 Ashish Joshi1*
Ashish Joshi1* Laura Magana2
Laura Magana2 Kun-Hsien Tsai3
Kun-Hsien Tsai3 Diana Maddah4
Diana Maddah4 Kerry Mitchell5Diana Ruggiero6
Kerry Mitchell5Diana Ruggiero6 W. Bradley Hawkins7Shafik Dharamsi8Jihad Makhoul9Rodrigo Reis10
W. Bradley Hawkins7Shafik Dharamsi8Jihad Makhoul9Rodrigo Reis10 So Yoon Kim11
So Yoon Kim11 Wah Yun Low12
Wah Yun Low12 Woldekidan Amde13
Woldekidan Amde13 Glory Nja14
Glory Nja14 Michelle Jeu1
Michelle Jeu1 Bridget Kelly15
Bridget Kelly15 Bernard Saliba16
Bernard Saliba16 Niharika Jha1
Niharika Jha1 Ramune Kalediene17Giada Scarpetti18Erica Kastrup19Rajendra Surenthirakumaran20Catherine Kane21William Yotive22
Ramune Kalediene17Giada Scarpetti18Erica Kastrup19Rajendra Surenthirakumaran20Catherine Kane21William Yotive22 Matthew Brown23
Matthew Brown23 Xinhua Yu1Gretchen Peterson24Beverly Tsacoyianis25
Xinhua Yu1Gretchen Peterson24Beverly Tsacoyianis25 Michael Arthur Ofori1
Michael Arthur Ofori1 Marian Levy1Stella Chirwa1Maryam Karimi1
Marian Levy1Stella Chirwa1Maryam Karimi1 Kami Geron1Saloni Patel1Dorothy Biberman2Michelle Taylor26Aeryn Longuevan1Steve Shular1
Kami Geron1Saloni Patel1Dorothy Biberman2Michelle Taylor26Aeryn Longuevan1Steve Shular1 Tim K. Mackey27
Tim K. Mackey27- 1School of Public Health, University of Memphis, Memphis, TN, United States
- 2Association of Schools and Programs of Public Health (ASPPH), Washington, DC, United States
- 3Department of Public Health, National Taiwan University, Taipei, Taiwan
- 4Public Health Department, Qatar University, Doha, Qatar
- 5Department of Public Health and Preventive Medicine, St. George’s University, St. George, Grenada
- 6Department of World Languages and Literatures, University of Memphis, Memphis, TN, United States
- 7Institute for Medicine and Public Health, Vanderbilt University, Nashville, TN, United States
- 8School of Public Health, University of North Texas Health Science Center, Fort Worth, TX, United States
- 9Department of Health Promotion and Community Health, American University of Beirut, Beirut, Lebanon
- 10People Health and Place Unit, Prevention Research Center, Washington University in St. Louis, St. Louis, MO, United States
- 11Department of Medical Law and Ethics, Yonsei University, Seoul, Republic of Korea
- 12Asia-Europe Institute, University Malaya, Kuala Lumpur, Malaysia
- 13School of Public Health, University of the Western Cape, Bellville, South Africa
- 14Department of Public Health, University of Calabar, Calabar, Nigeria
- 15Early Start, School of Social Sciences, University of Wollongong, Wollongong, NSW, Australia
- 16University of Technology Sydney, Sydney, NSW, Australia
- 17Department of Health Management, Lithuanian University of Health Sciences, Kaunas, Lithuania
- 18Department of Healthcare Management, Technische Universität Berlin, Berlin, Germany
- 19CRIS Center for International Relations in Health of the Oswaldo Cruz Foundation, Rio de Janeiro, Brazil
- 20Department of Community Medicine, University of Jaffna, Jaffna, Sri Lanka
- 21Independent Researcher, Geneva, Switzerland
- 22World Federation of United Nations Associations, Geneva, Switzerland
- 23Global Health Policy and Data Institute, San Diego, CA, United States
- 24Department of Sociology, University of Memphis, Memphis, TN, United States
- 25Department of History, University of Memphis, Memphis, TN, United States
- 26Shelby County Health Department, Shelbyville, IN, United States
- 27Global Health Program, Department of Anthropology, UC San Diego, San Diego, CA, United States
Public health diplomacy addresses global challenges impacting societies, economies, the environment, and health by integrating foreign policy and development. The University of Memphis School of Public Health hosted a multistakeholder summit to identify strategies and competencies essential for effective public health diplomacy. A 3-day summit included 29 participants from 15 countries, representing the WHO, the World Federation of United Nations, and seven regional public health associations. An iterative human-centered design (HCD) approach and concept mapping were employed to facilitate discussions and generate actionable recommendations. Developed a working definition of Public Health Diplomacy emphasizing cross-disciplinary collaborations, communication, negotiation, and consensus building. Produced a 9-point action plan to establish a global framework, launch capacity-building initiatives, and institutionalize public health diplomacy as a public health discipline.
Introduction
Global health issues, including the COVID-19 pandemic, climate change, misinformation, conflicts, and humanitarian crises, create complex health, economic, and geopolitical challenges (1). These crises disproportionately affect vulnerable populations, particularly women, girls, and children, underscoring the need for inclusive and equity-focused governance. Addressing these challenges effectively requires integrating public health into all policy areas through a “Health in All Policies” approach, which targets wider social determinants of health and promotes health equity across populations (2). Public health diplomacy is essential for fostering collaboration across governments, multilateral organizations, NGOs, academia, and the private sector, advancing global health priorities while contributing to shared development and security goals (3).
The COVID-19 pandemic exposed gaps in global health governance and highlighted the critical need for stronger and more equitable international cooperation (4). It demonstrated the duality of diplomacy during crises: one fostering solidarity and equity, and another seeking geopolitical advantage (5–7). Initiatives such as COVAX for vaccine access and the WHO Investment Round illustrate the potential of multilateral cooperation but also reveal inequities in implementation and access (8). Lessons from the pandemic stress the importance of combining formal diplomacy (e.g., health attachés and diplomats) with informal diplomacy, involving non-state actors like NGOs and private enterprises. Strengthening health diplomacy requires multidisciplinary approaches and cross-sector training to prepare professionals to navigate the sociopolitical and cultural complexities of global health (9–11).
This policy brief paper summarizes the outcomes of a first Public Health Diplomacy Summit organized by the University of Memphis, Public Health Diplomacy Lab, which aimed to define the field, emphasize its importance, and establish an action plan for education, capacity building, and the practice of public health diplomacy.
Public Health Diplomacy Lab
The University of Memphis School of Public Health established the nation’s first Public Health Diplomacy Lab with an aim to bring together different disciplines and stakeholders—governments, NGOs, academics, and civic society to improve collaboration and coordination among all actors to promote health and well-being through the understanding of broad stakeholder engagement, consensus building, and negotiations.
Public Health Diplomacy Summit
Growing numbers of countries have become increasingly more engaged in health policy, health governance, and health diplomacy. This includes recognition that even core health diplomacy actors, such as accredited diplomats, require more direct training, help, and active engagement with health experts. Hence, there is an urgent need to design and establish health diplomacy governance and partnership frameworks that can activate public health and other allies to collectively address global health challenges through traditional vehicles of policy mobilization and generating public support for health objectives. Recognizing this need for a new community of health diplomacy practitioners and advocates, the 2024 Public Health Diplomacy Summit, organized by the Public Health Diplomacy Lab, aimed to bring together stakeholders from diverse geographic, professional, and academic backgrounds to discuss the intersection of health and diplomacy and its role in advancing health equity.
The lab, led by A Joshi, collaborated with the Association of Schools and Programs of Public Health (ASPPH) and reached out to all seven regional public health associations globally including Association of Schools and Programs in Public Health (ASPPH), Asia-Pacific Academic Consortium for Public Health (APACPH), Association of Schools of Public Health in Africa (ASPHA), Council of Academic Public Health Institutions Australia (CAPHIA), Association of Schools of Public Health in the European Region (ASPHER), Latin American Alliance for Global Health/Alianza Latin-American de Salud Global (ALSAG) and South-East Asia Public Health Education Institutions Network for representation in the summit (Figure 1). Diplomacy actors such as the WHO and the World Federation of United Nations Associations were also invited.

Figure 1. Participation of 15 countries (n = 29) representing 7 regional academic public health associations.
The summit featured 29 experts from 15 countries (Figure 1) with additional engagement from local public health agencies like the Shelby County Health Department. Of the 29 representatives, 28 attended in person, while one participated via Zoom due to unavoidable circumstances. The virtual attendee was fully integrated into the discussions through a hybrid meeting setup, ensuring real-time engagement and participation. This setup allowed for seamless interaction, with the participant contributing to discussions and accessing presentation materials alongside in-person attendees.
Methodology of Public Health Diplomacy Summit
The summit employed an iterative human-centered design (HCD) approach (12) to engage attendees and gather insights on defining public health diplomacy and establishing it as a new field of study or core competency in public health. Held from September 25–27, 2024, the three-day event included both in-person and virtual sessions. On the first day, participants introduced themselves and shared their positions, perspectives, and objectives. The agenda and discussion questions were shared in advance. On the second day, participants were divided into five roundtable groups based on their academic, professional, and regional backgrounds. Facilitators led 40–45 min discussions on assigned topics, summarizing key insights for comparative analysis. To facilitate open and candid discussions, the Chatham House Rule was applied, meaning that while participants were free to use the information shared, the identity and affiliation of speakers could not be disclosed. This approach encouraged attendees to speak more freely, share honest perspectives, and engage in constructive debate without concern for political or professional repercussions. The third day focused on synthesizing these discussions, reaching consensus on core objectives, and developing actions to operationalize public health diplomacy, including building a global collaboration network.
Four key questions guided the discussions, (I) exploring the intersection of health and diplomacy, (II) required competencies for public health professionals, (III) resources for students engaging with health diplomacy, and (IV) global collaborations for education development. Using Dedoose software, the team applied thematic analysis to qualitative data, identifying four major discussion topics, 16 themes, and 47 sub-themes. These findings offer a detailed interpretation of public health diplomacy perspectives.
Ethical considerations
Since the paper is based on observations of discussions at the summit and focuses on summarizing expert opinions under the Chatham House Rule, we did not seek approval from the Institutional Review Board. We did not collect any personal information from the participating experts.
Results
Core concepts of the definition of health diplomacy and global health diplomacy were introduced to participants and used to develop a general gap analysis of what could formulate a working definition of “public health diplomacy.” The existing definitions were not inclusive enough of informal health diplomacy actors and not precise enough to the needs of public health professionals. Following are the themes generated from the participant discussions across the four discussion questions.
1. Health functions requiring diplomatic skills
Discussion one (Table 1) highlights how public health diplomacy can leverage multilateral collaboration to tackle global health challenges.
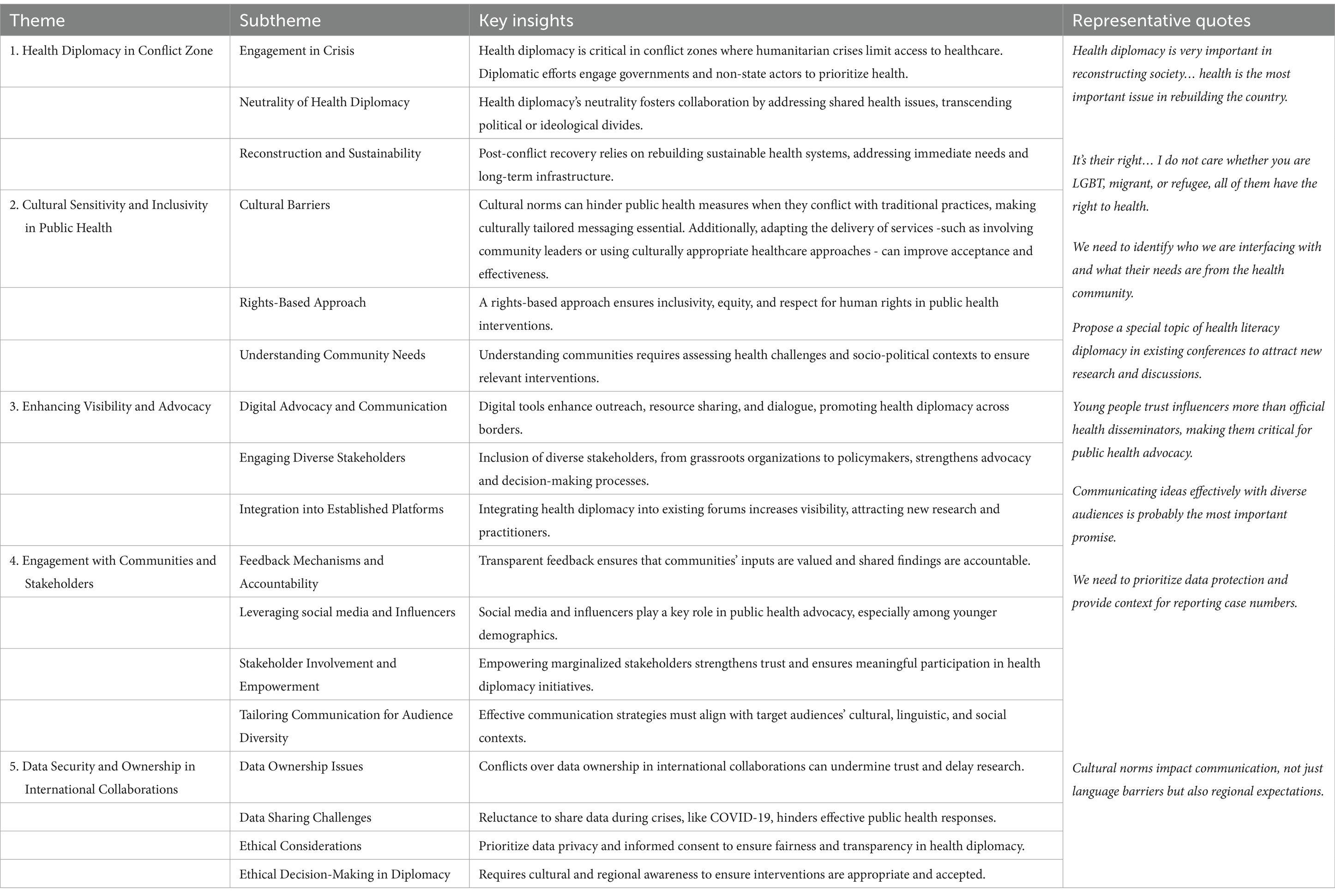
Table 1. Key themes and insights from discussion 1 of the public health diplomacy summit.
2. Required competencies and specific training to help public health professionals serve as public health diplomats
The second discussion (Table 2) prompt yielded three overall themes and several additional topics on the training, skills, and knowledge necessary for public health professionals to excel as public health diplomacy advocates.
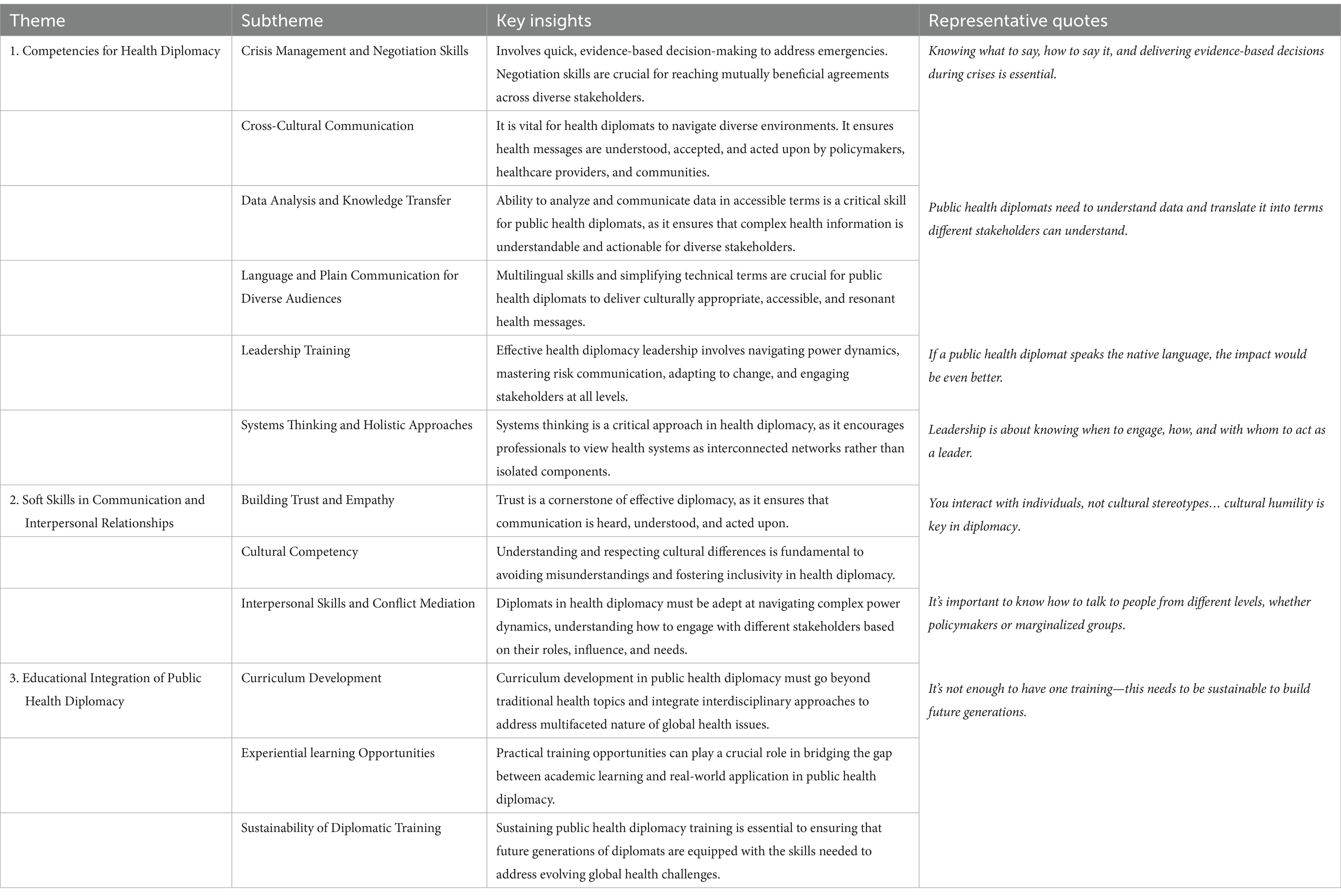
Table 2. Key themes and insights from discussion 2 of the public health diplomacy summit.
3. Existing resources available for public health students toward health diplomacy in a complex, rapidly changing, multilateral system, and the gaps for new resources
The discussion (Table 3) emphasizes building and enhancing resources, including formal training programs, global events, digital resource hubs, and regional training hubs. It also addresses the involvement of academic institutes, governments, and international organizations in strengthening the field.
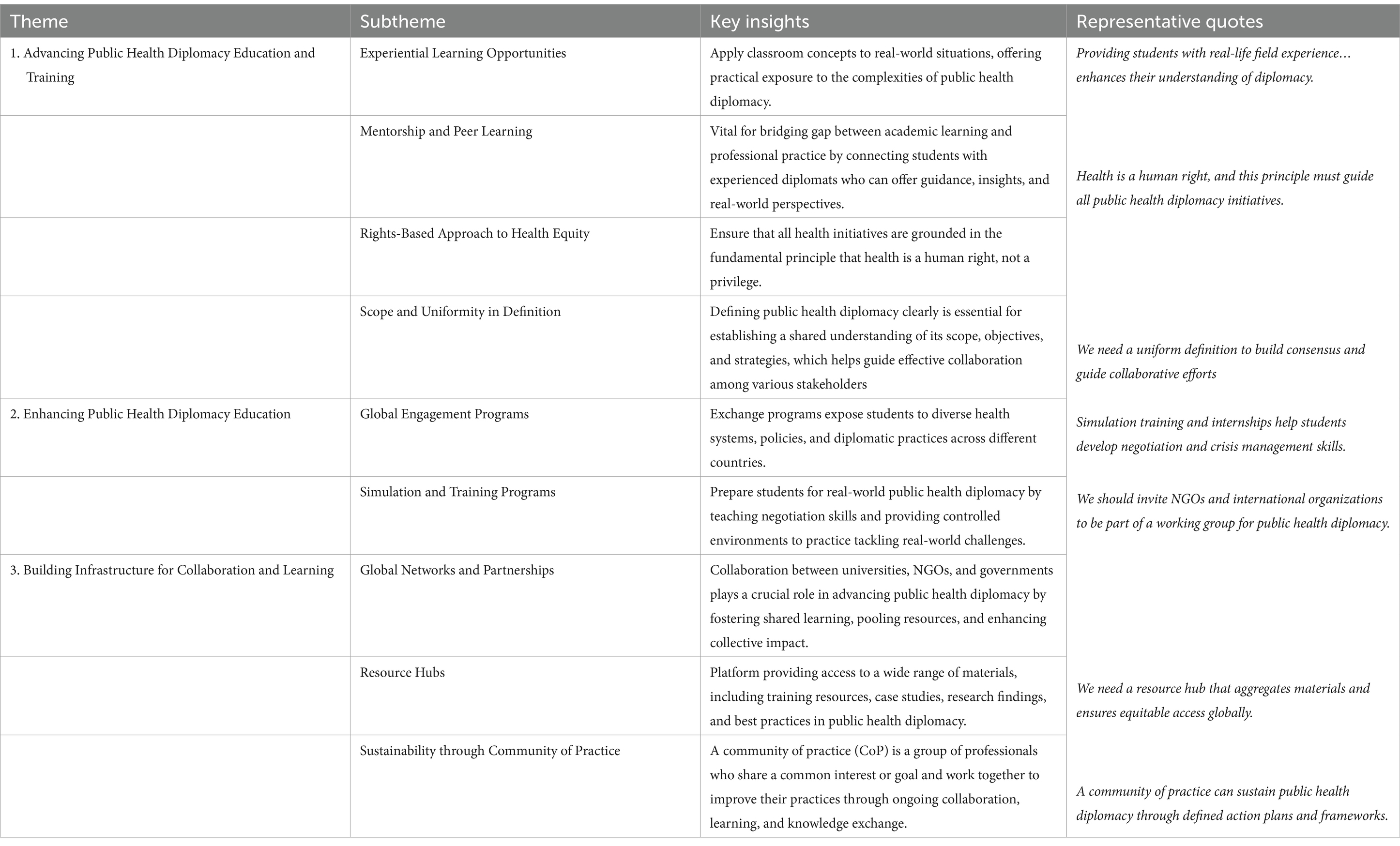
Table 3. Key themes and insights from discussion 3 of the public health diplomacy summit.
4. Global and regional collaborations to develop resources for health diplomacy education
This discussion (Table 4) focused on the importance of partnerships, working groups, and initiatives to advance public health diplomacy. It included topics like mentorship and networking programs, collaboration with governments and NGOs, and creating opportunities for experiential learning.
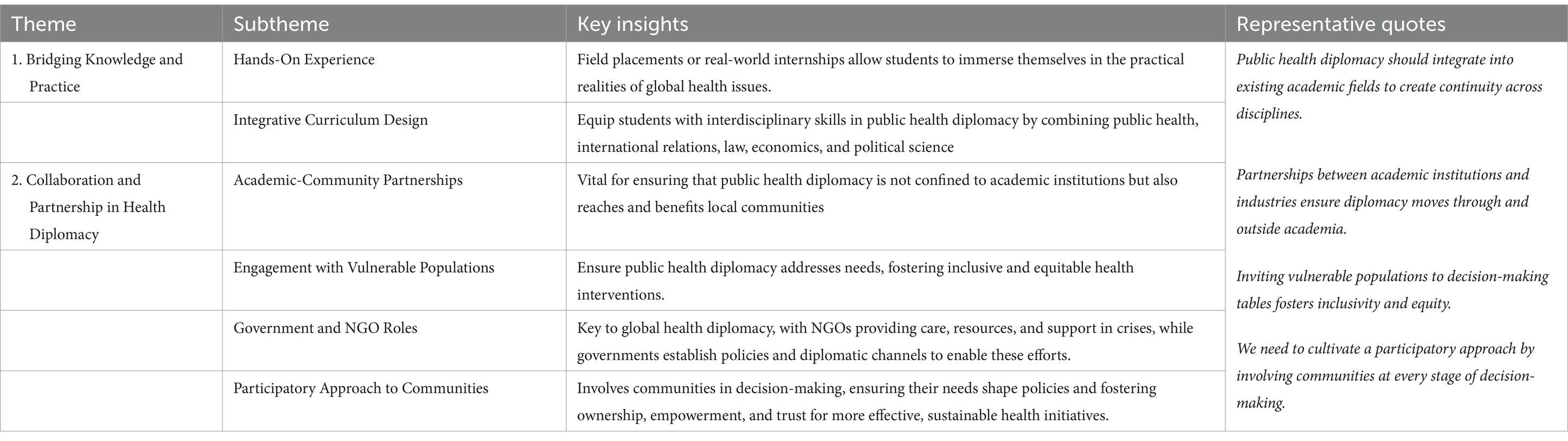
Table 4. Key themes and insights from discussion 4 of the public health diplomacy summit.
Participants also noted that currently, no established and widely accepted definition exists specifically for the public health diplomacy and so initial discussions were focused on establishing a working definition that was more aligned with the needs of informal health diplomacy actors and the actual practice of health diplomacy among public health communities and stakeholders. This task was assessed as a priority since the term “public health diplomacy” was associated with other established terms associated with the diplomacy such as “health diplomacy,” “global health diplomacy,” and/or “global diplomacy,” that have generally focused on the actions of core and multistakeholder diplomacy actors. Consensus was built around the definition of public health diplomacy, defined as:
Public health diplomacy is a multidisciplinary field that enables its practitioners to effectively communicate, facilitate, negotiate and build consensus using systems thinking, evidence based, community-informed approaches, based on equity-focused and human-centered values to improve health and well-being for all.
Following the discussions over the three days, the following 9-point action plan was established.
1. Participants proposed the establishment of a “Global Public Health Diplomacy Working Group” by inviting member schools and programs from ASPPH and GNAPH to review and build on the concept map to reflect and reconcile different perspectives and disciplines and the factors contributing to public health diplomacy.
2. Participants proposed the creation of “Public Health Diplomacy capacity-building group” globally that will work with key public health training and academic institutions across various regions to gather insights into the skills and competencies essential for public health students. The working group would also explore options and partnerships that could implement the review.
3. Participants agreed to Identify “global and region-specific learning outcomes” to prepare public health students to succeed in an interconnected and complex world through public health diplomacy. Participants assessed this task to be a priority.
4. Participants agreed to advance “public health diplomacy by engaging decision-makers and stakeholders” (including foreign services, ministries of health, academic institutes, civil society members, policy makers, and other international organizations like WHO and UN) in their geographic regions to create more awareness about the field.
5. Participants agreed to develop an online, interactive resource hub to disseminate global learning opportunities for Public Health Diplomacy Research, Innovation, Skills, and Experiential learning (PHD-RISE).
6. Participants agreed to “organize events” to help raise awareness about public health diplomacy in the field of public health.
7. Participants agreed to “analyze and share the region’s experiences, best practices and achievements” in public health diplomacy across various communication outlets to further develop the field.
8. Participants agreed to “expand regional and institutional partnerships” in collaboration with the University of Memphis School of Public Health, ASPPH and GNAPH to advance public health diplomacy.
9. Participants agreed to disseminate recommendations from participants to their respective institutions to move forward.
These nine-point action plan is not intended to be sequential; rather, the actions should be pursued concurrently based on needs and capacities. Additionally, the numbering does not indicate prioritization, as implementation strategies may vary across different contexts.
Conclusion
Public health diplomacy is a multidisciplinary field enabling practitioners to communicate, negotiate, and build consensus using equity-focused, evidence-based, and community-informed approaches to improve global health. Key recommendations included forming capacity-building groups, creating global learning outcomes, and establishing a resource hub for research, innovation, and skills development. Participants emphasized collaboration among governments, NGOs, academia, and communities to address health challenges through inclusive solutions.
Effective health diplomacy requires experiential learning, mentorship, and interdisciplinary education, but challenges like data sharing, cultural communication, and sustainability remain. Training in “practical diplomacy” equips global health students to navigate local and global challenges effectively.
Ethics statement
Ethical review and approval was not required for the study of human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants OR patients/participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
AJ: Conceptualization, Methodology, Writing – original draft. LM: Writing – review & editing. K-HT: Writing – review & editing. DM: Writing – review & editing. KM: Writing – review & editing. DR: Writing – review & editing. WH: Writing – review & editing. ShD: Writing – review & editing. JM: Writing – review & editing. RR: Writing – review & editing. SK: Writing – review & editing. WL: Writing – review & editing. WA: Writing – review & editing. GN: Writing – review & editing. MJ: Writing – review & editing. BK: Writing – review & editing. BS: Writing – review & editing. NJ: Formal Analysis, Software, Writing – review & editing. RK: Writing – review & editing. GS: Writing – review & editing. EK: Writing – review & editing. RS: Writing – review & editing. CK: Writing – review & editing. WY: Writing – review & editing. MB: Writing – review & editing. XY: Writing – review & editing. GP: Writing – review & editing. BT: Writing – review & editing. MO: Writing – review & editing. ML: Writing – review & editing. StC: Writing – review & editing. MK: Writing – review & editing. KG: Writing – review & editing. SP: Writing – review & editing. DB: Writing – review & editing. MT: Writing – review & editing. AL: Writing – review & editing. SS: Writing – review & editing. TM: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1564709/full#supplementary-material
References
1. Sykes, S, Watkins, M, and Wills, J. Public health practitioners as policy advocates: skills, attributes and development needs. Health Promot Int. (2023) 38:daad102. doi: 10.1093/heapro/daad102
2. WHO. Health promotion glossary of terms 2021. 1st ed. Geneva: World Health Organization (2021). 1 p.
3. Katz, R, Kornblet, S, Arnold, G, Lief, E, and Fischer, JE. Defining health diplomacy: changing demands in the era of globalization. Milbank Q [Internet]. (2011) 89:503–23. doi: 10.1111/j.1468-0009.2011.00637.x
4. Colglazier, EW, Told, M, Yilla, M, Garay, J, and Fernandez, G. COVID-19 as a revelation: challenges in Global Health Diplomacy & Disaster Diplomacy | Sci Diplomacy [Internet] (2021). Available online at: https://www.sciencediplomacy.org/perspective/2021/covid-19-revelation-challenges-in-global-health-diplomacy-disaster-diplomacy (Accessed January 8, 2025)
5. Mackey, TK, and Strathdee, SA. Responding to the public health consequences of the Ukraine crisis: an opportunity for global health diplomacy. J Int AIDS Soc. (2015) 18:19410. doi: 10.7448/IAS.18.1.19410
6. Mackey, TK. Global health diplomacy and the governance of counterfeit medicines: a mapping exercise of institutional approaches. J Health Dipl [Internet]. (2013). Available online at: http://www.ghd-net.org/abstracts/volume-1/5 (Accessed January 8, 2025)
7. Shakeel, SI, Brown, M, Sethi, S, and Mackey, TK. Achieving the end game: employing “vaccine diplomacy” to eradicate polio in Pakistan. BMC Public Health [Internet]. (2019) 19:79. doi: 10.1186/s12889-019-6393-1
8. Kickbusch, I, and Liu, A. Global health diplomacy-reconstructing power and governance. Lancet Lond Engl. (2022) 399:2156–66. doi: 10.1016/S0140-6736(22)00583-9
9. Hotez, PJ, and Narayan, KMV. Restoring vaccine diplomacy. JAMA [Internet]. (2021) 325:2337–8. doi: 10.1001/jama.2021.7439
10. Brown, MD, Bergmann, JN, Novotny, TE, and Mackey, TK. Applied global health diplomacy: profile of health diplomats accredited to the United States and foreign governments. Glob Health [Internet]. 14:2. doi: 10.1186/s12992-017-0316-7
11. Kickbusch, I. Global health diplomacy: how foreign policy can influence health. BMJ [Internet]. (2011) 342:d3154. doi: 10.1136/bmj.d3154
12. Harte, R, Glynn, L, Rodríguez-Molinero, A, Baker, PM, Scharf, T, Quinlan, LR, et al. A human-centered design methodology to enhance the usability, human factors, and user experience of connected health systems: a three-phase methodology. JMIR Hum Factors [Internet]. (2017) 4:e5443. doi: 10.2196/humanfactors.5443
Keywords: health diplomacy, public health diplomacy, global health governance, health policy, Global Health Security, public health competencies
Citation: Joshi A, Magana L, Tsai K-H, Maddah D, Mitchell K, Ruggiero D, Hawkins WB, Dharamsi S, Makhoul J, Reis R, Kim SY, Low WY, Amde W, Nja G, Jeu M, Kelly B, Saliba B, Jha N, Kalediene R, Scarpetti G, Kastrup E, Surenthirakumaran R, Kane C, Yotive W, Brown M, Yu X, Peterson G, Tsacoyianis B, Ofori MA, Levy M, Chirwa S, Karimi M, Geron K, Patel S, Biberman D, Taylor M, Longuevan A, Shular S and Mackey TK (2025) Public health diplomacy: summary of the methods and outcome of the 1st University of Memphis School of Public Health Diplomacy Summit. Front. Public Health. 13:1564709. doi: 10.3389/fpubh.2025.1564709
Edited by:
Sunel Kumar, Jiangsu University, ChinaReviewed by:
María Antonieta Moreno-Reynosa, National Institute of Public Health, MexicoJenny Samaan, Child Family Health International (CFHI), United States
Copyright © 2025 Joshi, Magana, Tsai, Maddah, Mitchell, Ruggiero, Hawkins, Dharamsi, Makhoul, Reis, Kim, Low, Amde, Nja, Jeu, Kelly, Saliba, Jha, Kalediene, Scarpetti, Kastrup, Surenthirakumaran, Kane, Yotive, Brown, Yu, Peterson, Tsacoyianis, Ofori, Levy, Chirwa, Karimi, Geron, Patel, Biberman, Taylor, Longuevan, Shular and Mackey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ashish Joshi, YXNoaXNoLmpvc2hpQG1lbXBoaXMuZWR1