 Andrew Wister1*†
Andrew Wister1*† Boah Kim2†
Boah Kim2† Mélanie Levasseur3,4†
Mélanie Levasseur3,4† Valérie Poulin5Sarah Qiu2Esther Yuwono2
Valérie Poulin5Sarah Qiu2Esther Yuwono2 Stéphanie Meynet3,4Julie Beadle6Laura Kadowaki7†
Stéphanie Meynet3,4Julie Beadle6Laura Kadowaki7† Katarzyna Klasa8,9†
Katarzyna Klasa8,9† Igor Linkov10
Igor Linkov10- 1Gerontology Research Centre and Department of Gerontology, Simon Fraser University, Vancouver, BC, Canada
- 2Gerontology Research Centre, Simon Fraser University, Vancouver, BC, Canada
- 3School of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada
- 4Research Centre on Aging, Eastern Townships Integrated University Centre for Health and Social Services–Sherbrooke Hospital University Centre, Sherbrooke, QC, Canada
- 5Department of Occupational Therapy, Université du Québec à Trois-Rivières, Trois-Rivières, QC, Canada
- 6Gerontology Research Centre, Simon Fraser University, Vancouver, BC, Canada
- 7Department of Gerontology, Simon Fraser University, Vancouver, BC, Canada
- 8US Army Engineer Research and Development Center, Concord, MA, United States
- 9University of Michigan School of Public Health, Ann Arbor, MI, United States
- 10US Army Engineer Research and Development Center, Concord, MA, United States
Background: The development of a theoretical model applied to social isolation and loneliness (SI/L) among older adults has not kept pace with the exponential growth in empirical research, especially since the COVID-19 pandemic. One promising but under-investigated area is the contribution of resilience models to this field. This paper provides a scoping review of the application of resilience theoretical models to social isolation and loneliness and suggests directions for the development of an integrated new model.
Method: Using the Arksey and O’Malley scoping review method, searches of four databases with 13 keywords were conducted April 9, 2024, with 17 articles meeting the inclusion criteria of the 1,671 extracted articles.
Results: Findings were summarized using thematic analysis separated into four major themes: (1) coping self-efficacy to reduce SI/L; (2) moderating expectations to foster resilience to SI/L; (3) the effects of social support, the environment and resilience on COVID-19 stressors, and; (4) resilience as a mediator between SI/L and mental health. We integrate these findings into a new model entitled the Resilience and Social Isolation Model of Aging (RSIMA).
Conclusion: RSIMA highlights SI/L as a dynamic process on a continuum, as well as elucidating what broader factors can lead to improved social connection, contributing to both individual-level and community resilience. To address the looming public health crisis of social isolation and loneliness among older people, future research studies must consider a systems-level perspective to SI/L and resilience.
Background
Social isolation and loneliness (SI/L) have received increasing attention as important public health issues for older adults (1). Over the last two decades in particular, there has been growing alienation due to increased social media uptake coupled with major events such as COVID-19 pandemic policies that reduced social contact and fostered fears of social contact (2, 3). Social isolation is defined as the reduced quantity and quality of social relationships; whereas loneliness pertains to the perception that social needs are not being met (4). It is recognized that while social isolation and loneliness often occur together, they can be unique since a person can have many social contacts but feel lonely and vice versa (5). We distinguish social isolation and loneliness when used separately in research, but combine them to discuss overlapping conceptual or empirical findings. SI/L has been shown to double the risk of all-cause mortality in older adults (6, 7), and to a spectrum of physical and mental health outcomes (4, 8–10). Indeed, a recent report by the US Surgeon General warned that an epidemic of SI/L has been an overlooked public health crisis with the potential to significantly harm the health of the nation (11).
Prevalence rates of SI/L pre-pandemic have been estimated in many studies and countries with variations based on populations and research design. In a systematic review pre-pandemic, Chawla et al. (12) reviewed 31 studies globally and calculated an overall prevalence of loneliness of 28.5 per cent. These rates have been found to be higher peri-pandemic and post-pandemic. For instance, Canadian Longitudinal Study on Aging (CLSA) data estimated relative increases in loneliness during the pandemic ranging between 33 and 67 per cent depending on age/gender group (13). In 2022, the National Institutes on Aging (NIA) surveyed adults aged 50 and over and found that up to 58% have experienced some degree of loneliness and that 41% are at risk of social isolation (1). Overall, SI/L is a common experience among a significant proportion and number of older adults.
There have also been many studies that have identified numerous modifiable and non-modifiable risk factors for SI/L among older adults [(e.g., 4, 14–17)]. This identification has also been extended to include the pandemic period [(e.g., 18, 19)]. These risk factors fall into several demographic and socio-ecological domains, including environment (e.g., housing/living arrangement, geographic location, and access to technology), individual and social characteristics (e.g., ethnicity, immigrant status, and caregiver status), physical characteristics (e.g., functional mobility and multimorbidity), and psychological factors (e.g., mental health and well-being). For instance, SL/I has been linked to sex, gender, partnership status and living arrangement, especially those of advanced age who are unattached (single, widowed, and divorced) and living alone (4, 15, 17, 18, 20). Additionally, risk for SI/L is higher among individuals with low income, poverty, or living in economically deprived or rural/remote communities (19, 21) and ethnic and gender minority groups (including Indigenous elders, new immigrants, and LGBTQ2+; 102) (13, 22). People with sensory loss, multimorbidity or other physical health challenges (4, 19) or poor mental health conditions (depression, anxiety, psychoses, etc.); and caregivers (23, 24) are also at greater risk for SI/L.
A wide range of protective factors have also been linked to SI/L. Some of these include: having strong support networks, engaging in rewarding leisure pursuits, and participating socially (15, 25–27); living with others (28); having a positive or resilient attitude (29); and access to technologies, such as computers, tablets, and smartphones (30, 31). Taken together, the nexus of risk/protective factors likely work in tandem or culminate to influence SI/L. These associations are further complicated by the fact that there may be bidirectional patterns between risk/protective factors and SI/L.
The development of theoretical models to link and add coherence to the plethora of risk and protective factors has not kept pace with the often-siloed research studies. One promising area has been the theoretical development of resilience applied to aging contexts. These build on a strength-based approach to understanding the ways in which older individuals bounce back and sometimes exhibit growth, in the face of various adversities, such as natural disasters, loss of a spouse, multimorbidity, and pandemics (32).
Early research on resilience stemming from the early 2000s focused on psychological resilience in reaction to mental health and family adversities among children or young adults that allowed for positive adaptation and growth. Psychological resilience includes positive psychology, adaptation to stress, with the inclusion of concepts such as self-efficacy, mastery and coping processes (33–38). More recently, resilience models have been applied to a variety of vulnerable groups facing various adversities at the environmental, community, family and individual levels, including older adults (39–48, 103). Specifically, social resilience has incorporated elements of social participation, social isolation, and community belonging (27, 49, 50, 103).
One comprehensive interdisciplinary model is the Unified Model of Resilience and Aging (UMRA) which have been developed and applied to the pandemic context (48). Resilience models, like the UMRA, seek to understand how and why some individuals, families, and communities recover from adversity better than others. The UMRA integrates individual and system-level processes that occur over the life course, acknowledging that an adverse event (a pandemic, illness, personal loss) creates disruption that can be age and time-dependent. As such, resilience depends not only on the activation of internal resources (positive attitude) but also external resources (e.g., support from family, friends or organization), which can vary with age and other factors. It also includes four system-level (organizational) functions used by the US National Academy of Sciences Resilience Model (51, 52) which are central to the present study: (1) Planning for adverse events requiring reductions in risk in response to an identified threat, (2) Absorption of stressors and outcomes associated with an adversity which is necessary to initiate resilience through recovery and adaptation, (3) Recovery occurring through various forms of short and long-term strength-based resilience, and (4) Adaptation relating to changes in the system to promote future resilience. Together, these contexts are understood as manifested across the life courses of individuals. However, to our knowledge, none of these models have yet to be applied to SI/L. This scoping review aims to answer the following question: what are the major thematic theoretical developments that connect resilience and aging to SI/L? The review also intends to develop a new model of resilience and SI/L applied to aging and older adults, and offer a research agenda to guide future studies.
Methods
Search strategy
This scoping review used the methodology outlined by the Joanna Briggs Institute’s (JBI) Reviewer Manual (53), which provides an overview of scoping review methods (54) and highlights the most recent updates, primarily based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) (55). We used the Population-Concept-Context (PCC) framework to guide the scope and eligibility criteria of this review. The population was defined as older adults aged 50 or older. The concept focused on resilience models/frameworks related to SI/L; and the context included diverse care settings where older adults reside and receive care, especially related to resilience, coping strategies, and/or SI/L (a more detailed eligibility criteria is shown below). A specific three-step search strategy was employed. First, the initial search was conducted using four targeted academic online databases—APA PsycInfo, AgeLine, CINAHL Complete and MEDLINE. The following set of keywords was used: (“resilience” OR “strengths” OR “coping”) AND (“isolation” OR “social isolation” OR “loneliness”) AND (“older adults” OR “older persons” OR “older adults” OR “aging”) AND (“theory” OR “model” or “framework”). The full search strategy is presented in Appendix 1. To ensure enough articles, no limitation was placed on the publication date. After screening the title and abstract of retrieved studies, the second step entailed comprehensive research using identified keywords and index terms across all targeted databases. The third step included a hand search based on the reference list of identified articles to obtain additional sources. Also, we reviewed the reference lists of identified systematic review articles to supplement the initial electronic search to identify missing articles.
Inclusion and exclusion criteria
To maximize theoretical developments in this area, the age criterion included older adults aged 50 or older. The specific inclusion criteria entailed: (1) studies with a focus on resilience models/frameworks or coping strategies applied to SI/L, (2) studies whose target population was older adults aged 50 or over, (3) empirical studies including quantitative, qualitative, mixed or multi-methods research, and (4) studies published in English. An article was excluded if it: (1) targeted pediatric, youth, or young adult populations, (2) did not focus on resilience or coping/adaptation conceptual or theoretical conceptual frameworks and SI/L, (3) did not focus on SI/L as a study outcome; gray area articles not published in peer-reviewed outlets; and (4) if the article was a systematic review/scoping review.
Procedure
The screening procedure was conducted using the Covidence online platform1 (accessed on 9 April 2024). Covidence is a web-based systematic review program to streamline evidence synthesis process (56) and is well-suited for rigorous scoping reviews (57). Articles that met the inclusion criteria were imported to Covidence and duplicates were deleted. Two independent reviewers (BK, EY) completed two rounds of screening for the review. The first stage of screening entailed title and abstracts was conducted based on the eligibility criteria. Issues during this process were resolved based on the discussion with a third independent reviewer (AW). The second stage was a full-text review. A detailed screening process for exclusion is presented in a PRISMA flow diagram (Figure 1).
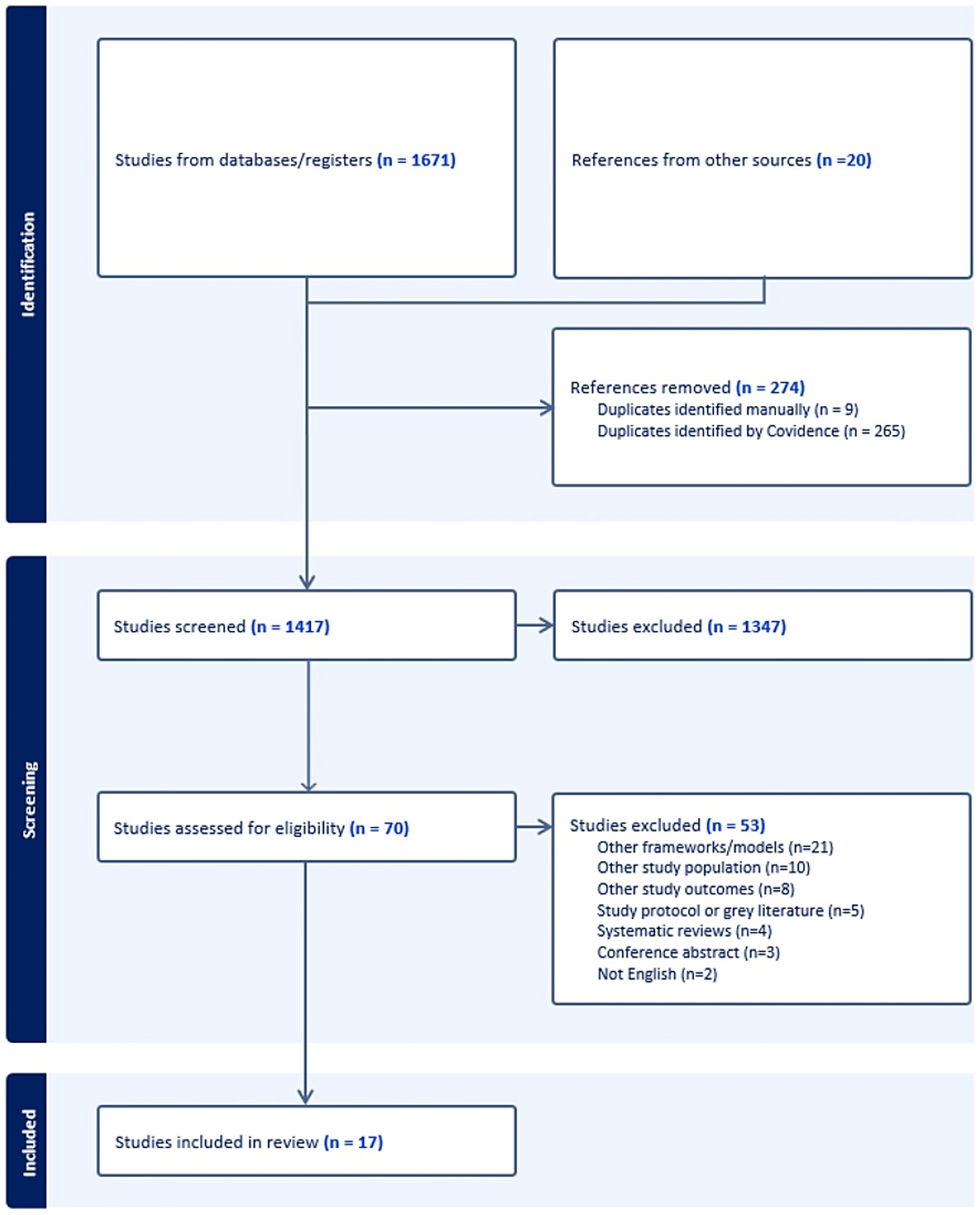
Figure 1. PRISMA flow diagram.
Data analysis
The key characteristics of selected articles were extracted and organized by the main author into a spreadsheet. Data extraction included article identifiers (authors and year of publication), study details (population/sample size, country, objectives, design, data collection methods), type of adversity faced, and key findings. These data were crosschecked by other reviewers (AW, BK, ML, and VP) to discuss and adjust the detailed content. Thematic analysis following the approach proposed by Braun and Clarke (58, 101) was conducted by the same researchers to identify and synthetize the key themes across the selected studies. This method is useful in terms of systematically generating robust research findings by summarizing key features, patterns, common themes, and ideas within and across data, as it forces the researcher to take a well-structured approach to handle data in selected articles (59–62, 104). Using this approach, our study organized major themes to identify how resilience models/frameworks can be applied to address SI/L among older adults (Table 1).
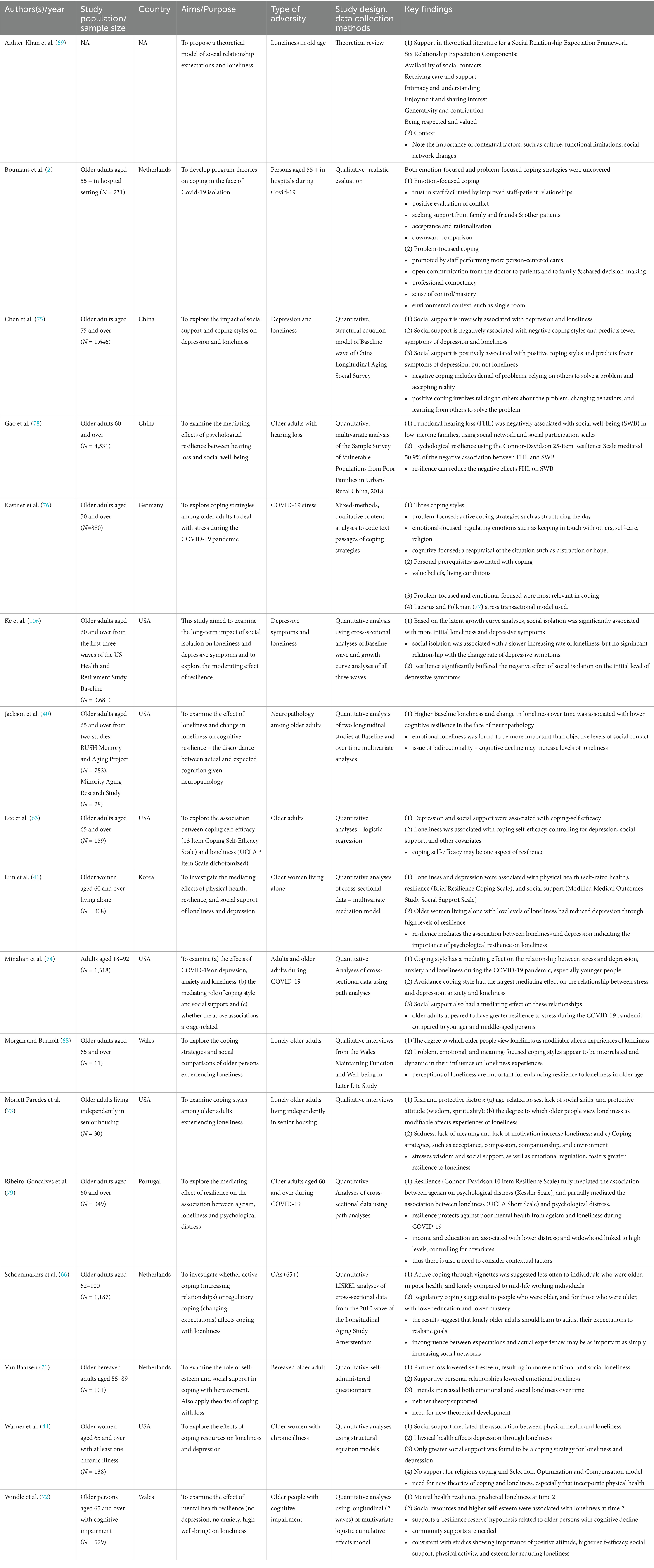
Table 1. Characteristics of included studies.
Results
Description of studies
All 17 papers were published after 2001, with the majority (n = 15; 88.2%) in the last 5 years. Their studies were mainly conducted in Europe (n = 7; 41.2%) and North America (n = 6; 35.3%), but also in Asia (n = 3; 17.6%). Most (n = 12; 70.6%) used a quantitative design, three (17.6%) included qualitative methods, one (5.9%) a mixed-methods design, and one (5.9%) used a theoretical review. With sample sizes ranging from 11 to 4,531 older participants, eight studies (47%) focused on the general population, including one with adults aged 18 and over, and two (11.7%) specifically targeted women. The other studies each (5.9%) targeted: (i) widows, individuals with: (ii) chronic illness, (iii) hearing loss or (iv) cognitive impairment, or people living: (v) alone, (vi) in senior residences or (vii) hospitalized. While six studies (35.3%) investigated resilience in the context of loneliness, including two in the presence of depressive symptoms, three (17.6%) explored the strategies of older adults during the COVID-19 pandemic, and the other seven each focused on the specificity of their target population.
Major thematic conceptual and theoretical developments that connect resilience and aging to social isolation and loneliness
Four themes provided unique resilience components and processes related to SI/L. These include: (1) Coping self-efficacy to reduce SI/L; (2) Moderating expectations to foster resilience to SI/L; (3) Effects of social support, the environment, and resilience on COVID-19 stressors and; (4) Resilience as a mediator between loneliness and aging-related challenges.
Coping self-efficacy to reduce SI/L
Several studies provide theoretical and empirical evidence for the role of coping self-efficacy as a core concept in resilience processes linked to SI/L mitigation. Lee et al. (63) draw on Social Learning Theory developed by Bandura (64), and specifically its extension to coping self-efficacy, which is defined by the authors as “self-confidence in one’s ability to effectively manage challenges using problem-solving, emotional regulation, and coping through social support.” (p. 271). Using the 13-item Coping Self-efficacy Scale (65), the authors provide findings supporting an association between higher levels of problem-solving, emotional regulation, and social support subscales and lower levels of loneliness (63). Schoenmakers et al. (66) distinguish between two styles of coping: active coping which entails enhancing one’s social relationships, and regulative coping which involves lowering expectations pertaining to social relationships. Socio-emotional selectivity theory (67) posits that older people can employ several processes to lower expectations to foster higher levels of well-being. Schoenmakers et al. (66) build on Carstensen’s theory, specifically on the idea that, due to a reduced time perspective, older adults are more inclined toward regulatory adaptation. This involves prioritizing meaningful, high-quality relationships and activities over quantity, fostering immediate well-being and potentially reducing SI/L. Schoenmakers et al. (105) used four vignettes of loneliness experiences to identify their preferred coping styles and found that older adults with lower education and lower mastery more often used regulative coping than the other styles. Morgan & Burholt (68) also examine coping, finding that older adults who are confident that loneliness is modifiable are more likely to engage in a wide range of coping styles. These include problem-solving (e.g., enhancing social relationships), regulatory coping (e.g., lowering expectations of support), and meaning-focused coping (e.g., religiosity). The authors incorporate self-efficacy in terms of learning new coping skills through a computer education program, which was augmented through enhancement of social contacts with other mature students. Taken together, the authors (63, 66, 68) contend that these processes are not separate, but rather, comprise a dynamic process of resilience to reduce social isolation and loneliness.
Modifying expectations to foster resilience to SI/L
A second major theme found in the articles of focus entails assessments and modifications to expectations (toward) and actual social relationships. In a theoretical paper that draws on psychology, gerontology and anthropology, Akhter-Khan et al. (69) develop the Social Relationship Expectation (SRE) framework to understand loneliness in old age from a life span sociocultural perspective. The six identified areas central to appraisals and actual social relationships include availability of contacts, receiving care and support, feeling close and understood, enjoyment and shared interests, generativity, and being respected and valued (69). The authors further contend that culture, functional status, and social network changes over the life course comprise contextual factors affecting relationship expectations among older adults and, ultimately, their loneliness. The primary coping strategies through which older adults adapt to relationship expectation incongruencies to maintain resilience is the Selective Optimization with Compensation (SOC) Model (70). Strategic selection, optimizing one’s available resources, and adapting to losses through compensation adaptation comprise the SOC Model. This model has been used to explain why some older adults during the pandemic adjusted to restricted social isolation by adjusting their expectations, and employing new strategies of communication to mitigate loneliness.
Other articles empirically tested theoretical concepts used to explain coping with loneliness. Focusing on partner loss among older adults, Van Baarsen (71) tests constructs derived from a general coping and specific theory of coping. The Theory of Mental Incongruity in which loneliness is the result of discrepancies between social relations desired and actual ones, contends that, at the general level, having higher self-esteem and social support results in better coping with loss. Similar to the SRE framework, the Theory of Relational Loneliness is a specific approach to loss and recovery that is understood as deficits in attachment, social integration and self-worth that affect identity formation as well as social and emotional loneliness. The equivocal results for both theories suggest a need to better integrate concepts into a more unified theory.
Jackson et al. (40) found that the incongruity between older adults’ actual and expected cognition, given their neuropathology, is deemed to represent cognitive resilience (CR). In other words, those showing cognitive reserve that exceeds their neurological assessments suggests a resilience to detriments linked to brain health. Using two longitudinal data sets, loneliness was associated with lower CR, suggesting that older adults with higher loneliness experienced steeper cognitive decline than expected (40), p. 944. Defining mental health resilience (MHR) as the absence of depression and anxiety and exhibiting high well-being, Windle et al. (72) found in longitudinal data that the odds of MHR were increased in males, and those having higher self-esteem, more social resources and fewer memory complaints. In a qualitative study of loneliness among older adults living in a senior housing community, Morlett Paredes et al. (73) found that aspects of wisdom, through pathways such as spirituality, emotional regulation, self-reflection, decisiveness and compassion, were protective against loneliness. Furthermore, the authors identify coping strategies to mitigate loneliness, including acceptance of aging, compassion, companionship and the role of environmental programming to cultivate meaning and positive relationships were important. In a related study, Morgan and Burholt (68) found that loneliness trajectories in old age are affected by social comparisons and whether or not loneliness is modifiable. Further, Minahan et al. (74) discovered that avoidant coping mediated the effects between pandemic-related stress and psychosocial outcomes, especially depression, although the findings for loneliness were weak. However, one study (75) did not find that positive coping styles affect loneliness, but these did reduce levels of depression in a Chinese sample.
This theme epitomizes several core social-psychological aspects of the resilience-SI/L connection. Enhanced self-esteem and social relationships, and the incongruence and realignment of deficits in social expectation relativity, appear to be core processes underlying this association. In addition, emotional regulation, SOC and wisdom are coping strategies of relevance.
Effects of social support, the environment and resilience on COVID-19 stressors
Three studies specifically address coping styles among older adults to reduce loneliness during the COVID-19 pandemic (2, 74, 76). Boumans et al. (2) and Kastner et al. (76) draw on Lazarus and Folkman’s (77) Stress and Coping Model in which coping resources and styles are viewed as potentially buffering effects between stressors and mental health outcomes. These authors found that emotion-focused and problem-focused coping strategies were employed by older adults to support resilience to loneliness during the pandemic, especially pertaining to long-term care (LTC) where the disease risk was highest. In a qualitative study, Boumans et al. (2) support five emotion-focused coping strategies: trust in staff; positive appraisals and acceptance of the situation; seeking support from family, friends, and other patients; emotional regulation; and positive relative comparisons. Problem-focused coping strategies entail: training of staff to provide personalized care and having familiar staff, provision of information to the patient and family and shared decision-making enhancing sense of control, single room occupancy and personal items to enhance familiarity. In a quantitative study of older people living in the community during the pandemic (76), several coping styles associated with pandemic resilience were identified. Beliefs such as positive attitude, confidence and adaptability, spirituality, and prior experiences with being alone contributed to lower loneliness. Material, living and financial contexts were also important, such as living with others, good health care, better living and housing conditions and financial security, and higher functional mobility and transportation options. Kastner et al. (76) also supported the relevance of psycho-social evaluations of the stressful pandemic events that mitigate loneliness, such as positive appraisals of being alone and lower concerns for threatening aspects of Covid-19. Similar to the prior study, Kastner et al. (76) found that problem-focused approaches included social relationships and keeping busy. Emotion-focused strategies entailed maintaining social contacts, engaging in health behaviors, mindfulness, and spirituality among others. In a quantitative study of pandemic stress on mental health and loneliness and the mediating role of social support and coping style across age, Minahan et al., (74) found that reducing avoidance coping and enhancing social support lower the effect of pandemic stress on loneliness. Older adults reflected greater resilience than younger persons through more positive coping styles, providing support for a stress-coping model.
Coping styles, coupled with social, psychological and financial resources during the pandemic enhance resilience processes that reduced loneliness during the COVID-19 pandemic. This theme emphasizes the importance of linking system-level contexts of social isolation and resilience to adversities nested in the broader socio-ecological domains embedded within individuals, families, communities and the physical environments in which individuals live.
Resilience as a mediator between SI/L and mental health
Several quantitative studies focus on mediation models of resilience on SI/L among older adults facing different types of adversity, including mental health challenges, hearing loss, living alone, ageism, and chronic illness. Ke et al. (106) found support for the mediating effect of resilience on the association between social isolation on depression. For instance, resilience was negatively associated with both the intercept and slope of loneliness (B = −1.15, SE = 0.05, p < 0.001; B = −0.22, SE = 0.03, p < 0.001); and depressive symptoms (B = −0.21, SE = 0.02, p < 0.001; B = −0.07, SE = 0.01, p < 0.001). Psychological resilience also mediated the relationship between hearing impairment and social well-being (social engagement and network characteristics) (78). In addition, Lim et al. (41) showed that physical health, resilience and social support mediated the association between loneliness and depression. Similarly, Warner et al. (44) and Chen et al. (75) showed that social support mediated the association between loneliness and depression, suggesting a resilience process among older adults. In a parallel study, Ribeiro-Gonçalves et al. (79) demonstrated that resilience also mediated the relationship between the effect of loneliness on psychological distress.
This theme positions resilience as an important mediator that can reduce the negative effect of SI/L on deleterious mental health outcomes among older people. Some studies utilize individual resilience measures, such as the Connor-Davidson Resilience Scale, whereas others used ecological resilience measures, and one employed social support as a proxy for resilience.
Discussion
Theoretical building blocks and gaps
This scoping review focuses on resilience and coping/adaptive theoretical applications applied to social isolation and loneliness among older adults. Taken together, the theoretical developments connecting resilience and SI/L have primarily drawn from psychological or social psychological approaches, including five primary theoretical models (see Figure 2). Akhter-Khan et al.’s (69) Social Relationship Expectation (SRE) framework; Lazarus and Folkman’s (77) Stress and Coping Model; Bandura’s (64) Social Learning Theory (especially self-efficacy concepts); Selective Optimization with Compensation Model (70); and Socio-emotional Selectivity Theory (67). In addition, empirically driven mediation models have also positioned resilience and social support as buffers between adversity stress and SI/L, either explicitly or implicitly framed using a Stress-Coping Model.
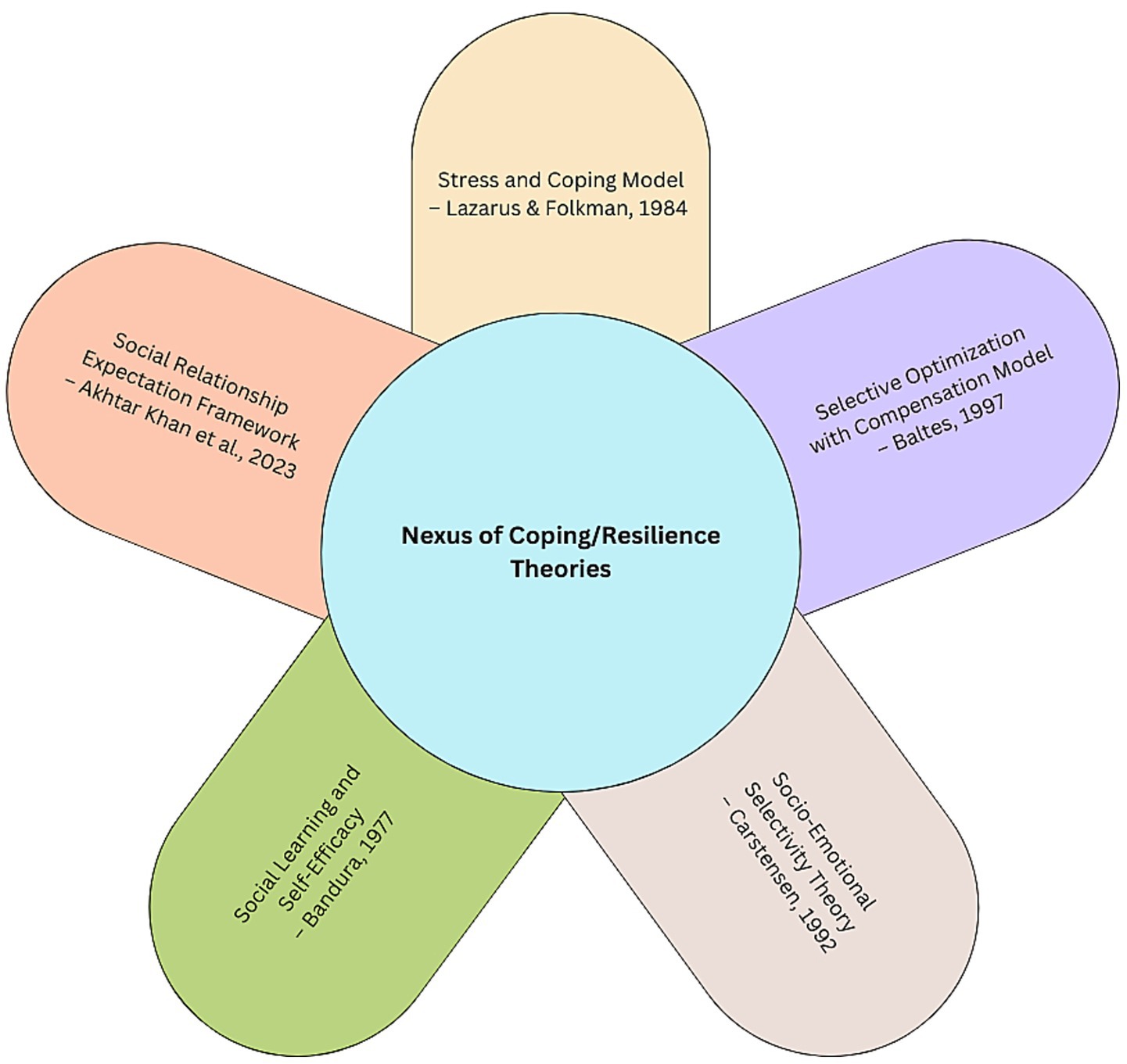
Figure 2. Coping and resilience theories applied to social isolation and loneliness.
The conceptual and theoretical applications identify protective factors (e.g., strong self-efficacy, robust social relationships, positive attitude, etc.); coping strategies (e.g., problem-focused and emotional focused approaches; emotional regulation, expectation control, health behaviors, etc.); and environmental, financial and structural contexts (e.g., housing, LTC staffing, financial capital, etc.). While the themes overlap to some degree, they point to several central factors and processes that can be employed to enhance resilience to mitigate SI/L. Coping self-efficacy linked to both emotional and problem-solving is influenced by psycho-social attributes of the individual coupled with the role of social support. This core theoretical building block is important for the management of expectations. Additionally, the SRE emphasizes the regulation of expectations to align with social contexts in which older adults find themselves. Targeted selection and optimization with compensation where needed fosters greater adaptation to SI/L adversities. Thus, dealing with the incongruities of expected and actual social relationships and realignment of these manifests into improved resilience to SI/L. Stress and coping framing of SI/L points to the importance of buffering effects, which may include social support but also resilience facets. In addition, the pandemic-related stressors that exasperated SI/L were often structural in nature and point to the importance of moving beyond social-psychological resilience and coping to a system-level lens. For instance, the preparedness and adaptability of long-term care environments (e.g., personal protective equipment access and use, staff training, number of residents per room, and rapid response ability) during the COVID-19 lockdown phase directly affected the resilience processes of older people. All of these conceptual and theoretical developments occur against the backdrop of various social, environmental and physical contexts. In other words, it is understood that psycho-social coping and resilience attributes and processes can not be understood outside of the broader socio-ecological environments in which aging occurs.
Limitations
Several limitations affect the integration and application of these conceptual developments. First, while we specify research findings focusing on social isolation, loneliness or both, and integrate the results into an SI/L combined model, there may be nuanced theoretical implications for each concept. Second, the majority fall within a specific discipline, especially psychology. There is a gap in unifying theoretical developments that occur within a primarily siloed disciplinary context. Third, the broader socio-ecological domains, such as age-friendly community contexts, rurality, and the physical environment, have not been centrally positioned, although some of these environmental contextual factors were incorporated into Kastner et al.’s (76) and Boumans et al.’s (2) articles. This could be due to the limited amount of public health literature on resilience and social isolation and loneliness. Fourth, there have been few attempts to connect the micro and macro environmental contexts of the nexus of resilience and SI/L, although pandemic research has given attention to system-level factors affecting SI/L. Fifth, resilience has been measured in several different ways (e.g., Connor-Davidson Resilience Measure, short resilience scale, proxy variables such as social support, etc.), making comparison between studies’ results difficult. Sixth, measures social isolation and loneliness also differ across studies, such that interpretations need to be made with care. Seventh, resilience and social isolation theoretical connections need to apply to a broad range of adversities, ranging from individual-level mental health and cognitive challenges to disaster research, such as pandemics, climate change adversities, and other catastrophes. Further specification of the model may be required in future research. Seventh, many studies reviewed included both depression and SI/L, which convoluted some of the theoretical interpretations. Eighth, the role of prevention to protect against adversity stressors (e.g., COVID-19 shutdowns), versus active resilience coping processes (e.g., realigning expected and actual levels of social connections during the pandemic) have not been clearly delineated in the literature. Finally, our scoping review itself is limited by the data used (e.g., these may have resulted in a bias toward social-psychological approaches to resilience and SI/L), the possibility of missing relevant articles in the search strategy, and our interpretation of the themes.
Toward an integrated resilience and social isolation model of aging
The development of theoretical work in this field exposes an opportunity for an integrated theoretical model of resilience and SI/L. Currently in the literature on social isolation and loneliness, there has been an absence of an interdisciplinary model that bridges psychological, social, environmental and socio-ecological domains. We aim to fill this void by connecting the themes identified in this scoping review into an integrated resilience and SI/L model applied to aging.
One recent theoretical framework positioned within the resilience and aging literature that has the potential for application to SI/L is the Unified Model of Resilience and Aging (UMRA) (48). This interdisciplinary model was developed and applied to adversities created by the COVID-19 pandemic including SI/L, and can be applied to a range of adversities (48). The UMRA guides the understanding of why some individuals, families, and communities adapt, recover, and sometimes grow out of adversity, and the attributes and processes that facilitate positive responses. Given that this model integrates individual and system-level processes that occur over the life course, it also responds to the themes and gaps revealed in the scoping review.
Figure 3 presents an integrated model called the Resilience and Social Isolation Model of Aging (RSIMA), which is built on the scoping review and imputed into the UMRA. We use ‘social isolation’ in the title to capture both social isolation and loneliness. The primary difference between the UMRA and this proposed resilience model applied to SI/L entails the specification of the individual-level resilience processes based on this scoping review, and applying these to the original model. The central circle in Figure 3 of our proposed RSIMA model presents these individual resilience processes, some of which overlap the UMRA and three of which are unique. First, the RSIMA includes protective/preventive factors and mechanisms as a key component based on the scoping review results, in particular, the importance of social support. Second, we have incorporated emotional regulation with the adaptation and coping process consistent with our results depicted in Figure 2. Finally, RSIMA incorporates reintegration with wellness, recovery and growth to reflect the interconnections of these components as part of the final stages of the individual resilience processes.
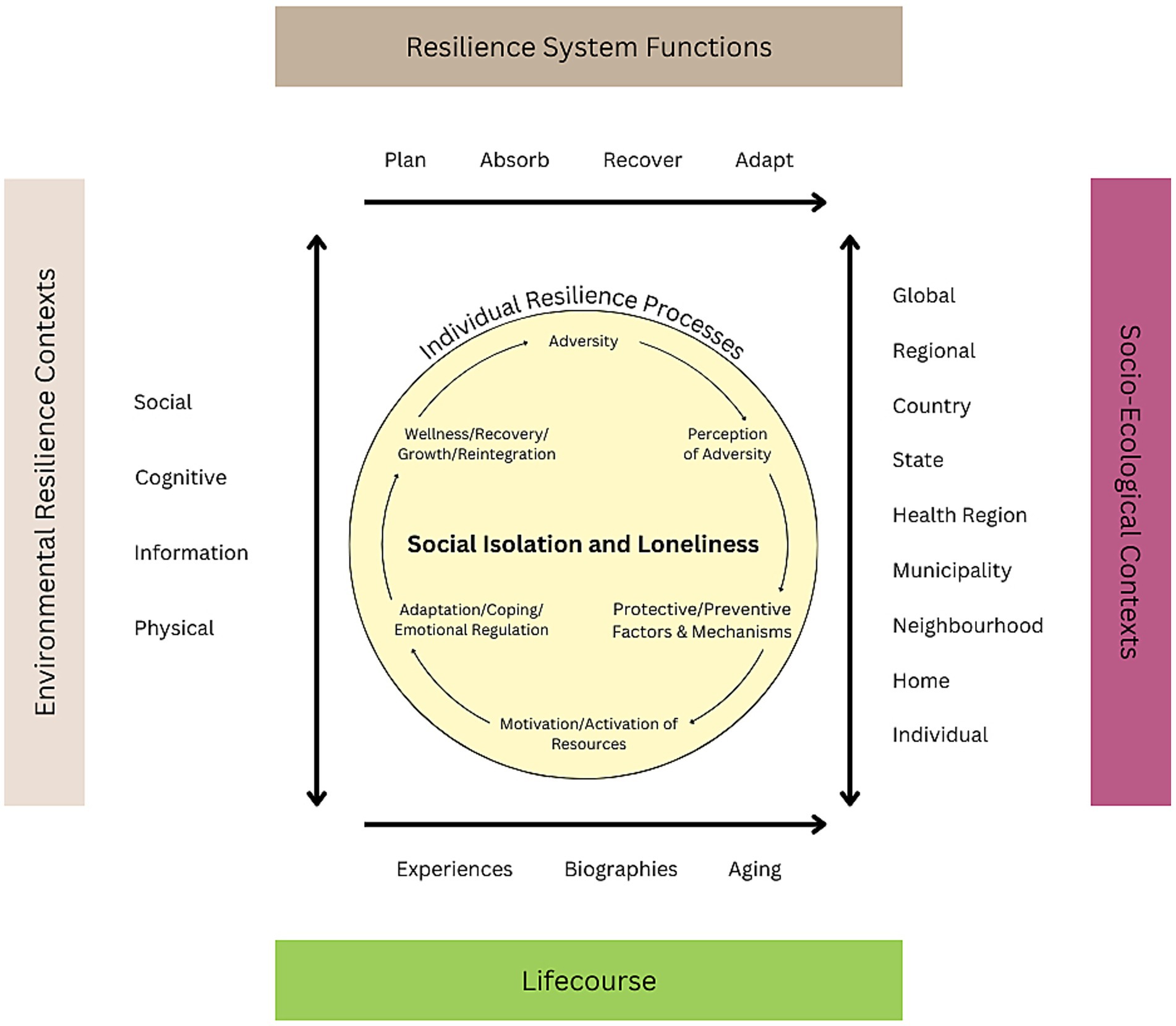
Figure 3. Resilience and social isolation model of aging.
The processes presented in the inner circle of Figure 3 demonstrate that, in response to SI/L adversity, resilience depends on (a) perceptions of the adversity (e.g., expectation realignment, severity, seriousness); (b) protective/preventive factors and behaviors (e.g., positive attitude, previous successful coping experiences); (c) potential disruption (e.g., disturbance to social roles, status, cognitive and physical health); (d) the activation of internal resources (e.g., self-efficacy, motivation to change attitude or behavior; and activation of external resources (e.g., buffering of stress and social support from family, friends, communities or organization, health behaviors); and (e) adaptation/coping/emotional regulation (emotional and problem-solving coping, selective optimization with compensation, buffering effects). The above processes culminate to affect wellness/recovery/growth, and reintegration).
The outer sections of the RSIMA model shown in Figure 3 borrows from the original UMRA model (48), which incorporates the primary system-level contexts within which individual processes are manifested (51). These align with the scoping themes pertaining to structural and socio-ecological contexts, especially related to, but not exclusive to, pandemic-related stressors that exasperated SI/L. These entail: (1) Resilience System Functions drawn from the US National Academy of Sciences Resilience formulation (plan, absorb, recover, and adapt) that was further codified in the US National Resilience Strategy (80); (2) the Socio-ecological spectrum from individual to global; (3) Environmental Resilience Contexts (social, cognitive, information and physical); and (4) Lifecourse temporal elements (experiences, biographies, aging). Specific to disaster research, including the recent COVID-19 pandemic, this resilience framing (51, 52) emphasizes: (1) Planning for adverse events requires reductions in risk in response to an identified threat, (2) Absorption of stressors and outcomes associated with adversity is necessary to initiate resilience through recovery and adaptation, (3) Recovery occurs through various forms of short and long-term strength-based resilience, and (4) Adaptation relates to changes in the system to promote future resilience. The coping processes are shaped by the socio-environmental contextual areas and the experiences, biographies, and aging processes embedded in the life courses of individuals.
Thus, this model highlights the dynamic multifaceted associations between social isolation, loneliness, and broader social determinants of health. It helps to frame our understanding of not only the causes of SI/L but also the effects of SI/L on the lives and experiences of aging and older adults. RSIMA emphasizes that individual-level resilience (i.e., psychological factors, physical health, life course changes, etc.) is intricately linked with community-level resilience (i.e., social factors of vulnerability, presence of robust safety net programs, etc.). Most existing models on resilience and SI/L do not use a systems-level approach. While individual-level factors are important in overcoming adversity, many broader upstream factors can have increasingly pronounced effects over the course of an individual’s life span (i.e., lack of health insurance or limited access to healthcare, poverty, non-English speaking populations, climate-induced changes to Indigenous peoples’ ways of life, etc.). Politics, programs, and greater global crises such as climate change are outside of a single person’s direct control, but they can directly impact both an individual’s level of resilience and a community’s ability to bounce back and adapt to any disruptions in their critical functioning (e.g., an area that burned down from wildfires).
Applications to social isolation and loneliness
The causes and consequences of SI/L can be understood from the RSIMA—a dynamic interdisciplinary integrative model that recognizes the socio-environmental and system-level contexts in which individuals engage in a variety of coping and adaptive resilience processes that are cumulative across the life course. These multilayered contexts comprising the RSIMA are specifically linked to the type, severity, and source of adversity, for instance, pandemic-related SI/L has unique properties compared to SI/L occurring during different periods or different contexts (e.g., individual, community, LTC).
The RSIMA framework adds to the understanding of theoretical and empirical work on SI/L applied to older adults in a number of significant ways. The expanding literature on social isolation and loneliness has been preoccupied with primarily identifying the risk and protective factors associated with SI/L, their consequences for health and well-being, as well as a variety of interventions [(e.g., 8, 9, 17, 19, 81, 82)]. This is evidenced in over 30 systematic and scoping reviews pre-, peri-, and post COVID-19 pandemic [(see 4, 13, 21, 83–85)]. However, much of this work has been empirically driven and typically has been located within disciplinary silos. The RSIMA offers an interdisciplinary, integrative framework with a resilience process lens applied to SI/L among older adults emphasizing a strength-based approach that can guide our understanding of the causes and consequences of SI/L and the development of practice and policy interventions. To this point, this model points toward the ways in which we can enhance coping processes to overcome the adversity embedded in SI/L.
Specifically, the RSIMA articulates protective and risk factors that reduce adversity associated with SI/L; reactive factors in response to adversity; activation of domain-specific resources; and adaptive processes in the formation of resilience. All of these lead to wellness, recovery, growth or reintegration in response to SI/L. Environmental risk factors, living alone, living in rural/remote areas, community and social deprivation, pandemic and other government policies, and other environmental adversities can increase the risk of SI/L among older adults (13, 72). Yet, these are interpreted as interacting with resilience strengthening protective and reactive factors, processes, and resources that can be activated, for instance, the existence or development of robust social support systems (71, 75), healthy lifestyles (48), and human and financial capital (79). Furthermore, these socio-environmental and resource-based domains shape and are interpreted through coping or adaptive social psychological resilience processes, such as realigning expectations against actual realities (2, 68, 76). For example, research suggests that older adults adapted well to isolating pandemic policies relative to other age groups since they adjusted expectations and drew upon life experiences of SI/L (74, 76). In this sense, the model provides a rationale for prevention, as well as proactive and reactive responses.
Furthermore, the RSIMA can be applied to this form of adversity to predict the potential outcomes of SI/L on older individuals, or the mediating or buffering effects of resilience on mental health, such as depression and anxiety (23, 41, 75, 86), and physical health, such as challenges to functional disability (4, 41, 87). In part, this is due to the dynamic reciprocal associations between SI/L and mental and physical health (19, 48). Additionally, as evidenced in the thematic analysis, the mediating role of resilience may interpret or buffer associations between risk factors, such as a functional hearing loss or cognitive decline, and SI/L (75, 78, 79, 106).
Finally, this model can also be potentially useful to analyze and guide the strategies that various organizations (e.g., community organizations, LCT, allied health and social services) use to adapt their services to promote the resilience of older adults in situations of SI/L or at risk of SI/L during and beyond a pandemic (88). Notably, this model can help different organizations visualize and understand the need for more interconnected services and improved collaboration and coordination across actors and organizations to meet not just individual needs but also population health needs for older adults.
For instance, hearing loss as a form of adversity has been associated with SI/L and cognitive decline (89); yet gaps remain in reducing the social, psychological, and physical effects of hearing loss. A resilience approach directs interventions to address this area through coordinated programs across multiple sectors (e.g., media campaigns, community services, government policies) at the individual, family, community, and system level. Based on RSIMA, these mechanisms can raise awareness, shift attitudes pertaining to hearing loss such as reduce stigma, enhance hearing testing and uptake of hearing aid use prior to deleterious effects on SI/L, and foster innovation in reaching hard-to-reach populations. Individuals can enhance their resilience to hearing loss effects on SI/L by also shifting their emotional regulation, attitudes and expectations, forms of individual adaptation and coping that are highly influenced by their social networks and support levels. Access to hearing aids, and the training and educational components needed for effective use, emphasize the salience of resource activation. Policy changes, such as health care insurance or policy changes to maximize coverage of hearing aids, represent the system-level of the model. These resilience factors and processes applied to hearing loss and cognition require future research to fine-tune the most effective mechanisms.
A major impediment to the development of programs and policies that aim to foster resilience and tackle SI/L are siloed and do not use a systems-level approach. With the growth in climate-driven crises (i.e., wildfires, heatwaves, avian flu) and the complex political challenges (i.e., migration, refugees, homelessness) that they create, strategies to bolster resilience in older adults will require a multi-sectoral approach that engages a broad group of stakeholders. Combating SI/Lin older populations will require strong collaborations between public health agencies and emergency management agencies, as well as private actors and non-governmental organizations.
Formulating a theory-driven research agenda
Several research gaps can be identified and filled based on the RSIMA. First, comparative research needs to be conducted on different types, severity, and origins of SI/L. For example, current and future pre-pandemic, peri-pandemic, and post-pandemic SI/L adversity have both unique and shared elements. Pre-pandemic SI/L has been shown to have several predictors related to demographic, social, psychological, and environmental vectors often related to risk, marginalization, and vulnerability. Since pandemic-induced SI/L originated through government and public policy, there are likely nuanced experiences that may reveal new patterns of SI/L, as well as others that are similar to prior patterns but exacerbated. Post-pandemic SI/L may be a blending of the former types. More research that examines the effectiveness and the impacts of policies and programs that aim to increase resilience and decrease social isolation among older adults is needed. While resilience is a known concept among public health practitioners, it is a relatively new public health policy priority. Second, research is needed that employs an interdisciplinary lens to integrate the multilevel facets of SI/L stemming from this model. This requires data sets, in particular longitudinal data, that capture these contexts in conjunction with different designs and methods (e.g., multi-methods). Third, the assessment of risk for SI/L requires the development of indices that capture the different contexts in which it occurs, such as cultural, economic, and psychological ones (87, 90). One research gap is the investigation into inequality and diversity, such as gender, race, ethnicity, socio-economic status and other measures. Fourth, new data sources that contain complex multilevel measures (e.g., Artificial Intelligence to integrate multiple big data; national interdisciplinary longitudinal studies) are needed to reveal the complex interactions that are often overlooked in most statistical models. Fifth, although fixed variables are important in describing those at risk and forecasting trends (e.g., rates of living alone or singledom across age), there is a significant gap in knowledge about modifiable risk or protective factors, and how these factors are linked with higher level system components. Sixth, longitudinal interdisciplinary data are imperative to disentangle age, period, and cohort patterns in the predictors, contexts, and patterns of SI/L. For instance, shifts in systemic ageism in society over time may profoundly affect the prevalence and consequences of SI/L. Additionally, declining birth rates in some countries, particularly across Asia, are leading to a growing cohort of childless older peoples who will need to rely on non-traditional family structures and caregiving (91–93). Seventh, both basic and applied research are required to provide research evidence supporting this model, and the development, implementation, and evaluation of programs and interventions aimed at mitigating SI/L. Finally, policy research can assess the strengths and weaknesses of current approaches and point to the most promising and impactful innovations on the horizon. Our proposed and other theories and models of resilience across the life course need to be operationalized into actual policies and programs. Additionally, little is known about effective governance models that help support resilient communities. Future research should explore existing initiatives across urban and rural areas that aim to improve either resilience (overall) or social isolation in aging populations, identifying which actors are involved, what governance models look like, and whether these models promote a systems-level approach toward increasing resilience across the lifespan. Additionally, future research should also explore the role of multiple and/or cumulative crises on individual and community resilience. Short-term crisis governance can have important policy impacts that can either hinder or promote resilience as compound disasters increase in frequency and intensity over time (94).
Conclusion
Neither Canada nor the United States have a comprehensive national policy that addresses social isolation and loneliness in older populations. While the US released its Federal Action Plan for Suicide Prevention in 2024 (95), SI/L is not directly addressed or discussed. In 2023, the US Surgeon General declared SI/L a key public health concern and released the first US national strategy to advance social connection (96). However, this strategy is yet to be operationalized and implemented across all US states. In 2024, the Canadian Coalition for Seniors’ Mental Health (CCSMH) established its first ever clinical guidelines on SI/L (81). However, similar guidelines for increasing social connection (and addressing SI/L) in older adults at a population health scale have yet to be created by public health agencies. SI/L is a growing public health concern with not only individual-level health consequences but broader societal impacts such as increased political polarization, decreased trust in institutions, and democratic backsliding or erosion.
The theoretical developments of the nexus of resilience and SI/L have grown rapidly in recent years. Understanding social connection—its structure, function, and quality—as well as the root causes of social isolation and loneliness are critical research priorities (96). SI/L are intricately linked to broader social determinants of health. This has been particularly apparent since the COVID-19 pandemic revealed significant individual and system-level gaps in knowledge, especially related to SI/L among older adults. These gaps in knowledge will only grow in importance as climate change and related crises grow, including the increased individual and societal risks related to compound disasters. For example, SI/L and social connection are found to contribute toward a community’s resilience (or lack thereof) to external crises such as natural disasters and other hazards (97–100). Most of the four themes that we identified focus on social psychological resilience and coping processes and mechanisms. There is a gap in existing research in exploring SI/L from a socio-ecological and system-level perspective.
The Resilience and Social Isolation Model of Aging (RSIMA) is an original theoretical framing that integrates interdisciplinary theories with a socio-ecological framing of resilience as a core component of social isolation, loneliness and social connectedness among older adults. RSIMA helps highlight how SI/L is a dynamic process on a continuum, as well as understand what broader factors can lead to improved social connection, contributing to both individual-level and community resilience. It is recognized that there have been public health interventions to address SI/L (e.g., UK Campaign to End Loneliness) that incorporate an integrative approach; however, many of these have not explicitly focused on older adults. Also, the limitations of this scoping review noted above warrant supplementary study in this field. Further empirical evidence, particularly using sophisticated systems-level analytic models in conjunction with social-psychological models, is needed to test the propositions drawn from this model. Future research studies must consider an integrated perspective to SI/L resilience to develop effective policies, programs, and interventions that address the public health crisis of social isolation and loneliness among older people.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AW: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – original draft, Writing – review & editing. BK: Data curation, Formal analysis, Methodology, Writing – original draft. ML: Conceptualization, Writing – review & editing. VP: Writing – review & editing. SQ: Writing – review & editing. EY: Data curation, Methodology, Writing – review & editing. SM: Writing – review & editing. JB: Writing – review & editing. LK: Writing – review & editing. KK: Writing – review & editing. IL: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1589781/full#supplementary-material
Footnotes
References
1. National Institute on Aging. (2023). Perspectives on growing older in Canada: the 2023 aging in Canada survey. Available online at: https://www.niageing.ca/2023-annual-survey (Accessed 9th. July 2024)
2. Boumans, J, Scheffelaar, A, van Druten, VP, Hendriksen, THG, Nahar-van Venrooij, LMW, and Rozema, AD. Coping strategies used by older adults to deal with contact isolation in the hospital during the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:7317. doi: 10.3390/ijerph18147317
3. Kannan, VD, and Veazie, PJ. US trends in social isolation, social engagement, and companionship⎯ nationally and by age, sex, race/ethnicity, family income, and work hours, 2003–2020. SSM-Population Health. (2023) 21:101331. doi: 10.1016/j.ssmph.2022.101331
4. Courtin, E, and Knapp, M. Social isolation, loneliness, and health in old age: a scoping review. Health Soc Care Community. (2017) 25:799–812. doi: 10.1111/hsc.12311
5. Cornwell, EY, and Waite, LJ. Social disconnectedness, perceived isolation, and health among older adults. J Health Soc Behav. (2009) 50:31–48. doi: 10.1177/002214650905000103
6. Rico-Uribe, LA, Caballero, FF, Martin-Maria, N, Cabello, M, Ayuso-Mateos, JL, and Miret, M. Association of loneliness with all-cause mortality: a meta-analysis. PLoS One. (2018) 13:e0190033. doi: 10.1371/journal.pone.0190033
7. Steptoe, A, Shankar, A, Demakakos, P, and Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proceed National Acad Sci-PNAS. (2013) 110:5797–801. doi: 10.1073/pnas.1219686110
8. Holt-Lunstad, J. Loneliness and social isolation as risk factors: the power of social connection in prevention. Am J Lifestyle Med. (2021) 15:567–73. doi: 10.1177/15598276211009454
9. Holt-Lunstad, J, and Perissinotto, C. Social isolation and loneliness as medical issues. N Engl J Med. (2023) 388:193–5. doi: 10.1056/NEJMp2208029
10. Wister, A, Li, L, Levasseur, M, Kadowaki, L, and Pickering, J. The effects of loneliness on depressive symptoms among older adults during COVID-19: longitudinal analyses of the Canadian longitudinal study on aging. J Aging Health. (2023) 35:439–52. doi: 10.1177/08982643221129686
11. U.S. Surgeon General’s Office. Our epidemic of loneliness and isolation: The U.S. Surgeon general’s advisory on the healing effects of social connection and community. Washington, DC: Office of the U.S. Surgeon General (2023).
12. Chawla, K, Kunonga, TP, Stow, D, Barker, R, Craig, D, and Hanratty, B. Prevalence of loneliness amongst older people in high-income countries: a systematic review and meta-analysis. PLoS One. (2021) 16:e0255088. doi: 10.1371/journal.pone.0255088
13. Kadowaki, L, and Wister, A. Older adults and social isolation and loneliness during the COVID-19 pandemic: an integrated review of patterns, effects, and interventions. Canadian J Aging / La Revue canadienne du vieillissement. (2022) 42:199–216. doi: 10.1017/S0714980822000459
14. Dahlberg, L, McKee, KJ, Frank, A, and Naseer, M. A systematic review of longitudinal risk factors for loneliness in older adults. Aging Ment Health. (2021) 26:225–49. doi: 10.1080/13607863.2021.1876638
15. De Jong Gierveld, J, Keating, N, and Fast, JE. Determinants of loneliness among older adults in Canada. Can J Aging. (2015) 34:125–36. doi: 10.1017/S0714980815000070
16. Donovan, NJ, and Blazer, D. Social isolation and loneliness in older adults: review and commentary of a national academies report. Am J Geriatr Psychiatry. (2020) 28:1233–44. doi: 10.1016/j.jagp.2020.08.005
17. National Seniors Council (2016) Who’s at Risk and What Can Be Done about It? A Review of the Literature on the Social Isolation of Different Groups of Seniors. Available online at: https://www.canada.ca/en/national-seniors-council/programs/publications-reports/2017/review-social-isolation-seniors.html (Accessed October 14, 2024).
18. Choi, EY, Farina, MP, Wu, Q, and Ailshire, J. COVID-19 social distancing measures and loneliness among older adults. J Gerontol: Series B. (2021) 77:e167–78. doi: 10.1093/geronb/gbab009
19. Kirkland, S, Griffith, L, Oz, E, Thompson, M, Wister, A, Kadowaki, L, et al. Increased prevalence of loneliness and associated risk factors during the COVID-19 pandemic: findings from the Canadian longitudinal study on aging (CLSA). BMC Public Health. (2023) 23:872–2. doi: 10.1186/s12889-023-15807-4
20. Wister, AV, and Kadowaki, L. Social isolation among older adults during the pandemic. Employment and Social Development Canada. (2021).
21. Pickering, J, Wister, A, O’Dea, E, and Chaudhury, C. Social isolation and loneliness among older adults living in rural areas during the COVID-19 pandemic: a scoping review. BMC Geriatr. (2023) 23:1–511. doi: 10.1186/s12877-023-04196-3
22. Georgeou, N, Schismenos, S, Wali, N, Mackay, K, and Moraitakis, E. A scoping review of aging experiences among culturally and linguistically diverse people in Australia: toward better aging policy and cultural well-being for migrant and refugee adults. The Gerontologist. (2023) 63:182–99. doi: 10.1093/geront/gnab191
23. Li, K, Tang, F, Albert, SM, Rauktis, ME, and Ohmer, ML. Social isolation, loneliness, and depressive symptoms among older adults: the moderating effect of resilience. The Gerontologist. (2024) 64:1–10. doi: 10.1093/geront/gnae056
24. Li, L, Wister, A, and Mitchell, B. Social isolation among spousal and adult-child caregivers: findings from the Canadian longitudinal study on aging. J Gerontol: Series B. (2020) 76:1415–29. doi: 10.1093/geronb/gbaa197
25. Burholt, V, Winter, B, Aartsen, M, Constantinou, C, Dahlberg, L, Feliciano, V, et al. A critical review and development of a conceptual model of exclusion from social relations for older people. Eur J Ageing. (2019) 17:3–19. doi: 10.1007/s10433-019-00506-0
26. Levasseur, M, Cohen, AA, Dubois, MF, Généreux, M, Richard, L, Therrien, FH, et al. Environmental factors associated with social participation of older adults living in metropolitan, urban, and rural areas: the NuAge study. Am J Public Health. (2015) 105:1718–25. doi: 10.2105/AJPH.2014.302415
27. Levasseur, M, Roy, M, Michallet, B, St-Hilaire, F, Maltais, D, and Généreux, M. Associations between resilience, community belonging, and social participation among community-dwelling older adults: results from the eastern townships population health survey. Arch Phys Med Rehabil. (2017) 98:2422–32. doi: 10.1016/j.apmr.2017.03.025
28. Van Tilburg, TG, Steinmetz, S, Stolte, E, van der Roest, H, and de Vries, DH. Loneliness and mental health during the COVID-19 pandemic: a study among Dutch older adults. J Gerontol B Psychol Sci Soc Sci. (2021) 76:e249–55. doi: 10.1093/geronb/gbaa111
29. Coughtrey, A., Birken, M., Steare, T., Bennett, S., and Johnson, S. (2019) Initial evidence review – strategies for encouraging psychological and emotional resilience in response to loneliness Available online at: https://www.ucl.ac.uk/psychiatry/sites/psychiatry/files/evidence-synthesis-for-psychology-of-loneliness-report.pdf (Accessed October 14, 2024).
30. Ibarra, F, Baez, M, Cernuzzi, L, and Casati, F. A systematic review on technology-supported interventions to improve old-age social wellbeing: loneliness, social isolation, and connectedness. J Healthcare Eng. (2020) 2020:1–14. doi: 10.1155/2020/2036842
31. Strutt, PA, Johnco, CJ, Chen, J, Muir, C, Maurice, O, Dawes, P, et al. Stress and coping in older Australians during COVID-19: health, service utilization, grandparenting, and technology use. Clin Gerontol. (2021) 45:106–19. doi: 10.1080/07317115.2021.1884158
32. Shih, RA, Acosta, JD, Chen, EK, Carbone, EG, Xenakis, L, Adamson, DM, et al. Improving disaster resilience among older adults: insights from public health departments and aging-in-place efforts. Rand Health Q. (2018) 8
34. Herrman, H, Stewart, D, Diaz-Granados, N, Berger, E, Jackson, B, and Yuen, T. What is resilience? Can J Psychiatr. (2011) 56:258–65. doi: 10.1177/0706743711056005
35. Luthar, SS, and Brown, P. Maximizing resilience through diverse levels of inquiry: prevailing paradigms, possibilities and priorities for the future. Dev Psychopathol. (2007) 19:931–55. doi: 10.1017/S0954579407000454
36. Masten, A. Ordinary magic: resilience processes in development. Am Psychol. (2001) 56:227–38. doi: 10.1037/0003-066X.56.3.227
37. Masten, A. Resilience in developing systems: progress and promise as the fourth wave rises. Dev Psychopathol. (2007) 19:921–30. doi: 10.1017/S0954579407000442
38. Richardson, GE. The metatheory of resilience and resiliency. J Clin Psychol. (2002) 58:307–21. doi: 10.1002/jclp.10020
39. Infurna, FJ. Utilizing principles of life-span developmental psychology to study the complexities of resilience across the adult life span. The Gerontologist. (2021) 61:807–18. doi: 10.1093/geront/gnab086
40. Jackson, KL, Luo, J, Willroth, EC, Ong, AD, James, BD, Bennett, DA, et al. Associations between loneliness and cognitive resilience to neuropathology in older adults. J Gerontol B Psychol Sci Soc Sci. (2023) 78:939–47. doi: 10.1093/geronb/gbad023
41. Lim, YM, Baek, J, Lee, S, and Kim, JS. Association between loneliness and depression among community-dwelling older women living alone in South Korea: the mediating effects of subjective physical health, resilience, and social support. Int J Environ Res Public Health. (2022) 19:9246. doi: 10.3390/ijerph19159246
42. Ong, AD, Bergeman, CS, and Boker, SM. Resilience comes of age: defining features in later adulthood. J Pers. (2009) 77:1777–804. doi: 10.1111/j.1467-6494.2009.00600.x
43. Seong, H, Lashley, H, Bowers, K, Holmes, S, Fortinsky, RH, Zhu, S, et al. Resilience in relation to older adults with multimorbidity: a scoping review. Geriatr Nurs. (2022) 48:85–93. doi: 10.1016/j.gerinurse.2022.08.017
44. Warner, CB, Roberts, AR, Jeanblanc, AB, and Adams, KB. Coping resources, loneliness, and depressive symptoms of older women with chronic illness. J Appl Gerontol. (2019) 38:295–322. doi: 10.1177/0733464816687218
45. Windle, G. What is resilience? A review and concept analysis. Rev Clin Gerontol. (2011) 21:152–69. doi: 10.1017/S0959259810000420
46. Windle, G. The contribution of resilience to health ageing. Perspect Public Health. (2012) 132:159–60. doi: 10.1177/1757913912449572
47. Wister, A, Coatta, K, Schuurman, N, Lear, S, Rosin, M, and MacKey, D. A Lifecourse model of multimorbidity resilience: theoretical and research developments. Int J Aging Hum Dev. (2016) 82:290–313. doi: 10.1177/0091415016641686
48. Wister, A, Klasa, K, and Linkov, L. A unified model of resilience and aging: applications to COVID-19. Front Public Health. (2022) 886:1–14. doi: 10.3389/fpubh.2022.865459
49. Linkov, I, Keenan, J, and Trump, BD. COVID-19: Systemic risk and resilience. Amsterdam: Springer (2021).
50. Sells, D, Sledge, W, Wieland, M, Walden, D, Flanagan, E, Miller, R, et al. Cascading crises, resilience, and social support within the onset and development of multiple chronic conditions. Chronic Illn. (2009) 5:92–102. doi: 10.1177/1742395309104166
51. Klasa, K, Galaitsi, S, Wister, A, and Linkov, I. System models for resilience in gerontology: application to the COVID-19 pandemic. BMC Geriatr. (2021) 21:51–1. doi: 10.1186/s12877-020-01965-2
53. Peters, MD, Godfrey, C, McInerney, P, Munn, Z, Tricco, AC, and Khalil, H. Scoping reviews. JBI Manual for Evidence Synthesis. (2020) 169:467–73. doi: 10.46658/JBIMES-20-12
54. Arksey, H, and O’Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
55. Tricco, A., Strauss, S., and Moher, D. (2015). Preferred reporting items for systematic reviews and Meta-analysis: Extension for scoping reviews (PRISMA-ScR)Universit. Y of Oxford, London: Enhancing the QUAlity and transparency of Health Research (EQUATOR) network, Centre for Statistics in medicine, NDORMS. Available online at: http://www.equator-network.org/library/reporting-guide-lines-under-development/#55 (Accessed on October 14, 2024)
56. Babineau, J. Product review: Covidence (systematic review software). J Canadian Health Libraries Assoc/Journal de l'Association des bibliothèques de la santé du Canada. (2014) 35:68–71. doi: 10.5596/c14-016
57. Kellermeyer, L, Harnke, B, and Knight, S. Covidence and rayyan. J Medical Library Assoc: JMLA. (2018) 106:580–3. doi: 10.5195/jmla.2018.513
58. Braun, V, and Clarke, V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
59. Clarke, V, Braun, V, and Hayfield, N. Thematic analysis. In: Smith JA, editor. Qualitative psychology: A practical guide to research methods. London: Sage Publications (2015). p. 222–48.
60. Maguire, M, and Delahunt, B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. Ireland J Higher Educ. (2017) 9:3351–9. doi: 10.62707/aishej.v9i3.335
61. Peel, KL. A beginner’s guide to applied educational research using thematic analysis. Pract Assess Res Eval. (2020) 25:1–15. doi: 10.7275/ryr5-k983
62. Swain, J. A hybrid approach to thematic analysis in qualitative research: Using a practical example. UK: Sage Publications, Ltd. (2018).
63. Lee, JW, Nersesian, PV, Suen, JJ, Mensah Cudjoe, TK, Gill, J, Szanton, SL, et al. Loneliness is associated with lower coping self-efficacy among older adults. J Appl Gerontol. (2023) 42:270–9. doi: 10.1177/07334648221129858
64. Bandura, A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215.
65. Chesney, MA, Neilands, TB, Chambers, DB, Taylor, JM, and Folkman, S. A validity and reliability study of the coping self-efficacy scale. Br J Health Psychol. (2006) 11:421–37. doi: 10.1348/135910705X53155
66. Schoenmakers, EC, Van Tilburg, TG, and Fokkema, T. Coping with loneliness: what do older adults suggest? Aging Ment Health. (2012) 16:353–60. doi: 10.1080/13607863.2011.630373
67. Carstensen, LL. Social and emotional patterns in adulthood: support for socioemotional selectivity theory. Psychol Aging. (1992) 7:331–8.
68. Morgan, D, and Burholt, V. Transitions in loneliness in later life: the role of social comparisons and coping strategies. Ageing Soc. (2022) 42:1607–28. doi: 10.1017/S0144686X20001634
69. Akhter-Khan, SC, Prina, M, Wong, GH-Y, Mayston, R, and Li, L. Understanding and addressing older adults’ loneliness: the social relationship expectations framework. Perspect Psychol Sci. (2023) 18:762–77. doi: 10.1177/17456916221127218
70. Baltes, PB. On the incomplete architecture of human ontogeny: selection, optimization, and compensation as foundation of developmental theory. Am Psychol. (1997) 52:366–80.
71. Van Baarsen, B. Theories on coping with loss: the impact of social support and self-esteem on adjustment to emotional and social loneliness following a partner's death in later life. J Gerontol B Psychol Sci Soc Sci. (2002) 57:S33–42. doi: 10.1093/geronb/57.1.S33
72. Windle, G, Hoare, Z, Woods, B, Huisman, M, and Burholt, V. A longitudinal exploration of mental health resilience, cognitive impairment and loneliness. Int J Geriatr Psychiatry. (2021) 36:1020–8. doi: 10.1002/gps.5504
73. Morlett Paredes, A, Lee, EE, Chik, L, Gupta, S, Palmer, BW, Palinkas, LA, et al. Qualitative study of loneliness in a senior housing community: the importance of wisdom and other coping strategies. Aging Ment Health. (2021) 25:559–66. doi: 10.1080/13607863.2019.1699022
74. Minahan, J, Falzarano, F, Yazdani, N, and Siedlecki, KL. The COVID-19 pandemic and psychosocial outcomes across age through the stress and coping framework. The Gerontologist. (2021) 61:228–39. doi: 10.1093/geront/gnaa205
75. Chen, L, Alston, M, and Guo, W. The influence of social support on loneliness and depression among older elderly people in China: coping styles as mediators. J Community Psychol. (2019) 47:1235–45. doi: 10.1002/jcop.22185
76. Kastner, L, Suenkel, U, Eschweiler, GW, Dankowski, T, von Thaler, A-K, Mychajliw, C, et al. Older adults’ coping strategies during the COVID-19 pandemic – a longitudinal mixed-methods study. Front Psychol. (2023) 14:1209021–1. doi: 10.3389/fpsyg.2023.1209021
77. Lazarus, R, and Folkman, S. Stress, appraisal and coping. New York: Springer Publishing Company (1984).
78. Gao, J, Hu, H, and He, H. Functional hearing impairment, psychological resilience, and social well-being among Chinese older adults in low-income households. J Speech Lang Hear Res. (2023) 66:2141–54. doi: 10.1044/2023_JSLHR-22-00209
79. Ribeiro-Gonçalves, JA, Costa, PA, and Leal, I. Loneliness, ageism, and mental health: the buffering role of resilience in seniors. Int J Clin Health Psychol. (2023) 23:100339–9. doi: 10.1016/j.ijchp.2022.100339
80. National Resilience Strategy. (2025). The United States National Resilience Strategy. The white house. The United States executive branch. Available online at: https://bidenwhitehouse.archives.gov/wp-content/uploads/2025/01/National-Resilience-Strategy.pdf (Accessed on 22 February 2025)
81. Conn, DK, Billard, T, Dupuis-Blanchard, S, Freedman, AK, Hoang, PM, Levasseur, M, et al. Canadian clinical guidelines on social isolation and loneliness in older adults. Canadian Geriatrics J: CGJ. (2024) 27:531–8. doi: 10.5770/cgj.27.772
82. Wister, A, O’Dea, E, Fyffe, I, and Cosco, T. Technological interventions to reduce loneliness and social isolation among community-living older adults: a scoping review. Gerontologie. (2021) 20:1–16. doi: 10.4017/gt.2021.20.2.30-471.11
83. Hoang, P, King, JA, Moore, S, Moore, K, Reich, K, Sidhu, H, et al. Interventions associated with reduced loneliness and social isolation in older adults: a systematic review and meta-analysis. JAMA Netw Open. (2022) 5:e2236676. doi: 10.1001/jamanetworkopen.2022.36676
84. Paquet, C, Whitehead, J, Shah, R, Adams, AM, Dooley, D, Spreng, RN, et al. Social prescription interventions addressing social isolation and loneliness in older adults: Meta-review integrating on-the-ground resources. J Med Internet Res. (2023) 25:e40213. doi: 10.2196/40213
85. Su, Y, Rao, W, Li, M, Caron, G, D’Arcy, C, and Meng, X. Prevalence of loneliness and social isolation among older adults during the COVID-19 pandemic: a systematic review and meta-analysis. Int Psychogeriatr. (2023) 35:229–41. doi: 10.1017/S1041610222000199
86. Robb, CE, de Jager, CA, Ahmadi-Abhari, S, Giannakopoulou, P, Udeh-Momoh, C, McKeand, J, et al. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: a survey of older adults in London. UK Front Psychiatry. (2020) 11:591120. doi: 10.3389/fpsyt.2020.591120
87. Li, W, Yin, H, Song, Y, Tu, W, Wang, L, Liang, Y, et al. Evaluating the risk of social isolation in older people: AHP-fuzzy comprehensive evaluation. Risk Manag Health Care Policy. (2023) 16:79–92. doi: 10.2147/RMHP.S383031
88. Poulin, V, Provencher, V, Levasseur, M, Bier, N, Aubin, G, Lord, M, et al. Experiences of community organizations providing services supporting older adults: social participation during the first eighteen months of the COVID-19 pandemic. J Aging Soc Change. (2024) 14:123–57. doi: 10.18848/2576-5310/CGP/v14i01/123-157
89. Sterne, JA, Hernan, MA, Reeves, BC, Savovic, J, and Berkman, ND. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
90. Wister, A, Cosco, T, Mitchell, B, Menec, V, and Fyffe, I. Development and concurrent validity of a composite social isolation index for older adults using the Canadian longitudinal study on aging. Can J Aging. (2019) 38:180–92. doi: 10.1017/S0714980818000612
91. Glaser, K, Agree, EM, Costenbader, E, Camargo, A, Trench, B, Natividad, J, et al. Fertility decline, family structure, and support for older persons in Latin America and Asia. J Aging Health. (2006) 18:259–91. doi: 10.1177/0898264305285668
92. Liu, N, Zeng, L, Li, Z, and Wang, J. Health-related quality of life and long-term care needs among elderly individuals living alone: a cross-sectional study in rural areas of Shaanxi Province, China. BMC Public Health. (2013) 13:1–7. doi: 10.1186/1471-2458-13-313
93. Menon, RJ, and Gangopadhyay, J. Childlessness and elderly Care in Asia: shortcomings and gaps in law and policy. In: Park D, editor. Handbook of Aging, Health and Public Policy: Perspectives from Asia. Singapore: Springer Nature Singapore (2024). 1–17.
94. Klasa, K, Trump, BD, Dulin, S, Smith, M, Jarman, H, and Linkov, I. A resilience-augmented approach to compound threats and risk governance: a systems perspective on navigating complex crises. Environment. (2025) 12:64. doi: 10.3390/environments12020064
95. HSS, U.S. Department of Health and Human Services. National Strategy for suicide prevention Federal Action Plan: FY 2024–26. Washington, DC: HHS (2024).
96. Murthy, VH. Our epidemic of loneliness and isolation: The U.S. surgeon general’s advisory on the healing effects of social connection and community. Washington, DC: Office of the U.S. Surgeon General. United States Department of Health and Human Services (2023).
97. Amberson, T, Heagele, T, Wyte-Lake, T, Couig, MP, Bell, SA, Mammen, MJ, et al. Social support, educational, and behavioral modification interventions for improving household disaster preparedness in the general community-dwelling population: a systematic review and meta-analysis. Front Public Health. (2024) 11:1257714. doi: 10.3389/fpubh.2023.1257714
98. Bell, SA, Singer, D, Solway, E, Kirch, M, Kullgren, J, and Malani, P. Predictors of emergency preparedness among older adults in the United States. Disaster Med Public Health Prep. (2021) 15:624–30. doi: 10.1017/dmp.2020.80
99. Howard, A, Agllias, K, Bevis, M, and Blakemore, T. How social isolation affects disaster preparedness and response in Australia: implications for social work. Aust Soc Work. (2018) 71:392–404. doi: 10.1080/0312407X.2018.1487461
100. Kawachi, I, Aida, J, Hikichi, H, and Kondo, K. Disaster resilience in aging populations: lessons from the 2011 great East Japan earthquake and tsunami. J R Soc N Z. (2020) 50:263–78. doi: 10.1080/03036758.2020.1722186
101. Braun, V, and Clarke, V. Reflecting on reflexive thematic analysis. Qual Res Sport, Exerc Health. (2019) 11:589–97. doi: 10.1080/2159676X.2019.1628806
102. Kneale, D, and Bécares, L. How can health inequalities be addressed through health and care policy? Insights from social care in the UK. Health Soc Care Community. (2021) 29:1745–53. doi: 10.1111/hsc.13174
103. Resnick, B, Galik, E, Vigne, E, and Carew, AP. The impact of person-centered care interventions on geriatric outcomes in nursing homes. J Am Med Dir Assoc. (2019) 20:714–20. doi: 10.1016/j.jamda.2018.11.023
104. Cassell, C, and Symon, G. Essential guide to qualitative methods in organizational research. London: SAGE Publications. (2004).
105. Schoenmakers, B, Van Der Veken, L, Dequeker, C, and Buntinx, F. How to support older adults during challenging life transitions: a qualitative study. Eur Geriatr Med. (2023) 14:1173–81. doi: 10.1007/s41999-023-00785-4
Keywords: resilience, social isolation, loneliness, older adults, theoretical model
Citation: Wister A, Kim B, Levasseur M, Poulin V, Qiu S, Yuwono E, Meynet S, Beadle J, Kadowaki L, Klasa K and Linkov I (2025) Resilience applications to social isolation and loneliness in older adults: a scoping review to develop a model and research agenda. Front. Public Health. 13:1589781. doi: 10.3389/fpubh.2025.1589781
Edited by:
Nan Jiang, Southern Medical University, ChinaReviewed by:
Sugarmaa Myagmarjav, Mongolian National University of Medical Sciences, MongoliaJinghang Cui, Northeastern University, United States
Copyright © 2025 Wister, Kim, Levasseur, Poulin, Qiu, Yuwono, Meynet, Beadle, Kadowaki, Klasa and Linkov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrew Wister, d2lzdGVyQHNmdS5jYQ==
†ORCID: Andrew Wister, orcid.org/0000-0002-0045-7428
†ORCID: Boah Kim, orcid.org/0000-0002-3104-8563
†ORCID: Mélanie Levasseur, orcid.org/0000-0002-5914-0708
†ORCID: Laura Kadowaki, orcid.org/0000-0001-6899-3801
†ORCID: Katarzyna Klasa, orcid.org/0000-0002-0045-7428