 Matteo Marconi1†
Matteo Marconi1† Ughetta Maria Favazzi2†
Ughetta Maria Favazzi2† Pietro Carbone2
Pietro Carbone2 Debora Guerrera2
Debora Guerrera2 Angela Ruocco1
Angela Ruocco1 Martina Manoli1,3Cristiana Barbati4
Martina Manoli1,3Cristiana Barbati4 Francesca Molinaro2
Francesca Molinaro2 Federica Maria Regini2
Federica Maria Regini2 Andrea Vittozzi2
Andrea Vittozzi2 Alfonso Mazzaccara2
Alfonso Mazzaccara2 Marina Pierdominici1*
Marina Pierdominici1*- 1Reference Centre for Gender Medicine, Istituto Superiore di Sanità, Rome, Italy
- 2Training Office, Istituto Superiore di Sanità, Rome, Italy
- 3Department of Medical and Surgical Sciences and Advanced Technologies “GF Ingrassia”, University of Catania, Catania, Italy
- 4Department of Infectious Diseases, Istituto Superiore di Sanità, Rome, Italy
Introduction: Transgender and gender-diverse (TGD) individuals face significant health disparities, often due to healthcare providers’ (HCPs) insufficient training and awareness. Comprehensive educational interventions are essential to improve both cultural competence and medical knowledge. While previous evaluations of training programs have shown short-term benefits, evidence on long-term outcomes remains scarce. This study extends the findings of an earlier evaluation of a distance learning course on TGD healthcare, exploring the sustainability of its effects over time.
Objectives: To assess changes in self-reported attitudes, skills, practices, and knowledge retention 6 months after course completion.
Methods: A longitudinal design was used with assessments at baseline (T0), post-course (T1), and six-month follow-up (T2). Participants completed the Attitudes, Skills, and Practices Questionnaire (ASPQ) and a 10-item knowledge test at all time points. Paired t-tests were used to compare mean scores for attitudes and skills. Knowledge retention was analyzed with McNemar tests. Changes in practice items were evaluated using Cochran’s Q and Friedman tests for paired categorical data.
Results: A total of 3,102 participants (17% of the original cohort) completed the follow-up. All self-reported skills and most attitudes improved significantly from baseline to follow-up (p < 0.001 for skills; p ≤ 0.02 for attitudes), with modest declines from T1. Practice items showed significant variation over time (Cochran’s Q and Friedman tests, p < 0.001), though without a consistent increase in engagement. Knowledge improved in 8 of 10 items from baseline to follow-up (McNemar, p < 0.001), particularly in sexual identity, hormone therapy, and legal rights, despite partial declines from post-course levels.
Conclusion: This study highlights sustained improvements in self-reported attitudes, skills, and knowledge following a national TGD healthcare training, reinforcing its value in addressing health disparities. The findings underscore the need for structural support and integrated reinforcement to embed gender-affirming care into routine practice.
1 Introduction
Transgender and gender-diverse (TGD) individuals experience significant health disparities, often exacerbated by stigma, discrimination, and insufficient knowledge among healthcare professionals (HCPs) (1–4). Comprehensive training for HCPs is a crucial step in addressing these barriers and fostering equitable, gender-affirming care (5). Evidence suggests that educational interventions can positively impact HCPs’ knowledge, attitudes, and competencies in TGD healthcare. However, much of the existing research has focused on short-term outcomes, often measured immediately after training, with limited attention to the long-term retention of these improvements (6, 7). Longitudinal studies are essential to determine whether initial gains persist over time and translate into sustainable changes in clinical practice. The few available longitudinal evaluations of TGD health education for HCPs are often limited by small sample sizes or restricted to specific institutional settings (8–14), leaving a critical gap in the literature. This study builds upon our earlier work, which evaluated the impact of a 16-h, Continuing Medical Education (CME) accredited distance learning course on TGD health (15). The course encompassed a broad array of topics, including effective communication strategies, preventive care and lifestyle considerations, medical pathways for gender affirmation, and legal aspects of TGD healthcare. The initial results demonstrated significant improvements in participants’ knowledge and high levels of satisfaction. The current study examines six-month follow-up outcomes, focusing on self-reported attitudes, skills, practices, and knowledge retention, among over 3,000 participants. To the best of our knowledge, this investigation represents the largest longitudinal study in the field to date, providing valuable insights into the durability of training outcomes and the potential for large-scale educational interventions to drive systemic change in healthcare practices.
2 Materials and methods
2.1 Course design, learning methodology, and participant overview
The distance learning course, “Transgender Population: From Health to Rights,” was freely offered through the Istituto Superiore di Sanità (ISS)—National Institute of Health in Italy e-learning platform (EDUISS, www.eduiss.it) and delivered entirely in Italian. Details of this course have been published previously (15). It employed a Problem-Based Learning (PBL) framework, a methodology rooted in andragogic principles that fosters self-directed learning by engaging participants in solving real-world problems pertinent to their professional domains (16). The PBL methodology was adapted for e-learning, allowing participants to independently complete a structured seven-step cycle supported by interactive tools such as forums, quizzes, and curated resource materials.
A scientific board comprising experts in TGD healthcare, legal scholars, and representatives from TGD advocacy organizations designed this pioneering course. The curriculum systematically addressed critical areas of TGD care, including:
• Biological underpinnings of sexual identity.
• Psychological support spanning developmental and adult stages.
• Evidence-based approaches to hormone therapy.
• Core principles and practices in gender-affirmation surgery.
• Legal frameworks governing gender identity rights in Italy.
These topics were distilled into five targeted Learning Objectives (LOs). The course was accessible to all healthcare professionals and ran from March 27 to September 22, 2023, with a participant capacity of up to 30,000. Upon successful completion, participants earned 16 CME credits, requiring approximately 16 h of engagement. In accordance with current Italian and European Union regulations, this type of non-interventional educational study did not require formal approval by an ethics committee. Participation was voluntary, and informed consent for the use of pseudonymized data was obtained from all participants at the time of course registration.
The course was systematically divided into four sections:
1. Introductory section
a. This section provided a comprehensive overview, outlining the course’s relevance, objectives, structure, and intended goals. Participants received detailed guidelines to facilitate their participation.
b. It included the Attitudes, Skills, and Practices Questionnaire (ASPQ) at baseline (T0) and a Multiple Choice Question (MCQ) knowledge assessment test to assess prior knowledge (pre-test). No minimum score was required for pre-test completion.
2. PBL cycle
This section provided an array of resources to support the PBL cycle. These included problem scenarios, a Sharable Content Object Reference Model (SCORM) exercise for problem analysis and identification of LOs, research materials (e.g., bibliographic references, recommended websites, specialized readings, and expert-led audio-video tutorials), and activities for problem resolution.
3. Concluding section
a. Participants completed the ASPQ at T1 (immediate post-course) and the same MCQ knowledge assessment test used in the pre-test to evaluate knowledge acquisition (post-test). This section concluded with a final certification exam and an optional Satisfaction Questionnaire (SQ).
b. The SQ was available exclusively to participants who finished all learning units. To qualify for CME credits, participants were required to pass the final exam, which consisted of 48 MCQs and required a minimum passing score of 75%. A maximum of three attempts was permitted.
4. Follow-up section
Six months post-course (T2), participants completed the follow-up administration of the ASPQ and repeated the same MCQ knowledge assessment test used at T0 and T1. Both were available from March 26 to May 20, 2024.
2.2 Data collection and tools
As part of the enrollment process for the advanced educational course hosted on the ISS e-learning platform, participants were required to provide demographic and professional details, including gender, age, geographic location, CME profession, and discipline. Two key tools were used throughout the study to establish a baseline and monitor progress over time:
1. ASPQ: the ASPQ is a purpose-built instrument developed specifically for this study, aligned with the course objectives. It was administered at three time points—T0 (baseline), T1 (immediate post-course), and T2 (six-month follow-up)—to assess changes over time. It consists of item batteries using Likert-scale formats across several domains:
a. Attitudes: five items rated on a 5-point Likert scale
b. Skills: five items rated on a 5-point Likert scale
c. Practices: four items, combining dichotomous and polytomous response formats
2. Knowledge assessment test: this test comprises 10 MCQs (two items per LO), designed to evaluate core conceptual knowledge aligned with the specific objectives of the course. The same version of this test was administered at three time points:
a. T0 (Pre-test): to establish a baseline prior to course access
b. T1 (Post-test): immediately after course completion, to assess knowledge acquisition
c. T2 (Follow-up): 6 months after course completion, to assess long-term knowledge retention
The SQ, administered only at T1, includes 18 items on a 5-point Likert scale and two open-ended questions aimed at evaluating course satisfaction and collecting suggestions for improvement.
The results of the knowledge assessment test at T0 and T1, as well as those of the SQ have been published previously (15). The present analysis focused on participants who successfully completed the course, passed the final certification, and voluntarily participated in the six-month follow-up phase. This cohort consisted of 3,102 individuals who completed both follow-up instruments (ASPQ and the knowledge assessment test), ensuring a robust dataset for longitudinal analysis.
2.3 Statistical analysis
All data were extracted from the EDUISS platform. A descriptive analysis, including absolute numbers and percentages, was performed to present demographic and professional characteristics.
To assess the psychometric properties of the Attitudes and Skills sections of the ASPQ, an Exploratory Factor Analysis (EFA) was performed at T0, T1, and T2 using principal axis factoring with Promax rotation. The analysis consistently revealed a two-factor structure aligned with the theoretical constructs of self-perceived skills (Items 1–5) and attitudes (Items 6–10). Internal consistency was evaluated using Cronbach’s alpha, which indicated high reliability across all three time points (Skills: α = 0.897–0.914; Attitudes: α = 0.862–0.918).
The Practices section was excluded from these psychometric analyses because it consists of one dichotomous item and three ordinal items with five response options. Due to their categorical nature and heterogeneity, these items were analyzed descriptively.
The Likert-scale data from the ASPQ, focusing on Attitudes and Skills, were analyzed using two approaches: (1) frequency distributions of responses were examined at T0, T1, and T2; (2) paired t-tests were conducted to compare mean scores between T0 and T2 and T1 and T2, to identify statistically significant differences. Changes in responses to the Practices items over time were assessed using non-parametric tests suitable for paired data. For the dichotomous item assessing whether participants had ever provided care to TGD individuals, Cochran’s Q test was used to assess differences across T0, T1, and T2. For the three ordinal items related to family engagement and the provision of information on gender-affirming care and legal aspects, Friedman tests were conducted to evaluate changes in response distributions over time. Results from the knowledge assessment test at T0, T1 and T2 were expressed as the percentage of correct answers for each question and compared using the McNemar’s test.
All statistical analyses were performed using IBM SPSS Statistics version 28.0. Statistical significance was set at p < 0.05.
3 Results
3.1 Characteristics of participants
The study population refers to a broader group of 18,282 individuals who completed the course, as described in a previous study (15). The current analysis included 3,102 healthcare professionals. The majority of participants were female (73.9%), while 26.1% were male. The participants’ mean age was 49.6 years (SD 10.3), and the age group most represented was 46 to 55 years (38.5%), followed by those over 55 years (32.1%). Younger professionals, specifically those up to 35 years, accounted for only 13.1% of the sample.
In terms of geographical distribution, the Northwest region of Italy had the highest participation, with 35.4% of individuals coming from this area. The Center followed with 23.9%, while the South and the Islands accounted for 15.6 and 10.0%, respectively. Professionally, the participants came from a variety of healthcare roles. Nurses represented 47.8% of the sample, making them the largest professional group among the participants. These results are reported in Table 1.
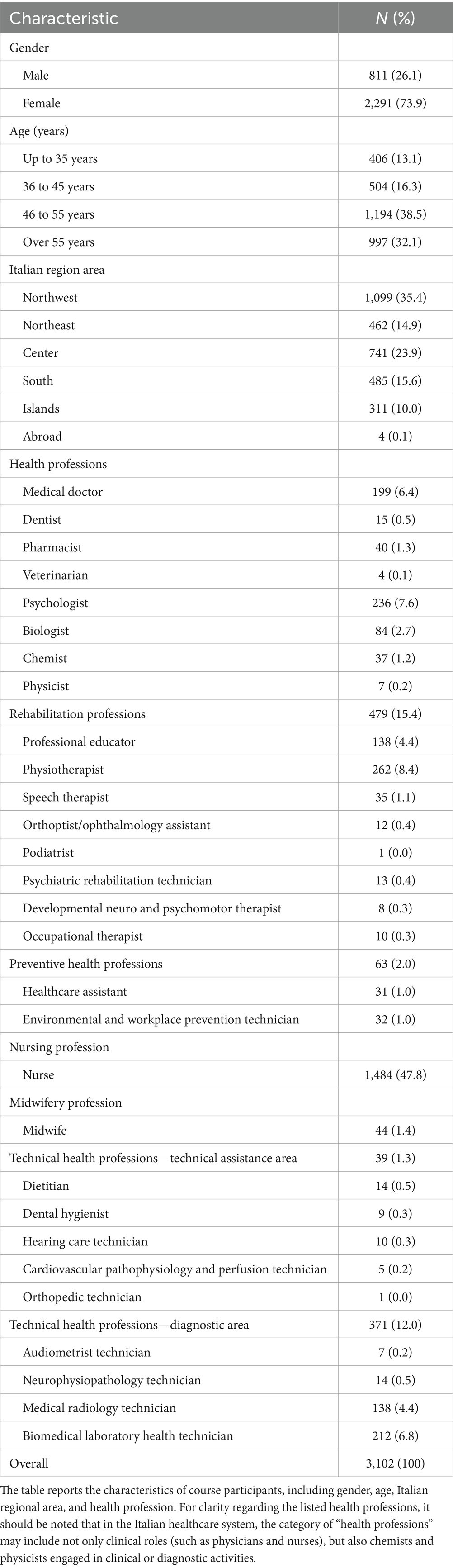
Table 1. Characteristics of participants.
3.2 Changes in self-reported attitudes
The results, presented in Table 2 as mean scores and in Supplementary Table 1 as percentage distributions across the Likert scale, indicate significant changes over time in participants’ beliefs regarding the care of TGD individuals.
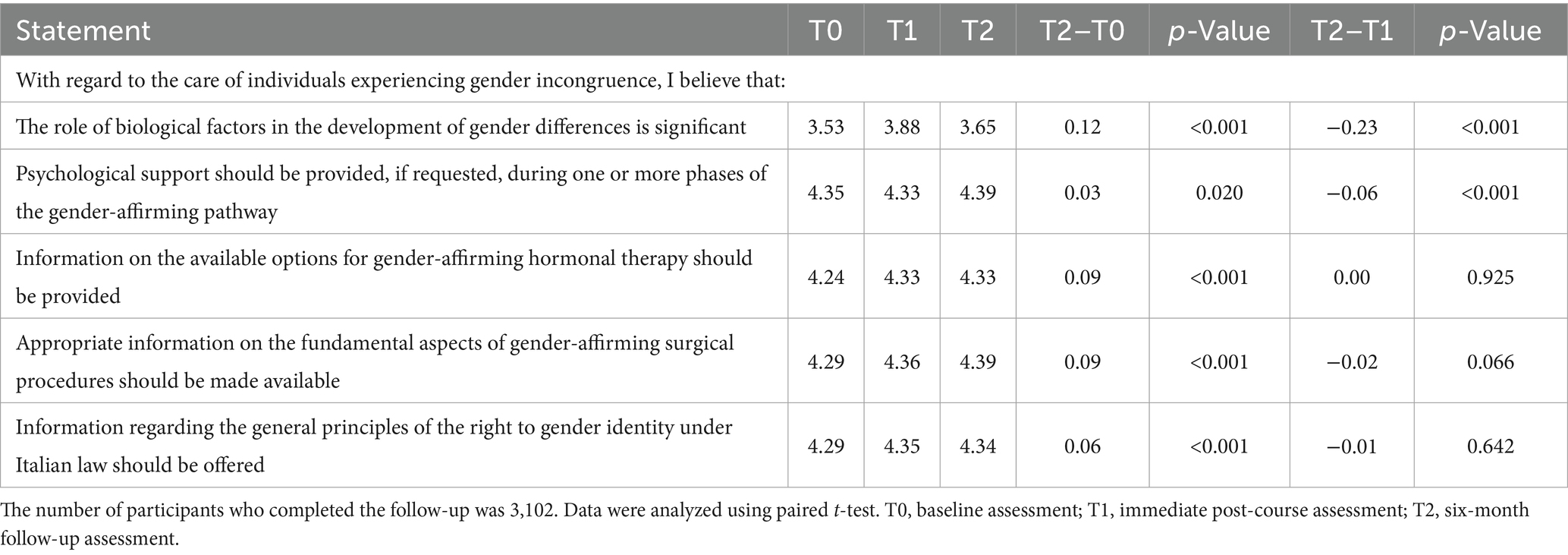
Table 2. Self-reported attitudes toward the care of TGD individuals.
Regarding the belief that the role of biological factors in the development of gender differences is relevant, the mean score increased from 3.53 at T0 to 3.88 at T1 and slightly decreased to 3.65 at T2, with a mean difference of 0.12 between T0 and T2 (p < 0.001). For the belief that psychological support should be provided, if required, during one or more stages of the gender-affirming treatment, scores remained high, increasing slightly from 4.35 at T0 to 4.39 at T2, with a mean difference of 0.03 between T0 and T2 (p = 0.020).
The belief that individuals should be informed on possible gender-affirming hormone therapy options showed a slight increase from 4.24 at T0 to 4.33 at T1 and T2, with a mean difference of 0.09 between T0 and T2 (p < 0.001). Similarly, for the belief that appropriate information should be provided on the key aspects of gender-affirming surgery, the mean score increased from 4.29 at T0 to 4.36 at T1 and further to 4.39 at T2, with a mean difference of 0.09 between T0 and T2 (p < 0.001). Finally, regarding the belief that information should be provided on the general principles of the right to gender identity in Italian law, the mean score increased slightly from 4.29 at T0 to 4.35 at T1 and slightly decreased to 4.34 at T2, with a mean difference of 0.06 between T0 and T2 (p < 0.001). In summary, the findings demonstrate meaningful changes in beliefs regarding the care of TGD individuals, with small but statistically significant differences observed between baseline (T0) and follow-up (T2). Comparisons between T1 and T2 showed minimal or small variations, some of which reached statistical significance but were limited in magnitude, indicating that attitudes were generally sustained over time.
3.3 Changes in self-reported skills
The results, presented in Table 3 as mean scores and in Supplementary Table 2 as percentage distributions across the Likert scale, indicate significant changes over time in participants’ self-reported capabilities. Regarding the ability to describe the components of sexual identity, the mean score increased from 2.70 at T0 to 3.72 at T1, then slightly declined to 3.35 at T2, with a mean difference of 1.02 between T0 and T2 (p < 0.001). For the ability to recognize key aspects relevant to psychological support during both developmental stages and adulthood, the mean score rose from 2.70 at T0 to 3.77 at T1 and slightly decreased to 3.49 at T2, with a mean difference of 0.79 between T0 and T2 (p < 0.001). The ability to identify best practices for gender-affirming hormonal treatment across developmental stages and adulthood showed an increase in mean scores from 2.20 at T0 to 3.55 at T1, followed by a slight decline to 3.14 at T2, with a mean difference of 0.94 between T0 and T2 (p < 0.001). Similarly, the ability to define the fundamental principles underlying gender-affirming surgery rose from 2.18 at T0 to 3.61 at T1 and decreased to 3.24 at T2, with a mean difference of 1.06 between T0 and T2 (p < 0.001). Lastly, for the ability to outline the general principles governing the right to gender identity within the framework of Italian law, the mean score increased from 2.40 at T0 to 3.77 at T1, then slightly decreased to 3.37 at T2, with a mean difference of 0.98 between T0 and T2 (p < 0.001).
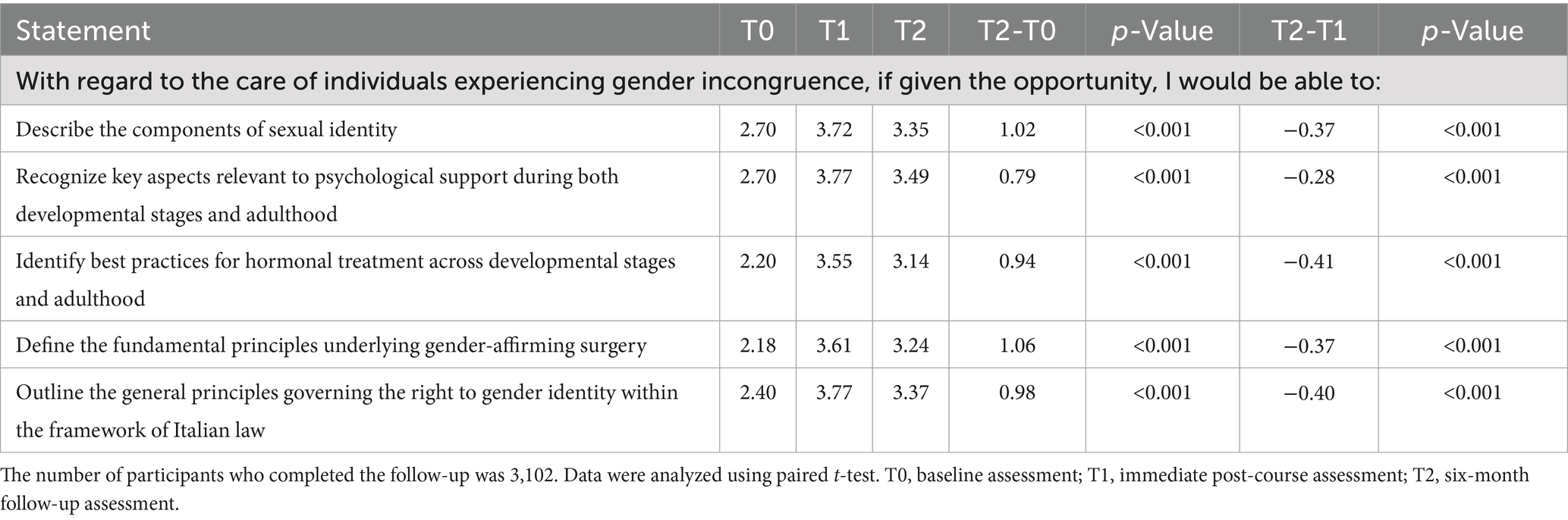
Table 3. Self-reported skills in the care of TGD individuals.
In summary, while all capabilities demonstrated a statistically significant decline at T2 compared to immediate post-course scores (T1), mean scores remained substantially higher than baseline (T0), indicating sustained improvement over time. These findings suggest that, despite some attenuation, self-reported competencies were meaningfully retained 6 months after course completion.
3.4 Changes in self-reported practices
The results, summarized in Table 4, indicate that the direct management of gender-affirming care remains a relatively uncommon component of clinical practice for most participants. Statistically significant variations over time were observed across the four self-reported practices assessed, although these did not uniformly reflect increased engagement. The proportion of respondents who reported having provided care to TGD individuals decreased from 33.0% at T0 to 31.7% at T1 and 28.2% at T2 (p < 0.001), possibly reflecting a more cautious or accurate interpretation of what constitutes gender-specific care following the training intervention. Responses concerning interactions with the families of TGD individuals changed significantly over time (p < 0.001), as did the frequency of providing information on gender-affirming pathways (p < 0.001) and on legal aspects of gender-affirming care (p < 0.001). These shifts in response distributions were statistically significant, but no consistent directional trend (e.g., toward more frequent engagement) was observed across time points.
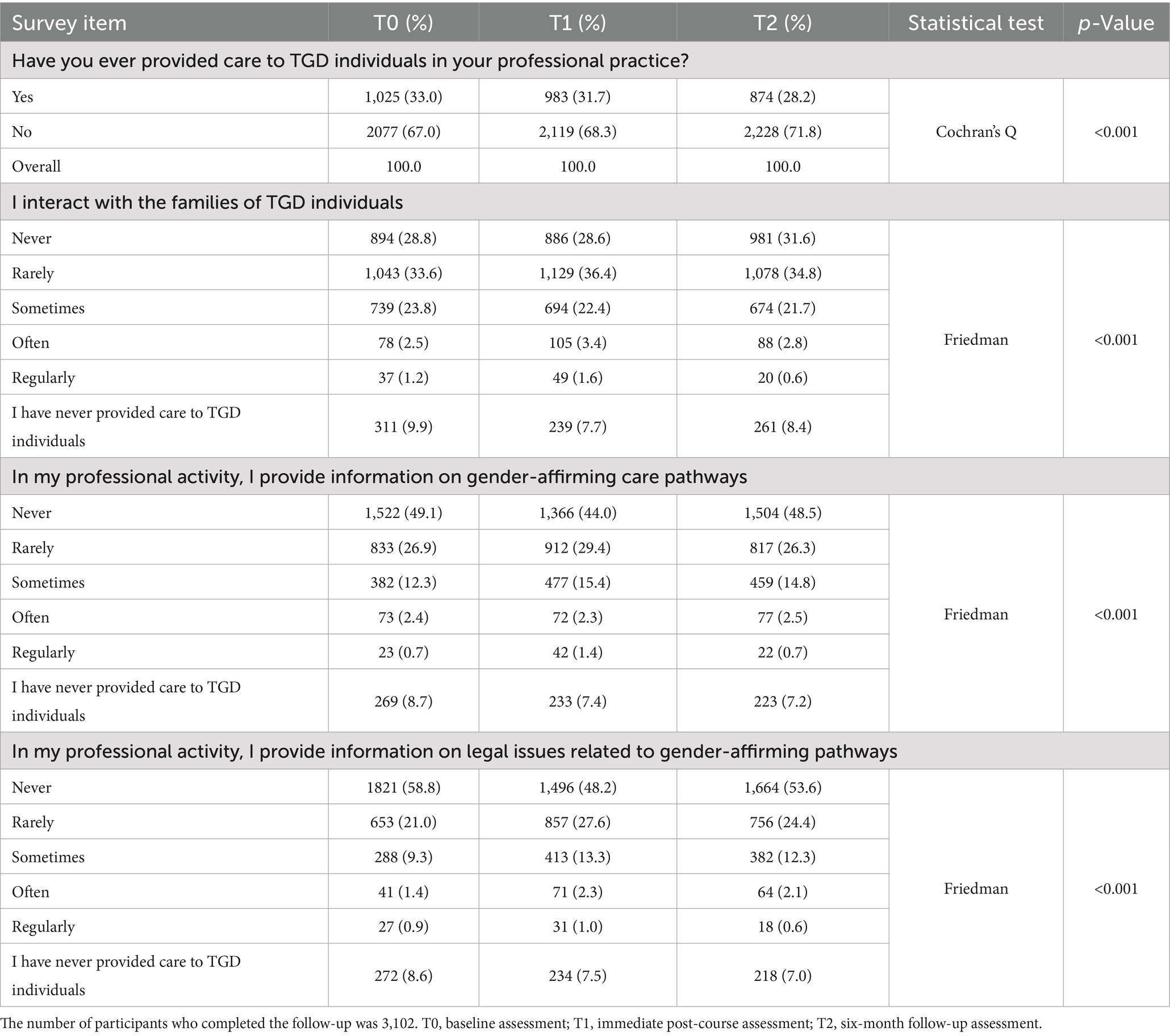
Table 4. Self-reported practices regarding TGD individuals.
3.5 Knowledge retention
The results, presented in Table 5 as percentages of correct answers at T0, T1, and T2, indicate significant changes in participants’ knowledge across all LOs.
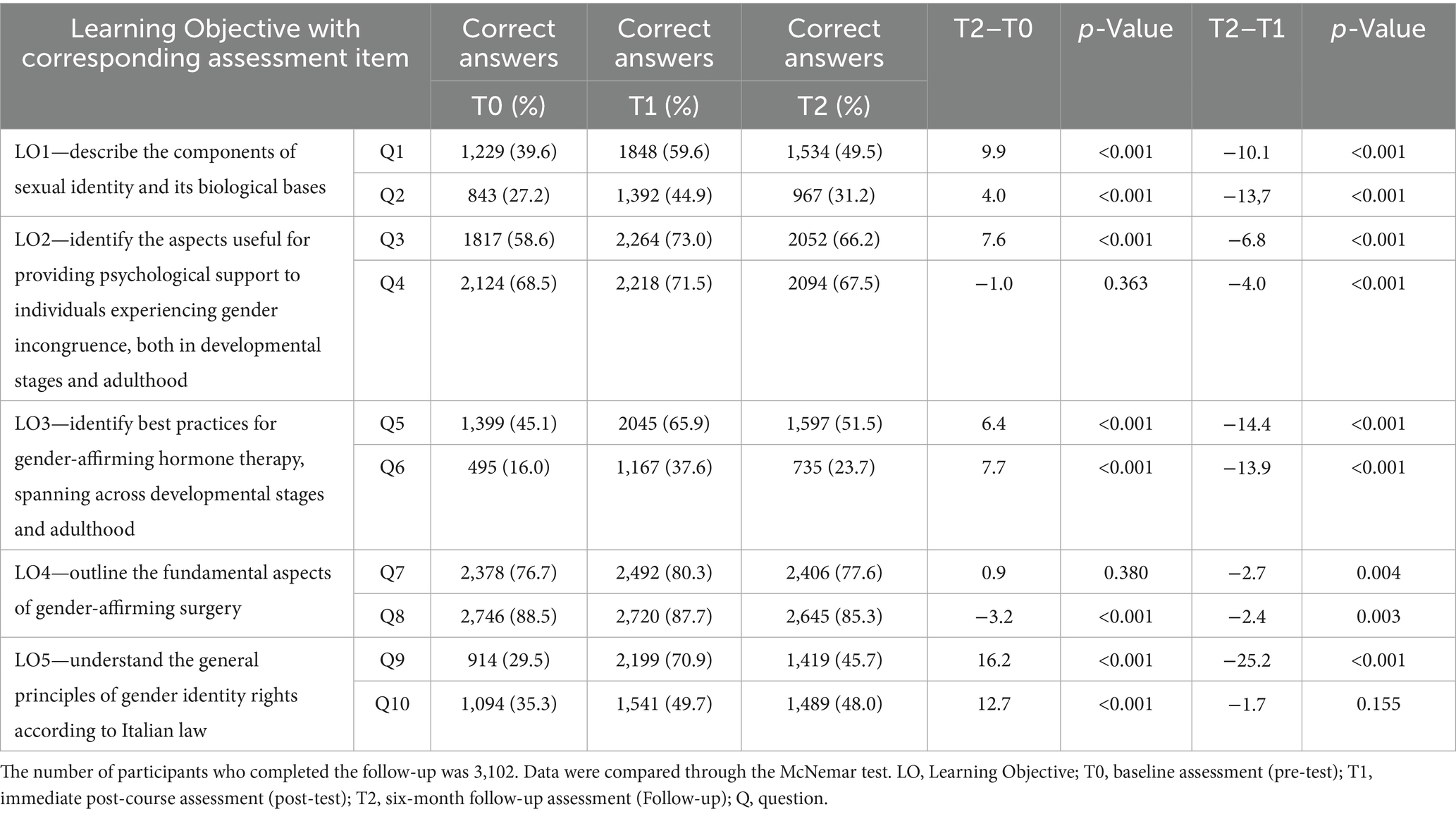
Table 5. Knowledge assessment test: retention over time.
For LO1: Describe the components of sexual identity and its biological bases, question Q1 showed an increase in correct responses from 39.6% at T0 to 59.6% at T1, followed by a decrease to 49.5% at T2, yielding a net gain of 9.9% between T0 and T2 (p < 0.001). Similarly, Q2 increased from 27.2% at T0 to 44.9% at T1, then decreased to 31.2% at T2, with a net gain of 4.0% between T0 and T2 (p < 0.001).
For LO2: Identify the aspects useful for providing psychological support, Q3 rose from 58.6% at T0 to 73.0% at T1, followed by a decline to 66.2% at T2, reflecting a net gain of 7.6% between T0 and T2 (p < 0.001). In contrast, Q4 showed minimal change, increasing from 68.5% at T0 to 71.5% at T1 and declining slightly to 67.5% at T2, with no significant difference between T0 and T2 (p = 0.363).
For LO3: Identify best practices for gender-affirming hormone therapy, Q5 increased from 45.1% at T0 to 65.9% at T1 before declining to 51.5% at T2, resulting in a net gain of 6.4% (p < 0.001). Q6 showed more notable improvement, rising from 16.0% at T0 to 37.6% at T1 and stabilizing at 23.7% at T2, with a net gain of 7.7% (p < 0.001).
For LO4: Outline the fundamental aspects of gender-affirming surgery, Q7 demonstrated stable performance, slightly increasing from 76.7% at T0 to 80.3% at T1 and returning to 77.6% at T2, with no significant difference between T0 and T2 (p = 0.380). Q8, however, showed a modest decline from 88.5% at T0 to 87.7% at T1 and further to 85.3% at T2, resulting in a net decrease of 3.2% (p < 0.001).
Finally, for LO5: Understand the general principles of gender identity rights according to Italian law, Q9 exhibited substantial improvement, increasing from 29.5% at T0 to 70.9% at T1 and stabilizing at 45.7% at T2, resulting in a net gain of 16.2% (p < 0.001). Similarly, Q10 rose from 35.3% at T0 to 49.7% at T1, with a slight decline to 48.0% at T2, resulting in a net gain of 12.7% (p < 0.001).
In summary, the results highlight net improvements across most LOs at T2 compared to T0. Notable gains were sustained for LO1, LO3, and LO5, while LO2 and LO4 showed minimal or no significant changes. Although a partial decline in knowledge retention was observed between T2 and immediate post-course performance (T1), overall knowledge at T2 remained markedly higher than at baseline.
4 Discussion
This study builds upon the work of Favazzi et al. (15), which demonstrated significant short-term improvements in HCPs’ knowledge following a distance learning program on gender-affirming care. By evaluating outcomes 6 months post-training, it provides a unique perspective on the sustainability of these improvements, with a focus on self-reported attitudes, skills, practices, and knowledge retention among a large cohort of over 3,000 participants.
Previous research has consistently highlighted the potential of educational interventions to enhance HCPs’ competence in TGD care. Short-term follow-up studies—typically conducted within 3 months of training—have demonstrated marked improvements in knowledge, comfort, and perceived confidence (11–14). The few available long-term evaluations, often conducted with small cohorts, have underscored the benefits of targeted training while emphasizing the necessity of ongoing reinforcement to maintain progress (9, 10, 17, 18). For example, Zheng et al. (10) reported sustained but gradually declining knowledge and confidence 1 year after a training session, underscoring the well-documented need for periodic refreshers.
Our study distinguishes itself in several significant ways. First, it represents, to our knowledge, the largest longitudinal cohort to date assessing the outcomes of a structured, institutionalized educational program in TGD healthcare. Second, while much of the existing literature is US-centric, this study provides crucial data from a European context, broadening the geographical scope of evidence. Third, the program’s inclusive design—targeting a wide range of HCPs—enhances its generalizability and applicability across diverse professional settings.
The analysis of attitudes reflects progress and challenges in fostering enduring change. Attitudes toward the importance of psychological support and the provision of information on gender-affirming treatments were consistently high, suggesting that participants already valued these aspects or that the training reinforced pre-existing beliefs. However, limited attitudinal shifts over time may indicate a need for more experiential learning approaches, such as role-playing or direct interaction with TGD individuals, to deepen empathy and internalize these principles more effectively. Such methods could move participants from abstract agreement to active, patient-centered practice (18).
Self-reported skills—such as the ability to describe the components of sexual identity, recognize psychological support needs, and identify best practices for gender-affirming medical and surgical care— also showed substantial gains from baseline (T0) to immediate post-training (T1) and remained meaningfully elevated at six-month follow-up (T2), despite a modest decline relative to T1. This pattern aligns with cognitive theories such as Ebbinghaus’ forgetting curve (19), confirming that without reinforcement, skills and knowledge naturally attenuate over time. Nevertheless, the persistence of improved competencies at T2 demonstrates the program’s efficacy in fostering durable learning.
The practices domain warrants particular attention. Consistent with prior literature highlighting HCPs’ limited exposure to TGD individuals (6), our findings confirm that direct management of gender-affirming pathways remains relatively infrequent. While the overall proportion of participants who reported providing direct care to TGD individuals declined slightly over time, significant shifts were noted in behaviors such as engaging with families and disseminating information about gender-affirming pathways and legal rights. These changes suggest that, despite limited direct clinical engagement—often constrained by structural factors—the training influenced broader aspects of care delivery. Notably, the slight reduction in reported direct care may reflect a more refined understanding of gender-specific clinical roles following the training. This underscores the critical need for institutional and systemic support to translate individual competencies into routine practice. Future initiatives should prioritize not only education at the individual level but also organizational strategies—such as clear protocols and supportive infrastructures—to enable sustained integration of gender-affirming care across healthcare settings.
Finally, knowledge retention varied across LOs. Gains were particularly notable in understanding the biological foundations of sexual identity and the legal frameworks governing gender identity rights in Italy. Although knowledge related to psychological support and gender-affirming surgery showed less pronounced change—likely reflecting high baseline familiarity or potential limitations in the complexity of assessment items—overall performance at T2 remained markedly higher than at T0. Revising the assessment tools to incorporate greater complexity and better reflect the multifaceted realities of clinical practice could further enhance the accuracy of progress evaluations and the overall impact of the training.
Despite its strengths, this study is not without limitations. The reliance on self-reported measures to assess attitudes and skills, and practices while valuable, may not fully capture real-world clinical behaviors or patient outcomes. Additionally, the reduction in participant numbers at the six-month follow-up, though still yielding a robust sample, raises the possibility of selection bias, as those who completed the follow-up may represent the most motivated or engaged participants. This could lead to an overestimation of the program’s overall impact. The absence of a control group further limits the ability to isolate the program’s effects from external factors, such as exposure to other educational resources. Another important limitation concerns the ASPQ tool itself, which, although internally validated through exploratory factor analysis and internal consistency testing, remains a novel instrument that has not yet undergone external validation. While this limits the generalizability of the findings and calls for cautious interpretation, it may nonetheless serve as a useful foundation for future research and practice aimed at strengthening the assessment of competencies in gender-affirming care. Finally, the design of some assessment items may have contributed to high baseline scores in certain areas, necessitating revisions to improve their discriminatory power and ensure a more comprehensive evaluation of knowledge acquisition.
Taken together, the findings demonstrate that the program was effective in enhancing self-reported attitudes, skills, and knowledge among participants over the long term. Sustained improvements will likely require the integration of periodic reinforcement strategies to consolidate learning and promote the consistent delivery of gender-affirming care in clinical practice.
5 Conclusion
This study offers valuable insights into the long-term outcomes of a national educational initiative on TGD healthcare in Italy. By demonstrating sustained improvements in self-reported attitudes, skills, and knowledge, it provides a strong foundation for addressing healthcare disparities affecting TGD individuals. Although self-reported practices showed significant shifts over time, the results were heterogeneous, underscoring the importance of structural and organizational support in translating individual learning into consistent clinical practice. Moving forward, expanding and refining such programs—coupled with institutional policies and integrated reinforcement strategies—will be crucial for embedding gender-affirming care into routine healthcare delivery and advancing equity both nationally and internationally.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving humans because the registration to the online course served as implicit consent for the anonymous use of participant data. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants in accordance with the national legislation and institutional requirements because the registration to the online course served as implicit consent for the anonymous use of participant data.
Author contributions
MatM: Conceptualization, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing. UF: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. PC: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. DG: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. AR: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. MarM: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – review & editing. CB: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. FM: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. FR: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. AV: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. AM: Data curation, Formal analysis, Methodology, Writing – review & editing. MP: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The project was established with the co-funding of the European Union, National Operational Programme for social inclusion—European Social Fund 2014–2020.
Acknowledgments
We are deeply grateful to all experts in TGD healthcare and legal domains who played a role in the success of this project: Teresa Bini, Andrea D’Ambrosio, Marco Falcone, Ilaria Ferro, Alessandra D. Fisher, Cathy La Torre, Giulia Lo Russo, Francesca Mazzoli, Maria Cristina Meriggiola, Federica Peretti, Mirko Preto, Jiska Ristori, Alessia Romani, Daniele Tesoro. We also express our gratitude to the study participants for generously sharing their experiences. Furthermore, we thank TGD organizations for their active contribution in the project (ALA Milano; Associazione Consultorio Transgenere, Associazione Libellula Italia APS; Associazione Maurice GLBT, Spo. T Sportello Trans; Associazione Transessuale Napoli, ATN; Azione Trans; Boramosa, Centro Salute Trans e Gender Variant, CEST; Gruppo Ascolto Giovani Arcobaleno, G.A.G.A.; Gay Center; Gender X; Gruppo Trans APS; I Ken; Intersexioni; Movimento Identità Trans, MIT; Sat Pink APS; Sunderam; T Genus: Magna Grecia).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Generative AI has been utilized for the evaluation of the English language.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1550470/full#supplementary-material
References
1. Coleman, E, Radix, AE, Bouman, WP, Brown, GR, de Vries, ALC, Deutsch, MB, et al. Standards of care for the health of transgender and gender diverse people, version 8. Int J Transgend Health. (2022) 23:S1–S259. doi: 10.1080/26895269.2022.2100644
2. Reisner, SL, Poteat, T, Keatley, JA, Cabral, M, Mothopeng, T, Dunham, E, et al. Global health burden and needs of transgender populations: a review. Lancet. (2016) 388:412–36. doi: 10.1016/S0140-6736(16)00684-X
3. Safer, JD, Coleman, E, Feldman, J, Garofalo, R, Hembree, W, Radix, A, et al. Barriers to healthcare for transgender individuals. Curr Opin Endocrinol Diabetes Obes. (2016) 23:168–71. doi: 10.1097/MED.0000000000000227
4. Winter, S, Diamond, M, Green, J, Karasic, D, Reed, T, Whittle, S, et al. Transgender people: health at the margins of society. Lancet. (2016) 388:390–400. doi: 10.1016/S0140-6736(16)00683-8
5. de Vries, E, Kathard, H, and Müller, A. Debate: why should gender-affirming health care be included in health science curricula? BMC Med Educ. (2020) 20:51. doi: 10.1186/s12909-020-1963-6
6. Dubin, SN, Nolan, IT, Streed, CGJr, Greene, RE, Radix, AE, and Morrison, SD. Transgender health care: improving medical students’ and residents’ training and awareness. Adv Med Educ Pract. (2018) 9:377–91. doi: 10.2147/AMEP.S147183
7. Nolan, IT, Blasdel, G, Dubin, SN, Goetz, TG, Greene, RE, and Morrison, SD. Current state of transgender medical education in the United States and Canada: update to a scoping review. J Med Educ Curri Dev. (2020) 7:238212052093481. doi: 10.1177/2382120520934813
8. Kidd, JD, Bockting, W, Cabaniss, DL, and Blumenshine, P. Special-“T” training: extended follow-up results from a residency-wide professionalism workshop on transgender health. Acad Psychiatry. (2016) 40:802–6. doi: 10.1007/s40596-016-0570-7
9. Najor, AJ, Kling, JM, Imhof, RL, Sussman, JD, Nippoldt, TB, and Davidge-Pitts, CJ. Transgender health care curriculum development: a dual-site medical school campus pilot. Health Equity. (2020) 4:102–13. doi: 10.1089/heq.2019.0106
10. Zheng, C, D’Costa, Z, Zachow, RJ, Lebeau, R, and Bachmann, GA. Teaching trans-centric curricular content using modified jigsaw. MedEdPORTAL. (2022) 18:11257. doi: 10.15766/mep_2374-8265.11257
11. Chaudhary, S, Lindsay, D, Ray, R, and Glass, BD. Evaluation of a transgender health training program for pharmacists and pharmacy students in Australia: a pre-post study. Explor Res Clin Soc Pharm. (2024) 13:100394. doi: 10.1016/j.rcsop.2023.100394
12. Cherabie, J, Nilsen, K, and Houssayni, S. Transgender health medical education intervention and its effects on beliefs, attitudes, comfort, and knowledge. Kans J Med. (2018) 11:106–9. doi: 10.17161/kjm.v11i4.8707
13. Braun, HM, Garcia-Grossman, IR, Quiñones-Rivera, A, and Deutsch, MB. Outcome and impact evaluation of a transgender health course for health profession students. LGBT Health. (2017) 4:55–61. doi: 10.1089/lgbt.2016.0119
14. Click, IA, Mann, AK, Buda, M, Rahimi-Saber, A, Schultz, A, Shelton, KM, et al. Transgender health education for medical students. Clin Teach. (2020) 17:190–4. doi: 10.1111/tct.13074
15. Favazzi, UM, Marconi, M, Carbone, P, Guerrera, D, Ruocco, A, Manoli, M, et al. Evaluating the impact of distance learning on gender-affirming healthcare competence: knowledge acquisition and satisfaction among healthcare professionals in Italy. Front Public Health. (2024) 12:1393188. doi: 10.3389/fpubh.2024.1393188
16. Schmidt, HG, Rotgans, JI, and Yew, EH. The process of problem-based learning: what works and why. Med Educ. (2011) 45:792–806. doi: 10.1111/j.1365-2923.2011.04035.x
17. Kreines, FM, Quinn, GP, Cardamone, S, Pi, GE, Cook, T, Salas-Humara, C, et al. Training clinicians in culturally relevant care: a curriculum to improve knowledge and comfort with the transgender and gender diverse population. J Assist Reprod Genet. (2022) 39:2755–66. doi: 10.1007/s10815-022-02655-1
18. Dubin, S, Kutscher, E, Nolan, I, Levitt, N, Cook, TE, and Greene, RE. Assessment of medical education on transgender health: a scoping literature review. Eval Health Prof. (2024) 47:296–303. doi: 10.1177/01632787231214531
Keywords: transgender and gender diverse, healthcare professionals, distance learning, continuing medical education, knowledge retention, gender-affirming care
Citation: Marconi M, Favazzi UM, Carbone P, Guerrera D, Ruocco A, Manoli M, Barbati C, Molinaro F, Regini FM, Vittozzi A, Mazzaccara A and Pierdominici M (2025) Evaluating the long-term impact of a distance learning course on attitudes, skills, practices, and knowledge in gender-affirming healthcare among healthcare professionals in Italy. Front. Public Health. 13:1550470. doi: 10.3389/fpubh.2025.1550470
Edited by:
Yi Sub Kwak, Dong-Eui University, Republic of KoreaReviewed by:
Gianluca Tornese, Institute for Maternal and Child Health Burlo Garofolo (IRCCS), ItalyAlbina Veltman, McMaster University, Canada
Copyright © 2025 Marconi, Favazzi, Carbone, Guerrera, Ruocco, Manoli, Barbati, Molinaro, Regini, Vittozzi, Mazzaccara and Pierdominici. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marina Pierdominici, bWFyaW5hLnBpZXJkb21pbmljaUBpc3MuaXQ=
†These authors share first authorship