at the time of admission to HEPP, which restricted the sample size. This lack of documentation is a limitation in itself, as in clinical practice, the absence of a record is often interpreted as the absence of the procedure. Only 69.0% of patients had the vaccines registered in the Pregnancy Card at the time of admission in the HEPP limiting the conclusion of the scope of the study showing the poor quality of data entry by healthcare professionals, and this underreporting constitutes a limitation, as the lack of records presupposes that the procedures were not performed. (iv) The study is subject to the inherent biases of observational and retrospective designs. The questionnaire data, in particular, may be subject to recall bias, as participants’ memories of information received during pregnancy can be imperfect. Furthermore, the analysis of card records is subject to information bias due to reliance on potentially inaccurate or incomplete historical data. Finally, the observed associations may be influenced by unmeasured confounding variables.
5 Conclusion
Despite significant progress in expanding access to prenatal care in Brazil, this study reveals that the documentation of maternal vaccinations on prenatal cards remains critically low in the western region of São Paulo. This finding, coupled with the identification of significant knowledge gaps among pregnant women, raises serious concerns about the quality of prenatal counseling and the accuracy of health records within public health services. Our results show that even when women are vaccinated, they often lack adequate information about the specific immunizations they have received. Furthermore, this study challenges the common assumption that higher education invariably leads to better health practices, as we found no significant association between maternal education and Tdap vaccination registration in this population.
The challenges identified here—including low documentation rates, prevalent knowledge gaps, and the complex influence of socioeconomic factors—are not unique to this region. These findings likely reflect a broader national trend and may be applicable to other Latin American countries facing similar issues of suboptimal vaccination rates and widespread misinformation. Therefore, addressing these deficiencies requires a multi-pronged approach: concerted efforts must be made to improve the training of healthcare providers, strengthen public health education campaigns to empower pregnant women with clear information, and standardize documentation practices to ensure every vaccine counts.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, upon request.
Ethics statement
The studies involving humans were approved by Comitê de Ética em Pesquisa, Universidade do Oeste Paulista, Presidente Prudente, São Paulo, Brazil protocol number 57425522.8.0000.5515. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LP: Conceptualization, Project administration, Writing – review & editing. LS: Writing – review & editing, Formal analysis, Investigation, Methodology. JR: Formal analysis, Writing – review & editing. EF: Formal analysis, Writing – review & editing, Methodology. RG: Formal analysis, Writing – review & editing. LP-C: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The grant of PAPESP was obtained by LS, number 2022/13972-0.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sato, APS, Boing, AC, Almeida, RLF, Xavier, MO, Moreira, RS, Martinez, EZ, et al. Vacinação do sarampo no Brasil: onde estivemos e para onde vamos? Ciênc Saúde Colet. (2023) 28:351–62. doi: 10.1590/1413-81232023282.19172022
2. Beeler, JA, Lambach, P, Fulton, TR, Narayanan, D, Ortiz, JR, and Omer, SB. A systematic review of ethical issues in vaccine studies involving pregnant women. Hum Vaccin Immunother. (2016) 12:1952–9. doi: 10.1080/21645515.2016.1186312
3. Chaudhari, T. Vaccinations in the newborn. Best Pract Res Clin Obstet Gynaecol. (2021) 76:66–82. doi: 10.1016/j.bpobgyn.2020.09.004
4. Mello, LR, Marano, D, Moreira, MEL, Domingues, RMSM, Costa, ACC, and Dias, MAB. Avaliação da completitude de preenchimento do cartão da gestante do Ministério da Saúde: estudo seccional, de âmbito nacional. Ciênc Saúde Colet. (2022) 27:2337–48. doi: 10.1590/1413-81232022276.14292021
5. Costa, GD, Cotta, RMM, Reis, JR, Siqueira-Batista, R, Gomes, AP, and Franceschini, SCC. Avaliação do cuidado à saúde da gestante no contexto do Programa Saúde da Família. Ciênc Saúde Colet. (2009) 14:1347–57. doi: 10.1590/s1413-81232009000800007
6. Ministério da Saúde. Assistência pré-natal. Divisão Nacional de Saúde Materno-Infantil, Secretaria Nacional de Programas Especiais de Saúde. Brasília, Brazil: Ministério da Saúde (1988).
7. Ministério da Saúde. (2022) Nova versão da Caderneta da Gestante traz orientações sobre alimentação, saúde bucal, trabalho de parto e nascimento. Available from: https://www.gov.br/pt-br/noticias/saude-e-vigilancia-sanitaria/2022/05/nova-versao-da-caderneta-da-gestante-traz-orientacoes-sobre-alimentacao-saude-bucal-trabalho-de-parto-e-nascimento. [Accessed February 17, 2025]
8. Bittencourt, SDA, Cunha, EM, Domingues, RMSM, Dias, BAS, Dias, MAB, Torres, JA, et al. Nascer no Brasil: continuity of care during pregnancy and postpartum period for women and newborns. Rev Saude Publica. (2020) 54:100. doi: 10.11606/s1518-8787.2020054002021
9. Barreto, FDFP, and Albuquerque, RM. Discrepâncias entre o informe verbal e os registros no cartão da gestante, um instrumento negligenciado. Rev Bras Ginecol Obstet. (2012) 34:259–67. doi: 10.1590/S0100-72032012000600004
10. Silveira, MM, Conrad, NL, and Leite, FPL. Effect of COVID-19 on vaccination coverage in Brazil. J Med Microbiol. (2021) 70:1466. doi: 10.1099/jmm.0.001466
11. Zajacova, A, and Lawrence, EM. The relationship between education and health: reducing disparities through a contextual approach. Annu Rev Public Health. (2018) 39:273–89. doi: 10.1146/annurev-publhealth-031816-044628
12. Raghupathi, V, and Raghupathi, W. The influence of education on health: an empirical assessment of OECD countries for the period 1995–2015. Arch Public Health. (2020) 78:20. doi: 10.1186/s13690-020-00402-5
13. World Health Organization. Global vaccine action plan 2030. Geneva, Switzerland: World Health Organization (2023).
14. Costantino, C, Mazzucco, W, Bonaccorso, N, Cimino, L, Conforto, A, Sciortino, M, et al. Educational interventions on pregnancy vaccinations during childbirth classes improves vaccine coverages among pregnant women in Palermo’s province. Vaccines. (2021) 9:1455. doi: 10.3390/vaccines9121455
15. Domingues, CMAS, Maranhão, AGK, Teixeira, AM, Fantinato, FFS, and Domingues, RAS. The Brazilian National Immunization Program: 46 years of achievements and challenges. Cad Saude Publica. (2020) 36:e00222919. doi: 10.1590/0102-311X00222919
16. Ministério da Saúde. (2025) Cobertura Vacinal – Residência. Available online at: http://tabnet.datasus.gov.br/cgi/dhdat.exe?bd_pni/cpnibr.def and https://infoms.saude.gov.br/extensions/SEIDIGI_DEMAS_VACINACAO_CALENDARIO_NACIONAL_COBERTURA_RESIDENCIA/SEIDIGI_DEMAS_VACINACAO_CALENDARIO_NACIONAL_COBERTURA_RESIDENCIA.html. [Accessed February 17, 2025].
17. Boton Pereira, DH, Primo, LS, Pelizari, G, Flores, E, de Moraes-Vasconcelos, D, Condino-Neto, A, et al. Primary immunodeficiencies in a mesoregion of São Paulo, Brazil: epidemiologic, clinical, and geospatial approach. Front Immunol. (2020) 11:862. doi: 10.3389/fimmu.2020.00862
18. Instituto Brasileiro de Geografia e Estatística. (2025). Portal do IBGE. Cidades e Estados/Portal de Mapas. Available online at: https://www.ibge.gov.br/cidades-e-estados/sp/.html? [Accessed January 19, 2025].
19. Strassberg, ER, Power, M, Schulkin, J, Stark, LM, Mackeen, AD, Murtough, KL, et al. Patient attitudes toward influenza and tetanus, diphtheria, and acellular pertussis vaccination in pregnancy. Vaccine. (2018) 36:4548–54. doi: 10.1016/j.vaccine.2018.05.121
20. Karafillakis, E, Francis, MR, Paterson, P, and Larson, HJ. Trust, emotions, and risks: pregnant women’s perceptions, confidence, and decision-making practices around maternal vaccination in France. Vaccine. (2021) 39:4117–25. doi: 10.1016/j.vaccine.2021.05.096
21. Fundação Oswaldo Cruz (FIOCRUZ). (2025). Perguntas e respostas sobre vacinação. Available from: https://portal.fiocruz.br/perguntas-e-respostas-sobre-vacinacao?page=2. [Accessed February 03, 2025].
22. Rocha, BC, Carvalheira, AP, Ferrari, AP, Tonete, VL, Duarte, MT, and Parada, CM. Cobertura vacinal e fatores associados em puérperas de município Paulista [immunization coverage and associated factors of women who have recently given birth in a city in São Paulo state]. Ciênc Saúde Colet. (2016) 21:2287–92. doi: 10.1590/1413-81232015217.16862015
23. Santos Neto, ET, Oliveira, AE, Zandonade, E, Gama, SGN, and Leal, MC. O que os cartões de pré-natal das gestantes revelam sobre a assistência nos serviços do SUS da Região Metropolitana da Grande Vitória, Espírito Santo, Brasil? Cad Saude Publica. (2012) 28:1650–62. doi: 10.1590/s0102-311x2012000900005
24. Guzman-Holst, A, DeAntonio, R, Prado-Cohrs, D, and Juliao, P. Barriers to vaccination in Latin America: a systematic literature review. Vaccine. (2020) 38:470–81. doi: 10.1016/j.vaccine.2019.10.088
25. Razzaghi, H, Kahn, KE, Calhoun, K, Garacci, E, Skoff, TH, Ellington, SR, et al. Influenza, Tdap, and COVID-19 vaccination coverage and hesitancy among pregnant women—United States, April 2023. MMWR Morb Mortal Wkly Rep. (2023) 72:1065–71. doi: 10.15585/mmwr.mm7239a4
26. Seravalli, V, Romualdi, I, Ammar, O, De Blasi, C, Boccalini, S, Bechini, A, et al. Vaccination coverage during pregnancy and factors associated with refusal of recommended vaccinations: an Italian cross-sectional study. Vaccine X. (2024) 18:100483. doi: 10.1016/j.jvacx.2024.100483
27. Tsiaousi, I, Psarris, A, Theodora, M, Antsaklis, P, Sindos, M, Koutroumanis, P, et al. COVID-19 vaccination acceptance during pregnancy in Europe. Cureus. (2024) 16:e63562. doi: 10.7759/cureus.63562
28. Borges, MASB, Florentino, PTV, Cerqueira-Silva, T, Carvalho, LF, Araújo Oliveira, V, Aguilar, GMO, et al. Factors associated with COVID-19 vaccination among pregnant women in Rio de Janeiro City, Brazil. Sci Rep. (2023) 13:18235. doi: 10.1038/s41598-023-44370-6
29. Fernandes, FCGM, Santos, EG, and Barbosa, IR. Age of first pregnancy in Brazil: data from the national health survey. J Hum Growth Dev. (2019) 29:304–12. doi: 10.7322/jhgd.v29.9523
30. Soares Santana, R, Briguenti Souza, K, Lussari, F, Fonseca, ES, Andrade, CO, Meidas, MMK, et al. Cases and distribution of visceral leishmaniasis in western São Paulo: a neglected disease in this region of Brazil. PLoS Negl Trop Dis. (2021) 15:e0009411. doi: 10.1371/journal.pntd.0009411
31. Jacob, LMDS, Santos, AP, Lopes, MHBM, and Shimo, AKK. Socioeconomic, demographic and obstetric profile of pregnant women with hypertensive syndrome in a public maternity. Rev Gaucha Enferm. (2020) 41:e20190180. doi: 10.1590/1983-1447.2020.20190180
32. Fauzia Malik, A, Belizan, M, Gutierrez, M, Vilajeliu, A, Sanclemente, LN, Gonzalez Casanova, I, et al. Pregnant women’s perspectives about maternal immunization in Latin America. Vaccine. (2021) 39:B44–9. doi: 10.1016/j.vaccine.2020.09.009
33. Silva, TPRD, Dumont-Pena, E, Moreira, AD, Camargos, BA, Meireles, MQ, Souza, KV, et al. Factors associated with normal and cesarean delivery in public and private maternity hospitals: a cross-sectional study. Rev Bras Enferm. (2020) 73:e20180996. doi: 10.1590/0034-7167-2018-0996
Keywords: prenatal card, Brazilian National Immunization Program, vaccination coverage, pregnancy, misinformation pregnant card, vaccines, vaccine knowledge, maternal education
Citation: Panucci LAG, Sant’Anna Pinheiro L, Roque JPT, Flores EF, Giuffrida R and Prestes-Carneiro LE (2025) Evaluation of vaccination coverage and the knowledge of parturient admitted for labor in a public tertiary maternity hospital in western São Paulo, Brazil. Front. Public Health. 13:1542321. doi: 10.3389/fpubh.2025.1542321
Edited by:
Marc Jean Struelens, Université Libre de Bruxelles, BelgiumReviewed by:
Prakamya Gupta, National Health Systems Resource Center, IndiaEstevao Salvador Langa, Paulista University, Brazil
Copyright © 2025 Panucci, Sant’Anna Pinheiro, Roque, Flores, Giuffrida and Prestes-Carneiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luiz Euribel Prestes-Carneiro, bHVpemVwY2FybmVpcm9AZ21haWwuY29t