 Vincenzo De Luca1*
Vincenzo De Luca1* Michele Virgolesi1Claudia Vetrani2,3Sara Aprano3,4
Michele Virgolesi1Claudia Vetrani2,3Sara Aprano3,4 Federica Cantelli5
Federica Cantelli5 Annamaria Di Martino5
Annamaria Di Martino5 Lorenzo Mercurio1
Lorenzo Mercurio1 Guido Iaccarino5
Guido Iaccarino5 Francesco Isgrò4,6
Francesco Isgrò4,6 Pasquale Arpaia4,6Annamaria Colao3,5
Pasquale Arpaia4,6Annamaria Colao3,5 Maddalena Illario1,4
Maddalena Illario1,4- 1Department of Public Health, Federico II University of Naples, Naples, Italy
- 2Department of Wellbeing, Nutrition and Sport, Pegaso Telematic University, Naples, Italy
- 3Italian Centre for the Care and Wellbeing of Patients with Obesity, Federico II University Hospital, Naples, Italy
- 4Interdepartmental Research Centre on Healthcare Management and Innovation, Federico II University of Naples, Naples, Italy
- 5Department of Clinical Medicine and Surgery, Federico II University of Naples, Naples, Italy
- 6Department of Electrical Engineering and Information Technologies, Federico II University of Naples, Naples, Italy
Background: Obesity is a common, serious, and costly chronic disease of adults and children that poses serious long-term health risks. Recent global estimates from the World Health Organization (WHO) show that the number of adolescents living with overweight or obesity is now increasing in low- and middle-income countries, particularly in urban settings. Health interventions using information technology (IT), especially diet and activity tracking, can lead to significant reductions in weight status.
Objective: This systematic review aimed to map IT-supported interventions designed to prevent obesity in adolescents, promoting healthy nutrition and physical activity. Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist was used. A search of the electronic databases Medical Literature Analysis and Retrieval System Online (MEDLINE) and Excerpta Medica Database (EMBASE) was conducted using search terms in various combinations appropriate to the research objective. The Effective Public Health Practice Project (EPHPP) quality assessment tool was used to assess quality.
Results: A total of 21 English language studies were eligible for inclusion. The systematic review synthesized information on weight control IT-supported intervention trials to prevent obesity, their domains of intervention, implementation setting, digital tool adopted, and the outcomes assessed.
Conclusion: The interventions included in the present study mainly concern nutritional aspects and physical activity, but motivational and psychological support also play a fundamental role in their success.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024412913, identifier [CRD42024412913].
1 Introduction
Obesity is a common, serious, and costly chronic disease of adults and children that poses serious long-term health risks. According to the World Health Organisation (WHO) global estimates, in 2019, 38.2 million children under the age of 5 years were overweight or obese. This number is now on the rise in low- and middle-income countries, particularly in urban settings. In 2016, over 340 million children and adolescents aged 5–19 were overweight or obese. The rise has occurred similarly among boys and girls: in 2016, 18% of girls and 19% of boys were overweight (1). In Europe in 2007, the WHO Regional Office established the European Childhood Obesity Surveillance Initiative (COSI) in response to the need for standardized surveillance data on the prevalence of children living with overweight or obesity among school-aged children. The latest COSI data collection was carried out in primary schools in 33 countries in 2018–20, including children aged 6–9 who had their weight and height measured. The prevalence of children aged 7–9 living with overweight or obesity is 29%, with a higher value among boys (31%) than girls (28%). However, the data show considerable variability across countries, with an overall prevalence of overweight ranging from 43% in Cyprus to 6% in Tajikistan, and an overall prevalence of obesity from 19% in Cyprus to 1% in Tajikistan (2). Italy is one of the countries with the highest prevalence: 39% overweight (including obesity) and 17% obesity among boys and girls aged 8 years old (2). In 2019, 206 schools (96.3%) in Campania (a region in southern Italy with about 6 million inhabitants) participated in the “Okkio alla Salute” survey for the COSI initiative, with 3,453 children enrolled. The survey suggests that 6.2% (n = 214) of children were in conditions of severe obesity, 12.6% (n = 435) were obese, and 25.4% (n = 877) were overweight. Regarding the perception of parents, as many as 63.3% of mothers of overweight children and 14.5% of mothers of obese children believe that their child is of normal weight or underweight (3). The “WHO Global Strategy on Diet, Physical Activity and Health” describes the importance of increasing general awareness and understanding of the effects of diet and physical activity on health, and this approach encourages health systems to collaborate with civil society, the private sector and the media to achieve this important goal (4). In 2023, the European Commission launched the “Joint Action for the implementation of best practices and research results on Healthy Lifestyle for the health promotion and prevention of non-communicable diseases and risk factors” (JA-Health4EUkids) to achieve results in terms of promoting healthy lifestyles and preventing childhood and school-age obesity. This action includes increasing physical activity and promoting healthy nutrition in boys and girls from the first 1.000 days of life, in families and communities. The JA-Health4EUkids aims to generate more interest and engagement in tackling childhood obesity in EU Member States, developing and applying a Health in All Policy (HiAP) approach (5). Given the multifactorial nature of obesity and its variability in terms of severity and implications for health, treating childhood obesity must be integrated at the healthcare level and involve professionals (6). The primary intervention for weight control is universal, targeting the entire population to reduce the incidence of obesity. The secondary intervention, defined as selective prevention, is aimed at the groups at risk, i.e., children of parents, children with low birth weight due to intrauterine growth restriction, and macrosomic children who tend to anticipate the adiposity rebound (7). Recent literature points out that parental body shape and an “obesogenic environment,” including increasingly early exposure to technological devices, are risk factors of early rebound adiposity (8, 9). Selective prevention is aimed at reducing the incidence of obesity in those already experiencing obesity from worsening the severity of their overweight and/or developing complications. It affects the prodromal risk factors of cardiovascular and metabolic mortality and is therefore aimed at preventing avoidable mortality. The tertiary prevention is aimed at children and adolescents affected by overweight or obesity, along with associated comorbidities, and is aimed at reducing complications (10). Several studies suggest that technology is a powerful ally in maintaining a healthy diet and lifestyle in the young population (11). In particular, digital interventions monitoring diet and physical activity can lead to significant reductions in weight status (12). Technological advances have made smartphone sensors more stable for real-time data collection, allowing them to be shared and processed for multiple analyses (13). Given the widespread use of smartphones in our daily lives—with 7.2 billion users worldwide, with peaks above 70% even in low- and middle-income countries—mHealth solutions can improve accessibility, quality, and efficiency. They also enhance the cost-effectiveness of interventions for the medium and long-term management of patients suffering from obesity or at potential risk group (14, 15). Information Technologies (IT) can contribute to the healthcare outcomes if they are adequately integrated into end users’ care processes, work routines and daily life. Technology can support the intervention of caregivers and health professionals (pediatricians, nutritionists, kinesiologists), providing more information on lifestyle behaviors and improving communication. Still, they cannot replace them in any way. Despite the potential of mHealth to support this aim, further adaptation to the context and a service delivery business model are needed. In Italy, I-Perseo project, financed by the National Center for Diseases Prevention and Monitoring (Centro Nazionale per la Prevenzione e il Controllo delle Malattie—CCM) of the Italian Ministry of Health, aims to address the unmet needs of overweight and obese adolescents, through the design and implementation of an innovative diagnostic and therapeutic pathway, integrating areas and levels of service delivery through digital solutions (16). There are many digital solutions, especially mHealth for interventions on obesity (17), but they lack evidence to assess clinical and organizational efficacy, technical usability, and patients’ engagement and satisfaction (18, 19). This review aims to identify interventions that investigated interventions for weight control to prevent obesity in adolescents, supported by digital solutions, identifying the target population, the setting and the level of intervention.
2 Materials and methods
2.1 Study design
The present systematic review was performed following the Preferred Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (20), and the study protocol was registered with PROSPERO (Registration No CRD42024412913). In March 2023, articles on digital interventions to prevent obesity among adolescents were searched through the Medical Literature Analysis and Retrieval System Online (MEDLINE) and Excerpta Medica database (EMBASE) electronic databases. Clinical trials or randomized controlled trial articles published in peer-reviewed scientific journals between 2013 and 2023 (until February 28, 2023) were included in the search. The review used the PICOS framework reported in Table 1 to identify search terms. Only articles written in English have been included. The terms used for the search at the title and abstract level were reported in Table 2, combined with the Boolean operators “OR” and “AND.”
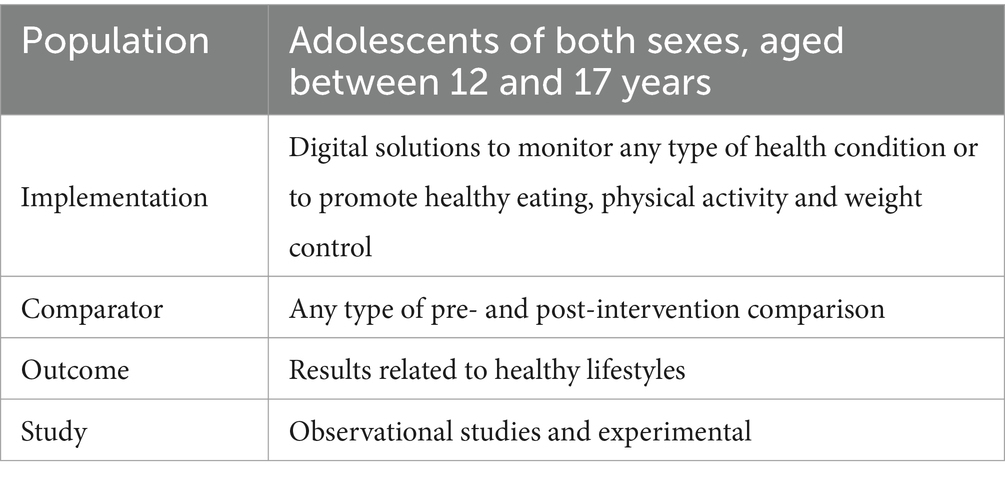
Table 1. PICOS framework to identify search terms.
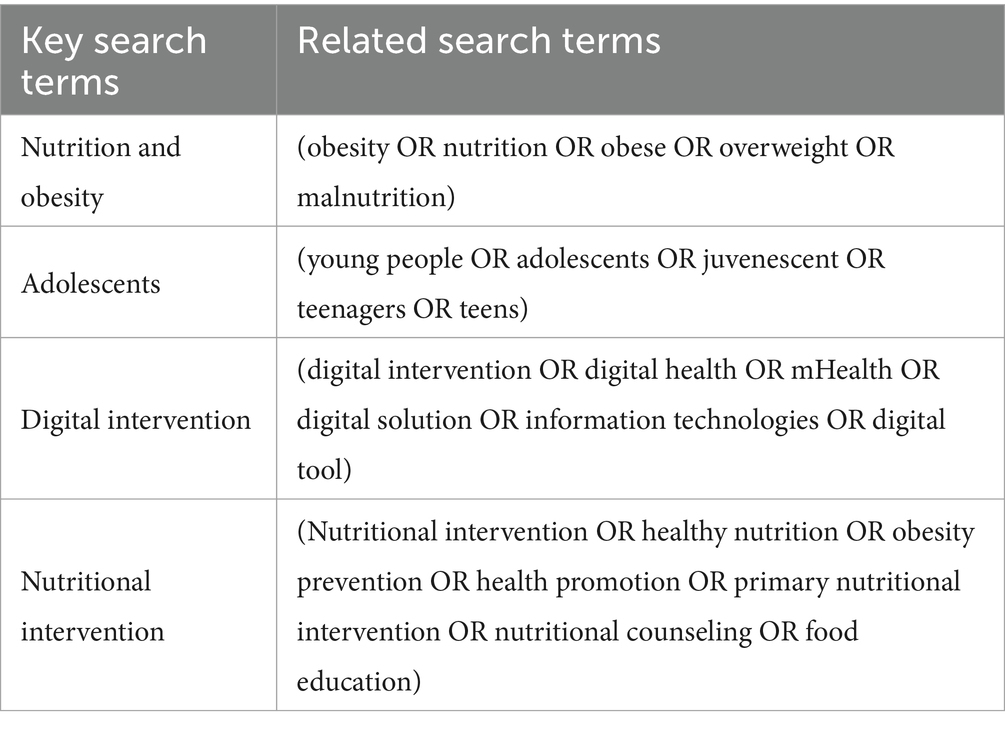
Table 2. Search terms used for the present review’s search strategy.
2.2 Data extraction
Duplicate entries from the database search have been eliminated. Three reviewers subsequently independently reviewed the title and abstract for eligibility. All articles were read before determining which studies should be included. Each reviewer recorded their inclusion and exclusion decisions on an electronic form, and differences were discussed and resolved by consensus. The main discussions were about excluding studies that targeted specific patient groups, whose nutritional and weight control interventions aimed to treat the disease. Four reviewers performed data extraction and harmonization. The data were reported following a standardized approach based on the following elements: (1) general information (name of the author and year of publication of the study), (2) age of the sample, (3) size of the sample, (4) sex of the sample, (5) type of study, (6) context of implementation, (7) level of intervention, (8) purpose of the study, (9) procedures, (10) digital tool adopted, (11) inclusion criteria, (12) measures, and (13) results. The resolution of disagreements was carefully recorded. A copy of the “as extracted” data (in addition to the consent data) was recorded on an electronic form. Six items were used to assess the study quality. The above elements include study design, confounding variables, data collection methods/tools, whether raters and participants were “blinded,” reports of withdrawals and dropouts. A weak, moderate, or strong score was assigned for each item according to Thomas et al.’s standardized guide and dictionary (21). The rating of the six components determines the overall study rating. Those with no weak and at least four strong ratings are considered strong. Those with less than four strong ratings and one weak rating are considered moderate. Finally, those with two or more weak ratings are considered weak. Three reviewers performed this process separately. Differences were discussed and resolved by consensus.
3 Results
3.1 Study selection
As shown in Figure 1, 236 articles were identified by searching for the selected electronic databases. Two hundred twenty-five remained for eligibility after the removal of duplicates. One hundred and fourteen articles were eliminated during the title and abstract screening phase. One hundred eleven articles were fully assessed, and 20 were chosen as pertinent for inclusion.
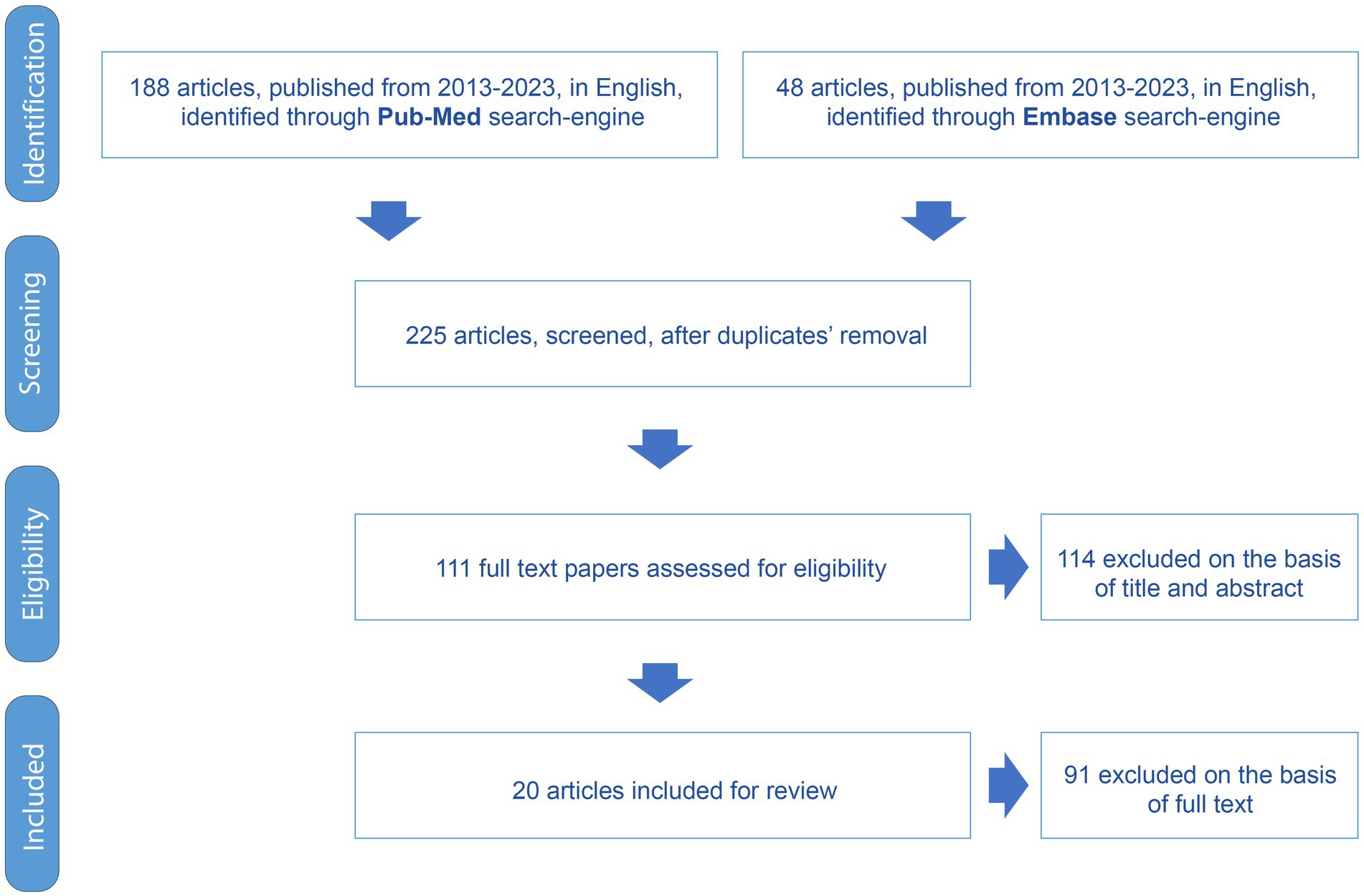
Figure 1. Flowchart of the PRISMA study selection procedure.
3.2 Study characteristics
Table 3 reports the characteristics of each study included in this review.

Table 3. Main characteristics of the studies included in the present review.
3.3 Quality assessment
The study quality assessment is reported in Table 4.
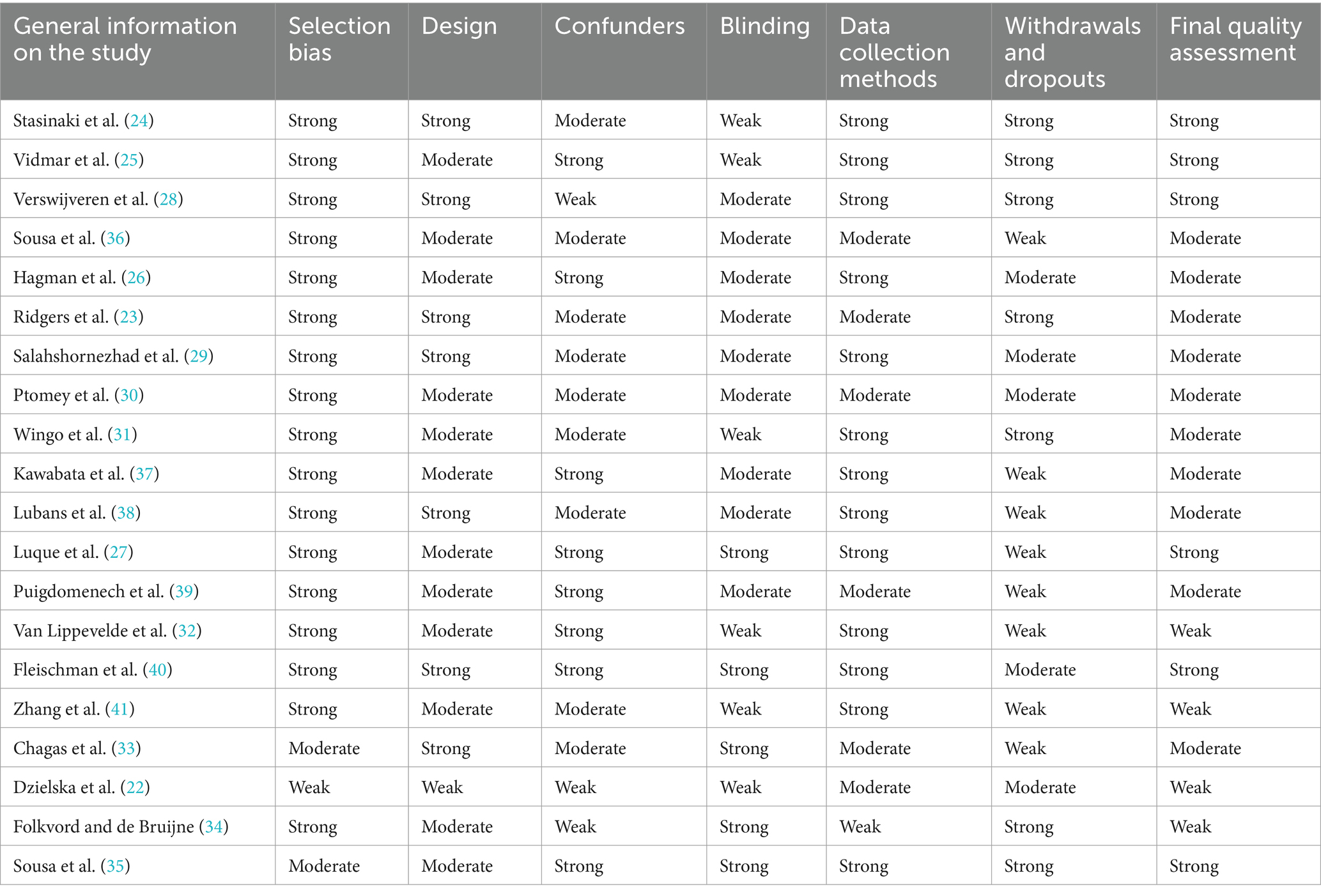
Table 4. Results of the study quality assessment.
4 Discussion
This work systematically reviewed obesity prevention interventions in children and adolescents supported by digital solutions. Twenty studies with various experimental designs, characteristics, durations, and intensities were identified after conducting a deep search across two databases. The designs of the selected studies were rigorous: n = 10 studies were Randomized Controlled Trials (RCT); n = 2 were cluster-RCT; n = 2 were non-RCT; n = 3 were observational; n = 1 was a Pragmatical clinical Trial; n = 1 was a quasi-experimental controlled cluster trial; and n = 1 was a pre–post feasibility randomized trial. The studies described interventions in a population ranging from the age of 4–18 years. N = 18 studies enrolled female and male populations, n = 2 studies enrolled only girls (22, 23). The studies described interventions for weight control to prevent obesity as effective in 50% of the cases (n = 10), in 20% of the cases, there was no significant increase in outcomes and in 30% (n = 6) of the studies, the results were unavailable. According to the literature (13, 14), the results of the present review suggest that technology can support multidimensional interventions for obesity prevention, often combining and integrating different digital solutions. Most of the studies (n = 8; 40%) included nutritional intervention, n = 3 (15%) studies included a physical activity intervention, n = 4 studies (19%) included both interventions, n = 5 (23%) studies included, in addition to physical activity and nutritional intervention, psychological or behavioral interventions. The review aims to provide a perception of the state-of-the-art digital interventions to prevent obesity in adolescents. Heterogeneity among studies represents the most critical limitation of this review, which affected the generalizability of the results and the comparison between studies. This did not allow for a meta-analysis because the study design, age, objectives, assessment measures and tools are different and do not allow for an aggregate analysis. Despite this, the review confirmed that interventions for preventing obesity in adolescents mainly concerned adherence to physical activity and a greater awareness of healthy nutritional prescriptions. Mobile apps are the most effective digital tools to promote changes in adolescents’ behaviors. From a clinical point of view, there is an increasing demand for tools to monitor adherence to nutritional prescriptions and physical activity, such as activity trackers and innovative diet diaries. Some of the studies are directly focused on interventions that impact clinical parameters such as BMI, weight and blood pressure (24–27) while some focus on behavior change for nutrition and physical activity (23, 28–35), and others on both (22, 36–41). The studies implemented at healthcare centers produced significant improvements in clinical parameters, demonstrating their greater interest in the clinical component of the intervention (24–26, 40). The studies on lifestyle changes that produced better results are the ones developed at school (22, 33, 35, 36, 41). This demonstrates the importance of the school setting for behavior change in the target population. Only one study produced significant results on adherence to monitoring eating habits and clinical parameters in healthcare setting (30). Although some studies do not describe statistically significant improvements, they encourage further studies with larger samples and include cost-effectiveness analysis (36). A key component of Verswijveren et al., intervention is the activity tracker that self-monitor physical activity, increasing the adolescents’ awareness of low activity levels, thus perceiving more barriers than those in the control group (28) According to literature, some level of intrinsic motivation must be present within the user to ensure continued use of digital solutions for lifestyle changes (42). Ridgers et al. (23), in describing the disappointing results in improving students’ adherence to physical activity, highlighted the need to combine wearable activity trackers with appropriately engaging digital resources. Wingo et al. weight control intervention failed because it was necessary to balance the need for greater child involvement with technology, and the parents’ desire for less interaction (31). Folkvord and de Bruijne argue that the failure of social media awareness campaigns depends on the careful development of content, rather than on the ability of influencers to impact the habits of teenagers (34).
4.1 Digital tools
Most studies (n = 11; 55%) use mobile apps to implement the intervention but are associated with other solutions (n = 7). The apps described in the various studies have different objectives and act on several dimensions (i.e., physical, nutritional, behavioral, etc.) with different modalities. Five studies implemented a digital intervention based on gaming. In the study conducted by Sousa et al. (35), a game-based learning process was developed through a mobile app. The tool includes prizes, points, and progress to the adolescent reported to be in the wall of fame. In another study (39), in addition to the reward system and the gamification module that allows users to get one-time awards for the selected target behavior, an avatar was developed on a mobile app that educates, cares and empowers adolescents in developing healthy habits. Through the avatar, the tool provides the user with educational and motivational messages and updates on their results and the results shared by their friends. Also, in the study conducted by Salahshornezhad et al. (29), there is a game-based intervention focusing on nutritional education accessible via smartphone. The mobile app enables aerobic exercise under the supervision of a trainer, along with cognitive behavioral therapy sessions specifically designed for adolescents by a clinical psychologist. The “Snack Track School” app (32) reproduces a virtual school environment with classrooms, gym, bicycle area, bathrooms, etc., where users have their locker, their own Snack Track tool and their own “anonymous” avatar, which they can customize. During the four-week intervention, users receive a storyline with challenges that help them track their eating habits. The “Snack Track School” tool allows users to earn credits/points based on the nutritional value of their snacks, performing positive reinforcement to influence automatic behavior. Rango Cards is a game-based mobile app that utilizes virtual reality (33). Rango Cards occurs in a virtual school where players visit different environments, including the canteen. The game is divided into phases that address food classification, healthy eating practices, the importance of cooking, misleading advertising, and reading food labels to understand their nutritional content. Other apps used in the study were integrated with the wearable activity tracker to monitor physical exercise. The app’s interface was often attractive to encourage its use by adolescents and make understandable the progress achieved in the different sessions (22, 23, 26–28, 39). The use of smartphones for nutritional interventions based on motivational reinforcement, diet control, and support systems in patients with intellectual disabilities is interesting. In these two studies, parents were also involved when necessary (30, 31).
4.2 Setting
The settings for enrollment of adolescents that received interventions for the prevention of obesity were schools (n = 13; 65%), healthcare centers (n = 6; 30%), such as pediatric services, and patients’ homes (n = 1; 5%). School is the most diffused place for implementing interventions to prevent obesity, probably because it provides a practical setting for educating about the consumption of healthy foods. Schools represent an optimal learning environment that reaches children from all socio-economic backgrounds (43). There is a need to prove the effectiveness of interventions in schools by implementing a multi-component educational approach dedicated to the children directly; the school environment, including school staff; and family members. This multi-component approach was often not described in the studies examined, except for patients with disabilities. A limitation of this review is the lack of a more complete understanding of the contextual factors that could influence behavior change (44). No information was found about public campaigns to raise awareness of adopting healthier behaviors and, therefore, motivate the use of digital tools. There is a lack of information about the presence of school policies that discourage the intake of sugar-sweetened beverages. Without this information, the evaluation of the success of digital interventions remains partially explained. However, further investigation is needed in this area to obtain more data. The studies implemented in the healthcare facilities enrolled children who already had a condition of overweight or obesity (≥ 85th percentile BMI). In these cases, interventions mediated by digital technologies allow monitoring patients’ behaviors in their living environment, representing a sustainable alternative to the outpatient visit for weight management. In the two studies in which the child was recruited at home, the children had intellectual disabilities. Adolescents with physical disabilities are at greater risk because physical inactivity, poor food intake and unhealthy lifestyle behaviors are neglected compared to the clinical and social management of disability. They are also more reluctant to participate in health promotion activities at school or in the community, and are much more likely to be sedentary and eat poorly. In this scenario, digital solutions to prevent obesity represent a valid and very effective strategy to improve adherence to healthy lifestyles and motivate the patient to socialize.
4.3 Level of intervention
Distinguishing between primary, secondary, or tertiary prevention is essential to identify the factors that drive weight gain among healthy adolescents and the achievement of therapeutic targets in overweight or obese adolescents (45). Primary prevention interventions aim to maintain a healthy weight, estimated at a BMI between the 5th and 85th percentiles in children and adolescents, corresponding to an adult BMI of 18.5–25 kg/m2. The present review revealed that most primary prevention interventions were conducted in schools (n = 13; 65%). n = 8 studies demonstrated that digital solutions are effective in supporting obesity prevention interventions. A meta-analysis study suggested that obesity prevention interventions for children aged 6–18 years at school have a small beneficial impact on BMI (46). The great diversity of interventions suggests that a more comprehensive assessment is required to identify the clinical and behavioral factors that allow effective interventions and to inform future obesity prevention public health policy (32).
Secondary prevention interventions aim to control weight in overweight individuals, thus keeping the BMI stable or reducing it from the overweight level to a healthy weight. The studies examined in the present review that provided a secondary prevention intervention were n = 4 (20%). Two studies enrolled adolescents in a healthcare center (25, 27); in n = 1 study, the adolescents were enrolled by a healthcare service integrated with school (26); and in n = 1 they have been enrolled at school (26). Except one, all studies confirmed the effectiveness of the interventions. Vidmar et al. compared a traditional clinical intervention versus an intervention supported by digital technology for weight loss in adolescents (25). Results demonstrated high retention and adherence rates, and reduced zBMI and %BMIp95 are more cost-effective than in the traditional clinical intervention. Hagman E. et al., 2022 confirmed that a digital support system for personalized weight-loss target curve and daily weight measurements, shared with family and healthcare professionals (HCP) is more effective than a standard childhood obesity treatment (26).
Tertiary prevention aims to hinder severe obesity (i.e., BMI > 95th percentile, corresponding to adult BMI > 30 kg/m2), prevent weight regain, and avoid comorbidities in children and adolescents who are living with obesity. In the present review, only one study implemented a tertiary prevention intervention. The intervention consists of counseling via a mobile app to support overweight or obese adolescents in adopting a healthy lifestyle, compared to a multi-component behavior change program. The study showed a significant decrease in BMI-SDS in the control group, rather than in the mobile app group. Muscle mass, strength and agility improved significantly in both groups. The group that used the mobile app significantly reduced body fat. The average daily usage of mobile apps is very encouraging (24). For this reason, the author suggested digital interventions to manage or sustainably follow up adolescent obesity, becoming an essential part of teletherapy and offering additional services to patients and families.
5 Conclusion
The review aimed to identify studies that implemented interventions supported by digital technologies to prevent obesity or promote weight control. The prevention levels, the setting, the digital tool adopted, and the effectiveness of the interventions were identified in the selected studies. The interventions mainly concerned nutritional aspects and physical activity. The studies demonstrated that motivational and psychological support play a fundamental role in the success of the intervention. The most widespread solutions were mobile apps and wearable devices for monitoring physical activity, often integrated. Interventions spread via social media are also popular. The use of smartphones is strategic. This review confirms that IT-supported personalized secondary prevention interventions for the treatment of obesity, with a strong integration between the different actors (i.e., health service, school, parents), present positive results in terms of weight loss. It is necessary to encourage integration among the various actors interacting with adolescents in multiple settings (School, Healthcare center, Home, Leisure-time facility). The widespread use of digital devices ensures new possibilities both for prevention strategies and personalized treatments to curb the expansion of the obesity epidemic (47). Investing in new digital technologies to prevent obesity is advantageous in terms of the effectiveness and sustainability of interventions, with positive impacton service delivery organization. This work aims to contribute to the discussion on designing and implementing an innovative diagnostic and therapeutic path. The present review suggests that the efficacy of digital solutions remains limited; they can play a strategic role in the interventions, especially if they provide different integrated solutions, connected to traditional clinical interventions. Mobile applications, web-based tools, text messages, portable monitoring devices/personal digital assistants (PDAs) and pedometers allow accessible interaction, frequent contact, and data monitoring through mobile applications, which improve short-term outcomes (48).
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: Medical Literature Analysis and Retrieval System Online (MEDLINE) and Excerpta Medica Database (EMBASE).
Author contributions
VL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MV: Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. CV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. SA: Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. FC: Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. AM: Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. LM: Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. GI: Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. FI: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. PA: Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MI: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was financed by “Prevent and reduce overweight in the adolescent population through the design of an integrated Dignostic and Therapeutic Pathway” (Prevenire e ridurre l’eccesso ponderale nella popolazione in età adolescenziale attraverso la costruzione di un PDTA integrato), in the frame of the National Center for Diseases Prevention and Monitoring (Centro Nazionale per la Prevenzione e il Controllo delle Malattie -CCM) of the Italian Ministry of Health (Grant No. D17G22000300001).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organisation. Obesity and overweight (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (Accessed on February 27, 2025).
2. Italian Superior Institute of Health. WHO European childhood obesity surveillance initiative – COSI (2022). Available online at: https://www.epicentro.iss.it/obesita/cosi-2022 (Accessed on February 27, 2025).
3. Italian Superior Institute of Health. OKKIO alla SALUTE: i risultati dell’indagine 2019 in Campania (2021). Available online at: https://www.epicentro.iss.it/okkioallasalute/indagine-2019-report-campania (Accessed on February 27, 2025).
4. World Health Organisation. WHO global strategy on diet, physical activity and health (2004). Available online at: https://apps.who.int/gb/ebwha/pdf_files/WHA57/A57_R17-en.pdf (Accessed on February 27, 2025).
5. Vantarakis, A, Velissari, J, and Brouma, M. Health4EUKids project and best practices against obesity. Eur J Public Health. (2023) 33:ckad160.329. doi: 10.1093/eurpub/ckad160.329
6. Weiler, A. mHealth and big data will bring meaning and value to patient-reported outcomes. mHealth. (2016) 2:2. doi: 10.3978/j.issn.2306-9740.2016.01.02
7. Fornari, E, Brusati, M, and Maffeis, C. Nutritional strategies for childhood obesity prevention. Life. (2021) 11:532. doi: 10.3390/life11060532
8. Cissé, AH, Lioret, S, de Lauzon-Guillain, B, Forhan, A, Ong, KK, Charles, MA, et al. Association between perinatal factors, genetic susceptibility to obesity and age at adiposity rebound in children of the EDEN mother-child cohort. Int J Obes. (2021) 45:1802–10. doi: 10.1038/s41366-021-00847-w
9. Pomi, AL, Pepe, G, Aversa, T, Corica, D, Valenzise, M, Messina, MF, et al. Early adiposity rebound: predictors and outcomes. Ital J Pediatr. (2024) 50:98. doi: 10.1186/s13052-024-01671-4
10. Smith, JD, Fu, E, and Kobayashi, MA. Prevention and Management of Childhood Obesity and its Psychological and health comorbidities. Annu Rev Clin Psychol. (2020) 16:351–78. doi: 10.1146/annurev-clinpsy-100219-060201
11. Chau, MM, Burgermaster, M, and Mamykina, L. The use of social media in nutrition interventions for adolescents and young adults-a systematic review. Int J Med Inform. (2018) 120:77–91. doi: 10.1016/j.ijmedinf.2018.10.001
12. Yonker, LM, Zan, S, Scirica, CV, Jethwani, K, and Kinane, TB. "Friending" teens: systematic review of social media in adolescent and young adult health care. J Med Internet Res. (2015) 17:e4. doi: 10.2196/jmir.3692
13. Jelalian, E, Darling, K, Foster, GD, Runyan, T, and Cardel, MI. Effectiveness of a scalable mHealth intervention for children with overweight and obesity. Childh Obes. (2023) 19:552–9. doi: 10.1089/chi.2022.0154
14. Patalano, R, De Luca, V, Vogt, J, Birov, S, Giovannelli, L, Carruba, G, et al. An innovative approach to designing digital health solutions addressing the unmet needs of obese patients in Europe. Int J Environ Res Public Health. (2021) 18:579. doi: 10.3390/ijerph18020579
15. Pucciarelli, G, Simeone, S, Madonna, G, and Virgolesi, M. L’uso degli smartphone nel personale infermieristico: una revisione narrativa della letteratura [Smartphone use in nursing population: a narrative review]. Prof Inferm. (2017) 70:102–15. doi: 10.7429/pi.2017.702102
16. Progetto iPerseo Prevenire e ridurre l’eccesso ponderale nella popolazione in età adolescenziale attraverso la costruzione di un PDTA integrato. (2023). Available online at: https://iperseo.dieti.unina.it/index.php/il-progetto (Accessed on February 27, 2025).
17. DiFilippo, KN, Huang, WH, Andrade, JE, and Chapman-Novakofski, KM. The use of mobile apps to improve nutrition outcomes: a systematic literature review. J Telemed Telecare. (2015) 21:243–53. doi: 10.1177/1357633X15572203
18. Nour, M, Chen, J, and Allman-Farinelli, M. Efficacy and external validity of electronic and Mobile phone-based interventions promoting vegetable intake in young adults: systematic review and meta-analysis. J Med Internet Res. (2016) 18:e58. doi: 10.2196/jmir.5082
19. Arthurs, N, Tully, L, O'Malley, G, and Browne, S. Usability and engagement testing of mHealth apps in paediatric obesity: a narrative review of current literature. Int J Environ Res Public Health. (2022) 19:1453. doi: 10.3390/ijerph19031453
20. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Thomas, BH, Ciliska, D, Dobbins, M, and Micucci, S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid-Based Nurs. (2004) 1:176–84. doi: 10.1111/j.1524-475X.2004.04006.x
22. Dzielska, A, Mazur, J, Nałęcz, H, Oblacińska, A, and Fijałkowska, A. Importance of self-efficacy in eating behavior and physical activity change of overweight and non-overweight adolescent girls participating in healthy me: a lifestyle intervention with Mobile technology. Nutrients. (2020) 12:2128. doi: 10.3390/nu12072128
23. Ridgers, ND, Timperio, A, Ball, K, Lai, SK, Brown, H, Macfarlane, S, et al. Effect of commercial wearables and digital behaviour change resources on the physical activity of adolescents attending schools in socio-economically disadvantaged areas: the RAW-PA cluster-randomised controlled trial. Int J Behav Nutr Phys Act. (2021) 18:52. doi: 10.1186/s12966-021-01110-1
24. Stasinaki, A, Büchter, D, Shih, CI, Heldt, K, Güsewell, S, Brogle, B, et al. Effects of a novel mobile health intervention compared to a multi-component behaviour changing program on body mass index, physical capacities and stress parameters in adolescents with obesity: a randomized controlled trial. BMC Pediatr. (2021) 21:308. doi: 10.1186/s12887-021-02781-2
25. Vidmar, AP, Pretlow, R, Borzutzky, C, Wee, CP, Fox, DS, Fink, C, et al. An addiction model-based mobile health weight loss intervention in adolescents with obesity. Pediatr Obes. (2019) 14:e12464. doi: 10.1111/ijpo.12464
26. Hagman, E, Johansson, L, Kollin, C, Marcus, E, Drangel, A, Marcus, L, et al. Effect of an interactive mobile health support system and daily weight measurements for pediatric obesity treatment, a 1-year pragmatical clinical trial. Int J Obes. (2022) 46:1527–33. doi: 10.1038/s41366-022-01146-8
27. Luque, V, Feliu, A, Escribano, J, Ferré, N, Flores, G, Monné, R, et al. The Obemat2.0 study: a clinical trial of a motivational intervention for childhood obesity treatment. Nutrients. (2019) 11:419. doi: 10.3390/nu11020419
28. Verswijveren, SJJM, Abbott, G, Lai, SK, Salmon, J, Timperio, A, Brown, H, et al. Mediators of effects on physical activity and sedentary time in an activity tracker and behavior change intervention for adolescents: secondary analysis of a cluster randomized controlled trial. JMIR Mhealth Uhealth. (2022) 10:e35261. doi: 10.2196/35261
29. Salahshornezhad, S, Sohrabi, Z, Doaei, S, Gholamalizadeh, M, Mani, A, Mehrabi, M, et al. A multi-disciplinary approach to weight management of school-age girls: a study protocol. Multidyscyplinarne podejście do kontroli masy ciała dziewcząt w wieku szkolnym – protokół badania. Pediatr Endocrinol Diabetes Metab. (2021) 27:76–81. doi: 10.5114/pedm.2021.107162
30. Ptomey, LT, Willis, EA, Reitmeier, K, Dreyer Gillette, ML, Sherman, JR, and Sullivan, DK. Comparison of energy intake assessed by image-assisted food records to doubly labelled water in adolescents with intellectual and developmental disabilities: a feasibility study. J Intellect Disabil Res. (2021) 65:340–7. doi: 10.1111/jir.12816
31. Wingo, BC, Yang, D, Davis, D, Padalabalanarayanan, S, Hopson, B, Thirumalai, M, et al. Lessons learned from a blended telephone/e-health platform for caregivers in promoting physical activity and nutrition in children with a mobility disability. Disabil Health J. (2020) 13:100826. doi: 10.1016/j.dhjo.2019.100826
32. Van Lippevelde, W, Vangeel, J, De Cock, N, Lachat, C, Goossens, L, Beullens, K, et al. Using a gamified monitoring app to change adolescents' snack intake: the development of the REWARD app and evaluation design. BMC Public Health. (2016) 16:725. doi: 10.1186/s12889-016-3286-4
33. Chagas, CMDS, Melo, GR, Botelho, RBA, and Toral, N. Effects of the Rango cards game intervention on food consumption, nutritional knowledge and self-efficacy in the adoption of healthy eating practices of high school students: a cluster randomised controlled trial. Public Health Nutr. (2020) 23:2424–33. doi: 10.1017/S1368980020000531
34. Folkvord, F, and de Bruijne, M. The effect of the promotion of vegetables by a social influencer on adolescents' subsequent vegetable intake: a pilot study. Int J Environ Res Public Health. (2020) 17:2243. doi: 10.3390/ijerph17072243
35. Sousa, P, Martinho, R, Reis, CI, Dias, SS, Gaspar, PJS, Dixe, MDA, et al. Controlled trial of an mHealth intervention to promote healthy behaviours in adolescence (TeenPower): effectiveness analysis. J Adv Nurs. (2020) 76:1057–68. doi: 10.1111/jan.14301
36. Sousa, P, Fonseca, H, Gaspar, P, and Gaspar, F. Controlled trial of an internet-based intervention for overweight teens (Next.Step): effectiveness analysis. Eur J Pediatr. (2015) 174:1143–57. doi: 10.1007/s00431-015-2502-z
37. Kawabata, M, Chua, KL, and Chatzisarantis, NLD. A school-based intervention program in promoting leisure-time physical activity: trial protocol. BMC Public Health. (2018) 18:433. doi: 10.1186/s12889-018-5320-1
38. Lubans, DR, Smith, JJ, Peralta, LR, Plotnikoff, RC, Okely, AD, Salmon, J, et al. A school-based intervention incorporating smartphone technology to improve health-related fitness among adolescents: rationale and study protocol for the NEAT and ATLAS 2.0 cluster randomised controlled trial and dissemination study. BMJ Open. (2016) 6:e010448. doi: 10.1136/bmjopen-2015-010448
39. Martin, A, Caon, M, Adorni, F, Andreoni, G, Ascolese, A, Atkinson, S, et al. A Mobile phone intervention to improve obesity-related health behaviors of adolescents across Europe: iterative co-design and feasibility study. JMIR Mhealth Uhealth. (2020) 8:e14118. doi: 10.2196/14118
40. Fleischman, A, Hourigan, SE, Lyon, HN, Landry, MG, Reynolds, J, Steltz, SK, et al. Creating an integrated care model for childhood obesity: a randomized pilot study utilizing telehealth in a community primary care setting. Clin Obes. (2016) 6:380–8. doi: 10.1111/cob.12166
41. Zhang, Q, O'Connor, DB, and Hugh-Jones, S. Feasibility of a multiple-component mindfulness intervention for Chinese adolescents living with overweight: a pilot randomized trial. Appl Psychol Health Well Being. (2023) 15:516–35. doi: 10.1111/aphw.12393
42. Shabir, H, D'Costa, M, Mohiaddin, Z, Moti, Z, Rashid, H, Sadowska, D, et al. The barriers and facilitators to the use of lifestyle apps: a systematic review of qualitative studies. Eur J Invest Health Psychol Educ. (2022) 12:144–65. doi: 10.3390/ejihpe12020012
43. Genner, S, Suter, L, Waller, G, Schoch, P, Willemse, I, and Süss, D. MIKE – Medien, Interaktion, Kinder, Eltern: Ergebnisbericht zur MIKE-Studie. Zürich: Zürcher Hochschule für Angewandte Wissenschaften (2017).
44. Verdonschot, A, Follong, BM, Collins, CE, de Vet, E, Haveman-Nies, A, and Bucher, T. Effectiveness of school-based nutrition intervention components on fruit and vegetable intake and nutrition knowledge in children aged 4-12 years old: an umbrella review. Nutr Rev. (2023) 81:304–21. doi: 10.1093/nutrit/nuac057
45. von Philipsborn, P, Stratil, JM, Burns, J, Busert, LK, Pfadenhauer, LM, Polus, S, et al. Environmental interventions to reduce the consumption of sugar-sweetened beverages and their effects on health. Cochrane Database Syst Rev. (2019) 2019:CD012292. doi: 10.1002/14651858.CD012292.pub2
46. Olsen, NJ, Østergaard, JN, Bjerregaard, LG, Høy, TV, Kierkegaard, L, Michaelsen, KF, et al. A literature review of evidence for primary prevention of overweight and obesity in healthy weight children and adolescents: a report produced by a working group of the Danish council on health and disease prevention. Obes Rev. (2024) 25:e13641. doi: 10.1111/obr.13641
47. Hodder, RK, O'Brien, KM, Lorien, S, Wolfenden, L, Moore, THM, Hall, A, et al. Interventions to prevent obesity in school-aged children 6-18 years: an update of a Cochrane systematic review and meta-analysis including studies from 2015-2021. EClinicalMedicine. (2022) 54:101635. doi: 10.1016/j.eclinm.2022.101635
Keywords: digital health, obesity prevention, adolescents, mHealth, nutrition
Citation: De Luca V, Virgolesi M, Vetrani C, Aprano S, Cantelli F, Di Martino A, Mercurio L, Iaccarino G, Isgrò F, Arpaia P, Colao A and Illario M (2025) Digital interventions for weight control to prevent obesity in adolescents: a systematic review. Front. Public Health. 13:1584595. doi: 10.3389/fpubh.2025.1584595
Edited by:
Bibiana Scelfo, Institute of Social Economic Research of Piedmont, ItalyReviewed by:
Letteria Anna Morabito, University Hospital of Policlinico G. Martino, ItalyMaija Kale, University of Latvia, Latvia
Jed Senthil, Nanyang Technological University, Singapore
Copyright © 2025 De Luca, Virgolesi, Vetrani, Aprano, Cantelli, Di Martino, Mercurio, Iaccarino, Isgrò, Arpaia, Colao and Illario. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vincenzo De Luca, dmluYy5kZWx1Y2FAZ21haWwuY29t