 Rander Junior Rosa1*
Rander Junior Rosa1* Rubia Laine de Paula Andrade1
Rubia Laine de Paula Andrade1 Letícia Perticarrara Ferezin1Mônica Chiodi Toscano de Campos1,2Heriederson Sávio Dias Moura1
Letícia Perticarrara Ferezin1Mônica Chiodi Toscano de Campos1,2Heriederson Sávio Dias Moura1 Thais Zamboni Berra1Natacha Martins Ribeiro1Titilade Kehinde Ayandeyi Teibo1André Luiz Teixeira Vinci1
Thais Zamboni Berra1Natacha Martins Ribeiro1Titilade Kehinde Ayandeyi Teibo1André Luiz Teixeira Vinci1 Felipe Mendes Delpino3Miguel Ángel Fuentealba Torres4Ricardo Alexandre Arcêncio1
Felipe Mendes Delpino3Miguel Ángel Fuentealba Torres4Ricardo Alexandre Arcêncio1- 1University of São Paulo at Ribeirão Preto College of Nursing, Ribeirão Preto, São Paulo, Brazil
- 2University of Brasília, Brasília, Brazil
- 3Federal University of Pelotas, Capão do Leão, Rio Grande do Sul, Brazil
- 4Faculty of Nursing and Obstetrics of the Universidad de los Andes, Santiago, Chile
Background: Health risk perception and factors associated with the severity or death from COVID-19 were key elements that influenced individuals' protective behaviors during the pandemic. Understanding these perceptions is crucial for public health guidelines that encourage preventive measures and improve an outbreak response strategy. Thus, this systematic review aimed to identify factors associated with the perception of risk of severity or death from COVID-19.
Methods: A systematic review was conducted with an article search performed in March 2024 across five databases, utilizing both controlled and free vocabulary. Studies published from 2020 onward were included. Two reviewers independently selected articles, with disagreements resolved by a third reviewer. The data were extracted using a structured form, and the findings were synthesized narratively. The studies included in the review underwent a methodological quality assessment using tools proposed by the Joanna Briggs Institute.
Results: Nineteen articles were included in the review. Among the factors most frequently associated with the perception of severe illness or death from COVID-19 were advanced age, female gender, personal experience or witnessing of adverse COVID-19 outcomes, the presence of chronic non-communicable diseases, and lower educational attainment.
Conclusion: The study highlights that the perception of risk for COVID-19 severity or death varied according to age, gender, and prior experiences with the disease. Such findings can guide healthcare practices and contribute to the formulation of public policies, strengthening responses to future public health crises.
Systematic review registration: identifier CRD42024444734, https://www.crd.york.ac.uk/PROSPERO/view/CRD42024444734.
1 Introduction
COVID-19, caused by the novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), poses a significant challenge to global public health. Common symptoms of the disease include dry cough, fatigue, sore throat, and fever, which can progress to severe clinical complications, such as pneumonia, requiring supportive care measures like mechanical ventilation (1).
The risk perception is related to severe complications or death from COVID-19, which refers to an individual's perceived vulnerability to the severity of the disease (2) may influence the adoption of protective and/or risky behaviors, along with fear, prosocial attitudes, the perceived effectiveness of preventive measures, and trust in healthcare professionals and science (3). Risk perception may therefore continue to influence people's daily decisions, potentially reducing their adherence to mask-wearing, social distancing, and vaccination. Moreover, as health threats become more imminent and severe, risk perceptions also increase, significantly impacting mental health, with individuals, in the case of COVID-19, tending to report elevated levels of worry and fear (4, 5).
Risk perception is subjective and varies among individuals. It can be heightened or reduced based on several factors, including the manner in which information about COVID-19 is disseminated by media outlets and health authorities, personal experiences with the disease and observed instances of COVID-19 progression in others (6). The concept of risk extends beyond cultural worldviews and cognitive processes (7–10), being influenced by factors such as trust in governmental institutions, scientific bodies, and medical professionals, as well as an individual's understanding of government strategies and their sense of personal and collective efficacy (3, 11).
Trust in scientific and public health institutions can influence risk perception and adherence to preventive measures in various ways, depending on how this trust is measured and contextualized (8). An individual's risk perception and subsequent behavioral responses during the pandemic are further shaped by the interplay of interpersonal trust, media communication, and personal experiences (7). Understanding these factors is crucial for developing effective public health interventions and improving communication strategies. This knowledge can help increase adherence to protective measures and, consequently, prevent the spread of communicable diseases such as COVID-19.
Despite the extensive literature on COVID-19 (3, 7, 8, 10–13), there remains a gap in the systematic synthesis of data on risk perception and its determinants across diverse populations. Moreover, current research often provides fragmented insights or focuses on single-population studies, lacking a comprehensive approach to comparing findings across various contexts and demographic profiles.
A systematic review could address this gap by consolidating evidence on variations in risk perception, identifying common trends, and highlighting how these perceptions influenced adherence to preventive measures. Additionally, by synthesizing existing data, this review may offer a clearer understanding of the psychological, social, and cultural factors that have impacted public response to health crises, thereby informing future pandemic preparedness strategies.
Given the scarcity of a comprehensive study on the associate factors influencing risk perception of COVID-19 severity or mortality, particularly in the context of a global health crisis, this study aimed to analyze, through a systematic literature review, the factors that shape the perception of risk regarding COVID-19 severity or mortality, with a focus on the interplay between sociocultural and behavioral factors.
2 Methods
This review was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (14) and the steps outlined in the “Methodological Guidelines: Development of Systematic Review and Meta-Analysis of Comparative Observational Studies on Risk Factors and Prognosis” (Brazil, 2014). The study protocol was registered with the International Prospective Register for Systematic Reviews (PROSPERO ID: CRD42024444734).
2.1 Research question
The investigation was guided by the “PEO” strategy, which poses the question: “What are the factors associated with the perception of risk of severity or death from COVID-19?” In this context, “PEO” is an abbreviation that breaks down as follows: “P” for Population (adult individuals), “E” for Exposure (associated factors), and “O” for Outcome (risk perception regarding the development of severe illness or death from COVID-19). The details of this approach are presented in Table 1, showing the structure of the PEO.
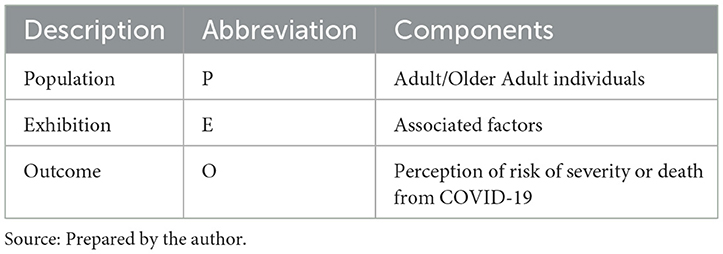
Table 1. PEO framework for research question.
2.2 Eligibility criteria
Studies published in all languages between 2020 and 2024 were included, focusing on research involving humans aged 18 years or older. Only studies that aimed to identify and analyze factors associated with the perception of risk regarding severity or death from COVID-19 were considered, regardless of methodological quality. The review included analytical observational studies, irrespective of the country of origin and/or publication.
The studies excluded from the review were those that: (1) did not provide information on the outcome of interest (risk perception of severe illness or death from COVID-19); (2) assessed and provided information solely on factors associated with COVID-19 infection; and (3) offered information on factors associated with COVID-19 protective measures.
2.3 Sources of information
In March 2024, the bibliographic survey was carried out in the following electronic databases: LILACS (Latin American and Caribbean Literature in Health Sciences); MEDLINE (Medical Literature Analysis and Retrieval System online) via PubMed (Public/Publisher MEDLINE); Embase (Excerpta Medica Database); Web of Science (Web of Science Core Collection) via CAPES journal portal; and Scopus (SciVerse Scopus).
2.4 Search strategy
The keywords and descriptors for the searches were extracted from the Health Sciences Descriptors (DeCS) and Medical Subject Headings (MeSH) and through previous searches in the databases. The search strategies were individually adjusted for each database, using a combination of Boolean operators (“AND” and “OR”), as shown in Table 2.

Table 2. Search strategies used in the systematic review of factors associated with the perception of risk of severity or death from COVID-19, according to the databases consulted, Brazil, 2024.
2.5 Screening process
The selection process utilized Rayyan QCRI software, chosen for its intuitive interface and collaborative screening tools. As a first step, duplicate publications were eliminated. Two independent reviewers (RJR and LPF) conducted the selection based on pre-defined criteria, where they considered research objectives, study type and population characteristics. Studies were included if they met the following criteria: original research, published in English, Portuguese, or Spanish and involved human samples, used quantitative or qualitative methodologies. Studies were excluded if they were review articles, based on non-representative samples and failed to meet methodological standards. The screening process occurred in two stages: reading titles and abstracts and, full analysis of selected texts. In cases of disagreement, a third reviewer (RLPA) was consulted to ensure selection consistency. This process ensured high agreement between reviewers and maintained the methodological robustness of the review.
2.6 Data extraction process
The data extraction process was carried out meticulously by two reviewers (RJR and LPF), who utilized a standardized form developed by the research team. This form included the following items: authors, year of publication, country of the study, study objective, study type, study location, population characteristics, data analysis, and study results. The reviewers independently extracted data from all included studies, and the collected data were compared, with a third reviewer involved in case of any disagreements. The obtained data were then organized and systematically entered into a table in Word software, allowing for a clear and structured visualization of the results.
2.7 Assessment of the quality of studies
The studies were evaluated for methodological quality by the researcher (RJR) using the Joanna Briggs Institute (JBI) critical appraisal tool for cross-sectional studies (15). This tool consists of eight questions addressing inclusion criteria, participant and setting descriptions, exposure measurement, standardized criteria, confounding factors, strategies for confounding factors, outcome measurement, and statistical analysis. Each study's score was evaluated as: “yes,” if the criterion was clearly met; “no,” if the criterion was not met; “unclear,” if it was not clear whether the criterion was met; and “not applicable.” A “yes” response was scored as “1,” while the responses “no,” “unclear,” and “not applicable” were scored as “0.” The quality score for each study was calculated and expressed as a percentage (16).
2.8 Summary of results
The results of the studies were narratively synthesized.
3 Results
Through the search conducted in the databases, 1,601 publications were identified. After the removal of duplicates, 808 studies were screened for relevance regarding inclusion in the study. A total of 778 studies were excluded after reading the titles, two studies were excluded because they could not be located in full-text, and nine studies were excluded after full-text reading. Thus, 19 studies that addressed factors associated with the perception of risk regarding severity or death from COVID-19 were included in the review. Figure 1 illustrates the steps taken during the study selection process.
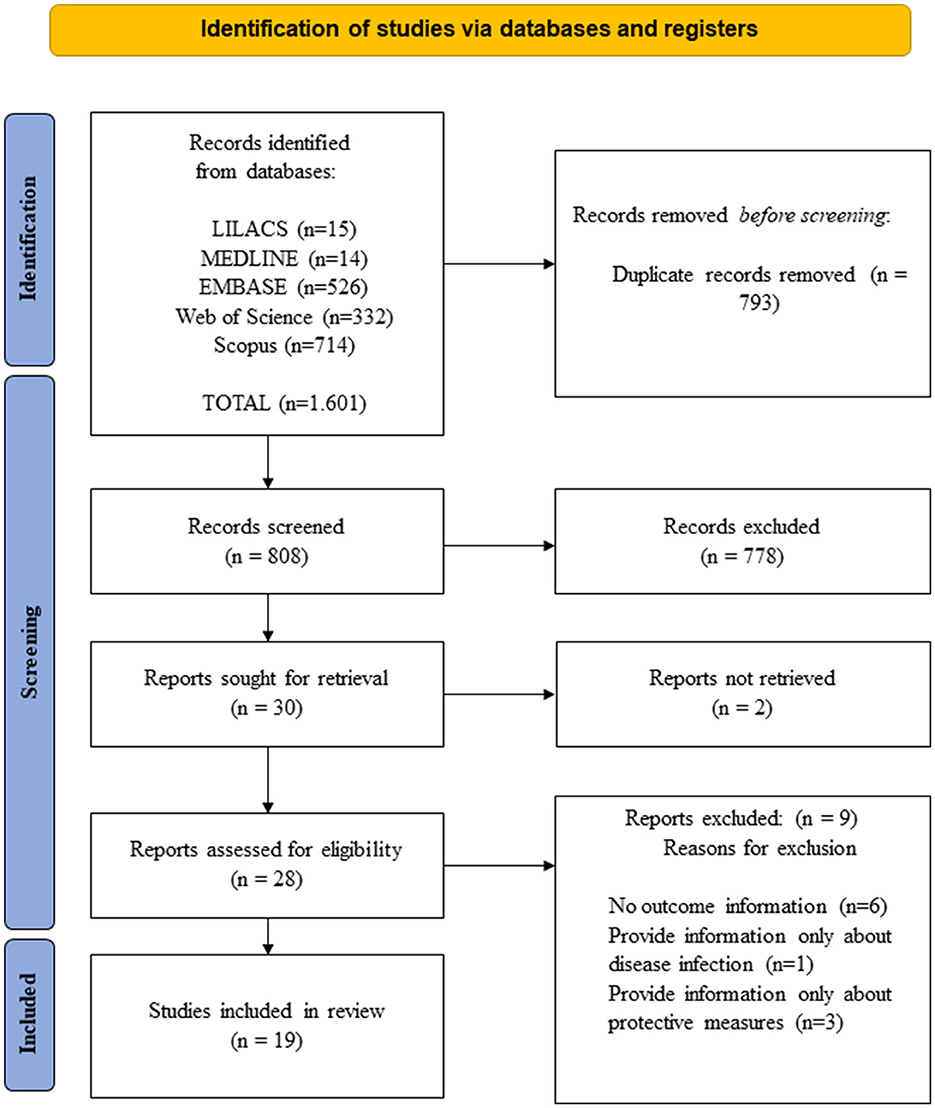
Figure 1. PRISMA flowchart of study selection in the systematic review on factors associated with the perception of risk regarding severity or death from COVID-19, Brazil, 2024. Source: Adapted from Page et al. (14).
Two studies on the topic were published in 2020 (17, 18), eight in 2021 (19–25, 45), four in, (26–29) and five in 2023 [(30–34); Table 2].
Eight studies included in the review were conducted in the United States (17, 18, 20, 22, 26, 31, 34, 45), two in Ecuador (23, 32), and one each in Brazil (27), Germany (25), Portugal (24), Pakistan (19), Russia (33), Japan (29), Saudi Arabia (30), Iran (21), Kenya (32) and Indonesia (28) (Table 2, Figure 2).
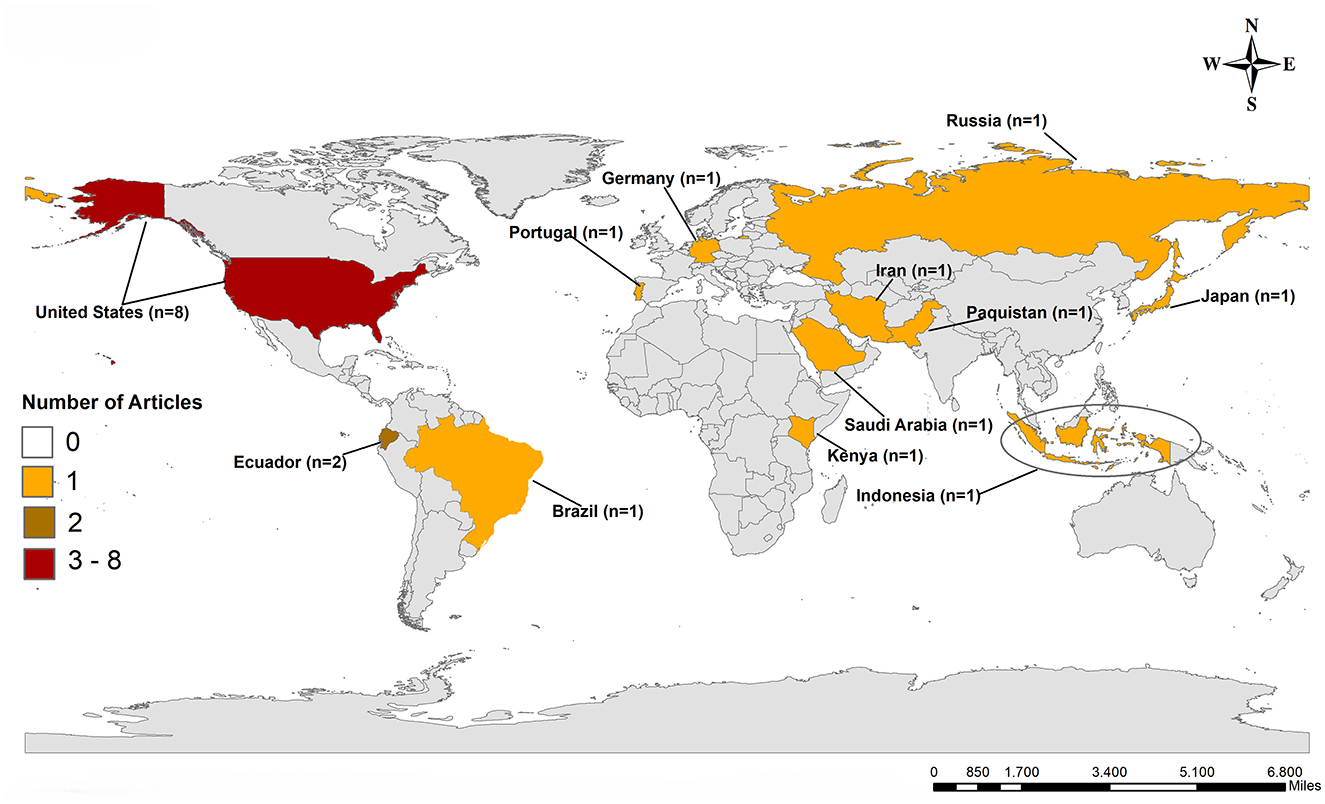
Figure 2. Geographical distribution of studies included in the systematic review on factors associated with perceived risk of severity or death from COVID-19, according to databases consulted, Brazil, 2024.
All studies included in the systematic review were cross-sectional in design, with the study populations and main results presented in Table 3.
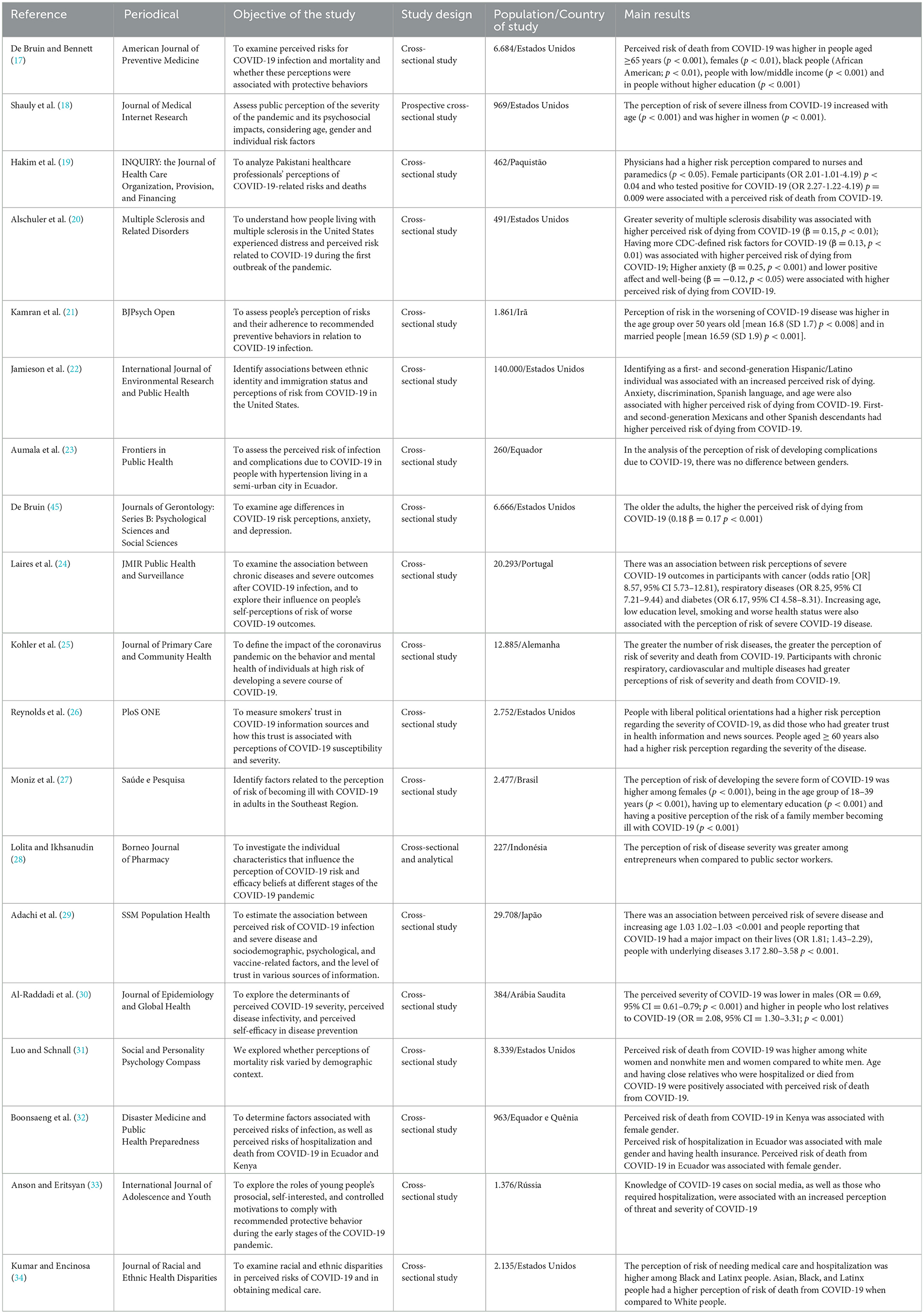
Table 3. Characteristics and main results found in published studies on factors associated with the perception of risk of severity or death from COVID-19, according to the consulted databases, Brazil, 2024.
Among the main factors associated with the perception of risk of severity or death from COVID-19 are: older age—identified by nine studies (17, 18, 21, 22, 24, 26, 29, 32, 45); female sex/gender—identified by six studies (17–19, 27, 30, 32); having previous negative personal or close experiences with COVID-19—identified in four studies (19, 28, 30, 33); having chronic non-communicable diseases (24, 25, 29) or low education level (17, 24, 27)—identified by three studies each; being foreign or of foreign descent (22, 34), being black (17, 34), having worse health status (20, 24) and having anxiety and/or less positive affect and wellbeing (20, 22)—identified in two studies each. Other factors that were mentioned only once were shown in Table 4.

Table 4. Summary of the main factors associated with the perception of risk of severity or death from COVID-19, Brazil, 2024.
A critical assessment of the methodological quality of the included studies was conducted using the Joanna Briggs Institute (JBI) tool, enabling the verification of rigor and reliability in the analyzed research. The results revealed an overall average methodological quality of 65.8%, with significant variations among studies, whose scores ranged from 25 to 100%. Only one study, by De Bruin and Bennett (17), achieved the maximum score, demonstrating exceptional methodological rigor by meeting all assessed criteria. Other studies exhibiting high methodological quality (≥80%) included those by Shauly et al. (18), Alschuler et al. (20), Kamran et al. (21), and Kohler et al. (25), indicating a more robust evidence base in these investigations. Conversely, studies with lower scores, such as those by Reynolds et al. (26) and Luo and Schnall (31), which obtained only 25%, displayed methodological weaknesses that may potentially compromise the reliability of their findings (Table 5).
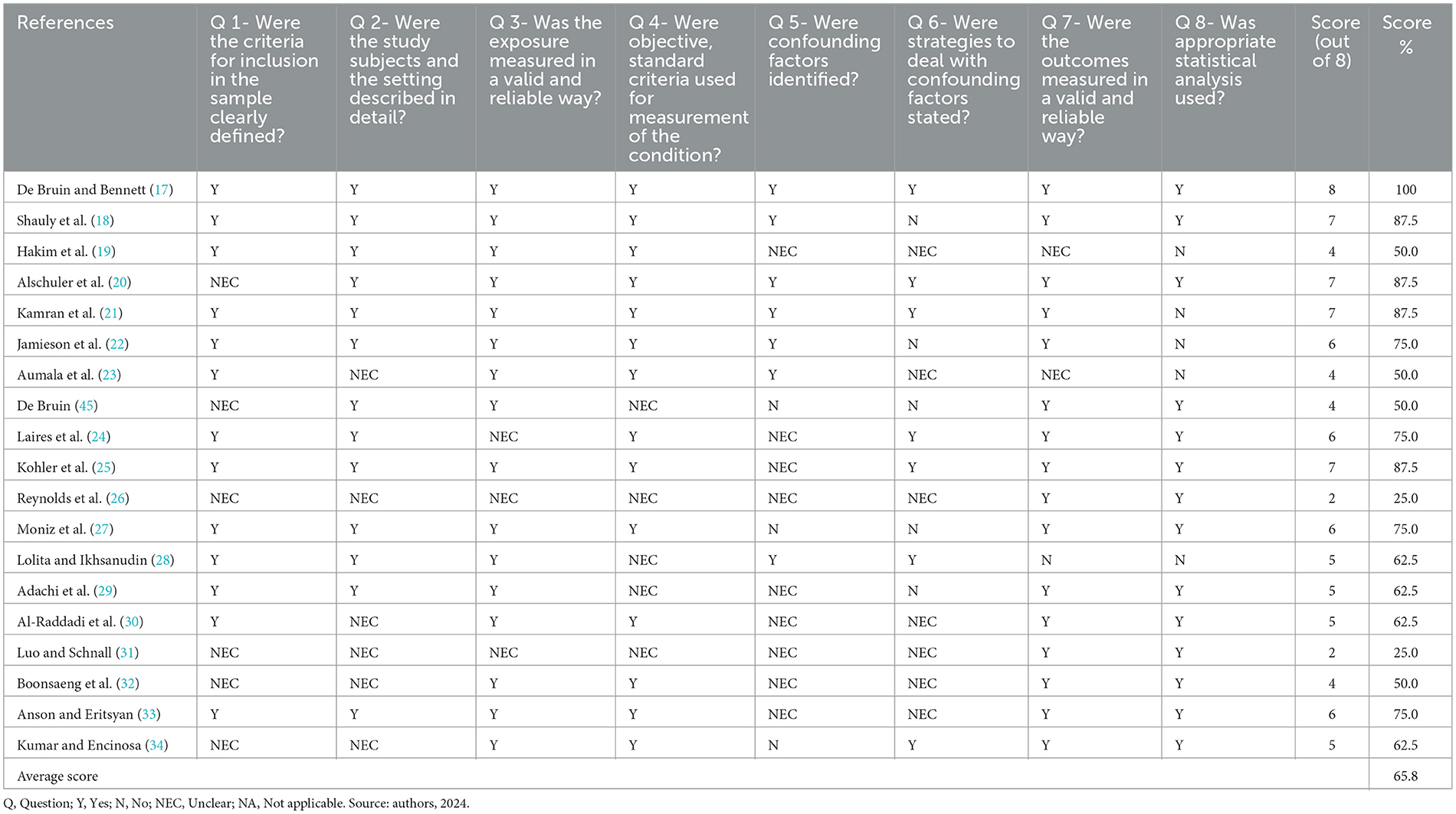
Table 5. Assessment of the methodological quality of the studies included in the systematic review on the factors associated with the perception of risk of severity or death from COVID-19, according to the databases consulted, Brazil, 2024.
Table 5 shows the results of the methodological quality assessment of the studies included in the review. The studies showed an average score of 65.8%, with the highest score in the studies by De Bruin and Benett (17), Shauly et al. (18); Alschuler et al. (20), Kamran et al. (21), and Kohler et al. (25). The methodological quality of the studies varied significantly, with scores ranging from 25 to 100%.
4 Discussion
The aim of this systematic review was to identify factors associated with the perception of risk for severe illness or death from COVID-19 and thus contribute to the formulation of effective strategies to mitigate the impact of future pandemics on the population.
The study evidenced that older individuals exhibit a heightened perception of risk regarding the potential worsening of COVID-19 compared to younger populations. This heightened awareness is likely attributed to the increased vulnerability of older adults to severe forms of the disease, as evidenced by studies highlighting their greater susceptibility to complications (35). In contrast, younger adults, particularly those aged 18 to 39 years, have been found to underestimate the severity of COVID-19, a tendency that may contribute to engaging in riskier behaviors and lower adherence to preventive measures (26). This discrepancy in risk perception across age groups highlights the need for targeted health communication strategies that resonate with the specific concerns and behaviors of different demographic segments.
Moreover, marital status has emerged as another factor influencing risk perception. Findings show that married individuals often report a greater perception of risk (34). This observation could be partially explained by the fact that married individuals are generally older on average than their single counterparts, suggesting that age might play a pivotal role in shaping their heightened awareness. However, it is also possible that the responsibilities and interdependencies associated with marriage contribute to an increased sensitivity to health risks, underscoring the interplay of social and demographic factors in risk assessment.
These findings highlight the complex dynamics between individual characteristics and risk perception, emphasizing the importance of tailoring public health messaging and interventions to address these nuanced differences. By understanding how age, marital status, and other factors influence risk perception, policymakers and health professionals can design more effective strategies to promote adherence to protective measures and reduce the impact of future pandemics.
In the present study, women exhibited a higher perception of the risk of developing severe COVID-19 compared to men. This finding is consistent with the literature, which reveals that women tend to report greater sensitivity to risk perception and fear of life-threatening events compared to men (17). In addition, the results showed that people who identify as African-American, Mexican, of Spanish descent, Hispanic/Latino, as well as first-generation immigrants, reported a significantly higher perceived risk of death due to COVID-19 compared to other population groups (17, 34). This heightened perception of risk can be attributed to a number of factors, including limited access to health services in host countries, especially for those who have migrated recently. The lack of a structured support network in destination countries, coupled with language and cultural barriers, can increase these groups' sense of vulnerability to the complications associated with the disease.
In the context of public health, communication goes beyond the simple transmission of data, promoting an expanded debate on the population's needs, advocating for collective interests, and strengthening the comprehensiveness of care and the intersectoral nature of health actions (36). The WHO emphasizes risk communication and community engagement as essential pillars for successful responses to public health emergencies. Failures in this process can result in loss of public trust, damage to the reputation of institutions, negative economic impacts, and, ultimately, an increase in the number of deaths (37).
In this scenario, it is crucial to adopt tailored health communication strategies for the vulnerable populations, considering their sociocultural particularities and challenges in accessing information (38). Educational campaigns should be developed in multiple languages and disseminated through accessible media for these groups, such as community radios, social media, and printed materials distributed at strategic locations like community centers and health units. In this regard, the involvement of community leaders and healthcare professionals who share cultural experiences with these populations can help spread reliable information and increase adherence to COVID-19 protective measures (39).
In addition, these populations may face difficulties in accessing adequate health information, which contributes to a greater perception of risk and greater apprehension about the impacts of the pandemic. Vulnerable populations, characterized by lower levels of education, income and limited access to information about health risks due to COVID-19 (17, 24, 27). This perception of risk may be related to several factors, including difficulties in accessing reliable health information and a lack of resources to respond effectively to the pandemic. On the other hand, individuals with higher levels of education, particularly those in high-risk occupations, also showed a higher perception of the risk of serious illness caused by COVID-19. Doctors, for example, tend to have a more pronounced perception of this risk due to their professional training, direct exposure to COVID-19 cases and extensive experience in managing critically ill patients. Their in-depth knowledge of the complications associated with the virus strengthens this awareness. However, this heightened perception may be somewhat mitigated by their confidence in their own self-care skills and access to advanced medical resources, which are often not available to more vulnerable groups (19).
Another factor that can impact the perception of risk of developing severe forms of COVID-19 is personal experience with the disease, such as having family members or friends who have died as a result of the infection. This type of experience tends to increase awareness of the fragility of life and the potential for adverse events, intensifying the sense of vulnerability (30). One study revealed that the majority of individuals with chronic illnesses considered themselves to be at high risk of serious complications from COVID-19, with one in four patients with chronic illnesses believing that their condition could worsen due to the virus. This feeling of high risk can be explained by the fact that more than 80% of these individuals have witnessed patients with chronic conditions who, after contracting COVID-19, have progressed to severe stages, resulting in death (23, 40).
In addition to the presence of NCDs, our results indicate that individuals with anxiety have a greater perception of the risk associated with the severity of COVID-19. Together, these findings contribute to the collective understanding of psychological manifestations and their association with the severity of COVID-19, illustrating how mental health status influences individuals' risk perceptions during public health emergencies such as the COVID-19 pandemic. This may occur because a perception of high risk evokes feelings of fear, which can lead individuals to adopt protective measures (44).
The presence of anxiety symptoms in our study is consistent with other studies on psychological distress during the COVID-19 pandemic. Anxiety was found to be more prevalent in populations with a negative perception of COVID-19. This condition was particularly common among older individuals, those with greater intolerance of uncertainty about the disease, less optimistic people and those who experienced greater loneliness. In this sense, health crises such as COVID-19, distress, fear and suffering make the threat seem more immediate and tangible (41). The recognition that fear of the severity and contagiousness of COVID-19 is the most significant stressor associated with the disease in a sample of the general population further reinforces this finding (42).
The liberal rhetoric in some countries often downplayed the severity of the COVID-19 pandemic and opposed containment measures like lockdowns, which contributed to the polarization of information. This, in turn, heightened feelings of insecurity and uncertainty among the public (43). Individuals who expressed greater trust in key sources of information, such as the World Health Organization (WHO), the Food and Drug Administration (FDA), and the media, tended to have higher perceptions of the risk associated with COVID-19. This underscores the importance for healthcare professionals to provide clear guidance on the severity of the disease, as there is a significant ideological divide that undermines trust in conventional information sources (26).
The COVID-19 pandemic was also marked by the widespread dissemination of misinformation, which became a major challenge and further complicated the global health crisis. False or misleading information about the virus, treatments, vaccines, and prevention measures created an environment of fear and uncertainty, which hindered public adherence to health guidelines and, in some cases, worsened the impact of the pandemic. Misinformation also had economic consequences, eroding trust in health institutions and science, which ultimately influenced health insurance costs and medical agreements (7). The uncertainty surrounding the disease placed additional pressure on healthcare systems, with many individuals seeking ineffective treatments or delaying necessary care. This led to an increased demand for medical services and a subsequent rise in costs.
The methodological quality of the reviewed studies exhibited remarkable diversity, reflecting a wide spectrum of research rigor and adherence to best practices. Scores ranged dramatically from 25 to 100%, highlighting the stark contrast between studies that exemplified methodological excellence and those that fell short of established quality standards. This variation underscores the importance of critical evaluation when interpreting research findings.
At the pinnacle of methodological rigor, the study by De Bruin and Bennett (17) stood out, achieving a perfect score of 100% and setting a gold standard for research quality. Close behind, studies by Shauly et al. (18), Alschuler et al. (20), Kamran et al. (21), and Kohler et al. (25) also demonstrated high methodological quality, with scores of 80% or above. These high-scoring studies provide a more reliable evidence base, offering greater confidence in their findings and conclusions. In contrast, studies at the lower end of the spectrum raise significant concerns about the reliability of their results. These methodological weaknesses not only compromise the internal validity of the affected studies but also limit the generalizability of their findings and their applications in healthcare.
The clarity and consistency of research findings are crucial for accurate interpretation. However, studies in our review exhibited concerning discrepancies between their tabulated results and textual descriptions (19, 22, 28). The conclusions drawn from the data presented in tables often diverged from the interpretations offered in the main text, which might difficult the reader in the reading and raise questions about the overall reliability of the studies' findings. While the results in the table suggest a certain conclusion, the text appears to indicate a different direction, creating a lack of coherence and clarity in the information provided. This incongruity can lead to misinterpretations and hinder readers' understanding of the true findings of the research.
One of the main limitations of this study lies in the methodological heterogeneity of the included studies, which utilize different theoretical models to investigate the perceived risk of severe illness or death from COVID-19. This diversity in theoretical approaches may have hindered direct comparisons of results and the formulation of more robust and generalizable conclusions. These factors, combined with the lack of standardization in definitions and measures of risk perception, may have introduced bias into the findings, complicating the precise identification of factors associated with COVID-19 risk perception.
Finally, it is important to consider that the review was limited to studies available up to the time of the research, which may introduce a temporal bias in the interpretation of results, given the dynamic nature of the pandemic and the ongoing evolution of scientific knowledge about COVID-19. Additionally, several studies were conducted using online questionnaires filled out independently by participants, which raises concerns such as the potential for subjective self-assessment when professional interviewer supervision is absent. Individuals with limited internet access were likely not included in the study, creating a selection bias in the studied population. Another concern is the overrepresentation of women in most studies. The selection bias and the overrepresentation of specific groups suggest that the majority of studies may not be representative of the actual population.
The findings from this study not only enhance our understanding of COVID-19 risk perception but also open up possibilities for exploring this phenomenon in other contexts. This knowledge can improve preparedness and response from local health systems to new pandemics and help address current health problems and diseases. The influence of sociodemographic, emotional, and cultural factors on risk perception, as discussed throughout this study, can be applied to various areas to enhance interventions that promote preventive behaviors and adherence to safety measures.
Furthermore, it is crucial for future research to incorporate more standardized methodological approaches and precise measures to capture the diverse influences that shape risk perception. This approach will lead to more robust and comparable results across different studies and contexts, ultimately contributing to more effective risk communication and management strategies in public health. By building on these findings and refining research methodologies, it is also necessary to develop a more comprehensive understanding of risk perception through strategic research approaches such as community-based participatory research. This is an equitable study approach where researchers, organizations, and community members collaborate on all aspects of a research project.
Such collaboration is essential for understanding all determinants that shape risk perception. This inclusive method ensures that diverse perspectives are incorporated, leading to a more comprehensive and nuanced understanding of how individuals and communities perceive and respond to risks. By engaging community members as active participants in the research process, it is gained deeper insights into the cultural, social, and contextual factors that influence risk perception, ultimately leading to more effective and tailored public health strategies.
5 Conclusion
The study revealed that during the COVID-19 pandemic, several factors influenced the perception of risk for severe illness or death from COVID-19. These factors included advanced age, female gender, personal experiences or witnessing adverse COVID-19 outcomes, the presence of chronic non-communicable diseases, and lower educational attainment. The findings indicate a concerning situation, as individuals with these characteristics may have overestimated the infectiousness of the virus. This heightened perception likely played a vital role in motivating the adoption of health-protective behaviors.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Author contributions
RR: Conceptualization, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing. RA: Data curation, Writing – review & editing. LP: Methodology, Writing – review & editing. MC: Data curation, Project administration, Writing – review & editing. HM: Data curation, Writing – review & editing. TB: Data curation, Writing – review & editing, Methodology. NR: Data curation, Writing – review & editing. TT: Project administration, Writing – review & editing. AV: Data curation, Methodology, Writing – review & editing. FM: Methodology, Writing – review & editing. MT: Conceptualization, Methodology, Writing – review & editing. RAA: Conceptualization, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Escola Nacional de Saúde Pública Sergio Arouca of the Oswaldo Cruz Foundation, Escola Nacional de Saúde Pública of the Nova Lisboa University and this study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001; Coordination for the Improvement of Higher Education Personnel [process: 88887.657730/2021-00]; the São Paulo Research Foundation Personnel [process: 2021/08263-7 and 2022/08510-7]; and the National Council for Scientific and Technological Development [process: 405902/2021-2].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ramezani S, Ezzatifar F, Hojjatipour T, Hemmatzadeh M, Shabgah AG, Navashenaq JG, et al. Association of the matrix metalloproteinases (MMPs) family gene polymorphisms and the risk of coronavirus disease 2019 (COVID-19); implications of contribution for development of neurological symptoms in the COVID-19 patients. Mol Biol Rep. (2023) 50:173–83. doi: 10.1007/s11033-022-07907-y
2. Fischhoff B. Risk perception and communication unplugged: twenty years of process 1. Risk analysis. (1995) 15:137–45. doi: 10.1111/j.1539-6924.1995.tb00308.x
3. Dryhurst S, Schneider CR, Kerr J, Freeman ALJ, Recchia G, van der Bles AM, et al. Risk perceptions of COVID-19 around the world. J Risk Res. (2020) 23:994–1006. doi: 10.1080/13669877.2020.1758193
4. Forte G, Favieri F, Tambelli R, Casagrande M. The enemy which sealed the world: effects of COVID-19 diffusion on the psychological state of the Italian population. J Clin Med. (2020) 9:1802. doi: 10.3390/jcm9061802
5. Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. (2020) 584:430–6. doi: 10.1038/s41586-020-2521-4
6. Chen LS, Kaphingst KA. Risk perceptions and family history of lung cancer: differences by smoking status. Public Health Genomics. (2010) 14:26–34. doi: 10.1159/000294151
7. Siegrist M, Bearth A. Worldviews, trust, and risk perceptions shape public acceptance of COVID-19 public health measures. Proc Nat Acad Sci. (2021) 118:e2100411118. doi: 10.1073/pnas.2100411118
8. Zeng J, Yuan M, Huang G. Individual characteristics or cultures? Public risk perception in the coronavirus pandemic. J Risk Res. (2022) 25:1413–43. doi: 10.1080/13669877.2022.2142951
9. Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. (2020) 287:112921. doi: 10.1016/j.psychres.2020.112921
10. Yuan M, Mayorga M, Johnson BB, Swedlow B. Explaining compliance with COVID-19 regulation in China and the United States: cultural biases, political trust, and perceptions of risk and protective actions. J Public Policy. (2024) 44:284–326. doi: 10.1017/S0143814X23000429
11. Yuan M. Psychological perceptions and voluntary protective behaviors during COVID-19 pandemic in China: the roles of cultural worldview. Hum Ecol Risk Assess. (2021) 1–19. doi: 10.1080/10807039.2021.2023316
12. Wilson RS, Zwickle A, Walpole H. Developing a broadly applicable measure of risk perception. Risk Analysis. (2019) 39:777–91. doi: 10.1111/risa.13207
13. Liu Z, Yang J. Public support for COVID-19 responses: cultural cognition, risk perception, and emotions. Health Commun. (2023) 38:648–58. doi: 10.1080/10410236.2021.1965710
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. BMJ. (2021) 372:n.e1. doi: 10.1136/bmj.n71
15. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute reviewer's. (2017) 5:217–69. doi: 10.46658/JBIMES-20-08
16. Khanijahani A, Iezadi S, Gholipour K, Azami-Aghdash S, Naghibi D. A systematic review of racial/ethnic and socioeconomic disparities in COVID-19. Int J Equity Health. (2021) 20:1–30. doi: 10.1186/s12939-021-01582-4
17. De Bruin WB, Bennett D. Relationships between initial COVID-19 risk perceptions and protective health behaviors: a national survey. Am J Prev Med. (2020) 59:157–67. doi: 10.1016/j.amepre.2020.05.001
18. Shauly O, Stone G, Gould D. The public's perception of the severity and global impact at the start of the SARS-CoV-2 pandemic: a crowdsourcing-based cross-sectional analysis. J Med Internet Res. (2020) 22:e19768. doi: 10.2196/19768
19. Hakim M, Afaq S, Khattak FA, Jawad M, Ul Islam S, Ayub Rose M, et al. Perceptions of COVID−19-related risks and deaths among health care professionals during COVID-19 pandemic in Pakistan: a cross-sectional study. Inquiry. (2021) 58:00469580211067475. doi: 10.1177/00469580211067475
20. Alschuler KN, Roberts MK, Herring TE, Ehde DM. Distress and risk perception in people living with multiple sclerosis during the early phase of the COVID-19 pandemic. Mult Scler Relat Disord. (2021) 47:102618. doi: 10.1016/j.msard.2020.102618
21. Kamran A, Isazadehfar K, Heydary H, Nasimi R, Naeim M. Risk perception and adherence to preventive behaviours related to the COVID-19 pandemic: a community-based study applying the health belief model. BJPsych Open. (2021) 7:e133. doi: 10.1192/bjo.2021.980
22. Jamieson T, Caldwell D, Gomez-Aguinaga B, Doña-Reveco C. Race, ethnicity, nativity and perceptions of health risk during the COVID-19 pandemic in the US. Int J Environ Res Public Health. (2021) 18:11113. doi: 10.3390/ijerph182111113
23. Aumala T, Cardenas M, Vergara D, Vasconez M, Palacios I, Terán E. Risk perception and knowledge, attitudes, and practices against COVID-19 in a hypertensive population from a semi-urban city of Ecuador. Front Public Health. (2021) 9:734065. doi: 10.3389/fpubh.2021.734065
24. Laires PA, Dias S, Gama A, Moniz M, Pedro AR, Soares P, et al. The association between chronic disease and serious COVID-19 outcomes and its influence on risk perception: survey study and database analysis. JMIR Public Health Surveill. (2021) 7:e22794. doi: 10.2196/22794
25. Kohler H, Bäuerle A, Schweda A, Weismüller B, Fink M, Musche V, et al. Increased COVID-19-related fear and subjective risk perception regarding COVID-19 affects behavior in individuals with internal high-risk diseases. J Prim Care Community Health. (2021) 12:2150132721996898. doi: 10.1177/2150132721996898
26. Reynolds RM, Weaver SR, Nyman AL, Eriksen MP. Trust in COVID-19 information sources and perceived risk among smokers: a nationally representative survey. PLoS ONE. (2022) 17:e0262097. doi: 10.1371/journal.pone.0262097
27. Moniz MA, Carmo CN, Soares LS, Campos CA, Rocha BCO, Muniz EF. Fatores relacionados à percepção do risco de adoecer por COVID-19 em adultos da Região Sudeste. Saúde e pesquisa. (2022) 15:e10420. doi: 10.17765/2176-9206.2022v15n2.e10420
28. Lolita L, Ikhsanudin A. Illness risk perceptions and efficacy beliefs among indonesian in the course of COVID-19 pandemic. Borneo J Pharm. (2022) 5:396–405. doi: 10.33084/bjop.v5i4.3287
29. Adachi M, Murakami M, Yoneoka D, Kawashima T, Hashizume M, Sakamoto H, et al. Factors associated with the risk perception of COVID-19 infection and severe illness: a cross-sectional study in Japan. SSM Popul Health. (2022) 18:101–5. doi: 10.1016/j.ssmph.2022.101105
30. Al-Raddadi R, Bahabri N, AlRaddadi Z. Perceived COVID-19 severity, risk of infection, and prevention self-efficacy in Saudi Arabia during lockdown: a population-based national study. J Epidemiol Glob Health. (2023) 13:32–46. doi: 10.1007/s44197-022-00083-z
31. Luo E, Schnall S. The ‘white male effect' in perceptions of risk of dying from COVID-19. Soc Personal Psychol Compass. (2023) 17:e12877. doi: 10.1111/spc3.12877
32. Boonsaeng T, Carpio CE, Guerrero P, Sarasty O, Borja I, Hudson D, et al. Perceived risks of infection, hospitalization, and death from COVID-19 at the Equator: Ecuador and Kenya. Disaster Med Public Health Prep. (2023) 17:e34. doi: 10.1017/dmp.2021.268
33. Anson M, Eritsyan K. COVID-19 in social networks: unravelling its impact on youth risk perception, motivations and protective behaviours during the initial stages of the pandemic. Int J Adolesc Youth. (2023) 28:2245012. doi: 10.1080/02673843.2023.2245012
34. Kumar V, Encinosa W. Racial disparities in the perceived risk of COVID-19 and in getting needed medical care. J Racial Ethn Health Disparities. (2021) 10:4–13. doi: 10.1007/s40615-021-01191-5
35. Li JB, Yang A, Dou K, Wang LX, Zhang MC, Lin XQ. Chinese public's knowledge, perceived severity, and perceived controllability of COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: a national survey. BMC Public Health. (2020) 20:1–14. doi: 10.1186/s12889-020-09695-1
36. Dos Santos MOS, Peixinho BC, Cavalcanti AMC, Silva LGF, Silva LIM, Lins DOA, et al. Estratégias de comunicação adotadas pela gestão do Sistema Único de Saúde durante a pandemia de Covid-19–Brasil. Interface-comunicação, Saúde, Educação (2021) 25:e200785. doi: 10.1590/interface.200785
37. Organização Mundial da Saúde (OMS). Comunicação de risco e engajamento comunitário: prontidão e resposta à doença do coronavírus (COVID-19): orientação provisória - 19 de março de 2020. Geneva: OMS (2020) Available online at: https://iris.paho.org/handle/10665.2/51983 (Accessed 11 maio, 2025).
38. Cardoso JM, Rocha RL. Interfaces e desafios comunicacionais do Sistema Único de Saúde. Ciência and Saúde Coletiva. (2018) 23:1871–80. doi: 10.1590/1413-81232018236.01312018
39. Cavaca AG, Oliveira IM, Araujo RI, Elias WC, Araújo IS, Lisboa M, et al. Comunicação e pandemia: interlocuções criativas de populações vulnerabilizadas no Distrito Federal. Saúde e Sociedade. (2023) 32:e220914en. doi: 10.1590/s0104-12902023220914en
40. Hu Y, Lu Y, Dong J, Xia D, Li J, Wang H, et al. Epidemiological and clinical characteristics of COVID-19 mortality: a retrospective study. Front Med. (2025) 12:1464274. doi: 10.3389/fmed.2025.1464274
41. Vogel AC, Schmidt H, Loud S, McBurney R, Mateen FJ. Impact of the COVID-19 pandemic on the health care of >1,000 people living with multiple sclerosis: a cross-sectional study. Mult Scler Relat Disord. (2020) 46:102512. doi: 10.1016/j.msard.2020.102512
42. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J. Americans' COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
43. Weaver SR, Jazwa A, Popova L, Slovic P, Rothenberg RB, Eriksen MP. Worldviews and trust of sources for health information on electronic nicotine delivery systems: effects on risk perceptions and use. SSM-popul Health. (2017) 3:787–94. doi: 10.1016/j.ssmph.2017.09.003
44. Motta Zanin G, Gentile E, Parisi A, Spasiano D. A preliminary evaluation of the public risk perception related to the COVID-19 health emergency in Italy. Int J Environ Res Public Health (2020) 17:3024. doi: 10.3390/ijerph17093024
Keywords: COVID-19, severe illness, associated factors, perception, risk
Citation: Rosa RJ, Andrade RLdP, Perticarrara Ferezin L, de Campos MCT, Moura HSD, Berra TZ, Ribeiro NM, Teibo TKA, Vinci ALT, Mendes Delpino F, Torres MÁF and Arcêncio RA (2025) Risk perception of severity or death from COVID-19: a systematic review of the factors associated. Front. Public Health 13:1543629. doi: 10.3389/fpubh.2025.1543629
Received: 11 December 2024; Accepted: 28 April 2025;
Published: 26 May 2025.
Edited by:
Ginés Navarro-Carrillo, University of Granada, SpainReviewed by:
Meng Yuan, Chongqing University, ChinaTri Siswati, Health Polytechnic Ministry of Health, Indonesia
Copyright © 2025 Rosa, Andrade, Perticarrara Ferezin, de Campos, Moura, Berra, Ribeiro, Teibo, Vinci, Mendes Delpino, Torres and Arcêncio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rander Junior Rosa, cmFuZGVyMWp1bmlvckBnbWFpbC5jb20=