 Alex Véliz
Alex Véliz Raquel Pereira2
Raquel Pereira2 Cristian Álvarez
Cristian Álvarez- 1Departamento de Ciencias Sociales, Universidad de Los Lagos, Puerto Montt, Chile
- 2Departamento de Ciencias de La Actividad Física, Universidad de Los Lagos, Puerto Montt, Chile
- 3Departamento de Salud, Universidad de Los Lagos, Puerto Montt, Chile
- 4Exercise and Rehabilitation Sciences Institute, School of Physical Therapy, Faculty of Rehabilitation Sciences, Universidad Andres Bello, Santiago, Chile
Introduction: Although a lack of gravitational stimuli decreases bone mineral content in some populations, such as astronauts’ bone mineral content (BMC), little is known about the association of BMC with handgrip muscle strength (HGS) in divers of different years of diving experience.
Objectives: To describe the BMC and body composition of diver workers of different years of diving experience. A second objective was to associate the level of BMC with HGS.
Materials and methods: A descriptive and longitudinal pilot study was carried out in adult men divers of different years of diving experience; tertile 1 of diving experience 1–20 years (T1DE, n = 27), tertile 2 of diving experience 21–35 years (T2DE, n = 11), and tertile 3 of diving experience 36–45 years (T3DE, n = 17). Primary variables were BMC, total fat-free mass (FFM), and total body fat mass (BF), which were analyzed using dual X-ray absorptiometry (iDXA) equipment and the average of both arms’ handgrip strength (HGSav). Secondary variables were lifestyle patterns, anthropometry, and other socio-demographic variables.
Results: T3DE showed significant differences vs. T1DE group in BMCLegs (diff. −107.9 g, p = 0.029), BMCRL (diff. −51.4 g, p = 0.039), and BMCLL (diff. −55.7 g, p = 0.037). T3DE showed significant differences vs. T1DE group in outcomes total FFM (diff. −5011.9 g, p = 0.015), FFMArms (diff. −1275.1 g, p = 0.009), FFMRA (diff. −472.3 g, p = 0.012), FFMLA (diff. −406.6 g, p = 0.028), FFMLegs (diff. −2117.8 g, p = 0.031), FFMRL (diff. −1046.3 g, p = 0.037), and FFMLL (diff. −1071.3 g, p = 0.031). There was a significant correlation between HGSav and total BMC (R2 = 21.3%), between HGSRA and total BMC (R2 = 21.1%), between HGSLA and total BMC (R2 = 20.2%), between HGSav and BMCArms (R2 = 28.8%), between HGSRA and BMCArms (R2 = 27.9%), between HGSLA and BMCArms (R2 = 27.8%), between HGSav and BMCLegs (R2 = 13.3%), between HGSRA and BMCLegs (R2 = 13.8%), and between HGSLA and BMCLegs (R2 = 11.9%).
Conclusion: Diver workers with greater years of experience exhibit a reduced level of BMC and FFM in the legs compared to peers with less experience, and HGS is associated with BMC. Future longitudinal studies in diver workers could explore BMC and body composition in these populations to confirm our findings and include other physical fitness parameters in different diving specialties.
Introduction
The worldwide prevalence of the most common bone diseases, such as osteoporosis and osteopenia, has been increasing in recent decades, particularly in the adult and older adult populations (1, 2). The World Health Organization (WHO) defines osteoporosis as a criterion defined as a T-score of at least −2.5 standard deviations (SD) at the femoral head or lumbar spine compared to young people in the same population, with a lower score of −1.0 to −2.5 SD using bone mineral content (BMC) (3), being a low BMC of (43.1%), a precursor to a diagnosis of osteoporosis (2).
In the United States, approximately 12% of the population over 50 years of age has osteoporosis, with a higher prevalence in women (19.6%) compared to men (4.4%) (2). Other epidemiological evidence from a recent cross-sectional study based on the National Health Survey of Chile revealed a prevalence of 10.9% of frailty and 59% of pre-frailty, with women representing 64.9% and men 35.1% (i.e., frailty as defined by Fried’s Phenotype Scale) (4). There are few studies in Chile about BMC and the prevalence of osteoporosis in divers, and there is an important need to increase studies in body composition analyses to favor a major policy of preventing bone diseases. Although hydrodensitometry and air displacement plethysmography are valid methods, in parallel, computed tomography with magnetic resonance imaging are considered gold standard methods for body composition analysis (particularly for fat depots) (5). However, for BMC estimation, dual-energy X-ray absorptiometry (iDXA) is also considered a gold standard, with minimum radiation exposure (5–7). Previous studies by iDXA analyses reported that low BMC is consecutively associated with an increased risk of frailty in the adult population (8).
Several outcomes associated with physical activity, such as muscle strength, stimulate bone formation and preserve BMC in adult males (9). Briefly, tennis and squash players show higher BMC levels in the upper limbs and upper extremities compared to non-athlete controls, showing a bone-specific adaptation from the skeleton/muscle behavior (10). The same applies to other body segments, in which endurance athletes (i.e., that regularly are walking and running) in comparison to those trained in muscle strength (i.e., weightlifting) the latter have a higher BMC about endurance athletes, being recommended to population with lower BMC to practice more exercise/sport of muscle strength to improve their bone mineralization (11). Conversely, other factors are related to a reduction in BMC, such as diseases like cancer (12), environmental pollution (13), sleep disturbance (14), or the conditions of sedentarism or physical inactivity, where both situations can worsen or improve the BMC process (15, 16). Other factors, such as a diet rich in ultra˗processed foods (1), menopause, and aging, can also contribute significantly to accelerating the reduction of BMC. Considering this information and the need to predict frailty and BMC deterioration, some physical fitness outcomes are associated with the BMC, such as energy expenditure (17) and muscle size (18, 19). However, there is little knowledge about other physical fitness outcomes, such as handgrip muscle strength (HGS), for predicting BMC in adult workers.
Far from athletes or the sedentary population, there are jobs with specific environmental conditions that can put health maintenance at risk, such as diving. Diver fishermen (i.e., divers who live on the Chilean coast littoral) have behavioral and lifestyle characteristics that modulate their musculoskeletal health. Diving reduces the gravitational environment under the water, similar to sedentary lifestyle actions, or lying in bed, or space (20). Since the viscosity of water is greater than that of air, diving creates a significant load, raising the pressure by 1 atmosphere (atm) for every 10 m of depth. Therefore, diving provides a low-gravity environment, and while it requires repetitive muscular movements (i.e., in the context of the diver fisherman work), these actions do not impose a substantial impact load on the human skeleton, potentially affecting BMC (21) and leading to changes in gut microbiota (22). Conversely, muscular movement in the human skeleton, through muscle strength exercise, is considered a potent osteogenic stimulus (23). A recent governmental study conducted by the Chilean Superintendence of Social Security (SUSESO) showed that 36% of divers in the aquaculture and fishing industry sector report a smoking habit, while a concerning 76% admit to occasional alcohol consumption. Moreover, bone fractures (~4 to 5%) are the primary type of accidents reported (24). Furthermore, they have a high prevalence of overweight and obesity (86.7%, almost double the national Chilean prevalence), which further increases their cardiovascular risk (24). These lifestyle conditions and the physiological demands of diving underscore the need for increased research in physiological adaptations to body composition and occupational areas.
Moreover, epidemiological studies in Chile have shown an increase in the prevalence of cardiometabolic diseases, including hypertension, diabetes, and metabolic syndrome in the adult population, with a significant prevalence in people over 65 years (25–27). Furthermore, considering the importance of preventing osteoporosis and low BMC in the adult population, the abundance of risk factors for preserving the skeletal muscle mass (i.e., body composition), there is a need to add more knowledge about other easy-to-measure outcomes for predicting BMC and body composition, such as HGS. Thus, due to physiological diving conditions promote an environment of high risk in the vascular system, and considering the current unhealthy lifestyle of diver workers, there is a particular need to ask the questions whether HGS show relationship with BMC, muscle mass or fat free mass in diver workers and to clarify if the accumulation of more years of experience working on diving (i.e., under a low gravitational work) play a role in the total or segmental BMC deterioration. In solving these questions, HGS could be used to monitor bone health and the body composition risk when muscle mass declines in these populations. Thus, the objective of the present study was to describe the BMC and body composition of diver workers of different years of diving experience. A second objective was to associate the level of BMC with HGS. A second objective was to associate the level of HGS with BMC. We hypothesized that HGS is significantly associated with BMC in Chilean diver workers.
Materials and methods
Population and study design
A pilot, descriptive and longitudinal type study developed in the laboratory of the Universidad de Los Lagos, in the city of Puerto Montt, Chile, between June and September 2024, with diver workers from diving social groups of the cities Puerto Montt, Calbuco, Maullín and Ancud, all corresponding to the geographical southern macro-zone coast of Chile. The participants were contacted through a broad call through social networks or by directly contacting the leaders of each organization. Each group was explained by the objectives of the study, its scope, and the processes for delivering evaluations and counseling in this regard.
The study was approved by the Scientific Ethical Committee of Scientific Ethical Committee of Universidad Mayor, by the approval folio N° 0492. All participants had previously signed an informed consent form indicating the procedures to be performed, protection of personal data, anonymity, potential risks, among other aspects. The sample was calculated using a similar adult male population based on standard deviation (SD 8.6 kg) (28). Thus, looking for detecting associations and a moderate effect size, a sample size of (n = 55) participants provides a statistical power of 80% in correlation/regression analyses. This calculation was developed using the freely available G*Power software (version 3.1.9.6, Franz Faul, Universität Kiel, Kiel, Germany). The final sample included groups of diver workers of different tertiles of years of diving experience, and was (n = 55) distributed by the following tertiles; tertile 1 of years of diving experience 1–20 years (T1DE, n = 27), tertile 2 of years of diving experience 21–35 years (T2DE, n = 11), and tertile 3 of years of diving experience 36–45 years (T1DE, n = 17). The study design can be seen in Figure 1.
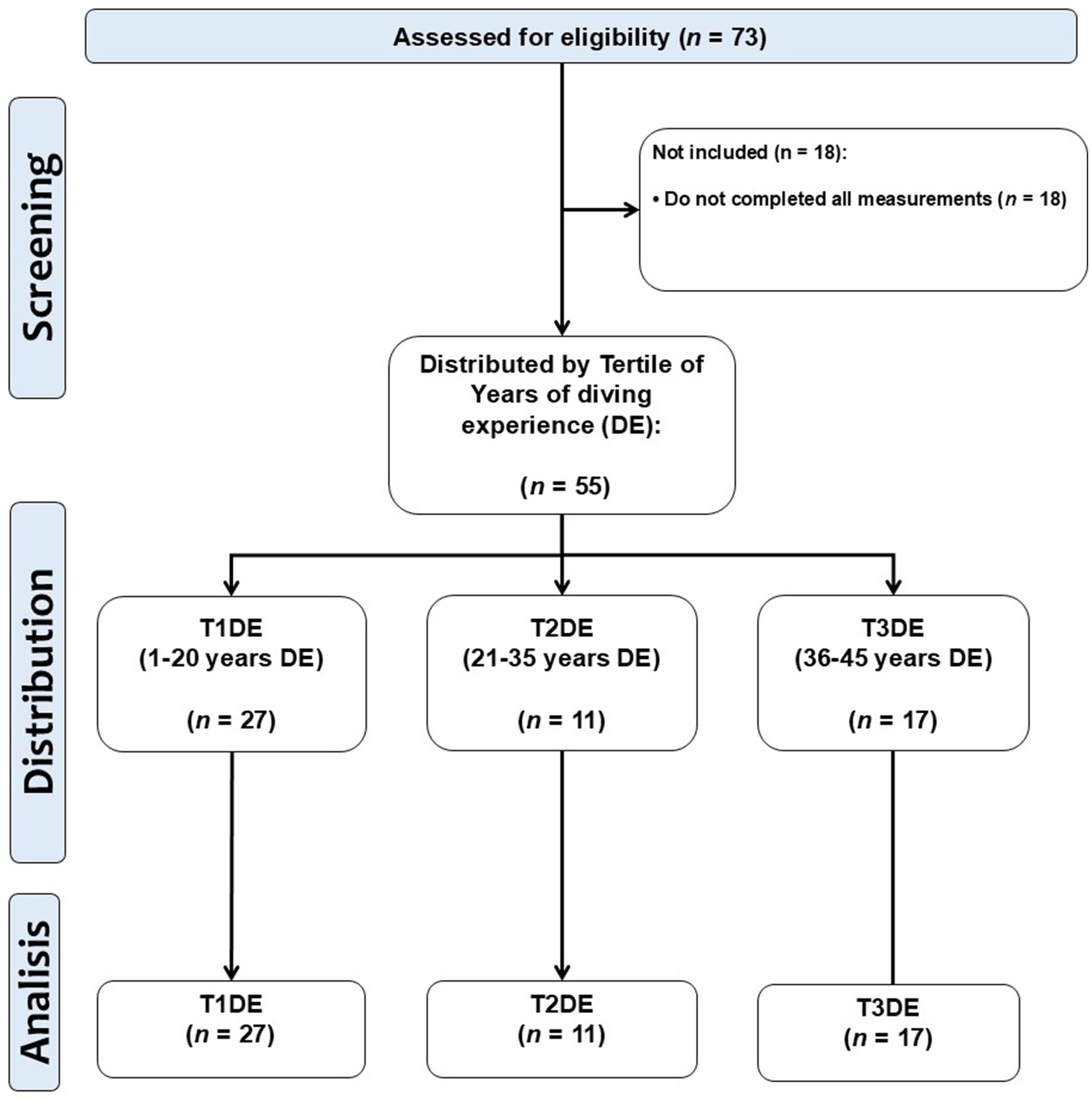
Figure 1. Study design.
Bone mineral content by dual X ray absorptiometry analysis (main outcomes)
The subjects attended the Universidad de Los Lagos laboratory for the body composition evaluation from Monday to Friday from 9:00 to 13:00 in the morning for these procedures. Before the measurement of body composition with the iDXA equipment (Healthcare General Electric Company, ENCORE 18 Software, United States), a preliminary interview was conducted to rule out the use of electronic devices such as pacemakers, insulin pumps, among others that could be declared and interrupt the operation of the equipment or could affect the health of each participant. For the iDXA measurement, each subject was placed in a supine position on the stretcher of the equipment, wearing light clothing and without shoes or metal objects. The evaluation process lasted an average of 10 min, but each subject participating was inside the evaluation room for 20 min. The iDXA measurements and the characteristics of the diver’s work can be seen from (Figures 2A–C).
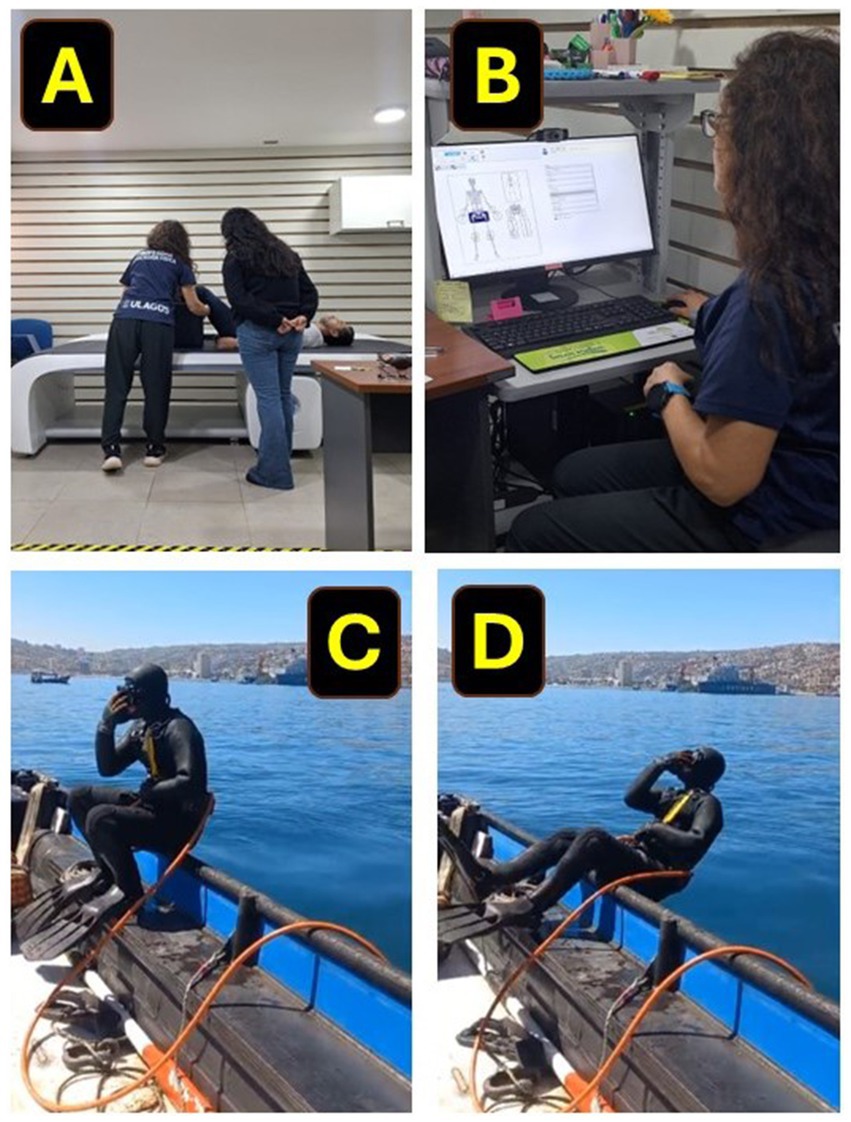
Figure 2. Dual X absorptiometry measurement in Latin American diver workers from the coast of Chile. (A) Show the preparation phase of the divers for the iDXA measurement. (B) Show the evaluator scanning BMC and body composition in the computer software. (C) Show the characteristic equipment in which diver workers operate on the Chilean coast, and (D) show the position where the divers usually contact the seawater.
Lifestyle patterns
The physical activity (PA) levels of the population were determined with the international physical activity questionnaire “Global Physical Activity Questionnaire” (GPAQ v2) (29). From here, the min/week of vigorous (PAVI), moderate (PAMI), and light (PALI) was determined and registered by each diver participant. The sedentary time per week was determined by self-reporting time spent on activities involving sitting or reclining during leisure time.
To determine the variables related to smoking habits, questions were considered based on the minimum smoking surveillance instrument used by the Pan-American Health Organization. These identified the current smokers (daily and occasionally) and ex-smokers, allowing for the number of cigarettes smoked and the persistence of the habit; however, in this study, the information was registered only as non-smokers and smokers (30).
Handgrip strength (main outcomes)
For HGS, measurements of both hands were used in three attempts in a seated position, and we used the average of both arms (HGSav), handgrip of the right (HGSRA: HGS right arm), and left (HGSLA: HGS left arm) arm to be registered. These measurements were developed by using a digital handheld dynamometer (Jamar®, PLUS+, Sammons Preston, Patterson Medical, Illinois, United States) following previous studies in Latin American populations (31).
Anthropometry (secondary variables)
Weight was measured with a BIA equipment InBody120™ scale (tetrapolar 8-point tactile electrode system, model BPM040S12F07, Biospace, Inc., Seoul, Korea) with a 0.1 kg precision, following previous studies (32). Height was measured with a SECA™ 213-Topmedic portable stadiometer (Germany). BMI was calculated using weight and height squared.
Blood pressure
Blood pressure was measured on three attempts with at least 1 min rest intervals between measurements, using a digital cuff instrument positioned in the arm OMRON™ (Model HEM-7142, United States). Blood pressure was categorized according to the criteria of the European Society of Cardiology into hypertension (systolic blood pressure [SBP] ≥ 140 or diastolic blood pressure [DBP] ≥ 90 mmHg), normal-high blood pressure (SBP 130–139 mmHg or DBP 85–89 mmHg) (33).
Ruffier test
All the subjects evaluated were instructed in the following way: firstly, the heart rate at rest was measured in a standing position for 15 s multiplied by 4 to know the equivalent beats per minute, recorded as (HR1), then the person stood up, did leg flexion-extensions at a steady pace with the throne straight at 90° of knee flexion, raising arms in front of the front while flexing for 45 s. Immediately after performing the leg flexion-extensions exercise, the heart rate (HR2) is recorded again, followed by a 1-min rest in a seated position. Finally, the heart rate (HR3) is recorded again. The results are then interpreted using the following formula, Ruffier index: [(HR1 + HR2 + HR3)–200]/100, where the aerobic endurance is determined according to the following values [0 very good performance, 0.1–5 good performance, 5.1–10 average performance, >10–15 insufficient performance, 15.1–20 poor performance] (requires medical evaluation).
Statistical analysis
Data are shown as mean and (±) standard deviation for continuous variables and as frequency (n =) and percentage (%) for categorical variables. The sample was divided into tertiles of years of diving experience (T1DE, T2DE, and T3DE). The Shapiro–Wilk test was applied to test the normal distribution of the main and secondary outcomes (See Supplementary material https://figshare.com/s/b6f46fecbb2a71e0fc23). To test differences between groups, One-way ANOVA and Tukey’s post hoc test for multiple comparisons between groups at p < 0.05 alpha error level were applied for outcomes with normal distribution. Furthermore, Cohen’s d effect size test was reported at the p < 0.05 level for this interaction. Conversely, the Kruskal-Wallis test was applied to outcomes with no normal distribution, with Dunn’s post hoc test for multiple comparisons at p < 0.05 alpha error level. To the secondary outcome of physical activity of vigorous intensity (PAVI), the mixed-effects model (REML) was applied with the Holm-Sidak test for multiple comparisons. Simple linear regression was applied to test the association between total BMC, arm, and leg BMC with the variables HGSav and HGS of the right (HGSRA) and left arm (HGSLA). The level of prediction of BMC was recorded using the R2 determination coefficient, and the predictive equation was reported. The analyses used GraphPad Prism v. 8.0 statistical software (Chicago, Illinois, United States).
Results
The results indicate that there were significant differences among T1DE, T2DE and T3DE in the variable age (T1DE 46.1 ± 2.2; T2DE 56.3 ± 0.5 and T3DE 64.2 ± 1.6 years, p < 0.0001) (Table 1), years of diving experience (T1DE 19.8 ± 1.7; T2DE 34.8 ± 0.3 and T3DE 41.5 ± 0.7 years of diving experience, p < 0.0001) (Table 1). In the anthropometry, it was observed that height was significantly higher in the T2DE vs. T3DE group (173.0 ± 2.0 vs. 165.0 ± 2.0 cm, p = 0.016), while weight and BMI showed no significant differences (Table 1). Regarding cardiovascular parameters, systolic, diastolic blood pressure, and heart rate at rest did not show significant differences among T1DE, T2DE, and T3DE (Table 1). On the other hand, basal metabolism showed a decreasing trend with more years of diving experience, being significantly different between T3DE vs. T1DE (1403.0 ± 90.0 vs. 1468.0 ± 89.0 Kcal/kg) and between T3DE vs. T2DE (1403.0 ± 90.0 vs. 1463.0 ± 151.0 Kcal/kg) (Table 1).
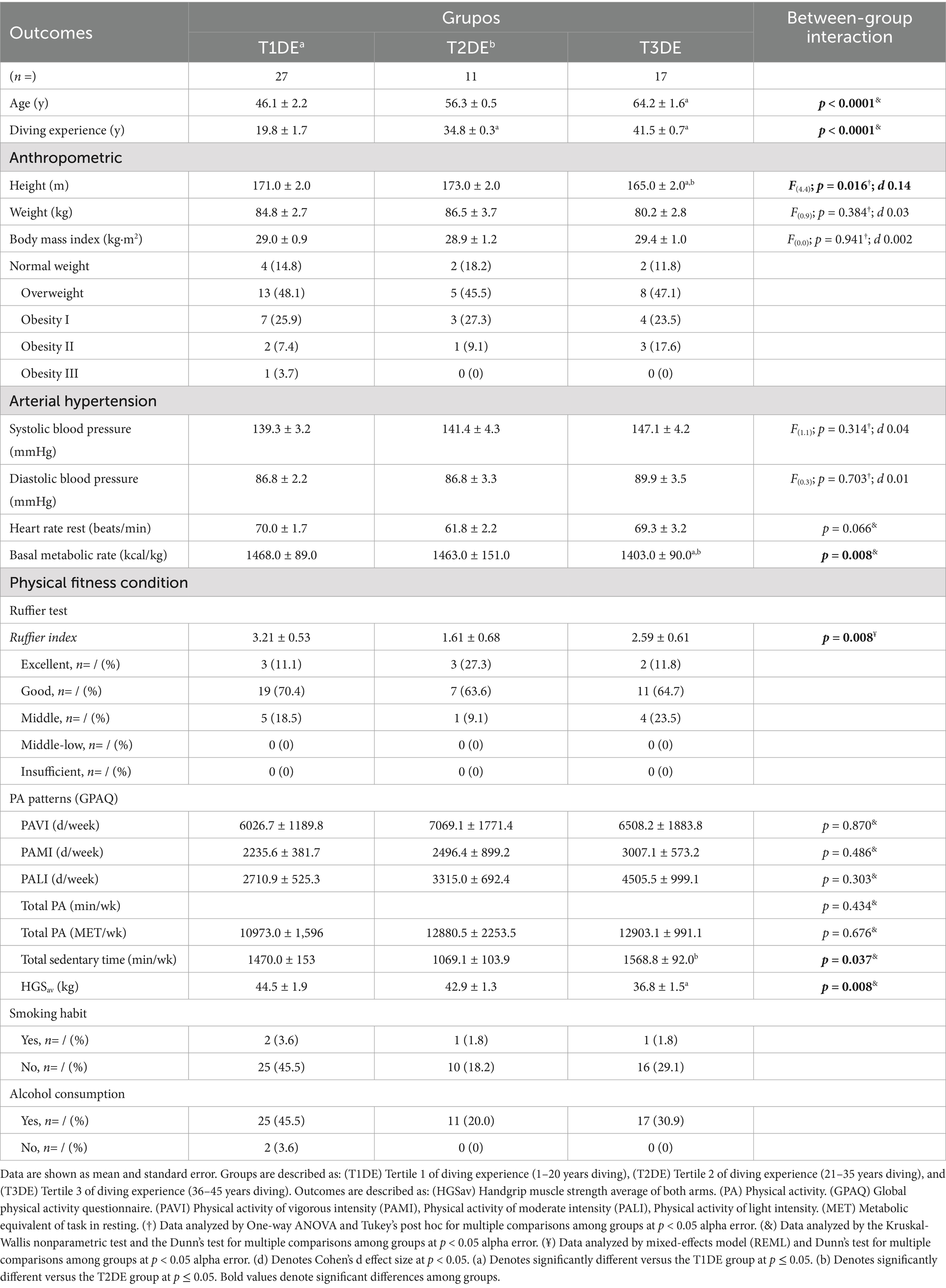
Table 1. Cardiovascular, anthropometric, and behavioral characteristics in three different groups of diver workers of different years of diving experience.
In terms of cardiovascular recovery after physical effort, the Ruffier index showed better values in the T2DE group, where a higher proportion of divers classified as “excellent” (27.3%) in their cardiovascular recovery was observed compared to the T1DE (11.1%) and T3DE (11.8%) groups (p = 0.008) (Table 1). The total sedentary time per week differed between T3DE vs. T2DE (1568.8 ± 92.0 vs. 1069.1 ± 103.9 min/week, p = 0.037) (Table 1). The HGSav decreased with years of diving experience, being significantly lower in the T3DE vs. T1DE (36.8 ± 1.5 vs. 44.5 ± 1.9 kg, p = 0.008) compared to the T1DE and T2DE group (p = 0.008) (Table 1). The levels of the different types of physical activity intensities per week did not show significant differences between groups (Table 1). About lifestyle habits, alcohol consumption was high in all groups, being higher in T1DE (93.6%), while smoking was reported by a small percentage of the divers, with no significant differences between groups.
Bone mineral content
When comparing total BMC, BMC of both arms, and BMC of left and right arm among T1DE, T2DE, and T3DE groups, no significant differences between groups were detected (Figures 3A–D). Conversely, there were significant differences between groups T3DE vs. T1DE in outcomes BMC of the legs (1009.5 ± 101.0 vs. 1117.4 ± 197.4 g, p = 0.029) (Figure 3E), BMC of the right leg (503.8 ± 47.1 vs. 555.2 ± 96.6 g, p = 0.039) (Figure 3F), and BMC of the left leg (506.4 ± 56.5 vs. 562.1 ± 101.9 g, p = 0.037) (Figure 3G).
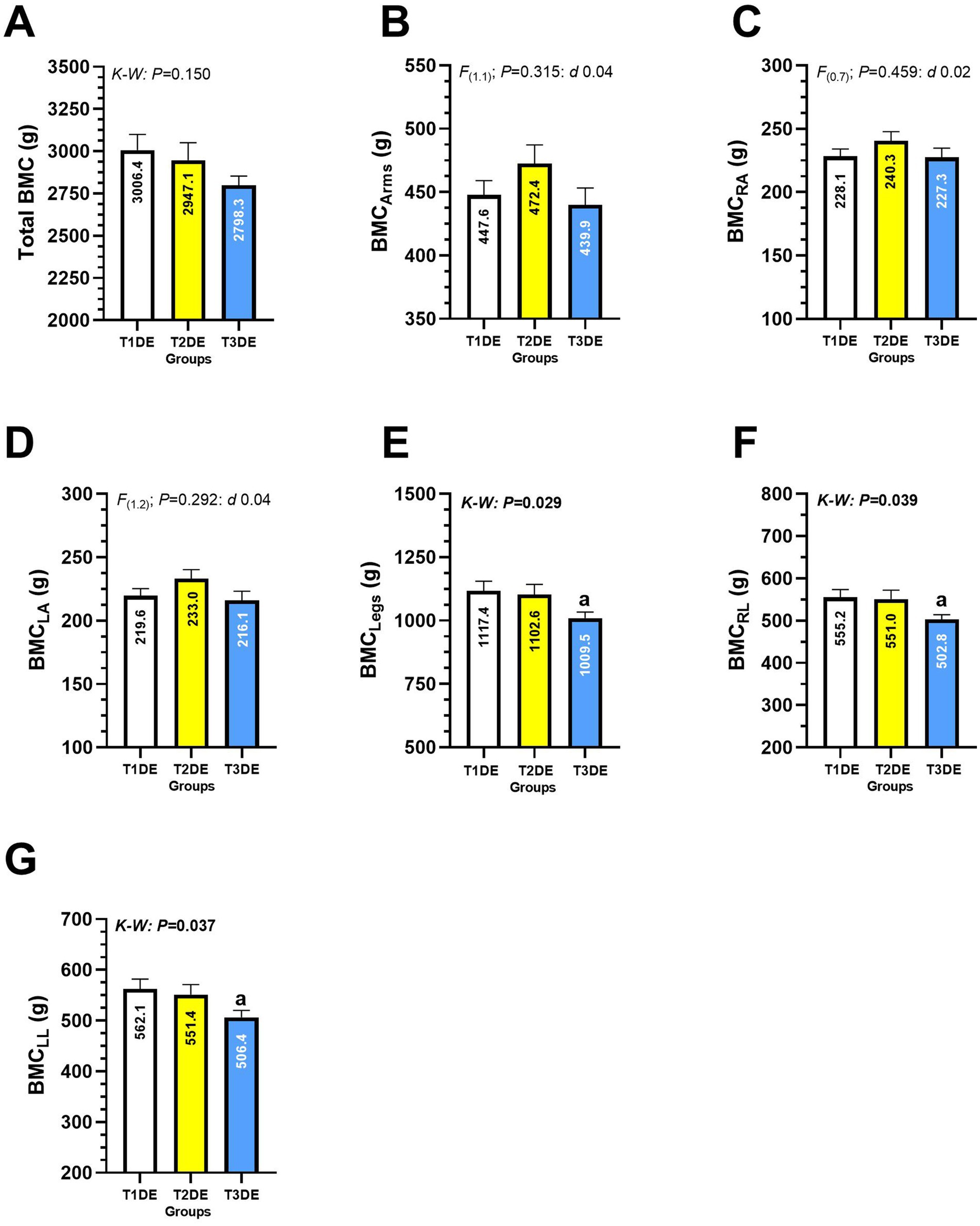
Figure 3. Total bone mineral content (A), of the arms (B), right arm (C), left arm (D), legs (E), right leg (F), and bone mineral content of the left leg (G) in Latin American diving workers. Groups are described as: (T1DE) Tertile 1 of diving experience (1–20 years diving), (T2DE) Tertile 2 of diving experience (21–35 years diving), and (T3DE) Tertile 3 of diving experience (36–45 years diving). Outcomes are described as: (BMCArms) Bone mineral content of the arms, (BMCRA) Bone mineral content of the right arm, (BMCLA) Bone mineral content of the left arm, (BMCLegs) Bone mineral content of the legs, (BMCRL) Bone mineral content of the right leg, (BMCLL) Bone mineral content of the left leg. (K-W) Denotes data analyzed by nonparametric Kruskal-Wallis test at p < 0.05 level. (a) Denotes significant differences between T3DE vs. T1DE group at p < 0.05 level.
When comparing total BF, BF of both arms, BF of right arm, BF of left arm, BF of legs, BF of right leg and BF of left leg of T1DE, T2DE and T3DE groups of different years of diving experience, no significant differences between groups were reported (Figures 4A–G).
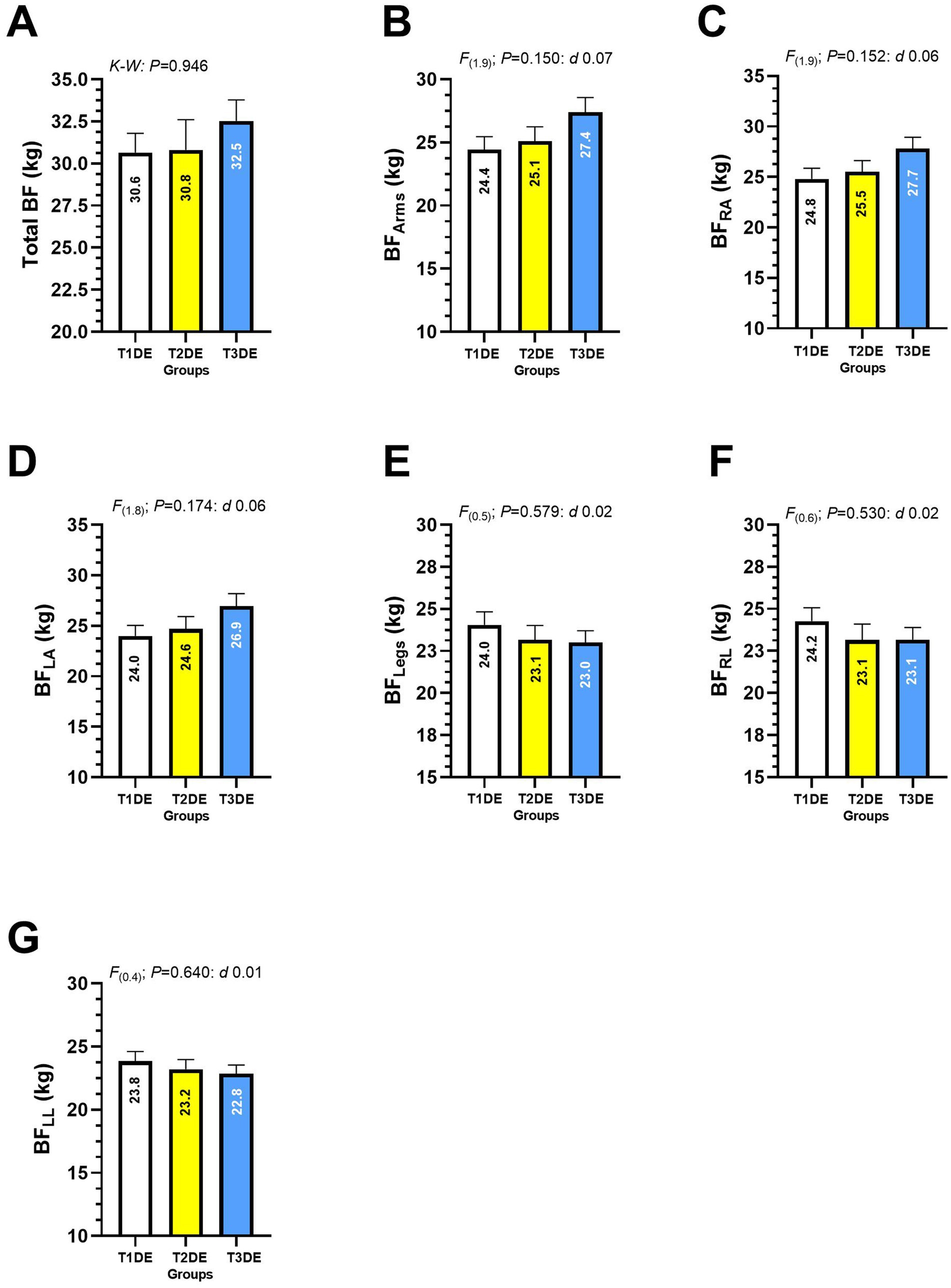
Figure 4. Total body fat (A), body fat of the arms (B), right arm (C), left arm (D), legs (E), right leg (F), and body fat of the left leg (G) in Latin American diving workers. Groups are described as: (T1DE) Tertile 1 of diving experience (1–20 years diving), (T2DE) Tertile 2 of diving experience (21–35 years diving), and (T3DE) Tertile 3 of diving experience (36–45 years diving). (BF) Body fat. Outcomes are described as: (BFArms) Body fat of the arms, (BFRA) Body fat of the right arm, (BFLA) Body fat of the left arm, BFLegs Body fat of the legs, (BFRL) Body fat of the right leg, (BFLL) Body fat of the left leg.
Significant differences were comparing T3DE vs. T1DE group in the outcomes total FFM (52169.9 ± 4138.0 vs. 57181.8 ± 6805.0 g, p = 0.015, d 0.14) (Figure 5A), FFM of arms (6359.5 ± 1851.0 vs. 7634.6 ± 1117.0 g, p = 0.009) (Figure 5B), FFM of right arm (3410.5 ± 430.8 vs. 3882.8 ± 569.2 g, p = 0.012) (Figure 5C panel C), FFM of left arm (3352.4 ± 463.1 vs. 3759.0 ± 546.4 g, p = 0.028, d 0.12) (Figure 5D), FFM of the legs (17192.3 ± 1919.0 vs. 19310.1 ± 3249.0 g, p = 0.031, d 0.12) (Figure 5E), FFM of right leg (8621.7 ± 993.5 vs. 9668.0 ± 1591.0 g, p = 0.037, d 0.11) (Figure 5F) and FFM of left leg (8570.7 ± 965.2 vs. 9642.0 ± 1681.0 g, p = 0.031, d 0.12) (Figure 5G).
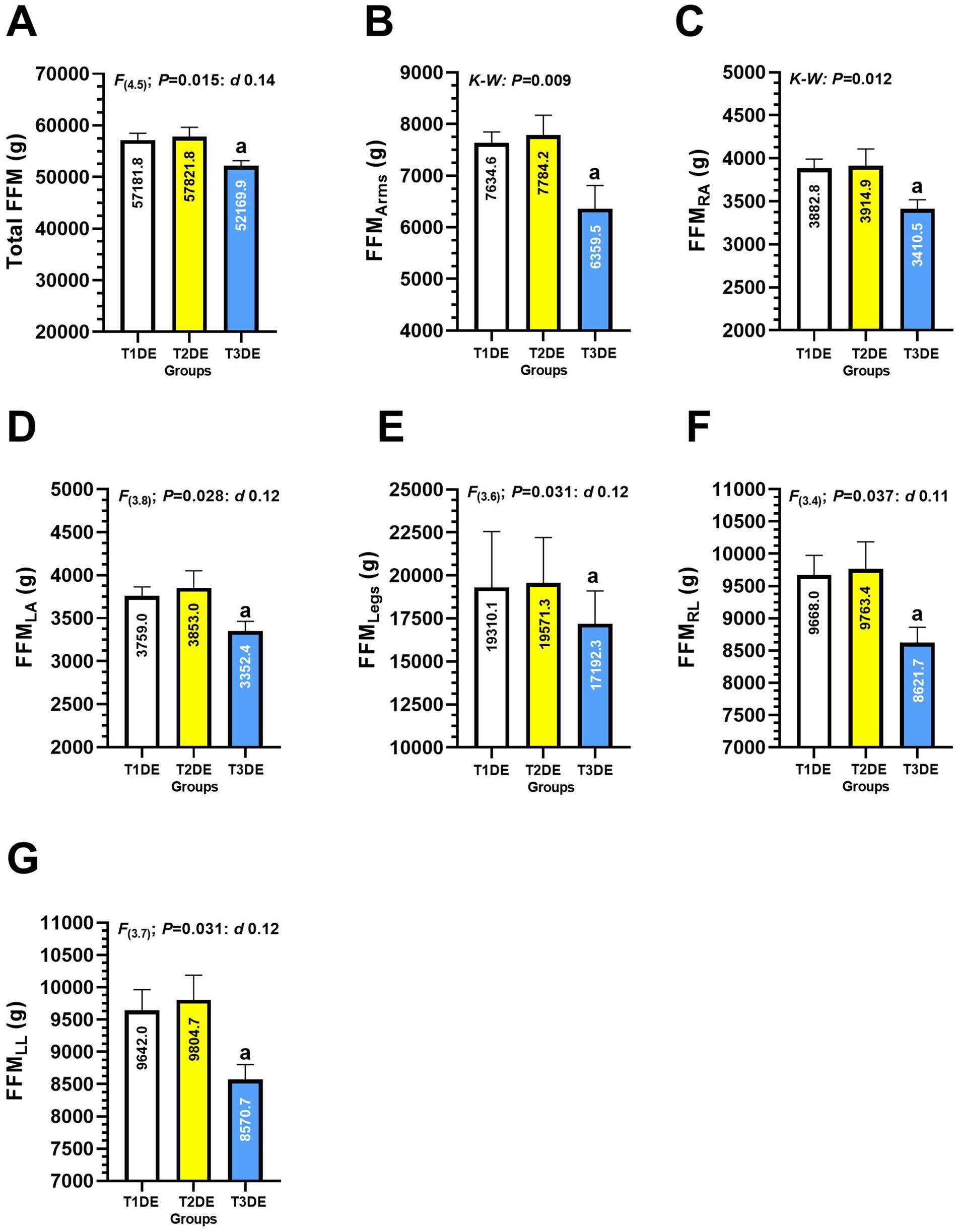
Figure 5. Total fat-free mass (A), arms (B), right arm (C), left arm (D), legs (E), right leg (F), and fat-free mass of the left leg (G) in Latin American divers. Groups are described as: (T1DE) Tertile 1 of diving experience (1–20 years diving), (T2DE) Tertile 2 of diving experience (21–35 years diving), and (T3DE) Tertile 3 of diving experience (36–45 years diving). Outcomes are described as: (FFMArms) Fat-free mass of the arms, (FFMRA) Fat-free mass of the right arm, (FFMLA) Fat-free mass of the left arm, (FFMLegs) Fat-free mass of the legs, (FFMRL) Fat-free mass of the right leg, (FFMLL) Fat-free mass of the left leg. (K-W) Denotes data analyzed by Kruscal-Wallis non-parametric test at p < 0.05 level. (a) Denotes significant differences between group T3DE vs. T1DE at p < 0.05 level.
Associations between handgrip strength and bone mineral density
There was a significant correlation between HGSav and Total BMC (R2 = 0.213, predictive value; 21.3% of variance explained by total BMC; Regression equation: Y = 0.00996*X + 12.54 and p = 0.0004) (Figure 6A). There was a significant correlation between HGS right arm and the Total BMC variable (R2 = 0.211, predictive value; 21.1% of the variance; Regression equation: Y = 0.01037*X + 11.83, p = 0.0004) (Figure 6B). There was a significant correlation between HGS left arm and the Total BMC variable (R2 = 0.202, predictive value; 20.2% of variance; Regression equation: Y = 0.00962*X + 13.26, p = 0.0006) (Figure 6C).
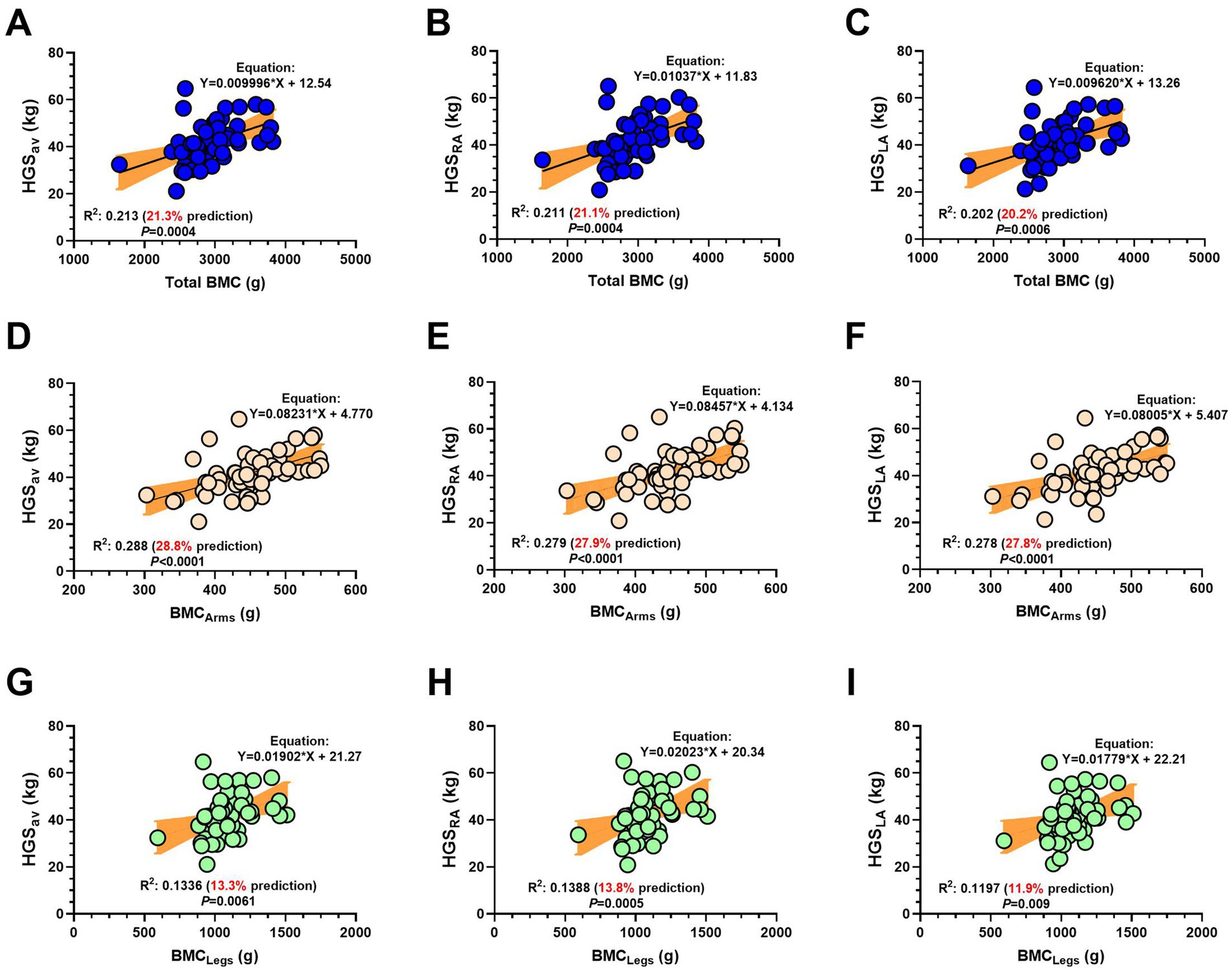
Figure 6. Association between handgrip strength average of both arms (A,D,G), handgrip strength of the right arm (B,E,H) and handgrip strength of the left arm (C,F,I) with total bone mineral content (A–C), bone mineral content of the arms (D–F) and bone mineral content of the legs (G–I) in adult Latin American diver workers. (HGS) Handgrip strength. (HGSav) Handgrip strength average of both arms. (BMC) Bone mineral content. (R2) Coefficient of determination, variability, and prediction. Values in red denote the % prediction of BMC concerning the HGS variable.
There was a significant correlation between HGSav and BMC arms (R2 = 0.288, predictive value; 28.8% of variance explained; Regression equation: Y = 0.08231*X + 4.770, p < 0.0001) (Figure 6D). There was a significant correlation between HGS right arm BMC of the arms (R2 = 0.279, predictive value; 27.9% of variance explained; Regression equation: Y = 0.08457*X + 4.134, p < 0.0001) (Figure 6E). There was a significant correlation between HGS left arm and the variable BMC of the arms [R2 = 0.278 (27.8% predictive; Regression equation: Y = 0.08005*X + 5.407, p < 0.0001)] (Figure 6F).
There was a significant correlation between average HGSav and BMC of the legs R2 = 0.1336, predictive value; 13.3% prediction; Regression equation: Y = 0.01902*X + 21.27, p = 0.0061, (Figure 6G). There was a significant correlation between HGS right arm and BMC of the legs (R2 = 0.1388, predictive value: 13.8%; Regression equation: Y = 0.0223*X + 20.34, p = 0.0005) (Figure 6H). Finally, there was a significant correlation between HGS left arm and BMC of the legs (R2 = 0.1197, predictive value: 11.9%), with regression equation: Y = 0.01797*X + 22.21, p = 0.009 (Figure 6I).
Discussion
The objective of the present study was to describe the BMC and body composition of diver workers of different years of diving experience. A second objective was to associate the level of BMC with HGS. A second objective was to analyze the association between handgrip strength and BMC in these workers. The main results of the present study indicate that (i) there is a reduced level of BMC and FFM in the right and left leg in diver workers who have more years of diving experience (T3DE) compared to peers with less years of diving experience (T1DE) (Figure 2), (ii) there were significant correlations between HGSav, and HGS of the left and right arm with total BMC (~28%) and BMC of the upper body (~20%) relative to BMC of the lower body (~13%) of diver workers. Correlations are observably stronger in the arms than in the legs, and HGSav was reported to have a higher predictive ability in R2 on total and regional BMC (Figure 3).
Regarding our first finding, we reported reduced BMC and FFM. A previous study used iDXA analyses in Korean female divers reported that BMC was lower proportionally to higher pressure and depth of dive, correlating with BMC and longer exposure time to water (21). In long-lived post-menopausal women divers ~72 years old, Seo et al. (34) reported that female divers did not show different BMC (measured by iDXA) compared to non-diving control pairs, however, when they experienced some type of osteoporotic spinal fracture, the divers were shown to develop compensatory mechanisms in some bone anatomical regions of the skeleton such as increased cervical lordosis and pelvic tilt relative to controls. The authors concluded that the adaptive phenomenon at the bone level was explained by the superior strength of the back muscles and the spinal mobility of the diving condition.
A study (35) that involved three groups—sprint runners, distance swimmers, and divers— reported that over 8 months of monitoring, the divers increased their body weight, without modifying their BMC or FFM. In this context, considering our results, we believe that even though the T3DE group is the group with more years of experience in diving (41.5 years) and therefore also more older (64.2 years) (Table 1) it could be considered physiologically acceptable to present a low BMC as indicated by epidemiological studies in the adult population (2, 4), however, diving activity reports an early reduction of BMC in both legs and in an isolated way in the BMC of the right and left leg (Figures 4E–G) but in parallel also presents a reduction of the FFM in the right and left leg (Figures 4A–G), putting at risk not only their capacity of muscle strength during diving tasks, but also this reduced BMC and muscle tissue increases the musculoskeletal frailty of the diver workers in daily life actions. Regarding the reduced FFM, considering that the rate of BMC loss or reduction is slower compared to changes in muscle or fat tissue, it is also consistent that divers with more diving experience, along with reporting lower BMC in legs, also present a low amount of FFM. The relevance of maintaining proper muscle mass lies in its role in maintaining appropriate levels of strength and metabolic control. For example, the muscle mass of an adult subject can uptake about 80% of the total carbohydrate (i.e., insulin-stimulated pathway) consumed by the 75 g glucose tolerance test (36). Therefore, a lower FFM reduces glucose control and increases the risk of type 2 diabetes mellitus.
The present study also found differences between groups of younger and more experienced divers in variables such as basal metabolic rate, Ruffier index, sedentary time, and HGS. Studies in young divers ~24–33 years have shown a basal metabolic rate of 2,115 Kcal/day, these values being higher than our study (range 1,403–1,468 Kcal/day), however our three groups with different years of diving experience were older (46–64 years), it being known that with age the metabolism is reduced under basal conditions (37). Conversely, the general physical capacity and cardiovascular recovery after an effort such as the Ruffier test, which on average was categorized as “Good” across the three groups of diving experience, however, there were differences in the proportions between groups, where the subjects of the T3DE group reported a smaller number of subjects in “Excellent” condition and a larger number in the “Medium” physical capacity category (Table 1). Furthermore, the time spent on sedentary activities was higher between the T3DE vs. T2DE groups (Table 1), where we speculate that, apart from the physiological implications in the slowing of metabolism at rest, when aging is combined with greater sedentary activity, the risk of suffering from cardiovascular and metabolic diseases is exaggeratedly increased. Similarly, it is logical to speculate that part of the low levels of HGSav in the T3DE group among younger subjects and years of diving could very well be attributed to the longer time of sedentary lifestyle, much more than by the age factor, with lifestyle playing a greater role than the biological factor.
At the metabolic level (37) reported in divers ~30 years old, in overweight (BMI 25 to 30 kg/m2) that diving at 6 m of depth but at a T° of −5°C increased body thermogenesis, translating into a reduction in skin T° from 36.8 to 28.5°C but at the same time increasing energy expenditure from 1.9 to 2.8 Kcal/min, resulting in 6 h of diving an average metabolic utilization of 57% carbohydrates (0.40 g/min), and 42.5% fat utilization (0.13 g/min) and a higher heart rate compared to when donning equipment before diving (6.7 versus 4.3 mL/kg/min).
Regarding our third result, previous studies have reported the association between HGSav and BMC in both children and adolescents (38) and adults (39). In brief, Saraiva et al. (38) reported in (n = 243) children and adolescents aged 4–15 years, in girls, HGS was associated with BMC of the arms, legs, trunk, spine, and total BMC of girls and boys. Thus, previous studies in both children and adult populations assess the predictive capacity of muscle strength assessed by the HGSav test on BMC; however, the present study adds this additional knowledge in the present sample of Chilean diver workers. Interestingly, the reduction in BMC in divers, particularly in those with more years of diving experience, as in the T3DE group, would have a similar physiological effect in relation to life conditions without gravity, as is the case with astronauts (20). For example, space travel has been reported to cause a loss of BMC, especially in the lower body (pelvis, lumbar vertebrae, and femoral head). Part of the mechanisms attributable to this bone effect in astronauts has been reported in altered calcium metabolism, increasing the stimulation of calcium excretion through urine and a reduced intestinal calcium reabsorption (20), although in summary, long-duration space travel has negative effects on astronauts’ musculoskeletal system (20). We believe that, in the case of diver workers, considering this knowledge, more public policies should be promoted to protect muscle and bone health, especially for those with more years of diving experience, as they are at greater risk of fragility and cardiovascular disease, as can be seen from (Table 1) where in average the systolic blood pressure of the three groups are ~140 mmHg.
In secondary results, the high values of systolic blood pressure 139 to 147 mmHg and diastolic (86–9 mmHg) in the three groups of diving experience categorize the groups into high blood pressure and arterial hypertension (Table 1), which is a worrying way. Previous reports about the lifestyle of Chilean divers have already warned about the lifestyle of these workers, which includes unhealthy habits (24). Therefore, ruling out cardiovascular deterioration due to aging and promoting a much healthier lifestyle among workers in these contexts would reduce the cardiovascular and metabolic risk of these people, despite the parallel physiological risk of a reduced BMC generated by the work of diving.
In addition, due to the increased prevalence of osteoporosis and osteopenia (1, 2), and that a low BMC is a precursor to a diagnosis of osteoporosis (2), and that previous Chilean studies revealed a prevalence of frailty in men 35.1% (i.e., frailty as defined by Fried’s Phenotype Scale) (4), there is little information regarding some physiological and environmental conditions of some employment conditions such as diver workers dedicated to mollusks extraction in the coast. Moreover, to prevent risk factors for frailty, there is a need to look for predicting early a frailty condition and BMC deterioration, such as the previous reports of energy expenditure (17), and muscle size for these aims (18, 19). Here we added more information about the utility of HGS associated with BMF and the fat-free mass in diver workers, and future studies could continue exploring in larger sample sizes and by cross-sectional and longitudinal studies the HGS capacity for predicting BMC and body composition in diver workers. Potential future hypothesis of interest to solve could include whether other physical fitness variables in both young and more older diver workers (i.e., cardiorespiratory or other muscle strength outcomes) are associated and predict BMC in divers with history of bone accident, and include not only diver workers of the aquiculture/fishing area but also other types of diving specialties such as rescue and deeper diving with different lifestyle.
Limitations and strengths
This study is not without its weaknesses, for example, (i) only people who attended voluntarily were assessed and not the total number of active member subjects of each social group invited from the cities involved, (ii) the heart rate was recorded manually by taking heart rate per minute during the Ruffier test, however, this parameter was obtained from an exercise specialist in the diving area, (iii) the seasons with longer or shorter diving times were not considered, nor was the temperature of the water in which they dived, and (iv) the sample size was statistically sufficient but future studies could increase the sample size amount to increase the statistical power.
However, it also has some strengths; (i) the measurements were taken in a population that is not usually accessible and that usually does not attend preventive health checks at health system, (ii) the body composition analyses were carried out using the iDXA equipment, which is gold standard for the total and segmental analysis of BF, FFM and BMC, and (iii) the measurements taken are preventive, which will allow future health promotion actions to be proposed for the participants in this study.
Conclusion
Diver workers with more years of experience have a reduced level of BMC and FFM in the legs compared to peers with less experience, and HGS shows a significant association with BMC. These results suggest the need for future longitudinal studies to monitor health in diver workers based on robust iDXA body composition analyses to confirm our findings and include other physical fitness parameters in different diving specialties.
Data availability statement
The data presented in the study are deposited in the https://figshare.com repository, accession link: https://figshare.com/articles/dataset/Database_Divers/28914317?file=54128975.
Ethics statement
The studies involving humans were approved by Scientific Ethical Committee of Reloncaví of the city of Puerto MonttScientific Ethical Committee of Reloncaví of the city of Puerto Montt, Los Lagos region, by means of the approval folio No. 0492. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AV: Conceptualization, Funding acquisition, Validation, Writing – original draft, Writing – review & editing, Data curation, Investigation, Methodology, Project administration. RP: Conceptualization, Data curation, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing, Resources, Supervision, Visualization. AD: Data curation, Investigation, Project administration, Resources, Supervision, Visualization, Funding acquisition, Writing – review & editing, Writing – original draft. CÁ: Funding acquisition, Writing – review & editing, Conceptualization, Formal analysis, Software, Validation, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Agencia Nacional de Investigación y Desarrollo de Chile ANID-FONDEQUIP 2021 Code EQM210056 Research Project and by the Redes Territoriales de investigación 2024–2025 of the Universidad de Los Lagos.
Acknowledgments
We thank all the participants for their commitment to the measurements, particularly to the divers from Puerto Montt, Calbuco, Maullín, and Ancud cities of the Chilean coast.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1591242/full#supplementary-material
References
1. Brooks, ELG, Tangney, CC, and Ritz, EM. Ultra-processed food intake and prevalence of osteoporosis in US adults aged 50 years and older: a cross-sectional analysis. Osteoporos Int. (2025) 36:455–64. doi: 10.1007/s00198-025-07394-4
2. Sarafrazi, N, Wambogo, EA, and Shepherd, JA. Osteoporosis or low bone mass in older adults: United States, 2017–2018. NCHS Data Brief. (2021) 2–8. doi: 10.15620/cdc:103477
3. Kanis, JA, Adachi, JD, Cooper, C, Clark, P, Cummings, SR, Diaz-Curiel, M, et al. Standardising the descriptive epidemiology of osteoporosis: recommendations from the epidemiology and quality of life working group of IOF. Osteoporos Int. (2013) 24:2763–4. doi: 10.1007/s00198-013-2413-7
4. Troncoso-Pantoja, C, Concha-Cisternas, Y, Leiva-Ordoñez, AM, Martínez-Sanguinetti, MA, Petermann-Rocha, F, Díaz-Martínez, X, et al. Prevalencia de fragilidad en personas mayores de Chile: resultados de la Encuesta Nacional de Salud 2016-2017. Rev Med Chile. (2020) 148:1418–26. doi: 10.4067/S0034-98872020001001418
5. Thomas, DM, Crofford, I, Scudder, J, Oletti, B, Deb, A, and Heymsfield, SB. Updates on methods for body composition analysis: implications for clinical practice. Curr Obes Rep. (2025) 14:8. doi: 10.1007/s13679-024-00593-w
6. Barberán, MM, Campusano, MC, Trincado, MP, Oviedo, GS, Brantes, GS, Sapunar, ZJ, et al. Guidelines of the Chilean endocrinology society for the correct clinical use of bone densitometry. Rev Med Chile. (2018) 146:1471–80. doi: 10.4067/s0034-98872018001201471
7. Slart, RHJA, Punda, M, Ali, DS, Bazzocchi, A, Bock, O, Camacho, P, et al. Updated practice guideline for dual-energy X-ray absorptiometry (DXA). Eur J Nucl Med Mol Imaging. (2025) 52:539–63. doi: 10.1007/s00259-024-06912-6
8. Chapelon, J, Sourdet, S, Angioni, D, Steinmeyer, Z, Briand, M, Rolland, Y, et al. Body composition of older adults with normal body mass index. Cross-sectional analysis of the Toulouse frailty clinic. J Frailty Aging. (2025) 14:100003. doi: 10.1016/j.tjfa.2024.100003
9. Bloch-Ibenfeldt, M, Gates, AT, Jørgensen, NR, Linneberg, A, Aadahl, M, Kjær, M, et al. Heavy resistance training provides short-term benefits on bone formation in well-functioning older adults. Bone. (2025) 193:117393. doi: 10.1016/j.bone.2025.117393
10. Kannus, P, Haapasalo, H, Sankelo, M, Sievanen, H, Pasanen, M, Heinonen, A, et al. Effect of starting age of physical activity on bone mass in the dominant arm of tennis and squash players. Ann Intern Med. (1995) 123:27–31. doi: 10.7326/0003-4819-123-1-199507010-00003
11. Waza, NUD, and Deol, NS. Body fat and bone mineral density of endurance sports persons and resistance training persons. International conference of the Indian Society of Ergonomics; (2025). Springer; 97–102 p.
12. Goodenough, CG, Baedke, JL, Delaney, AM, Wilson, CL, Brinkman, TM, Im, C, et al. Attributable risk and consequences of bone mineral density deficits in childhood cancer survivors. JAMA Netw Open. (2025) 8:e2454069. doi: 10.1001/jamanetworkopen.2024.54069
13. Prabowo, NA, Soetrisno, S, Nurwati, I, Ardyanto, TD, Poncorini, E, Nurudhin, A, et al. Association between air pollution and osteoporosis: a systematic review. BIO Web of Conferences; (2025). EDP Sciences; 10004. 155.
14. Chen, R, Deng, Z, Yang, Z, Xu, J, and Liu, Z. Association between bone mineral density, sleep disturbance and sleep duration: results from observational and Mendelian randomization study. (2025) Available at: https://assets-eu.researchsquare.com/files/rs-5838245/v1/e3114723-966f-4be5-801a-2415a5ee308c.pdf?c=1737368698
15. Wang, LY, Liang, LM, Zhang, XX, Chi, H, and Peng, FL. Short bouts and long-term exercise reduce sedentary-induced bone loss and microstructural changes by modulating bone formation and resorption in healthy young male rats. Sci Rep. (2025) 15:1825. doi: 10.1038/s41598-024-82243-8
16. Mata, KJM, Chávez, JFA, Gallegos, LIF, and Hernández, GSIR. Metaanálisis del impacto de la actividad física en la salud ósea y muscular en mujeres postmenopáusicas. Retos. (2025) 62:777–86. Available at: https://openurl.ebsco.com/EPDB%3Agcd%3A14%3A20191774/detailv2?sid=ebsco%3Aocu%3Arecord&id=ebsco%3Agcd%3A182392072&bquery=IS%201579-1726%20AND%20IP%2062%20AND%20DT%202025&page=1&link_origin=scholar.google.com&searchDescription=Retos%3A%20Nuevas%20Perspectivas%20de%20Educaci%C3%B3n%20F%C3%ADsica%2C%20Deporte%20y%20Recreaci%C3%B3n%2C%202025%2C%20Issue%2062
17. Chen, R, Wang, S, Li, L, Zhang, H, Peng, X, Fang, H, et al. Association between physical activity energy expenditure and bone mineral density in US adults: a cross-sectional analysis of NHANES 2011–2018. Public Health. (2025) 240:195–202. doi: 10.1016/j.puhe.2025.01.026
18. Gao, J, and Li, Y. Relationship between muscle size and density and proximal femoral bone mineral density in elderly men with hip fractures across different age groups. J Orthop Surg Res. (2025) 20:162. doi: 10.1186/s13018-025-05570-0
19. Graybeal, AJ, Swafford, SH, Compton, AT, Renna, ME, Thorsen, T, and Stavres, J. Predicting bone mineral content from smartphone digital anthropometrics: evaluation of an existing application and the development of new prediction models. J Clin Densitom. (2025) 28:101537. doi: 10.1016/j.jocd.2024.101537
20. Turner, RT. Invited review: what do we know about the effects of spaceflight on bone? J Appl Physiol. (2000) 89:840–7. doi: 10.1152/jappl.2000.89.2.840
21. Hwang, H, Bae, J, Hwang, S, Park, H, and Kim, I. Effects of breath-hold diving on bone mineral density of women divers. Joint Bone Spine. (2006) 73:419–23. doi: 10.1016/j.jbspin.2005.07.005
22. Monnoyer, R, Haugum, K, Lautridou, J, Flatberg, A, Hjelde, A, and Eftedal, I. Shifts in the oral microbiota during a four-week commercial saturation dive to 200 meters. Front Physiol. (2021) 12:669355. doi: 10.3389/fphys.2021.669355
23. Bevier, WC, Wiswell, RA, Pyka, G, Kozak, KC, Newhall, KM, and Marcus, R. Relationship of body composition, muscle strength, and aerobic capacity to bone mineral density in older men and women. J Bone Miner Res. (1989) 4:421–32. doi: 10.1002/jbmr.5650040318
24. SUSESO. Superintendencia de Seguridad Social. Documento 16: Estudio observacional de buzos dedicados a la acuicultura 2014-2019. Centro de Estudios de Sistemas Sociales. Santiago, Chile. Marzo. (2020). Available at: https://www.suseso.cl/607/w3-article-586071.html
25. Petermann, F, Durán, E, Labraña, AM, Martínez, MA, Leiva, AM, Garrido-Méndez, A, et al. Factores de riesgo asociados al desarrollo de hipertensión arterial en Chile. Rev Med Chile. (2017) 145:996–1004. doi: 10.4067/s0034-98872017000800996
26. Petermann, F, Troncoso-Pantoja, C, Martínez, MA, Leiva, AM, Ramírez-Campillo, R, Poblete-Valderrama, F, et al. Asociación entre diabetes mellitus tipo 2, historia familiar de diabetes y deterioro cognitivo en adultos mayores chilenos. Rev Med Chile. (2018) 146:872–81. doi: 10.4067/s0034-98872018000800872
27. Díaz-Martínez, X, Petermann, F, Leiva, AM, Garrido-Méndez, A, Salas-Bravo, C, Martínez, MA, et al. No cumplir con las recomendaciones de actividad física se asocia a mayores niveles de obesidad, diabetes, hipertensión y síndrome metabólico en población chilena. Rev Med Chile. (2018) 146:585–95. doi: 10.4067/s0034-98872018000500585
28. Smith, NR, Ferraro, KF, Kemp, BR, Morton, PM, Mustillo, SA, and Angel, JL. Childhood misfortune and handgrip strength among black, white, and Hispanic Americans. J Gerontol B Psychol Sci Soc Sci. (2016) 74:526–35. doi: 10.1093/geronb/gbw147
29. WHO. Global physical activity questionnaire: GPAQ version 2.0. Ginebra, Suiza: World Health Organization (2009). Available at: https://www.who.int/es/publications/m/item/global-physical-activity-questionnaire
30. Guatibonza-García, V, Gnecco-González, S, Pérez-Londoño, A, Betancourt-Villamizar, C, and Mendivil, CO. A descriptive study of smoking, socioeconomic position, and health-related behaviors in urban Colombia. Discov Public Health. (2025) 22:22. doi: 10.1186/s12982-025-00405-z
31. Santos, CA, Maia, HF, Pitanga, FJG, de Almeida, MCC, da Fonseca, MJM, de Aquino, EML, et al. Hand grip strength cut-off points as a discriminator of sarcopenia and sarcopenic obesity: results from the ELSA-Brasil cohort. J Cachexia Sarcopenia Muscle. (2025) 16:e13723. doi: 10.1002/jcsm.13723
32. Marfell-Jones, M. J., Stewart, A. D, and de Ridder, J. H. (2012). International standards for anthropometric assessment. Wellington, New Zealand: International Society for the Advancement of Kinanthropometry. Available at: https://repository.openpolytechnic.ac.nz/items/cb3ad790
33. Marx, N, Federici, M, Schütt, K, Müller-Wieland, D, Ajjan, RA, Antunes, MJ, et al. 2023 ESC guidelines for the management of cardiovascular disease in patients with diabetes: developed by the task force on the management of cardiovascular disease in patients with diabetes of the European Society of Cardiology (ESC). Eur Heart J. (2023) 44:4043–140. doi: 10.1093/eurheartj/ehad192
34. Seo, J-Y, Ha, K-Y, Kim, Y-H, Kim, S-C, Yoon, E-J, and Park, H-Y. Bone mineral density and osteoporotic vertebral fractures in traditional, unassisted, free-diving women (Haenyeos). J Korean Med Sci. (2018) 33:e316. doi: 10.3346/jkms.2018.33.e316
35. Roelofs, EJ, Smith-Ryan, AE, Trexler, ET, and Hirsch, KR. Seasonal effects on body composition, muscle characteristics, and performance of collegiate swimmers and divers. J Athl Train. (2017) 52:45–50. doi: 10.4085/1062-6050-51.12.26
36. DeFronzo, RA, Gunnarsson, R, Bjarkman, O, Olsson, M, and Wahren, J. Effects of insulin on peripheral and splanchnic glucose metabolism in noninsulin-dependent (type II) diabetes mellitus. J Clin Invest. (1985) 76:149–55. doi: 10.1172/jci111938
37. Chapin, AC, Arrington, LJ, Bernards, JR, and Kelly, KR. Thermoregulatory and metabolic demands of naval special warfare divers during a 6-h cold-water training dive. Front Physiol. (2021) 12:674323. doi: 10.3389/fphys.2021.674323
38. Saraiva, BTC, Agostinete, RR, Freitas Júnior, IF, de Sousa, DER, Gobbo, LA, Tebar, WR, et al. Association between handgrip strength and bone mineral density of Brazilian children and adolescents stratified by sex: a cross-sectional study. BMC Pediatr. (2021) 21:207. doi: 10.1186/s12887-021-02669-1
39. Valente, AMM, de Almeida-Pititto, B, Archanjo Ferraro, A, Dias Folchetti, LG, Tande Silva, I, and Ferreira, SRG. Birth weight associated with dual energy X-ray absorptiometry-determined muscle–bone unit in young healthy women from the nutritionists’ health study. J Dev Orig Health Dis. (2021) 12:42–9. doi: 10.1017/S2040174419000874
Keywords: bone mineral density, blood pressure, cardiometabolic risk, diver, body composition, fat-free mass, handgrip, dual X ray absorptiometry
Citation: Véliz A, Pereira R, Dörner A and Álvarez C (2025) Bone mineral content determined by energy X-ray absorptiometry correlates with handgrip strength in Latin American divers. Front. Public Health. 13:1591242. doi: 10.3389/fpubh.2025.1591242
Edited by:
Mohammad Hossein Ebrahimi, Shahroud University of Medical Sciences, Shahroud, IranReviewed by:
Ricardo Valentim, Federal University of Rio Grande do Norte, BrazilSeyfullah Çelik, Ankara Yıldırım Beyazıt University, Türkiye
Gabriela Carrasco, University of Chile, Chile
Copyright © 2025 Véliz, Pereira, Dörner and Álvarez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristian Álvarez, Y3Jpc3RpYW4uYWx2YXJlekB1bmFiLmNs