 Maria Heloisa do Nascimento Silva1
Maria Heloisa do Nascimento Silva1 Caroline Lopes Ciofi-Silva2
Caroline Lopes Ciofi-Silva2 Verusca Soares de Souza3
Verusca Soares de Souza3 Daniel de Macêdo Rocha4
Daniel de Macêdo Rocha4 Alvaro Francisco Lopes de Sousa1,5*
Alvaro Francisco Lopes de Sousa1,5* Adriana M. S. Felix5
Adriana M. S. Felix5 Aires Garcia dos Santos Júnior1
Aires Garcia dos Santos Júnior1- 1Universidade Federal de Mato Grosso do Sul, Campus de Três Lagoas, Três Lagoas, Mato Grosso do Sul, Brazil
- 2School of Nursing, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brazil
- 3Universidade Estadual do Paraná, Paranavaí, PR, Brazil
- 4Universidade de Mato Grosso do Sul, Campus Coxim, Coxim, Mato Grosso do Sul, Brazil
- 5Instituto de Ensino e Pesquisa, Hospital Sírio-Libanês, São Paulo, SP, Brazil
Objective: To compare the impact of a package of interventions on surface cleaning and disinfection in two public and private neonatal intensive care units (NICUs).
Method: This is a quasi-experimental, quantitative study. The study consisted of three phases: baseline (phase I), implementation of the intervention package without feedback to the team (phase II), and, finally, short-term monitoring with feedback to the team (phase III). A total of 864 evaluations were carried out according to the monitoring methods: adenosine triphosphate, visual inspection, microbial load counting, and detection of Staphylococcus aureus and testing for its methicillin resistance (MRSA) in each unit over 4 months, evaluating six high-frequency touch surfaces, before and after cleaning and disinfection carried out by nursing and sanitizing professionals.
Results: When comparing the effect of the package in the two units (public and private), no significant differences were found in the proportions of MRSA-positive surfaces in all the phases evaluated. The same occurred concerning the ATP method, which showed no significant differences between the hospitals in all study phases. Concerning the microbial count, in phase II of the study, only on one surface (scales) was a significantly lower difference found in the private hospital compared to the public one. Visual inspection indicated that the private NICU had a substantially higher proportion of surfaces with adequate hygiene in phase I: the infusion pump and the armchair; in phase II, the counter and in phase III again the counter surface. Concerning human factors, when comparing the two institutions, there were no statistically significant associations or correlations with job satisfaction. However, the public institution had higher work performance scores than the private one.
Conclusion: The study highlights that the rigorous implementation of intervention packages for cleaning in NICUs, even though they are different, still showed similar results in terms of effectiveness for all the methods used, except visual inspection. This study showed that even though the employees had various levels of work performance, there was still a similar effect on the outcome of the intervention package.
Introduction
Healthcare-associated infections (HAIs) pose a serious threat to patient safety worldwide, leading to increased morbidity, mortality, and hospital costs. The complexity of cases, particularly in intensive care units, contributes to adverse clinical outcomes (1, 2).
Infections are a critical issue in Neonatal Intensive Care Units (NICUs), affecting ~30% of newborns and contributing to up to 40% of neonatal deaths in developing countries. Therefore, surveillance and control measures are essential to reducing morbidity and mortality, including hand hygiene, rational antibiotic use, standard precautions, and control of environmental contamination (3, 4).
To prevent the transmission of HAIs, it is crucial to adopt rigorous cleaning and disinfection (C&D) practices, which involve the removal of visible dirt and the use of effective disinfectants on high-contact surfaces. These measures are essential for protecting public health and reducing infection risks (5). Despite this, shortcomings in C&D practices persist (6). To ensure the effectiveness of C&D processes, it is necessary to implement quality monitoring methods that guide protocol adjustments and staff training. Several methods are available, including visual inspection, quantitative and qualitative microbiological analysis (identification of microorganism species), and the quantification of adenosine triphosphate (ATP) (7).
Visual inspection is a simple and low-cost method; however, it does not provide an objective assessment of cleanliness. In contrast, microbial load testing quantifies the presence of microorganisms on surfaces by measuring colony-forming units (CFU), but this method is more expensive, time-consuming, and requires specialized laboratory facilities (7, 8). One epidemiologically relevant species is MRSA.
Another commonly used method is ATP bioluminescence testing, which is a simple, rapid, and quantitative approach. Initially applied in the food industry, ATP assays have recently been adopted in healthcare settings to monitor the cleanliness of environmental surfaces (9, 10).
The C&D process is primarily carried out by nursing professionals (NPs) and hygiene professionals (HPs). To ensure compliance with cleaning standards, the active engagement of these professionals is essential. Understanding organizational culture-related factors, such as the commitment and work performance of NPs and HPs, not only enhances employee wellbeing but also improves the quality of care provided (11, 12).
Educational strategies, feedback mechanisms, and the standardization of practices and supplies are widely employed to strengthen adherence to C&D protocols. A systematic review found that studies on the subject provided limited information regarding HP-related aspects, workload, the impact of training, and the frequency of object and surface cleaning per shift. The review recommended further studies with detailed evaluations of the effectiveness of interventions (13).
Despite the growing recognition of the role of environmental service workers in infection prevention, significant gaps remain in understanding the daily work dynamics of these professionals. NPs and HPs face constant challenges in an environment that demands repetitive tasks under high pressure, often in conditions that negatively impact their health and wellbeing. Although they play a crucial role in hygiene and infection control, these workers are frequently overlooked within organizational contexts and do not receive the necessary recognition. Their inclusion in interdisciplinary discussions and training initiatives is rare, limiting opportunities for skill development and appreciation of their essential contributions to public health (14).
This study contributes to the scientific literature on this topic. The research is guided by the following questions: Are there differences in the effectiveness of an intervention package when comparing two NICUs, one public and one private? What are the levels of job satisfaction and performance among the professionals responsible for the C&D process in the two NICUs?
Objective
To compare the effect of an intervention package on surface C&D, as well as the levels of job satisfaction and performance of nursing and hygiene professionals responsible for environmental hygiene in public and private neonatal units.
Materials and methods
Ethical aspects
This study was approved by the institutional Research Ethics Committee under opinion number 5.961.710.
Type of study
This is a quasi-experimental, quantitative study.
Study site
The research was conducted simultaneously in two NICUs, one public and one private, each with 10 beds. Both NICUs had a qualified multidisciplinary team. Data collection took place from August to November 2023.
In Brazil, according to the guidelines of the Health Surveillance Agency, the responsibility for surface C&D can be shared between NPs and HPs. In this study, surfaces under the responsibility of both teams were evaluated. It is up to each institution to determine, through internal policies and procedures, the specific responsibilities of each professional (15).
Selection of participants (inclusion and exclusion criteria)
The study included all NPs (directly hired by the institution) responsible for the C&D process in the two participating NICUs.
In the private NICU, the team consisted of 17 professionals, including 15 nursing staff and two hygiene staff, all of whom agreed to participate in the research. In the public NICU, all 29 professionals responsible for C&D participated in the study, including 25 from the nursing team and four from hygiene services. Trainees were excluded from the sample.
Protocol and products used before the educational intervention
The institution had an established ICU sanitization protocol. However, this protocol did not specify which product should be used for each type of surface or the appropriate cleaning materials. According to the standard protocol, concurrent cleaning was recommended once a day. HPs were responsible for cleaning the ceiling, floor, shelves, and walls, while NPs were in charge of disinfecting incubators during the weekly terminal cleaning.
A preliminary observation of the C&D process was conducted over a week using a checklist adapted from CDC guidelines (2010). It was noted that each professional used a different cleaning product for surface C&D.
In the NICUs, alcohol gel dispensers were available near all beds, as well as in other locations throughout the unit. Visitors had unrestricted access to the unit, and guidance on proper hand hygiene techniques was provided at the entrance.
Procedures
Data collection occurred between August and November 2023 and was divided into three phases: I. Baseline assessment; II. Implementation of the Intervention Package without providing feedback to the team (PI); and III. Medium-term monitoring with feedback to the team.
In phase I (baseline), detailed monitoring of the C&D process was carried out using the following methods: a) visual inspection; b) ATP measurement; c) quantitative assessment of microbial load using RODAC-type contact plates; d) detection of MRSA.
The 10 × 10 cm area proposed by the area delimiter provided by the manufacturer LaborClin (“Produtos para Laboratórios Ltd.”; Pinhais, PR, Brazil) was standardized for ATP data collection. The swab was applied to the surfaces using horizontal and vertical movements, then agitated for 10 s to ensure proper contact with the reagent before being inserted into the luminometer. A reading of < 250 relative light units (RLUs) was considered acceptable (16).
For microbial load assessment, Rodac-type contact plates (manufacturer) were used. These plates, made of tryptic soy agar, have a 24 cm2 surface area and hold up to 20 ml of medium. To quantify microbial load, the plates were pressed onto the surfaces for 10 s and then incubated at 37°C. CFU counts were assessed after 48 h using a stereomicroscope under reflected light (17).
For the identification of Staphylococcus aureus, Petrifilm™ Staph Express plates (manufacturer) were used. These plates contain a chromogenic and selective culture medium, which enables the differentiation of S. aureus by producing red-violet colonies (manufacturer's guide).
To detect MRSA, colonies were inoculated onto a selective culture medium (manufacturer). This medium contains inhibitors to prevent the growth of non-target bacteria and differential indicators that allow MRSA to be identified. The addition of chromogenic substrates facilitates visualization through distinct colony staining (manufacturer's guide).
In phase II (Implementation of the Intervention Package), interventions were designed based on the findings from phase I. These interventions included educational activities, standardization of practices, and selection of appropriate cleaning supplies.
After consenting to participate in the study, formalized through the Informed Consent Form (ICF), NPs and HPs completed the Work Performance and Job Satisfaction Scale, detailed below.
An educational intervention was conducted in each NICU, comprising 12 training sessions per unit, with each session lasting 1 h, over a 1-week period. Institutional protocols were revised based on the recommendations of the Centers for Disease Control and Prevention (CDC) and the National Health Surveillance Agency (ANVISA), as well as validated educational materials from worker health promotion programs (15, 18, 19).
The intervention aimed to improve the sanitization of high-touch surfaces in patient areas and locations associated with direct clinical care. A key component was training staff on thorough cleaning techniques for surfaces and equipment (20).
In collaboration with the Hospital Infection Control Committees, NICU Nursing Coordinators, and Hygiene Service Coordinators, protocols were updated to standardize concurrent cleaning twice daily and as needed (15).
The use of a specific disinfectant for floors, walls, furniture, and equipment was established. This disinfectant contains 5th-generation di-decyl quaternary ammonium compounds combined with polymeric biguanide from the chlorhexidine family (Polyhexamethylene Biguanide), providing broad-spectrum microbicidal activity against bacteria, yeasts, fungi, viruses, and spores. The product must be applied in a manner that ensures the surface remains moist for 10 min (21).
Additionally, the use of microfiber cloths for cleaning was standardized, as they have been shown to enhance microbial removal efficiency (22).
During the intervention, the cleaning process was adjusted, demonstrating the correct technique: when cleaning incubators and cradles, the process should begin from the inside out, always in one direction, to prevent the dispersion of dirt. If the cloth accumulates visible dirt or is used in highly contaminated areas, it should be replaced to avoid redistributing contaminants. The procedure consists of three stages, if necessary: in the first, a cloth dampened with the disinfectant solution is used to remove surface dirt; in the second, a dry cloth is applied to ensure the complete removal of any dirt residue or disinfectant remnants; and, if needed, a third application of the cloth is performed until the surface is entirely clean and free of visible residue. Photos demonstrating the correct procedure were provided to facilitate proper execution.
After this first week of team training, surface monitoring commenced immediately and continued for 30 days using the same monitoring methods applied in phase I of the study (23–25).
In phase III, surface monitoring was conducted again to evaluate the C&D process using the same methods as in phase I; however, this time, feedback was provided to the professionals. The lead researcher offered feedback on C&D practices to NPs and HPs, who were given immediate access to the assessment results, including ATP readings and visual inspections (25).
This phase lasted 30 days (23–25). The objective was to repeat the procedures to assess adherence to the implemented measures 60 days after the educational intervention.
It is important to note that in phase I, before the educational intervention, there was no Hawthorne effect on participants' professional practices, minimizing the possibility of external factors influencing the results. The participants were not informed about the study's objective, and sample collections followed the same protocols used for institutional testing of cleaning product effectiveness. Samples were always collected before and after the team performed the C&D process. In the subsequent phases, data collection was conducted by research team members, ensuring that the processes involved remained consistent across the different phases.
Using an intentional and non-probabilistic approach, the following items were selected for surface monitoring: the counter (marble in Unit A and wood in Unit B, used for medication preparation in both units), incubator (metal and acrylic structure in both units), armchair (polyvinyl chloride and polyester mesh), infusion pump (polycarbonate in both units), preparation table (stainless steel in both units), desk, and scale (polypropylene in both units). These items were chosen based on systematic observation, prioritizing high-touch surfaces, as recommended by the CDC (26).
Samples were collected twice weekly in each NICU, totaling eight sampling days per phase. Considering the analyzed surfaces, six samples were obtained before and six after the cleaning process, totaling 12 samples per day and 24 samples per week from each institution. Consequently, 96 samples were collected per method at the end of each month, leading to 864 evaluations conducted in each NICU, as detailed in Table 1.

Table 1. Evaluations conducted in each phase of the study in each NICU. Três Lagoas, MS, Brazil, 2023.
Scales used to collect human factors data
The Job Satisfaction Scale (27) and the Performance scale developed by Vandenabeele (28) were used to collect data on satisfaction levels. The scales used to assess job satisfaction and performance levels in hospital contexts are essential for understanding professionals' perceptions. The Job Performance Scale by Vandenabeele (28), comprised of four variables, uses a Likert-type approach, offering five response options, with minimum and maximum values ranging from 4 to 20. The Job Satisfaction Scale, developed by Dépré and Hondeghem in 1995, consists of a single dimension with six variables, the answers to which are captured by a five-point Likert scale, ranging from “strongly disagree” (1) to “strongly agree” (5). Thus, the results of this scale can range from a minimum of 6 to a maximum of 30.
Statistical analysis
The following statistical tests were applied: the Wilcoxon rank-sum test to compare the results of ATP measurements and microbial load/CFU. The Mann-Whitney test was used to compare microbial load/UFC and ATP measurements. This test uses the data median, employing a comparative and non-parametric analysis.
In addition, a quantitative analysis of the data was carried out, comparing the microbial load/CFU and ATP measurements at the different stages of the study. To achieve this, the variation in the quantitative data, which includes the total microbial load (CFU/cm2) and ATP, was calculated using the following expression:
Fisher's exact test was applied when analyzing the surfaces by visual inspection in all phases to compare two proportions and check for any differences. A descriptive analysis was carried out for the variables related to job satisfaction and performance. The study adopted a significance level of 5% (p < 0.05).
Results
Table 2 shows the percentages of surfaces that passed the visual inspection for both hospitals in all the phases evaluated.
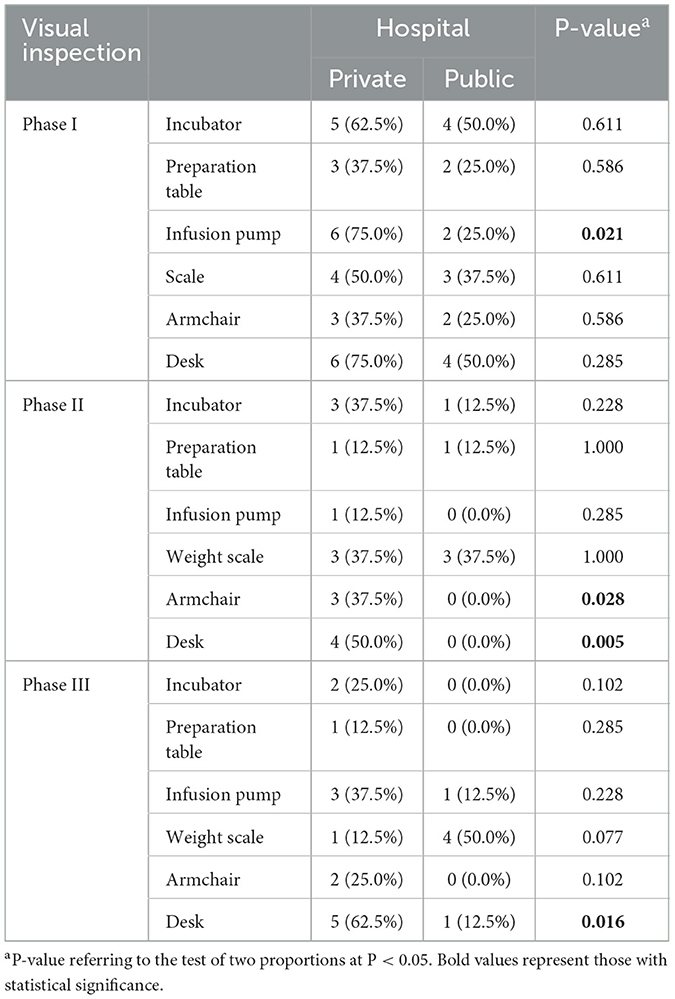
Table 2. Results of the visual inspection of approved surfaces for both hospitals in the phases evaluated in the study.
The results in Table 2 show four cases of proportions of approved surfaces that differed significantly when the hospitals were compared (P < 0.05). In phase I, the approval proportion for the infusion pump was substantially higher for the private than for the public hospital. The same situation occurred in phase II for the armchair and counter, showing that the approval proportion was significantly higher for the private hospital. In phase III, the desk also showed significant differences, with a higher proportion of approval for the private sector. In all critical cases, the private sector had a higher proportion of approved surfaces than the public sector, which means that the intervention was more effective in the private sector than in the public sector.
The data in Table 3 shows the results of the parameters assessed in the study comparing the hospitals.

Table 3. In relative light units, Adenosine Triphosphate (ATP) results for both hospitals in the phases evaluated in the study.
Table 3 shows no significant differences in ATP values for all study phases when comparing the hospitals evaluated. All P-values were higher than 0.05. Therefore, regardless of the phase evaluated, the ATP values on all surfaces in both hospitals did not differ significantly.
Table 4 shows the results of the microbial loads (CFU) compared to the hospitals.
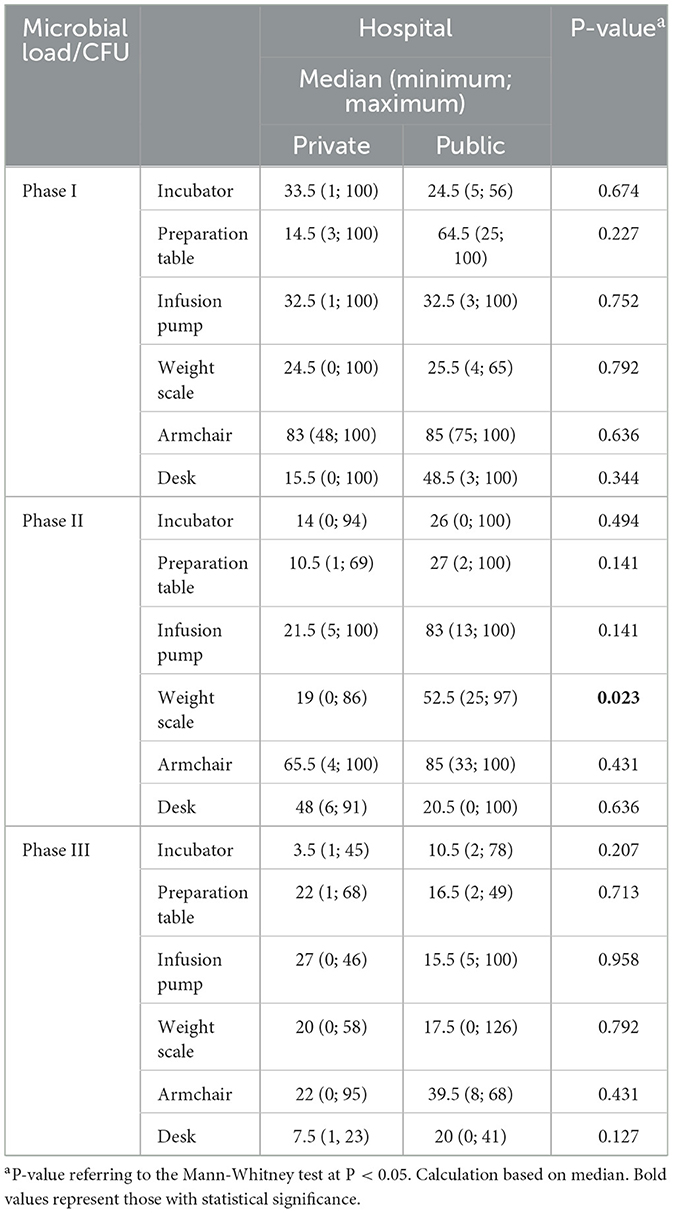
Table 4. Results of microbial load/CFU for both hospitals in the phases evaluated in the study.
According to the data in Table 4, there was one significant difference in the microbial count between the hospitals evaluated, the surface being a scale in phase II (P = 0.023). In this case, the microbial count was significantly lower in the private hospital than in the public one. There were no significant differences in the microbial count for the other surfaces.
Table 5 shows the results of comparing hospitals with Staphylococcus aureus (SA). There were no significant differences, regardless of phase.
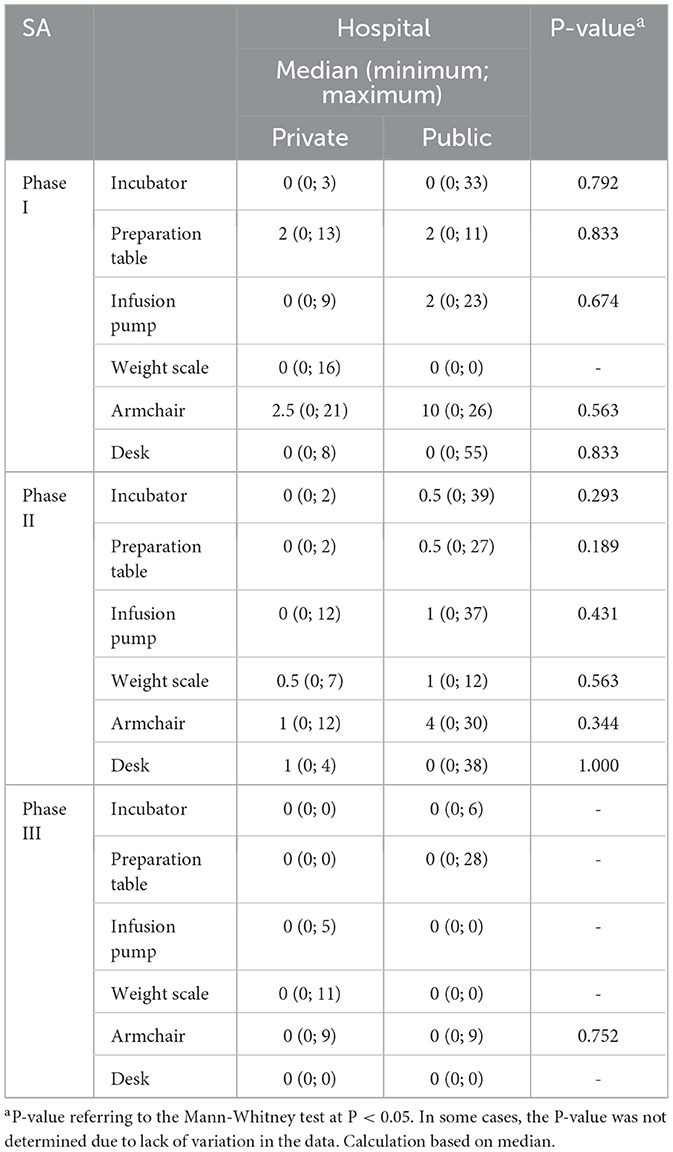
Table 5. It shows the results of Staphylococcus aureus (SA) for both hospitals in the phases evaluated in the study.
Table 6 shows the percentages of MRSA-positive surfaces for both hospitals in all the phases evaluated.
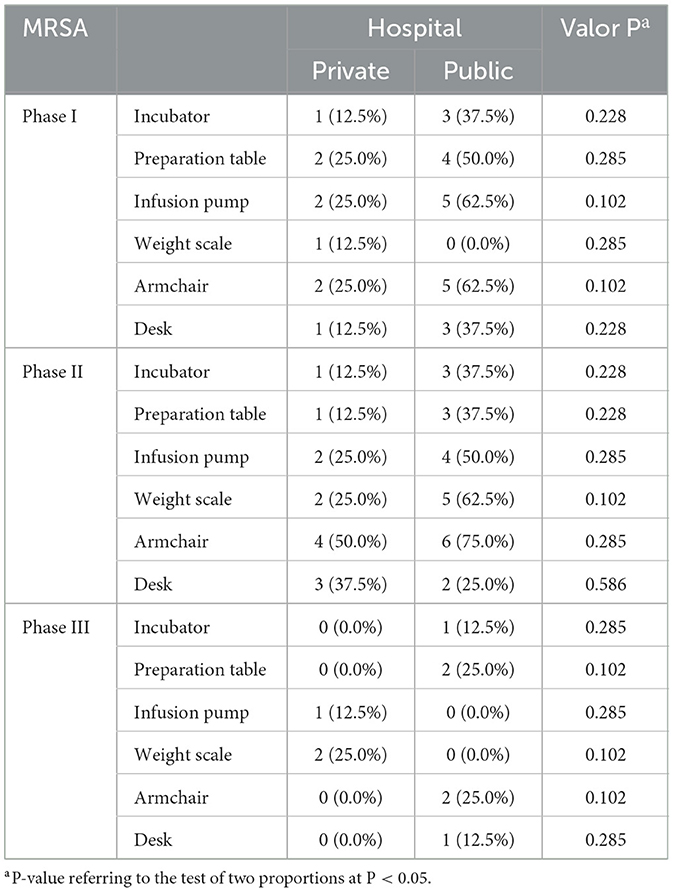
Table 6. The results of the surfaces were positive for methicillin-resistant Staphylococcus aureus (MRSA) for both hospitals in the phases evaluated in the study.
The results in Table 6 show no significant differences in the proportions of MRSA-positive surfaces in all the phases evaluated when the hospitals were compared (P > 0.05). In this context, the evaluated hospitals had no significant differences regarding MRSA-positive status.
Regarding human factors, comparing the two ICUs, it was found that there was no statistically significant difference between the two units in terms of age (p = 0.825, Mann-Whitney test), and there was also no statistically significant difference in terms of schooling (p = 0.286, Mann-Whitney test). There was also no difference between the two groups regarding the length of time they had worked in the ICU (p = 0.430, Fisher's exact test). Concerning job satisfaction, there were no statistically significant associations or correlations when assessing the scores obtained from the 0.067 d scale (r = 0.19). However, the public institution scored higher on the work performance scale than the private institution (Mann Whitney W = 366.5, p = 0.006), as seen in Table 7.
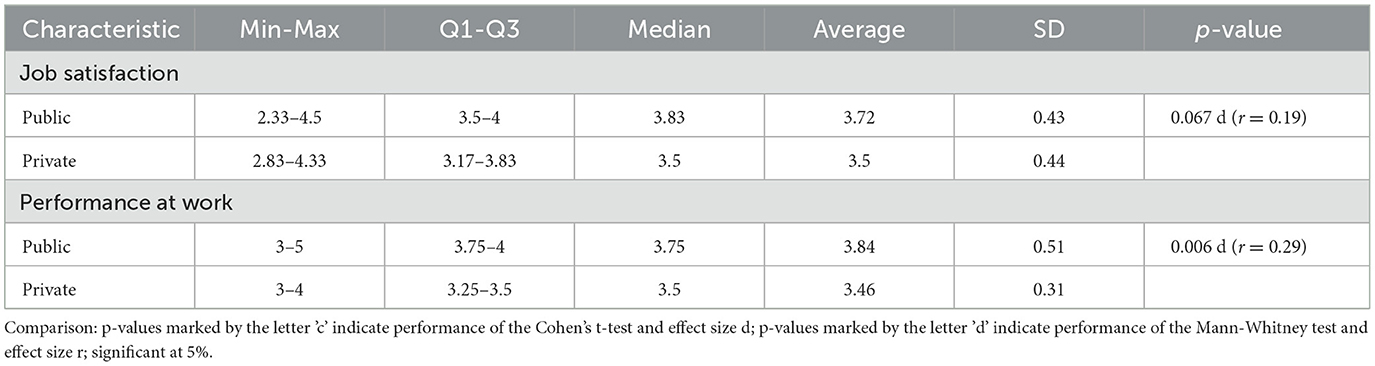
Table 7. Comparison of the level of job satisfaction and performance of the professionals responsible for cleaning (nursing and hygiene) in the two institutions.
Discussion
This study showed that, overall, for most surfaces monitored using various methods, there was no statistically significant difference between the results from the public and private NICUs. However, regarding visual inspection, it was observed that in the private NICU, four surfaces—the infusion pump (phase I), armchair (phase II), and desk (phases II and III)—showed a statistically significant reduction.
Visual inspection is the most widely used method by professionals, although other methods are available (29, 30). A study conducted in a private general ICU found that, according to the visual inspection method, surfaces such as the infusion pump, alcohol dispenser, and telephone had the highest percentage of accumulated dirt, accounting for 75% of occurrences (31). In contrast, our study in the neonatal ICU found different results, with an approval rate for the infusion pump in phase I of 75% in the private NICU, whereas in the public NICU, the disapproval rate was 75%.
Regarding the ATP method, there was no statistical difference between the two NICUs. However, when analyzing the six surfaces evaluated in the three phases (18 surfaces), it was noted that the absolute median values in relative light units (RLUs) obtained in the public hospital were higher on 12 surfaces, indicating a greater organic matter load. Additionally, the counter surface in the public NICU during phase I had the highest recorded value, with 395 RLUs, while the incubator surface in the private NICU had the lowest median value, at 17 RLUs. A study conducted in an adult ICU found that the telephone surface had the highest median, with 1,012 RLUs, whereas the bed rail had a median of 26 RLUs (31). The surfaces closest to the patient generally had lower median values.
The effectiveness of C&D in NICUs is crucial for preventing HAIs in newborns, particularly in premature and very low birth weight infants. This study compared the microbial count on hospital surfaces and found a significant difference in microbial load only on the scale surface in the private NICU during phase II (P = 0.023). In another NICU study, researchers found a median microbial load of 24 CFU, which was significantly reduced to 5 CFU after staff training (32).
A study conducted in an ICU to assess the effectiveness of daily cleaning found that routine cleaning significantly reduced the bacterial load in patient rooms (reduction of 0.14 log10 CFU, P = 0.008; reduction of 0.21 log10 RLU, P < 0.001). One key aspect influencing these results was the importance of providing feedback to the team (10). These findings align with the results observed in both public and private NICUs, as phase III showed a reduction in median values compared to phase I.
Regarding the presence of MRSA, there was no statistically significant difference between the public and private institutions. Resistance percentages remained ≤ 50% in phases II and III of the study, except for the scale surface (62.5%) and the armchair (75%) in the public NICU. These results differ from a study conducted in a Moroccan NICU to assess surface C&D, in which 60% of Staphylococcus aureus strains were methicillin-resistant (32).
Continuing education
The literature indicates that interventions often lead to short-term improvements in the C&D process. However, sustaining these improvements over time remains a challenge. One study found that interventions incorporating training, monitoring, and feedback for allied health professionals (AHPs) resulted in improvements lasting more than 10 years (33). In a study conducted in a neonatal care unit, a multimodal intervention—including cleaning audits with feedback, cleaning checklists, in-room cleaning wipes, and training for staff and mothers—led to significant improvements in the C&D process (20).
A study analyzing the monitoring of hospital cleanliness over a decade identified progressive improvements in cleanliness rates. Throughout this period, cleaning rates steadily increased, reaching an average of 93.0% over the last five years. This upward trend reflects the effectiveness of a long-term monitoring program, which enabled continuous adjustments and interventions to maintain and enhance cleaning standards. Additionally, the periodic revision of cleanliness targets, including an updated benchmark of 93%, demonstrates an ongoing commitment to excellence in environmental hygiene. These findings underscore the importance of long-term monitoring as an effective strategy to ensure the consistent quality of hospital cleaning, ultimately yielding tangible benefits for patient safety and wellbeing (33).
Human factors
The study indicated no statistically significant difference in the self-reported satisfaction and performance of the NPs and HPs responsible for the C&D process. However, it was observed that the median values for satisfaction and performance were higher in the public institution.
The study's findings highlight the participants' job satisfaction. Job satisfaction refers to a worker's perception of their job, which is influenced by personal beliefs, values, interactions with colleagues and the institution, and a sense of belonging (34).
NPs and HPs responsible for C&D in a hospital setting often report higher satisfaction levels regarding supervision and coworkers, while satisfaction is lower regarding salary, benefits, promotion opportunities, and working conditions. In contrast, nurses working in management positions tend to report higher job satisfaction than nursing assistants and technicians (35).
Among professionals involved in the C&D process in hospitals, job dissatisfaction is linked to remuneration, institutional policies, level of autonomy, and professional responsibilities, all of which can contribute to career abandonment. Other factors influencing job satisfaction include gender, age, marital status, education level, living conditions, and external factors such as professional success, career advancement, and the nature of the work performed (36, 37).
Work performance reflects an employee's commitment to implementing the principles and objectives of health programs and policies, which serve as a foundation for maintaining and improving healthcare quality and supporting decision-making in the field (38).
Most participants perceived their work performance and contribution to the institution positively. Training and continuing education initiatives are essential for promoting autonomy and restructuring work processes, which positively impact worker performance. It is recommended that training programs for human resources involved in C&D be developed to mitigate negative health impacts and reinforce environmental preservation. It is also noteworthy that both institutions employ direct-hire staff rather than outsourced workers.
The results observed in NICUs and an Emergency Care Unit (UPA) during the COVID-19 pandemic revealed both similarities and differences regarding human factors and workplace motivation. In the NICU study, no statistically significant differences were found between professionals from the two institutions in terms of age, education level, or length of time working, suggesting a certain homogeneity between the groups. However, in the UPA, a significant association was observed between education level and intrinsic motivation, with individuals with lower educational attainment demonstrating greater motivation linked to work enjoyment (p = 0.031). These differences may reflect variations in work environments and the demands of each healthcare setting (29).
Regarding job satisfaction, the NICUs exhibited an interesting distinction: the public institution scored higher on the job performance scale than the private one (p = 0.006). In the UPA, satisfaction levels varied significantly, ranging from indifference to agreement with overall job satisfaction. Additionally, female participants in the UPA reported greater satisfaction regarding their work expectations being met (p = 0.014), a trend not observed in the NICUs. This comparison suggests that while both environments present challenges, the intrinsic and extrinsic factors influencing motivation and job satisfaction may vary depending on the nature of the job and the specific conditions of each workplace (29).
Study limitations
Although the study has provided valuable insights into comparing surface C&D in public and private NICUs, some limitations should be considered. The sample was not randomly selected; surfaces were chosen intentionally, which may introduce bias and limit the generalizability of the findings to other NICUs. Additionally, variability in adherence to standardized practices and differences in the use of cleaning products between teams may have influenced ATP and CFU measurements as well as visual inspection results.
Conclusion
This study emphasizes the importance of implementing and monitoring robust intervention packages for C&D in NICUs, demonstrating that there was no statistically significant difference in most of the monitoring methods used between the two NICUs. The findings suggest that even with differences in institutional settings, the rigorous application of intervention packages resulted in similar outcomes. Furthermore, despite variations in employee performance and job satisfaction levels, the intervention package had a comparable effect on improving C&D practices in both NICUs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, provided that a reasonable request is made to the corresponding author.
Ethics statement
The studies involving humans were approved by Universidade Federal do Mato Grosso do Sul. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MHNS: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing, Methodology. CLC-S: Methodology, Data curation, Supervision, Writing – review & editing. VSS: Methodology, Writing – original draft, Writing – review & editing, Visualization. DMR: Writing – original draft, Writing – review & editing, Funding acquisition, Validation. AFLS: Conceptualization, Formal analysis, Project administration, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition. AMSF: Conceptualization, Visualization, Writing – original draft, Writing – review & editing, Funding acquisition. AGSJ: Conceptualization, Formal analysis, Investigation, Visualization, Funding acquisition, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Funding Code 001; Fundação de Apoio ao Desenvolvimento do Ensino, Ciência e Tecnologia do Estado de Mato Grosso do Sul (FUNDECT); Universidade Federal do Mato Grosso do Sul; and Hospital Sírio-Libanês. The funders had no role in the design, analysis, or conclusions of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. The authors used Gemini AI (version 1.5, model Flash, source: https://www.geminiai.com/) during the preparation of this work to revise the technical quality of the manuscript's translation into English. After utilizing the tool/service, the authors thoroughly reviewed and edited the content as necessary and assumed full responsibility for the publication's content.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rangelova V, Raycheva R, Kevorkyan A, Krasteva M, Dermendzhiev T. Surveillance of nosocomial infections in a Bulgarian neonatal intensive care unit. Folia Med. (2020) 62:753–61. doi: 10.3897/folmed.62.e50437
2. Peters A, Schmid MN, Parneix P, Lebowitz D, de Kraker M, Sauser J, et al. Impact of environmental hygiene interventions on healthcare-associated infections and patient colonization: a systematic review. Antimicrob Resist Infect Control. (2022) 11:1–38. doi: 10.1186/s13756-022-01075-1
3. Berberian G, Brizuela M, Rosanova MT, Travaglianti M, Mastroiani A, Reijtman V, et al. Multidrug resistant gram-negative infections in neonatology. Arch Argent Pediatr. (2019) 117:6–11. doi: 10.5546/aap.2019.eng.6
4. Wang L, Du KN, Zhao YL, Yu YJ, Sun L, Jiang HB. Risk factors of nosocomial infection for infants in neonatal intensive care units: a systematic review and meta-analysis. Med Sci Monit. (2019) 25:8213–20. doi: 10.12659/MSM.917185
5. Geng Y, Wang Y. Stability and transmissibility of SARS-CoV-2 in the environment. J Med Virol. (2023) 95:e28103. doi: 10.1002/jmv.28103
6. Meyer J, Nippak P, Cumming A. An evaluation of cleaning practices at a teaching hospital. Am J Infect Control. (2021) 49:40–3. doi: 10.1016/j.ajic.2020.06.187
7. Nascimento EA, Poveda VD, Monteiro J. Evaluation of different monitoring methods of surface cleanliness in operating rooms. Rev Bras Enferm. (2021) 74:e20201263. doi: 10.1590/0034-7167-2020-1263
8. Da Silva Lima F, Miranda MK, da Silva Bezerra J, Ferreira MS, de Oliveira SM, de Aguiar Valentim L, et al. Água ozonizada: uma nova proposta na desinfecção de superfícies em salas de cirurgias ortopédicas. Rev Eletr Acervo Saúde. (2022) 15:e9588. doi: 10.25248/reas.e9588.2022
9. Ishino N, Miyaji C, Ogata M, Inada M, Nagata M, Shimamoto M. Applicability of the ATP assay in monitoring the cleanliness of hospital environments. Infect Dis Health. (2024) 29:32–8. doi: 10.1016/j.idh.2023.09.034
10. Deshpande A, Dunn AN, Fox J, Cadnum JL, Mana TS, Jencson A, et al. Monitoring the effectiveness of daily cleaning practices in an intensive care unit (ICU) setting using an adenosine triphosphate (ATP) bioluminescence assay. Am J Infect Control. (2020) 48:757–60. doi: 10.1016/j.ajic.2019.11.031
11. Rodrigues FMA, Pereira RPG, Martins MM. Cultura organizacional para a mudança num contexto hospitalar: uma perspectiva de enfermagem. Acta paulista de enfermagem. (2023) 36:eAPE00551. doi: 10.37689/acta-ape/2023AO00551
12. De Souza Guimarães PT, Oderich CL. Cultura organizacional na gestão hospitalar. Revista Pleiade. (2023) 17:28–38. doi: 10.32915/pleiade.v17i41.949
13. Thomas RE, Thomas BC, Lorenzetti D, Conly J. Hospital and long-term care facility environmental service workers' training, skills, activities and effectiveness in cleaning and disinfection: a systematic review. J Hosp Infect. (2022) 124:56–66. doi: 10.1016/j.jhin.2022.03.002
14. Yanke E, Moriarty H, Carayon P, Safdar N. The invisible staff: a qualitative analysis of environmental service workers' perceptions of the VA Clostridium difficile prevention bundle using a human factors engineering approach. J Patient Saf . (2021) 17:e806–14. doi: 10.1097/PTS.0000000000000500
15. Brasil. Agência Nacional de Vigilância Sanitária. Segurança do paciente em serviços de saúde: limpeza e desinfecção de superfícies. Brasília: Anvisa (2010).
16. Boyce JM. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob Resist Infect Control. (2016) 5:10. doi: 10.1186/s13756-016-0111-x
17. Cloutman-Green E, D'Arcy N, Spratt DA, Hartley JC, Klein N. How clean is clean—is a new microbiology standard required? Am J Infect Control. (2014) 42:1002–3. doi: 10.1016/j.ajic.2014.04.025
18. Centers for Disease Control and Prevention and Infection Control Africa Network. Best Practices for Environmental Cleaning in Healthcare Facilities in Resource-Limited Settings. CDC, Atlanta; ICAN, Cape Town (2019). Available online at: http://www.icanetwork.co.za/icanguideline2019/ (accessed April 13, 2025).
19. Porto JS, Marziale MHP. Construção e validação de vídeo educativo para adesão às precauções-padrão por profissionais de enfermagem. Texto and Contexto-Enfermagem. (2020) 29:e20180413. doi: 10.1590/1980-265X-TCE-2018-0413
20. Dramowski A, Aucamp M, Bekker A, Pillay S, Moloto K, Whitelaw AC, et al. NeoCLEAN: a multimodal strategy to enhance environmental cleaning in a resource-limited neonatal unit. Antimicrob Resist Infect Control. (2021) 10:1–9. doi: 10.1186/s13756-021-00905-y
21. Nipponchemical. Descrição desinfetante. (2019). Available online at: https://energis8solucoes.com/wp-content/uploads/2020/06/Cat%C3%A1logo-Nippo-Bac-Plus-Dez-19.pdf (accessed April 13, 2025).
22. Fulenchek J, Glenn D, Fite M, Clark C. Comparing the microbial removal efficacy of new and reprocessed microfiber on health care surfaces. Am J Infect Control. (2022) 50:1274–6. doi: 10.1016/j.ajic.2022.05.002
23. Frota OP, Ferreira AM, Guerra OG, Rigotti MA, Andrade DD, Borges NM, et al. (2017). Eficiência da limpeza e desinfecção de superfícies: correlação entre métodos de avaliação. Rev Bras Enferm. 70, 1176–83. doi: 10.1590/0034-7167-2016-0608
24. Furlan MC, Ferreira AM, Rigotti MA, Guerra OG, Frota OP, Sousa AF, et al. Correlação entre métodos de monitoramento de limpeza e desinfecção de superfícies ambulatoriais. Acta Paul Enferm. (2019) 32:282–9. doi: 10.1590/1982-0194201900039
25. Santos Junior AG, Ferreira AM, Rigotti MA, Santos FR, Furlan MC, Andrade DD. Avaliação da eficiência da limpeza e desinfecção de superfícies em uma unidade básica de saúde. Texto Contexto Enferm. (2018) 27:e3720017. doi: 10.1590/0104-07072018003720017
26. Centers for Disease Control and Prevention. Options for Evaluating Environmental Cleaning: Centers for Disease Control and Prevention. (2014). Available online at: https://www.cdc.gov/hai/toolkits/evaluating-environmental-cleaning.html (accessed May 20, 2017).
27. Depré R, Hondeghem A, Moreels A. Motivatie van ambtenaren-voorwaarde voor een efficiënt en effectief bestuur. Federale diensten voor Wetenschappelijke, Technische en Culturele Aangelegenheden en V.C.O.B. (1995). Available online at: https://lib.ugent.be/nl/catalog/rug01:000333704 (accessed April 13, 2025).
28. Vandenabeele W. The mediating effect of job satisfaction and organizational commitment on self-reported performance: more robust evidence of the PSM-performance relationship. Int Rev Adm Sci. (2009) 75:11–34. doi: 10.1177/0020852308099504
29. Rigonato EM, de Pádua Lima H, de Sousa Alvaro AF, dos Santos JL, Maria Jorge B, Klock P, et al. Cleaning and disinfection of surfaces in a COVID-19 respiratory syndrome unit: a quasi-experimental study. Coronaviruses. (2024). doi: 10.2174/0126667975333048241025050846
30. Bernardes LO, Dos Santos FR, Angeloni NLN, Ribeiro Furlan MC, Barcelos LDS, Ferreira AM, et al. Monitoring of surface cleaning and disinfection in a Brazilian pediatric unit. Ther Adv Infect Dis. (2023) 10:20499361221148007. doi: 10.1177/20499361221148007
31. Alvim AL, Pimenta FG, Coelho AD, da Costa Carbogim F, de Abreu Varoto A, Ferreira AM, et al. Assessment of soiling on highly touched clinical surfaces in intensive care units. Florence Nightingale J Nurs. (2023) 31:188. doi: 10.5152/FNJN.2023.23027
32. Chiguer M, Maleb A, Amrani R, Abda N, Alami Z. Assessment of surface cleaning and disinfection in neonatal intensive care unit. Heliyon. (2019) 5:e02966. doi: 10.1016/j.heliyon.2019.e02966
33. Parry MF, Sestovic M, Renz C, Pangan A, Grant B, Shah AK. Environmental cleaning and disinfection: sustaining changed practice and improving quality in the community hospital. Antimicrob Steward Healthc Epidemiol. (2022) 2:e113. doi: 10.1017/ash.2022.257
34. Cabay-Huebla KE, Noroña-Salcedo DR, Veja-Falcon V. Relationship between job stress and job satisfaction of the administrative staff of the general hospital riobamba. Revista Médica Electrónica. (2024) 44:69–83. Available online at: https://www.medigraphic.com/pdfs/revmedele/me-2022/me221g.pdf
35. Pirino MVB, Nascimento Sobrinho CL, Dini AP. Professional satisfaction in nursing during the COVID-19 pandemic. Rev Lat Am Enfermagem. (2023) 31:e3893. doi: 10.1590/1518-8345.6364.3895
36. Vieira GC, Granadeiro DD, Raimundo DD, Silva JF, Hanzelmann RD, Passos JP, et al. (2021). Professional satisfaction and quality of life of nurses in a brazilian hospital. Av Enferm. 39, 52–62. doi: 10.15446/avenferm.v39n1.85701
37. Rodrigues M, Gaspar F, Lucas P. A satisfação profissional dos enfermeiros em contexto hospitalar: revisão scoping. N Trends Qual Res. (2022) 13:e650. doi: 10.36367/ntqr.13.2022.e650
38. Almeida GM, Magalhães Alves ME, Rodrigues Bastos R, Sueli do Vale Marinho C, Costa Arantes D, Silva do Nascimento L. Impacto do processo de trabalho e da atenção ao câncer de boca no desempenho das equipes de saúde bucal em estado amazônico. Arquivos em Odontologia. (2022) 58:21–31. doi: 10.35699/2178-1990.2022.29072
Keywords: disinfection, infection control, training programs, personal satisfaction, work performance
Citation: Silva MHN, Ciofi-Silva CL, Souza VS, Rocha DM, Sousa AFL, Felix AMS and Santos Júnior AG (2025) Comparative effectiveness of a multimodal intervention package on surface cleaning and disinfection in Brazilian neonatal intensive care units. Front. Public Health 13:1557538. doi: 10.3389/fpubh.2025.1557538
Received: 08 January 2025; Accepted: 24 March 2025;
Published: 06 May 2025.
Edited by:
Xiaodong Gao, Fudan University, ChinaReviewed by:
Brian Crook, Health and Safety Laboratory (HSL), United KingdomMarija Spevan, University of Rijeka, Croatia
Copyright © 2025 Silva, Ciofi-Silva, de Souza, Rocha, de Sousa, Felix and Santos Júnior. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alvaro Francisco Lopes de Sousa, c291c2EuYWx2YXJvbWRAZ21haWwuY29t