 Tenesha Littleton
Tenesha Littleton Luciana Giorgio Cosenzo
Luciana Giorgio Cosenzo Joana Okine
Joana Okine Sharlene D. Newman
Sharlene D. Newman- 1School of Social Work, The University of Alabama, Tuscaloosa, AL, United States
- 2Alabama Life Research Institute, The University of Alabama, Tuscaloosa, AL, United States
Introduction: Disproportionate exposure to psychosocial stressors, such as racial discrimination, and other forms of adversity across the life course contributes to higher rates of hypertension among Black Americans. However, prior literature is limited by the underrepresentation of rural populations and narrow measurements of racial discrimination. This study examines associations between perceived racial discrimination (through a historical trauma lens), childhood adversity, and self-reported high blood pressure among adults living in predominantly Black communities in rural Alabama.
Methods: Data were collected using paper-and-pencil surveys from 184 participants across five rural communities in Alabama in Spring 2023. High blood pressure was assessed via self-report from a list of chronic conditions. Perceived racial discrimination was measured by a 5-item subscale of the African American Historical Trauma Questionnaire. Childhood adversity was measured by the 10-item ACE Study Questionnaire. Binary logistic regression examined associations between high blood pressure, childhood adversity, and perceived racial discrimination, adjusting for psychological distress and sociodemographic factors.
Results: Ninety-two percent of the sample were Black Americans. Older age (OR = 1.09, 95% CI = 1.05, 1.12) and higher perceived racial discrimination scores (OR = 1.15, 95% CI = 1.04, 1.27) were significantly associated with increased odds of high blood pressure.
Discussion: Findings highlight the importance of multilevel interventions that are both trauma-informed and culturally tailored to reduce health disparities in rural Black communities.
Introduction
Hypertension (also referred to as high blood pressure herein) is a public health epidemic both nationally and globally. In the United States (US), approximately half of adults (48.1%) have been diagnosed with hypertension based on the new American College of Cardiology and the American Heart Association defining hypertension as a blood pressure of 130/80 mmHg or above (1, 2). The prevalence of hypertension is highest in rural areas of the US and the Deep South (3, 4). Hypertension rates for the state of Alabama are among the highest in the country (4) where 82% of the counties in the state are classified as rural areas (5). Hypertension has consistently been associated with an increased risk of cardiovascular disease, stroke, and premature death (1, 6, 7). Additionally, individuals with hypertension, on average, experience $2000 more in healthcare expenditures than their non-hypertensive counterparts (8). It has been estimated that hypertension accounts for $131 billion annually in the US (8).
In the US, racial disparities exist in the prevalence of hypertension with Black Americans experiencing a significantly higher prevalence of this condition than White Americans (56% vs. 48%, respectively) (1, 9, 10). Alarmingly, Black Americans have an earlier onset of hypertension and experience greater complications from this condition than their White counterparts (11). The reasons for this disparity are complex however, research suggests that disproportionate exposure to psychosocial stressors, such as racial discrimination, and adversity across the life course contributes to the higher rates of hypertension among Black Americans (12). Chronic exposure to psychosocial stressors can trigger a cascade of physiological responses across multiple systems within the body that regulate stress including the nervous, neuroendocrine, and immune systems (13, 14). When experiencing stress, blood pressure rises in response to the release of hormones (i.e., adrenaline and cortisol) which increase heart rate and narrow the blood vessels to prepare the body to respond to the stressor (15). Repeated activation of this biological stress response can result in failing to return to resting blood pressure levels (12).
Structural racism has resulted in unequal access to the social determinants of health for Black Americans, exposing them to a higher burden of stress than White Americans (16). For example, due to a long history of discriminatory policies that have limited access to economic mobility and intergenerational wealth transfers, Black Americans earn less and have less wealth than White Americans (17). Multiple indicators of socioeconomic status have been linked to hypertension (18). The racial wealth gap limits access to occupational, educational, and social resources that promote health while also limiting the ability to cope with the accumulation of chronic stressors that increase the risk of hypertension (12). In addition, because of persistent racial residential segregation, Black Americans are more likely to reside in high poverty neighborhoods with less green space (19), reduced access to healthy food options (20), and higher crime rates (21). These social determinants of health impact health disparities directly (22) and indirectly by increasing the risk of experiencing adverse childhood experiences (ACEs) (23).
ACEs are traumatic events that occur during the first 18 years of life and include physical, sexual, and emotional abuse, neglect, as well as experiences of household dysfunction such as parental separation or divorce, witnessing intimate partner violence against the mother, and living with an adult experiencing mental illness, substance abuse, or incarceration (24). ACEs are common among adults in the US however, Black Americans experience a greater number of ACEs compared to other racial and ethnic groups (25, 26). A dose-effect relationship has been observed between ACEs and negative outcomes including higher risk of mental and physical health problems (27). Research examining the link between ACEs and hypertension have been limited and findings have produced mixed results. A study analyzing data spanning 10 countries from the World Mental Health Survey found that two or more ACEs was associated with self-reported hypertension (28). Similarly, a study of 12,229 low-income adults in the US also found an association between ACEs and self-reported history of hypertension (29). However, other studies did not observe a relationship (30, 31). The mixed findings have been attributed to inconsistences in how childhood adversity and blood pressure are measured (32).
The traditional ACEs framework has been critiqued for not including racial discrimination as a traumatic event (33). Racial discrimination refers to unfair treatment based on racial identity. It can take various forms including interpersonal interactions or institutional practices that systematically treat certain groups unfavorably (34). Racial discrimination is often perceived as a threat to safety that can trigger intense emotional reactions and possibly lead to race-based traumatic stress (35). Race-based traumatic stress can mimic reactions observed among individuals experiencing Post-Traumatic Stress Disorder including avoidance, hypervigilance, and severe psychological distress (35). Racial discrimination is a distinct type of ACE that also increases the risk for other ACEs and restricts access to the supportive resources needed to help buffer against adverse physical and mental health outcomes (33).
Acts of racial discrimination do not have to be directly experienced to induce race-based traumatic stress for group members. Traumatic events include those that are observed or vicariously experienced (36). Theories of historical trauma suggests that mass level collective experiences of racism across multiple generations can contribute to the adverse physical and mental health functioning of future generations (37). For Black Americans, historical trauma is “the collective spiritual, psychological, emotional, and cognitive distress perpetuated intergenerationally deriving from multiple denigrating experiences originating with slavery and continuing with pattern forms of racism and discrimination to the present day” (p. 32) (38). Historical trauma is transmitted intergenerationally through biological, epigenetic, environmental, social, economic, and political systems (39, 40). In addition, technological advances and the proliferation of social media increases widespread exposure to traumatic events that can lead to vicarious encounters of racism and symptoms of traumatic stress (41).
Evidence of a positive association between racial discrimination and hypertension, specifically among Black Americans, has been increasing over the past two decades (42–44). Although studies have yielded mixed results, most findings suggest racial discrimination partially explains the racial disparities in the prevalence of hypertension seen among Black vs. White Americans. The variance in study results has been attributed to inconsistencies in the measurement of racial discrimination (e.g., everyday discrimination, lifetime discrimination) (42). Results from studies using a lifetime measurement of discrimination have demonstrated more consistently a significant and positive association between racial discrimination and hypertension among Black Americans. For example, a recent study using longitudinal data from the Jackson Heart Study, found that medium to high reports of lifetime racial discrimination were significantly associated with a higher risk of hypertension compared to low lifetime racial discrimination, even when adjusting for hypertension risk factors (45). However, the association between everyday discrimination and hypertension risk was not statistically significant (45). Yet even the lifetime discrimination scale is limited to capturing daily experiences at interpersonal and institutional levels while failing to capture the collective experiences of racial trauma that impact the psyche of Black Americans that a historical trauma framework suggests (46). Other measures of racial discrimination, such as the African American Historical Trauma Questionnaire, can capture perceptions of discrimination originating from the enduring effects of slavery, structural racism, and other traumatic events Black Americans have experienced and that are passed down intergenerationally (46). To date, the association between hypertension and racial discrimination from a historical trauma perspective has not been examined.
The purpose of this study is to examine the association between childhood adversity, perceived racial discrimination, and self-reported high blood pressure among a sample of adults living in predominantly Black communities in rural Alabama. This study adds to the literature in three important ways. First, we use a novel measure of perceived racial discrimination from a historical trauma perspective rather than focusing on direct, everyday experiences of racial discrimination that are typical of research in this area. Second, this study focuses on an underserved, rural population that is often underrepresented in research studies of hypertension (47). This is particularly troubling considering that for the last two decades, mortality rates for hypertension have consistently been highest among Black adults living in rural parts of the United States (48). Lastly, our study controls for childhood adversity and psychological distress which can confound the association between perceived racial discrimination and hypertension and are often not included as variables in prior research.
Materials and methods
Study population and design
The data collection for this cross-sectional study was a part of an ongoing research collaboration between the University and five rural, predominately Black communities in the Alabama Black Belt Region. Originally named for its fertile soil, the Black Belt region has a long history of racial and economic injustice dating back to chattel slavery and the Jim Crow era. The region is home to some of the poorest counties in the country and experiences the worst health outcomes in Alabama (49, 50). The goal of the research collaboration is to use community-based participatory approaches to improve the health outcomes of these communities [for a more detailed discussion of the community-academic partnership see Newman et al. (51)]. Using a convenience sampling strategy, community representatives recruited participants at community events, local stores, government offices, and churches. One hundred and eighty-four participants completed the 34-item survey at community sites in the Spring of 2023. This study was approved by the Institutional Review Board of the University of Alabama.
Measures
Dependent variable
Participants reported whether they had high blood pressure by selecting from a list of chronic health conditions. High blood pressure was measured as a dichotomized variable (0 = no, 1 = yes).
Sociodemographic characteristics
Age, gender, education, and marital status were included as covariates in this study. Age was measured in years as a continuous variable. Participants were asked, “How many years of school have you completed?” and response options included: less than high school, high school graduate, some college, associate degree, bachelor’s degree, and graduate degree or higher. The variable was recoded into a dichotomous variable due to low observations in multiple categories (0 = high school graduate or less, 1 = some college or higher). Gender (0 = male, 1 = female) and marital status (0 = not married, 1 = married) were also analyzed as dichotomous variables.
Childhood adversity
Childhood adversity was measured by the ACE Study Questionnaire (24). This 10-item questionnaire asks participants to indicate (yes/no) if they had experienced abuse or other household dysfunction during the first 18 years of life. The categories of abuse include emotional abuse, emotional neglect, physical neglect, physical abuse, and sexual abuse. The categories of household dysfunction include exposure to substance use, mental illness, intimate partner violence against the mother or stepmother, and the incarceration of a household member. An ACE score was derived for each participant by summing the number of yes responses to the questions.
Perceived racial discrimination
Perceived racial discrimination was measured by a subscale of the African American Historical Trauma Questionnaire (46). Using a 4-point Likert scale (ranging from 0 = never to 3 = always), this 5-item measure asks participants to indicate: (1) “How often do you believe life is an uphill battle?” (2) “How often do you believe you are constantly being held back?” (3) “How often do you believe African Americans typically endure unnecessary hardship due to race?” (4) “How often do you believe the world is against you just because you are African American?” (5) “How often do you believe it is necessary to work twice as hard to succeed as an African American?” Responses to the items were summed to create a perceived racial discrimination score ranging from 0 to 15 (Cronbach’s alpha = 0.92).
Psychological distress
Psychological distress was assessed using the Patient Health Questionnaire for Depression and Anxiety (PHQ-4) (52). This 4-item measure assesses symptoms of depression and anxiety (e.g., feeling nervous on edge, feeling down or hopeless) using a 4-point Likert scale with response options ranging from 0 = never to 3 = nearly every day. Responses to the items were summed to create a psychological distress score ranging from 0 to 12 (Cronbach’s alpha = 0.93).
Analytic strategy
Before conducting analyses, data were screened for missing values. Percent missing among the variables ranged from 0 to 14.1%. Variables with more than 10% missing were recoded with missing values coded as 1 and all other values coded as 0. Bivariate analyses were performed between the recoded variables and all other variables to determine if relationships were present. Effect sizes did not exceed 0.5, indicating that no patterns were present, and the data were missing at random. Thus, the pairwise deletion method was applied for missing data.
Descriptive analyses for all variables were conducted to analyze the characteristics of the sample. Bivariate analyses were conducted to assess the relationships between self-reported high blood pressure and independent variables using independent sample t-test for continuous independent variables and chi squares for dichotomous independent variables. Binary logistic regression was used to examine the relationship between self-reported high blood pressure, childhood adversity, and perceived racial discrimination while controlling for psychological distress and sociodemographic characteristics. Data analyses were performed using IBM SPSS Version 27.
Results
Descriptive and bivariate analyses
Descriptive and bivariate analyses are presented in Table 1. About 63% of the sample reported high blood pressure. The mean ACE score was 1.89 (SD = 2.32). Figure 1 displays the percentage of participants by total ACE score. Figure 2 illustrates the prevalence of each type of ACE reported by participants. The mean discrimination score was 8.81 (SD = 4.76). The mean psychological distress score was 1.7 (SD = 2.60) with about 10% of the sample experiencing moderate to severe psychological distress. The mean age was 50.63 (SD = 18.58). About 92% of the sample was Black/African American. Most participants were women (57.6%), unmarried (51.6%), and did not have any college experience (79.6%).
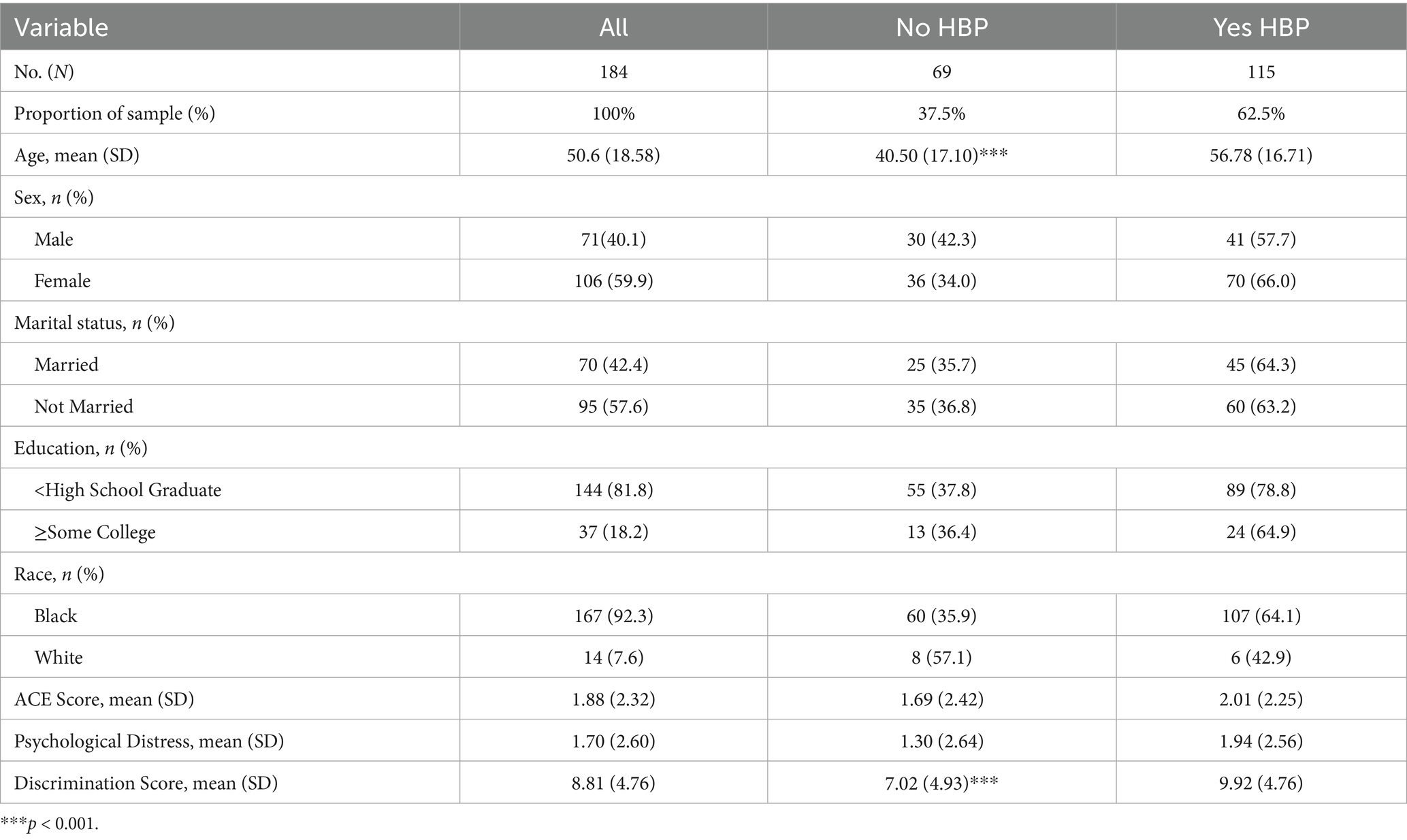
Table 1. Descriptive characteristics by high blood pressure status.
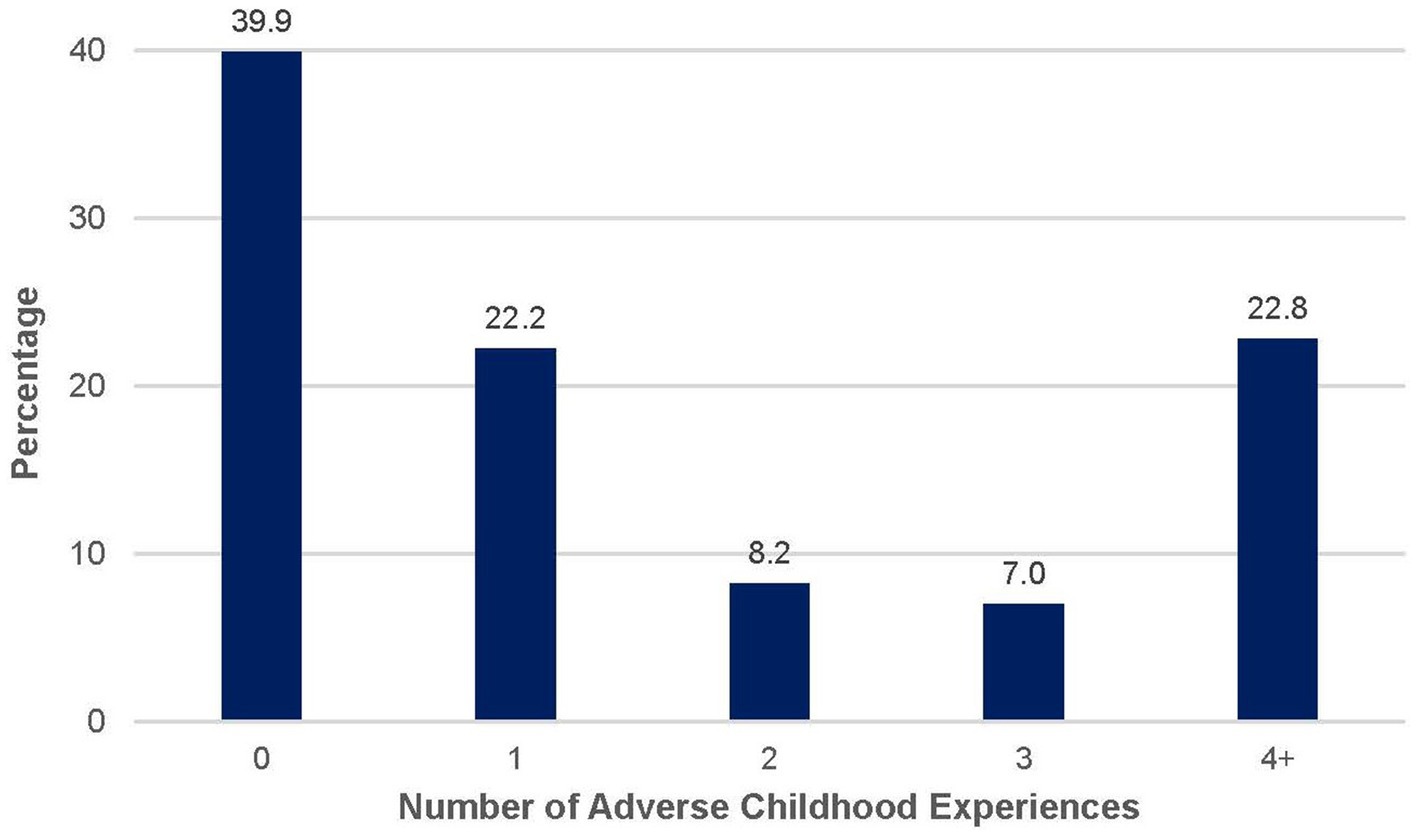
Figure 1. Total number of adverse childhood experiences reported by participants. Bar graph displaying the percentage of participants (N = 184) by total ACE score. Percentages are based on valid responses; sample size may vary slightly across items due to missing data.
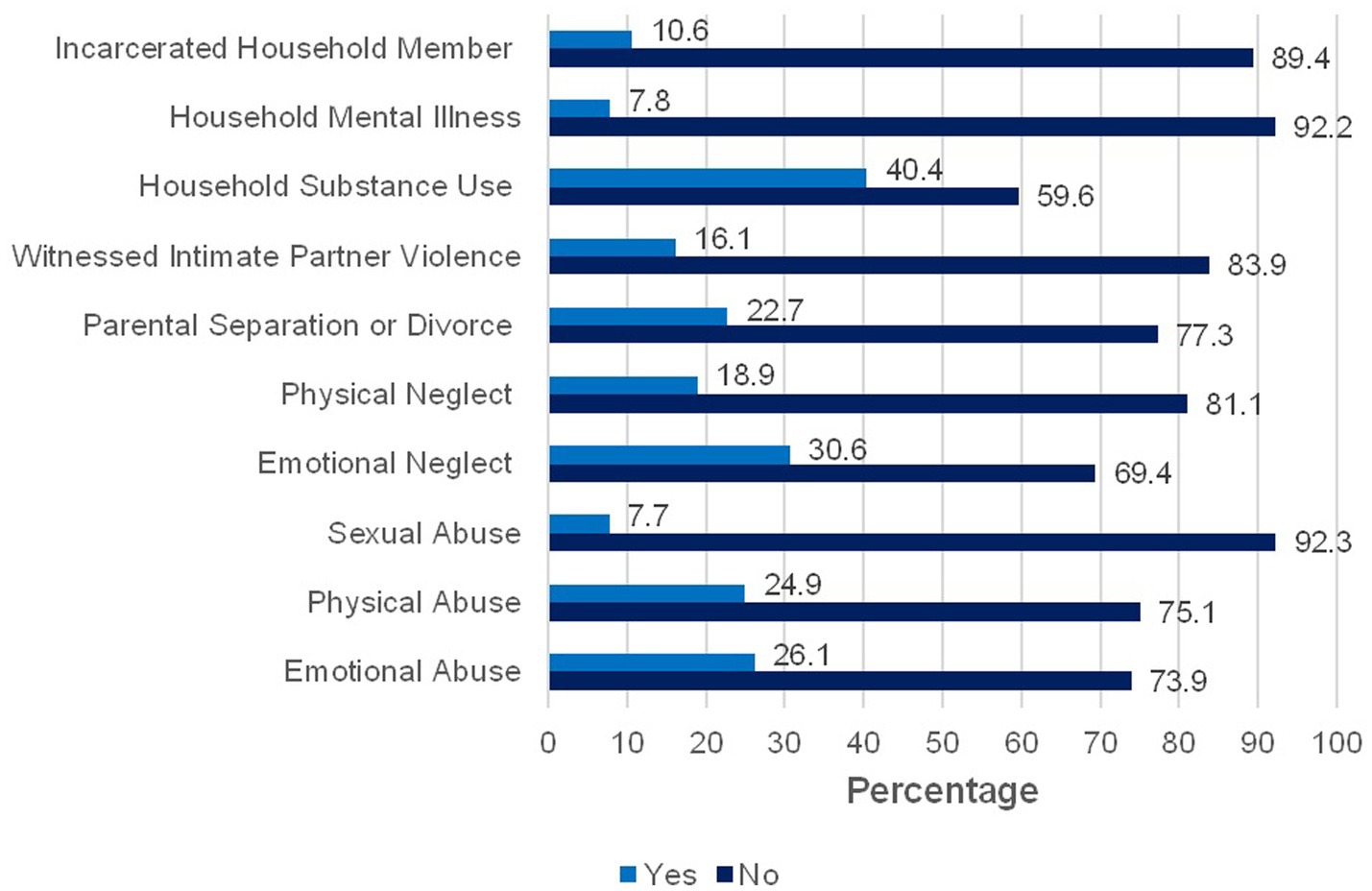
Figure 2. Prevalence of each adverse childhood experience in the study sample. Bar chart displaying the percentage of participants (N = 184) who reported experiencing each type of adverse childhood experience. Percentages are based on valid responses; sample size may vary slightly across items due to missing data.
At the bivariate level, participants with high blood pressure endorsed higher levels of perceived racial discrimination, t(170) = −4.074, p = 0.000. Participants with high blood pressure were also older on average than participants who did not report high blood pressure, t(178) = −6.282, p = 0.000. The other variables were not associated with high blood pressure.
Binary logistic regression
The results of the binary logistic regression are presented in Table 2. Older age (OR = 1.09, 95% CI = 1.05, 1.13) and higher perceived racial discrimination scores were associated with higher odds of high blood pressure (OR = 1.15, 95% CI = 1.04, 1.27). ACE score was not associated with high blood pressure. All variance inflation factor (VIF) values were close to 1, indicating that multicollinearity was not a concern. The model demonstrated good fit (Hosmer–Lemeshow χ2 = 10.25, p = 0.25) and strong discriminatory ability (AUC = 0.847), indicating high accuracy in distinguishing individuals with and without self-reported high blood pressure. The model also explained 44.7% of the variance in the dependent variable (Nagelkerke R2 = 0.447).
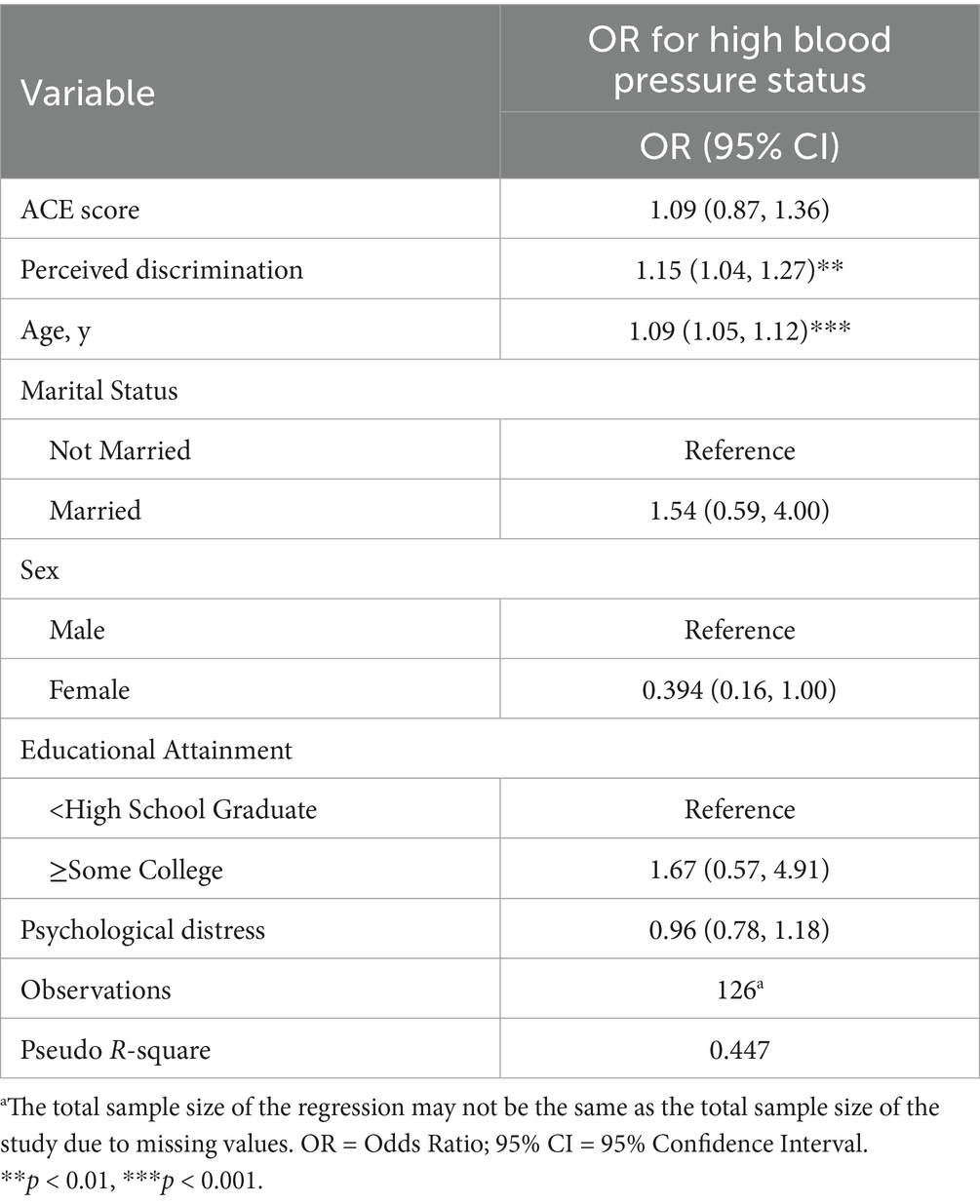
Table 2. Logistic regression analysis of childhood adversity, perceived racial discrimination, and high blood pressure status (N = 184a).
Discussion
This study examined the relationship between perceived racial discrimination, childhood adversity, and self-reported high blood pressure among a sample of adults from rural, majority Black communities in Alabama. This study sought to address important gaps in the literature by examining high blood pressure risk among adults in under-resourced communities in the rural Deep South utilizing a historical trauma lens to conceptualize perceived racial discrimination while controlling for psychological distress and childhood adversity. Older age and higher levels of perceived discrimination were associated with higher odds of high blood pressure.
The prevalence of high blood pressure in the sample was seven percentage points above the national average for Black Americans (3). The higher rates are likely attributed to characteristics of the sample and the study location. The Deep South has consistently had the highest prevalence of hypertension in the United States with Alabama having rates among the highest in the country (3). Second, the sample overall is older, with half of participants at age 50 or older. Rates of chronic diseases including high blood pressure tend to increase with age (53) which is consistent with our finding that higher age was associated with increased odds of high blood pressure.
High levels of perceived racial discrimination were present among participants in the sample. The legacy of chattel slavery and Jim Crow still shapes the social and economic context of communities in the Deep South negatively impacting intergenerational mobility in the region (54, 55). Rather than focus on direct, individual experiences of discrimination, our broad measure captures generalized perceptions of disparate treatment and lower quality of life because of racial identity that aligns with a historical trauma perspective. Consistent with some prior research using conventional measures of racial discrimination, higher levels of perceived racial discrimination were associated with increased odds of high blood pressure in our study. For example, everyday racial discrimination was associated with increased odds of self-reported hypertension among Black women with higher levels of education (56). Similarly, a longitudinal study of a multi-ethnic cohort of 3,297 adults found that lifetime discrimination was associated with incident hypertension among Black Americans in the sample (57). Research suggests that two possible pathways link perceived racial discrimination to increased risk of high blood pressure. First, race-based traumatic stress can trigger repeated activation of the stress response leading to physiological changes in the body, including difficulty returning to resting levels of blood pressure. The weathering hypothesis suggests that chronic stress and other accumulated disadvantages over the life course can lead to premature biological aging and health disparities among Black Americans (58, 59). Second, the psychological impact of perceived racial discrimination can contribute to difficulty engaging in health promoting behaviors due to unhealthy coping strategies (60).
ACEs were also common among participants. Sixty percent of the sample experienced at least one ACE which is fairly consistent with national estimates (61). About a quarter of the sample experienced four or more ACEs which is higher than national estimates indicating that 17% of the general population has experienced four or more ACEs (61). The greater likelihood of experiencing multiple ACEs in the sample is consistent with prior research that has found a higher prevalence of ACEs among Black Americans (25, 26). These disparities in ACEs prevalence have been attributed to the inequitable social and economic contexts that Black families disproportionately experience.
Consistent with some prior research, the number of ACEs was not associated with high blood pressure. For example, a population level cohort study of US middle aged adults did not find a direct association between ACEs and self-reported hypertension (30). Similarly, a study of childhood adversity and hypertension among mostly midlife women found no direct association (31). Like our study, these studies included mostly middle aged and older adults, which may partially explain the null findings. Research suggests that developmental timing may be important for detecting differences in risk of high blood pressure related to ACEs. For example, Su et al. (62) examined the long-term effect of ACEs on blood pressure trajectories from childhood to young adulthood and found a statistically significant association between the number of ACEs and longitudinal blood pressure trajectories such that the effect sizes increased as the participants aged into young adulthood. Similarly, among a sample of 45,482 participants ranging in age from 18 to 99 years, a dose effect of ACEs on hypertension risk was most pronounced among the younger adults (63). Thus, the risk associated with developing high blood pressure may be elevated at earlier ages for those with a history of ACEs compared to those without a history (62). In addition, as noted previously, the traditional ACEs framework does not include racial discrimination which may lead to an underestimation of childhood adversity within this sample and contribute to the null findings. Moreover, the traditional ACEs framework focuses solely on household-level dysfunction and fails to account for the community-level adversities (e.g., concentrated poverty, failing schools) that can impact health and wellbeing over time. This limitation is particularly relevant for the Black Belt region where communities face significant structural inequities.
Limitations and directions for future research
This exploratory study adds to the relatively scarce literature examining factors that may be associated with high blood pressure among Black Americans in rural, under-resourced communities, however there are several noteworthy limitations. First, this study is cross-sectional. Thus, causation and the temporal direction of the relationships observed in this study cannot be ascertained. Future studies should incorporate longitudinal research designs with larger samples from these communities. Second, the sample was convenient and thus not representative of the population, limiting the generalizability of our findings. Third, our measure of high blood pressure is self-reported as clinical measures of blood pressure were not collected. While self-reported high blood pressure has demonstrated reasonable concordance with clinical measurements in large scale epidemiological studies (64), it may introduce recall bias or risk of misclassification. Similarly, our study did not collect other biomarker data such as body mass index, or other hypertension risk factors like smoking status or physical activity. However, it is important to note that prior research has found a statistically significant relationship between racial discrimination and hypertension when controlling for these risk factors (42, 54). Fourth, psychological distress was included as a control variable to account for potential confounding. However, as a possible mediator between perceived racial discrimination and high blood pressure, its inclusion could introduce overadjustment bias and attenuate observed associations. Lastly, our use of the African American Historical Trauma Questionnaire is exploratory, and additional research is needed to examine its association with health outcomes among Black Americans.
Implications for public health interventions
Public health efforts to address health disparities in rural Black communities should utilize multilevel strategies that include community-based participatory approaches to engage community members in identifying community needs and developing culturally relevant solutions. First, it is critical to address the social drivers of health and rectify systemic inequities in health care infrastructure, housing, and transportation through targeted policy investments in rural Black communities. These systemic barriers make it difficult for people to adopt the lifestyle modifications that help reduce risk of hypertension. At the micro level, trauma-informed primary care (TIPC) models should be implemented in rural Black communities. TIPC involves screening for patient trauma history (including race-based traumatic stress), educating patients about the effect of stress on health, emphasizing cultural strengths in managing health, and making appropriate referrals for mental health care (65). In addition, programs like Mental Health First Aid teaches laypersons in the community how to identify, understand, and respond to signs of mental illness and substance abuse (66). MHA has shown promise in raising awareness of behavioral health issues and reducing stigma in rural communities (66). MHA also aligns with the tradition of mutual aid among Black Americans and the strong informal networks of support present in many rural communities (67). Lastly, public health interventions should include efforts to help communities heal from racial trauma through the use of expressive arts such as storytelling to create counternarratives that emphasize collective strength and affirm the dignity and worth of Black identity (39, 68). The reframing of harmful narratives can help empower Black communities to increase individual agency and spur collective social action to improve the health and wellbeing of the community.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Alabama Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
TL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. LC: Writing – original draft, Writing – review & editing. JO: Writing – original draft, Writing – review & editing. SN: Conceptualization, Funding acquisition, Investigation, Project administration, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project was supported by the Office of Minority Health of the U. S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $2.9 M with 100 percent funded by HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HHS, or the U. S. Government. For more information, please visit https://www.minorityhealth.hhs.gov/.
Acknowledgments
We would like to thank Kimberly Moss, Melonie Pichon, and Deborah Scott for their support in collecting the data and the parents and children who participated.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. CDC, “Facts about hypertension | cdc.Gov,” Ctr Dis Control Prev. Available online at: https://www.cdc.gov/bloodpressure/facts.htm (accessed October 03, 2023)
2. Whelton, PK, Carey, RM, Aronow, WS, Casey, DE, Collins, KJ, Dennison Himmelfarb, C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Hypertension. (2018) 71:1269–324. doi: 10.1161/HYP.0000000000000066
3. CDC, “Facts about hypertension | cdc.Gov,” Centers for Disease Control and Prevention. Available online at: https://www.cdc.gov/bloodpressure/facts.htm (accessed September 01, 2023)
4. Explore high blood pressure in Alabama | AHR. America’s health rankings. Available online at: https://www.americashealthrankings.org/explore/measures/hypertension/AL (accessed: July 27, 2023)
5. Analysis of Urban vs. rural, Alabama rural health association. Available online at: https://arhaonline.org/analysis-of-urban-vs-rural/ (accessed March 29, 2024)
6. Chobanian, AV, Bakris, GL, Black, HR, Cushman, WC, Green, LA, Izzo, JL, et al. The seventh report of the joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. (2003) 289:2560–72. doi: 10.1001/jama.289.19.2560
7. O’donnell, MJ, Xavier, D, Liu, L, Zhang, H, Chin, SL, Rao-Melacini, P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. (2010) 376:112–23. doi: 10.1016/S0140-6736(10)60834-3
8. Kirkland, EB, Heincelman, M, Bishu, KG, Schumann, SO, Schreiner, A, Axon, RN, et al. Trends in healthcare expenditures among US adults with hypertension: National Estimates, 2003–2014. J Am Heart Assoc. (2018) 7:e008731. doi: 10.1161/JAHA.118.008731
9. Dorans, KS, Mills, KT, Liu, Y, and He, J. Trends in prevalence and control of hypertension according to the 2017 American College of Cardiology/American Heart Association (ACC/AHA) guideline. J Am Heart Assoc. (2018) 7:e008888. doi: 10.1161/JAHA.118.008888
10. Ogunniyi, MO, Commodore, MY, and Ferdinand, KC. Race, ethnicity, hypertension, and heart disease. J Am Coll Cardiol. (2021) 78:2460–70. doi: 10.1016/j.jacc.2021.06.017
11. Ferdinand, KC, and Townsend, RR. Hypertension in the US Black population: risk factors, complications, and potential impact of central aortic pressure on effective treatment. Cardiovasc Drugs Ther. (2012) 26:157–65. doi: 10.1007/s10557-011-6367-8
12. Cuevas, AG, Williams, DR, and Albert, MA. Psychosocial factors and hypertension: a review of the literature. Cardiol Clin. (2017) 35:223–30. doi: 10.1016/j.ccl.2016.12.004
13. Black, PH, and Garbutt, LD. Stress, inflammation and cardiovascular disease. J Psychosom Res. (2002) 52:1–23. doi: 10.1016/S0022-3999(01)00302-6
14. Spruill, TM. Chronic psychosocial stress and hypertension. Current Science Inc. (2010) 12:10–6. doi: 10.1007/s11906-009-0084-8
15. Curtis, BM, and O’Keefe, JH. Autonomic tone as a cardiovascular risk factor: the dangers of chronic fight or flight. Mayo Clin Proc. (2002) 77:45–54. doi: 10.4065/77.1.45
16. Myers, HF. Ethnicity- and socio-economic status-related stresses in context: an integrative review and conceptual model. J Behav Med. (2009) 32:9–19. doi: 10.1007/s10865-008-9181-4
17. Aladangady, A., and Forde, A. Wealth inequality and the racial wealth gap. (2021). Available online at: https://www.federalreserve.gov/econres/notes/feds-notes/wealth-inequality-and-the-racial-wealth-gap-20211022.html (accessed January 30, 2025)
18. Leng, B, Jin, Y, Li, G, Chen, L, and Jin, N. Socioeconomic status and hypertension: a meta-analysis. J Hypertens. (2015) 33:221. doi: 10.1097/HJH.0000000000000428
19. Casey, JA, James, P, Cushing, L, Jesdale, BM, and Morello-Frosch, R. Race, ethnicity, income concentration and 10-year change in urban greenness in the United States. Int J Environ Res Public Health. (2017) 14:1546. doi: 10.3390/ijerph14121546
20. Bower, KM, Thorpe, RJ, Rohde, C, and Gaskin, DJ. The intersection of neighborhood racial segregation, poverty, and urbanicity and its impact on food store availability in the United States. Prev Med. (2014) 58:33–9. doi: 10.1016/j.ypmed.2013.10.010
21. Krivo, LJ, Peterson, RD, and Kuhl, DC. Segregation, racial structure, and neighborhood violent crime. Am J Sociol. (2009) 114:1765–802. doi: 10.1086/597285
22. Kramer, MR, and Hogue, CR. Is segregation bad for your health? Epidemiol Rev. (2009) 31:178–94. doi: 10.1093/epirev/mxp001
23. Maguire-Jack, K, Font, S, Dillard, R, Dvalishvili, D, and Barnhart, S. Neighborhood poverty and adverse childhood experiences over the first 15 years of life. Int Journal on Child Malt. (2021) 4, 93–114. doi: 10.1007/s42448-021-00072-y
24. Felitti, VJ, Anda, RF, Nordenberg, D, Williamson, DF, Spitz, AM, Edwards, V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/S0749-3797(98)00017-8
25. Slopen, N, Shonkoff, JP, Albert, MA, Yoshikawa, H, Jacobs, A, Stoltz, R, et al. Racial disparities in child adversity in the U.S. Am J Prev Med. (2016) 50:47–56. doi: 10.1016/j.amepre.2015.06.013
26. Merrick, MT, Ford, DC, Ports, KA, and Guinn, AS. Prevalence of adverse childhood experiences from the 2011-2014 behavioral risk factor surveillance system in 23 states. JAMA Pediatr. (2018) 172:1038–44. doi: 10.1001/jamapediatrics.2018.2537
27. Petruccelli, K, Davis, J, and Berman, T. Adverse childhood experiences and associated health outcomes: a systematic review and meta-analysis. Child Abuse Negl. (2019) 97:104127. doi: 10.1016/j.chiabu.2019.104127
28. Stein, DJ, Scott, K, Haro Abad, JM, Aguilar-Gaxiola, S, Alonso, J, Angermeyer, M, et al. Early childhood adversity and later hypertension: data from the world mental health survey. Ann Clin Psychiatry. (2010) 22:19–28. doi: 10.1177/104012371002200104
29. Allen, H, Wright, BJ, Vartanian, K, Dulacki, K, and Li, H-F. Examining the prevalence of adverse childhood experiences and associated cardiovascular disease risk factors among low-income uninsured adults. Circ Cardiovasc Qual Outcomes. (2019) 12:e004391. doi: 10.1161/CIRCOUTCOMES.117.004391
30. Matthews, TA, Zhu, Y, Robbins, W, Rezk-Hanna, M, Macey, PM, Song, Y, et al. Adulthood psychosocial disadvantages and risk of hypertension in U.S. workers: effect modification by adverse childhood experiences. Life. (2022) 12:1507. doi: 10.3390/life12101507
31. Cubbin, C, Kim, Y, and Panisch, LS. Familial childhood adversity is associated with chronic disease among women: data from the geographic research on wellbeing (GROW) study. Matern Child Health J. (2019) 23:1117–29. doi: 10.1007/s10995-019-02758-9
32. Scott, J, McMillian-Bohler, J, Johnson, R, and Simmons, LA. Adverse childhood experiences and blood pressure in women in the United States: a systematic review. J Midwifery Womens Health. (2021) 66:78–87. doi: 10.1111/jmwh.13213
33. Bernard, DL, Calhoun, CD, Banks, DE, Halliday, CA, Hughes-Halbert, C, and Danielson, CK. Making the ‘C-ACE’ for a culturally-informed adverse childhood experiences framework to understand the pervasive mental health impact of racism on Black youth. J Child Adolesc Trauma. (2020) 14:233–47. doi: 10.1007/s40653-020-00319-9
34. Lockwood, KG, Marsland, AL, Matthews, KA, and Gianaros, PJ. Perceived discrimination and cardiovascular health disparities: a multisystem review and health neuroscience perspective. Ann N Y Acad Sci. (2018) 1428:170–207. doi: 10.1111/nyas.13939
35. Carter, RT, Mazzula, S, Victoria, R, Vazquez, R, Hall, S, Smith, S, et al. Initial development of the race-based traumatic stress symptom scale: assessing the emotional impact of racism. Psychol Trauma Theory Res Pract Policy. (2013) 5:1–9. doi: 10.1037/a0025911
36. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington (VA): American Psychiatric Publishing (2013).
37. Heart, MYHB. The historical trauma response among natives and its relationship with substance abuse: a Lakota illustration. J Psychoactive Drugs. (2003) 35:7–13. doi: 10.1080/02791072.2003.10399988
38. Hampton, RL, Gullotta, TP, and Crowel, RL. Handbook of African American health In: Handbook of African American health. New York, NY, US: The Guilford Press (2010). 612.
39. Ortega-Williams, A, Beltrán, R, Schultz, K, Ru-Glo Henderson, Z, Colón, L, and Teyra, C. An integrated historical trauma and posttraumatic growth framework: a cross-cultural exploration. J Trauma Dissociation. (2021) 22:220–40. doi: 10.1080/15299732.2020.1869106
40. Yehuda, R, and Lehrner, A. Intergenerational transmission of trauma effects: putative role of epigenetic mechanisms. World Psychiatry. (2018) 17:243–57. doi: 10.1002/wps.20568
41. Tynes, BM, Willis, HA, Stewart, AM, and Hamilton, MW. Race-related traumatic events online and mental health among adolescents of color. J Adolesc Health. (2019) 65:371–7. doi: 10.1016/j.jadohealth.2019.03.006
42. Dolezsar, CM, McGrath, JJ, Herzig, AJM, and Miller, SB. Perceived racial discrimination and hypertension: a comprehensive systematic review. Health Psychol. (2014) 33:20–34. doi: 10.1037/a0033718
43. Williams, DR, and Mohammed, SA. Discrimination and racial disparities in health: evidence and needed research. J Behav Med. (2009) 32:20–47. doi: 10.1007/s10865-008-9185-0
44. Brondolo, E, Love, EE, Pencille, M, Schoenthaler, A, and Ogedegbe, G. Racism and hypertension: a review of the empirical evidence and implications for clinical practice. Am J Hypertens. (2011) 24:518–29. doi: 10.1038/ajh.2011.9
45. Forde, AT, Sims, M, Muntner, P, Lewis, T, Onwuka, A, Moore, K, et al. Discrimination and hypertension risk among African Americans in the Jackson Heart study. Hypertension. (2020) 76:715–23. doi: 10.1161/HYPERTENSIONAHA.119.14492
46. Williams-Washington, KN, and Mills, CP. African American historical trauma: creating an inclusive measure. J Multicult Counsel Dev. (2018) 46:246–63. doi: 10.1002/jmcd.12113
47. Harrington, RA, Califf, RM, Balamurugan, A, Brown, N, Benjamin, RM, Braund, WE, et al. Call to action: rural health: a presidential advisory from the American Heart Association and American Stroke Association. Circulation. (2020) 141:e615–44. doi: 10.1161/CIR.0000000000000753
48. Aggarwal, R, Chiu, N, Loccoh, EC, Kazi, DS, Yeh, RW, and Wadhera, RK. Rural-urban disparities. J Am Coll Cardiol. (2021) 77:1480–1. doi: 10.1016/j.jacc.2021.01.032
49. Katsinas, S. G., Till, G., Corley, E. G., O’Brien, S., Courchesne, E., and Bray, N., Poverty, housing, and GDP in Alabama’s Black Belt. Tuscaloosa, AL: Education Policy Center; The University of Alabama.
50. Alabama | County health rankings and roadmaps. Available online at: https://www.countyhealthrankings.org/health-data/alabama (accessed: January 30, 2025)
51. Newman, SD, Moss, K, Pichon, M, Scott, D, Rogers, K, Orr, A, et al. The health of rural Black communities during COVID: some affirmations, some surprises. Front Public Health. (2023) 11:2451. doi: 10.3389/fpubh.2023.932451
52. Kroenke, K, Spitzer, RL, Williams, JBW, and Löwe, B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. (2009) 50:613–21. doi: 10.1176/appi.psy.50.6.613
53. Oliveros, E, Patel, H, Kyung, S, Fugar, S, Goldberg, A, Madan, N, et al. Hypertension in older adults: assessment, management, and challenges. Clin Cardiol. (2020) 43:99–107. doi: 10.1002/clc.23303
54. Berger, T. Places of persistence: slavery and the geography of intergenerational mobility in the United States. Demography. (2018) 55:1547–65. doi: 10.1007/s13524-018-0693-4
55. Baker, RS. The historical racial regime and racial inequality in poverty in the American south. Am J Sociol. (2022) 127:1721–81. doi: 10.1086/719653
56. Gaston, SA, Forde, AT, Green, M, Sandler, DP, and Jackson, CL. Racial and ethnic discrimination and hypertension by educational attainment among a cohort of US women. JAMA Netw Open. (2023) 6:e2344707. doi: 10.1001/jamanetworkopen.2023.44707
57. Forde, AT, Lewis, TT, Kershaw, KN, Bellamy, SL, and Diez Roux, AV. Perceived discrimination and hypertension risk among participants in the multi-ethnic study of atherosclerosis. J Am Heart Assoc. (2021) 10:e019541. doi: 10.1161/JAHA.120.019541
58. Geronimus, AT, Hicken, M, Keene, D, and Bound, J. ‘Weathering’ and age patterns of Allostatic load scores among blacks and whites in the United States. Am J Public Health. (2006) 96:826–33. doi: 10.2105/AJPH.2004.060749
59. Forde, AT, Crookes, DM, Suglia, SF, and Demmer, RT. The weathering hypothesis as an explanation for racial disparities in health: a systematic review. Ann Epidemiol. (2019) 33:1–18.e3. doi: 10.1016/j.annepidem.2019.02.011
60. Sims, M, Diez-Roux, AV, Gebreab, SY, Brenner, A, Dubbert, P, Wyatt, S, et al. Perceived discrimination is associated with health behaviours among African-Americans in the Jackson Heart study. J Epidemiol Community Health. (2016) 70:187–94. doi: 10.1136/jech-2015-206390
61. Swedo, EA, Aslam, MV, Dahlberg, LL, Niolon, PH, Guinn, AS, Simon, TR, et al. Prevalence of adverse childhood experiences among U.S. adults — behavioral risk factor surveillance system, 2011–2020. MMWR Morb Mortal Wkly Rep. (2023) 72:707–15. doi: 10.15585/mmwr.mm7226a2
62. Su, S, Wang, X, Pollock, JS, Treiber, FA, Xu, X, Snieder, H, et al. Adverse childhood experiences and blood pressure trajectories from childhood to young adulthood. Circulation. (2015) 131:1674–81. doi: 10.1161/CIRCULATIONAHA.114.013104
63. Kreatsoulas, C, Fleegler, EW, Kubzansky, LD, McGorrian, CM, and Subramanian, SV. Young adults and adverse childhood events: a potent measure of cardiovascular risk. Am J Med. (2019) 132:605–13. doi: 10.1016/j.amjmed.2018.12.022
64. Okura, Y, Urban, LH, Mahoney, DW, Jacobsen, SJ, and Rodeheffer, RJ. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol. (2004) 57:1096–103. doi: 10.1016/j.jclinepi.2004.04.005
65. Roberts, SJ, Chandler, GE, and Kalmakis, K. A model for trauma-informed primary care. J Am Assoc Nurse Pract. (2019) 31:139–44. doi: 10.1097/JXX.0000000000000116
66. Talbot, JA, Ziller, EC, and Szlosek, DA. Mental health first aid in rural communities: appropriateness and outcomes. J Rural Health. (2017) 33:82–91. doi: 10.1111/jrh.12173
67. Seiling, SB, Manoogian, MM, and Son, S. ‘I Don’t know how we would make it’—social support in rural low-income families, in rural families and work: context and problems In: JW Bauer and EM Dolan, editors. International series on consumer science. New York, NY: Springer (2011). 157–83.
Keywords: hypertension, racial discrimination, childhood adversity, trauma, rural populations, health disparities
Citation: Littleton T, Cosenzo LG, Okine J and Newman SD (2025) Perceived racial discrimination, childhood adversity, and self-reported high blood pressure among adults in rural Alabama. Front. Public Health. 13:1575793. doi: 10.3389/fpubh.2025.1575793
Edited by:
Cyrille Delpierre, INSERM Public Health, FranceReviewed by:
Milad Mohkam, Shiraz University of Medical Sciences, IranBruno Špiljak, University of Zagreb, Croatia
Copyright © 2025 Littleton, Cosenzo, Okine and Newman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tenesha Littleton, dGxpdHRsZXRvbkB1YS5lZHU=