 Daniel Schröder1†Sumire Sorano2,3†Elena Shipitsyna1,4Enesia Banda Chaponda5
Daniel Schröder1†Sumire Sorano2,3†Elena Shipitsyna1,4Enesia Banda Chaponda5 Daniel Golparian1Ephraim Chikwanda6Vivian Mwewa7Joyce M. Mulenga6Mike Chaponda6Chris Smith2,3Matsui Mitsuaki3,8Massimo Mirandola9Karel Blondeel10,11Igor Toskin11
Daniel Golparian1Ephraim Chikwanda6Vivian Mwewa7Joyce M. Mulenga6Mike Chaponda6Chris Smith2,3Matsui Mitsuaki3,8Massimo Mirandola9Karel Blondeel10,11Igor Toskin11 R. Matthew Chico2
R. Matthew Chico2 Magnus Unemo1,12*
Magnus Unemo1,12*- 1Department of Laboratory Medicine, Faculty of Medicine and Health, WHO Collaborating Centre for Gonorrhoea and Other STIs, Örebro University, Örebro, Sweden
- 2Faculty of Infectious and Tropical Diseases, London School of Hygiene & Tropical Medicine, London, United Kingdom
- 3School of Tropical Medicine and Global Health, Nagasaki University, Nagasaki, Japan
- 4Department of Medical Microbiology, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductive Medicine, St. Petersburg, Russia
- 5Department of Biological Sciences, University of Zambia, Lusaka, Zambia
- 6Tropical Diseases Research Centre, Ndola, Zambia
- 7St. Paul’s Mission Hospital, Nchelenge, Zambia
- 8Division of Global Health, Department of Public Health, Graduate School of Health Sciences, Kobe University, Kobe, Japan
- 9Department of Diagnostics and Public Health, University of Verona, Verona, Italy
- 10Faculty of Medicine and Health Sciences, Ghent University, Ghent, Belgium
- 11Department of Sexual and Reproductive Health and Research, World Health Organization, Geneva, Switzerland
- 12Institute for Global Health, University College London (UCL), London, United Kingdom
Introduction: Mycoplasma genitalium (MG) is a sexually transmitted bacterium of public health importance, associated with genitourinary disorders, and adverse reproductive and perinatal outcomes. Global data on MG prevalence and antimicrobial resistance (AMR) are primarily available from high-income countries, whereas there is a dearth of information from resource-constrained settings including sub-Saharan Africa. Furthermore, international data on MG rates and AMR in the antenatal population are scarce. Understanding MG prevalence and AMR patterns is crucial for developing effective public health strategies and treatment guidelines. The aim of this study was to investigate the prevalence and epidemiology of MG and the presence of macrolide resistance-associated mutations (MRAMs) among pregnant women attending antenatal care facilities in Zambia.
Methods: A cross-sectional study was conducted at four antenatal care facilities in Nchelenge, Zambia, among 1,021 pregnant women. Vaginal swabs were collected and tested using the Aptima Mycoplasma genitalium assay, Aptima Combo 2 assay and Aptima Trichomonas vaginalis assay on the Panther System (Hologic). MG-positive samples were further analyzed for MRAMs using the ResistancePlus™ MG assay (SpeeDx).
Results: The prevalence of MG was 12.6% (127 of 1,005 valid samples) among the pregnant women. Only 12 MG-positive women (9.4%) had symptoms of a genitourinary infection, which was similar to the frequency of genitourinary symptoms among MG-negative women (6.1%). The rates of Chlamydia trachomatis, Neisseria gonorrhoeae, T. vaginalis, and HIV seropositivity were 7.4, 8.3, 23.0, and 8.6%, respectively. MG infection was significantly associated with the presence of all other tested sexually transmitted infections and HIV seropositivity: the detection rates of C. trachomatis, N. gonorrhoeae, T. vaginalis, and HIV seropositivity were significantly higher in MG-positive than in MG-negative women (15.1% vs. 6.2, 15.0% vs. 7.5, 32.3% vs. 22.0, and 14.3% vs. 7.5%, respectively). The ResistancePlus™ MG assay detected MG in 66.1% (84/127) of samples positive by the Aptima M. genitalium assay, however, no MRAMs were detected in the 23S rRNA gene for any of these 84 samples.
Discussion: This study emphasizes the high prevalence of MG among pregnant women in Zambia, but also lack of MRAMs in MG. These findings suggest that azithromycin remains an efficacious treatment option for MG in this population. Nevertheless, continuous surveillance and judicious macrolide use to maintain treatment efficacy are imperative. Further research and sustained monitoring of MG are essential to inform public health strategies and clinical guidelines in Zambia and similar settings worldwide.
Introduction
The global concern surrounding the prevalence of and antimicrobial resistance (AMR) in Mycoplasma genitalium is significant, yet comprehensive data remain lacking worldwide. Most of the available prevalence data for M. genitalium and its AMR are derived from high-income regions such as North America (United States and Canada), the European Union (especially Scandinavia and the United Kingdom), Australia, and Japan (1, 2). Accordingly, there is very limited information on M. genitalium prevalence and AMR from the World Health Organization (WHO)’s African Region, the Eastern Mediterranean Region, and Latin America and the Caribbean, which belong to the WHO Region of the Americas (1–5).
In women, M. genitalium is associated with cervicitis and pelvic inflammatory disease (6, 7), and during pregnancy M. genitalium infection is associated with an increased risk of preterm birth (7, 8). In antenatal care, the choice of antimicrobials for M. genitalium treatment is limited to macrolides, as fluoroquinolones and tetracyclines, other classes of antimicrobials effective against M. genitalium, are not recommended in pregnancy (9). Due to the potential adverse pregnancy outcomes associated with M. genitalium infections and the limited choice of treatment options in pregnancy, research into M. genitalium prevalence and macrolide resistance-associated mutations in the antenatal population is of great importance.
In the past decade, there has been a marked global increase in macrolide resistance among M. genitalium strains (2, 4, 5). The primary mechanism for macrolide resistance in M. genitalium is mutations in the 23S rRNA gene, specifically at nucleotide positions A2058 or A2059 (Escherichia coli numbering). M. genitalium has only one rRNA gene operon and specific mutations in one of these two 23S rRNA gene nucleotide positions changes the azithromycin minimum inhibitory concentration (MIC) value from <0.063 mg/L to >8 mg/L. Consequently, mutations in the 23S rRNA A2058 or A2059 nucleotide positions correlate well with both in vitro and clinical azithromycin resistance (4). Many countries worldwide mostly use syndromic management of sexually transmitted infections (STIs) and lack etiological diagnosis of bacterial STIs in general and M. genitalium, in particular. This has stymied M. genitalium diagnostics and efforts to quantify M. genitalium prevalence and AMR data, and hampered development of effective public health strategies and treatment guidelines in response. Gathering detailed global data on the prevalence of M. genitalium infection and AMR is crucial for public health (2, 4, 5). Such data are necessary to support evidence-based strategies for the prevention, management, and control of M. genitalium infections. Additionally, this information is vital for updating guidelines based on both etiological and syndromic management, ensuring they are informed by the most current and comprehensive evidence. In sub-Saharan Africa, including Zambia, there is an urgent need to understand the local epidemiology of M. genitalium and its AMR to inform public health interventions and policy decisions.
The Aptima M. genitalium assay (Hologic, San Diego, United States) was the first M. genitalium diagnostic test to receive approval from the US FDA. This nucleic acid amplification test (NAAT) has shown a 20–25% increase in sensitivity while maintaining high specificity compared to previously used diagnostic PCR assays (10, 11). The ResistancePlus™ MG (SpeeDx Pty. Ltd., NSW, Australia) is a CE-IVD approved real-time qPCR assay that detects M. genitalium by targeting the mgpB gene and additionally identifies the five key macrolide resistance-associated mutations in the 23S rRNA gene: A2058G, A2059G, A2058C, A2059C, and A2058T (E. coli numbering).
The main aim of the present study was to investigate the prevalence and epidemiology of M. genitalium among pregnant women attending antenatal care facilities in Zambia using the Aptima M. genitalium assay on the Panther Platform (Hologic). Additionally, the prevalence of macrolide resistance-associated mutations in M. genitalium-positive samples was examined using the ResistancePlus™ MG real-time qPCR assay (SpeeDx). Accordingly, this study aimed to provide critical data on M. genitalium infection and macrolide resistance patterns, which are essential for developing effective public health strategies and updating clinical guidelines. This research is particularly important in the antenatal care setting, where timely and accurate diagnosis and treatment of M. genitalium can significantly impact maternal and neonatal health outcomes.
Materials and methods
Study population and specimen collection
This was a nested study that was part of a larger evaluation of point-of-care tests for Trichomonas vaginalis and bacterial vaginosis registered in the Pan African Clinical Trials Registry (PACTR202302766902029) and conducted from 15 February to 26 May 2023 at four antenatal care facilities in Nchelenge, Zambia: Kabuta, Kafutuma, Kashikishi, and Nchelenge. Pregnant women attending these facilities were recruited based on the following inclusion criteria: (i) at least 13 weeks of gestation; (ii) no self-reported use of metronidazole or clindamycin during the current pregnancy; (iii) no known allergies or contraindications to metronidazole; and (iv) no use of vaginal creams or ointments, douching, or vaginal lubricants within 72 h prior to recruitment. These inclusion criteria were designed for the initial T. vaginalis study, results of which have been published elsewhere (12). Written informed consent was obtained from all participants before specimen collection. Vaginal swabs were collected from each participant using the Aptima Vaginal Swab Specimen Collection kit (Hologic). Background and clinical information including self-reported genitourinary symptoms (for example, unusual vaginal discharge, pain during urination, itching or burning of the vulva) was collected from all consenting participants.
Detection of Mycoplasma genitalium and other STIs
The Aptima M. genitalium assay, Aptima Combo 2 assay and Aptima T. vaginalis assay on the Panther System were used to detect M. genitalium, C. trachomatis plus N. gonorrhoeae and T. vaginalis, respectively, in full concordance with the manufacturer’s instructions. Determine® HIV Test Kit (Abbott, Illinois, United States) was used for HIV screening.
Detection of macrolide resistance-associated mutations
Samples positive for M. genitalium using the Aptima M. genitalium assay were further analyzed for macrolide resistance-associated mutations using the ResistancePlus™ MG assay (SpeeDx).
Statistics
All numerical variables were ranked as having non-normal distribution using the Shapiro–Wilk test and were presented by medians with interquartile range (IQR), with differences between the groups computed using the Mann–Whitney test. Categorical variables were presented by percentages and prevalence rates were reported with 95% confidence intervals (95% CIs). The differences in the frequencies of M. genitalium associates between M. genitalium-positive and M. genitalium-negative women were evaluated using Pearson’s chi-square or Fisher’s exact (whenever appropriate) tests. Statistical analyses were performed with the use of the statistics package IBM SPSS Statistics 27 (IBM). All tests for significance were two-sided, and statistically significant differences were assumed when p < 0.05.
Results
Prevalence and epidemiology of Mycoplasma genitalium
A total of 1,021 women were enrolled in the study; 16 samples were reported by the Panther System as invalid in the Aptima M. genitalium assay. Of the 1,005 valid vaginal swab samples, 127 (12.6% [95% CI 10.7–14.8%]) tested positive for M. genitalium using the Aptima M. genitalium assay (Table 1).
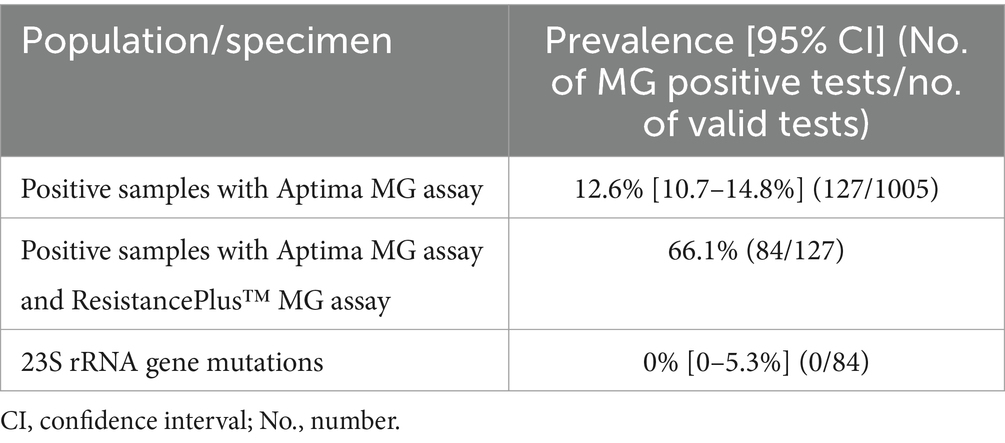
Table 1. Prevalence of Mycoplasma genitalium (MG) and macrolide resistance-associated mutations in women attending antenatal care in Zambia.
Women with M. genitalium infection were significantly younger (median, 22 years; IQR, 19–25 years) than M. genitalium-negative women (median, 23 years; IQR, 20–30 years; p = 0.015). Gestational age of M. genitalium-positive women (median, 25 weeks; IQR, 21–31 weeks) did not differ from that of M. genitalium-negative women (median, 26 weeks; IQR, 21–32 weeks; p = 0.458). Only 12 women (9.4%) infected with M. genitalium had symptoms of a genitourinary infection, which did not significantly differ from the frequency of genitourinary symptoms among M. genitalium-negative women (6.1%; Table 2).
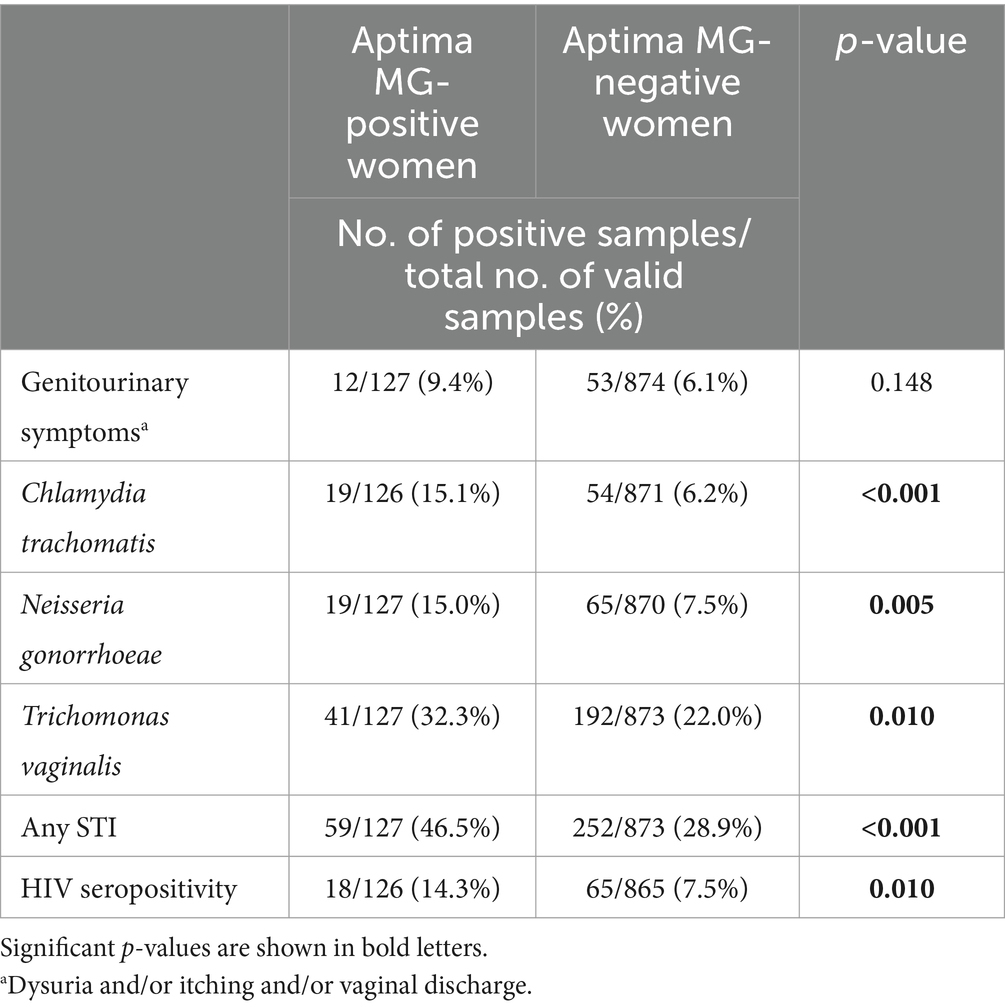
Table 2. Mycoplasma genitalium (MG) correlates in women attending antenatal care in Zambia.
The frequencies of C. trachomatis, N. gonorrhoeae, T. vaginalis, and HIV seropositivity were 7.4% [95% CI 6.0–9.2%] (75/1011), 8.3% [95% CI 6.8–10.2%] (84/1011), 23.0% [95% CI 20.5–25.6%] (233/1015), and 8.6% [95% CI 7.0–10.5%] (87/1011), respectively. M. genitalium infection was significantly associated with presence of all the other tested STIs: the detection rates of C. trachomatis, N. gonorrhoeae, T. vaginalis, and any of the three STIs were significantly higher in M. genitalium-positive than in M. genitalium-negative women (15.1% vs. 6.2, 15.0% vs. 7.5, 32.3% vs. 22.0, and 46.5% vs. 28.9%, respectively; Table 2). There was also a significant association between M. genitalium infection and HIV seropositivity (14.3% vs. 7.5%; Table 2).
Detection of macrolide resistance-associated mutations
The ResistancePlus™ MG assay detected MG in 66.1% (84/127) of samples positive by the Aptima M. genitalium assay. However, none of these 84 M. genitalium-positive samples exhibited any macrolide resistance-associated mutations (A2058G, A2059G, A2058C, A2059C, and A2058T) in the 23S rRNA gene (Table 1).
Discussion
The present study on the prevalence and epidemiology of M. genitalium and its lack of macrolide resistance among pregnant women attending antenatal care facilities in Zambia contributes valuable data to the limited information available from the WHO African Region. A high prevalence (12.6%) of M. genitalium was identified in this population in Zambia, but no macrolide resistance-associated mutations were detected in any M. genitalium-positive sample. This lack of macrolide resistance in M. genitalium stands in contrast to the rising global trends of high prevalence of macrolide resistance-associated mutations in M. genitalium-positive samples, especially in regions such as North America, Europe, Australia, and Japan (2, 4, 5).
Globally, M. genitalium prevalence and AMR data are predominantly available from high-income countries with significant gaps in data from resource-limited settings such as sub-Saharan Africa (2, 4, 5). Studies in high-risk populations across multiple countries have shown M. genitalium prevalence rates ranging from 10% to over 20%, with rates of macrolide resistance-associated mutations frequently exceeding 40% in several regions (1, 2, 4, 5). For instance, a recent study detected M. genitalium in 19.1% of women at high risk of STIs (12.4% in Guatemala, 16.0% Morocco, 22.1% South Africa) (13). The prevalence of macrolide resistance-associated mutations among women at risk in South Africa was found to be relatively low (2.4%). In contrast, other regions showed higher resistance rates: Morocco had 11.6% macrolide resistance-associated mutations and Guatemala 4.8% (13). These variations highlight the significant geographical differences in M. genitalium prevalence and AMR patterns, underscoring the need for region-specific public health strategies and continuous surveillance to effectively manage M. genitalium infections.
Because most research efforts regarding M. genitalium prevalence and AMR are focused on high-risk populations, there are limited data in lower-risk patients, such as pregnant women. In the antenatal population, the prevalence of M. genitalium is estimated to be around 1% in high-income settings, similar to that in the general population (1). According to one study, frequency of macrolide resistance-associated mutations in antenatal care in high-income settings may be as high as 30% (14). In low- and middle-income countries, M. genitalium prevalences of 3.6 to 12.5% have been reported among pregnant women in South Africa and Papua New Guinea (15–19), which aligns with this study. We also found no macrolide resistance-associated mutations in the antenatal population in Zambia as reported in several studies from South Africa and Papua New Guinea (16, 18, 20). However, one study from 2022 examining South African pregnant women found a single M. genitalium-positive sample (1 of 14 samples) with macrolide resistance-associated mutations (23S rRNA A2059G mutation) (17). The absence of detected macrolide resistance-associated mutations among M. genitalium-positive samples in our study population is a critical finding, which may be associated with the lack of etiological STI screening and subsequent treatment of asymptomatic M. genitalium infections in Zambia. It suggests that unlike in many other regions, the use of azithromycin for treating M. genitalium infections in Zambia may remain effective. This is in sharp contrast to findings from regions where macrolide resistance is high, and alternative treatments such as moxifloxacin are often recommended (2–4). Notably, in Zambia the first-line syndromic treatment for vaginal and urethral discharge is ceftriaxone 500 mg plus azithromycin 1 g plus metronidazole 2 g.1 However, international guidelines on the management of M. genitalium infections recommend a first-line treatment including azithromycin 1.5–2.5 g taken over 3–5 days, that is, if no macrolide resistance has been detected. These extended azithromycin dose regimens have a higher efficacy than the azithromycin 1 g single dose and also reduce the risk of azithromycin resistance emergence. Furthermore, in several of these international guidelines the azithromycin treatment is preceded by a doxycycline regimen (100 mg twice daily for 7 days). In Zambia and elsewhere, the use of azithromycin for treatment of STIs should be approached with caution and for the treatment of M. genitalium infections, azithromycin 1 g single dose therapy should ideally not be used (4). The global increase in macrolide resistance in M. genitalium and other STIs is alarming and underscores the importance of ongoing surveillance and judicious antibiotic stewardship. Maximizing the useful therapeutic life of azithromycin requires stringent measures to ensure proper diagnosis before treatment and prevent its overuse.
Our results align with global data from previous studies (1, 2, 4, 5, 10), which emphasize significant geographical variation in M. genitalium prevalence and AMR patterns. While our study did not detect any macrolide resistance, the high prevalence of M. genitalium shows a substantial burden of M. genitalium infections (many with concomitant other STIs) among pregnant women in Zambia, necessitating attention to both screening and treatment protocols. These findings underscore the importance of regional surveillance to identify and address specific public health needs with the global aim of filling gaps in data from sub-Saharan Africa.
The results of our study confirm that M. genitalium infection in women is mostly asymptomatic, i.e., only 9.4% of the M. genitalium-positive women had genitourinary symptoms, which was similar to the frequency of genitourinary symptoms among M. genitalium-negative women (6.1%). Furthermore, high rates of other STIs and HIV seropositivity (7.4%, 8.3%, 23.0%, 8.6% for C. trachomatis, N. gonorrhoeae, T. vaginalis, and HIV seropositivity, respectively), as well as strong associations of M. genitalium with other STIs and HIV seropositivity were observed among pregnant women in Zambia. Nearly half of the M. genitalium-positive women had one or more of the other three STIs. Our results support recent findings from Papua New Guinea (18) where around 40% of M. genitalium-positive pregnant women had one or more concurrent STIs. In resource-constrained settings, etiological diagnosis of STIs remains difficult, and syndromic management is mostly used. The limitations of syndromic management for STIs, as highlighted by Wi et al. (21), underscore the importance of integrating accurate and affordable NAATs (laboratory-based and at point-of-care) for detection of M. genitalium and other STIs into public health strategies, including antenatal care. This approach can significantly improve the diagnosis and treatment of M. genitalium and other STIs, thereby reducing the rates of overtreatment and missed diagnoses.
The cross-sectional design of our study provides a snapshot of the current prevalence and AMR patterns but does not account for temporal changes. Longitudinal studies are needed to monitor trends over time and assess the impact of interventions aimed at reducing M. genitalium prevalence and AMR. Such studies will help understand the dynamics of M. genitalium infections and AMR development. Nevertheless, our findings highlight several key recommendations for public health practice in Zambia and similar settings. Continuous monitoring of M. genitalium prevalence and AMR patterns is essential, and establishing robust surveillance systems will provide timely data to guide treatment protocols and public health interventions. Judicious use of antibiotics, particularly azithromycin, is critical to prevent the development of AMR. This requires ensuring accurate diagnosis and appropriate use of antibiotics. With the lack of appropriate natural history studies estimating the risk of sequelae subsequent to asymptomatic infections, the benefits of treating many asymptomatic infections have been considered to be outweighed by the risk of increased AMR from widespread treatment (3, 4). Appropriate education of healthcare providers and the public about M. genitalium and its potential implications for reproductive health is crucial; awareness campaigns can help reduce the stigma associated with STIs and promote timely healthcare-seeking behaviors.
In conclusion, the 12.6% prevalence of M. genitalium among pregnant women in Zambia, coupled with the absence of azithromycin resistance-associated mutations, provides critical insights into the epidemiology of M. genitalium in Zambia and the sub-Saharan African region. These findings underscore the need for targeted public health strategies to manage M. genitalium infections effectively and prevent the emergence of resistance. Further research and sustained surveillance efforts are essential to safeguard the reproductive health of women in Zambia and similar settings. Additionally, it is crucial to, as feasible, replace the syndromic STI management with etiological diagnosis of non-viral STIs in these settings.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by WHO Ethics Review Committee (Protocol ID: ITD 8960), the London School of Hygiene & Tropical Medicine Ethics Committee (Protocol No. 26262), the Tropical Disease Research Centre Ethics Committee (IRB Registration: 00002911), and the Zambian National Health Research Authority (NHRA000002/01/06/2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DS: Data curation, Formal analysis, Writing – original draft, Writing – review & editing. SS: Conceptualization, Investigation, Writing – review & editing. ES: Conceptualization, Formal analysis, Investigation, Writing – review & editing. EBC: Supervision, Writing – review & editing. DG: Conceptualization, Formal analysis, Investigation, Methodology, Writing – review & editing. EC: Supervision, Writing – review & editing. VM: Supervision, Writing – review & editing. JM: Supervision, Writing – review & editing. MC: Supervision, Writing – review & editing. CS: Supervision, Writing – review & editing. MtM: Supervision, Writing – review & editing. MsM: Data curation, Validation, Writing – review & editing. KB: Methodology, Writing – review & editing. IT: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. RMC: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing. MU: Conceptualization, Funding acquisition, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The primary T. vaginalis and bacterial vaginosis study was supported by the WISE Program (Doctoral Program for World-leading Innovative & Smart Education) of Ministry of Education, Culture, Sports, Science and Technology of Japan and Nagasaki University, School of Tropical Medicine and Global Health. This M. genitalium study was supported by the Örebro County Council Research Committee and the Foundation for Medical Research at Örebro University Hospital, Örebro, Sweden. Hologic provided all the Aptima tests. No funder had any role in the design, conduct or report of the study.
Acknowledgments
We are very grateful to the study doctors, nurses and participants at all the study sites. We express our many thanks also to Damon Getman and Philip Mueller at Hologic for providing the Aptima M. genitalium, Aptima Combo 2, and Aptima T. vaginalis tests.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^https://www.differentiatedservicedelivery.org/wp-content/uploads/August-2022-Zambia-Consolidated-Guidelines.pdf
References
1. Baumann, L, Cina, M, Egli-Gany, D, Goutaki, M, Halbeisen, FS, Lohrer, GR, et al. Prevalence of Mycoplasma genitalium in different population groups: systematic review and meta-analysis. Sex Transm Infect. (2018) 94:255–62. doi: 10.1136/sextrans-2017-053384
2. Chua, T-P, Vodstrcil, LA, Murray, GL, Plummer, EL, Jensen, JS, Unemo, M, et al. Evolving patterns of macrolide and fluoroquinolone resistance in Mycoplasma genitalium: an updated systematic review and meta-analysis. Lancet Microbe. (2025):101047. doi: 10.1016/j.lanmic.2024.101047
3. Jensen, JS, Cusini, M, Gomberg, M, Moi, H, Wilson, J, and Unemo, M. 2021 European guideline on the management of Mycoplasma genitalium infections. J Eur Acad Dermatol Venereol. (2022) 36:641–50. doi: 10.1111/jdv.17972
4. Jensen, JS, and Unemo, M. Antimicrobial treatment and resistance in sexually transmitted bacterial infections. Nat Rev Microbiol. (2024) 22:435–50. doi: 10.1038/s41579-024-01023-3
5. Machalek, DA, Tao, Y, Shilling, H, Jensen, JS, Unemo, M, Murray, G, et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: a systematic review and meta-analysis. Lancet Infect Dis. (2020) 20:1302–14. doi: 10.1016/S1473-3099(20)30154-7
6. Htaik, K, Vodstrcil, LA, Plummer, EL, Sfameni, AM, Machalek, DA, Manhart, LE, et al. Systematic review and meta-analysis of the association between Mycoplasma genitalium and pelvic inflammatory disease (PID). Clin Infect Dis. (2024):ciae295. doi: 10.1093/CID/CIAE295
7. Lis, R, Rowhani-Rahbar, A, and Manhart, LE. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis. (2015) 61:418–26. doi: 10.1093/cid/civ312
8. Frenzer, C, Egli-Gany, D, Vallely, LM, Vallely, AJ, and Low, N. Adverse pregnancy and perinatal outcomes associated with Mycoplasma genitalium: systematic review and meta-analysis. Sex Transm Infect. (2022) 98:222–7. doi: 10.1136/SEXTRANS-2021-055352
9. Bookstaver, PB, Bland, CM, Griffin, B, Stover, KR, Eiland, LS, and McLaughlin, M. A review of antibiotic use in pregnancy. Pharmacotherapy. (2015) 35:1052–62. doi: 10.1002/PHAR.1649
10. Shipitsyna, E, and Unemo, M. A profile of the FDA-approved and CE/IVD-marked Aptima Mycoplasma genitalium assay (Hologic) and key priorities in the management of M. genitalium infections. Expert Rev Mol Diagn. (2020) 20:1063–74. doi: 10.1080/14737159.2020.1842198
11. Unemo, M, Salado-Rasmussen, K, Hansen, M, Olsen, AO, Falk, M, Golparian, D, et al. Clinical and analytical evaluation of the new Aptima Mycoplasma genitalium assay, with data on M. genitalium prevalence and antimicrobial resistance in M. genitalium in Denmark, Norway and Sweden in 2016. Clin Microbiol Infect. (2018) 24:533–9. doi: 10.1016/j.cmi.2017.09.006
12. Sorano, S, Chaponda, EB, Mirandola, M, Chikwanda, E, Mwewa, V, Mulenga, JM, et al. Diagnostic accuracy of an antigen-based point-of-care test versus nucleic acid amplification testing for genital trichomoniasis among pregnant women attending antenatal care facilities in Zambia. BMC Infect Dis. (2025) 24:1482. doi: 10.1186/s12879-025-10698-9
13. Shipitsyna, E, Kularatne, R, Golparian, D, Müller, EE, Vargas, SK, Hadad, R, et al. Mycoplasma genitalium prevalence, antimicrobial resistance-associated mutations, and coinfections with non-viral sexually transmitted infections in high-risk populations in Guatemala, Malta, Morocco, Peru. Front Microbiol. (2023) 14:1130762. doi: 10.3389/fmicb.2023.1130762
14. Stafford, IA, Hummel, K, Dunn, JJ, Muldrew, K, Berra, A, Kravitz, ES, et al. Retrospective analysis of infection and antimicrobial resistance patterns of Mycoplasma genitalium among pregnant women in the southwestern USA. BMJ Open. (2021) 11:50475. doi: 10.1136/bmjopen-2021-050475
15. Govender, V, Moodley, D, Naidoo, M, Connoly, C, Ngcapu, S, and Abdool Karim, Q. Sexually transmitted infections in pregnancy and adverse pregnancy outcomes: a retrospective cohort study. Int J Gynaecol Obstet. (2024) 166:62–70. doi: 10.1002/ijgo.15529
16. Naicker, M, Singh, R, Tinarwo, P, and Abbai, NS. Lack of resistance to macrolides in Mycoplasma genitalium detected in South African pregnant women. South Afr J Infect Dis. (2021) 36:209. doi: 10.4102/SAJID.V36I1.209
17. Ngobese, B, Swe-Han, KS, Tinarwo, P, and Abbai, NS. Low prevalence of macrolide resistance in Mycoplasma genitalium infections in a cohort of pregnant women living with human immunodeficiency virus. Int J STD AIDS. (2022) 33:1174–82. doi: 10.1177/09564624221129412
18. Scoullar, MJL, Boeuf, P, Peach, E, Fidelis, R, Tokmun, K, Melepia, P, et al. Mycoplasma genitalium and other reproductive tract infections in pregnant women, Papua New Guinea, 2015-2017. Emerg Infect Dis. (2021) 27:894–904. doi: 10.3201/EID2703.201783
19. Smullin, CP, Green, H, Peters, R, Nyemba, D, Qayiya, Y, Myer, L, et al. Prevalence and incidence of Mycoplasma genitalium in a cohort of HIV-infected and HIV-uninfected pregnant women in Cape Town, South Africa. Sex Transm Infect. (2020) 96:501–8. doi: 10.1136/SEXTRANS-2019-054255
20. Jonduo, ME, Vallely, AJ, Whiley, DM, Riddell, MA, Pomat, W, Low, N, et al. Mycoplasma genitalium macrolide and fluoroquinolone resistance in pregnant women in Papua New Guinea. Sex Transm Infect. (2022) 99:71–2. doi: 10.1136/sextrans-2022-055552
Keywords: Mycoplasma genitalium, pregnancy, prevalence, antimicrobial resistance, azithromycin, macrolide resistance, Zambia, antenatal care
Citation: Schröder D, Sorano S, Shipitsyna E, Chaponda EB, Golparian D, Chikwanda E, Mwewa V, Mulenga JM, Chaponda M, Smith C, Mitsuaki M, Mirandola M, Blondeel K, Toskin I, Chico RM and Unemo M (2025) Prevalence and epidemiology of Mycoplasma genitalium and the absence of macrolide resistance in M. genitalium among pregnant women attending antenatal care in Zambia. Front. Public Health. 13:1576376. doi: 10.3389/fpubh.2025.1576376
Edited by:
Suncanica Ljubin-Sternak, University of Zagreb, CroatiaReviewed by:
Gwendolyn Wood, University of Washington, United StatesNaokatsu Ando, National Center For Global Health and Medicine, Japan
Copyright © 2025 Schröder, Sorano, Shipitsyna, Chaponda, Golparian, Chikwanda, Mwewa, Mulenga, Chaponda, Smith, Mitsuaki, Mirandola, Blondeel, Toskin, Chico and Unemo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magnus Unemo, bWFnbnVzLnVuZW1vQHJlZ2lvbm9yZWJyb2xhbi5zZQ==
†These authors share first authorship