 Bharti Singh*
Bharti Singh* Shri K. Singh
Shri K. Singh- Department of Survey Research and Data Analytics, International Institute for Population Sciences, Mumbai, India
Background: India has one of the highest burdens of child undernutrition, globally. Undernutrition is a persistent challenge despite the country’s economic growth. Empowering women is essential in addressing child undernutrition since empowered mothers are more inclined to obtain healthcare, enhance dietary diversity, and make informed choices that benefit their children’s health outcomes.
Objective: The study aims to investigate the relationship between women’s empowerment and child undernutrition in India from 2006 to 2021.
Methods: This study is based on three recent rounds of the National Family Health Survey. A composite index of women’s empowerment has been used to measure women’s empowerment. Further, binary logistic regression and decomposition analysis have been used to analyze the association and identify the key determinants that contribute to the reduction of undernutrition among children in India.
Result: Our research offers significant insights into the evolving dynamics of child undernutrition in India, particularly concerning the linkages with women’s empowerment. While empowerment was statistically insignificant in NFHS-3, it became a significant driver of child undernutrition in NFHS-4 (−0.12**[−0.21, −0.03]) and NFHS-5 (−0.15***[−0.24, −0.06]). Additionally, birth order, birth weight, and mother’s BMI are critical determinants of undernourishment status among children under age five. Wealth remains a consistently significant factor across all three survey rounds. Decomposition analysis further reinforces the significance of women’s empowerment, demonstrating that it accounts for a 3.3% reduction in child undernutrition In India.
Conclusion: The study underscores the critical role that empowering woman plays in combating child undernutrition, indicating the need for comprehensive strategies that prioritize women’s empowerment alongside other critical determinants to effectively tackle the persistent challenge of child undernutrition in India.
1 Introduction
In the tapestry of progress, the empowerment of women weaves the threads of a nourished generation and a brighter future for India.
Child malnutrition is a multifaceted issue that transcends geographical boundaries. Malnutrition is a deficiency, excess or imbalance in an individual’s intake of energy and/or nutrients. The consequences of malnutrition are dire as it not only stunts physical growth but also leads to a spectrum of morbidities and child mortality (48). The urgency of addressing this issue cannot be overstated, as malnourishment among children extends to their adulthood, restricts a person’s life biologically and diminishes the quality of their life (1, 2).
In 2022, Globally, 149 million (22.3%) children under age five were stunted, 45 million (6.8%) wasted, and 37 million (5.6%) were overweight or obese (3). Undernutrition is prevalent in developing regions, reflecting the complex relationship among socioeconomic disparities, inadequate healthcare, and insufficient access to nutritious food (2, 4, 5). Despite economic progress and advancements in healthcare, child malnutrition remains a formidable challenge for India. The recent round of the National Family Health Survey reveals a stagnant scenario. While there have been marginal improvements from 2005–06 to 2019–21 in stunting (decline of 12 percent point), wasting (decline of 1 percent point), and underweight (decline of 11 percent point), the rates continue to be frightening (6).
There are three key domains are used to comprehend malnutrition among children: stunting, wasting, and being overweight. Low height for age, or stunting, is a sign of chronic undernutrition caused by inadequate nutrition over a long period, including recurrent and chronic illnesses (7). Children who were stunted in their early childhood reported poor psychological functioning in their youth and suffered from higher levels of anxiety, depressive symptoms, and low self-esteem (2). In contrast to stunting, wasting reflects acute undernutrition, yet it has an equally profound impact. It has an immediate effect on the child’s health, leading to weight loss, development, and susceptibility to infectious diseases (8). Alongside these, underweight, defined as low weight for age, captures both chronic (stunting) and acute (wasting) forms of undernutrition. Underweight children face elevated risks of delayed cognitive development, poor school performance, and higher mortality, underscoring its role as a critical marker of child well-being (8). Overweight, the opposite of wasting, indicates overnutrition (8).
Numerous studies have explored the association between different socioeconomic factors and child nutrition, shedding light on the vivid nature of this challenge (9–12). Studies have revealed that undernutrition is more prevalent among children of lower birth weight and higher birth order under the age of five (11, 13). Maternal socioeconomic status emerges as a robust predictor of child undernutrition in India, suggesting that addressing multi-generational poverty and improving environmental factors are promising investments (10). Along with socioeconomic conditions, parental nutritional status, dietary diversity, hygiene practices, and women’s empowerment significantly contribute to child nutrition (9, 14). Some studies have independently linked women’s empowerment to improved childhood nutritional status, advocating for comprehensive interventions that integrate strategies for women’s empowerment (15, 16). Women play a pivotal role in shaping child nutrition as primary caregivers. Empowered women are better equipped to make informed decisions about nutrition, healthcare, and sanitation, thus positively influencing the nutritional outcomes of their children. Evidence from regions like Maharashtra and marginalized communities in Karnataka reaffirms the pivotal role of women’s empowerment in improving child nutrition, showcasing significant declines in child nutrition linked to women’s empowerment initiatives (17, 18). However, despite this recognition, only few studies have comprehensively explored how women’s empowerment impacts child nutrition over time, especially in the context of India.
Initially, scholars defined women’s empowerment as the ability to make choices for themselves and their families, emphasizing access and control over marital and social resources within families, communities, and society (19). This definition evolved over time and included the ability to influence and control one’s environment (20). Researchers expanded the concept to encompass control over resources, participation in economic decisions, self-esteem, mobility, and freedom from domestic violence, highlighting empowerment as a multidimensional construct (21–25). However, India’s contextual reality adds complexity, as some regions still struggle with conservative beliefs, indicating the long journey ahead to achieve equality (21).
India has implemented various policy interventions to improve women’s empowerment and maternal and child health. Despite these efforts, nearly one-third of India’s children are undernourished, highlighting the critical public health challenge. Furthermore, there remains a significant gap in understanding how the relationship between women’s empowerment and child undernutrition has evolved over time in India. Although existing studies have emphasized the importance of women’s empowerment, they often face challenges in encompassing the multiple dimensions necessary for a comprehensive understanding of this complex concept. To address these gaps, our study aims to investigate the relationship between women’s empowerment and their child nutrition outcome in India using data from 2006 to 2021.
2 Methods and materials
2.1 Data
The study is based on secondary dataset. The study used data from the three most recent rounds of the National Family Health Survey (6, 26, 27). The NFHS is a major, nationwide, large-scale, and multi-round survey conducted in a representative sample of households at the national, state and (from 2015 to 16 onwards) at district levels. The NFHS is an Indian version of the Demographic and Health Survey (DHS) that provides consistent and reliable estimates of fertility, mortality, family planning, child nutritional status, morbidity, utilization of maternal and child health care services, anemia, utilization and quality of health and family planning services. NFHS-3 collected information from 109,041 households, 124,385 women aged 15–49. NFHS-4 covered 699,686 women from over 601,000 households across 640 districts. NFHS-5 fieldwork for India was conducted in two phases, phase one from 17 June 2019 to 30 January 2020 and phase two from 2 January 2020 to 30 April 2021, extended due to the COVID-19 pandemic. NFHS-5 has gathered information from 636,699 households, 724,115 women aged 15–49.
2.2 Target population
We have taken children under the age of five who live with their mother (aged 15–49 years). The mother should be currently married or living in a union, and not pregnant.
2.3 Variable description
2.3.1 Outcome variables
We have used underweight as the indicator of undernutrition among children under age five. Underweight is defined as a weight-for-age of 2 standard deviations (SD) or more below the corresponding median of the reference population.
2.3.2 Predictor variables
Women’s empowerment is created using Confirmatory Factor Analysis (28, 29). We have taken 27 items to construct the index under six domains named attitude toward violence, decision making, perceived sexual rights, freedom of mobility, financial security and societal norms. The description of each domain is in the Supplementary 1.
The result of the goodness of fit indices shows that the RMSEA value in all survey years was below the cutoff point, which was 0.05. The CFI and TLI values were higher than 0.950, indicating strong reliability. Finally, the SRMR value was less than 0.08 for all survey years. These results validate the robustness and reliability of the women’s empowerment index across all three NFHS surveys (Supplementary 1).
2.3.3 Background variables
Age of the child in months, Sex of the child, Birth weight, Birth order, Child anemia status, Age of the mother, Delivery by C-section, Institutional delivery, ANC visits, Mother’s Body Mass index, Contraceptive use, Mother’s anemia status, Mother’s occupation, Wealth quintile, Caste, Religion, Place of residence, and Region.
2.4 Statistical analysis
We have used descriptive analysis and binary logistic regression to decode the relationship between child undernutrition and women’s empowerment. Binary logistic regression is used to understand the predictors of child undernutrition in India. Before running the regression analysis, all the assumptions have been checked, and there was no multicollinearity (VIF < 3). The basic form of the logistic regression model, which yields the probability of occurring of an event, can be depicted as:
Where Yi is the binary response variable, Xi is the set of explanatory variables, and β1, β2…… βk are the coefficients of the Xi variables.
To assess the disparity from 2016 to 2021, we have used multivariate decomposition analysis to see the factors affecting and contributing to the reduction of undernutrition among children. Powers (30) suggested that nonlinear response outcomes be tested to determine the time-period differences in child undernutrition (30). The decomposition analysis was carried out by considering the 2015–16 and 2019–21 outcome groups, respectively. The overall difference in a measured outcome can be decomposed into a sum of components owing to group differences in risk factors and group differences in the effects of those characteristics (30). Specifically, the difference in overall rates for two groups, labelled A and B can be decomposed as
Where r denotes the child undernutrition in each population and F(Xβ) denotes a once differentiable function mapping a linear combination of risk factors X and effects β, in the below multivariate model
In the above equation (b), r denotes the N × 1 vectors of rates, X is a N × K matrix of independent variables, and β is a K × 1 vector of logistic regression coefficients. The results of the multivariate model are estimated separately. Here we have chosen the reference group to be 2015–16, (the group labelled B) and the comparison group to be 2019–21 labelled as A. The multivariate decomposition splits the child undernutrition difference into two components-endowment (E) and coefficient (C) in equation (a). The “endowment” is the part that can be attributed to the change in the composition of a set of indicators. The “coefficient” is the portion that can be attributed to the change in the effect of indicators included in the analysis. This decomposition approach addresses important questions concerning the potential impacts of equalizing characteristics across the group.
This study has been analyzed on STATA Version 17 All the results were derived by applying the sampling weight provided by the Demographic and Health Survey (DHS) India.
3 Results
Table 1 shows the prevalence of undernutrition among children under age five in India from 2006 to 2021. The overall prevalence of undernutrition among children is 42.9% in NFHS-3, 35.9% in NFHS-4, and 31.8% in NFHS-5. Undernutrition prevalence declines over the years, yet the rate remain high among older children, particularly for 46–59 months (NFHS-3 = 45.9%; NFHS-4 = 38.5%; NFHS-5 = 34.2%). Female children exhibit lower undernutrition rates than males across all survey rounds. Children with higher birth order and low birth weight persistently have high undernutrition rates across all NFHS rounds.
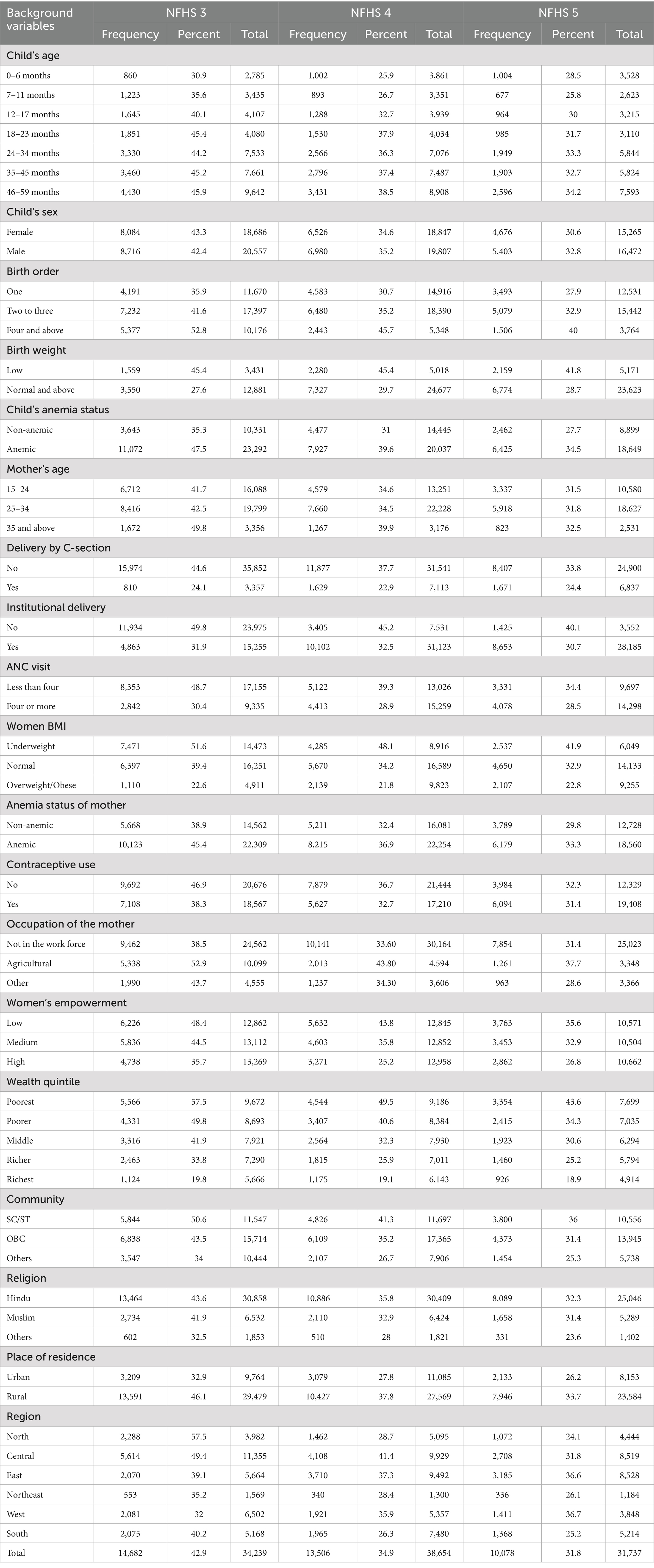
Table 1. Prevalence of undernourished children under age five by the background variables, NFHS 3, 4, and 5, India.
Anemia affects child nutrition significantly, there has been a consistently high prevalence of undernutrition among children if children themselves or their mother have higher rate of anemia. Further, Children of young mothers, particularly those aged 15–24, have higher undernutrition rates. Non-C-section deliveries show higher undernutrition rates. Whereas, children whose mother visited four or more ANC have lower prevalence of undernutrition.
Children of highly empowered mothers consistently show lower undernutrition rates. This trend is evident across all survey rounds, additionally, from NFHS-3 (37.5%) to NFHS-5 (26.8%), there is a 10 percent decline in the prevalence of child undernutrition among highly empowered women.
Socioeconomic and demographic disparities persist. Children from poorer households, SC/ST communities, rural areas, and regions like North and Central India exhibit higher undernutrition rates.
Tables 2–4 present binary logistic regression estimates on child undernutrition determinants, with a specific emphasis on the pivotal role of women’s empowerment.
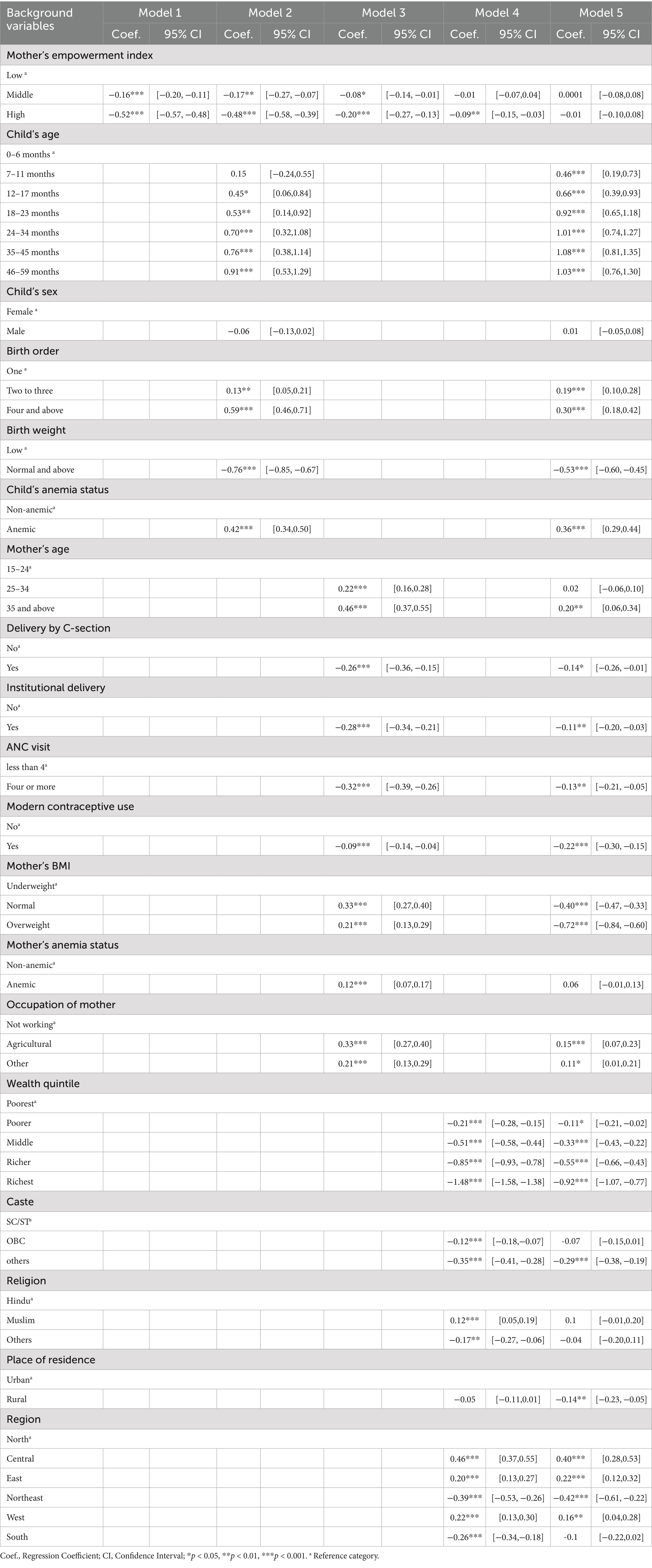
Table 2. Estimates of binary logistic regression of undernourished children under age five by background variables and women’s empowerment, NFHS 3, India.

Table 3. Estimates of binary logistic regression of undernourished children under age five by background variables and women’s empowerment, NFHS 4, India.
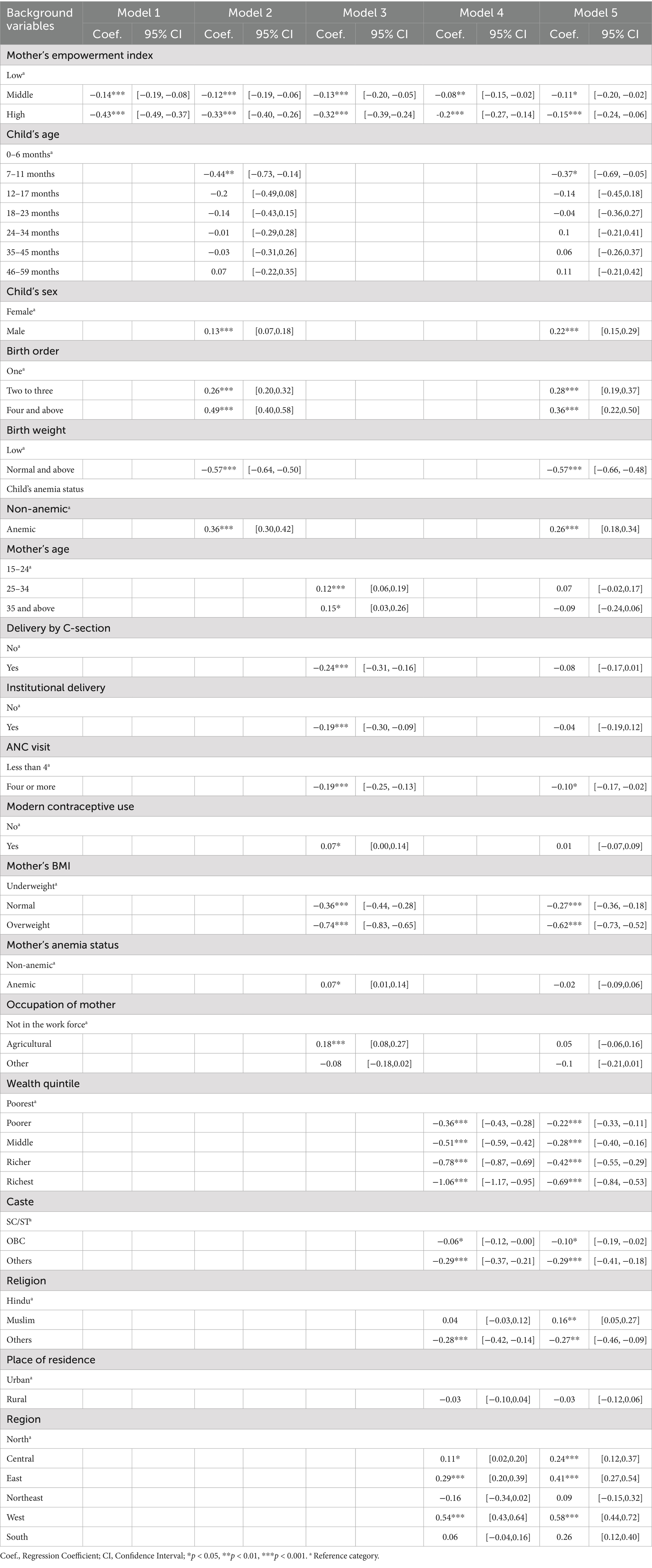
Table 4. Estimates of binary logistic regression of undernourished children under age five by background variables and women’s empowerment, NFHS 5, India.
Model 1 shows the unadjusted results from all three surveys, which consistently revealed a significant negative association between higher levels of women’s empowerment and child undernutrition. Upon adjustment for child-specific factors in Model 2, the significance of women’s empowerment on child undernutrition persists across all surveys. However, the effect was stronger in NFHS-3, where children with more empowered mothers were 48 % less likely to experience undernutrition.
Model 3, focusing solely on maternal variables, further reinforces the significant role of women empowerment in reducing child undernutrition. After controlling maternal characteristics such as age, delivery method, ANC visits, anemia status, occupation and women’s empowerment, higher levels of women’s empowerment continue to show a consistent negative association with child undernutrition in all three surveys. Model 4 (adjusted by all the household variables) demonstrates that despite the mediating influence of household factors, women’s empowerment remains a significant predictor of child undernutrition status in NFHS 3, 4, and 5. However, the effect and strength of the association were weakened in NFHS-3 (coef = −0.09**; CI [−0.15, −0.03]).
Further, the completely adjusted model (Model 5) indicate the effect of women’s empowerment on their child undernutrition when all covariates are considered. In NFHS-3 (2005–06), the impact of women’s empowerment was mitigated entirely in the presence of all the considered covariates. However, in NFHS-4, empowerment emerges as one of the crucial drivers of child undernutrition (coef = −0.12**; CI [−0.21, −0.03]), and by NFHS-5, this association and magnitude become more strong (coef = −0.15***; CI [−0.24, −0.06]).
The age of the child exhibits a significant negative association with undernutrition status in NFHS-3 and NFHS-4, indicating that as the child ages, the risk of undernutrition increases. Whereas, in NFHS-5 the effect of age was completely mitigated. Birth order, birth weight, and anemia status of the children emerge as significant contributors across all surveys, with higher birth order or child anemia increasing the risk of undernutrition, while normal or higher birth weight reduces this risk.
In NFHS-3, maternal age, institutional delivery, cesarean delivery, ANC visits, and maternal anemia are identified as significant Drivers to the risk of undernutrition among children. However, over time, the influence of these variables appears to diminish, suggesting potential shifts in maternal and healthcare practices or broader socioeconomic changes affecting child nutritional outcomes.
Further, the mother’s BMI stands out as a significant determinant of her child’s nutritional status across the years from 2006 to 2021. Additionally, the household’s wealth status emerges as a prominent driver of child undernutrition under the age of five in all the survey years.
Table 5 provides a broad perspective into the complex interplay of inherent characteristics (Endowment) and changes in influential factors (Coefficient). The multivariate decomposition analysis reveals that 30.35% of the reduction in child undernutrition between NFHS-4 and NFHS-5 is attributable to changes in endowments (due to differences in characteristics), while 69.65% is due to changes in coefficients (due to difference in coefficients). The total predicted change in undernutrition is 2.7 percentage points.
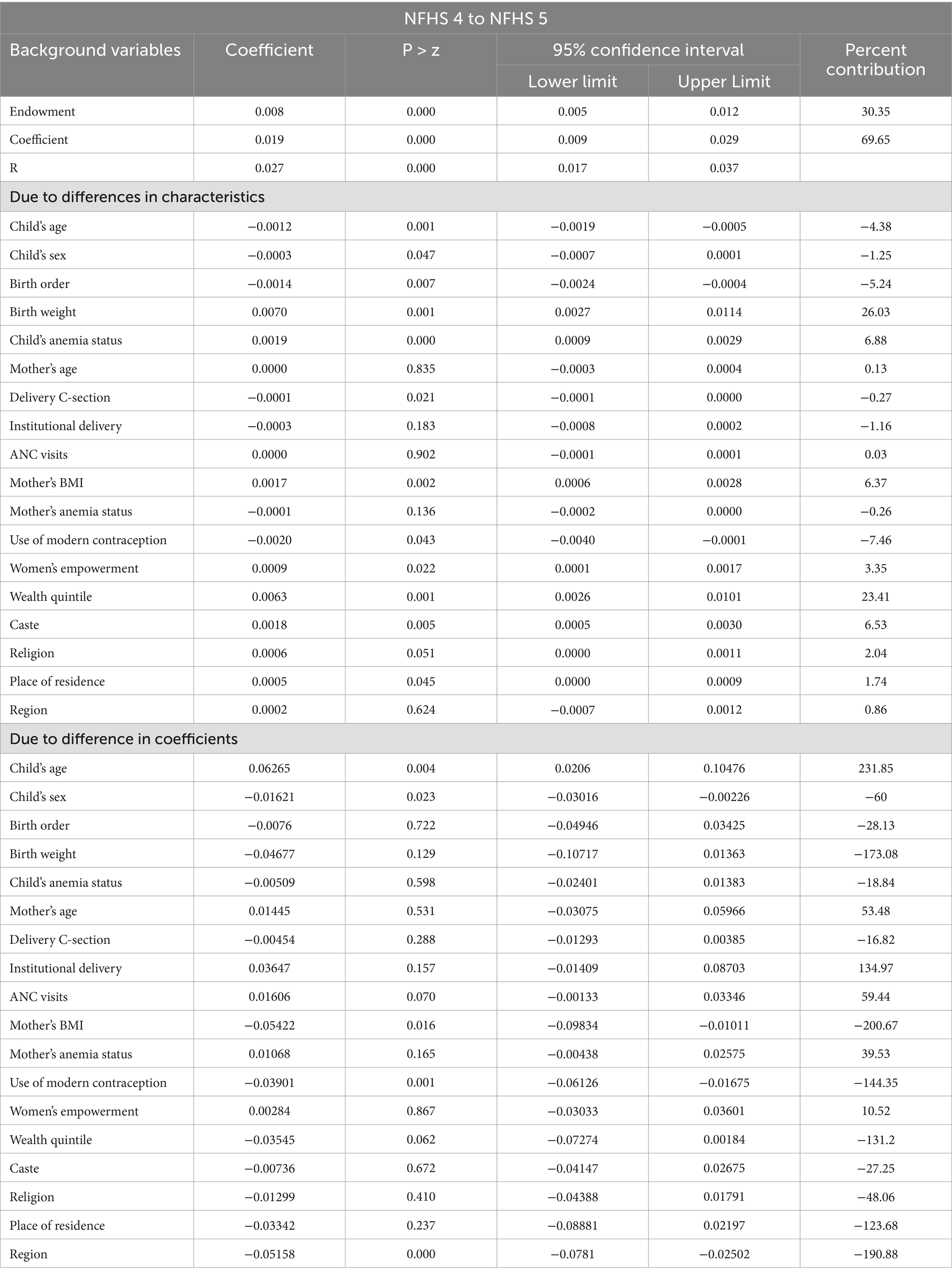
Table 5. Multivariate decomposition of undernourished child under age five with background and women’s empowerment variables, NFHS 4 to NFHS 5, India.
Among endowment-based contributors, birth weight emerged as the most influential factor, accounting for 26.03% of the reduction followed by wealth quintile (23.41%), and mother’s BMI (6.37%). Women’s empowerment contributed 3.35%, which, although lower than economic or biological determinants, is notable given its socio-behavioral nature. In contrast, factors such as higher birth order (−5.24%), and older child age (−4.38%) were associated with widening the gap, contributing negatively to the nutritional improvement.
The group differences in the effects of these predictors (due to coefficients) contribute 70 %, of which only the child’s age, Child’s sex, Mother’s BMI and the mother’s contraceptive use are significant contributors.
While women’s empowerment contributed less than traditional determinants like wealth and birth weight, its positive and significant influence underscores the growing relevance of gender-based interventions in public health.
4 Discussion
The current study embarks on a thorough exploration spanning three distinct time periods. It detangles the relationship between women’s empowerment and child undernutrition in India, highlighting that focusing on women’s empowerment may help to combat child undernutrition effectively. Existing research predominantly centers on limited dimensions of empowerment, such as women’s autonomy, control, and decision-making power within the household. Although maternal involvement in decision-making generally aligns with improved child nutritional status however, the strength and direction of these connections vary across different sub-domains of decision-making and depend on contextual factors such as child age, household wealth, and social support networks (16). Moreover, the domains of women’s empowerment are interconnected and interdependent. Neglecting certain aspects of empowerment may undermine the effectiveness of interventions aimed at improving child nutrition (15, 16, 31, 32). Women’s empowerment encompasses various dimensions and each of these domains plays a distinct yet interconnected role in shaping maternal and child health outcomes. (33, 34). While women’s empowerment, as measured by participation in household decision-making, freedom of mobility, and ownership, represents a distinct aspect of empowerment. Focusing solely on limited dimensions may overlook the broader context in which women navigate their lives and make choices regarding their own and their children’s health. Hence, the study utilizes women’s empowerment based on six dimensions to study its relationship with their child’s undernutrition.
One of the key finding of our study highlights the susceptibility of male children to undernutrition. Various studies support this finding that male children are more likely to be undernourished than female children, especially in the recent year (2019–21), which aligns with several studies as well (35–37). This disparity is multifaceted and can be attributed to a combination of biological, social, and environmental factors. Biologically, male children may face inherent vulnerabilities that predispose them to undernutrition, such as differences in metabolism, nutrient absorption, and susceptibility to infections. A comprehensive systematic review and meta-analysis of sex differences in undernutrition sheds further light on the complexity of this issue. The analysis revealed that approximately 14 % of the studies identified biological factors as primary contributors to the disparity, highlighting the importance of understanding the physiological differences between male and female children. However, a significant majority (39% of studies) shows that this disparity is due to the combination of social, and environmental factors in shaping the undernutrition landscape among children (37).
Our study examined the effect of birth order and birth weight on child undernutrition and found that a higher birth order and lower birth weight are associated with a higher risk of undernutrition. A study done by Rahman (11) in Bangladesh indicates that there are 38 % of children are stunted, of which children with fifth or higher birth order have approximately 70 % higher likelihood of being stunted (11). Another study done in sub-Saharan Africa found that low birth weight is a key determinant of undernutrition among children under age five years (13). Children with low birth weight are more likely to be underweight and prone to contracting diseases and infections, such as anemia and respiratory infections, which can increase their likelihood of being underweight (13).
Despite the widespread recognition of women’s empowerment as a pivotal factor in improving child nutrition outcomes, our findings present a complex picture. This study shows that women’s empowerment may not directly influence child undernutrition during the years 2005–06. This contrasting result may stem from population-specific factors, contextual variations, and methodological differences in measurement and analysis. Across various studies, a significant divergence exists in how empowerment is conceptualized and assessed (24, 38, 39). This lack of uniformity in methodologies and classification of empowerment indicators frequently results in conflicting conclusions regarding their correlation with child nutritional well-being, which demands a standardized measurement approach to draw definitive conclusions about the impact of women’s empowerment (32). Another possible reason is that key socioeconomic and demographic factors may have diluted the effect of women’s empowerment, as they serve as primary determinants of child nutrition (40). Furthermore, the study offers key insights into the changing dynamics of women’s empowerment on child undernutrition. By 2015–16, women’s empowerment emerged as a key driver of child undernutrition and contributed to a 3.3% reduction in undernutrition from 2015–16 to 2019–21, underscoring the transformative power of women’s empowerment in reshaping societal norms and public health outcomes.
The recognition of women’s empowerment as a critical determinant of child nutrition outcomes is well-supported in literature (15, 31, 32, 40). A systematic review published in 2019 emphasized the pivotal role of women’s empowerment, particularly during the first thousand days of a child’s life, in shaping nutritional outcomes. The review highlighted the need for further exploration of the pathways linking women’s empowerment to child nutrition, emphasizing its importance in public health discourse (32). Additionally, a longitudinal analysis conducted in India validated these findings, highlighting the positive influence of women autonomy on children’s health outcomes (41). Factors such as decision-making authority, freedom of movement, and financial autonomy were identified as key contributors to improved child nutrition in households where women enjoyed higher levels of empowerment.
The shifting landscape of child undernutrition in India reflects broader societal changes driven by various policies and programs aimed at empowering women and enhancing maternal and child health outcomes. Initiatives like the Integrated Child Development Services (ICDS) program, a flagship initiative, recognize the integral role of women in ensuring child health and nutrition (42). The National Rural Health Mission (NRHM), now part of the National Health Mission (NHM), focuses on enhancing healthcare delivery in rural areas, with maternal and child health as a crucial component (43, 44). Additionally, programs like the Janani Suraksha Yojana (JSY) and Pradhan Mantri Matru Vandana Yojana (PMMVY) aim to incentivize institutional deliveries and provide financial assistance to pregnant and lactating women. The National Nutrition Mission, or POSHAN Abhiyaan, launched in 2018, represents a concerted effort to address malnutrition comprehensively (27, 45, 46). By focusing on the first 1,000 days of a child’s life, this mission aims to empower women through targeted interventions, emphasizing the importance of nutrition, health, and sanitation. Moreover, initiatives such as Beti Bachao, Beti Padhao (Save the Girl Child, Educate the Girl Child) spotlight to escalate the education among female children (47). By challenging gender-based discrimination and promoting education for girls, these programs contribute to a broader narrative of empowering women to break the chains of malnutrition.
5 Recommendation(s)
Based on the above study, the following recommendations can be used to enhance the effectiveness of the existing program and policy.
1. Enhance Program Synergy and Integration: There is a pressing need to enhance synergy and integration between various programs on women’s empowerment and maternal and child health programs and services. Many initiatives currently operate in silos, which hinders their effectiveness. Integrating these programs would ensure a comprehensive approach to addressing the multifaceted determinants of child nutrition.
2. Targeted Interventions for High-Risk Groups: Modify existing programs to provide more targeted interventions for high-risk groups, such as children from economically disadvantaged households, those with multiple siblings, and regions with a high prevalence of undernutrition.
3. Comprehensive approach toward Women’s empowerment: Programs and policies should promote women’s empowerment across all the domains equally. Strengthening this area creates a supportive environment, enabling women to make better health choices and access essential services. This holistic approach may lead to more sustainable improvements in maternal and child health outcomes.
6 Conclusion
This study provides a comprehensive understanding of how women’s empowerment influences child undernutrition in India from 2006 to 2021. It underscores that in 2005–06, empowerment was not a significant factor in reducing child undernutrition, as child, maternal and socioeconomic factors played predominant roles. However, after socioeconomic improvements and interventions in mother–child-related programs and policies, both health and socioeconomic status improved, and empowerment emerged as a significant factor by 2015–16. This shift in the dynamics of child undernutrition aligns with the visionary perspective articulated by Kofi Annan, echoing, “There is no tool for development more effective than empowering women.” As India continues to progress toward achieving its developmental goals, the empowerment of women emerges as a cornerstone in fostering healthier and more prosperous communities, with benefits extending to future generations.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: https://dhsprogram.com/Data/.
Author contributions
BS: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. SS: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1583678/full#supplementary-material
References
1. Rai, RK, Kumar, S, Sekher, M, Pritchard, B, and Rammohan, A. A life-cycle approach to food and nutrition security in India. Public Health Nutr. (2015) 18:944–9. doi: 10.1017/S1368980014001037
2. Walker, AE. Multiple chronic diseases and quality of life: patterns emerging from a large national sample, Australia. Chronic Illn. (2007) 3:202–18. doi: 10.1177/1742395307081504
3. WHO (2013) WHO – malnutrition. Available online at: https://www.who.int/news-room/fact-sheets/detail/malnutrition (Accessed December 2, 2023).
4. Smith, LC, and Haddad, L. Reducing child undernutrition: past drivers and priorities for the post-MDG era. World Dev. (2015) 68:180–204. doi: 10.1016/J.WORLDDEV.2014.11.014
5. Smith, L. C., Haddad, L., Smith, L. C., and Haddad, L. (2000). Explaining child malnutrition in developing countries: A cross-country analysis. Available online at: https://EconPapers.repec.org/RePEc:fpr:resrep:111 (Accessed December 2, 2023).
6. NFHS-5. International institute for population sciences (IIPS) and ICF. 2021. National Family Health Survey (NFHS-5), 2019–21. India. Mumbai: IIPS (2021).
7. Caulfield, LE, Richard, SA, Rivera, JA, Musgrove, P, and Black, RE. Stunting, wasting, and micronutrient deficiency disorders. Dis Control Priorities Develop Countries. (2006)
8. Black, RE, Victora, CG, Walker, SP, Bhutta, ZA, Christian, P, De Onis, M, et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet (London, England). (2013) 382:427–51. doi: 10.1016/S0140-6736(13)60937-X
9. Agrawal, S, Kim, R, Gausman, J, Sharma, S, Sankar, R, Joe, W, et al. Socio-economic patterning of food consumption and dietary diversity among Indian children: evidence from NFHS-4. European J Clin Nutrition. (2019) 73:1361–72. doi: 10.1038/s41430-019-0406-0
10. Kim, R, Rajpal, S, Joe, W, Corsi, DJ, Sankar, R, Kumar, A, et al. Assessing associational strength of 23 correlates of child anthropometric failure: an econometric analysis of the 2015-2016 National Family Health Survey, India. Soc Sci Med. (2019) 238:112374. doi: 10.1016/J.SOCSCIMED.2019.112374
11. Rahman, M. Association between order of birth and chronic malnutrition of children: a study of nationally representative Bangladeshi sample. Cad Saude Publica. (2016) 32:e00011215. doi: 10.1590/0102-311X00011215
12. Smith, LC, Ruel, MT, and Ndiaye, A. Why is child malnutrition lower in urban than in rural areas? Evidence from 36 developing countries. World Dev. (2005) 33:1285–305. doi: 10.1016/J.WORLDDEV.2005.03.002
13. Aboagye, RG, Ahinkorah, BO, Seidu, AA, Frimpong, JB, Archer, AG, Adu, C, et al. Birth weight and nutritional status of children under five in sub-Saharan Africa. PLoS One. (2022) 17:e0269279. doi: 10.1371/JOURNAL.PONE.0269279
14. Pratley, P. Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Soc Sci Med. (2016) 169:119–31. doi: 10.1016/J.SOCSCIMED.2016.08.001
15. Cunningham, K, Ruel, M, Ferguson, E, and Uauy, R. Women’s empowerment and child nutritional status in South Asia: a synthesis of the literature. Matern Child Nutr. (2015) 11:1–19. doi: 10.1111/MCN.12125
16. Smith, LC, Ramakrishnan, U, Ndiaye, A, Haddad, L, and Martorell, R. The importance of women’s status for child nutrition in developing countries. Food and Nutrition Bulletin (2003) 24:287–8. doi: 10.1177/156482650302400309
17. Gupta, S, Pingali, P, and Pinstrup-Andersen, P. Women’s empowerment and nutrition status: the case of iron deficiency in India. Food Policy. (2019) 88:101763. doi: 10.1016/j.foodpol.2019.101763
18. Sethuraman, K, Lansdown, R, and Sullivan, K. Women’s empowerment and domestic violence: the role of sociocultural determinants in maternal and child undernutrition in tribal and rural communities in South India. Food Nutr Bull. (2006) 27:128–43. doi: 10.1177/156482650602700204
19. Mueller, D. Women and new world economy s an island s experience. Women Manag Rev. (1978) 17:308–17. doi: 10.1108/09649420210445767
20. Safilios-Rothschild, C. (1982). Female power, autonomy, and demographic change in the third world. Available online at: https://scholar.google.co.in/scholar?hl=en&as_sdt=0%2C5&q=Safilios-Rothschild+1982&btnG= (Accessed January 25, 2024).
21. Basu, A. (1992). Culture, the status of women, and demographic behaviour: Illustrated with the case of India. Available online at: https://www.cabdirect.org/cabdirect/abstract/19941800036 (Accessed November 10, 2023).
22. Duflo, E. Women empowerment and economic development. J Econ Lit. (2012) 50:1051–79. doi: 10.1257/JEL.50.4.1051
23. Jejeebhoy, SJ. Women’s education, autonomy, and reproductive behaviour: experience from developing countries. Women’s Educ, Autonomy Reproduct Behav: Experience Develop Countries. (1995)
24. Kabeer, N. Resources, agency, achievements: reflections on the measurement of women’s empowerment. Dev Chang. (1999) 30:435–64.
25. Kabeer, N. Gender equality and women’s empowerment: a critical analysis of the third millennium development goal 1. Gend Dev. (2010) 13:13–24. doi: 10.1080/13552070512331332273
26. NFHS-3. International Institute for Population Sciences (IIPS) and ICF. 2007. National Family Health Survey (NFHS-3), 2005–06: India. Mumbai: IIPS (2007).
27. NFHS-4. International Institute for Population Sciences (IIPS) and ICF. 2017. National Family Health Survey (NFHS-4), 2015–16: India. Mumbai: IIPS (2017).
28. Brown, TA, and Moore, MT. Confirmatory factor analysis In: RH Hoyle, editor. Handbook of structural equation modeling. New York, NY: Guilford Publications (2012)
29. Singh, B, and Singh, SK. Evolving dimensions of women’s empowerment in India. PLoS One. (2025) 20:e0327494. doi: 10.1371/JOURNAL.PONE.0327494
30. Powers, DA, Yoshioka, H, and Yun, MS. Mvdcmp: multivariate decomposition for nonlinear response models. Stata J: Promoting Commun Statistics Stata. (2012) 11:556–76. doi: 10.1177/1536867X1201100404
31. Jones, R, Haardörfer, R, Ramakrishnan, U, Yount, KM, Miedema, S, and Girard, AW. Women’s empowerment and child nutrition: the role of intrinsic agency. SSM - Population Health. (2019) 9:100475. doi: 10.1016/J.SSMPH.2019.100475
32. Santoso, MV, Kerr, RB, Hoddinott, J, Garigipati, P, Olmos, S, and Young, SL. Role of women’s empowerment in child nutrition outcomes: a systematic review. Adv Nutr. (2019) 10:1138–51. doi: 10.1093/ADVANCES/NMZ056
33. Bourey, C, Stephenson, R, and Hindin, MJ. Reproduction, functional autonomy and changing experiences of intimate partner violence within marriage in rural India. Int Perspect Sex Reprod Health. (2013) 39:215–26. doi: 10.1363/3921513
34. Ebrahim, NB, and Atteraya, MS. Women’s household decision-making and intimate partner violence in Ethiopia. Acad J Interdiscip Stud. (2019) 8:285–92. doi: 10.2478/ajis-2019-0041
35. Myatt, M, Khara, T, Schoenbuchner, S, Pietzsch, S, Dolan, C, Lelijveld, N, et al. Children who are both wasted and stunted are also underweight and have a high risk of death: a descriptive epidemiology of multiple anthropometric deficits using data from 51 countries. Archives of Public Health = Archives Belges de Sante Publique. (2018) 76. doi: 10.1186/S13690-018-0277-1
36. Thurstans, S, Opondo, C, Seal, A, Wells, JC, Khara, T, Dolan, C, et al. Understanding sex differences in childhood undernutrition: a narrative review. Nutrients. (2022) 14:948. doi: 10.3390/NU14050948
37. Thurstans, S, Opondo, C, Seal, A, Wells, J, Khara, T, Dolan, C, et al. Boys are more likely to be undernourished than girls: a systematic review and meta-analysis of sex differences in undernutrition. BMJ Glob Health. (2020) 5:e004030. doi: 10.1136/BMJGH-2020-004030
38. Agarwala, R, and Lynch, SM. Refining the measurement of women’s autonomy: an international application of a multi-dimensional construct. Soc Forces. (2006) 84:2077–98. doi: 10.1353/SOF.2006.0079
39. Cornwall, A. Women’s empowerment: what works? J Int Dev. (2016) 28:342–59. doi: 10.1002/JID.3210
40. Paul, P, and Saha, R. Is maternal autonomy associated with child nutritional status? Evidence from a cross-sectional study in India. PLoS One. (2022) 17:e0268126. doi: 10.1371/JOURNAL.PONE.0268126
41. Chatterjee, P, and Dubey, A. The role of women’s empowerment on child nutrition in India: a longitudinal analysis. Environ Dev Sustain. (2023) 26:1–24. doi: 10.1007/S10668-023-03183-3/TABLES/11
42. Sachdev, Y, and Dasgupta, J. Integrated child development services (ICDS) scheme. Med J Armed Forces India. (2001) 57:139–43. doi: 10.1016/S0377-1237(01)80135-0
43. Ghosh, SM. National health mission and the status of public healthcare in Indian states. Soc Change. (2023) 53:562–74. doi: 10.1177/00490857231203360
44. Nandan, D. National Rural Health Mission: turning into reality. Indian J Community Med: Official Pub Indian Assoc Prevent Soc Med. (2010) 35:453–4. doi: 10.4103/0970-0218.74338
45. Das, A, Rao, D, and Hagopian, A. India’s Janani Suraksha Yojana: further review needed. Lancet. (2011) 377:295–6. doi: 10.1016/S0140-6736(11)60085-8
46. PMMVY. (2017). PMMVY: Pradhan Mantri Matru Vandana Yojana. Available online at: https://wcd.nic.in/sites/default/files/PMMVY%20Scheme%20Implemetation%20Guidelines%20._0.pdf (Accessed May 27, 2024).
47. BBBP. (2015). BBBP: Beti Bachao Beti Padhao. Available online at: https://www.pmindia.gov.in/en/government_tr_rec/beti-bachao-beti-padhao-caring-for-the-girl-child/ (Accessed May 27, 2024).
Keywords: undernutrition, child nutrition, women’s empowerment, socioeconomic, NFHS, India
Citation: Singh B and Singh SK (2025) The evolving nexus of women’s empowerment and child nutrition in India. Front. Public Health. 13:1583678. doi: 10.3389/fpubh.2025.1583678
Edited by:
Suman Chakrabarty, West Bengal State University, IndiaReviewed by:
Sanjay Kumar, Dr. Hari Singh Gour University, IndiaChristian Rosales, University of La Laguna, Spain
Copyright © 2025 Singh and Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bharti Singh, YnMwOTU0N0BnbWFpbC5jb20=