 Wenjia Li
Wenjia Li Yuhan Zhu
Yuhan Zhu Xuehua Zhu
Xuehua Zhu- School of Nursing, Zhejiang Chinese Medical University, Hangzhou, China
Objective: This study aims to analyze the specific content and structural characteristics of rehabilitation nursing-related policies in China from 2007 to 2024, utilizing the perspective of policy tools. The goal is to provide insights for the subsequent optimization and enhancement of the rehabilitation nursing policy system.
Methods: According to the classification method of policy instruments proposed by public policy scholars Rothwell and Zegveld, this study identified the X dimension (basic policy instrument) and categorized the included policies into demand-oriented, supply-oriented, and environment-based policies. Simultaneously, in light of multi-level service needs, an analysis of the elements constituting the rehabilitation nursing system was conducted in conjunction with existing research. This led to the summarization of five levels within the rehabilitation nursing system: nursing staff, service objectives, service items, service methods, and safeguard measures. These levels were designated as the Y dimension (service system) for this study. Utilizing this two-dimensional analytical framework, researchers classified and coded relevant policy texts that met established criteria. Subsequently, they analyzed their content and performed a quantitative assessment regarding both quantity and distribution patterns.
Results: A total of 41 policy documents were analyzed, resulting in the extraction of 292 policy terms, and in dimension X, environment-based, supply-based, and demand-based policy instruments comprised 46.58, 36.64, and 16.78%, respectively. In dimension Y, nursing staff, service objectives, service items, service methods, and safeguard measures accounted for 22.95, 12.67, 12.67, 20.89, and 25.00%, respectively. Overall, the rehabilitation nursing policy in China is predominantly characterized by environment-based policy tools, while demand-based policy tools are comparatively underrepresented.
Conclusion: The government has increasingly prioritized rehabilitation nursing care; consequently, the current policy framework is evolving toward greater specialization, standardization, and systematization. Nevertheless, there remains a need to optimize the structural application of policy tools further, particularly concerning enhancing the utilization of demand-side policy instruments.
1 Introduction
With the global population aging at an accelerated pace, the demand for rehabilitation care is rapidly increasing across numerous countries (1). For example, the United States and Japan, as representatives of developed nations, have advanced their rehabilitation care services through initiatives such as the Older Americans Act and long-term care insurance systems (2). However, China faces more complex challenges in this domain. On one hand, its older adult population is significantly larger; on the other hand, disparities in economic development and healthcare resource distribution between urban and rural regions hinder both accessibility to and quality of rehabilitation care. As of 2023, China’s population aged 65 and above has reached 220 million (3), surpassing the combined older adult populations of the United States and Japan. This positions China among those countries with the highest global demand for rehabilitation care (4). This study examines the distribution and characteristics of policy instruments within China’s rehabilitation care framework, providing a case study on how an emerging economy addresses the challenges posed by an aging population while offering valuable insights for other developing nations.
Rehabilitation nursing is a comprehensive service tailored for individuals who are ill, injured, or disabled, emphasizing holistic, continuous, and diverse care (5). At the 2024 National People’s Congress, China reaffirmed the strategic significance of rehabilitation medicine. As an essential component of rehabilitation medicine, rehabilitation nursing not only concentrates on disease treatment but also aims to restore patients’ capacity for independent living (6). Its services cater to all age groups, with particular emphasis on the older adult population. Although rehabilitation care policies are increasingly critical in enhancing public health and addressing the challenges associated with aging, international research has predominantly concentrated on care practices, technological advancements, and patient outcomes (7, 8). Systematic analyses of policy structures and the distribution of policy tools remain limited, particularly those employing textual analysis through the lens of policy instruments. In contrast to the well-established and systematic policy frameworks found in developed countries, developing nations—struggling with transformations in their health service systems—have experienced relatively little comprehensive exploration of rehabilitation care policies (9, 10). This study seeks to fill this gap by analyzing Chinese rehabilitation care policy texts from 2007 to 2024. It identifies key characteristics, distributions of policy tools, and developmental trends, thereby offering new perspectives for international research while providing both theoretical and practical references for optimizing global health policies.
2 Materials and methods
2.1 Search strategy
The primary source of policy data for this study is the “Peking University Legal Information Network.” In alignment with the research topic, keywords such as “rehabilitation nursing” and “rehabilitation services” were utilized as titles, complemented by terms like “nursing”, “care”, “support”, and “assistance” as full-text keywords. To ensure comprehensive coverage of relevant policies, additional documents were sourced from official websites, including the Chinese Government website and the National Health Commission, particularly focusing on their policy and regulatory sections. This methodology was adopted to guarantee both the authority and timeliness of the included policy documents. In this study, rehabilitation care policies are defined as those issued at the central government level that directly or indirectly facilitate the advancement of rehabilitation care services. The search was conducted up to 2024.
2.2 Inclusion and exclusion criteria
Inclusion criteria:
(1) The policy must be issued by government entities, such as the National Health Commission. (2) The content of the policy should be closely related to rehabilitation nursing. (3) The document must be a formal government publication, which includes laws, regulations, plans, opinions, notices, etc. (4) The policy should be current and reflect the latest developments in China’s rehabilitation care sector.
Exclusion criteria:
(1) Policies categorized as “responses, ““replies, “or “letters” are excluded. (2) Documents with lower authority status, such as advisory documents, bulletins, or briefings will not be included. (3) Any documents that merely mention keywords without providing substantial content are excluded. (4) Duplicate documents will also be disregarded.
Based on these criteria, a total of 41 policy documents were ultimately included; some of these are listed in Table 1.
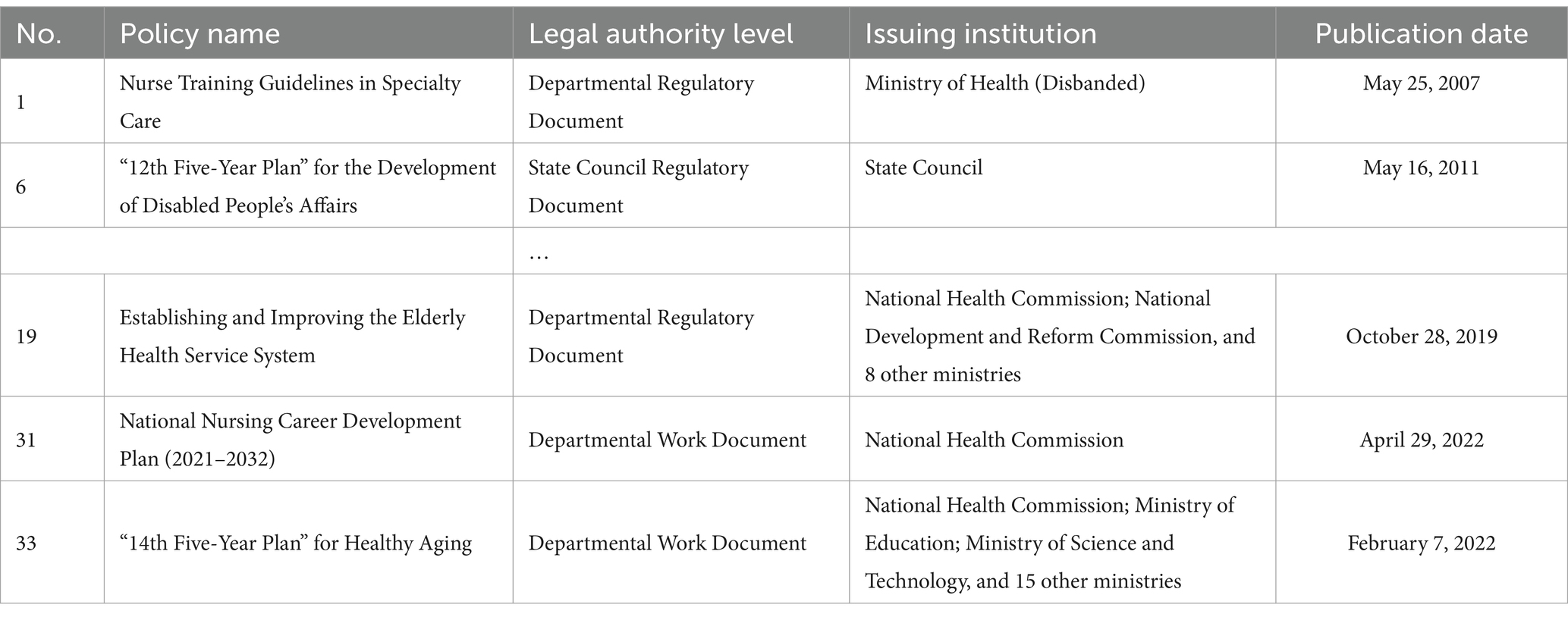
Table 1. Policy documents related to rehabilitation nursing (part).
2.3 Policy analysis framework construction
Different policy sub-goals necessitate distinct types of policy instruments, each yielding varying effects on these sub-goals. This study adopts the model proposed by public policy scholars Rothwell and Zegveld, which categorizes policy instruments into three primary types: supply-type, demand-type, and environment-type, with each type further subdivided into specific subtypes (11). To address the necessity for tailored services that cater to diverse groups, conditions, and rehabilitation needs within a multi-level service demand context, this study employs literature analysis (12–14) to classify the rehabilitation care system into five dimensions: caregivers, service goals, service programs, service methods, and safeguards. These dimensions constitute the analytical framework for the Y-axis and provide insights into the developmental trajectory of rehabilitation care policies while addressing critical challenges in this field.
Building upon this foundation, a two-dimensional policy analysis framework has been developed. This framework comprises an X-axis (policy instrument dimension) and a Y-axis (service demand dimension), as illustrated in Figure 1. It offers a systematic approach to understanding and evaluating the role of policy instruments in achieving specific sub-goals; thus serving as a valuable tool for guiding both policy formulation and implementation.
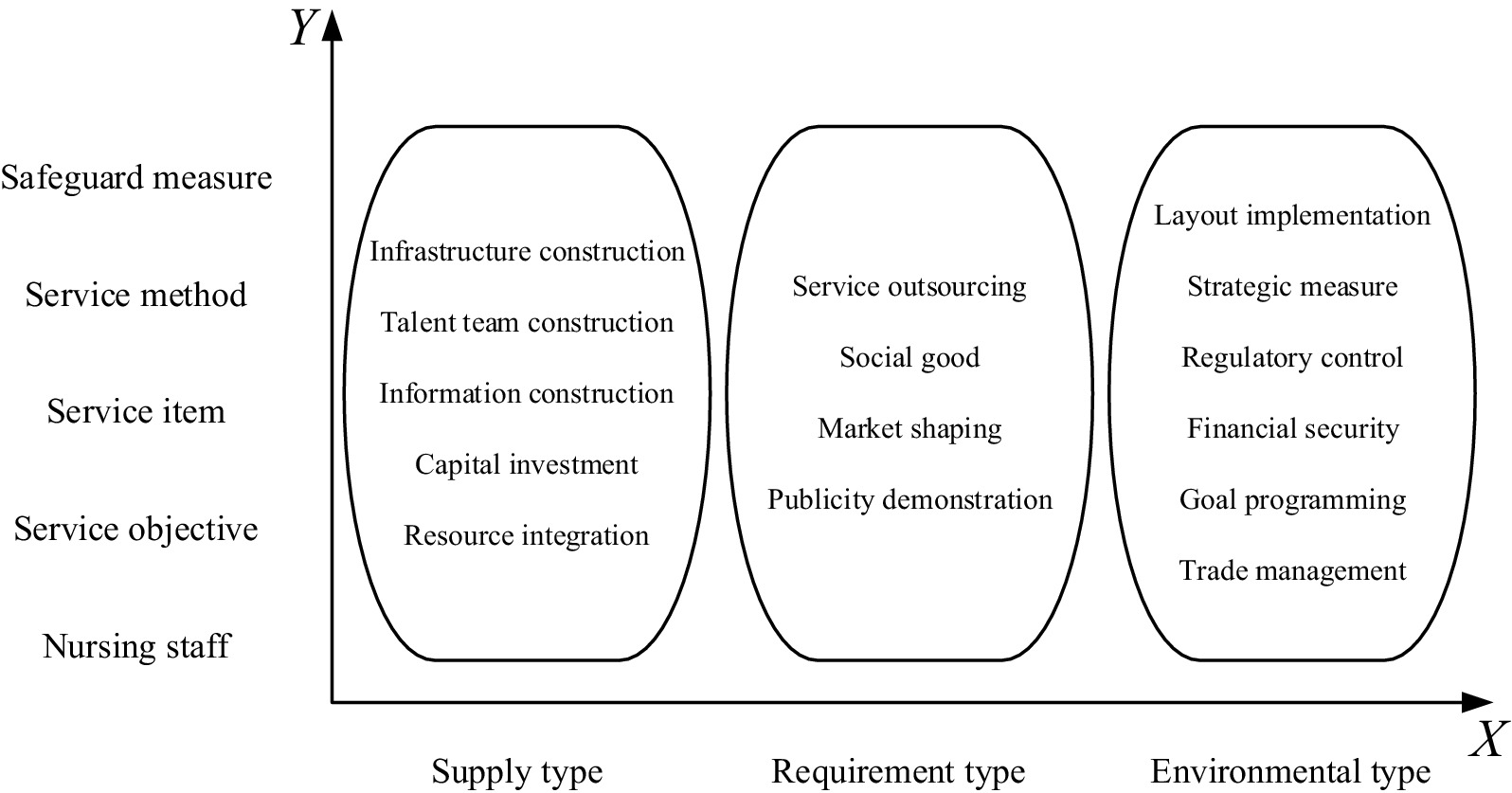
Figure 1. Two-dimensional analytical framework for rehabilitation care policy.
2.4 Literature screening and information extraction
In this study, the policy text analysis method was employed, utilizing NVIVO 12.0 for information extraction and quantitative analysis of the selected policy texts. The two researchers independently extracted information from the screened policy documents, focusing on articles related to rehabilitation nursing policies as their content analysis unit. Policies were systematically numbered in a “Policy number - Chapter - Clause serial number” format, and the researchers categorized them according to dimensions of the policy tool and service system, resulting in a total of 292 codes. Prior to commencing the study, researchers underwent training to ensure consistency and stability in the results obtained. In instances where discrepancies arose during the coding process between the two researchers, a third researcher was consulted following discussion to achieve consensus. The coding process included cross-checking for consistency and reliability to guarantee both accuracy and validity in the analysis. Examples of text content coding pertaining to rehabilitation nursing policies are presented in Table 2.

Table 2. Examples of text coding of rehabilitation nursing policies.
3 Policy coding analysis results
3.1 General information on policies
This study analyzed policy documents related to rehabilitation care published between 2007 and 2024. (1) In terms of the volume of issued documents, the highest number was recorded in 2022, with a total of six publications. This increase may be attributed to the ‘14th Five-Year Plan for National Health’ released by the General Office of the State Council in 2022, as well as the ‘14th Five-Year Plan for the Development of Health Care Personnel’ issued by the National Health Commission. The publication of these plans outlines a strategic direction for the development of the rehabilitation nursing sector, aiming to enhance the quality of rehabilitation nursing services and provide guidance and support to better address societal needs for rehabilitation nursing. (2) From an overall perspective, the number of policies related to rehabilitation care has shown a consistent upward trend. This indicates that the government is increasingly concerned about the development of the rehabilitation care industry and is actively formulating and implementing relevant policies to provide robust support for its growth. The sustained attention and backing from these policies have attracted more talent and funding into the field of rehabilitation nursing, thereby facilitating further development and expansion within the industry. (3) In terms of issuing bodies, most policies are primarily released by authoritative organizations such as the General Office of the State Council and the National Health Commission. Additionally, there are instances of joint issuance among multiple departments; for example, 15 ministries and commissions—including the National Health Commission, Ministry of Education, and Ministry of Science and Technology—collaboratively issued the “14th Five-Year Plan for Healthy Aging Notice.” Such interdepartmental collaboration fosters resource integration and synergy across various sectors, promoting the establishment of a mature and systematic policy framework that contributes to both national development and enhancement in the rehabilitation nursing care industry.
3.2 X-dimension analysis results
Statistical analysis revealed significant differences in the utilization of relevant policy tools within the realm of rehabilitation care. Specifically, supply-type, demand-type, and environment-type policy tools accounted for 36.64% (107/292), 16.10% (49/292), and 46.58% (136/292) respectively. Among these, environment-based tools were employed most frequently; within this category, target planning constituted the largest proportion at 13.36%, while financial security represented the smallest share at 4.11%. Supply-based tools ranked second in usage frequency, with human resource development being the most utilized tool at 15.41%, whereas financial investment accounted for only 1.03%. Demand-based tools were used least often; market shaping was the predominant tool in this category at 7.88%, while social welfare comprised merely 1.71%. These findings are summarized in Table 3.
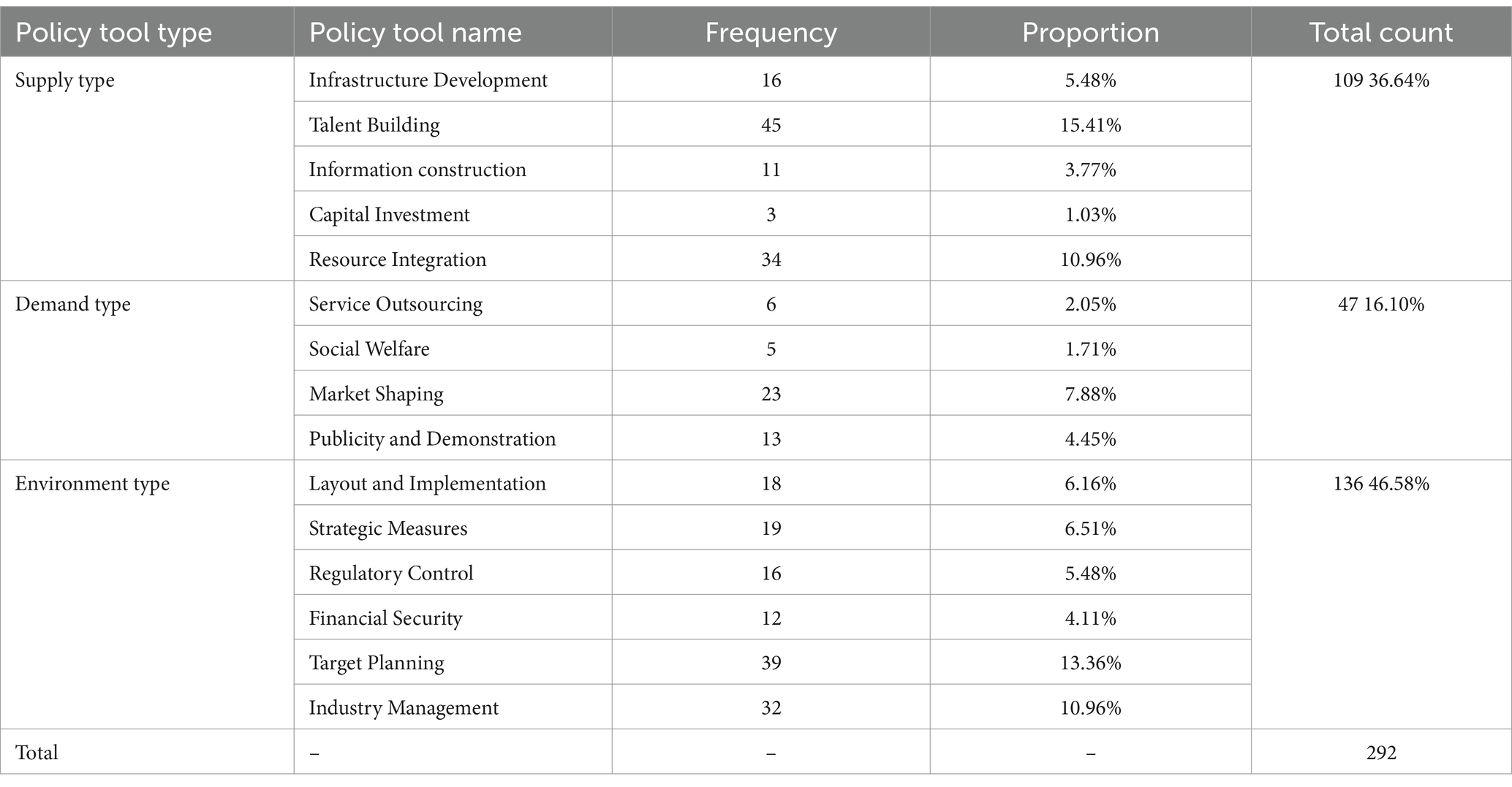
Table 3. Distribution of policy instruments (n = 292).
3.3 Results of Y-dimension analysis
According to the statistics regarding the number of policy tools within the service system dimension, as presented in Table 4, it is observed that 22.95% of these policy tools pertain to nursing staff, 12.67% relate to service objectives, 20.89% are associated with service items, 25.00% concern service methods, and 18.49% involve safeguards. The distribution of each element appears generally balanced; however, there is a relatively small proportion of policy tools related to the objective elements of rehabilitation care services, indicating a need for further clarification and specification in this area.
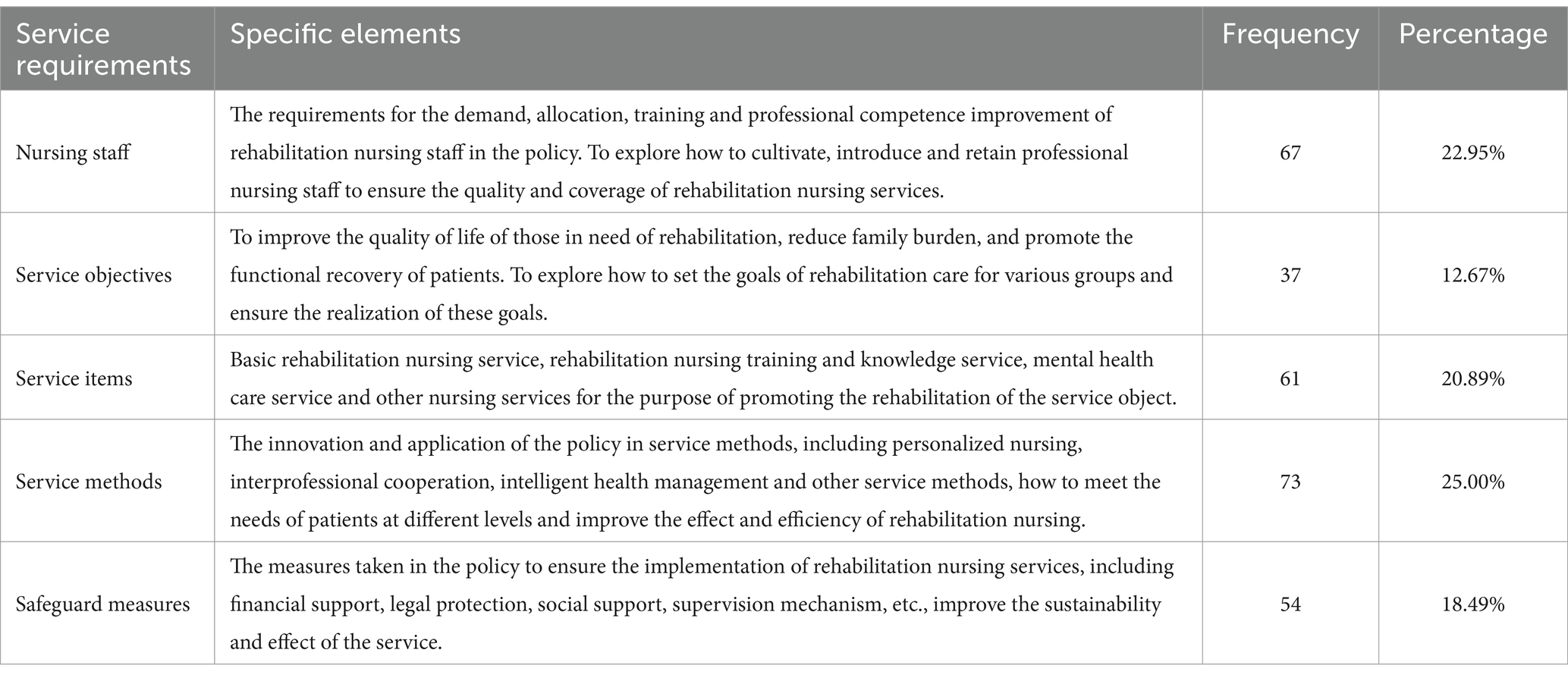
Table 4. Distribution of items in dimension of service needs (n = 292).
3.4 Results of X-Y dimension analysis
A comprehensive analysis of the X-dimension of basic policy tools and the Y-dimension of service systems reveals, as illustrated in Table 5, that supply-type policy tools place greater emphasis on the element of caregivers, with a frequency count of 47. In contrast, environment-type policy tools focus more on the elements related to service items and service methods, recording frequencies of 34. Demand-type policy tools prioritize service methods and safeguards, with frequencies of 16 and 13, respectively.
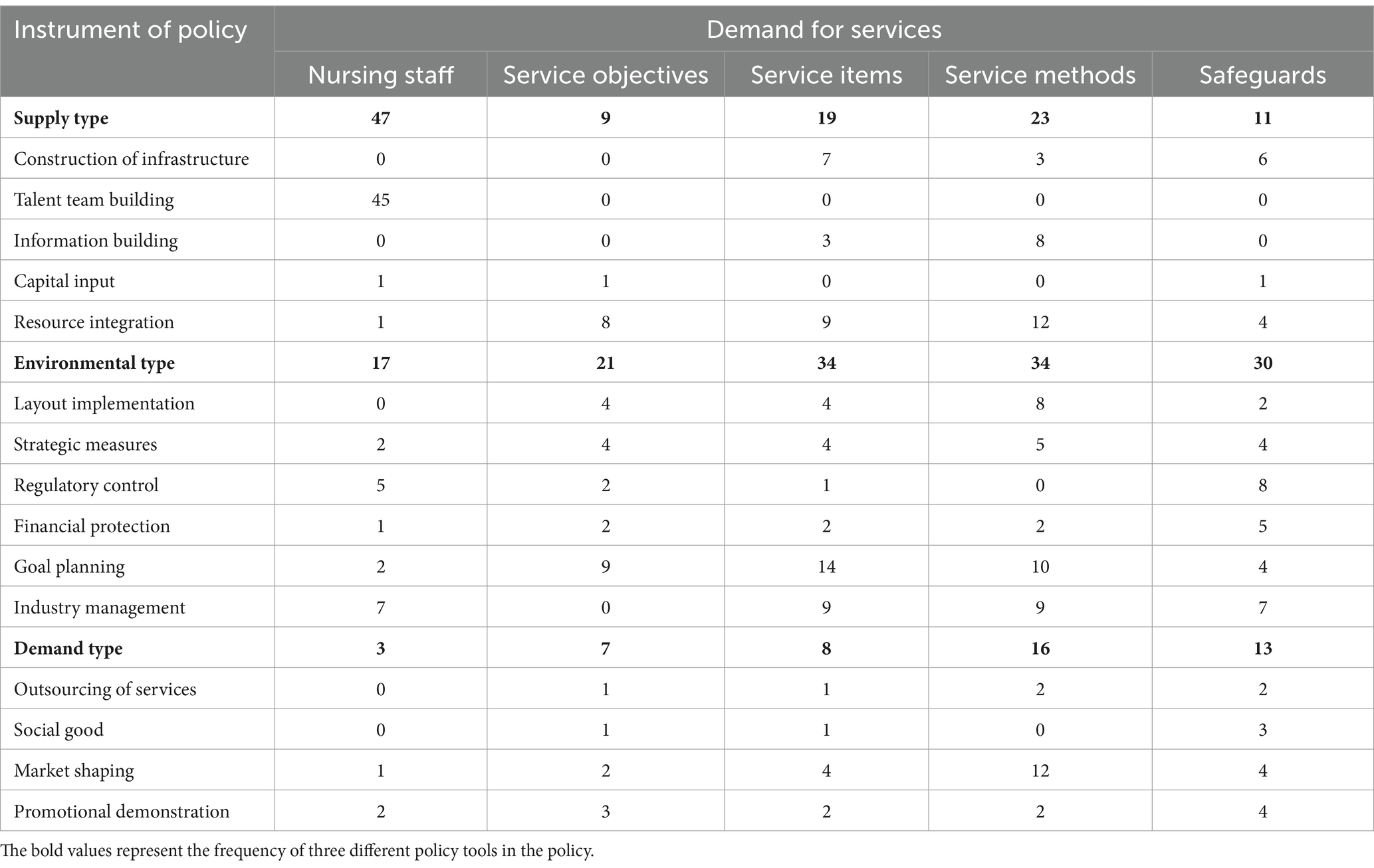
Table 5. L-shaped matrix of policy tools and service system elements (n = 292).
The varying emphasis on different elements within service systems across distinct types of policy tools suggests that when formulating policies, the government carefully considers the unique characteristics associated with each type to select the most suitable tool for specific policy objectives. This differentiation in focus among various types of policy instruments underscores how governmental decision-making is informed by an understanding of these characteristics, ultimately guiding them toward choosing the most appropriate instrument for achieving targeted outcomes.
4 Study conclusions and recommendations
4.1 Differences in the use of various types of policy instruments and structural optimization
This study revealed significant disparities in the utilization of three policy tools—environmental, supply, and demand—in rehabilitation nursing policies. Notably, environmental policy instruments accounted for the largest share (46.58%), indicating that the government places considerable emphasis on fostering a conducive development environment for the rehabilitation nursing industry. A favorable industry environment not only enhances the motivation of nursing staff but also ensures high-quality rehabilitation nursing services (15, 16). Conversely, while there was a relatively high frequency of use for supply-oriented policy tools (36.64%), applications related to infrastructure, information dissemination, and financial investment remained inadequate—particularly within community nursing services. The lack of personalized service offerings represents an urgent issue that requires resolution (17). Demand-oriented policy tools were utilized the least frequently (16.10%), which may be attributed to the developmental stage of China’s rehabilitation care industry. In comparison to the United States, rehabilitation nursing in China commenced later and has progressed slowly; moreover, the concept of rehabilitation nursing remains largely unrecognized among the general population. This is particularly evident in the insufficient attention given to the complex needs of middle-aged and older adult individuals, as well as patients with chronic diseases (18, 19). Despite having a considerable number of rehabilitation institutions, China faces several challenges including low service rates, disorganized operational models, inadequate facilities, and insufficient personnel training (20, 21). The existing social conditions interact negatively with the infrequent application of demand-oriented policy tools, resulting in an imperfect allocation of rehabilitation resources. Consequently, some patients are discharged directly after their acute phase without receiving systematic rehabilitation treatment at home, which significantly increases their risk for postoperative complications (22).
Therefore, it is crucial to draw upon existing achievements and experiences to optimize medical resource allocation and alleviate pressure on large hospitals. Implementing a three-tiered medical referral mechanism could effectively direct patients with varying conditions to appropriate specialized institutions for tailored treatment and care (23, 24). Furthermore, there is a pressing need to enhance standardized management practices, guide quality service outsourcing initiatives, promote high-quality policy tools, and rectify prevailing industry disarray. In light of the multi-level demand context, the government should optimize the structural utilization of various policy tools and reasonably allocate the proportions of environmental, supply-based, and demand-based instruments. In applying environmental policy tools, it is essential for the government to focus on establishing a conducive policy environment and a robust industry development framework. This includes providing enhanced support in terms of capital investment, legal regulations, and industry management (25). In relation to supply-based policy tools, there should be an emphasis on cultivating rehabilitation nursing professionals and developing infrastructure to adequately meet the diverse needs of patients at different levels (26). Regarding demand-based policy tools, the government ought to strengthen guidance for social capital involvement as well as support for social welfare initiatives. Furthermore, it is crucial to encourage multiple societal forces to engage actively in the construction of rehabilitation nursing services (27).
4.2 Distribution and optimization suggestions of service demand elements
This study introduced a Y dimension based on the X dimension to construct a two-dimensional framework for analyzing rehabilitation nursing policy texts. In the service needs dimension, the research findings indicated that elements related to service methods accounted for the highest proportion, reaching 25.00%. This result underscores the government’s significant emphasis on developing and implementing effective rehabilitation nursing service methods, highlighting the importance of providing support through these methods to achieve improved rehabilitation outcomes and service quality. Additionally, nursing staff and service items represented 22.95 and 20.89%, respectively, which aligns with existing research findings. The study demonstrated that training nursing staff in professional skills and competencies is a crucial prerequisite for enhancing the quality of care provided in rehabilitation settings (28). Conversely, elements pertaining to service targets constituted the lowest proportion at only 12.67%. Clearly defined service objectives are essential for delineating the scope of implementation in rehabilitation nursing and addressing the needs of those receiving services. Therefore, it is particularly necessary (29) to balance various factors according to actual circumstances, continuously enhance facilities within rehabilitation nursing institutions at all levels, and improve both education and professional standards among practitioners in order to establish a high-quality rehabilitation nursing team. Excellent talents are fundamental to the continuous progress of the industry. It is essential to reform the talent training system, focusing on international development trends while considering the actual circumstances. This involves actively exploring the construction of a new curriculum system and professional standards that align with the talent training objectives of medical colleges and universities (30). Furthermore, it is crucial to establish and enhance professional training programs that better meet the industry’s actual needs and closely correspond with the requirements of international rehabilitation industry support courses.
It is widely recognized that different groups have varying needs for rehabilitation care. To address these diverse requirements across different demographics and levels, it is recommended that policymakers strengthen service objective settings to ensure comprehensive coverage of needs at all levels (31). In light of multi-level needs, service goals should be articulated more clearly, with a focus on refining the rehabilitation nursing requirements for patients at different levels—ranging from basic health maintenance to personalized in-depth care (32). Policymakers should facilitate the coordination and integration of nursing staff training, service project design, and service objectives to ensure that policies effectively meet varying demands while simultaneously improving the overall efficacy and quality (33) of rehabilitation nursing.
4.3 Professional and systematic policy construction driven by multi-level service demand
Rehabilitation nursing, as a vital domain related to public health, is encountering an increasing array of multi-level needs. Currently, China has yet to establish a mature rehabilitation nursing industry system. The Outline of the Plan for the National Medical and Health Service System (2015–2020), issued by the General Office of the State Council in 2015, proposed promoting “the formation of a continuous service model encompassing diagnosis, treatment, rehabilitation, and long-term care.” This initiative aims to achieve a rational medical treatment framework characterized by “minor diseases managed at primary care facilities, serious illnesses treated in hospitals, and rehabilitation facilitated through primary care.” The document underscores the transitional role of rehabilitation nursing between hospital settings and home environments; particularly during patients’ recovery processes where home care can offer more personalized support (34). However, existing policies still exhibit a lack of clarity regarding both the temporal scope and service content associated with rehabilitation nursing. In light of diverse service demands across multiple levels, there is an urgent need for a more comprehensive collaboration mechanism.
The multi-level service demand indicates that rehabilitation nursing must not only address the fundamental rehabilitation needs of the older adult and disabled individuals but also extend to encompass chronic diseases, cancer, and other populations (35). This highlights the differentiated requirements for rehabilitation nursing across various groups (36). Therefore, it is recommended that the government enhance coordination among hospitals, communities, and families to promote a comprehensive and continuous service model (37, 38). This approach should particularly focus on achieving rational resource allocation and precise matching of needs at different stages of rehabilitation. Furthermore, the government should encourage the establishment of inter-agency collaboration mechanisms to facilitate effective information sharing and communication. Such measures will optimize service quality and improve resource utilization efficiency, thereby better addressing multi-level rehabilitation needs while promoting patients’ recovery and social integration (39).
Current policies primarily focus on the older adult and disabled populations, while insufficient attention is given to other groups with rehabilitation care needs, including individuals with chronic illnesses. Therefore, it is imperative for the government to clearly define the target population for rehabilitation nursing services, establish a robust service evaluation mechanism, and ensure accurate identification and assessment of service recipients. As high-quality nursing staff are essential in delivering effective rehabilitation nursing services, it is crucial to enhance the treatment of practitioners in order to attract more talented professionals into the field. It is recommended that welfare and security measures for these practitioners be improved. Concurrently, the government should bolster economic incentives within the industry through innovative mechanisms, resource integration, and diversified investment strategies (40). Such efforts will stimulate the engagement of stakeholders in social capital and effectively address multi-layered needs while ensuring that basic service requirements are met, thereby contributing to sustainable development within the sector. Adequate policy support plays a crucial role in the industry’s advancement. In 2021, China designated 15 provinces as pilot areas for rehabilitation medical services, with the government taking a proactive stance to promote the growth of the rehabilitation nursing industry (41). The study indicates that among the five provinces participating in this pilot initiative—Shandong, Jiangsu, Hunan, Guangdong, and Zhejiang—the distribution of rehabilitation institutions ranks among the highest in the country (42). However, it is insufficient to focus solely on developing rehabilitation nursing services in populous cities with high economic development; greater attention must be directed toward remote areas that lack adequate rehabilitation resources moving forward. Governments can implement capacity-building projects for less developed regions by adopting differentiated financial support policies. Furthermore, multi-sectoral coordination platforms can be established through integrated arrangements to ensure effective policy implementation across administrative boundaries.
5 Conclusion
Through a quantitative analysis of Chinese rehabilitation nursing policy texts, this study elucidates the distribution characteristics and potential issues associated with policy objectives and tools. The findings indicate that while China’s rehabilitation nursing policy system has seen gradual improvements in recent years, there remains significant room for enhancement regarding the clarity of objectives and the balance among policy instruments. In comparison to international rehabilitation nursing policies, China’s framework still requires strengthening in terms of service system improvement and diversification of tool utilization. This research not only addresses a gap in the quantitative analysis of domestic rehabilitation nursing policies but also offers a novel perspective for international policy studies. Moving forward, it is essential to further optimize policy design, enhance resource integration and service equity, thereby promoting the sustainable and healthy development of the rehabilitation nursing sector.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.gov.cn/.
Author contributions
WL: Data curation, Methodology, Software, Writing – original draft, Writing – review & editing. YZ: Conceptualization, Writing – review & editing. XZ: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Su, Y, Wang, S, Sun, J, Zhang, Y, Ma, S, Li, M, et al. Triglyceride glucose index associated with arterial stiffness in chinese community-dwelling elderly. Front Cardiovasc Med. (2021) 8:737899. doi: 10.3389/fcvm.2021.737899
2. Shie, A-J, Wu, W-F, Yang, M, Wan, X, and Li, H. Design and process optimization of combined medical and elderly care services: an integrated service blueprint-TRIZ model. Front Public Health. (2022) 10:965443. doi: 10.3389/fpubh.2022.965443
3. 2023 National Development Communique on Aging. The elderly population aged 60 and above in China was 296.97 million. 21.1% of the population - the Ministry of Civil Affairs of the People's Republic of China. Available online at:https://www.mca.gov.cn/n152/n166/c1662004999980001780/content.html. Accessed 13 Jan 2025.
4. Mi, T, Xue, J, Xue, P, and LV, H. Development status of rehabilitation nursing in secondary and above hospitals in Shanxi Province. Nurs Res. (2024) 38:735–739. doi: 10.12102/j.issn.1009-6493.2024.04.033
5. Yang, C-L, Labbe, D, Sakakibara, BM, Vissers, J, and Bird, M-L. World cafe - a community conversation: a Canadian perspective on stroke survivors needs for community integration. Top Stroke Rehabil. (2022) 29:392–400. doi: 10.1080/10749357.2021.1928839
6. Raj, VS, Pugh, TM, Yaguda, SI, Mitchell, CH, Mullan, SS, and Garces, NS. The who, what, why, when, where, and how of team-based interdisciplinary cancer rehabilitation. Semin Oncol Nurs. (2020) 36:150974. doi: 10.1016/j.soncn.2019.150974
7. Kumbhar, S, and Bhatia, M. Advancements and best practices in diabetic foot care: a comprehensive review of global progress. Diabetes Res Clin Pract. (2024) 217:111845. doi: 10.1016/j.diabres.2024.111845
8. Vasquez, B, Moreno-Lacalle, R, Soriano, GP, Juntasoopeepun, P, Locsin, RC, and Evangelista, LS. Technological machines and artificial intelligence in nursing practice. Nurs Health Sci. (2023) 25:474–81. doi: 10.1111/nhs.13029
9. Chang, B, Yang, Y, Buitrago Leon, GA, and Lu, Y. Effect of collaborative governance on medical and nursing service combination: an evaluation based on delphi and entropy method. Healthc (Basel Switz). (2021) 9. doi: 10.3390/healthcare9111456
10. Kandelman, D, Arpin, S, Baez, RJ, Baehni, PC, and Petersen, PE. Oral health care systems in developing and developed countries. Periodontol. (2000) 60:98–109. doi: 10.1111/j.1600-0757.2011.00427.x
11. Hanson, EC. Industrial innovation and public policy: preparing for the 1980s and the 1990s. By Roy rothwell and walter zegveld. (Westport, conn.: greenwood press, 1981. Pp. 251. $35.00.). Am Polit Sci Rev. (1982):699–700. doi: 10.2307/1963794
12. Gu, S, Wu, H, and Cao, D. Strategic thinking and suggestions on building a scientific and reasonable elderly care service system Popul Res (2017) 41:3–14.
13. Zhang, Y, Yan, F, Wang, H-L, Huang, Y-Q, Guo, Z-J, Li, X-R, et al. Application of "internet +" continuous nursing service model in patients with severe mental disorders in stable stage. China Nursing Educ. (2024). 21:96–103. doi: 10.3761/j.issn.1672-9234.2024.01.016
14. Ju Mei, D, Fengling, WK, Liu Xiaochu, S, and Meihong, LQ. Construction of evaluation index system of service quality in nursing institutions with combination of medical and nursing care. Milit Nursing. (2022) 39:5–9. doi: 10.3969/j.issn.2097-1826.2022.12.002
15. Tong, Y, Luo, Y, and Zhong, H. The practice and enlightenment of long-term care quality assurance in the United States. Chin J Nurs. (2024) 59:31–6. doi: 10.3761/j.issn.0254-1769.2024.12.019
16. Liu, J, Guo, J, and Qin, G. Research on the importance of rehabilitation nursing from the perspective of economic development. Econ Outlook Around Bohai Sea. (2019):122. doi: 10.16457/j.cnki.hbhjjlw.2019.04.086
17. Perjoc, R-S, Roza, E, Vladacenco, OA, Teleanu, DM, Neacsu, R, and Teleanu, RI. Functional neurological disorder-old problem new perspective. Int J Environ Res Public Health. (2023):When 99. 20. doi: 10.3390/ijerph20021099
18. Liu, Q, Me, W, and Geng, L. Research progress on rehabilitation nursing model of the aged under the background of the combination of medical care and old-age care in China. J Nurs. (2022) 37:20–3. doi: 10.3870/j.issn.1001-4152.2022.05.020
19. He, X, Zhu, L, Li, J, and Liu, Y. Research progress of digital twins in precision care of chronic diseases. J Nurs. (2024) 39:120–3. doi: 10.3870/j.issn.1001-4152.2024.24.120
20. Zhang, J, Gao, J, and Qiao, X. The medium term care service of the combination of medical and nursing care: concept, existing problems and professional development path. Popul Econ. (2024) 30-42. doi: 10.3969/j.issn.1000-4149.2024.00.018
21. Lu, S, Hu, Y, Sha, L, Zhang, Z, and Feng, X. Policy analysis of rehabilitation medical service in China from the perspective of policy tools. Chinese Hosp. (2024) 28:50–5. doi: 10.19660/j.issn.1671-0592.2024.9.12
22. Pan, H. Private rehabilitation institution operating mode research. Shanghai: Shanghai university of engineering science (2021). 100 p.
23. Walton, RF, Yeh, C, Shannon, R, Rosoklija, I, Rague, JT, Johnson, EK, et al. Variation in care between pediatric and adult patients presenting with nephrolithiasis to tertiary care pediatric emergency departments in the United States (2009-2020). J Pediatr Urol. (2022) 18:742.e1–742.e11. doi: 10.1016/j.jpurol2022.07.005
24. Hu Linlin, Z, Mengjia, HC, Yanyan, C, and Yuanli, L. American experience and enlightenment of Medicare payment methods for post-acute medical services. China Med Insur. (2021) 10:75–80. doi: 10.19546/j.issn.1674-3830.2021.10.011
25. Chen, S. Comparative study on combined medical and nursing services in Chinese and American elderly care institutions China Academy of Chinese Medical Sciences (2019). 266 p. Available at: https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CDFD&dbname=CDFDLAST2019&filename=1019240670.nh (Accessed January 13, 2025).
26. Zhang, Y, Luo, B, Li, J, and Li, Z. Training strategy of elderly nursing team under the background of combination of medical and nursing care. Chinese Med Ethics. (2024). doi: 10.12026/j.issn.1001-8565.2025.03.05
27. Li, M, and Dong, B. The development path of community health care service from the perspective of supply and demand matching. J Yunnan Minzu Univ. (2024) 41:88–94. doi: 10.13727/j.cnki.53-1191/c.20240702.002
28. Shang, X, Lin, Z, Xie, X, Fang, S, Chen, L, GU, Z, et al. Construction of standardized training system for new nurses based on post competency. Nurs Res. (2019) 33:1334–1337, 1341.
29. Zou, C, and Chen, Y. Effect of practical training of nursing skills and nursing teaching standards on improving nursing quality of patients in hospital units. Know Lib. (2024) 40:111–114.
30. Qiu, X, Zhao, J, and Zhao, C. Research on talent training model of industrial college based on integration of industry and education -- a case study of intelligent rehabilitation industry College of Guangdong Pharmaceutical University. Theoretical Research and Practice of Innovation and Entrepreneurship. Available at: https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CJFQ&dbname=CJFDLAST2024&filename=CXYL202404030
31. Rasheed, SP, Younas, A, and Mehdi, F. Challenges, extent of involvement, and the impact of nurses’ involvement in politics and policy making in in last two decades: an integrative review. J Nurs Scholarsh: Off Publ Sigma Theta Tau Int Honor Soc Nurs. (2020) 52:446–55. doi: 10.1111/jnu.12567
32. Han, Y, Mo, L, and Liu, A. Investigation on the expected home rehabilitation needs of stroke patients in Beijing Rehabilitation Hospital and its influencing factors. China Journal of Rehabilitation Medicine. (2024) 39:858–862. doi: 10.3969/j.issn.1001-1242.2024.06.015
33. Huang, J, ZHAO, L, LI, Y, and Zhou, M. The exploration of building a high-quality and efficient integrated medical service system with the construction of digital health as the center. China Contemp Med. (2022) 29:127–130.
34. Geng, Z, and Zhang, L. Our country actively responds to the aging population strategy background to promote the individual exercise of knowledge management strategy. Sci Res Aging (2022).
35. Garcon, L, Khasnabis, C, Walker, L, Nakatani, Y, Lapitan, J, Borg, J, et al. Medical and assistive health technology: meeting the needs of aging populations. Gerontologist. (2016) 56:S293–302. doi: 10.1093/geront/gnw005
36. Liu, L, and Zhang, K. Realistic demand, practical exploration and countermeasures of constructing county medical community under the background of healthy China. Rural Econ. (2024):90–102.
37. Liu, Q, Xue, L, ZHANG, L, GUO, Y, Lin, B, MEI, Y, et al. Study on posttraumatic growth in young and middle-aged stroke patients. Med Philos. (2020) 41:54–9. doi: 10.12014/j.issn.1002-0772.2020.24.13
38. Zhao, R, and Tong, X. The policy history and construction status of the development of medical service organization in our country. Chinese Health Econ. (2024) 43:37.
39. Xue, C, Teng, H, Zhang, R, Liu, H, and Tian, J. Research on the sinking policy of high quality nursing resources in China. Journal of. Nursing. (2023) 30:20–23. doi: 10.16460/j.issn1008-9969.2023.17.020
40. Wang, J, ZHANG, F, Wu, H, DING, Z, Li, X, Zhou, Y, et al. The policy analysis of "internet + nursing service" at the provincial level in China. China. Nurs Manag. (2023) 23:25–31. doi: 10.3969/j.issn.1672-1756.2023.01.006
41. The national health committee general office work pilot implementation of rehabilitation medical service notice. Available online at:http://www.nhc.gov.cn/yzygj/s7653pd/202110/9af02fe668e74aa3a0271e425ef0ea58.shtml [Accessed March 5, 2025]
Keywords: policy tools, rehabilitation care, nursing policy, text analysis, public health
Citation: Li W, Zhu Y and Zhu X (2025) Text analysis of rehabilitation nursing policy in China from the perspective of policy tools. Front. Public Health. 13:1562889. doi: 10.3389/fpubh.2025.1562889
Edited by:
Ana Oliveira-Kumakura, Université Paris Cité, FranceReviewed by:
Chen Li, Shanghai University of Engineering Sciences, ChinaSushma Jaiswal, Guru Ghasidas Vishwavidyalaya, India
Copyright © 2025 Li, Zhu and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuehua Zhu, c25vd196eGhAMTYzLmNvbQ==