 Piotr Karniej1,2
Piotr Karniej1,2 Anthony Dissen3
Anthony Dissen3 Pablo del Pozo-Herce4
Pablo del Pozo-Herce4 Raúl Juárez-Vela2
Raúl Juárez-Vela2 Antonio Martínez-Sabater2,5,6Vicente Gea-Caballero7
Antonio Martínez-Sabater2,5,6Vicente Gea-Caballero7 Emmanuel Echaniz-Serrano8
Emmanuel Echaniz-Serrano8 Iván Santolalla-Arnedo2
Iván Santolalla-Arnedo2 Michał Czapla2,9,10*
Michał Czapla2,9,10*- 1Faculty of Finance and Management, WSB MERITO University in Wroclaw, Wrocław, Poland
- 2Group of Research in Care and Health (GRUPAC), Faculty of Health Sciences, University of La Rioja, Logroño, Spain
- 3School of Health Sciences, Stockton University, Galloway, NJ, United States
- 4Research Group on Innovation in Health Care and Nursing Education (INcUidE), University of UNIE, Madrid, Spain
- 5Nursing Care and Education Research Group (GRIECE), GIUV2019-456, Nursing Department, University of Valencia, Valencia, Spain
- 6Care Research Group (INCLIVA), Hospital Clínico Universitario de Valencia, Valencia, Spain
- 7Faculty of Health Sciences, Research Group Community Health and Care, International University of Valencia, Valencia, Spain
- 8Sapienf (B53_23R) Research Group, Department of Physiatry and Nursing, Faculty of Health Sciences, University of Zaragoza, Zaragoza, Spain
- 9Division of Scientific Research and Innovation in Emergency Medical Service, Department of Emergency Medical Service, Faculty of Nursing and Midwifery, Wroclaw Medical University, Wrocław, Poland
- 10Institute of Heart Diseases, University Hospital, Wroclaw, Poland
Introduction: Healthcare professionals play a critical role in providing affirmative care to gay and lesbian patients. However, their attitudes and practices can vary significantly depending on cultural and educational contexts. This study aimed to evaluate differences in affirmative practices among healthcare professionals in Poland and Spain, focusing on their approach to these patient groups, utilizing the Gay Affirmative Practice (GAP) Scale, as well as identifying key factors influencing these practices.
Methods: A cross-sectional study was conducted among healthcare professionals in Poland and Spain using the GAP Scale, which assesses beliefs and behaviors toward gay and lesbian patients. Data collection included 495 participants, with 205 from Spain and 290 from Poland. Descriptive statistics, Mann–Whitney tests, and multivariate regression analyses were used to identify factors associated with affirmative practices.
Results: Spanish participants scored significantly higher on both the beliefs and behaviors scales compared to Polish participants (p < 0.001 and p = 0.009, respectively). Gender of healthcare providers was a significant factor in both groups, with women demonstrating more affirmative beliefs than men. In the Polish group, being male was associated with a decrease in the belief scale score by an average of 6.572 points (regression coefficient = −6.572, p < 0.001), while attending LGBT-related training 1–2 times was associated with an increase of 5.356 points on the belief scale (regression coefficient = 5.356, p = 0.039). No significant independent predictors were identified for behaviors in the Polish group, as all p-values exceeded 0.05.
Conclusion: Spanish healthcare professionals showed more affirmative practices toward gay and lesbian patients than their Polish counterparts. Sex and gay and lesbian related training influenced beliefs, with male sex linked to lower affirmative practice in Poland. These findings highlight the need for systematic integration of gay and lesbian specific training into healthcare education programs to foster cultural competence and reduce disparities in patient care.
1 Introduction
The concept of “health inequalities” refers to the impact of factors such as wealth, education, occupation, race or ethnicity, sexual orientation, and other socio-cultural determinants on population health. These inequalities in healthcare contribute to poorer health outcomes in vulnerable social and cultural groups (1). Biases among health professionals can influence the quality of care; implicit prejudices related to race, age, gender identity, and sexual orientation generate inequalities in care and negatively affect health outcomes in vulnerable groups (2). Access to healthcare for gay and lesbian individuals can be hindered by various factors, including biases and discrimination from medical personnel. Research from different healthcare systems, particularly in the United States, has shown that race and ethnicity significantly contribute to healthcare disparities, often exacerbating barriers to affirming medical care (3). While this issue is widely studied in the U.S., there is a lack of research exploring how racial and ethnic factors influence LGBT healthcare experiences in Poland and Spain patients (4). A recent study by the European Union Agency for Fundamental Rights found that 16% of all LGBTI individuals, including transgender people, faced discrimination in healthcare settings, while among transgender respondents, this figure increased to 34% (5).
In recent years, the health of LGBT individuals has gained attention due to specific health concerns and significant mental health disparities compared to heterosexual and cisgender individuals (6–9). Gay and lesbian individuals face elevated rates of mental health issues, such as anxiety, depression, substance abuse, and suicidal risk. Additionally, they encounter significant barriers in accessing culturally competent healthcare, which may contribute to health disparities (10). They also experience higher rates of sexually transmitted infections (STIs), substance abuse, and mental health issues, contributing to a greater disease burden (11, 12).
Despite the need for inclusive healthcare, LGBT individuals encounter significant barriers to access, including discrimination, stigma, and a lack of specific competencies among healthcare professionals (8, 9, 13, 14). Meyer’s study found that LGBT individuals experience high levels of psychosocial stress due to societal discrimination and stigma, which negatively impacts mental health, increasing the incidence of anxiety, depression, and other disorders (15). Exposure to stigma is linked to adverse mental health outcomes, which constitute key sources of both morbidity and mortality in this population (10). Such inequalities in healthcare, often stemming from negative or discriminatory experiences with professionals and care providers, prompt many in the LGBT+ community to delay healthcare needs, which negatively impacts health. Research by Katz-Wise suggests that fear of discrimination makes LGBT+ individuals less likely to seek medical care (16, 17).
A major barrier to inclusive care is the lack of adequate training on sexual and gender diversity for healthcare professionals. Training institutions often omit specific LGBT-related content, perpetuating biases and exclusionary practices. This lack of training affects care quality and fosters an environment of stigma, impacting both professionals and patients, with negative repercussions on patient care experiences and trust in providers (18, 19). Healthcare professionals emphasize the importance of awareness, collaboration, and specific training on LGBT+ health issues (14). However, a general lack of knowledge and certain insecurities about treating this group remain, sometimes exacerbated by the pathologization of minority gender identities and sexual orientations. This suggests that proper training would allow healthcare professionals to approach LGBT+ patient care with greater safety and empathy. This would help address health disparities in this group and promote more inclusive and effective care.
The cultural and social context has been shown to play a key role in shaping health professionals’ attitudes and practices when they are working with the patients that they serve. In countries such as Poland and Spain, regulatory frameworks, social climate, and public perception of LGBT+ individuals vary, influencing affirmative practices among professionals. While Spain has made significant progress in implementing laws protecting LGBT+ rights, Poland faces challenges in accepting and normalizing these rights, potentially affecting healthcare professionals’ readiness to adopt affirmative practices (20, 21).
The aim of this study was to evaluate the differences in affirmative practices toward gay and lesbian patients among healthcare professionals in Poland and Spain using the Gay Affirmative Practice Scale, and to identify which key factors were shown to have the greatest force of influencing these practices.
2 Methodology
2.1 Study design and participants
This cross-sectional study was conducted between February 2023 and August 2024 among healthcare professionals in Poland and Spain. Participants included a range of healthcare professionals and students in fields such as nursing, medicine, and the allied health professions. Eligibility criteria required participants to be at least 18 years old, proficient in Polish or Spanish, and active in a medical profession or education program.
2.2 Data collection and tools
Data were collected via an online platform Webankieta (22), using an anonymous, selfadministered questionnaire, which was distributed through targeted campaigns on social media platforms, including Facebook and Instagram. Participants were informed about the study’s purpose, objectives, and procedures, and provided informed consent before participating. The survey was designed to ensure the integrity of responses by utilizing IP filtering to prevent multiple submissions from the same user. It is worth emphasizing that this process was fully automated, and researchers had no direct access to individual IP addresses.
The questionnaire comprised two sections. The first section gathered demographic information, including age, gender, place of residence, marital status, profession, and participation in LGBT-related training within the last 5 years. In the interest of analytical clarity, only heterosexual respondents were included in further analyses. Additionally, certain demographic responses were consolidated: individuals who were divorced or widowed were grouped together, and only legally recognized marriages were considered.
The second section utilized the Gay Affirmative Practice (GAP) Scale, a psychometric tool originally developed by Catherine Crisp to evaluate healthcare providers’ beliefs and behaviors in their work with lesbian and gaypatients (23). For this study, the Polish (GAP-PL) (24) and Spanish (GAP-ES) (25) versions of the GAP Scale, previously adapted by Karniej et al., were used, both developed as part of the Health Exclusion Research in Europe (HERE) project (26).
The Polish version (GAP-PL) demonstrated high internal consistency, with Cronbach’s alpha values ranging from 0.936 to 0.949 across subscale domains, and a McDonald’s omega coefficient of 0.963, indicating excellent reliability (24). The Spanish version (GAP-ES) also showed strong internal consistency, with Cronbach’s alpha values of 0.915 for the beliefs subscale and 0.902 for the behaviors subscale, and a McDonald’s omega coefficient of 0.942 (25). Each item on the GAP Scale is scored from 15 to 75, with higher scores reflecting more affirmative practices. The robust reliability of these versions supports their use in cross-cultural comparisons between Polish and Spanish healthcare professionals.
2.3 Statistical analysis
The mean, standard deviation, median, quartiles, and range were calculated for quantitative variables. For categorical variables, absolute and relative frequencies (N and %) were presented. To compare categorical variables between groups, the chi-squared test was applied (with Yates correction for 2×2 tables), or Fisher’s exact test was used when expected values were low. For quantitative variable comparisons between two groups, the Mann–Whitney U test was employed, while comparisons across three or more groups were performed using the Kruskal-Wallis test, followed by Dunn’s post-hoc test if needed. Spearman’s correlation coefficient was used to examine relationships between two quantitative variables. Multiple linear regression was utilized to analyze the influence of various predictors on quantitative outcomes, with regression parameters and 95% confidence intervals reported. A significance level of 0.05 was set for all analyses. Statistical analyses were carried out using R software, version 4.4.1 (27).
3 Results
3.1 Characteristics of the study population
The study population comprised healthcare professionals from Spain and Poland, with notable demographic differences between the two groups. The proportion of male respondents was higher in the Polish group, whereas the Spanish group was older on average, with a significantly higher mean age (p < 0.001). Polish participants were more likely to reside in larger cities (p < 0.001). In terms of marital status, Polish respondents were more frequently single, while Spanish participants reported higher rates of formal partnerships and marriages (p < 0.001). Professionally, a higher percentage of nurses/midwives were found in the Spanish group, whereas the Polish group had a greater proportion of physicians, students, and other healthcare professionals (p < 0.001). Additionally, participation in LGBT-related trainings was more frequent among Spanish respondents (p < 0.001). Full data regarding the characteristics of the study group are presented in Table 1.
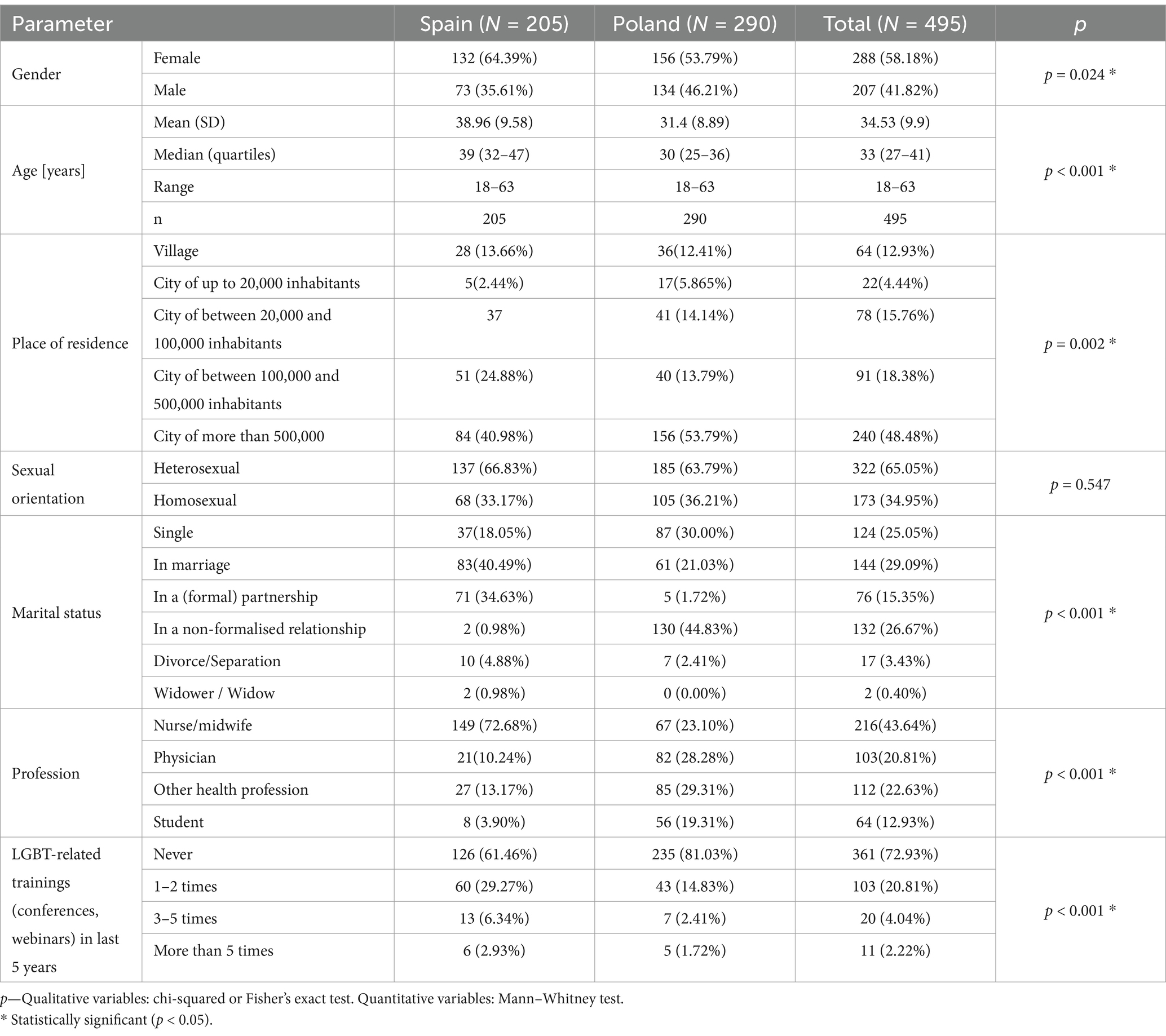
Table 1. Characteristics of the study population.
3.2 Results of GAP comparison between Poland and Spain
The GAP questionnaire evaluated respondents’ beliefs and behaviors towards gay and lesbian patients, with scores ranging from 15 to 75 on each scale. Higher scores indicate a more affirmative approach, and analysis was limited solely to heterosexual participants. The Spanish group scored significantly higher on the beliefs scale compared to the Polish group (p < 0.001), indicating more affirmative attitudes towards gay and lesbian patients. Similarly, the Spanish group scored higher on the behaviors scale than the Polish group (p = 0.009), reflecting more affirmative behavioral responses. Full data regarding the GAP scale scores are presented in Table 2.
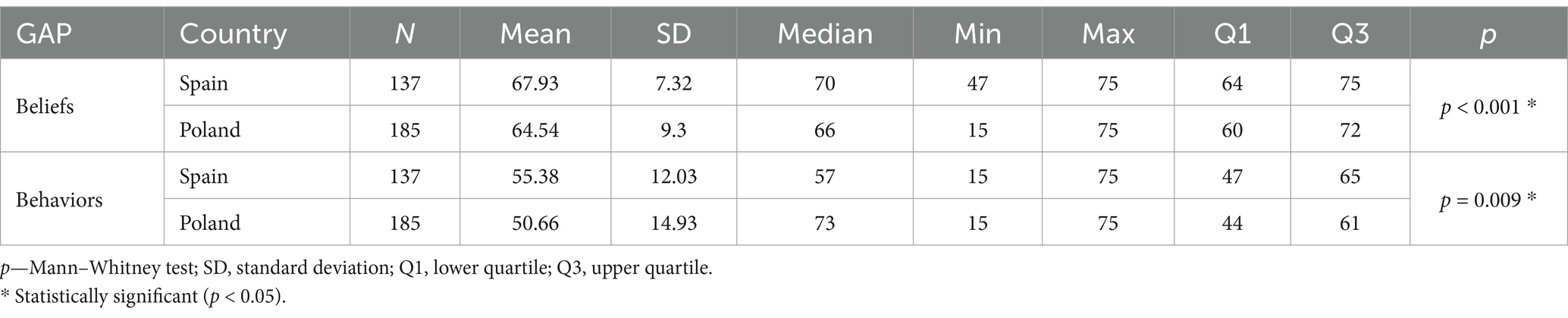
Table 2. Results of GAP comparison between Poland and Spain.
3.3 GAP scale scores in the Spanish group
In the Spanish heterosexual group, gender differences were observed on the belief scale, with women scoring significantly higher than men (p = 0.037). However, no statistically significant differences were found across other demographic variables, including place of residence, marital status, profession, and frequency of LGBT-related training in the past 5 years (all p-values > 0.05).
For marital status, widowed and divorced individuals were analyzed as a combined category, and distinctions between marriage to a man or woman were not considered, as the analysis was conducted separately for heterosexual and homosexual individuals. Additionally, participants who attended LGBT-related trainings more than five times were grouped with those who attended three to five times.
Regarding age, no significant correlations were identified with either the beliefs or behaviors domains. Specifically, Spearman’s correlation coefficient for age and beliefs was r = −0.019, p = 0.826, and for age and behaviors, r = 0.01, p = 0.908. Full data for these analyses are presented in Table 3.
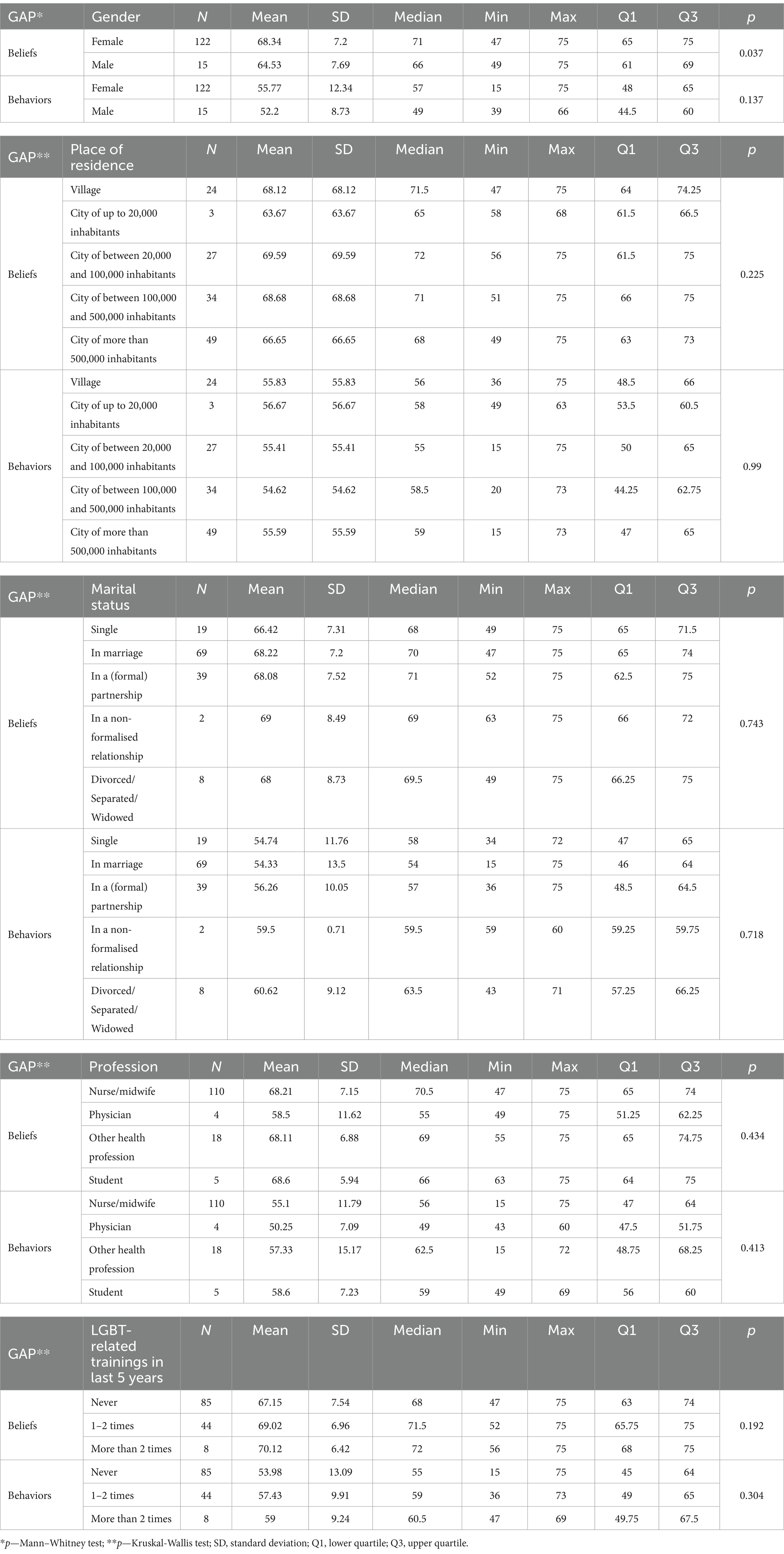
Table 3. Analysis of GAP scale scores by characteristics in the Spanish group.
3.4 GAP scale scores in the polish group
In the Polish heterosexual group, belief scale scores were significantly higher among women than men (p = 0.009). No statistically significant relationships were found across other demographic variables, including age, place of residence, marital status, profession, or frequency of LGBT-related training in the past 5 years (all p-values > 0.05). For age, Spearman’s correlation coefficient was r = −0.018, p = 0.809 for beliefs and r = −0.02, p = 0.788 for behaviors. Full data for these analyses are presented in Table 4.
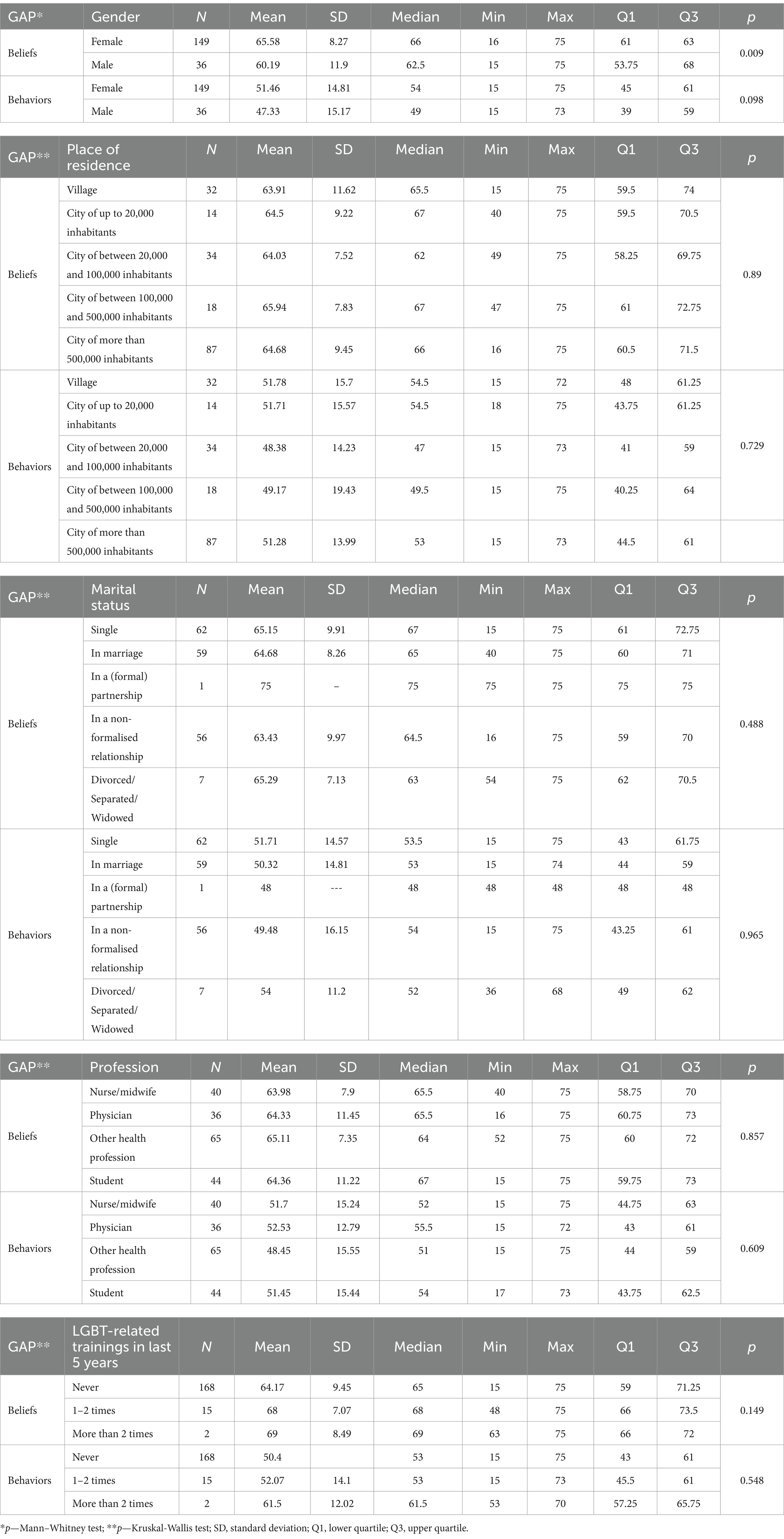
Table 4. Analysis of GAP scale scores by characteristics in the Polish group.
3.5 Multivariate analysis
In the Spanish group, the multivariate linear regression model indicated that none of the analyzed characteristics were significant independent predictors of scores on either the beliefs or behaviors scales, as all p-values were greater than 0.05. Table 5. Multivariate Analysis of Independent Predictors for GAP Scale Scores in the Spanish Group.
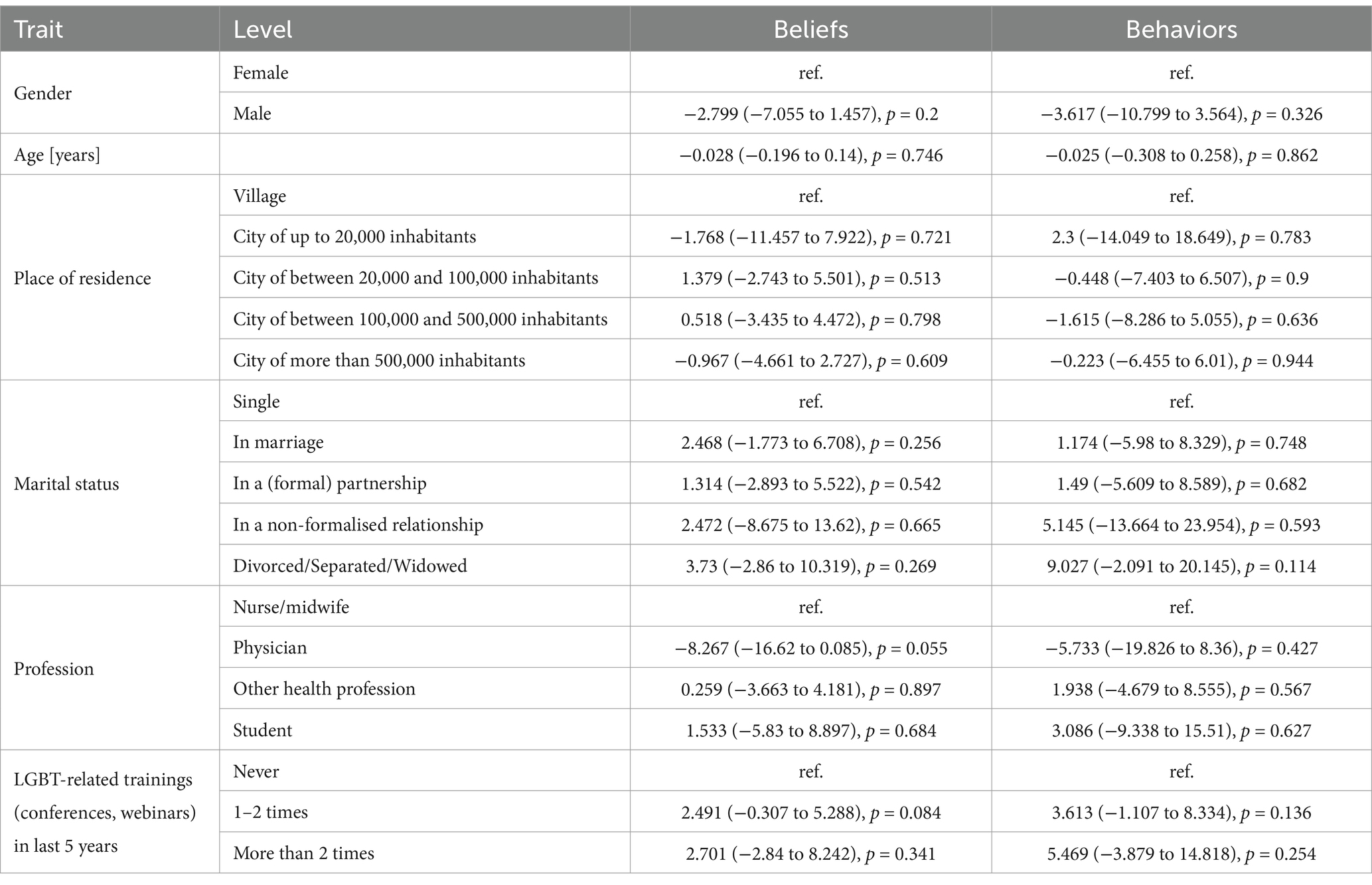
Table 5. Multivariate analysis of independent predictors for GAP scale scores in the Spanish group.
In the Polish heterosexual group, the multivariate linear regression model showed that being male decreases the belief scale score by an average of 6.572 points, as the regression coefficient is −6.572 (p < 0.001). Additionally, attending LGBT-related training 1–2 times increases the belief scale score by an average of 5.356 points, as the regression coefficient is 5.356 (p = 0.039). No significant independent predictors were identified for the behavior scale (all p-values > 0.05). Full data for these analyses are presented in Table 6.
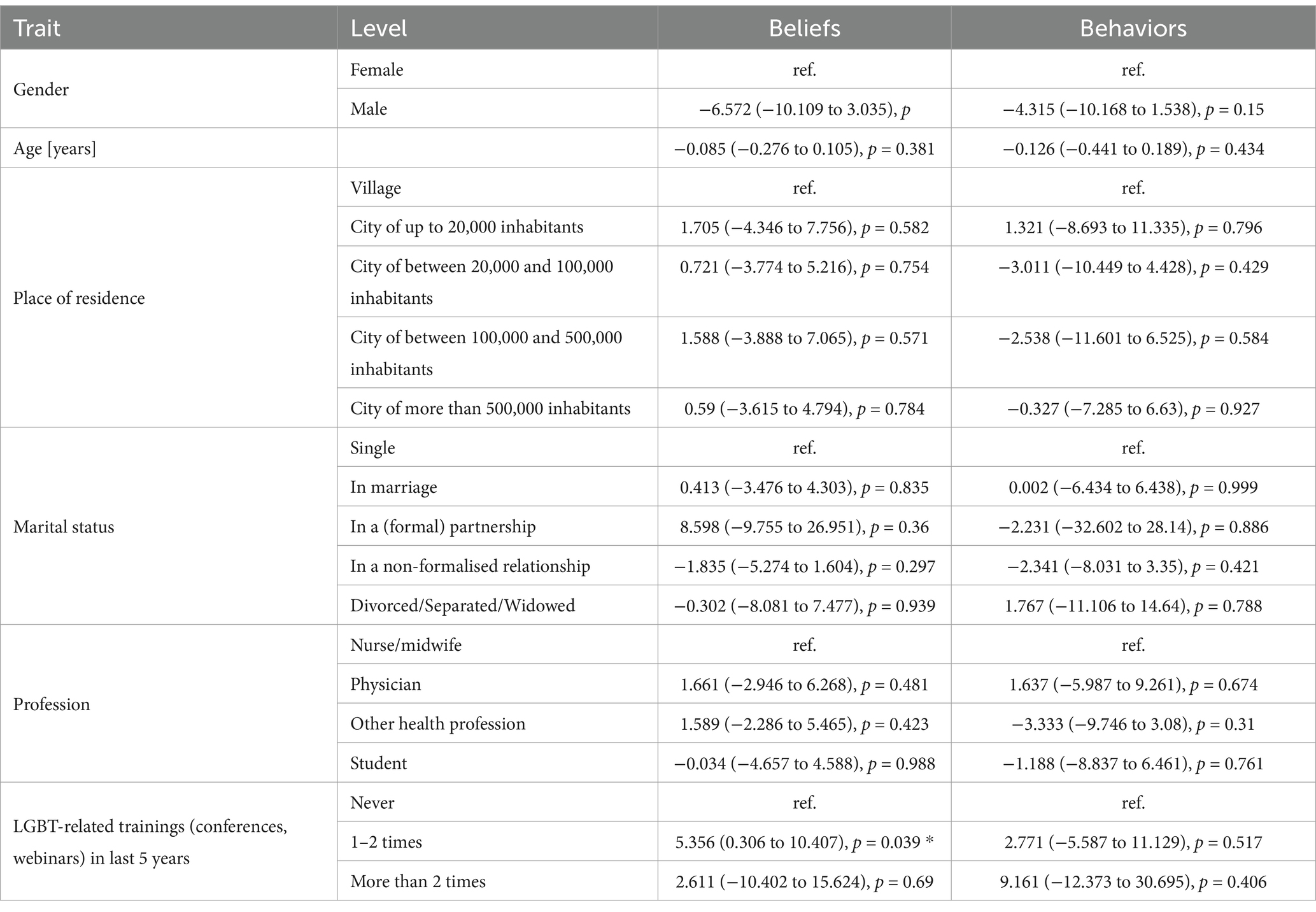
Table 6. Multivariate analysis of independent predictors for GAP scale scores in the Polish group.
4 Discussion
This study evaluated the differences in affirmative practices toward gay and lesbian patients among healthcare professionals in Poland and Spain using the GAP, highlighting the factors that most influence these practices, and their implications for addressing health inequalities in these two healthcare systems (28, 29). The findings reveal significant differences between the two countries, consistent with prior research showing how cultural and legislative environments shape healthcare professionals’ willingness to adopt inclusive practices (21). Demographic analysis indicated notable disparities. Spanish professionals were older on average, with a higher proportion of women, suggesting a potential link between professional experience and sensitivity to sexual diversity (8, 9). In contrast, the predominance of male and single professionals in Poland may reflect sociocultural factors that limit openness toward inclusive practices (30–32). Similar issues have been observed globally, where discrimination in LGBT care is linked to inadequate training among professionals and educators (33).
The results of the residency analysis also indicated that, while in Spain health professionals are more evenly distributed in urban and rural areas, in Poland there is a greater concentration in large cities. This difference may have important implications for the accessibility of health services in rural settings in both countries (34–36), as studies have shown that rural areas often present greater barriers to inclusive healthcare. This issue disproportionately affects lesbian and gay individuals (30, 31), who may experience stigma in their environment, leading to a lower willingness to seek healthcare services in their communities.
Along the same lines, the study revealed significant differences in LGBT-related training among professionals in both countries. A total of 61.46% of Spanish participants and 81.03% of Polish participants reported never having participated in such training. Among those who did, most attended events only once or twice in the past 5 years. These findings emphasize the persistent link between insufficient sexual diversity training and the stigmas affecting the healthcare of gay and lesbian individuals. According to the European Union Agency for Fundamental Rights, 34% of transgender individuals report discrimination in healthcare settings, while 46% of LGBT individuals avoid disclosing their identity to providers out of fear of discrimination (37). A lack of training on sexual and gender diversity issues remains a recurring barrier to developing competencies necessary for inclusive care (24–26, 28). Furthermore, insufficient training undermines the perceived quality of care and erodes trust between LGBT patients and healthcare providers, contributing to gaps in inclusive health services (38).
The frequency of training emerged as a positive predictor of affirmative attitudes in Poland, demonstrating that LGBT-specific competency training fosters inclusivity and reduces the risk of pathologizing sexual orientation, particularly in environments with lower social acceptance of sexual minorities (30, 32, 39). Limited access to such training appears to hinder healthcare professionals’ ability to provide respectful and affirming care (15, 39–42), especially in Polish settings where cultural sensitivity toward sexual diversity remains a significant challenge (32, 43). Comprehensive training programs could mitigate implicit biases and improve health outcomes, particularly for vulnerable groups who often encounter greater barriers to accessing affirmative healthcare (17, 44).
The GAP scale assessment revealed that Spanish healthcare professionals scored significantly higher than their Polish counterparts on both affirmative beliefs (mean: 67.93 vs. 64.54) and behaviors (mean: 55.38 vs. 50.66), with results showing statistical significance (p < 0.001). This disparity likely reflects the cultural and legislative differences between the two countries.
Spain’s legal and social framework supports LGBT rights, fostering a more inclusive and affirmative clinical environment. In contrast, Poland’s conservative policies and attitudes may hinder the ability of healthcare professionals to provide empathetic and inclusive care, posing a significant barrier to equality in the healthcare setting. For example, Poland does not legally recognize same-sex unions and has implemented restrictions on discussions of LGBT issues in schools and public institutions (4, 15, 30, 32, 39). The significant difference in the percentage of nonformalized relationships between Spain and Poland in our study (0.98% vs. 44.83%) may be explained by the fact that Spain has legalized same-sex marriage, while Poland still does not recognize same-sex unions, though legislative efforts have been initiated in recent years (4).
A detailed analysis of subgroups within the Spanish population revealed that while women scored higher on the belief scale compared to men, no significant differences were observed on the behavior scale or other demographic variables, such as place of residence or marital status. This suggests that, despite some gender-based variations, affirmative practices in Spain are generally consistent across demographics, likely reflecting the country’s supportive social and legal context for LGBT rights, which fosters a broadly affirmative attitude among healthcare professionals. In Poland, gender differences were more pronounced, with women showing significantly higher affirmative beliefs compared to men. This disparity may be shaped by sociocultural factors, including traditional gender roles and conservative norms, which could limit men’s openness to inclusivity and diversity. In many conservative societies, masculinity is often associated with rigid gender expectations and heteronormativity, which may lead to lower acceptance of sexual minorities and reluctance to engage in affirmative practices (45, 46). Notably, LGBT-related training in Poland was positively associated with affirming beliefs, underscoring the potential of such training to address these barriers and enhance cultural competence among healthcare professional (32, 47).
It is noteworthy that a study conducted in China identified nursing educators as the group with the lowest scores in attitudes and knowledge regarding LGBT issues, compared to nursing students and practicing nurses (48). This finding is particularly concerning, as these educators are responsible for training future healthcare professionals. This highlights the urgent need for targeted training initiatives aimed at educators to enhance their cultural competence. In the United States, Italy and Spain, the Attitudes Toward LGBT People Scales have been used to assess attitudes toward LGBT people among university students, finding that social contact can reduce prejudice. In Brazil, a cross-sectional online survey during the COVID-19 pandemic characterized the LGBT population and found high levels of violence and discrimination. In Europe, the European Social Survey has been used to compare health and wellbeing between individuals in same-sex and opposite-sex partnerships, showing significant disparities (49, 50). In summary, studies indicate that social contact may reduce prejudice. These studies indicate that discrimination and lack of competence in health care are common problems for LGBT people.
Such findings underscore the global nature of this issue, affecting diverse cultures and regions. Implementing transformative measures, such as diversity and inclusion training, has proven effective; interventions with nursing students have demonstrated significant improvements in GAP scores post-training. Similarly, self-reflection exercises have been shown to enhance affirmative attitudes (51).
5 Limitations
This study has several limitations. The cross-sectional design prevents the establishment of causal relationships between variables. The reliance on surveys for data collection may have excluded certain healthcare professionals, particularly those in rural areas with limited internet access, potentially skewing the sample. Additionally, a larger and more diverse cohort could have offered a more comprehensive understanding of affirmative attitudes across different subgroups. The study’s quantitative methodology also restricted the ability to investigate the underlying motivations or barriers influencing affirmative practices. Incorporating qualitative methods in future research could provide richer insights and enhance the interpretation of these findings.
6 Conclusion
Healthcare professionals in Spain demonstrated significantly more affirmative practices toward gay and lesbian patients than their Polish counterparts, as indicated by higher scores on the Gay Affirmative Practice Scale. Sex emerged as an influential factor, with female professionals exhibiting more affirmative beliefs in both countries. In Poland, male sex correlated with lower scores on the beliefs scale, while participation in gay and lesbian-related training was associated with improved affirmative practices. Notably, no significant predictors were identified for behaviors in the Polish group.
Given the significant impact of gay and lesbian-related training on healthcare professionals’ affirmative beliefs, we strongly recommend the integration of structured and mandatory gay and lesbian-focused education modules into medical and allied health curricula. Such training should include practical and experiential learning components, such as simulations, role-playing, and patient interactions, to ensure effective knowledge transfer and promote inclusivity in clinical practice. By addressing gaps in cultural competence, these interventions can help reduce healthcare disparities and foster equitable care for gay and lesbian patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Bioethics Committee of Wrocław Medical University in Poland (Approval No. KB 976/2022) and the University of Valencia in Spain (Approval No. 2024-ENFPOD-3314668). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. AD: Conceptualization, Writing – original draft, Writing – review & editing. PP-H: Writing – original draft, Writing – review & editing. RJ-V: Writing – original draft, Writing – review & editing. AM-S: Writing – original draft, Writing – review & editing. VG-C: Conceptualization, Writing – original draft, Writing – review & editing. EE: Writing – original draft, Writing – review & editing. IS-A: Writing – original draft, Writing – review & editing. MC: Formal analysis, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to express their appreciation for the participation of all volunteers in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. OpenAI’s ChatGPT, was utilized for language editing and proofreading to ensure clarity, coherence, and linguistic accuracy in the final manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nowaskie, DZ, and Najam, S. Lesbian, gay, bisexual, and/or transgender (LGBT) cultural competency across the intersectionalities of gender identity, sexual orientation, and race among healthcare professionals. PLoS One. (2022) 17:e0277682. doi: 10.1371/journal.pone.0277682
2. Urrutia, MT, and Cianelli, R. Disparidad en Salud: Un Fenómeno Multidimensional. Available online at: https://pmc.ncbi.nlm.nih.gov/articles/PMC3349157/ (Accessed November 17, 2024).
3. Macias-Konstantopoulos, WL, Collins, KA, Diaz, R, Duber, HC, Edwards, CD, Hsu, AP, et al. Race, healthcare, and health disparities: a critical review and recommendations for advancing health equity. West J Emerg Med. (2023) 24:906–18. doi: 10.5811/westjem.58408
4. Jesus, S. Annual review 2025 | ILGA-Europe. (2025). Available online at: https://www.ilga-europe.org/report/annual-review-2025/ (Accessed March 17, 2025)
5. Council of Europe. Report highlights inadequate healthcare access for LGBTI people, recommends solutions. Portal. Available online at: https://www.coe.int/en/web/committee-antidiscrimination-diversity-inclusion/-/report-highlights-inadequate-healthcare-access-for-lgbti-people-recommends-solutions (Accessed November 17, 2024)
6. Lucassen, MF, Stasiak, K, Samra, R, Frampton, CM, and Merry, SN. Sexual minority youth and depressive symptoms or depressive disorder: a systematic review and meta-analysis of population-based studies. Aust N Z J Psychiatry. (2017) 51:774–87. doi: 10.1177/0004867417713664
7. Pellicane, MJ, and Ciesla, JA. Associations between minority stress, depression, and suicidal ideation and attempts in transgender and gender diverse (TGD) individuals: systematic review and meta-analysis. Clin Psychol Rev. (2022) 91:102113. doi: 10.1016/j.cpr.2021.102113
8. Ho, SH, Shamsudin, AH, Liow, JW, Juhari, JA, Ling, SA, and Tan, K. Mental healthcare needs and experiences of LGBT+ individuals in Malaysia: utility, enablers, and barriers. Healthcare. (2024) 12:998. doi: 10.3390/healthcare12100998
9. Rees, SN, Crowe, M, and Harris, S. The lesbian, gay, bisexual and transgender communities’ mental health care needs and experiences of mental health services: an integrative review of qualitative studies. J Psychiatr Ment Health Nurs. (2021) 28:578–89. doi: 10.1111/jpm.12720
10. Adelson, SL, Walker-Cornetta, E, and Kalish, N. LGBT youth, mental health, and spiritual care: Psychiatric collaboration with health care chaplains. J Am Acad Child Adolesc Psychiatry. (2019) 58:651–655. doi: 10.1016/j.jaac.2019.02.009
11. Han, BH, Duncan, DT, Arcila-Mesa, M, and Palamar, JJ. Co-occurring mental illness, drug use, and medical multimorbidity among lesbian, gay, and bisexual middle-aged and older adults in the United States: a nationally representative study. BMC Public Health. (2020) 20:1123. doi: 10.1186/s12889-020-09210-6
12. Everett, BG. Sexual orientation disparities in sexually transmitted infections: examining the intersection between sexual identity and sexual behavior. Arch Sex Behav. (2013) 42:225–36. doi: 10.1007/s10508-012-9902-1
13. Cronin, TJ, Pepping, CA, and Lyons, A. Mental health service use and barriers to accessing services in a Cohort of transgender, gender diverse, and non-binary adults in Australia. Sex Res Soc Policy. (2023) 1–14. doi: 10.1007/s13178-023-00866-4
14. Talbot, J, and Finlay, F. Empowering healthcare professionals with health promotion information for transgender adolescents. Arch Dis Child Educ Pract Ed. (2023) 108:158–62. doi: 10.1136/archdischild-2022-324744
15. Meyer, IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. (2003) 129:674–97. doi: 10.1037/0033-2909.129.5.674
16. Dale, VH, and Philomin, R. Educating for quality transgender health care: a survey…: Education for health. Available online at: https://journals.lww.com/edhe/fulltext/2022/35010/educating_for_quality_transgender_health_care__a.7.aspx (Accessed November 17, 2024)
17. Katz-Wise, SL, and Hyde, JS. Sexual fluidity and related attitudes and beliefs among young adults with a same-gender orientation. Arch Sex Behav. (2014) 44:1459–70. doi: 10.1007/s10508-014-0420-1
18. Filice, E, and Meyer, SB. Patterns, predictors, and outcomes of mental health service utilization among lesbians, gay men, and bisexuals: a scoping review. J Gay Lesbian Ment Health. (2018) 22:162–95. doi: 10.1080/19359705.2017.1418468
19. Lerner, JE, and Robles, G. Perceived barriers and facilitators to health care utilization in the United States for transgender people: a review of recent literature. J Health Care Poor Underserved. (2017) 28:127–52. doi: 10.1353/hpu.2017.0014
20. Bucholc, M. The anti-LGBTIQ campaign in Poland: the established, the outsiders, and the legal performance of exclusion. Law Policy. (2022) 44:4–22. doi: 10.1111/lapo.12183
21. Annual Review 2024. Available online at: https://www.ilgaeurope.org/report/annual-review-2024/ (Accessed August 25, 2024)
22. Webankieta. Available online at: https://www.webankieta.pl/ (Accessed April 11, 2024)
23. Crisp, C. The gay affirmative practice scale (GAP): a new measure for assessing cultural competence with gay and lesbian clients. Soc Work. (2006) 51:115–26. doi: 10.1093/sw/51.2.115
24. Karniej, P, Dissen, A, Juárez-Vela, R, Santolalla-Arnedo, I, Sufrate-Sorzano, T, Garrote-Camara, ME, et al. Psychometric properties and cultural adaptation of the polish version of the gay affirmative practice scale. Front Public Health. (2024) 12:12. doi: 10.3389/fpubh.2024.1384429
25. Karniej, P, Dissen, A, Juárez-Vela, R, Martinez Sabater, A, Pozo-Herce, P, Gea-Caballero, V, et al. Cultural adaptation and psychometric properties of the Spanish version of the gay affirmative practice scale (GAP-ES). Healthcare. (2024) 12:2258. doi: 10.3390/healthcare12222258
26. Karniej, P, Dissen, A, Juarez-Vela, R, Gea-Caballero, V, Echániz-Serrano, E, and Czapla, M. Psychometric properties and cultural adaptation of the polish version of the lesbian, gay, bisexual, and transgender development of clinical skills scale (LGBT-DOCSS-PL). J Homosex. (2024) 72:45–59. doi: 10.1080/00918369.2024.2302970
27. R: The R project for statistical computing. Available online at: https://www.r-project.org/ (Accessed September 27, 2024)
28. Nowaskie, D. A national survey of U.S. psychiatry residents’ LGBT cultural competency: the importance of LGBT patient exposure and formal education. J Gay Lesbian Ment Health. (2020) 24:375–91. doi: 10.1080/19359705.2020.1774848
29. Council of Europe. New report highlights inadequate healthcare access for LGBTI people and recommends solutions – sexual orientation and gender identity. Available online at: https://www.coe.int/en/web/sogi/-/new-report-highlights-inadequate-healthcare-access-for-lgbti-people-and-recommends-solutions-1 (Accessed November 17, 2024)
30. Holt, E. Supporting Poland’s LGBT+ community through thick and thin. Lancet HIV. doi: 10.1016/S2352-3018(24)00261-3
31. Krok, A, Kardasz, Z, and Rogowska, AM. Network analysis of the association between minority stress and activism in LGB people from Poland. Eur J Investig Health Psychol Educ. (2024) 14:1853–67. doi: 10.3390/ejihpe14070122
32. Kardasz, Z, Gerymski, R, and Parker, A. Anxiety, attachment styles and life satisfaction in the polish LGBTQ+ community. Int J Environ Res Public Health. (2023) 20:6392. doi: 10.3390/ijerph20146392
33. Cole, HS, Barrow, MG, Strickland, H, and Robinson, S. Empowering nursing students through inclusivity training for LGBTQIA+ patients: a quasi-experimental study. Nurse Educ Today. (2024) 142:106345. doi: 10.1016/j.nedt.2024.106345
34. May, JT, and Rainbow, JG. A qualitative description of direct Care Workers of Lesbian, gay, bisexual, transgender older adults. J Appl Gerontol. (2023) 42:597–606. doi: 10.1177/07334648221139477
35. Hollinsaid, NL, Price, MA, and Hatzenbuehler, ML. Transgender-specific adolescent mental health provider availability is substantially lower in states with more restrictive policies. J Clin Child Adolesc Psychol. (2024) 53:828–39. doi: 10.1080/15374416.2022.2140433
36. Walter-McCabe, H, and Chen, A. Editors’ introduction: transgender health equity and the law. J Law Med Ethics. (2022) 50:401–8. doi: 10.1017/jme.2022.83
37. Council of Europe. New report reveals that LGBTI individuals face inadequate healthcare access and recommends solutions. Centro di Ateneo per i Diritti Umani. (2024). Available online at: https://unipd-centrodirittiumani.it/en/news/council-of-europe-new-report-reveals-that-lgbti-individualsface-inadequate-healthcare-access-and-recommends-solutions (Accessed November 17, 2024)
38. Balandan, K. Mental health inequity and disparity in LGBTQI youth. J Nurse Pract. (2023) 19:104640. doi: 10.1016/j.nurpra.2023.104640
39. Yu, H, Flores, DD, Bonett, S, and Bauermeister, JA. LGBTQ + cultural competency training for health professionals: a systematic review. BMC Med Educ. (2023) 23:558. doi: 10.1186/s12909-023-04373-3
40. Nair, JM, Waad, A, Byam, S, and Maher, M. Barriers to care and root cause analysis of LGBTQ+ patients’ experiences: a qualitative study. Nurs Res. (2021) 70:417–24. doi: 10.1097/NNR.0000000000000541
41. Budge, SL, Adelson, JL, and Howard, KAS. Anxiety and depression in transgender individuals: the roles of transition status, loss, social support, and coping. J Consult Clin Psychol. (2013) 81:545–57. doi: 10.1037/a0031774
42. Kanakubo, Y, Sugiyama, Y, Yoshida, E, Aoki, T, Mutai, R, Matsushima, M, et al. Development and validation of the Japanese version of the lesbian, gay, bisexual, and transgender development of clinical skills scale. PLoS One. (2024) 19:e0298574. doi: 10.1371/journal.pone.0298574
43. Lantos, D, Mole, RCM, and Golec de Zavala, A. Born this way? National collective narcissism, implicit homophobia, and homosexual essentialism in populist Poland. Arch Sex Behav. (2024) 53:3907–3924. doi: 10.1007/s10508-024-02952-z
44. Fricke, J, Siddique, SM, Aysola, J, Cohen, ME, and Mull, NK. Healthcare worker implicit bias training and education: Rapid review. In: Making healthcare safer IV: A continuous updating of patient safety harms and practices. Rockville (MD): Agency for Healthcare Research and Quality (US) (2024).
45. Mole, RCM, de Zavala, AG, and Ardag, MM. Homophobia and national collective narcissism in populist Poland. Eur J Sociol Arch Eur Sociol. (2021) 62:37–70. doi: 10.1017/S0003975621000072
46. Ferrari, F, Imperato, C, and Mancini, T. Heteronormativity and the justification of gender hierarchy: investigating the archival data from 16 European countries. Front Psychol. (2021) 12:686974. doi: 10.3389/fpsyg.2021.686974
47. Torres, JL, Gonçalves, GP, Pinho, AA, and Souza, MHN. The Brazilian LGBT+ health survey: Methodology and descriptive results. Available online at: https://www.scielo.br/j/csp/a/wJQNMDdWdz5BjwY3G376b4R/?lang=en (Accessed November 17, 2024)
48. Wang, YC, Miao, NF, and You, MH. Attitudes toward, knowledge of, and beliefs regarding providing care to LGBT patients among student nurses, nurses, and nursing educators: a cross-sectional survey. Nurse Educ Today. (2022) 116:105472. doi: 10.1016/j.nedt.2022.105472
49. Cruciani, G, Quintigliano, M, Mezzalira, S, Scandurra, C, and Carone, N. Attitudes and knowledge of mental health practitioners towards LGBTQ+ patients: a mixed-method systematic review. Clin Psychol Rev. (2024) 113:102488. doi: 10.1016/j.cpr.2024.102488
50. Affuso, G, Picone, N, Costa, PA, Bacchini, D, de Angelis, G, Esposito, C, et al. Minority stress and mental health in gay and lesbian youth: a comparative study of Italy and Spain. Am J Orthopsychiatry. (2024) 94:148–58. doi: 10.1037/ort0000709
Keywords: healthcare professionals, LGBTQ+ health, affirmative practice, cultural competency, attitude of health personnel
Citation: Karniej P, Dissen A, del Pozo-Herce P, Juárez-Vela R, Martínez-Sabater A, Gea-Caballero V, Echaniz-Serrano E, Santolalla-Arnedo I and Czapla M (2025) Gay affirmative practices among healthcare professionals in Poland and Spain: results of Health Exclusion Research in Europe (HERE) study. Front. Public Health. 13:1568486. doi: 10.3389/fpubh.2025.1568486
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Richard Greggory Johnson III, University of San Francisco, United StatesAlbina Veltman, McMaster University, Canada
Copyright © 2025 Karniej, Dissen, del Pozo-Herce, Juárez-Vela, Martínez-Sabater, Gea-Caballero, Echaniz-Serrano, Santolalla-Arnedo and Czapla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michał Czapla, bWljaGFsLmN6YXBsYUB1bXcuZWR1LnBs