 Qingwen Long
Qingwen Long Yongli Li1,2
Yongli Li1,2 Yujun Lee
Yujun Lee- 1Department of Nursing, Affiliated Hospital of North Sichuan Medical College, Nanchong, China
- 2Department of Nursing, North Sichuan Medical College, Nanchong, China
Aim: Limited researches have investigated the association between the Triglyceride-glucose index (TyG) and frailty vulnerability in middle-aged and older Chinese populations. This study aims to strengthen the scientific foundation for frailty prevention and management by analyzing the correlation between TyG and frailty, ultimately providing more targeted intervention strategies.
Methods: This study included middle-aged and older individuals who participated in the China Health and Retirement Longitudinal Study (CHARLS) from 2015. A multiple logistic regression model was constructed to assess the correlation between the TyG index and frailty. Additionally, restricted cubic spline (RCS) analysis was employed to evaluate the dose–response correlation between the two variables.
Results: Among the 3,978 participants included in the study, 667 individuals (16.8%) were identified with frailty. After adjusting for multiple factors in a logistic regression model, it was determined that individuals in the highest quartile group of the TyG index had a 1.43 times higher risk of frailty compared to those in the lowest quartile group (OR = 1.43, 95% CI: 1.10 ~ 1.85, p = 0.007). The RCS analysis further revealed a positive dose–response relationship, indicating that a higher TyG index was associated with an increased risk of frailty in middle-aged and older adults.
Conclusion: Research has shown a significant positive linear relationship between an increased TyG index and a higher prevalence of frailty in middle-aged and older individuals. Elevated TyG index levels could signal an increased vulnerability to frailty among individuals.
1 Introduction
Frailty, a multidimensional physiological condition, is marked by diminishing reserves and functions of various organ systems, weakened stress responses, increased vulnerability to diseases, and increased mortality risks (1, 2). It is commonly observed in middle-aged and older populations as they advance in age (3). As the population ages at a faster rate, frailty affects approximately 10% of community-dwelling older adults aged 60 and above, 15% for individuals aged 75–84, and 25% for those aged 85 and older in China (4, 5). In the world, the prevalence of frailty among individuals aged 50 and older is 24% across 62 countries or regions worldwide (6). Frailty is not a distinct disease but a constellation of symptoms and indicators potentially leading to disabilities, falls, depression, and reduced quality of life (7, 8). Moreover, it represents a significant contributor to mortality among middle-aged and older adults, placing substantial burdens on healthcare systems worldwide (9). However, frailty represents an early and reversible condition (3). Early identification of risk factors, regular frailty screening, and appropriate interventions are crucial for preventing and managing frailty. These measures are poised to significantly impact clinical practice and public health initiatives (3, 8, 9).
The syndrome of frailty is complex and influenced by multiple factors, sharing common pathogenic mechanisms with sarcopenia. Patients with muscle-wasting disorders often experience conditions with muscle strength and mass, which directly impacts physical function and increases vulnerability to frailty (10, 11). Consequently, mitigating and managing frailty primarily involves preventing the decline in muscle mass and function. Previous research has shown a strong correlation between insulin resistance (IR) and the decrease in muscle mass, along with the deterioration of muscle function (12, 13). IR is characterized by a decreased sensitivity of the body to insulin, leading to impaired glucose uptake and utilization (14, 15). A reduction in IR may cause muscle wasting and reduced strength, thereby worsening frailty. Studies have identified potential pathways linking IR and frailty, including muscle metabolism, inflammation, and oxidative stress (16, 17). The Triglyceride-glucose index (TyG), an emerging potential marker for IR, is significantly associated with the reduction of muscle mass and strength among older individuals (18–20). Research also demonstrates a direct relationship between the TyG index and sarcopenia, suggesting that elevated TyG index levels correspond to an increased risk of developing sarcopenia (21).
Compared to traditional approaches for measuring insulin, the TyG index offers advantages including operational convenience, quick reporting, and lowered economic impact (22). Researches have revealed a significant association between the TyG index and the onset of various chronic conditions, such as coronary artery disease, ischemic stroke, heart failure, chronic kidney disease, hypertension, and diabetes (21, 23–27). These studies show the value of the TyG index in predicting the risk of cardiovascular diseases, hypertension, diabetes, and sarcopenia. Furthermore, it is suggested that the TyG index may play an indirect role in the development of frailty.
With advancing age, bodily systems gradually deteriorate, leading to an increased risk of frailty. Aging also increases IR, with the TyG index serving as a marker of IR, thereby influencing the development of frailty (28). However, the association between the TyG index and frailty has been explicitly addressed in only two studies. These studies have shown that persistently elevated TyG index levels may have a potential impact on identifying older individuals at increased risk of frailty (29, 30). However, these studies are limited by their participant selection, predominantly concentrating on specific regions and ethnicities, thereby limiting their generalizability to the wider middle-aged and older population in China. Consequently, this study made use of the CHARLS database, which pertains to the middle-aged and older population in China, to examine the association between the TyG index and frailty. The purpose is to provide evidence supporting the prevention and management of frailty development.
2 Methods
Data from the China Health and Retirement Longitudinal Study (CHARLS) database were obtained for this study.1 CHARLS, a longitudinal study in mainland China targeting individuals aged 45 and older with a multi-stage sampling across 150 counties and 450 villages, with follow-ups conducted every 2–3 years (31). The participants in the CHARLS survey all provided written informed consent, and the survey obtained approval from the Peking University Biomedical Ethics Committee (No. IRB00001052-11015). We accessed data from the 2015 CHARLS after receiving approval from Peking University’s National School of Development. Participants younger than 50 or those with missing TyG index or frailty data were excluded from the data, resulting in a final sample of 3,978 participants, as shown in Figure 1.
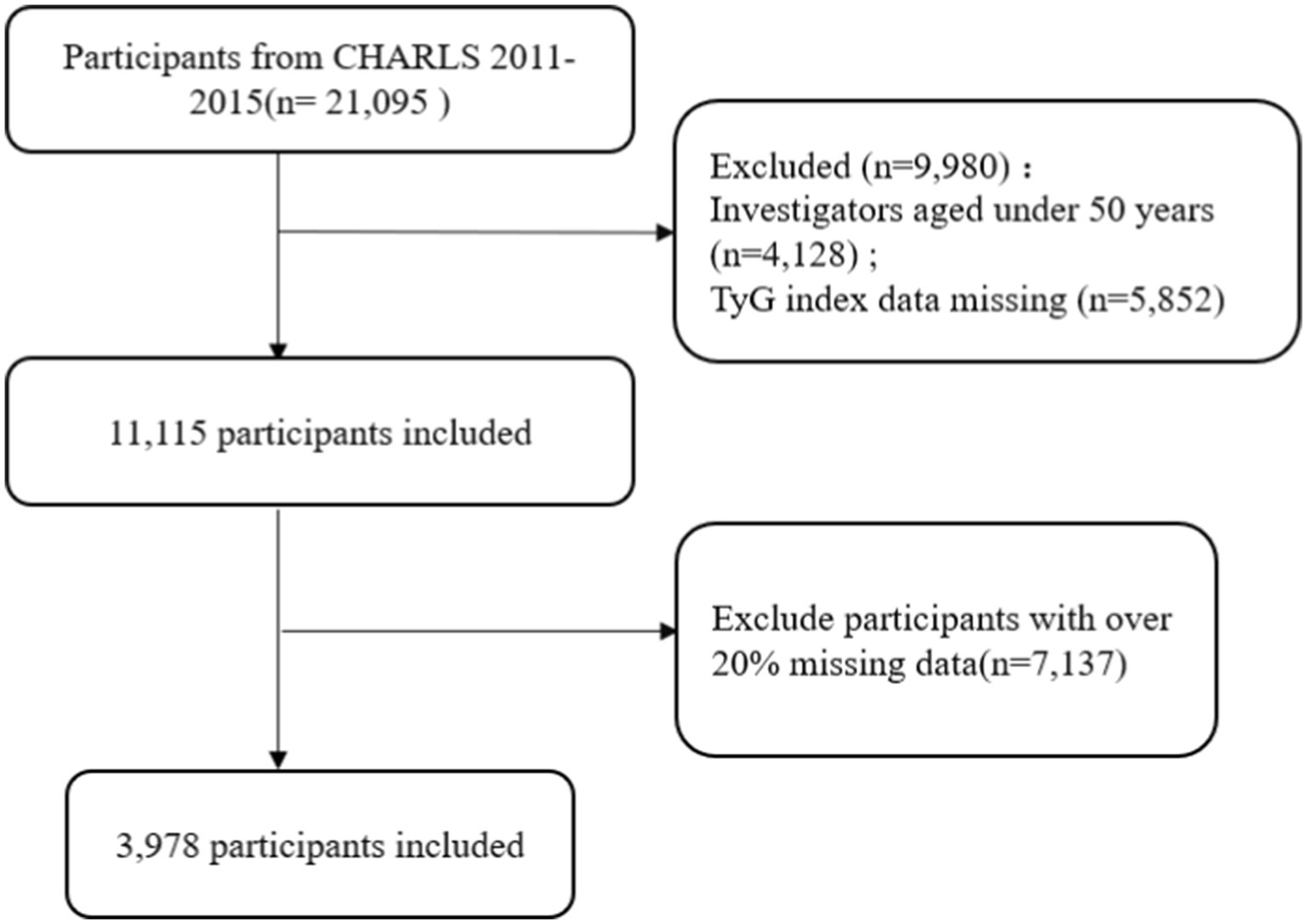
Figure 1. A flow diagram depicting the exclusion criteria for research participants.
3 Measures
3.1 Frailty
The frailty phenotype (FP) and frailty index (FI) are two main approaches used to evaluate frailty (32). Since the FP is considered more appropriate for older inpatients, this study adopted the FI developed by Searle et al. (33). An FI index was constructed using 36 health-related items, covering cognitive function, activities of daily living (ADL), instrumental activities of daily living (IADL), common chronic diseases (diabetes, stroke, heart disease, etc.), mental health, and sensory impairments. Detailed information on these items can be found in Supplementary Table 1. Each indicator was scored as 1 if the health standard was met and 0 otherwise. The FI was calculated by dividing the total impairment score by 36, yielding a value between 0 and 1. Based on previous researches (34), frailty is defined as having an FI ≥ 0.25, with higher FI scores indicating greater frailty severity.
3.2 TyG
Participants underwent blood tests of fasting triglyceride and blood glucose, which were used to calculate the TyG index using the formula: ln[fasting triglycerides (mg/dl) × fasting blood glucose (mg/dl)/2] (22). The fasting period was at least 8 h.
3.3 Covariates
This study considered covariates such as sociodemographic characteristics (age, gender, residential area, educational attainment, marital status), health behaviors (smoking status denotes the current smoking status, encompassing both daily and occasional smokers. Alcohol intake refers to the current drinking status, characterized by a consistent pattern of alcohol consumption.), physical indices (waist circumference, body mass index), and biochemical markers (hemoglobin, high-density lipoprotein, low-density lipoprotein, total cholesterol) to account for potential influences on the relationship between the TyG index and frailty.
3.4 Statistical analysis
Categorical variables are shown as frequencies and percentages (n %), analyzed with the χ2-test. Continuous variables are described by median and quartiles (M, P25, P75) and were compared using the Mann–Whitney U test. The relationship between the TyG index and the occurrence of frailty is analyzed through binary logistic regression when the index is viewed as a continuous variable. Through the utilization of quartiles of the TyG index, three logistic regression models were established to assess the risk of frailty. The outcomes were illustrated using odds ratios (OR) and 95% confidence intervals (95% CI). Model 1 serves as the initial coarse adjustment mode. Model 2 further refines the analysis by incorporating adjustments for age, gender, place of residence, and educational level. Moreover, Model 3 expands the scope of adjustments to include smoking, alcohol consumption, waist circumference, and BMI. All variables considered in the model adjustment were subsequently analyzed using the correlation matrix and multicollinearity tests. After adjusting for all covariates, we used the Restricted Cubic Spline (RCS) analysis to examine the dose–response relationship between the TyG index and frailty. Then, subgroups based on age, gender, and BMI index were assessed to examine potential interactions with the TyG index. Statistical analyses were performed utilizing R 4.4.0 and SPSS 26.0, with a significance level established at α = 0.05.
4 Results
4.1 Baseline features of individuals
With a total of 3,978 participants, the study consisted of 1,965 males (49.4%) and 2,013 females (50.6%), with a median age of 60 years, 16.8% (667 individuals) were found to have experienced frailty. Upon stratifying research participants according to frailty levels for comparative baseline characteristic analysis, it was evident that the frail cohort had a higher proportion of females relative to males, as well as being older, having elevated BMI, waist circumference, and TyG index. Furthermore, frail individuals residing in rural areas exhibited a heightened vulnerability to frailty compared to urban dwellers, with lower levels of education, high-density lipoprotein cholesterol, and hemoglobin. These differences were statistically significant, as presented in Table 1.
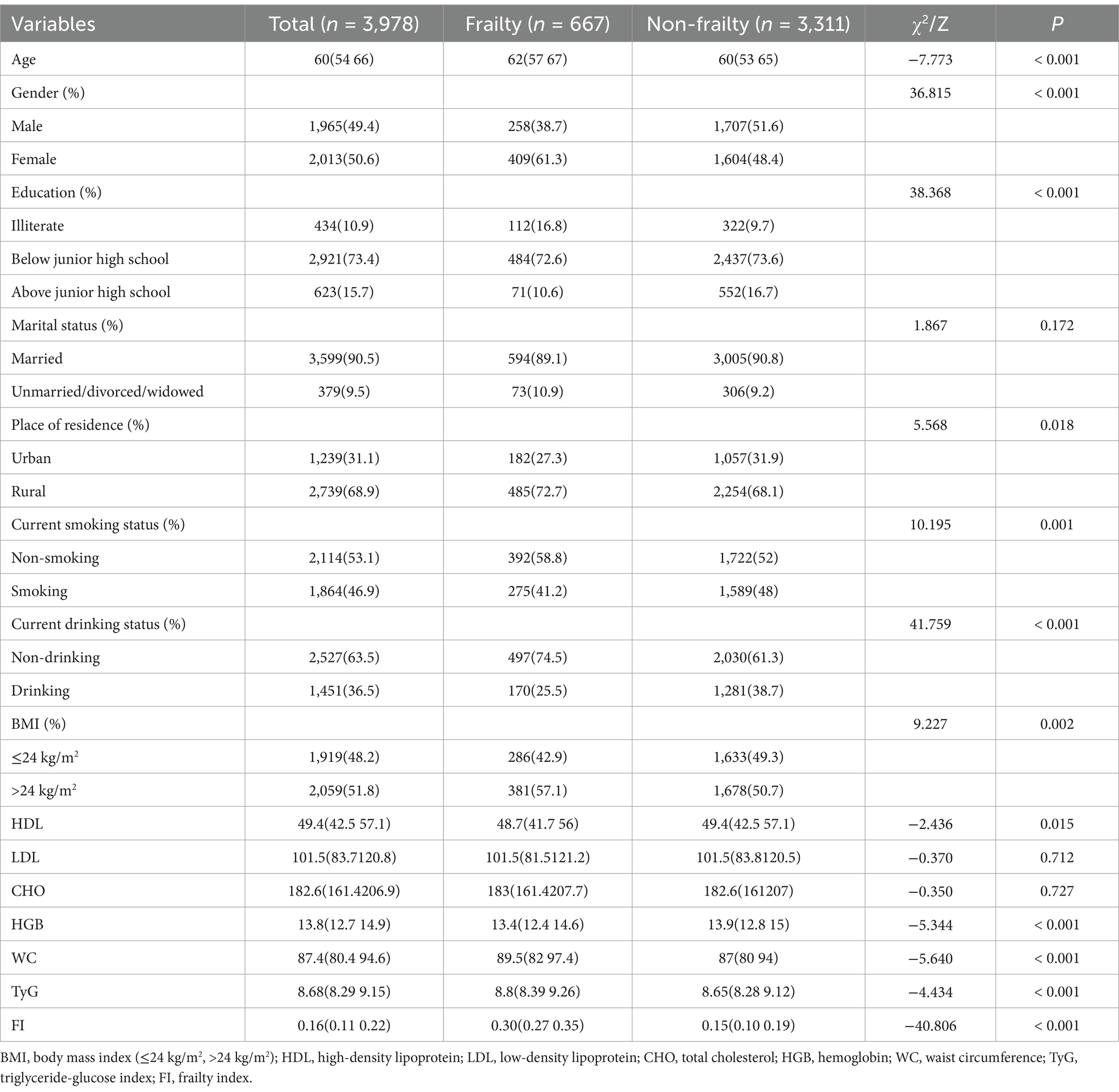
Table 1. The baseline features of the research subjects were compared through analysis.
4.2 Association between TyG index and frailty
The analysis of three logistic regression models detailed in Table 2 revealed a significant positive relationship between higher TyG index values and an increased incidence of frailty. In the unadjusted crude model 1, the risk of frailty occurrence was 1.57 times higher in the highest quartile (Q4) of the TyG index group compared to the lowest quartile (Q1) group (OR = 1.57, 95%CI: 1.24 ~ 1.99). Within model 3, after adjusting for covariates like gender, age, residence, education level, smoking habits, alcohol consumption, hemoglobin levels, waist circumference, and BMI, it was observed that individuals positioned in the highest quartile (Q4) of the TyG index were more likely to experience frailty than those placed in the lowest quartile (Q1) (TyG Q4 vs. Q1, OR = 1.43, 95%CI: 1.10 ~ 1.85, p = 0.007). The correlation matrix and multicollinearity tests showed that the variance inflation factors (VIFs) for all variables in the fully adjusted model were less than 2. Detailed findings can be found in Supplementary Figures 1–4. After adjusting for all covariates, employing RCS analysis showed a significant dose–response relationship between the TyG index and the occurrence of frailty. The risk of frailty demonstrates a slow escalation with TyG index values up to 8.68, at which point it commences a gradual ascent. A higher TyG index correlated with an elevated risk of frailty, suggesting a linear positive association between the TyG index and the risk of frailty (see Figure 2).
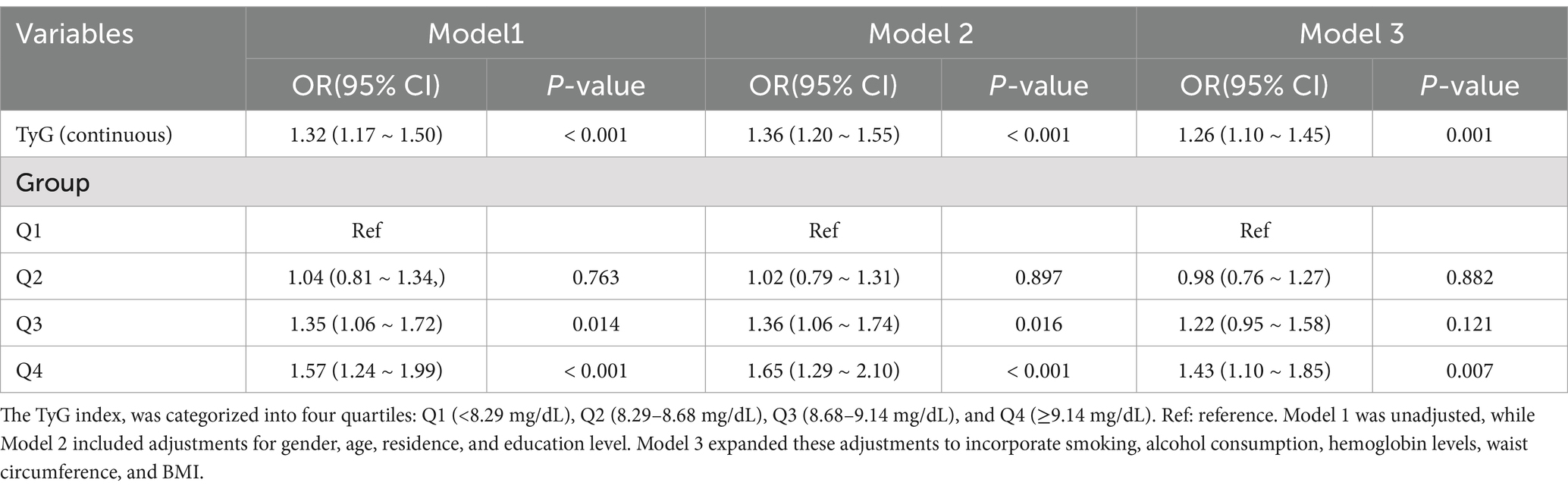
Table 2. The results of logistic analysis between TyG and frailty.
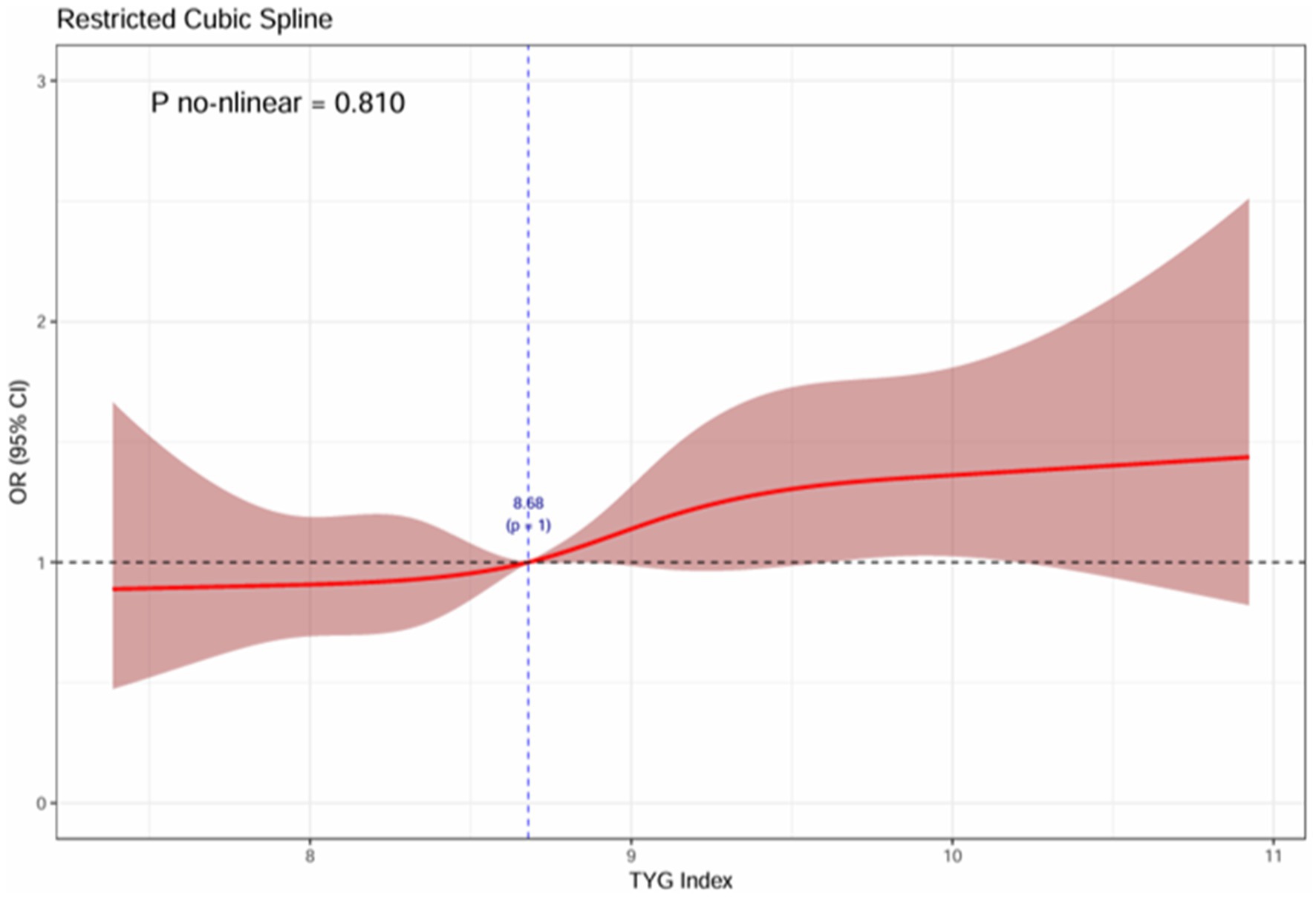
Figure 2. The association between TyG and the dose–response of frailty.
4.3 Subgroup analysis and interaction tests
After controlling for confounding variables, a subgroup analysis including gender, age, and BMI was conducted to explore potential interactions between subgroup variables and the TyG index regarding the risk of frailty onset (Table 3). No significant interaction was observed among the subgroups based on gender, age, and BMI, suggesting consistent outcomes.
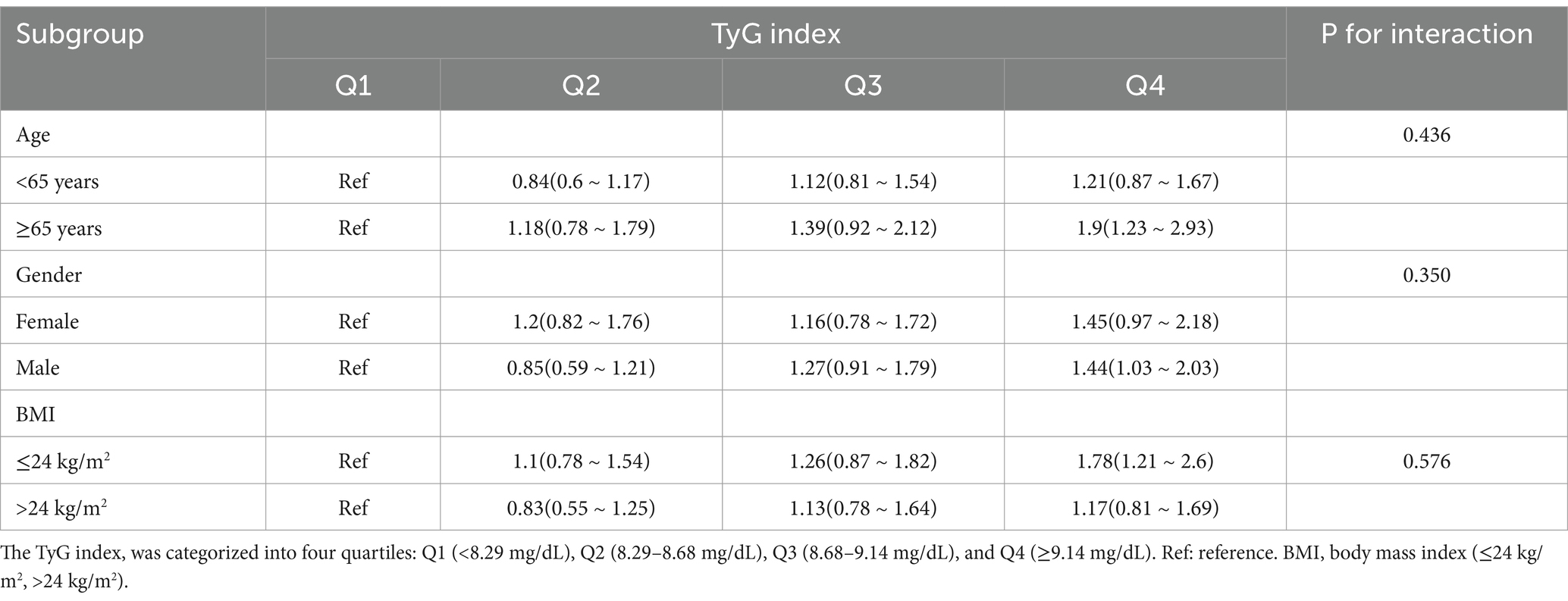
Table 3. Subgroup analysis of frailty with TyG index.
5 Discussion
In this large-scale, cross-sectional study, we investigated the association between the TyG index and frailty in middle-aged and older Chinese individuals for the first time. The study revealed that 16.8% of participants experienced frailty. After adjusting for confounding factors, individuals in the highest quartile (Q4) of the TyG index showed a 1.43 times higher risk of frailty compared to those in the lowest quartile (Q1), indicating a positive association between elevated TyG index levels and increased frailty occurrence. This association was further supported by the RSC analysis, which demonstrated a linear positive correlation between the TyG index and the risk of frailty development. In the subgroup analysis, there was no interaction observed between gender, age, and BMI with the TyG index, indicating consistent effects across diverse subgroups and thereby strengthening the generalizability and reliability of the study findings.
The current research results suggest a positive association between an increase in the TyG index and the occurrence of frailty, aligning closely with previous study outcomes. Among urban older residents aged 60 and above in a specific region of China, findings from a prospective cohort study suggest that an elevated TyG index and a consistently high trajectory of the TyG index are associated with an increased vulnerability to frailty (29). A recent cross-sectional study of individuals aged 50 and above in the United States revealed a positive association between the elevated TyG index and its related indices with a higher prevalence of frailty (30). There is a lack of research on the correlation between the TyG index and frailty. Previous studies have not determined the link between the TyG index and frailty in the older Chinese population due to geographical and racial diversity constraints. This study used the CHARLS database covering 28 provinces in China. With a sample of 23,000 participants from 12,400 households representing various urban and rural populations, the study aimed to explore the relationship between the TyG index and frailty risk among middle-aged and older individuals in China.
Frailty in the older is characterized by systemic dysregulation affecting multiple systems, leading to reduced physiological reserves, decreased stress resilience, and compromised recovery capacity, highlighting its importance as a significant geriatric syndrome (35, 36). The decline in muscle mass or strength among older adults significantly contributes to frailty. Prior research has suggested that a high TyG index poses a risk for reduced muscle mass or strength, especially in young and middle-aged individuals with hypertension (21, 37). There is a nonlinear correlation between the TyG index and sarcopenia in populations without metabolic syndrome or diabetes and with inadequate physical activity. Li et al. assessed the relationship between TyG index and low skeletal muscle mass and found a significant independent interaction regardless of age and gender (38).
The development and progression of frailty in the older can be affected by numerous factors, with the simultaneous presence of multiple diseases being a key risk factor that speeds up the onset of frailty (39). The TyG index, serving as a reliable surrogate biomarker for IR, is a critical metabolic parameter with demonstrated high specificity and sensitivity in the assessment and prediction of conditions such as hypertension, diabetes, and cardiovascular diseases (21, 22, 26). An increased risk of hypertension is linked to elevated TyG index and its long-term trajectory (40, 41), with the TyG index demonstrating superior predictive value for type 2 diabetes compared to fasting blood glucose and glycated hemoglobin (21, 25, 27). Furthermore, the TyG index is connected to the occurrence of microvascular complications in diabetes (42). The TyG index plays a critical role in the development, advancement, and prediction of cardiovascular diseases, as elevated TyG levels are associated with negative results in individuals with coronary artery disease and increased mortality rates in heart failure patients (26, 40, 43). Age is a non-modifiable factor that impacts the progression of frailty, as bodily systems deteriorate over time, leading to diminished muscle strength, cognitive capacity, and sensory functions, consequently heightening frailty susceptibility (1, 7, 44).
The potential mechanisms underlying the relationship between the TyG index and frailty remain unclear and may involve several mediating factors, including the following: (1) Skeletal muscle serves as the main location for insulin-mediated glucose metabolism (45). Aging, accompanied by diminishing hormone levels and decreased physical activity, induces a decline in skeletal muscle mass and a progressive impairment in peripheral glucose uptake capacity. Consequently, this sequence of events culminates in hyperinsulinemia and the development of IR. Elevated TyG index, utilized as a proxy for IR, may stem from decreased responsiveness to insulin, thereby influencing glucose and fatty acid metabolism, weakening proteolysis in skeletal muscles, disrupting muscle catabolism and quality, and ultimately leading to muscle loss and frailty (2, 12, 24). (2) An increase in the TyG index is correlated with increased levels of chronic inflammation and oxidative stress in the body, causing harm to cells and tissues, impeding the body’s repair and regeneration abilities, thus facilitating the progression of frailty (46–48).
This study reveals a positive linear correlation between the TyG index and frailty, offering a novel perspective for clinical practice. The TyG index is a cost-effective clinical parameter that requires only fasting blood glucose and triglyceride levels from routine tests. It is useful for screening high-risk populations, especially older individuals vulnerable to frailty. Early identification using the TyG index enables healthcare providers to initiate timely interventions and health managements to delay or prevent frailty onset. For patients with elevated TyG index values, personalized intervention plans can be devised, including lifestyle modifications (dietary adjustments and increased physical activity), along with targeted health education and lifestyle counseling to enhance metabolic health and reduce frailty risk. Monitoring changes in the TyG index during follow-up assessments facilitates the evaluation of intervention effectiveness and enables prompt adjustments to treatment and care plans.
6 Strengths and limitations
In this pioneering study on middle-aged and older individuals in China, we examined the link between the TyG index and frailty for the first time. Our cross-sectional analysis found a significant positive correlation between higher TyG index levels and frailty occurrence, which remained robust after adjusting for age, gender, lifestyle variables, and biochemical markers.
However, this study is subject to limitations. Firstly, this cross-sectional study does not enable the establishment of a causal relationship between the TyG index and frailty. Secondly, the evaluation of frailty is based on survey data, which can be susceptible to information bias. Lastly, while attempts are made to address confounding factors, it is difficult to entirely exclude their influence on the study findings.
7 Conclusion
To summarize, a direct linear association is evident between the TyG index and the vulnerability to frailty in the older. An increased risk of frailty is evident in older adults with higher TyG index levels. It is crucial to promptly counsel individuals in this group to adopt lifestyle modifications to prevent and postpone the onset or advancement of frailty.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Ethics statement
The studies involving humans were approved by Institutional Review Board for Biomedical Ethics of Peking University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
QL: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. YLi: Data curation, Methodology, Writing – original draft. ZS: Data curation, Methodology, Writing – original draft. YLe: Funding acquisition, Resources, Validation, Visualization, Writing – review & editing. LM: Funding acquisition, Resources, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We are very grateful to the National School of Development at Peking University and the China Social Science Survey Center at Peking University for providing the CHARLS data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1548222/full#supplementary-material
Footnotes
References
1. Clegg, A, Young, J, Iliffe, S, Rikkert, MO, and Rockwood, K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
2. Franceschi, C, Garagnani, P, Vitale, G, Capri, M, and Salvioli, S. Inflammaging and ‘Garb-aging’. Trends Endocrinol Metab. (2017) 28:199–212. doi: 10.1016/j.tem.2016.09.005
3. Gordon, EH, and Hubbard, RE. Frailty: understanding the difference between age and ageing. Age Ageing. (2022) 51:afac185. doi: 10.1093/ageing/afac185
4. Chinese Geriatrics Society EBoCJoG. Chinese expert consensus on prevention of frailty in the elderly. Chin J Geriatr. (2022) 41:503–11. doi: 10.3760/cma.j.issn.0254-9026.2022.05.001
5. Ya, ZYZZF. Study on the status of frailty and related determinants among the elderly in China. Chin. J Epidemiol. (2018) 39:1244–8. doi: 10.3760/cma.j.issn.0254-6450.2018.09.019
6. O’Caoimh, R, Sezgin, D, O’Donovan, MR, Molloy, DW, Clegg, A, Rockwood, K, et al. Prevalence of frailty in 62 countries across the world: a systematic review and meta-analysis of population-level studies. Age Ageing. (2021) 50:96–104. doi: 10.1093/ageing/afaa219
7. Dent, E, Martin, FC, Bergman, H, Woo, J, Romero-Ortuno, R, and Walston, JD. Management of frailty: opportunities, challenges, and future directions. Lancet. (2019) 394:1376–86. doi: 10.1016/S0140-6736(19)31785-4
8. Dlima, SD, Hall, A, Aminu, AQ, Akpan, A, Todd, C, and Vardy, ERLC. Frailty: a global health challenge in need of local action. BMJ. Glob Health. (2024) 9:e015173. doi: 10.1136/bmjgh-2024-015173
9. Hoogendijk, EO, Afilalo, J, Ensrud, KE, Kowal, P, Onder, G, and Fried, LP. Frailty: implications for clinical practice and public health. Lancet. (2019) 394:1365–75. doi: 10.1016/S0140-6736(19)31786-6
10. Cruz-Jentoft, AJ, Bahat, G, Bauer, J, Boirie, Y, Bruyère, O, Cederholm, T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. (2019) 48:16–31. doi: 10.1093/ageing/afy169
11. Larsson, L, Degens, H, Li, M, Salviati, L, Yi, L, Thompson, W, et al. Sarcopenia: aging-related loss of muscle mass and function. Physiol Rev. (2019) 99:427–511. doi: 10.1152/physrev.00061.2017
12. Consitt, LA, and Clark, BC. The vicious cycle of Myostatin signaling in Sarcopenic obesity: Myostatin role in skeletal muscle growth, insulin signaling and implications for clinical trials. J Frailty Aging. (2017) 7:21–7. doi: 10.14283/jfa.2017.33
13. Haines, MS, Dichtel, LE, Santoso, K, Torriani, M, Miller, KK, and Bredella, MA. Association between muscle mass and insulin sensitivity independent of detrimental adipose depots in young adults with overweight/obesity. Int J Obes. (2020) 44:1851–8. doi: 10.1038/s41366-020-0590-y
14. Kim, CH, Kim, HK, Kim, EH, Bae, SJ, Choe, J, and Park, JY. Longitudinal changes in insulin resistance, Beta-cell function and glucose regulation status in prediabetes. Am J Med Sci. (2018) 355:54–60. doi: 10.1016/j.amjms.2017.09.010
15. Wang, T, Lu, J, Shi, L, Chen, G, Xu, M, Xu, Y, et al. Association of insulin resistance and β-cell dysfunction with incident diabetes among adults in China: a nationwide, population-based, prospective cohort study. Lancet Diabetes Endocrinol. (2020) 8:115–24. doi: 10.1016/S2213-8587(19)30425-5
16. Keane, KN, Cruzat, VF, Carlessi, R, de Bittencourt, PI, and Newsholme, P. Molecular events linking oxidative stress and inflammation to insulin resistance and β-cell dysfunction. Oxidative Med Cell Longev. (2015) 2015:181643:1–15. doi: 10.1155/2015/181643
17. Rehman, K, and Akash, MSH. Mechanisms of inflammatory responses and development of insulin resistance: how are they interlinked? J Biomed Sci. (2016) 23:87. doi: 10.1186/s12929-016-0303-y
18. Ahn, S-H, Lee, J-H, and Lee, J-W. Inverse association between triglyceride glucose index and muscle mass in Korean adults: 2008–2011 KNHANES. Lipids Health Dis. (2020) 19:243. doi: 10.1186/s12944-020-01414-4
19. Chen, Z, and Wen, J. Elevated triglyceride-glucose (TyG) index predicts impaired islet β-cell function: a hospital-based cross-sectional study. Front Endocrinol. (2022) 13:13. doi: 10.3389/fendo.2022.973655
20. Sánchez-García, A, Rodríguez-Gutiérrez, R, Mancillas-Adame, L, González-Nava, V, Díaz González-Colmenero, A, Solis, RC, et al. Diagnostic accuracy of the triglyceride and glucose index for insulin resistance: a systematic review. Int J Endocrinol. (2020) 2020:4678526. doi: 10.1155/2020/4678526
21. Zhao, Q, Zhang, Z, Li, S, and Liu, M. Triglyceride-glucose index levels positively associated with higher risk of low muscle mass in patients with type 2 diabetes. Diabetes Metab Syndr Obes. (2024) 17:3355–63. doi: 10.2147/DMSO.S479900
22. Simental-Mendía, LE, Rodríguez-Morán, M, and Guerrero-Romero, F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. (2008) 6:299–304. doi: 10.1089/met.2008.0034
23. Chen, J, Wu, K, Lin, Y, Huang, M, and Xie, S. Association of triglyceride glucose index with all-cause and cardiovascular mortality in the general population. Cardiovasc Diabetol. (2023) 22:320. doi: 10.1186/s12933-023-02054-5
24. Siew, ED, Pupim, LB, Majchrzak, KM, Shintani, A, Flakoll, PJ, and Ikizler, TA. Insulin resistance is associated with skeletal muscle protein breakdown in non-diabetic chronic hemodialysis patients. Kidney Int. (2007) 71:146–52. doi: 10.1038/sj.ki.5001984
25. Teng, Z, Feng, J, Dong, Y, Xu, J, Jiang, X, Chen, H, et al. Triglyceride glucose index is associated with cerebral small vessel disease burden and cognitive impairment in elderly patients with type 2 diabetes mellitus. Front Endocrinol. (2022) 13:970122. doi: 10.3389/fendo.2022.970122
26. Wang, Y, Chen, X, Shi, J, Du, M, Li, S, Pang, J, et al. Relationship between triglyceride-glucose index baselines and trajectories with incident cardiovascular diseases in the elderly population. Cardiovasc Diabetol. (2024) 23:6. doi: 10.1186/s12933-023-02100-2
27. Zheng, J, Zhang, L, and Jiang, M. Lower handgrip strength levels probably precede triglyceride glucose index and associated with diabetes in men not in women. J Diab Invest. (2021) 13:148–55. doi: 10.1111/jdi.13626
28. Pan, R, Wang, T, Tang, R, and Qian, Z. Association of atherogenic index of plasma and triglyceride glucose-body mass index and sarcopenia in adults from 20 to 59: a cross-sectional study. Front Endocrinol. (2024) 15:1437379. doi: 10.3389/fendo.2024.1437379
29. Yuan, Y, Chen, S, Lin, C, Huang, X, Lin, S, Huang, F, et al. Association of triglyceride-glucose index trajectory and frailty in urban older residents: evidence from the 10-year follow-up in a cohort study. Cardiovasc Diabetol. (2023) 22:264. doi: 10.1186/s12933-023-02002-3
30. Yin, H, Guo, L, Zhu, W, Li, W, Zhou, Y, Wei, W, et al. Association of the triglyceride-glucose index and its related parameters with frailty. Lipids Health Dis. (2024) 23:150. doi: 10.1186/s12944-024-02147-4
31. Zhao, Y, Hu, Y, Smith, JP, Strauss, J, and Yang, G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. (2012) 43:61–8. doi: 10.1093/ije/dys203
32. Feenstra, M, Oud, FMM, Jansen, CJ, Smidt, N, van Munster, BC, and de Rooij, SE. Reproducibility and responsiveness of the frailty index and frailty phenotype in older hospitalized patients. BMC Geriatr. (2021) 21:499. doi: 10.1186/s12877-021-02444-y
33. Searle, SD, Mitnitski, A, Gahbauer, EA, Gill, TM, and Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. (2008) 8:24. doi: 10.1186/1471-2318-8-24
34. Fan, J, Yu, C, Guo, Y, Bian, Z, Sun, Z, Yang, L, et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: a prospective cohort study. Lancet Public Health. (2020) 5:e650–60. doi: 10.1016/S2468-2667(20)30113-4
35. Kato, N, Kimoto, A, Zhang, P, Bumrungkit, C, Karunaratne, S, Yanaka, N, et al. Relationship of low vitamin B6 status with sarcopenia, frailty, and mortality: a narrative review. Nutrients. (2024) 16:177. doi: 10.3390/nu16010177
36. Ye, L, Liang, R, Liu, X, Li, J, Yue, J, and Zhang, X. Frailty and sarcopenia: a bibliometric analysis of their association and potential targets for intervention. Ageing Res Rev. (2023) 92:102111. doi: 10.1016/j.arr.2023.102111
37. Chen, R, Zhang, L, Zhang, M, Wang, Y, Liu, D, Li, Z, et al. The triglyceride-glucose index as a novel marker associated with sarcopenia in non-diabetic patients on maintenance hemodialysis. Ren Fail. (2022) 44:1616–22. doi: 10.1080/0886022X.2022.2128373
38. Li, Z, Tong, X, Ma, Y, Bao, T, and Yue, J. Association between the triglyceride glucose index and low skeletal muscle mass: a cross-sectional study. BMJ Open. (2024) 14:e077484. doi: 10.1136/bmjopen-2023-077484
39. Fried, LP, Ferrucci, L, Darer, J, Williamson, JD, and Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. (2004) 59:255–63. doi: 10.1093/gerona/59.3.m255
40. Che, B, Zhong, C, Zhang, R, Pu, L, Zhao, T, Zhang, Y, et al. Triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio as potential cardiovascular disease risk factors: an analysis of UK biobank data. Cardiovasc Diabetol. (2023) 22:34. doi: 10.1186/s12933-023-01762-2
41. Xin, F, He, S, Zhou, Y, Jia, X, Zhao, Y, and Zhao, H. The triglyceride glucose index trajectory is associated with hypertension: a retrospective longitudinal cohort study. Cardiovasc Diabetol. (2023) 22:347. doi: 10.1186/s12933-023-02087-w
42. Zhang, Q, Xiao, S, Jiao, X, and Shen, Y. The triglyceride-glucose index is a predictor for cardiovascular and all-cause mortality in CVD patients with diabetes or pre-diabetes: evidence from NHANES 2001-2018. Cardiovasc Diabetol. (2023) 22:279. doi: 10.1186/s12933-023-02030-z
43. Dang, K, Wang, X, Hu, J, Zhang, Y, Cheng, L, Qi, X, et al. The association between triglyceride-glucose index and its combination with obesity indicators and cardiovascular disease: NHANES 2003–2018. Cardiovasc Diabetol. (2024) 23:8. doi: 10.1186/s12933-023-02115-9
44. Veronese, N, Custodero, C, Cella, A, Demurtas, J, Zora, S, Maggi, S, et al. Prevalence of multidimensional frailty and pre-frailty in older people in different settings: a systematic review and meta-analysis. Ageing Res Rev. (2021) 72:101498. doi: 10.1016/j.arr.2021.101498
45. Jin, L, Han, S, Lv, X, Li, X, Zhang, Z, Kuang, H, et al. The muscle-enriched myokine Musclin impairs beige fat thermogenesis and systemic energy homeostasis via Tfr1/PKA signaling in male mice. Nat Commun. (2023) 14:4257. doi: 10.1038/s41467-023-39710-z
46. Khalaji, A, Behnoush, AH, Khanmohammadi, S, Ghanbari Mardasi, K, Sharifkashani, S, Sahebkar, A, et al. Triglyceride-glucose index and heart failure: a systematic review and meta-analysis. Cardiovasc Diabetol. (2023) 22:244. doi: 10.1186/s12933-023-01973-7
47. Tao, LC, Xu, JN, Wang, TT, Hua, F, and Li, JJ. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. (2022) 21:68. doi: 10.1186/s12933-022-01511-x
Keywords: frailty, frailty index, middle-aged and older adults, triglycerides-glucose index, CHARLS
Citation: Long Q, Li Y, Shi Z, Lee Y and Mao L (2025) Investigation of the association between the triglyceride-glucose index and the incidence of frailty among middle-aged and older adults: evidence from the China health and retirement longitudinal study. Front. Public Health. 13:1548222. doi: 10.3389/fpubh.2025.1548222
Edited by:
Marios Kyriazis, National Gerontology Centre, CyprusReviewed by:
Barbara Ciastek, University of Opole, PolandJiling Liang, Central South University, China
Copyright © 2025 Long, Li, Shi, Lee and Mao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yujun Lee, c2FtbXlsZWVlQDE2My5jb20=; Lifang Mao, Mzk4NDg0MTgyQHFxLmNvbQ==