 Maria Wemrell1,2*
Maria Wemrell1,2* Mariam Hassan2,3,4
Mariam Hassan2,3,4 Raquel Perez-Vicente2
Raquel Perez-Vicente2 Martin Lindström5,6Johan Öberg2,3
Martin Lindström5,6Johan Öberg2,3 Juan Merlo2,5
Juan Merlo2,5- 1Department of Social Work, Faculty of Social Sciences, Linnaeus University, Växjö, Sweden
- 2Unit for Social Epidemiology, Faculty of Medicine, Lund University, Malmö, Sweden
- 3Department of Health and Medical Care Management, Region Skåne Corporate Office, Malmö, Sweden
- 4Department of Clinical Sciences Malmö, Section for Family Medicine and Community Medicine, Lund University, Malmö, Sweden
- 5Centre for Primary Health Care Research, Region Skåne, Malmö, Sweden
- 6Social Medicine and Health Policy, Faculty of Medicine, Lund University, Malmö, Sweden
Introduction: Trust in healthcare is central to the delivery of care and unequally distributed between groups in society. Experiences of perceived discrimination have been associated with lack of such trust. Although the importance of trust in healthcare has been highlighted in recent years, studies in this area are relatively scarce.
Materials and methods: We investigated the risk of low trust in healthcare in Sweden, using data from 11 consecutive National Public Health Surveys conducted in 2004–2014 (n = 83,135). Applying an analysis of individual heterogeneity and discriminatory accuracy (AIHDA), we investigated the risk of low trust in healthcare across intersectional strata defined by experiences of perceived discrimination as well as sex/gender, educational level, migration status and age. We calculated strata-specific prevalences and prevalence ratios (PR) with 95% confidence intervals (CI). The area under the receiver operating characteristic curve (AUC) was computed to evaluate the discriminatory accuracy (DA) of the intersectional strata.
Results: The overall prevalence of low trust in healthcare was 25.9%. While low trust was more common among individuals born abroad, with low education and of younger age, discrimination increased the risk of low trust in healthcare over and above the sociodemographic characteristics. The strata with the highest risk of low trust were foreign-born men aged 55–64 years with low income who had experienced discrimination (PR 3.13 [95% CI 2.49–3.95]) and foreign-born women aged 25–34 years with high education who had experienced discrimination (PR 3.05 [95% CI 2.50–3.73]). The DA of the intersectional strata was small (AUC = 0.64), indicating large overlaps between and heterogeneities within strata.
Conclusion: As experiences of discrimination, in healthcare and elsewhere, are associated with lack of trust in healthcare, it is incumbent on healthcare professionals to maintain trustworthiness by mitigating discriminatory practices including through striving toward patient-centered communication and care. Such efforts should be universal, although proportionally tailored to mitigate discrimination against patients with a migration background.
Introduction
Trust in healthcare is central to the delivery of care and to the patient-provider relationship. It can affect people’s willingness to seek care, reveal health-related information, participate in screening or testing, receive and adhere to treatment, follow public health recommendations and participate in research (1–4). Trust in healthcare has also been associated with better health outcomes, including self-rated and mental health, higher quality of life and stronger patient satisfaction (2, 5–7). As it is typically not equally distributed between population groups, lack of trust in healthcare can contribute toward and exacerbate health inequities (3, 8–10).
The issue of trust in healthcare has become intensely actualized in recent years, not least in association with the COVID-19 pandemic (4, 11), as changes in public trust in healthcare have been referred to in terms of an erosion or a crisis (12, 13). Research on trust in healthcare is nonetheless relatively scarce [(e.g., 9)], as Gille, Smith and Mays (12) indicate a clear imbalance between the centrality of trust for the functioning of healthcare and the low priority awarded to it in research.
Further research has been called for on the antecedents of lack of trust in healthcare (3), on how such trust is distributed between sociodemographic groups (9), how social and health inequalities associated with low trust can be addressed (4), and what behaviors or forms of communication may mitigate or aggravate lack of trust (4). Regarding the latter, studies have shown correlations between distrust in healthcare and previous experiences of discrimination (11, 14–17), i.e., differential and negative treatment of individuals due to being categorized as belonging in a particular demographic group [cf. (18)].
Aspects and determinants of trust in healthcare
While the lack of a clear definition of trust in healthcare has been noted (12, 19), conceptualizations of trust commonly stress the optimistic acceptance of a vulnerable situation in which the patient or care receiver believes that the healthcare provider will care for the patient’s best interests (1, 9).
Trust in healthcare has been seen to involve trust in the healthcare provider’s competence or expertise and in their motives, i.e., their good will or values aligning with one’s own (15, 20). Hall et al. (1) distinguish between five dimensions of trust, namely overall or global trust alongside trust in the healthcare provider’s fidelity (i.e., pursing the patient’s rather than any other competing interest), competence, honesty and confidentiality. Similarly, Griffiths et al. (19) relate medical trust to the components of healthcare competence, benevolence, integrity, predictability and quality assurance. Trust in healthcare can furthermore be separated into vertical trust in healthcare institutions and horizontal trust, or in the presence of a power gradient vertical trust, in individual healthcare professionals (2). Some have emphasized public or social dimensions of trust in healthcare, as being tied to confidence not only in the safety and efficacy of medical interventions, or in healthcare professionals, but also in the healthcare system, the research community, governmental regulatory or public health agencies, the mass media and society at large (12, 13, 15, 21). Moreover, distinctions can be made between trusting attitudes and trusting behaviors (1, 22) or between epistemic trust in the provided information and recommendation trust expressed through acting on that information (21, 23). Researchers have also distinguished between the evaluation of public or patient trust in healthcare and of the trustworthiness of healthcare, as trust is not necessarily always well founded but can also be misguided or blind (1). This is while lack of trust can be seen as a reasonable and legitimate response to previous negative experiences (19). Rather than categorically trusting or distrusting healthcare, patients can trust healthcare on some issues and not on others, and trust can change based on new information or experiences (19, 22). Due to the importance of building and maintaining trust, Gill, Smith and Mays (24) argue that measures of trust could be used as quality indicators of healthcare systems.
Having found a lower mortality rate among those with moderate trust in the healthcare system, compared to those with high trust, in the context of long waiting times for treatment, Lindström and Pirouzifard (25) conclude that strong trust may be less advantageous for patients through increasing the likelihood of accepting information and waiting times without asking questions or seeking alternatives. Other research shows correlations between trust in healthcare and positive self-rated health outcomes (7). A study using data from the same National Survey of Public Health in Sweden as the current one, although only from the year 2006 (6), showed that very low trust in healthcare was associated with an increased risk of psychological distress.
Lack of trust in healthcare is, as noted, typically not equally distributed across populations. In countries including Sweden, where a regional study found that 31.5% of the population did not strongly trust the health system (9), lower levels of such trust have been identified among racialized groups (3, 8, 9). Low trust in healthcare has also been found in groups with lower income or education (9, 10), although study results diverge results on this point (9, 26). Associations vary with regard to gender, with men reporting lower trust in some populations (27) and women in others (9). More consistently, lower trust has been found in younger age groups (9, 26).
Regarding reasons behind changing or faltering trust in healthcare in recent decades, many discussions have focused on the use of social media and the internet at large (11, 22). Lay online communication about health has often been associated with contestation of expert knowledge and the spread of misinformation (28, 29). The latter has been most intensely discussed in relation to vaccine hesitancy (30, 31), but also in connection with other health issues [(e.g., 32, 33)]. While the contemporary online information landscape is of obvious and crucial relevance for communication about and trust in healthcare today, previous research has also pointed to different aspects of healthcare itself as impacting trust. Continuity in care (34), waiting times (35), concerns regarding profit motives in healthcare (13, 15, 22) and the expertise (35–37) and interpersonal skills (1, 35, 37–39) of healthcare providers have thus been shown to affect such trust.
Personal experiences or historical examples of social inequality and discrimination are other factors noted to be associated with lack of trust in healthcare (11, 14–17). Discrimination has been tied to a lack of trust in healthcare when having occurred in a healthcare setting or elsewhere (3, 16), on an interpersonal or a structural level (16). Trust in healthcare has been shown to be affected not only by personal experiences of discrimination, but also by hearing about discrimination against others (3). Direct or vicarious experiences leading to a lack of trust in healthcare have included discrimination alongside stigmatization, poor treatment and inadequate communication in healthcare (17). While discrimination and other forms of differential treatment can be difficult to disentangle (40), measures of personal discrimination (18, 41) have included being treated with less courtesy or respect than other people, receiving poorer services than others or not being listened to. In the contemporary setting, experiences of discrimination have been tied to a lack of trust in healthcare overall as well as to lower acceptance of COVID-19 vaccination (42–44) and other recommended protective behaviors in the context of the pandemic (16).
A large share of studies on links between discrimination and trust in healthcare have focused on racialization (17, 45). Notably, Armstrong et al. (46) found that lower levels of trust in healthcare reported by African Americans, compared to white people, could be explained by experiences of racial discrimination. Discrimination based on other grounds, such as gender, sexual or gender minority status (19, 47), disability (48) or obesity (49), are also likely to have negative effects on trust in healthcare (50, 51). Relatedly, without necessarily specifying the attributed grounds for the treatment, studies conducted in a range of healthcare contexts have linked experiences of not being taken seriously by medical professionals to a lessening of trust in healthcare (22, 32, 35, 36, 38, 52, 53).
In Sweden, lower levels of trust in healthcare have been found among racialized groups (9, 54), and perceived discrimination has been tied to a lack of trust in healthcare among refugees (8). This is while 10% of reported cases of discrimination experienced by individuals with migration backgrounds in this country occurred in healthcare (55). Perceived discrimination has also been associated with refraining from seeking healthcare (56, 57). A lack of trust in healthcare has furthermore been found in more, rather than less, socioeconomically privileged groups in Sweden, as elsewhere (9, 26), as the distribution of such trust may be complex and changing [cf. (26)].
An intersectional perspective on trust in healthcare
While differences, including complex or potentially changing ones, have thus been found between groups defined by sociodemographic categorizations or experiences of discrimination, research is still scarce, not least in a Swedish context (9). In response to calls for integrating an intersectional perspective in quantitative population health research (58–60), i.e., conceptualizing and analyzing multiple dimensions of privilege and disadvantage in society as interlocking rather than as separate (61), an intersectional perspective can add valuable knowledge about the distribution of low trust in healthcare between population groups. Relatedly, studies of health inequalities including those pertaining to trust in healthcare may oversimplify differences by only assessing average differences between groups, thus disregarding heterogeneities in and overlaps between groups, potentially leading to unnecessary stigmatization of “high–risk” individuals or groups (62, 63). In response to this, assessments of discriminatory accuracy (DA), i.e., the capacity of the groups under study to accurately classify individuals by the outcome of interest (58, 62, 64), can complement such study.
Aim
This study aims to investigate any associations between lack of trust in healthcare and experiences of perceived discrimination, as well as sociodemographic characteristics, in a nationally representative population sample from Sweden. Applying an analysis of individual heterogeneity and discriminatory accuracy (AIHDA), using an intersectional approach (58, 64, 65), we will examine how trust in healthcare is distributed between groups defined by experiences of perceived discrimination as well as migration background, level of education, sex/gender and age.
Materials and methods
Study population and data collection
In this cross-sectional study, we use data from 11 consecutive National Public Health Surveys (NPHS) conducted in Sweden by the Public Health Agency (PHA) (66), in collaboration with Statistics Sweden and the Swedish Association of Local Authorities and Regions, during 2004–2014. The questionnaires included questions about health, lifestyle and living conditions and were distributed annually from 2004 to 2014, online and via post, to a randomized selected population sample encompassing 20,000 individuals aged 16–84 years. The response rates range from 60.8% in 2004 to 48.1% in 2014 (66). The NPHS database provided to us includes sociodemographic data acquired through record-linkage with population registers managed by Statistics Sweden. In the analyses, the data were weighted and expanded using survey weights provided by Statistics Sweden. For more information on the survey and data, see the NPHS reports (67).
Our sample consists of pooled data from the survey years 2004–2014, encompassing 103,433 respondents. The question about trust in healthcare, which serves as our outcome variable, was removed from 2015 and onwards, which is why we do not include more recent surveys. Participants younger than 25 years (16–24 years) were excluded (n = 9,761), as we use education as an indicator of socioeconomic position and younger individuals may not have had sufficient time to attain a higher education. Missing data on trust in healthcare (n = 2,375), perceived discrimination (n = 775) and educational attainment (n = 4,387) were also excluded. Thus, 83,135 individuals, 91.7% of the original sample (from age 25 years), are included in the study (Figure 1).
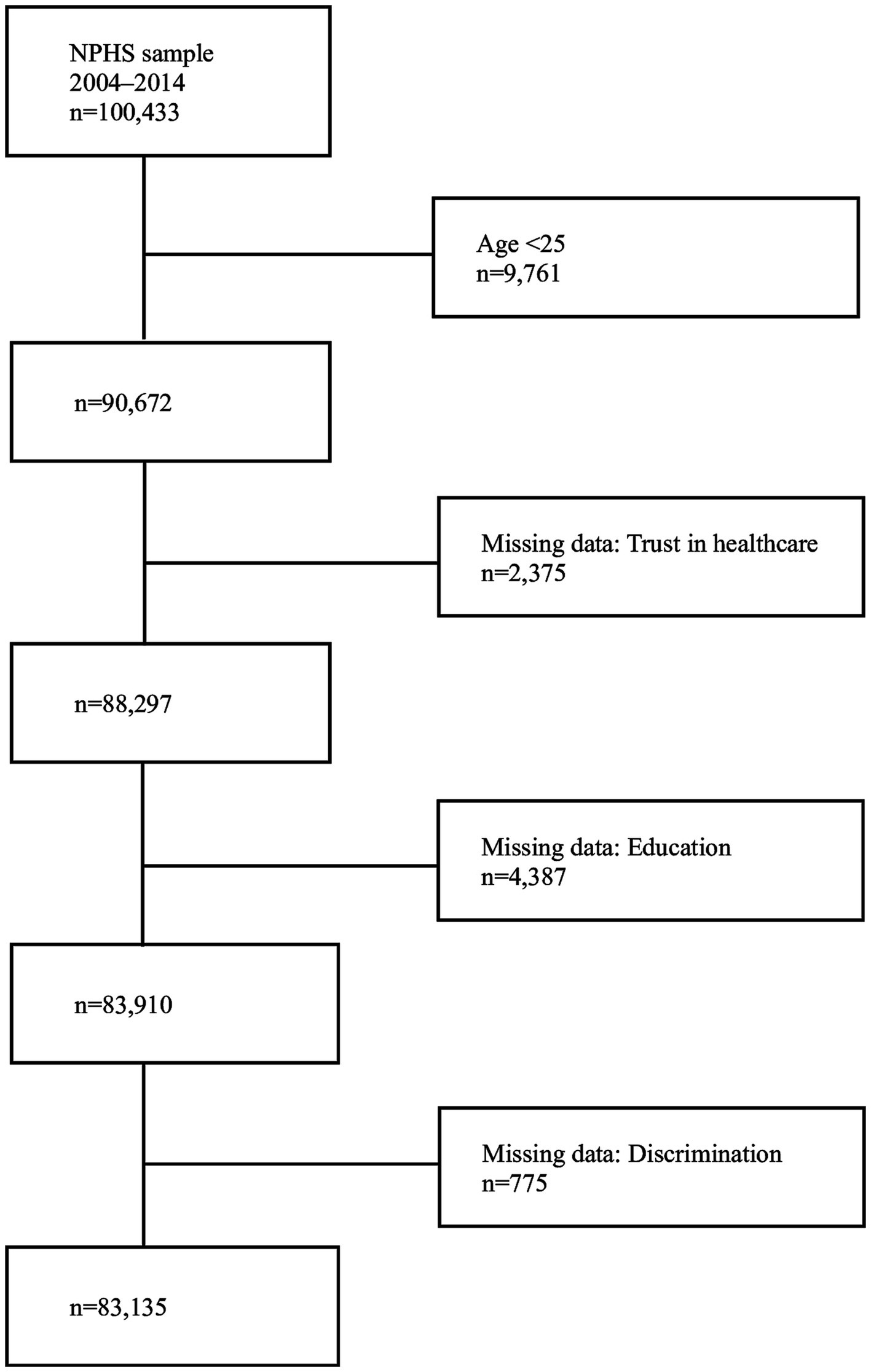
Figure 1. Study sample, with inclusion/exclusion criteria and missing data.
The study was approved by the Swedish Ethical Review Authorities (2019–01793) and by the PHA’s Ethical Council. NPHS respondents gave informed consent prior to participation.
Assessment of variables
Our outcome variable is based on the survey question “How much trust do you have in healthcare,” posed in conjunction with questions about trust in other societal institutions and enabling responses on a five-point scale. These were dichotomized into high vs. low trust (very strong; fairly strong; have no opinion vs. not that strong; not at all).
Perceived discrimination was assessed through the survey question “During the last three months, have you been treated in a way that made you feel humiliated?,” the response options being yes, sometimes; yes, several times; and no. Those responding yes were asked about the perceived grounds for this treatment, with response options including ethnicity, sex/gender, sexual orientation, age, disability, religion, gender identity, appearance, sexual identity, skin color, other, and do not know. These options have varied across the survey years, except for ethnicity, sex/gender, sexual orientation, age, disability, religion, other, and do not know. We therefore used the just noted grounds to construct our variable, in which we categorized those responding other or do not know as non-discriminated. The variable was dichotomized, categorizing respondents as having experienced perceived discrimination or not (yes vs. no), based on any of the noted grounds. We use the terms discriminated and discrimination synonymously with the perceived phenomena.
Information on sex/gender, obtained from the population register, was coded as female vs. male. Age was classified into four groups (25–34; 35–54; 55–64; 65–84 years). Education was dichotomized as high vs. low, with secondary schooling (12 years) or less being considered low and any tertiary studies as high. Migration status was dichotomized as native-born vs. foreign-born, with native-born respondents being born in Sweden and foreign-born ones in any other country.
We constructed an intersectional or multicategorical variable by combining the categories of discrimination, sex/gender, age, migration, and education into 64 strata (2 × 2 × 4 × 2 × 2 = 64). The reference stratum used in the analysis was native men aged 35–54 years with a high educational level who had not experienced discrimination. This stratum was assumed to occupy the position of the highest structural privilege and therefore have the lowest risk of reporting low trust in healthcare.
Statistical analyses
We applied an analysis of individual heterogeneity and discriminatory accuracy (AIHDA) using an intersectional approach, as described in detail elsewhere (58, 64). The purposes of the analysis were (i) to map the distribution of low trust in healthcare across the variables including the 64 intersectional strata, and (ii) to assess the discriminatory accuracy (DA) of the statistical models, i.e., the capacity of the variables used to accurately distinguish between individuals with low versus high trust in healthcare.
We calculated the prevalence or absolute risk, with 95% confidence intervals (CI), of low trust in healthcare in the respective categories and strata. We also assessed the absolute risk difference or attributable risk due to discrimination (ARD), with 95% CIs, for each pair of strata differing only on experiences of discrimination. These measures provide information about the risk of low trust in healthcare that could be eliminated through the absence of experiences of discrimination in the respective strata.
We used eight consecutive regression models to measure differences between categories and strata. Since the prevalence of low trust in healthcare was relatively high (25.9%) we used Cox proportional hazard regression with a constant follow-up time equal to 1 to obtain prevalence ratios (PR) with 95% confidence intervals (CI) (68). Model 1 included only survey year. Model 2 added one variable at a time, with Model 2a including age, Model 2b including sex/gender, Model 2c including migration status, Model 2d including education and Model 2e including discrimination. In Model 3 all these variables were entered simultaneously. Model 4 included the same information but using the multicategorical variable.
To assess the DA of the models, we obtained the received operating characteristics (ROC) curve and calculated the area under the curve (AUC) for each model (69). The ROC curve plots the true positive fraction (sensitivity) against the false positive fraction (1-specificity) across thresholds of predicted probability of low trust in healthcare. The larger the AUC (0.5–1), the larger the DA. In accordance with the criteria proposed by Hosmer and Lemeshow (70), we assess the DA as absent or very small (0.50 ≤ AUC ≤ 0.60), small (0.60 < AUC ≤ 0.70), large (0.70 < AUC ≤ 0.80), or very large (AUC > 0.80).
Results
The prevalence of low trust in healthcare in the pooled survey database was 25.9% (Table 1A). This prevalence remained relatively stable over the study period, although showed a slight u-shape, as it was higher in the first and final years (29.5% in 2004; 28.5% in 2014) and below 25% during 2008–2011. Overall, 12.4% of the respondents reported very strong trust and 60% indicated fairly strong trust. No opinion was reported by 2%. A small group, 2.7%, responded that they had no trust at all, while 23.2% reported that their trust was not that strong. The prevalence of low trust in healthcare decreased with age, being 8.3% higher in the youngest age group than in the oldest one. Low trust was more common among foreign-born individuals (37%) compared to those born in Sweden (23.9%), among those with low (27.8%) compared to high education (22.6%) and, very slightly so, among females (26.5%) compared to males (25.4%). The prevalence of low trust in healthcare was 19% higher among individuals who had experienced discrimination (44.1%), compared to those who had not (25.0%).
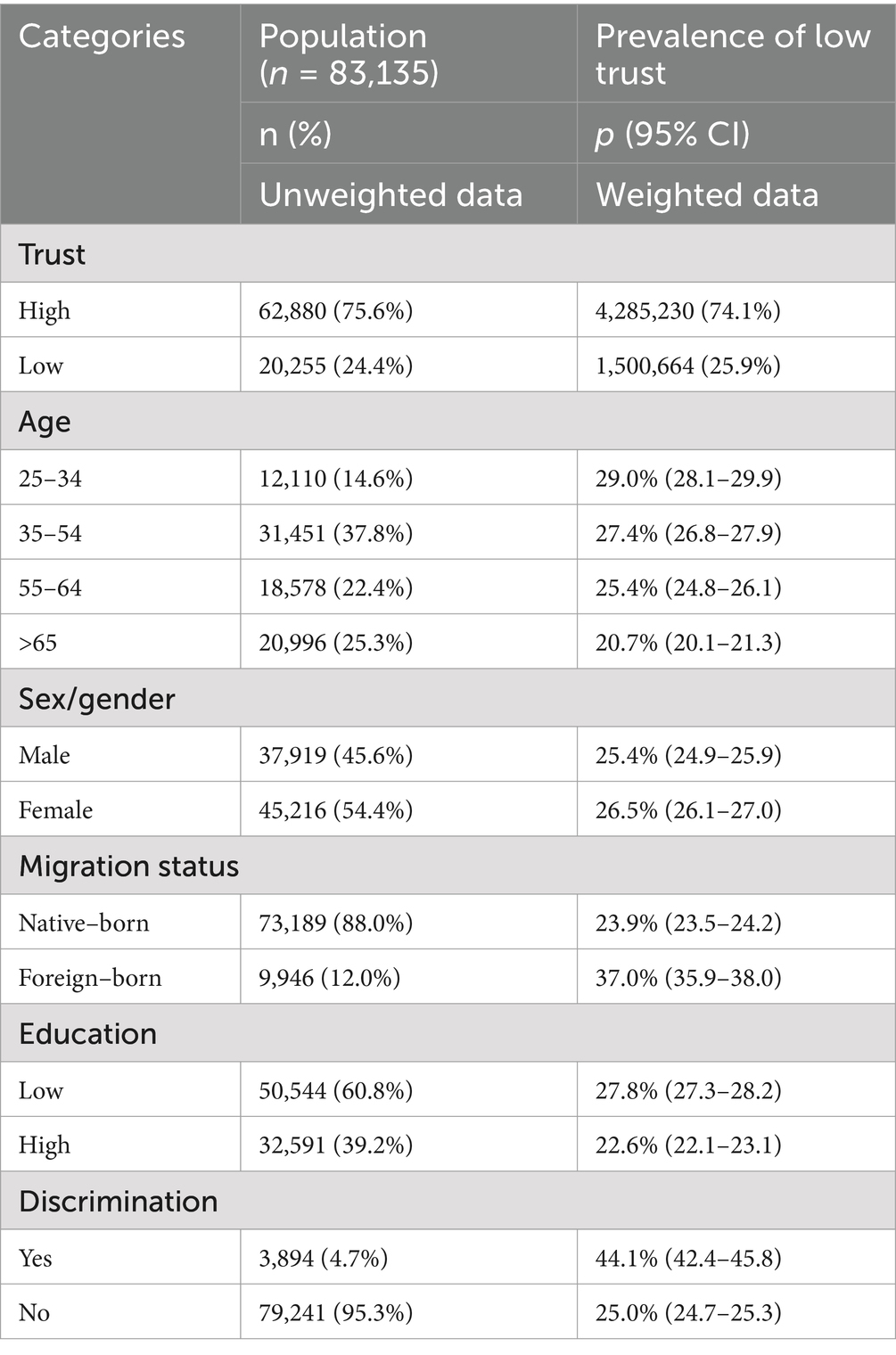
Table 1A. Description of the population and prevalence of low trust in healthcare, by categories of age, sex/gender, migration status, education and perceived discrimination, using NPHS data from 2004 to 2014.
Table 1B shows the prevalence of low trust in healthcare in the 64 intersectional strata. In 12 strata, the share of respondents reporting low trust in healthcare was above 50%. All these strata comprised individuals who had experienced discrimination. Eleven included foreign-born individuals, the exception being native-born men aged 25–34 years with a low education who had experienced discrimination. Eight of the strata comprised men, and seven included individuals with low education. The highest prevalence of low trust was found among foreign-born men with low education, 50–64 years old, who had experienced discrimination (64.2% [95% CI 48.8–77.1]) and foreign-born women aged 25–34 years with high education, who had experienced discrimination (62.4% [95% CI 50.1–73.3]).
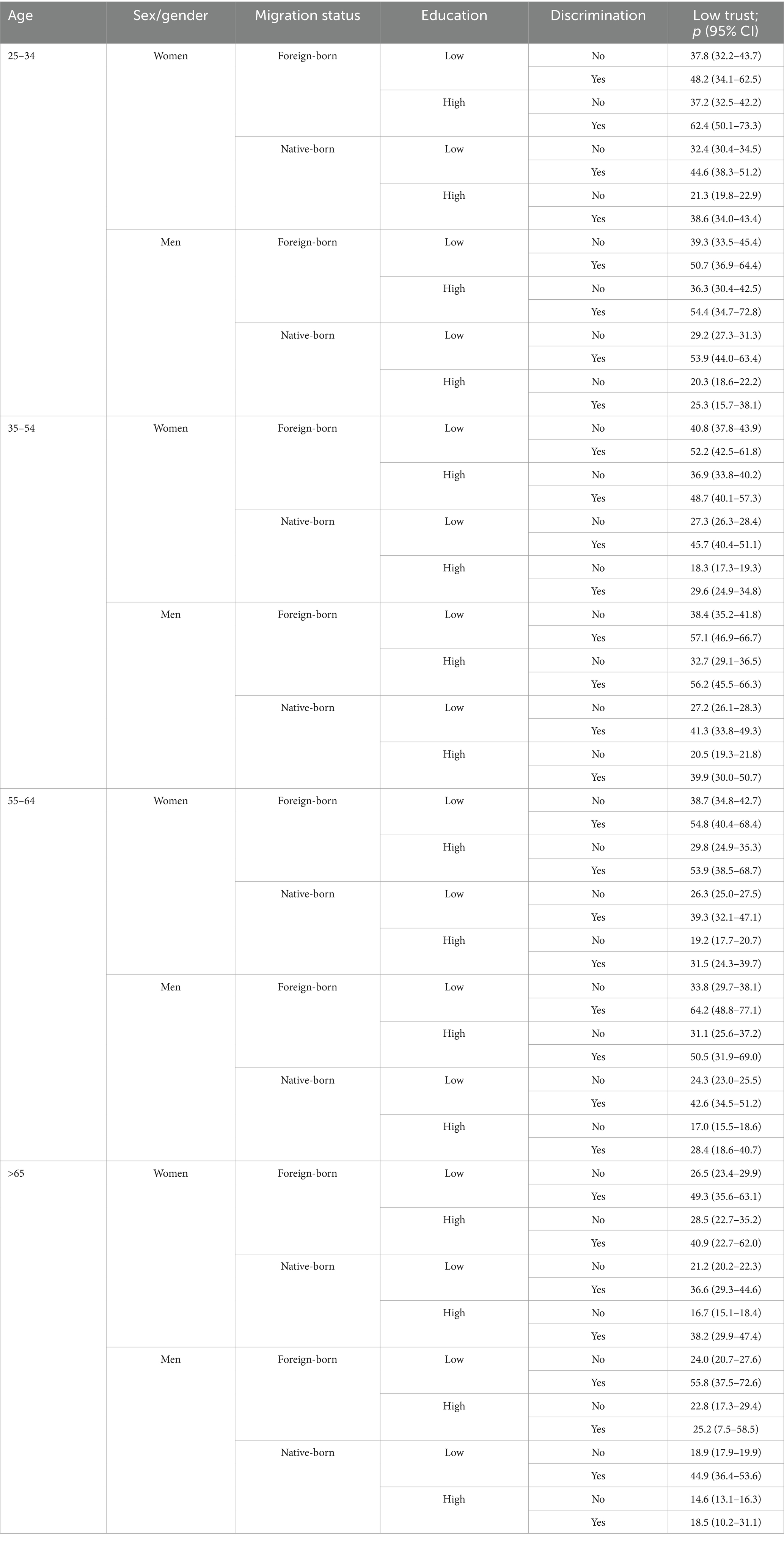
Table 1B. Prevalence of low trust in healthcare, with 95% confidence intervals, for intersectional strata combining categories of age, sex/gender, migration status, education and experiences of perceived discrimination, using weighted NPHS data from 2004 to 2014.
In seven strata, the prevalence of low trust was lower than 20%. All of these included native-born individuals. Six comprised people who had not experienced discrimination, the exception being a stratum including native men with high education, aged 65 years or more. Six of the strata included people with high education, four included men and four were comprised of individuals aged 65 years or more. The lowest prevalence was found among native-born men and women with high education, aged 65 years or more, who had not experienced discrimination (14.6% [95% CI 13.1–16.3]; 16.7% [95% CI 15.1–18.4]).
Accordingly, the regression analysis of the intersectional strata (Model 4; Table 2A) showed that in 10 strata the risk of low trust in healthcare was 2.5 to 3.1 times higher than in the reference stratum. Again, all but one of the strata with the highest risk included foreign-born individuals who had experienced discrimination, whereas their sex/gender, age and level of education varied.
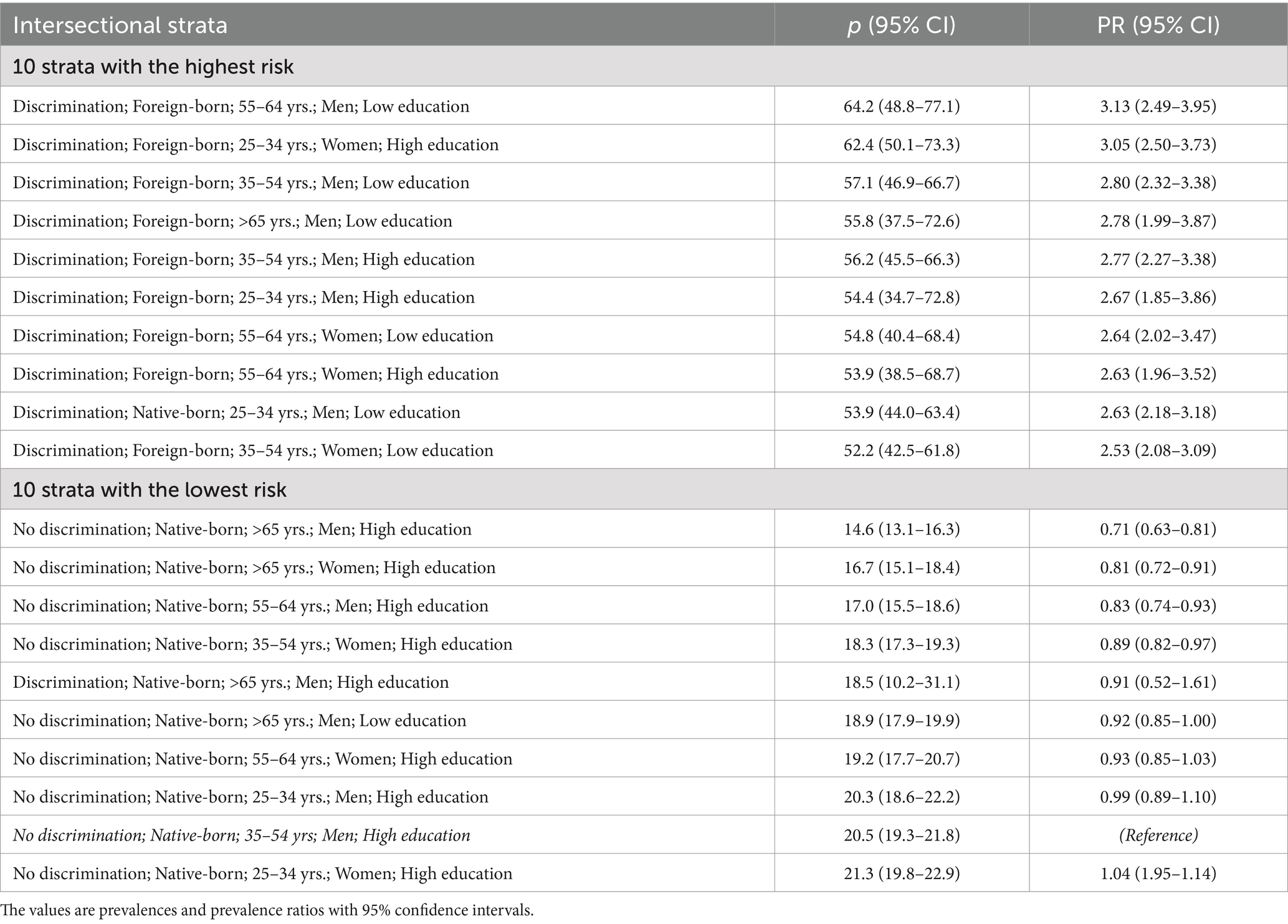
Table 2A. The 10 strata with the highest and lowest risk of low trust in healthcare, obtained through regression analysis (Model 4) using weighted NHPS data from 2004 to 2014.
Table 2B shows the ARs of low trust in healthcare in pairs of similar strata differing only on reported discrimination, as well as the ARD attributable to discrimination for each strata pair. Of the 32 strata, 29 showed an ARD ≥ 10, and nine had an ARD ≥ 20. This is while the ARD of eight of the 32 strata were inconclusive. The highest ARD, of 31.81 and 30.43, respectively, were found among foreign-born men with low education, aged 65 + and 55–64. Of the nine strata with an ARD ≥ 20, six included foreign-born individuals and three native-born ones. Five comprised men and five persons with low education.
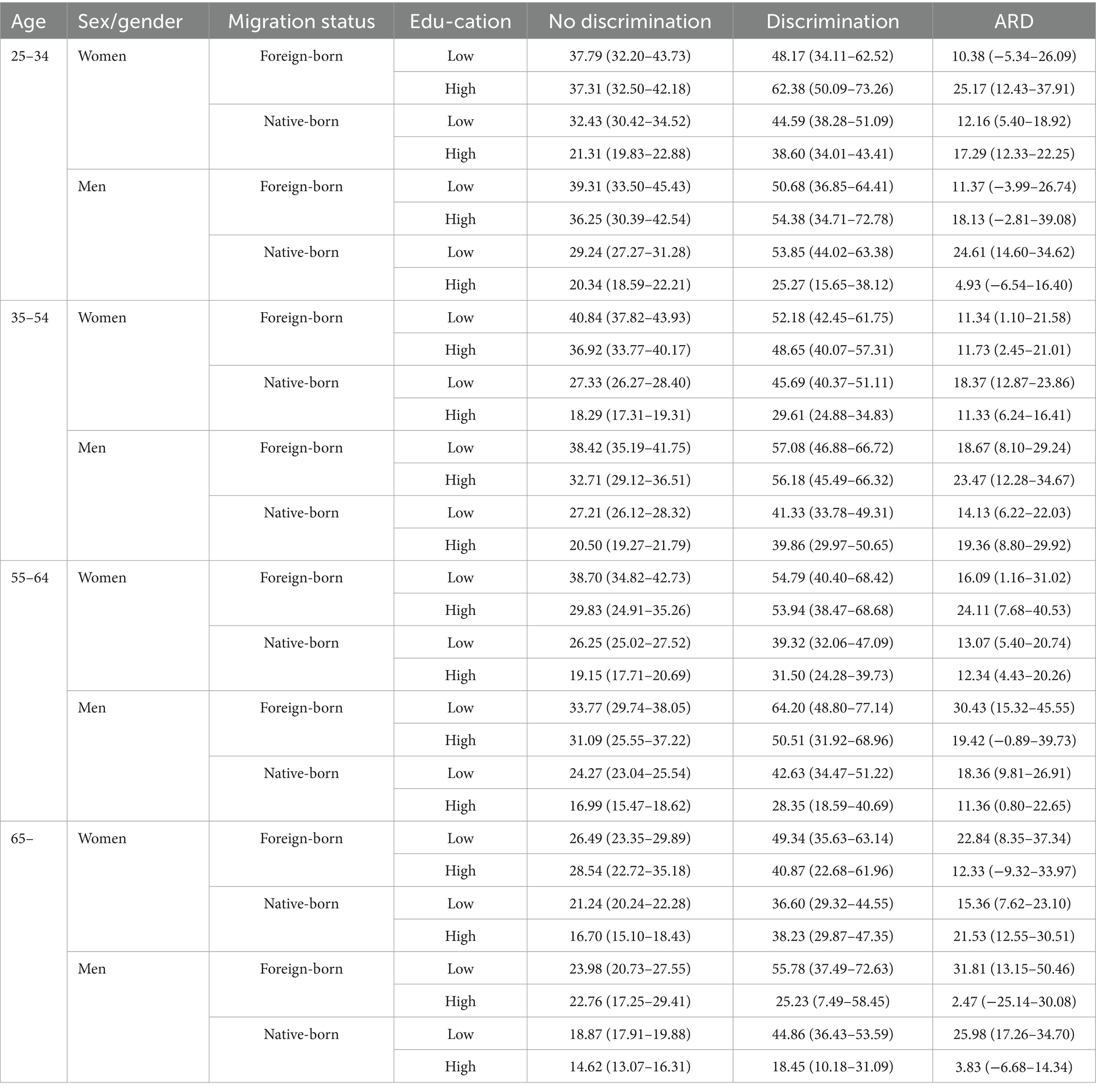
Table 2B. Prevalence or absolute risk (AR) of low trust in healthcare, and absolute risk difference (ARD) attributable to perceived discrimination, with 95% confidence intervals (CI) among pairs of otherwise similar intersectional strata, using weighted NHPH data from 2004 to 2014.
The DA of the strata was small (Table 3), with AUC = 0.61 (0.60–0.61) in Model 4 which includes the intersectional strata. That is, while substantial average differences can be seen between the strata, the group membership’s ability to classify individuals with low vs. high trust is limited due to large individual heterogeneity.

Table 3. Prevalence ratios of low trust in healthcare, with 95% confidence intervals, calculated in eight consecutive regression analyses using weighted NHPH data from 2004 to 2014.
Discussion
This cross-sectional study analyzed the effects of perceived discrimination and sociodemographic variables on trust in healthcare in Sweden, using data from the National Public Health Survey and adopting an AIHDA using an intersectional approach.
Of the survey respondents, 25.9% reported low trust in healthcare. This is similar to the result of a study conducted in northern Sweden, where 31.5% reported low trust in the health system (9). The difference between the two studies is not large, but can be accounted for by the latter excluding those reporting no opinion whereas we included them in the high-trust group, the latter being based on data from 2014 when the prevalence of low trust was at the second highest level in our 2004–2014 data, and the latter being focused on a northern region of Sweden while our sample was nation-wide.
Our finding that trust was lower among foreign-born individuals is also in line with previous research from Sweden and elsewhere, where lower trust was observed among persons with migration background, or with racialized or minority status (3, 8, 9). Other studies have also, like us, found lower trust in younger age groups (9, 26) and among those with lower education, although associations between trust in healthcare and income or educational levels have varied (9, 10, 26). Whereas previous research have observed differing associations with gender (9, 27), we saw no big differences between levels of trust among men and women. Notably, and in line with previous research (3, 15, 17), the strongest association with low trust in healthcare was that of having experienced discrimination.
This association between low trust in healthcare and having experienced discrimination was strengthened in an additional analysis, which distinguished the group reporting no trust at all from those indicating some trust in healthcare. The results of this analysis are available in the supplementary material (S1). Those in the small group reporting no trust at all in healthcare (2.7%) were nearly three times more likely to have experienced discrimination than to have not. Individuals in this group were also more than twice as likely to have a migration background than to be native-born.
The analysis of the intersectional strata, providing a more detailed mapping of the distribution of trust, showed a risk of low trust in healthcare three times higher in some strata compared to the reference group, although a low DA indicated substantial heterogeneities in and overlaps between groups. The strata with the highest prevalence were united by their experiences of discrimination and, in all cases except one, by their migration background, while their gender, age and educational level differed. The stratum comprising individuals without a migration background included men with low education, aged 25–35 years, which invites questions about the nature of the here experienced perceived discrimination. The strata with the lowest risk of low trust in healthcare included individuals born in Sweden who had, in all strata but one, not experienced discrimination. The exception was men aged 65 + with high education, who may have experienced discrimination due to, for example, age, sexual orientation or disability, but who still had strong trust in healthcare.
Moreover, the ARD due to discrimination, i.e., the risk of low trust in healthcare that could be eliminated in the absence of experiences of discrimination in each stratum, was above 10% in 29 of the 32 strata, and above 20% in nine of them.
All these analyses consider discrimination irrespective of where it occurred. However, in 2004–2005, the NPHS posed a question about where or by who the respondent was subjected to humiliating treatment (e.g., healthcare, public employment service, or by close relatives). An additional analysis of this data, the results of which can be found in the supplementary material (S2), showed that of those reporting having experienced discrimination in a healthcare setting, as many as two-thirds (65.6%) indicated low trust in healthcare. This result, which warrants an emphasis, indicates a clear correlation between low trust in healthcare and experiences of perceived discrimination in a healthcare setting.
Mitigating lack of trust in healthcare through avoiding discrimination
In recent years, lack of trust in healthcare has often been discussed in connection to online lay communication about health-related matters (33), including concerns about the spreading of misinformation (28) in the context of significant societal polarization (71). While such contemporary processes are undoubtedly highly relevant, among different and complex factors affecting trust in healthcare today [(e.g., 11)], this study focuses on the link between lack of such trust and experiences of discrimination occurring in healthcare and elsewhere. This link underscores that healthcare professionals and institutions have an important part to play in the building and maintaining of public trust in healthcare, not least among more marginalized populations (14, 42, 72), including through demonstrating or increasing trustworthiness (13, 73) by avoiding discriminatory practices (16, 19).
While discrimination occurring anywhere can affect trust in healthcare (3, 16), healthcare professionals and institutions obviously have limited abilities to respond to discrimination happening elsewhere. They can, however, mitigate discrimination in healthcare settings [cf. (18)].
Whereas further research has been called for on what behaviors and other contributing factors that elicit and sustain trust, how communication establishes, maintains, increases or diminishes trust, and how trust-and relationship-based approaches may help address health inequities (4), existing research (17) indicates that discrimination, alongside bias, stigmatization and inadequate communication, counteract trust in healthcare. Jaiswal (14) points out, for example, that while discrimination and stigma shape lack of trust in healthcare, trust is built through respectful interaction, clear and honest communication and provision of patient choice. Similarly, studies have found that healthcare providers’ interpersonal skills, such as taking patients seriously and treating patients with respect, have been strongly associated with patient trust (35, 38, 39). This has also been indicated in studies of care for racialized minorities, including in Sweden (8), where experiences of being dismissed, receiving inadequate care, and facing racism, have been associated with lack of trust, delay in seeking healthcare and going abroad to seek care (8). Lack of trust in healthcare can also arise from discrimination based on other grounds [(e.g., 19, 50, 51, 74)]. Without specifying the grounds for such treatment, and sometimes referring to limitations in patient-centered care rather than discrimination, studies have pointed to experiences of not being taken seriously, or not being listened to or supported, as being tied to a lessening of trust in healthcare in contexts including rare forms of cancer (36), endometriosis (37), chronic pain (53), contraceptive care (32, 52), and use of forms complementary or fringe medicine (22). Accordingly, the importance of patient-provider communication (6, 12), or of relationship-centered (11) or patient-centered care (32, 35), for the building of trust has been repeatedly emphasized. For this purpose, patient-centered communication should be respectful, emphatic, actively listening and involve adequate sharing of information (11, 12, 36, 72).
Our increasingly heterogeneous information environment can be seen to only increase the importance of healthcare providers doing what they can to safeguard patient trust (75). In this context, maintaining patient trust through patient-centered communication can encompass willingness toward open communication and dialog about patient concerns potentially including diverse issues or sources of information (22). This is while experiences of being dismissed or stigmatized by healthcare professionals have been noted among reasons for turning to online support groups (32, 37), and as experiences of discrimination have been shown to affect adherence to counter-authority beliefs regarding COVID-19 (16). Commenting on COVID-19 vaccine uptake, Paul et al. (42) observe that focusing only on aspects of information or misinformation will likely not serve to address mistrust that is largely due to past experiences of discrimination. Relatedly, it has been observed that practices of dismissing or ridiculing those hesitant or skeptical toward public health recommendations seen during the COVID-19 pandemic are likely to have diminished rather than augmented trust in healthcare (21), and researchers (76–78) have argued against practices of online content moderation, deplatforming or censorship of health-related content for reasons including that it will likely deepen lack of trust in healthcare. That is, while it is obviously important to counter false information (11), open and respectful communication and discussion remain highly important for the maintaining of trust in healthcare [(e.g., 12)]. In the contemporary setting, efforts to mitigate lack of trust in healthcare should not disregard the importance of avoiding discrimination, including by strengthening patient-centered communication and care, for maintaining such trust.
There is a relative lack of research on interventions or strategies to reduce discrimination in healthcare settings, and on their effects (79, 80). Such interventions have often been educational, aiming to increase self-reflection, humility and awareness of unconscious bias among healthcare providers, and to improve patient-provider interaction (79, 81, 82). In a small educational intervention conducted in medical training in Sweden (83), for example, case studies constructed after interviews about racism with healthcare staff were discussed and reflected on by students. Another suggested strategy is to begin the educational intervention with a survey in the participant group, as a basis for further discussions and in order to customize the training (84). While such educational elements can be highly important, it has been emphasized that these should be combined with interventions on organizational and policy levels, including long-term reflective approaches, supportive systemic structures, and the recruitment and retention of healthcare providers from minority groups (80, 81, 85). It should be noted here that healthcare providers and students also experience discrimination, by patients (86), teachers, co-students and colleagues (87), and that this needs to be acknowledged and addressed as part of efforts to avoid discrimination in healthcare. Accordingly, and in sum, Smith et al. (16) note that due to its impact on trust in healthcare, explicit and implicit discriminatory practices should be acknowledged and actively mitigated both on the individual level of medical professionals and on institutional levels.
This study presents a mapping of population strata with large average differences in trust in healthcare. At the same time, the DA of those strata is low. That is, while the average risk of low trust is higher for example in groups comprising individuals with a migration background, many persons reporting low trust can be found in the numerically larger groups consisting of people born in Sweden. This is in alignment with the preventive paradox outlined by Rose (88). Accordingly, efforts to avoid discrimination in healthcare should be universal, i.e., directed to the whole population, although proportionally targeted (89) to mitigate discrimination against specific strata such as those including patients with a migration background. This study provides information that can aid the tailoring of such efforts.
Finally, our survey data were gathered 10–20 years ago. Since then, the discrimination of foreign-born individuals has likely not decreased in Sweden (55), as immigration policies have become more restrictive and political debates have included a push for reduced entitlement to healthcare for refugees (90, 91).
Limitations
Alongside its strengths, which include being based on a large national-level data sample, this study has its limitations. Some of these pertain to the variables used. As noted, the concept of trust in healthcare can be conceptualized differently (1, 12, 19) and seen to incorporate various dimensions, such as trust in expertise and motives (20, 37), professionals and institutions (2) or trusting attitudes and behaviors (23). The variable used to measure trust in this study is simplistic, and further research should investigate dimensions of it more closely.
Regarding the measurement of discrimination, perceptions of whether a certain treatment was discriminatory or not may differ between individuals, as perceived or verifiable discrimination and other forms of differential treatment can be hard to disentangle (40). Still, associations between perceived discrimination and lack of trust in healthcare have been repeatedly shown [(e.g., 17)]. Furthermore, our variable fails to encompass the full scope of experiences of discrimination, as it includes responses to survey questions about only five grounds for such treatment. As we excluded grounds of discrimination introduced in the NPHS in more recent years, including skin color and gender identity, such response options may have been chosen as the attributed reason for the discriminatory treatment. Thus, the effects of discrimination on lack of trust in healthcare may have been underestimated. Also, only a small additional analysis using data from 2004 to 2005 pertains specifically to experiences of discrimination in healthcare, as that was the only available data permitting this analysis. In addition, we do not know to what extent the experienced discrimination can be understood to result from conscious or unconscious bias, or other factors such as poor communication skills.
Limitations pertain to the variables included in the intersectional strata. Other relevant dimensions, such as sexual orientation, were not included, sex/gender was included only as a binary variable, and the migration status variable (native-born vs. foreign-born) was very simple (92). A more complex migration status variable, distinguishing between different countries or areas of birth, would have been helpful. This would, however, have strongly increased the number of intersectional strata and many of the strata comprising individuals with a migration background would have been very small. We avoided using intersectional strata containing few or no individuals for the purpose of the statistical analysis, and our variables were based on the data available from the NPHS. Further research on the effects of discrimination on trust in healthcare should examine a more complete selection of grounds for discrimination, while investigating discrimination in healthcare settings and elsewhere.
The survey response rate was limited, at 48.1–60.8%, and decreased over time (66). A non-response analysis of an earlier edition of the NPHS showed that people in younger age groups, born outside Sweden, and with lower education were less likely to respond (93). As this tendency may increase alongside a decreasing response rate, our results may have been affected by survey response selection bias. To address this issue our results were weighted, using weights provided by Statistics Sweden, but this does not eliminate the risk of selection bias.
We used a cross-sectional design, appropriate for the investigation of the prevalence of low trust in healthcare and of correlations between low trust and experienced discrimination as well as sociodemographic variables. This design limits the basis on which the study can be used to draw inferences of causality, however. It could have been conducted using a multilevel MAIHDA approach (58), which was developed for assessing the impacts of intersecting identities or variables, and is rooted in intersectionality theory (60) although it can also be used for other forms of multicategorical analyses [(e.g., 94)]. MAIHDA has clear methodological and conceptual advantages (58, 60, 95). Still, the AIHDA fixed effects approach shares many of those advantages, such as providing an intersectional mapping of average risk and assessing DA. In addition, AIHDA is more accessible and therefore suitable for the analysis of public health surveys or reports [cf. (64)].
Conclusion
As experiences of discrimination in healthcare and elsewhere are associated with lack of trust in healthcare, it is incumbent on healthcare professionals to maintain trustworthiness by mitigating discriminatory practices including through striving toward patient-centered communication and care. Such efforts should be universal, although proportionally tailored to mitigate discrimination against patients with a migration background.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: the data that support the findings of this study are available from the Swedish Public Health Agency on request. Requests to access these datasets should be directed to https://www.folkhalsomyndigheten.se/the-public-health-agency-of-sweden.
Ethics statement
The study was approved by the Swedish Ethical Review Authorities (2019-01793) and by the PHA’s Ethical Council. The studies were conducted in accordance with the local legislation and institutional requirements. NPHS respondents gave informed consent prior to participation.
Author contributions
MW: Conceptualization, Formal analysis, Investigation, Writing – original draft, Funding acquisition, Writing – review & editing. MH: Formal analysis, Writing – review & editing, Investigation. RP-V: Formal analysis, Methodology, Writing – review & editing. ML: Writing – review & editing, Investigation. JÖ: Writing – review & editing, Investigation. JM: Data curation, Methodology, Project administration, Resources, Writing – review & editing, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by FORTE (Grant 2018–00951, PI Wemrell).
Acknowledgments
We thank the Public Health Agency of Sweden for its support and for providing the data for the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1557921/full#supplementary-material
Abbreviations
AIHDA, Analysis of individual heterogeneity and discriminatory accuracy; AUC, Area under the ROC; AR, Absolute risk; ARD, Absolute risk difference; CI, Confidence intervals; DA, Discriminatory accuracy; MAIHDA, Multilevel analysis of individual heterogeneity and discriminatory accuracyNPHSNational Public Health Surveys; PHA, Public Health Agency; PR, Prevalence Ratio; ROC, Receiver operating characteristics curve.
References
1. Hall, MA, Dugan, E, Zheng, BY, and Mishra, AK. Trust in physicians and medical institutions: what is it, can it be measured, and does it matter? Milbank Q. (2001) 79:613–39. doi: 10.1111/1468-0009.00223
2. Mohseni, M, and Lindstrom, M. Social capital, trust in the health-care system and self-rated health: the role of access to health care in a population-based study. Soc Sci Med. (2007) 64:1373–83. doi: 10.1016/j.socscimed.2006.11.023
3. Williamson, LD, Smith, MA, and Bigman, CA. Does discrimination breed mistrust? Examining the role of mediated and non-mediated discrimination experiences in medical mistrust. J Health Commun. (2019) 24:791–9. doi: 10.1080/10810730.2019.1669742
4. Schiavo, R, and Chou, WYS. Reflections and key learnings on the science of trust. J Commun Healthc. (2023) 16:315–9. doi: 10.1080/17538068.2023.2281731
5. Chen, D, and Yang, TC. The pathways from perceived discrimination to self-rated health: an investigation of the roles of distrust, social capital, and health behaviors. Soc Sci Med. (2014) 104:64–73. doi: 10.1016/j.socscimed.2013.12.021
6. Ahnquist, J, Wamala, SP, and Lindström, M. What has trust in the health-care system got to do with psychological distress? Analyses from the national Swedish survey of public health. Int J Qual Health Care. (2010) 22:250–8. doi: 10.1093/intqhc/mzq024
7. Birkhäuer, J, Gaab, J, Kossowsky, J, Hasler, S, Krummenacher, P, Werner, C, et al. Trust in the health care professional and health outcome: a meta-analysis. PLoS One. (2017) 12:e0170988. doi: 10.1371/journal.pone.0170988
8. Svenberg, K, Skott, C, and Lepp, M. Ambiguous expectations and reduced confidence: experience of Somali refugees encountering Swedish health care. J Refug Stud. (2011) 24:690–705. doi: 10.1093/jrs/fer026
9. Baroudi, M, Goicolea, I, Hurtig, AK, and San-Sebastian, M. Social factors associated with trust in the health system in northern Sweden: a cross-sectional study. BMC Public Health. (2022) 22:881. doi: 10.1186/s12889-022-13332-4
10. Richardson, A, Allen, J, Xiao, H, and Vallone, D. Effects of race/ethnicity and socioeconomic status on health information-seeking, confidence, and trust. J Health Care Poor Underserved. (2012) 23:1477–93. doi: 10.1353/hpu.2012.0181
11. Chou, WYS, and Gaysynsky, A. A relationship-centered approach to addressing mistrust. J Commun Healthc. (2023) 16:320–3. doi: 10.1080/17538068.2023.2258683
12. Gille, F, Smith, S, and Mays, N. Towards a broader conceptualisation of ‘public trust’in the health care system. Soc Theory Health. (2017) 15:25–43. doi: 10.1057/s41285-016-0017-y
13. Jamison, A, Quinn, SC, and Freimuth, VS. “You don't trust a government vaccine”: narratives of institutional trust and influenza vaccination among African American and white adults. Soc Sci Med. (2019) 221:87–94. doi: 10.1016/j.socscimed.2018.12.020
14. Jaiswal, J. Whose responsibility is it to dismantle medical mistrust? Future directions for researchers and health care providers. Behav Med. (2019) 45:188–96. doi: 10.1080/08964289.2019.1630357
15. Larson, HJ, Clarke, RM, Jarrett, C, Eckersberger, E, Levine, Z, Schulz, WS, et al. Measuring trust in vaccination: a systematic review. Hum Vaccin Immunother. (2018) 14:1599–609. doi: 10.1080/21645515.2018.1459252
16. Smith, AC, Woerner, J, and Perera, R. An investigation of associations between race, ethnicity, and past experiences of discrimination with medical mistrust and COVID-19 protective strategies. J Racial Ethn Health Disparities. (2022) 9:1430–42. doi: 10.1007/s40615-021-01080-x
17. Benkert, R, Cuevas, A, Thompson, HS, Dove-Medows, E, and Knuckles, D. Ubiquitous yet unclear: a systematic review of medical mistrust. Behav Med. (2019) 45:86–101. doi: 10.1080/08964289.2019.1588220
18. Hausmann, LR, Kressin, NR, Hanusa, BH, and Ibrahim, SA. Perceived racial discrimination in health care and its association with patients' healthcare experiences: does the measure matter? Ethn Dis. (2010) 20:40–7.
19. Griffith, DM, Bergner, EM, Fair, AS, and Wilkins, CH. Using mistrust, distrust, and low trust precisely in medical care and medical research advances health equity. Am J Prev Med. (2021) 60:442–5. doi: 10.1016/j.amepre.2020.08.019
20. Twyman, M, Harvey, N, and Harries, C. Trust in motives, trust in competence: separate factors determining the effectiveness of risk communication. Judgm Decis Mak. (2008) 3:111–20. doi: 10.1017/S1930297500000218
21. Freiman, O. Vaccine hesitancy and the concept of trust: an analysis based on the Israeli COVID-19 vaccination campaign. Minerva. (2023) 61:357–81. doi: 10.1007/s11024-023-09498-9
22. Vuolanto, P, Bergroth, H, Nurmi, J, and Salmenniemi, S. Reconfiguring health knowledges? Contemporary modes of self-care as ‘everyday fringe medicine’. Public Underst Sci. (2020) 29:508–23. doi: 10.1177/0963662520934752
23. Bennett, M. Should i do as i’m told? Trust, experts, and COVID-19. Kennedy Inst Ethics J. (2020) 30:243–63. doi: 10.1353/ken.2020.0014
24. Gille, F, Smith, S, and Mays, N. Why public trust in health care systems matters and deserves greater research attention. J Health Serv Res Policy. (2015) 20:62–4. doi: 10.1177/1355819614543161
25. Lindström, M, and Pirouzifard, M. Trust in the healthcare system and mortality: a population-based prospective cohort study in southern Sweden. SSM-Population Health. (2022) 18:101109. doi: 10.1016/j.ssmph.2022.101109
26. Grant, S, Liao, K, Miller, C, Peterson, S, Elting, L, and Guadagnolo, B. Lower levels of trust in the medical profession among white, younger, and more-educated individuals with cancer. Am J Clin Oncol. (2021) 44:150–7. doi: 10.1097/COC.0000000000000771
27. Ahern, M, and Hendryx, M. Social capital and trust in providers. Soc Sci Med. (2003) 57:1195–203. doi: 10.1016/s0277-9536(02)00494-x
28. Southwell, BG, Niederdeppe, J, Cappella, JN, Gaysynsky, A, Kelley, DE, Oh, A, et al. Misinformation as a misunderstood challenge to public health. Am J Prev Med. (2019) 57:282–5. doi: 10.1016/j.amepre.2019.03.009
29. Wang, Y, McKee, M, Torbica, A, and Stuckler, D. Systematic literature review on the spread of health-related misinformation on social media. Soc Sci Med. (2019) 240:112552. doi: 10.1016/j.socscimed.2019.112552
30. Machingaidze, S, and Wiysonge, CS. Understanding COVID-19 vaccine hesitancy. Nat Med. (2021) 27:1338–9. doi: 10.1038/s41591-021-01459-7
31. Wemrell, M, and Gunnarsson, L. Attitudes towards HPV vaccination in Sweden: a survey study. Front Public Health. (2022) 10:72949. doi: 10.3389/fpubh.2022.729497
32. Wemrell, M, and Gunnarsson, L. Claims in the clinic: a qualitative group interview study on healthcare communication about unestablished side effects of the copper IUD. PLoS One. (2023) 18:e0291966. doi: 10.1371/journal.pone.0291966
33. Crabu, S, Neresini, F, Agodi, MC, and Tosoni, S. Introduction: manufacturing knowledge at the border of science In: F Neresini, MC Agodi, S Crabu, and S Tosoni, editors. Manufacturing refused knowledge in the age of epistemic pluralism discourses, imaginaries, and practices on the border of science. Singapore: Palgrave Macmillan (2024)
34. Doescher, MP, Saver, BG, Franks, P, and Fiscella, K. Racial and ethnic disparities in perceptions of physician style and trust. Arch Fam Med. (2000) 9:1156–63. doi: 10.1001/archfami.9.10.1156
35. Calnan, MW, and Sanford, E. Public trust in health care: the system or the doctor? Qual Saf Health Care. (2004) 13:92–7. doi: 10.1136/qshc.2003.009001
36. Simons, BCR, Hillen, MA, and Aarts, JWM. Disentangling trust of patients with rare cancer in their healthcare professionals and the healthcare system: a qualitative interview study. J Cancer Surviv. (2024) 19:1059–68. doi: 10.1007/s11764-023-01531-w
37. Mikesell, L, and Bontempo, AC. Healthcare providers’ impact on the care experiences of patients with endometriosis: the value of trust. Health Commun. (2023) 38:1981–93. doi: 10.1080/10410236.2022.2048468
38. Croker, J, Swancutt, D, and Roberts, M. Factors affecting patients’ trust and confidence in GPs: evidence from the English national GP patient survey. BMJ Open. (2013) 3:e002762. doi: 10.1136/bmjopen-2013-002762
39. Murray, B, and McCrone, S. An integrative review of promoting trust in the patient–primary care provider relationship. J Adv Nurs. (2015) 71:3–23. doi: 10.1111/jan.12502
40. Bastos, JL, Bernardo, CO, Harnois, CE, Peres, MA, and Paradies, YC. When does differential treatment become perceived discrimination? An intersectional analysis in a southern Brazilian population. Sociol Race Ethnicity. (2017) 3:301–18. doi: 10.1177/2332649216681167
41. Williams, D, Yu, Y, Jackson, J, and Anderson, N. Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol. (1997) 2:335–51.
42. Paul, E, Fancourt, D, and Razai, M. Racial discrimination, low trust in the health system and COVID-19 vaccine uptake: a longitudinal observational study of 633 UK adults from ethnic minority groups. J R Soc Med. (2022) 115:439–47. doi: 10.1177/01410768221095241
43. Savoia, E, P-L, R, and Goldberg, B. Predictors of COVID-19 vaccine hesitancy: socio-demographics, co-morbidity, and past experience of racial discrimination. Vaccine. (2021) 9:767. doi: 10.3390/vaccines9070767
44. Morgan, KM, Maglalang, DD, and Monnig, MA. Medical mistrust, perceived discrimination, and race: a longitudinal analysis of predictors of COVID-19 vaccine hesitancy in US adults. J Racial Ethn Health Disparities. (2023) 10:1846–55. doi: 10.1007/s40615-022-01368-6
45. Washington, A, Chabaan, J, Fakih, A, Ford, S, Rutledge, L, Lilly, J, et al. “Why is it so necessary?”: African American parents’ perspectives on delaying and refusing HPV vaccination. J Pediatr Health Care. (2023) 37:373–80. doi: 10.1016/j.pedhc.2023.01.002
46. Armstrong, K, Putt, M, and Halbert, C. Prior experiences of racial discrimination and racial differences in health care system distrust. Med Care. (2013) 51:144–50. doi: 10.1097/MLR.0b013e31827310a1
47. Ayhan, CHB, Bilgin, H, Uluman, OT, Sukut, O, Yilmaz, S, and Buzlu, S. A systematic review of the discrimination against sexual and gender minority in health care settings. Int J Health Serv. (2020) 50:44–61. doi: 10.1177/0020731419885093
48. Ames, SG, Delaney, RK, and Houtrow, AJ. Perceived disability-based discrimination in health care for children with medical complexity. Pediatrics. (2023) 152:e2022060975. doi: 10.1542/peds.2022-060975
49. Spahlholz, J, Baer, N, König, HH, Riedel-Heller, SG, and Luck-Sikorski, C. Obesity and discrimination–a systematic review and meta-analysis of observational studies. Obes Rev. (2016) 17:43–55. doi: 10.1111/obr.12343
50. Brincks, A, Shiu-Yee, K, and Metsch, L. Physician mistrust, medical system mistrust, and perceived discrimination: associations with HIV care engagement and viral load. AIDS Behav. (2019) 23:2859–69. doi: 10.1007/s10461-019-02464-1
51. Guest, LMH, and Weinstein, N. The effect of healthcare provider support and discrimination on LGBT patients’ trust and adherence. Br Stud Doctor J. (2020) 4:37–9. doi: 10.18573/bsdj.204
52. Caddy, C, Williams, H, Hocking, J, and Coombe, J. “I never went to see that doctor again”: a qualitative study examining Australian women's experiences requesting removal of LARC within 12 months of insertion. Contraception. (2022) 110:81–5. doi: 10.1016/j.contraception.2021.11.006
53. Buchman, DZ, Ho, A, and Goldberg, DS. Investigating trust, expertise, and epistemic injustice in chronic pain. J Bioethical Inquiry. (2017) 14:31–42. doi: 10.1007/s11673-016-9761-x
54. Daerga, L, Sjolander, P, Jacobsson, L, and Edin-Liljegren, A. The confidence in health care and social services in northern Sweden - a comparison between reindeer-herding Sami and the non-Sami majority population. Scand J Public Health. (2012) 40:516–22. doi: 10.1177/1403494812453971
55. Nkulu Kalengayi, FK, Baroudi, M, and Hurtig, A. Prevalence of perceived discrimination, determinants and associations with self-rated general and sexual health, healthcare utilization and self-perceived integration: a cross-sectional survey of migrants in Sweden. BMC Public Health. (2024) 24:699. doi: 10.1186/s12889-024-18160-2
56. Wamala, S, Merlo, J, Boström, G, and Hogstedt, C. Perceived discrimination, socioeconomic disadvantage and refraining from seeking medical treatment in Sweden. J Epidemiol Community Health. (2007) 61:409–15. doi: 10.1136/jech.2006.049999
57. Hassan, M, Öberg, J, Wemrell, M, Perez Vicente, R, Lindström, M, and Merlo, J. Perceived discrimination and refraining from seeking physician’s care in Sweden: an intersectional analysis of individual heterogeneity and discriminatory accuracy (AIHDA). Int J Equity Health. (2024) 23:199. doi: 10.1186/s12939-024-02291-4
58. Merlo, J. Multilevel analysis of individual heterogeneity and discriminatory accuracy (MAIHDA) within an intersectional framework. Soc Sci Med. (2018) 203:74–80. doi: 10.1016/j.socscimed.2017.12.026
59. Kapilashrami, A, Hill, S, and Meer, N. What can health inequalities researchers learn from an intersectionality perspective? Understanding social dynamics with an inter-categorical approach? Soc Theory Health. (2015) 13:288–307. doi: 10.1057/sth.2015.16
60. Leckie, G, Bell, A, Merlo, J, Subramanian, SV, and Evans, C. The statistical advantages of MAIHDA in predicting intersectional inequalities. (2025) Preprint, SocArXic. doi: 10.31235/osf.io/dpyqm_v1
61. Crenshaw, K. Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ Chic Leg Forum. (1989) 1989:139–68.
62. Merlo, J, Mulinari, S, Wemrell, M, Subramanian, SV, and Hedblad, B. The tyranny of the averages and the indiscriminate use of risk factors in public health: the case of coronary heart disease. SSM. (2017) 3:684–98. doi: 10.1016/j.ssmph.2017.08.005
63. Merlo, J. Invited commentary: multilevel analysis of individual heterogeneity-a fundamental critique of the current probabilistic risk factor epidemiology. Am J Epidemiol. (2014) 180:208–12. doi: 10.1093/aje/kwu108
64. Ericsson, L, Wemrell, M, Lindstrom, M, Perez-Vicente, R, and Merlo, J. Revisiting socio-economic inequalities in sedentary leisure time in Sweden: an intersectional analysis of individual heterogeneity and discriminatory accuracy (AIHDA). Scand J Public Health. (2023) 51:570–8. doi: 10.1177/14034948221112465
65. Wemrell, M, Karlsson, N, Perez Vicente, R, and Merlo, J. An intersectional analysis providing more precise information on inequities in self-rated health. Int J Equity Health. (2021) 20:1–10. doi: 10.1186/s12939-020-01368-0
66. Public Health Agency of Sweden. Fakta om nationella folkhälsoenkäten "Hälsa på lika villkor?" (2024). Available online at: https://www.folkhalsomyndigheten.se/folkhalsorapportering-statistik/om-vara-datainsamlingar/nationella-folkhalsoenkaten/fakta-om-nationella-folkhalsoenkaten/ (Accessed June 14, 2024).
67. Statistics Sweden. Teknisk Rapport - En beskrivining av genomförande och metoder “Hälsa på lika villkor” ett nationellt urval. (2014). Available online at: https://www.folkhalsomyndigheten.se/contentassets/9b1b216c596a487ca6c6aa6dc413efb4/teknisk-rapport-nationella-inklusive-bilagor.pdf (Accessed June 15, 2024).
68. Barros, AJ, and Hirakata, VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. (2003) 3:21. doi: 10.1186/1471-2288-3-21
69. Merlo, J, Wagner, P, and Leckie, G. A simple multilevel approach for analysing geographical inequalities in public health reports: the case of municipality differences in obesity. Health Place. (2019) 58:102145. doi: 10.1016/j.healthplace.2019.102145
71. Harambam, J. The corona truth wars: where have all the STS’ERS gone when we need them most? Sci Technol Stud. (2020) 33:60–7.
72. Grasswick, H. Scientific and lay communities: earning epistemic trust through knowledge sharing. Synthese. (2010) 177:387–409. doi: 10.1007/s11229-010-9789-0
73. Wynne, B. Public engagement as a means of restoring public trust in science – hitting the notes, but missing the music? Public Health Genomics. (2006) 9:211–20. doi: 10.1159/000092659
74. Norris, M, and Borneskog, C. The cisnormative blindspot explained: healthcare experiences of trans men and non-binary persons and the accessibility to inclusive sexual & reproductive healthcare, an integrative review. Sex Reprod Healthc. (2022) 32:100733. doi: 10.1016/j.srhc.2022.100733
75. Baron, R, and Berinsky, A. Mistrust in science - a threat to the patient-physician relationship. N Engl J Med. (2019) 381:182–5. doi: 10.1056/NEJMms1813043
76. Armitage, R. Online 'anti-vax' campaigns and COVID-19: censorship is not the solution. Public Health. (2021) 190:e29–30. doi: 10.1016/j.puhe.2020.12.005
77. Baker, SA, Wade, M, and Walsh, MJ. The challenges of responding to misinformation during a pandemic: content moderation and the limitations of the concept of harm. Media Int Aust. (2020) 177:103–7. doi: 10.1177/1329878X20951301
78. Larson, HJ. Blocking information on COVID-19 can fuel the spread of misinformation. Nature. (2020) 580:306–7. doi: 10.1038/d41586-020-00920-w
79. Bohren, MA, Corona, MV, Odiase, OJ, Wilson, AN, Sudhinaraset, M, Diamond-Smith, N, et al. Strategies to reduce stigma and discrimination in sexual and reproductive healthcare settings: a mixed-methods systematic review. PLoS Glob Public Health. (2022) 2:e0000582. doi: 10.1371/journal.pgph.0000582
80. Webster, CS, Taylor, S, Thomas, C, and Weller, JM. Social bias, discrimination and inequity in healthcare: mechanisms, implications and recommendations. BJA Educ. (2022) 22:131–7. doi: 10.1016/j.bjae.2021.11.011
81. Hassen, N, Lofters, A, Michael, S, Mall, A, Pinto, AD, and Rackal, J. Implementing anti-racism interventions in healthcare settings: a scoping review. Int J Environ Res Public Health. (2021) 18:2993. doi: 10.3390/ijerph18062993
82. Höglund, AT, Carlsson, M, Holmström, IK, and Kaminsky, E. Impact of telephone nursing education program for equity in healthcare. Int J Equity Health. (2016) 15:1–11. doi: 10.1186/s12939-016-0447-0
83. Bradby, H, Hamed, S, Thapar-Björkert, S, and Ahlberg, BM. Designing an education intervention for understanding racism in healthcare in Sweden: development and implementation of anti-racist strategies through shared knowledge production and evaluation. Scand J Public Health. (2023) 51:531–4. doi: 10.1177/14034948211040963
84. Höglund, AT, Carlsson, M, Holmström, IK, Lännerström, L, and Kaminsky, E. From denial to awareness: a conceptual model for obtaining equity in healthcare. Int J Equity Health. (2018) 17:1–11. doi: 10.1186/s12939-018-0723-2
85. Cox, AB, Jaiswal, J, LoSchiavo, C, Witte, T, Wind, S, Griffin, M, et al. Medical mistrust among a racially and ethnically diverse sample of sexual minority men. LGBT Health. (2023) 10:471–9. doi: 10.1089/lgbt.2022.0252
86. Lindström, NB, and Girardelli, D. Patient bias in Sweden: an exploratory study on discrimination against migrant physicians. Eur J Health Commun. (2023) 4:73–92. doi: 10.47368/ejhc.2023.204
87. Velin, L, Chew, MS, and Pompermaier, L. Discrimination in an “equal country”—a survey amongst Swedish final-year medical students. BMC Med Educ. (2022) 22:503. doi: 10.1186/s12909-022-03558-6
88. Rose, GA. The strategy of preventive medicine. New York: Oxford University Press; (1992). xii–138 p.
89. Carey, G, Crammond, B, and De Leeuw, E. Towards health equity: a framework for the application of proportionate universalism. Int J Equity Health. (2015) 14:1–8. doi: 10.1186/s12939-015-0207-6
90. Tidöavtalet. Överenskommelse för Sverige. (2022). Available at: https://via.tt.se/data/attachments/00551/04f31218-dccc-4e58-a129-09952cae07e7.pdf (Accessed November 15, 2024).
91. Roos, M. Different systems, similar responses: policy reforms on asylum-seekers’ and refugees’ access to healthcare in Germany and Sweden in the wake of the 2015–17 ‘migration crisis’ In: M-L Jakobson, R King, L Moroşanu, and R Vetik, editors. Anxieties of migration and integration in turbulent times. Switzerland: Springer Nature (2023)
92. Mulinari, S, Bredstrom, A, and Merlo, J. Questioning the discriminatory accuracy of broad migrant categories in public health: self-rated health in Sweden. Eur J Pub Health. (2015) 25:911–7. doi: 10.1093/eurpub/ckv099
93. Statistics Sweden “Hälsa på lika villkor?” Enkät undersökning 2005, Det nationella urvalet [“Health on equal terms?" Survey conducted in 2005, the national sample]. (2005). Available online at: https://www.folkhalsomyndigheten.se/contentassets/9b1b216c596a487ca6c6aa6dc413efb4/teknisk-rapport-med-bilagor-hlv-2005.pdf (Accessed June 15, 2024).
94. Rodriguez-Lopez, M, Leckie, G, Kaufman, JS, and Merlo, J. Multilevel modelling for measuring interaction of effects between multiple categorical variables: an illustrative application using risk factors for preeclampsia. Paediatr Perinat Epidemiol. (2023) 37:154–64. doi: 10.1111/ppe.12932
Keywords: trust in healthcare, discrimination, health inequities, AIHDA, intersectionality, Sweden
Citation: Wemrell M, Hassan M, Perez-Vicente R, Lindström M, Öberg J and Merlo J (2025) Trust in healthcare and perceived discrimination in Sweden: a fixed effects analysis of individual heterogeneity and discriminatory accuracy. Front. Public Health. 13:1557921. doi: 10.3389/fpubh.2025.1557921
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Isain Zapata, Rocky Vista University, United StatesRakesh Sarwal, ESIC Medical College (Faridabad), India
Andrew A. Vernon, The University of Texas at El Paso, United States
Copyright © 2025 Wemrell, Hassan, Perez-Vicente, Lindström, Öberg and Merlo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Wemrell, bWFyaWEud2VtcmVsbEBsbnUuc2U=